Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Author: biomedicalopenaccessjournals
The only motto of Biomedical Journal of Scientific & Technical Research (BJSTR) Publishers is accelerating the scientific and technical research papers, considering the importance of technology and the human health in the advanced levels and several emergency medical and clinical issues associated with it, the key attention is given towards biomedical research. Thus, asserting the requirement of a common evoked and enriched information sharing platform for the craving readers.
BJSTR is such a unique platform to accumulate and publicize scientific knowledge on science and related discipline. This multidisciplinary open access publisher is rendering a global podium for the professors, academicians, researchers and students of the relevant disciplines to share their scientific excellence in the form of an original research article, review article, case reports, short communication, e-books, video articles, etc.
Tumors Originating from Fat Tissue in the Head and Neck Area: A Review of 40 Cases
Introduction
Lipomas, including spindle cell lipomas, pleomorphic lipomas, angiolipomas, lipoblastomas, and so on are benign tumors originating from fat tissue. Lipomas are the most frequently occurring benign tumors, and most lipomas arise subcutaneously. Liposarcoma is a malignant tumor consisting of a lipoblast. But, the degree of differentiation among all of these tumors are various, and the growth speed, metastasis, and prognosis of these tumors differ substantially by histological type. I therefore undertook this study to clarify the features of lipomas that had been operated on in Kitasato University Hospital (KUH) and diagnosed by reviewing a series of cases.
Materials and Methods
A. Ethical Consideration: patients included in this study were not subject to any harm. I ensured all patients had their privacy protected by ensuring anonymity of the data collected.
B. Study Design: A retrospective study of all patients who underwent tumor removal.
C. Setting: All patients having undergone tumor removal at Department of Otolaryngology-Head and Neck Surgery, KUH between January 2000 and December 2021. Patients were identified through pathology department records.
D. Participants: In each case, I recorded age, sex, pathological results, chief complaints, growth style, size, time until the first visit, primary lesion, treatment, complications and prognosis.
Results
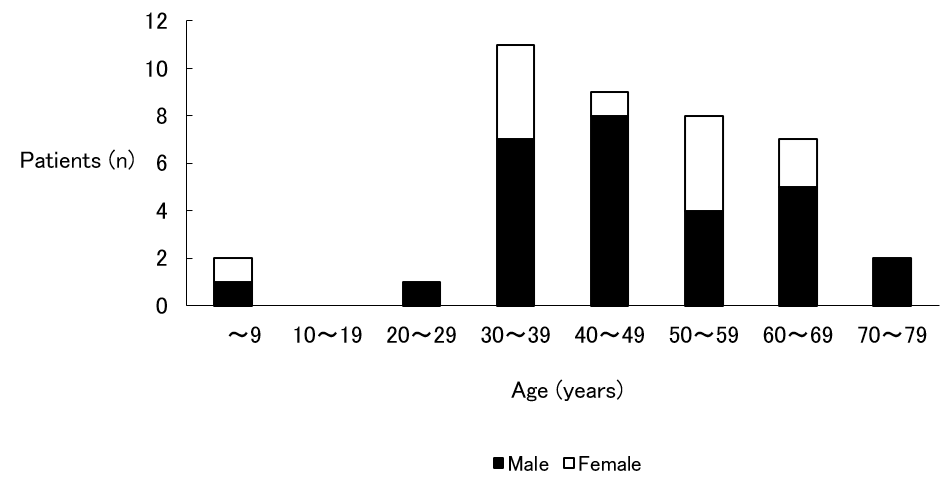
Age and Sex (Figure 1)
Figure 1: Age and Sex.
Note: Ages ranged from 2 to 80 years, and it was most common in the third decade of life. Sex difference was that male predominated.
Ages ranged from 2 to 80 years, with an average age of 47.1 years. Tumor removal was most common in the third decade of life. Sex difference: male (28 cases) and female (12 cases), so male predominated.
Pathological Results
Lipomas were benign in 38 cases (95 %) and malignant in 2 cases (5 %). One liposarcoma was a recurrent case; the other was a fresh case.
Chief Complaints
Swelling of the primary lesion without pain was observed in 37 cases (92.5 %). Swelling of the primary lesion with pain was observed in 1 case (2.5 %); this was a fresh case of liposarcoma. The remaining 2 cases (5 %) were asymptomatic and were accidentally found by image examination or by examination in another department.
Growth Style
Growth style was either unchanged (16 cases; 40 %) or slow (24 cases; 60 %). Two cases of liposarcoma were slow.
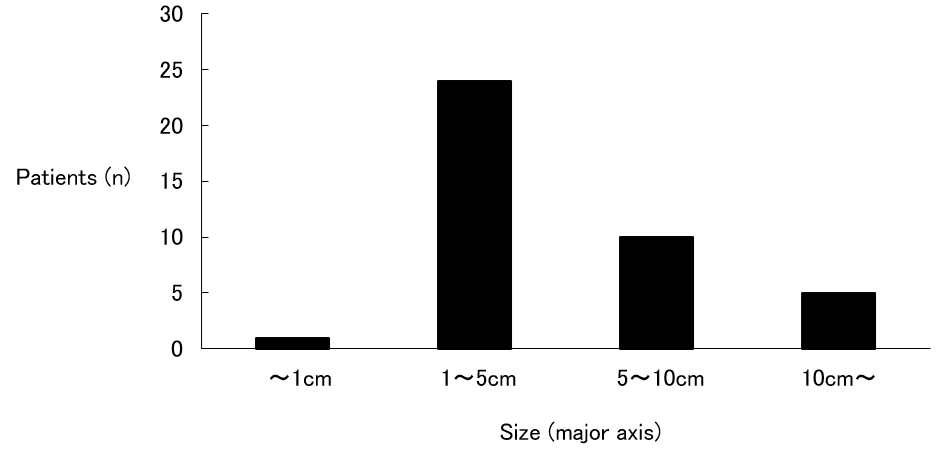
Size (Figure 2)
Lipoma size classes (along its major axis) were counted, and the following results were obtained: smaller than 1 cm (1 case; 2.5 %); 1 to 5 cm (24 cases; 60.0 %), the most common and accounting for more than half of all cases; 5 to 10 cm (10 cases; 25.0 %); and larger than 10 cm (5 cases; 12.5 %). The size of the recurrent case of liposarcoma was 6 cm, and the size of the fresh case was 11 cm.
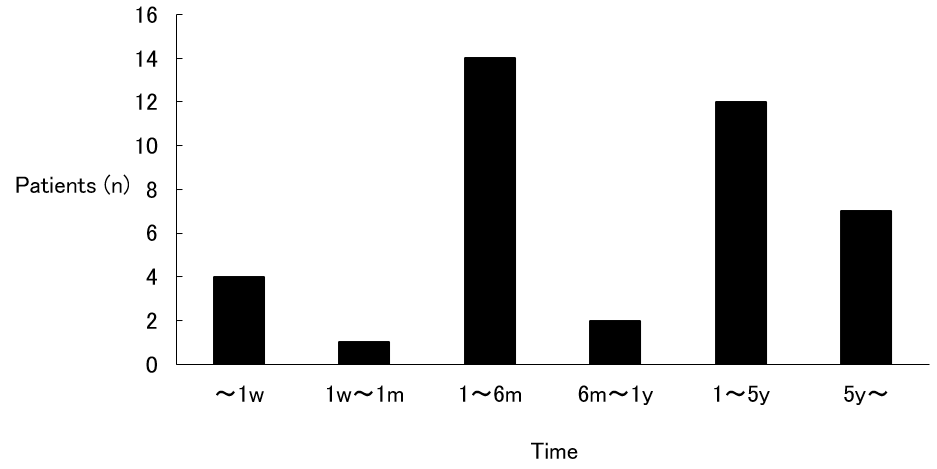
Time Until the First Visit (Figure 3)
A count of the times until the first visit to KUH was made, and the following results were obtained: within 1 week (4 cases; 10.0 %); 1 week to 1 month (1 case; 2.5 %); 1 month to 6 months (14 cases; 35.0 %), the most common; 6 months to 1 year (2 cases; 5.0 %); 1 year to 5 years (12 cases; 30.0 %); and over 5 years (7 cases; 17.5 %). There were 19 cases (47.5 %) that had been left for more than 1 year. In the recurrent case of liposarcoma, 6 days elapsed, and in the fresh case, 2 months elapsed.
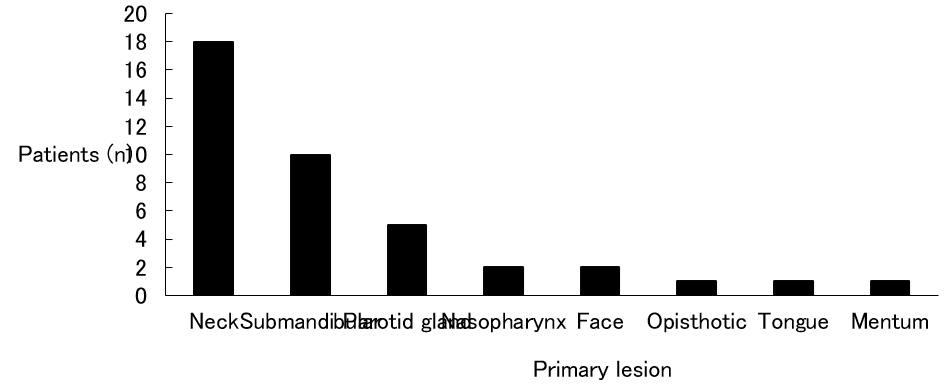
Primary lesion (Figure 4)
The neck was the most common with 18 cases (45 %) and was followed by the submandibular (10 cases; 25 %), the parotid gland (5 cases; 12.5 %), the nasopharynx (2 cases; 5 %), the face (2 cases; 5 %), the opisthotic (1 case; 2.5 %), the tongue (1 case; 2.5 %), and the mentum (1 case; 2.5 %). Laterality was right side in 27 cases (67.5 %) and left side in 10 cases (25 %), so the right side predominated. The remaining 3 cases (7.5 %) occurred at the nasopharynx and the mentum and were middle. Both cases of liposarcoma occurred at the right neck.
Figure 2: Size.
Note: 1 to 5 cm was the most common and accounting for more than half of all cases.
Figure 3: Time until the first visit
Note: Although 1 month to 6 months was the most common, there were 19 cases that had been left for more than 1 year. w: week, m: month(s), y: year(s)
Figure 4: Primary lesion.
Note: The neck was the most common with 18 cases.
Treatment
All 38 lipomas required only surgery. One of 2 liposarcomas was a recurrent case after surgery at another hospital. Dyspnea had occurred 1 week before the scheduled surgery date at KUH, and an emergency tracheostomy was performed. Surgery was still performed according to schedule 1 week later. In the fresh case of liposarcoma, because internal carotid artery was coarctated by the tumor, it was determined that surgery would be impossible. After a radiotherapy dose of 60 gray, insertion of superficial temporal artery catheter, and administration of 252.5 mg CDDP from the catheter, the tumor reduced. Therefore, surgery would be possible and was performed.
Complications
In cases of lipoma, 3 cases developed complications after surgery. One hemorrhaged after surgery and required a tracheostomy; another resulted in transient palsy of the marginal branch of the facial nerve; and the last resulted in transient palsy of the marginal branch of the facial nerve, fistulation, and an abscess at the wound.
In fresh case of liposarcoma, the recurrent laryngeal nerve (RLN) was involved in the tumor. Therefore, the RLN had to be cut and an RLN palsy occurred.
Prognosis
In the cases of lipoma, although postoperative results were varied and changing, there were no recurrences. In the cases of liposarcoma, the recurrent case died by another disease, and the fresh case is unknown because a change of address occurred. But, there were no recurrences or metastases during the follow-up period.
Discussion
Lipoma is a benign tumor that is composed of mature fat cells that grow relatively slowly. Pathologically, it is composed of crescentshaped and unevenly distributed nuclei, and round or oval cells that have monosegmental vacuolar cell bodies. It forms various sized lobules and is separated by narrow connective tissue. Lipoma is a soft globular or lobulated tumor by palpation, and there is almost no pain. Therefore, if there are no cosmetic problems or difficulties in daily life, patients tend to live for a long time. In this study, there were 19 cases (48.7 %) that lived for more than 1 year. Although treatment requires total removal, in some cases that lipoma grows not only subcutaneously but also inside requires partial removal [1]. The growth styles of all cases were unchanged and slow, and there were no complaints of pain in this study. Further, all patients could be totally removed, and there were no recurrences.
Although liposarcoma is one of the frequently encountered soft tissue tumors, liposarcoma in the head and neck area is rare (5.67 %) [2]. Pathologically, liposarcoma is composed of lipoblasts, and there are various differentiated types ranging from well to poor. Growth speed, metastasis, and the survival rate after 5 years varies markedly by differentiated type. Round cell types and pleomorphic types cause metastasis in the early stages, and prognosis is much worse. Differentiated type and mucous type have a low rate of metastasis, and prognosis is much better. Because the latter is greater than the former, liposarcoma is considered to be a tumor with a relatively better prognosis [3]. There were atypical nuclei abounding in chromatin and both large and small vacuolar and lipoblast cells here and there in the recurrent case. As to treatment, there is general removal and preoperative or postoperative chemotherapy and radiotherapy. Postoperative radiotherapy was not added in the recurrent case because the patient was in advanced age. Preoperative radiotherapy and chemotherapy were both performed in the fresh case. The recurrent case was pleomorphic type, and the fresh case was mucous type. Both cases did not cause recurrence and metastasis during the postoperative follow-up period.
Although differential diagnosis between benign and malignant tumors is based on biopsy, it is said that 10 to 15 % of malignant tumors have local pain or heat, clinically. Although the details of recurrent case were unknown, the fresh case did complain of pain. Further, although 2 liposarcoma cases did not perform computed tomography (CT) or magnetic resonance imaging (MRI) because they occurred in the early 1970’s, Ito, et al. [4] reported that both CT and MRI show lipoma as an almost isolated signal in subcutaneous fat. The margins are clear, and except for well-differentiated types, liposarcomas differ from fat and contain the part of CT is high density, T1 of MRI is low intensity and T2 of MRI is high intensity. Therefore, differential diagnosis between liposarcoma and lipoma is possible, but differential diagnosis between well-differentiated types of liposarcoma and lipoma is difficult.
Conclusion
Clinical files were reviewed for 40 patients who had been operated on and diagnosed as lipoma in the head and neck area. Ages ranged from 2 to 80 years, and the majority of patients were male. Lipomas were benign in 38 cases and malignant in 2 cases. Complications after surgery were seen in 3 cases. Although treatment requires total removal, in some cases require preoperative or postoperative chemotherapy and radiotherapy.
Correlation of Osteoarthritis of the Knee with Hypophosphatemia
Introduction
Phosphorus is an essential element in all living cells and has various functions [1-3]. The phosphate balance is a complex interplay between phosphate uptake and excretion. The extracellular to intracellular shift of phosphate and decreased reabsorption of phosphate in the intestinal tract and kidney are considered mechanism that cause hypophosphatemia [1,2,4]. Mild hypophosphatemia is relatively rare, and several causes may often overlap in patients with severe hypophosphatemia [5]. Familial tumoral calcinosis, X-linked hypophosphatemia (XLH), tumor-induced osteomalacia and chronic kidney disease are typical diseases that cause hypophosphatemia [6-10]. Although hypophosphatemia causes decreased bone strength in adulthood, it is not associated with the onset or progression of osteoarthritis (OA) of the knee. OA of the knee in relatively young patients is often secondary to previous trauma. We present the case of a relatively young patient with hypophosphatemia who underwent openingwedge high-tibial osteotomy (HTO) for OA of the knee.
Case
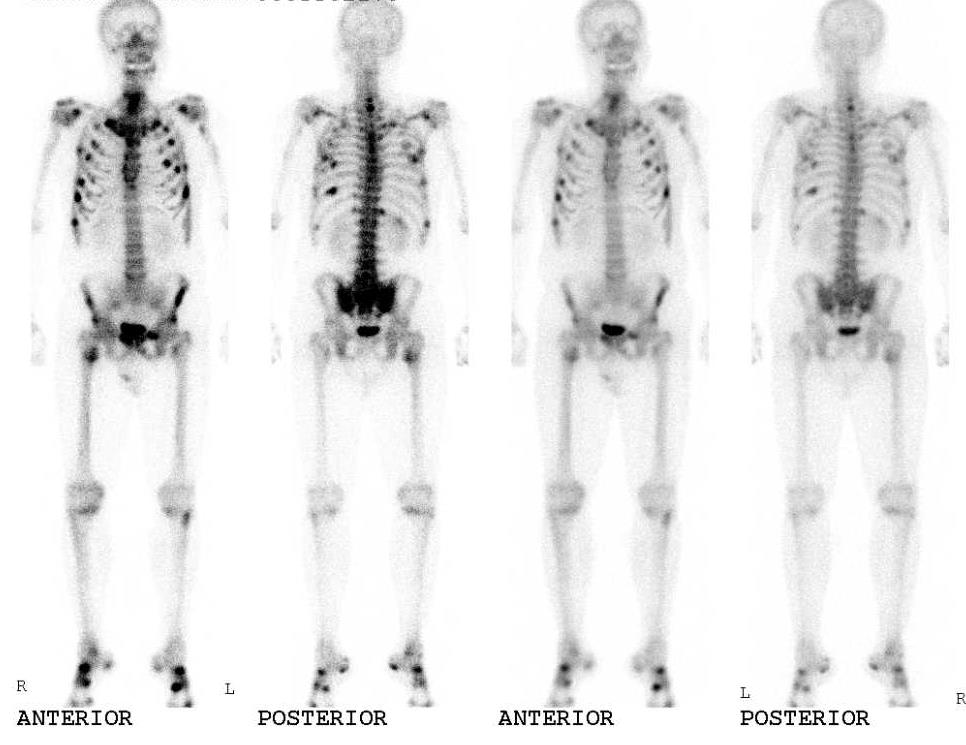
A 47-year-old man presented with progressive pain in the right knee and gait disturbance. The patient had developed progressive pain in his right hip five years previously, and laboratory test results had revealed a phosphate level of 0.58mmol/L. Bone scintigraphy had demonstrated high uptake of technetium-99m in many bones, including the proximal tibia (Figure 1). He was diagnosed with hypophosphatemia and was prescribed oral supplements of phosphate and vitamin D for the treatment of hypophosphatemia. Thereafter, he experienced relief in the hip joint symptoms. However, he developed progressive pain in the right knee four and a half years later. He was diagnosed with OA of the knee and received hyaluronic acid injections; however, the treatment was ineffective, and his right knee pain worsened. Therefore, the patient was referred to our department for surgery. He had a history of mild medial collateral ligament (MCL) injury in the right knee in adolescence. However, he had no symptoms in the knee until six months previously. The patient’s family history was unremarkable. Physical examination revealed swelling and tenderness of medial joint line in the right knee. The range of motion was from10° to 140°. The McMurray test for the medial meniscus showed negative results. The Hospital for Special Surgery (HSS) knee rating scale score was 74.
Figure 1: Bone scintigraphy had demonstrated high uptake of technetium-99m in many bones, including the proximal tibia.
Figure 2: Weight-bearing long leg plain film radiography showed Kellgren-Lawrence OA grade 2 and the anatomical lateral distal femoro-tibial angle (FTA) was 181°.
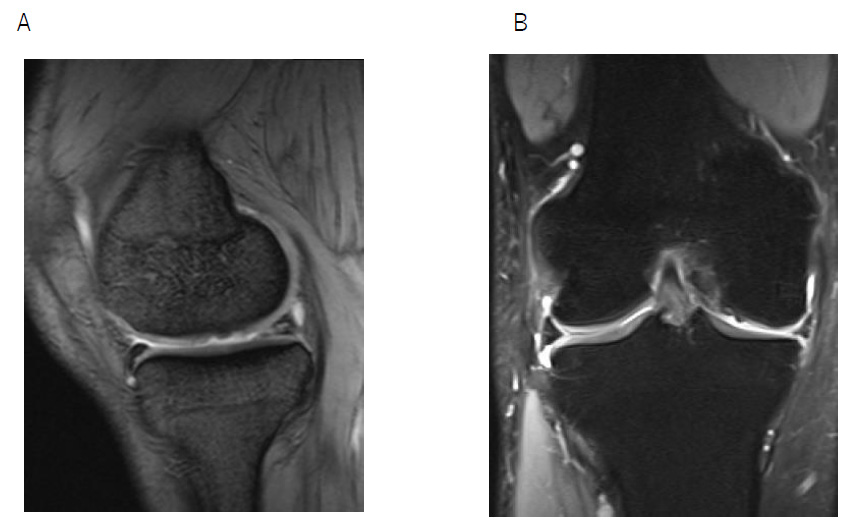
The Rosenberg view showed grade 2 OA according to the Kellgren-Lawrence classification, and the anatomical lateral distal femorotibial angle was 181° (Figure2). Magnetic resonance imaging revealed degeneration of the medial meniscus, slight joint effusion, an edematous area, and articular cartilage defect in the medial femoral cartilage (Figures 3A & B). The patient was diagnosed with OA of the right knee and opening wedge HTO was performed using TomoFix Japanese and a synthetic bone substitute (Figure 4). A knee brace was placed on the right leg for one week. In addition, the patient was instructed to avoid weight bearing for 1 week. Range of motion (ROM) exercises were started 1 week postoperatively. Full weight-bearing was allowed at 4 weeks. The bone fusion had been successful. At 18 months postoperatively, he had almost no symptoms in the right knee. The ROM was from 0° to 145°, and the HSS scale score was 97.
Figure 3: Preoperative magnetic resonance imaging (right knee)
A. T1-weighted image, sagittal view
B. T2-weighted, fat suppression image, coronal view.
Figure 4: Postoperative X-ray image.
A-P view
Discussion
In the musculoskeletal system, phosphate is associate with bone structure and striated muscle metabolism [11-13]. Hypophosphatemic osteomalacia causes bone deformities and growth and movement disorders during the growth phase. In adults, decreased bone strength causes fractures and pain [2,14]. Our patient developed mild hypophosphatemia in adulthood. Mild hypophosphatemia is not associated with the onset or progression of knee OA. In contrast, XLH typically causes hypophosphatemia. The most common symptom in adults with XLH is joint pain, which can be due to the development of enthesopathy and osteoarthritis, including thinning of the cartilage and sclerosis of the subchondral bone [3,6]. The Hyo mouse, a murine homolog of XLH, is known to have the same signs as humans with XLH, including hypophosphatemia [15]. Liang et al. reported that degenerative osteoarthropathy characterized by decreased articular cartilage thickness, increased chondrocyte alkaline phosphatase activity, defective mineralization, and vascular invasion of the cartilage, was prominent in these mice [14,15]. Therefore, degenerative osteoarthropathy may occur in patients with mild hypophosphatemia. Our patient had a history of an MCL injury in the right knee.
However, he had not experienced pain in the knee until six months prior to surgery. The past MCL injury might have been involved in the development of knee OA. With regard to the effect of hypophosphatemia to bone structure, bone scintigraphy demonstrated mildly elevated uptake of technetium-99m in both proximal tibiae. However, the patient had no symptoms in both knee until six months prior to surgery. Radiography revealed no deformity of the right proximal tibia. Thus, bone deformities that occur because of hypophosphatemia might not have been involved. Therefore, in our relatively young patient, degenerative medial meniscus changes and decreased articular cartilage thickness might be due to the past MCL injury and mild hypophosphatemia. Phosphate supplementation is indicated for the treatment of hypophosphatemia in symptomatic patients [16]. The safest mode of therapy is the oral route. Overzealous intravenous phosphate therapy for hypophosphatemia causes a precipitous decrease in serum calcium concentration. Liamis, et al. reported that oral phosphate can be administered as tablets of sodium or potassium phosphate at doses of 2.5-3.5g daily [17]. In our patient, hypophosphatemia was corrected with monitoring of serum phosphate levels and renal function, and mild hypophosphatemia did not affect bone fusion after HTO. Currently, 1200mg of phosphate and 3㎍of vitamin D are being administered orally, and the correction is under control.
Conclusion
HTO with successful bone fusion was performed in a relatively young patient with OA of the knee and hypophosphatemia. Past MCL injury and mild hypophosphatemia may be associated with the onset or progression of knee OA.
Using MRI Radiomics and Machine Learning Algorithms in Noninvasive Biopsy of Brain Tumor
Introduction
Brain cancer is diagnosed via samples acquired from a tumor biopsy. Since the 1970s, anatomical imaging methods (CT, MRI, PET/ CT, and PET/MRI ) have been employed for brain tumor diagnosis, treatment planning, and follow-up studies. Recent technology such as PET/CT and PET/MRI scanners created a significant quantity of detailed neuroimaging data in patients with brain tumors [1-3]. Using AI-based technologies may also speed up picture processing and analysis, enhancing productivity. Radiomics is a particular application within the vast subject of AI that involves computing, identifying, and extracting picture attributes. An overview of feature-based radiomics and machine learning algorithms in noninvasive biopsy of brain tumor using MRI image is presented [2,3].
Radiomics
Robert Gillies and colleagues provide a clear and concise description of radiomics. Radiomics is a high-throughput method that converts medical pictures into radiomics characteristics. This quantitative link may help improve early diagnosis and prognosis prediction in some illnesses, therefore enhancing treatment options. Radiomic analysis includes data gathering, segmentation, feature extraction, exploratory analysis, and modeling [4-6].
Data Selection and Image Preprocessing
Radiomics starts with digital imaging, and MRI is the most often utilized imaging modality; radiomics analysis can be performed on MRI, CT, PET, and ultrasound. Having enough imaging data is helpful for statistical inference, but variation in imaging procedures might impact the quality of retrieved features and radiomics models. Recent research shows that radiomics in MRI are substantially affected by image collection and reconstruction conditions, making them less reproducible. Many studies have demonstrated that many variations exist in radiomics, and preprocessing (normalization, voxel, and pixel resampling ) could improve and solve this problem [7,8].
Segmentation
Segmentation approaches are a crucial part of the radiomics process that separates a lesion from normal tissue. There are three types of segmentation (Manual, semi-automatic, and fully automated). Manual segmentation needs a skilled physician to reduce variability. It is attractive to use semi- or completely automatic segmentation to observe robust characteristics from a particular ROI [9,10]. Nowadays, machine learning softwares (3D-Slicer,Lifx, IBEX) can semi-automatically segment the lesion on MR images [6,11,12].
Feature Extraction
Numerous quantitative radiomics features, such as size and shape-based, histogram, matrix feature (run-length matrix (RLM), size zone matrix (SZM), gray-level co-occurrence matrix (GLCM), and neighborhood gray-tone difference matrix (NGTDM), wavelet feature base could be extracted from the medical images [8,10,12].
Feature Selection
All quantitative features collected from imaging data are not essential for predictive or prognostic models. Also, overfitting occurs when a created model closely fits the test data set; it makes the dependent model more susceptible to noise. Pre-selection of features reduces the probability of overfitting [5]. Radiomics uses both unsupervised and supervised reduction dimensions. The first methods try to remove unnecessary features; the two unsupervised feature selection approaches in radiomics are principal component analysis (PCA) and clustering [5]. There are three popular ways to reduce supervised feature sets:
Filter Techniques
Filter techniques often used include Wilcoxon rank-sum, Fisher score, Chi-squared score, Student’s t-test, and minimal redundancy maximum relevance [13-15]. These approaches investigate the full feature space, considering feature relations to other features in the dataset, and the prediction model is used to score a subset of characteristics [13,14].
Wrapper
Wrapper techniques are hence greedy algorithms. These are forward and backward feature selection, comprehensive feature selection, and search [14,15].
Embedded Approaches
Embedded techniques, mixed filter, and wrapper methods are more accurate than filter methods, quicker than wrapper methods, and less prone to overfitting data. (Regression, treebased techniques like random forest classifier, or the least absolute shrinkage and selection operator (LASSO)) [15-17].
Modeling and Evaluating
Depending on the study’s goal, after feature selection, a model may be created to predict tumor types, machine learning algorithms may develop predictive models. The decision trees and random forest are the most used radiomics algorithms for predicting tumor type. Creating and testing models on the same dataset is a methodological error that leads to overfitting; the train and test datasets and K-fold are in machine learning models can solve this problem [2,16,17].
Conclusion
Radionics is a new imaging biomarker that combines information from radiology, computer vision, and machine learning. With the growth of imaging examination datasets, emerging computational models, there are more demand to use radiomics biopsy in brain tumors. We think that novel diagnostic hypothesis in conjunction with machine-learning algorithms may improve predictive cancer diagnosis and speed up the practical use of quantitative cancer imaging data.
Biomedically Assisted Fertilization in the Republic of Slovenia
Biomedically Assisted Fertilization in the Republic of Slovenia
BMAF procedures are procedures to impregnate a woman using biomedical science to achieve conception by means other than sexual intercourse [1]. The BMAF procedure is regulated in detail by the Infertility treatment and procedures of biomedicallyassisted procreation act. As a general rule, BMAF procedures use the gametes of a man and a woman who are in a marital or cohabiting relationship, but if conception cannot be expected to occur using their gametes, the gametes of a male or female donor may be used [2]. The law provides that a woman and a man who are married or cohabiting and who, according to medical experience and professional opinion, cannot be expected to achieve conception through sexual intercourse and cannot be helped by other infertility treatments are eligible for the BMAF procedure. They are also entitled to the procedure if the procedure can prevent the transmission of a serious hereditary disease to the child [3]. The spouses or cohabiting partners must be of full age, of sound judgement, of suitable age and in such a psychosocial state that they can be expected to be able to perform their parental duties [4].
A woman who intends to give her child to a third party after birth, whether for payment or not, is not eligible for BMAF [5]. Nor may payment or any other benefit be given or accepted for donated gametes, except reimbursement of travel expenses incurred by the donor in coming to the BMAF centre [6]. The referendum on the amendment to the Infertility treatment and procedures of biomedically-assisted procreation act (ZZNPOB), which was rejected in 2001, also rejected the possibility of simultaneous use of biomedically-assisted donated gametes for infertile couples, artificial insemination for single women, and, consequently, the possibility of surrogacy in Slovenia [7].
Legal Regulation in the Republic of Slovenia
Article 55 of the Constitution of the Republic of Slovenia, as the fundamental and hierarchically supreme legal act in the country, stipulates that in Slovenia the decision on the birth of children is free and that in order to exercise this freedom, the state shall provide opportunities and create conditions that enable parents to decide on the birth of their children [8]. Infertile couples can become parents through biomedically-assisted fertilization procedures (BMAF) or adoption. While surrogacy is not directly prohibited, the prohibition of biomedical assistance in its implementation makes it impossible in practice [9]. Surrogacy is summarized in Article 7 of the ZZNPOB, which stipulates that a woman who intends to give her child to a third party after birth, whether for payment or not, is not eligible for BMAF. Sanctions are laid down in the Infertility treatment and procedures of biomedically-assisted procreation act in Article 43 [10]. The Criminal Code provides for a prison sentence of up to three years for anyone who unlawfully implements a BMAF procedure for surrogacy, in Article 121(4) in conjunction with Article 121(3) of the Criminal Code [11].
Surrogacy is also defined in Slovenia in the Code of Medical Ethics, which states in Article 24 that in the case of reduced fertility, the doctor shall offer counselling and the reasonable use of biomedical treatment procedures to those affected. Surrogacy is not allowed [12]. “Although it is not explicitly prohibited by Slovenian law, it is not possible to implement it in practice [13].” Article 112 of the Family Code defines a mother as a woman who has given birth to a child [14]. This definition also makes surrogacy legally impossible, since the mother of the child will therefore always be the woman who gave birth to it.
Establishing Parentage in a Biomedically-Assisted Fertilization Procedure
Biomedically-assisted fertilization is regulated by the ZZNPOB, while the parentage of children born during the procedure is regulated by the Family Code. Spouses or cohabiting partners who are of full age, of sound judgement, of suitable age and in a good psychosocial situation to be able to perform their parental duties are eligible for a biomedically-assisted fertilization procedure [15]. The BMAF procedure shall be carried out with the partners’ gametes or with one gamete from the partner and one donated male or female gamete. Donation of both gametes or donation of an embryo is not allowed. A child conceived with biomedical assistance must genetically descend from at least one person in the couple requesting the BMAF procedure [16]. If the child is conceived with an ovum from a donor, then her maternity cannot be established [17]. The mother of a child conceived with a BMAF procedure is the mother who gave birth to the child. This applies in both cases – if she is the genetic mother of the child, and also if she is not the genetic mother of the child. If the mother has given her consent to the procedure, she has thereby assumed the duty of care for the child [18].
The father of a child conceived with biomedical assistance is the mother’s husband or her cohabiting partner, who has formally consented to the BMAF procedure. The father is considered to be the father whether or not he is genetically related to the child. No one is allowed to establish the paternity of the donor, who must remain anonymous [19]. The child may, for medical reasons, request the competent centre to provide them with medically relevant information about the donor. He may do so if he is at least 15 years old and is capable of understanding the meaning and legal consequences, i.e. is of sound judgement [20]. In this case, the Slovenian legislation therefore restricts the child’s right to know their origin. Although the Constitutional Court of the Republic of Slovenia has not yet encountered in practice the question of the rights of a child conceived with biomedical assistance, it is questionable whether the provision in question would survive a constitutional review. The Court has in the past already ruled on the right to know one’s origins, which it classifies as a constitutionally protected right.
Even if Slovenia were to enact an open regime, the fear that this might lead to a reduction in the number of donors would certainly be unnecessary. The law excludes legal and other obligations or rights of the donor towards the child [21]. As already mentioned, one of the key elements for the development of an individual’s personality is the knowledge of one’s origins. If an individual does not know it, this can be a serious burden and uncertainty [22]. A German court decision that upheld the claim of a woman who was conceived with the BMAF has caused quite a stir. She had asked for information about her biological father to be disclosed. The Court was confronted with a clash of two rights, and judged primarily on the basis of the case-law of the German Constitutional Court, which had previously taken the view that the right to know one’s origins enjoys constitutional protection. In its judgement, the Court also considered the applicant’s interest in knowing her biological father and any half-brothers or half-sisters, as well as hereditary diseases. The Court also considered the rights of the donor and the clinic in the specific case. Given that the donation of gametes is anonymous, the donor could not have foreseen the possible legal consequences (inheritance, maintenance). However, weighing up the interests of all parties, the Court held that the child’s right to know their origins was paramount, since knowledge of biological parents is central to the development of the child’s personality [23-27].
Conclusion
The beneficiaries of the BMAF procedures in Slovenia are married or cohabiting couples who are unable to achieve a pregnancy through natural means or other procedures, and therefore the circle of beneficiaries can be said to be narrow, as the ZZNPOB does not allow the biomedically-assisted fertilization procedures for single women and same-sex couples. The problem in Slovenia arises in the case of donated gamete procedures, as there are too few donors, so the waiting times for donated gamete procedures are unacceptably long and many couples would no longer be ageappropriate if they were to wait for donated gametes in Slovenia. We believe that Slovenia should move with the times and broaden the range of those eligible for BMAF, as same-sex couples and single women can also meet the criteria of best interests of the child. Discrimination in this area should be eliminated on the basis of the right to free choice in childbirth, the principle of equal treatment and the principle of equal opportunities.
SNP Genotyping Enhancements: From Traditional PCR to Double Helix Structural Oligonucleotides (STexS)
Introduction
As the Human Genome Project was accomplished, series of subtle variations of polymorphisms were reported within the population [1,2]. Among the various types, single nucleotide polymorphisms (SNPs) are known as the most abundant, with more than 9 million reports in the public databases [3,4]. In a molecular aspect, SNPs are nucleotide alterations at a specific region in the genome. While the term is applied to nucleotide replacements, SNPs can be broadened with biallelic variations such as insertions, deletions, and allele frequencies less than 1% [5,6]. SNPs generally occur around one per 1000 bp within the human genome [7]. However, the distribution is not even, as SNPs tend to cluster in noncoding regions more than several hundred folds compared to actual coding regions [8]. In hindsight, SNPs located in the noncoding region may be neglected. But various reports soon regarded both locales as an important region in disease developments and other genetic malfunctions [9,10]. As more SNPs were found to be an important overlap in certain conditions, it soon served as a crucial genetic or pharmacogenetic marker for future practices. The reason for such importance lies on which specific region, coding or noncoding, the SNPs are found. Even though noncoding regions do not contribute to protein coding, regulatory sites with SNPs can affect transcription rates, which alters the overall production of protein encoding. This process later triggers malfunctions that may develop disorders and various cancers [11-13].
As important the SNPs were known for molecular, pharmacogenetic, and cancer targets, so too did the importance to accurately depict and sort out targeted SNPs from normal, far more abundant gene strands. A common approach for this identification is a patient-control study involving large SNP genotypes in patient groups and healthy control populations to compare genotypes differences for all phenotypes under study. And the relationship between specific genotypes and phenotypes characterizes diseaserelated sensitive genes and is used to find encrypted proteins for disease prevention and treatment. Another major application in which SNP is used as an indicator is pharmacogenetic approaches [14-16]. Because the vast population size of the cohorts, discovering valuable SNPs that mark a specific disorder is rather trivial. However, the hurdle has been elevated as treatments shifted from prognostic to predictive medicine. While patients who already developed severely will inevitably have high portions of SNPs which indicates the disease, normal or soon to develop potential cohorts will have very low abundance which in some cases are not detected by previous methods [17,18]. Other reports indicate patients having false negative results in a certain detection test which results in failure to prevent further disease development or early treatments [19]. As technology developed, the method to efficiently detect SNPs also enhanced. The most common and efficiently known method is the utilization of Polymerase Chain Reaction (PCR).
Hence, the overall format regarding the use of PCR has not been replaced. The improvements were acquired by usually two ways; enhance the efficiency to estimate relative amplification rates or apply adjustment reagents to further boost the amplification rate of the targeted DNA template [20,21]. The method to elevate relative amplification rates was achieved through quantitative PCR (qPCR) [22]. Further enhancements to effectively sort out and specifically amplify targeted SNP templates were done by adding allelespecific primers, reagents which clamp unwanted DNA templates, or utilizing hydrolysis probes for melting curve analysis [23,24]. Many attempts to improve the detection rate of targeted SNPs bore fruit but was not complete. Because certain DNA strains would still attach the allele-specific primers and result in false positive misdiagnosis [25]. In order to achieve early detection of a target SNP while not binding with the normal DNA strand, novel approaches were needed. In this review, we address the methods of known SNP specific amplification methods and the recently introduced double helix structural oligonucleotide added PCR (STexS) [26].
Traditional SNP Genotyping Technologies
Figure 1: Basic schematics of the “HotStart” PCR.
SNP genotyping generally regards generations of allele-specific templates commercially or custom-made to increase amplification of wanted SNP-containing genes. The continuous efforts to manufacture efficient primers lead to many discoveries of genes which associates with a specific disorder such as Myeloperoxidase, N-acetyltransferase 1, and N-acetyltransferase which affects cancer susceptibility in Lung cancer, Bladder cancer, and colon cancer [27]. Other discoveries include SNPs located in CYP3A4 leading to prostate cancer and Thiopurine S-methyltransferase which SNPs alter the pharmacokinetic effects of anticancer drugs [28]. Although the roles of genes with certain SNP types were found, the method to effectively detect such allele in drastically low abundant patients were consistently held back due to limitations. The major limitation was nonspecific binds of normal DNA strands leading to primer template mismatches, resulting in false-positive detections to personnel who has the potential to develop the disorder. The “HotStart” PCR was a method to overcome such nonspecific amplifications by increasing temperature during the annealing process (Figure 1) [29]. However, SNPs consisting less than 1% in a clinical sample required something more sophisticated to discriminate normal DNA. The recently introduced STexS PCR platform combines the concept of “HotStart” PCR and allele-specific primers and further restrains nonspecific binds using a known method called amplification refractory mutation system-PCR (ARMS-PCR) [30]. ARMS-PCR is meant to detect any mutation involved single nucleotide changes including insertions and deletions [31]. This method greatly improves the efficiency to sort mismatched primers, but ARMS-PCR alone declines the amplification rate drastically below the limit of detection tampering the overall SNP genotyping.
The Implementation of Oligonucleotides
Oligonucleotides has been used alongside the standard PCR for various purposes including SNP detection [32,33]. Oligonucleotides are used as a probe to detect a specific sequence that are complementary to the oligonucleotides. Because it is mainly consisted of a relatively short 12~25 nucleotide, it is also referred as primers in a conventional PCR for detecting and multiplying wanted complementary gene targets. Oligonucleotides are majorly single stranded, thus when performing PCR, both forward and backward templates of a targeted template is required for maximum efficiency. However, in SNP detection, nonspecific bindings of mismatched gene strands lead to misleading results. While the process to completely block the large portion of normal genes to be amplified is a challenge, giving the targeted SNP strand enough cycles to amplify firsthand by delaying mismatched DNA copies will make enough difference to successfully perform SNP genotyping.
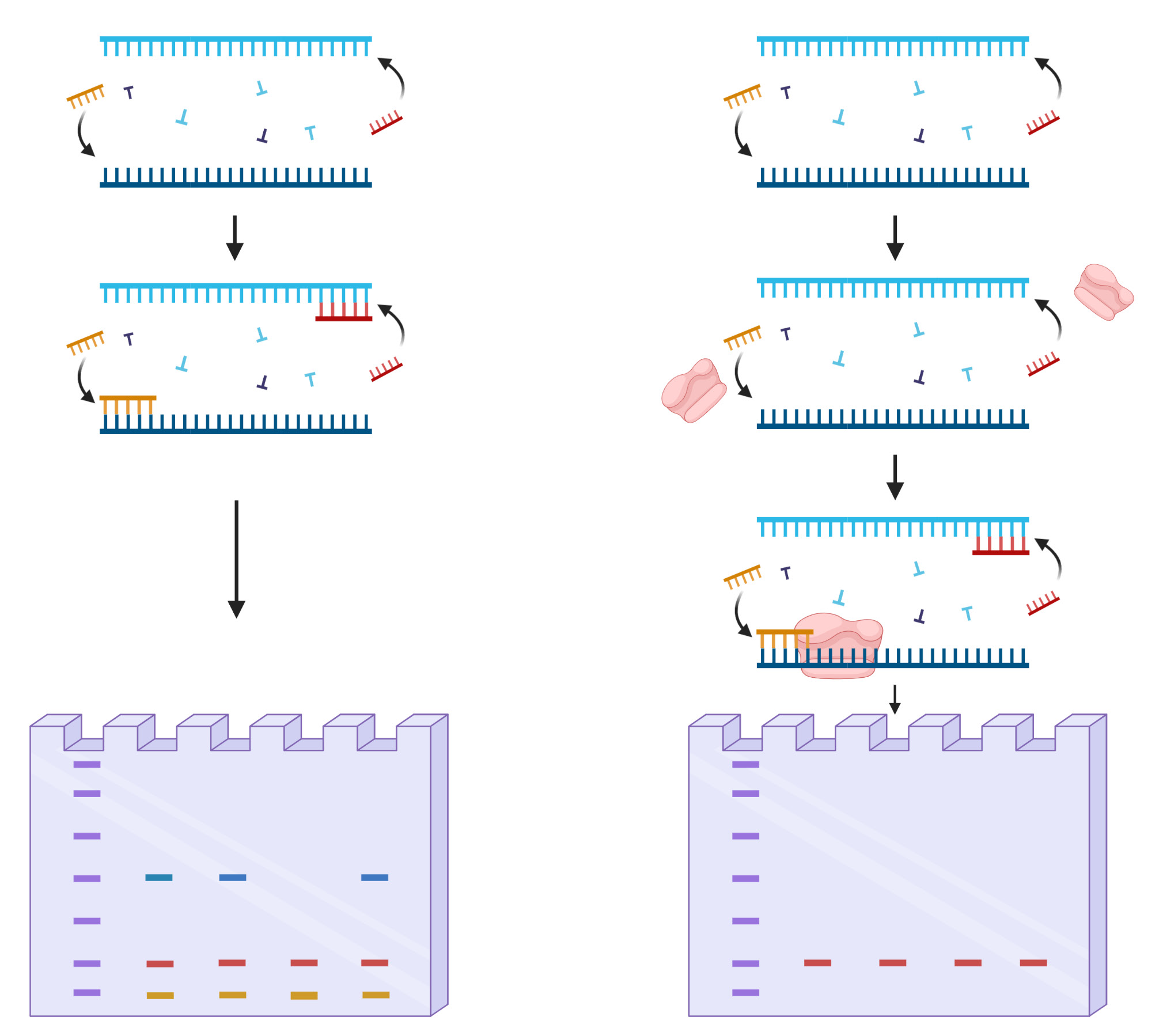
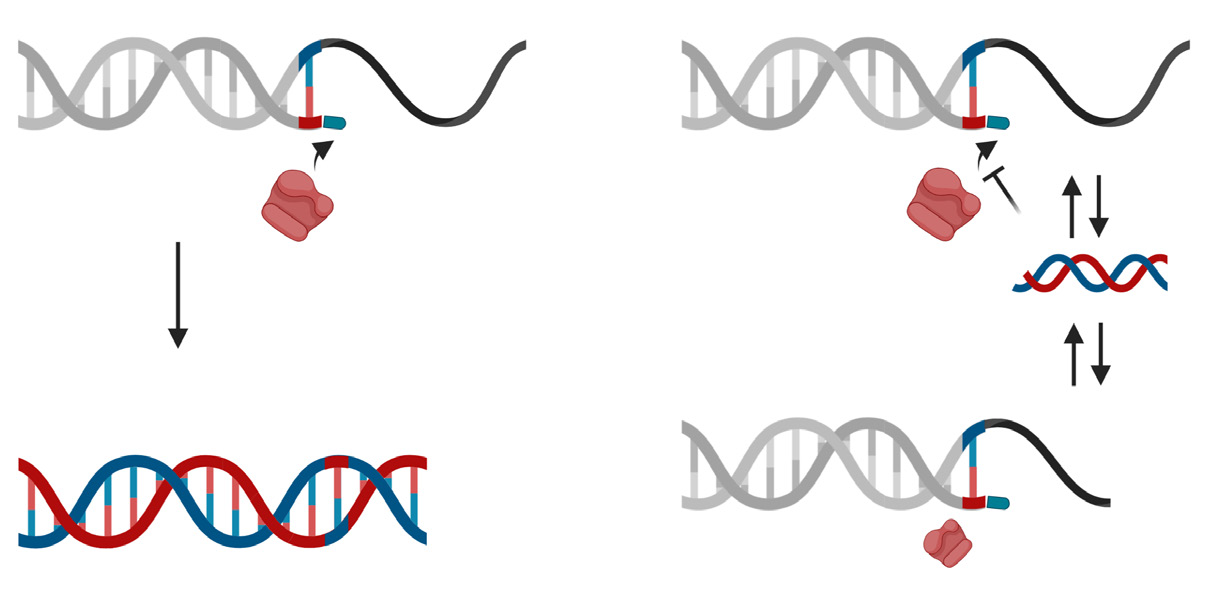
The STexS platform mentioned above uses a double helix forming oligonucleotide (discrimination boosting oligonucleotide, dbOligo) to fully utilize the concept of disrupting mismatched amplification. The annealing process is mainly contributed by the DNA polymerase (DNAP) that synthesizes matched or mismatched strands to a complete gene template, which in turn acts as an additional template for amplifying [34]. While intended matches of dbOligo does not boost or block the amplification rate compared to other commercially used primers, the kinetic energy of DNAP to attach and detach mismatched primers dwindles, resulting in a constant unstable state that ultimately delay the overall process of amplification (Figure 2). Combining with the “Hotstart” method, each dbOligo is deliberately designed to be at least 10 base pairs to adjust the annealing temperature to further block nonspecific bindings and primer dimers. Validation through previously reported SNPs contributing to several cancer types showed a reasonable contrast between matched and mismatched templates, further proving the importance of STexS method (Table 1).
Figure 2: Difference of mismatched amplification between conventional PCR and STexS PCR.
Table 1: SNP targets of different cancer and amplification difference between matched and mistmached DNA.
Conclusion and Future Directions
The ability to sort out even one mismatch between two different DNA strands is a fundamental technology not only limited to PCR techniques, but to other molecular extents. Fully discriminating matched targets from unwanted mismatched strands will also lead to improved specificity and sensitivity. Current diagnostics with various arrays and detection kits are challenged not just with its rate of success, but also constant incidents of false negatives misleading practitioners to judge poorly [35,36]. The importance of not neglecting cases of false negatives drastically increased, as contagious viral infections tend to spread among patients who cannot be scanned with conventional methods [37-39]. The recent spread of SARS-CoV-2 influenced generations of detection methods to effectively tackle and contain infections from further progression. However, due to the rapid mutation of the virus’s nature, the ongoing struggle seems to go ever on [40]. The STexS will definitely serve as a suitable bedrock for future detections arrays. Not just with currently known lethal mutated variants, the STexS platform can successfully detect hundreds of variants regarding both precedented and novel, hazardous and non-lethal but with potential to develop. Future applications for the STexS will be focused not only with SNPs related to early cancer detection, but also in precise diagnosis of the ongoing COVID-19. Further, the technology will improve molecular biology and medical science and reshape the current health care industry.
Biological Action of Sesterterpens. The Mini-Review
Introduction
Sesterterpenes represent the small terpenes group, which is allocated from different organisms and possesses by various biological properties, including such as anti-inflammatory, antimicrobes and anti-tubercular. Some sesterterpenes possess by multipurpose properties. For example, manoalid possesses by anti-inflammatory and anti-microbes actions [1,2]. According to Plemenkov [3] existing types with a biological action has being classified as two groups: native and gotten. In turn he divided the native properties on ecological, which include the properties of the first level providing the ability to live of an organism (for example, hormones) and also on the properties of the second level, which are carrying out functions of the chemical communications (for example, pheromones) and also on the benefit performance properties, which are used by the person for own needs: perfume, solvents, medicinal substances of a wide action spectrum etc. Separately he has allocated the gotten properties, which exist by the directed chemical updating of terpenes to produce the substances possessing the target pharmacological or other functions. It is necessary to notice that sesterterpenes are the poorly studied class of terpenes substances origins before their availability is limited. Behind some exception, they are received from marine organisms.
Therefore, the some complexities to obtain them are aroused. A biological activity of sesterterpenes in this fact is studied; first, pour but to use them directly in the practical purposes, i.e. according to the benefit performance properties by them. It is important that many sesterterpenes can suppress the growth of cancer cages in vitro, and it is the cause why they are considered as perspective candidates on antineoplastic preparations [1,2,4]. However, their functional mechanisms are insufficiently studied for today. Sesterterpenoids usually contain carbon skeletons C-25. Nevertheless, some its connections contain from C-21 to C-24 and they are grouped on the subgroup named nor-sesterterpenoids [1,2]. At present, all of them have been allocated from land mushrooms, lichens, the higher plants, insects and various marine organisms, but especially from marinesponges [2,5]. According to the degree of a cyclization, the molecular structures are classified on 5 subgroups, such as acyclic, mono-, bi-, tri- and tetracyclic [2,4,6].
In each subclass, the substances possessed by a different cytotoxic activity have been revealed. Besides, for acyclic sesterterpenes one found the antiprotozoan activity [7,8], for the mono- and bicyclic sesterterpenes – one found the anticancer activity [9,10], for the tricyclic sesterterpenes – one found the anticancer and antibacterial activity [11,12], for the tetracyclic sesterterpenes – one found the anticancer and antibacterial activity [13-15], also the antitubercular activity [16] and antivirural [17] activity and ichtiotoxic activity [18] has been revealed. For example, two acyclic sesterterpenes Ircinins-1 and-2 were isolated from Ircinia oros, the antiprotozoan activities of them [8] where found out in vitro. The monocyclic sesterterpene Acantholide A was isolated from Hyrtius communis [9], – it possesses by anticancer action and it inhibits the HIF-1 activity [IC50 of 7.1 μM (Cl of 6.7- 7.8 μM)]. Bicyclic sesterterpene Phorone B was isolated from Clathria gombawuiensis [19], – it possesses by the anticancer action and it was moderately active against the K562 and A549 celllines. Tricyclic sesterterpene Coscinolacton A was isolated from Coscinoderma sp [9], – it is awake against a line of cancer cells K562 and A549 with moderate cytotoxicity [IC50=0.95, 5M].
Another tricyclic sesterterpene Ophiobolin W was isolated from Aspergillus ustus [12], – it possesses by the inhibiting activity against Escherichia coli, Staphylococcus aureus and Artemia salina. Tetracyclic sesterterpene perisomalien A was isolated from Periploca somaliensis [20], and the cytotoxic activity of its metabolites was assessed towards MCF-7, HepG2, and HCT-116, which possessed the most potent effect towards HepG2 with IC50s 26.7 μM. Another tetracyclic sesterterpene Ansellone C was isolated from Clathria gombawuiensis [21], – it possesses by the moderate antibacterial action against gramme-positive and gramme-negative bacteria. Thus, because a raw-material base is low available, the biological researches of sesterterpenes were made to study their pharmacological properties of anticancer and antimicrobial directions pour but to apply them as possible proximately in practice.
A Randomized, Blinded, Calcium-Carbonate Controlled Cross Over Study of Serum Calcium Levels 24 Hours After CalGotm Oral Supplementation in Post- Menopausal Women
Introduction
Bone metabolism is a dynamic process between bone formation and bone resorption. In the formative years bone mass density progressively increases and a peak is reached in humans in the third decade of living [1]. From this point onwards bone resorption exceeds bone formation resulting in a gradual loss of BMD of 0.5-1.0% per year, and a concomitant deterioration of the bone microarchitecture. This eventually leads to osteopenia and osteoporosis [2,3]. Osteoporotic related fractures affect hundreds of millions of people and is a major health problem worldwide [4]. To put the burden of osteoporosis and fragility fractures into perspective, in Europe, fragility fractures cause a greater impairment of function compared to most types of cancer and is a leading cause of morbidity resulting from chronic disease [5]. Today the chronic treatment of osteoporosis aims to reduce bone resorption rather than to increase the rate of bone formation. Calcium supplementation has been a cornerstone in these attempts to prevent loss of BMD, as reflected in reports that more than 40% of Americans regularly take calcium supplementation [6]. However, calcium supplementation has not delivered the desired effect in preserving bone mass and preventing frailty fractures [7]. A review of 33 clinical studies found that supplementing with calcium, vitamin D, or both, failed to reduce fracture risk among otherwise healthy elderly individuals [8].
Fish bones have a high calcium content, and large quantities of this raw material are available as a by-product from the aquaculture industry. Fish bones have been previously described as an alternative to standard calcium carbonate supplementation [9]. Studies indicate that fish bone calcium induces bone biological activity, increasing bone formation. The investigational product in this current trial (CalGo™, produced by HBC) is derived from offcuts of salmon filet production, and contains 60% calcium salts, primarily in the form of natural hydroxyapatite (nHAP) and 36% protein, mainly Collagen. Studies have shown that the intake of Collagen has a positive effect of increasing BMD in several in-vivo bone growth models [10]. CalGo™ has also shown an osteoinductive effect by increasing osteoblast activity in-vitro [11] and in-vivo [12]. The main aim of this study was to investigate the serum level of calcium in healthy postmenopausal woman 24 hours after a single dose of CalGo™.
Material and Methods
Study Design and Study Subjects
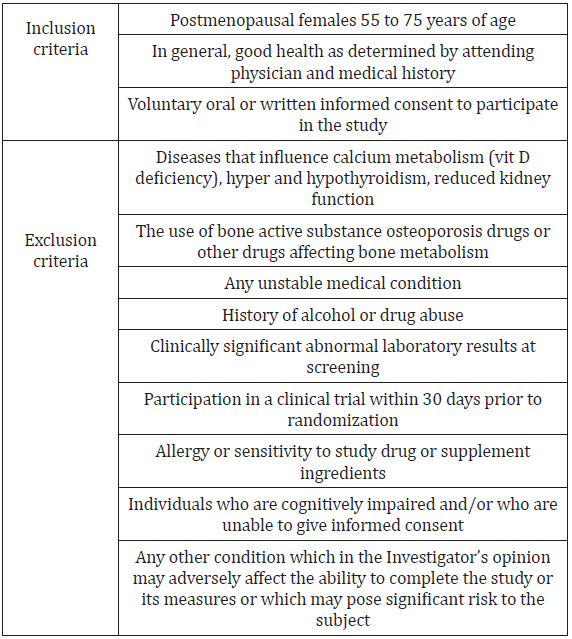
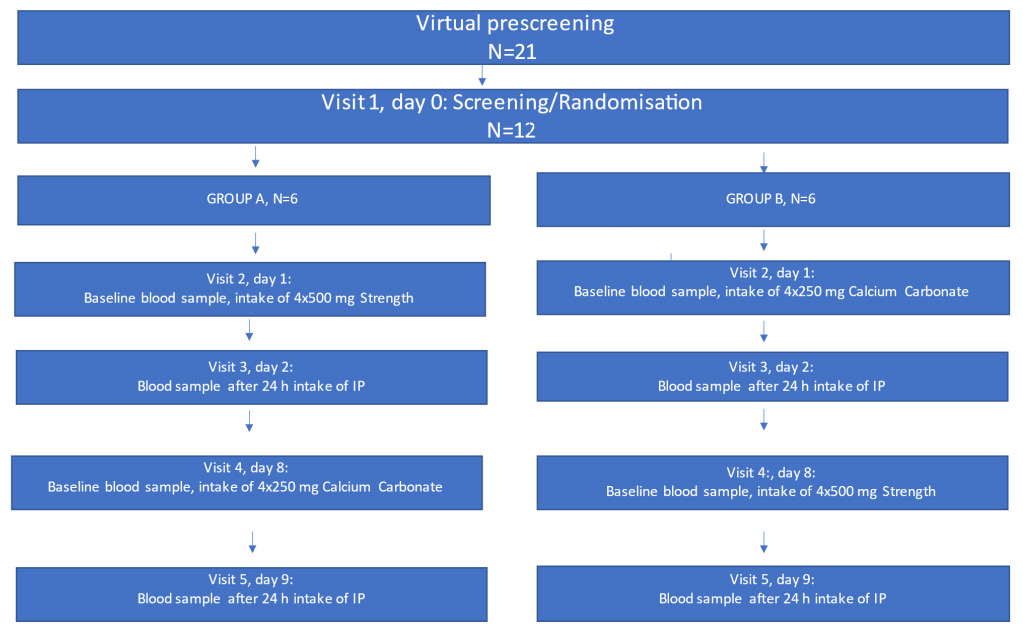
The present study was carried out at PGH Orthopedic & Urology Clinic, Mumbai, India. The study was designed as a randomized controlled, double blind, crossover study. The study-subjects had five study visits (Figure 1). At the first visit (day 0) they were randomized, using Research Randomizer (www.randomizer.org), into either Group A or Group B. The inclusion and exclusion criteria are given in (Table 1). A total of twenty-one subjects were assessed for inclusion, and twelve postmenopausal females between 55- 75 years of age met the eligibility criteria and were included. All subjects who were included completed the study. A standard 1g dose of calcium carbonate was selected and the dose of CalGo™ was calculated to deliver an equivalent quantity of elemental calcium. Both tablets were of similar appearance and size. Group A was given 4×500 mg CalGo™ at visit 2 (day 1), and their blood sampled at visit 3 (day 2). At visit 4, which followed a 7-day washout period (day 8) they were given 4×250 mg calcium carbonate, and the last visit 4 (day 9) the second blood samples were collected.
Table 1: Inclusion and exclusion criteria.
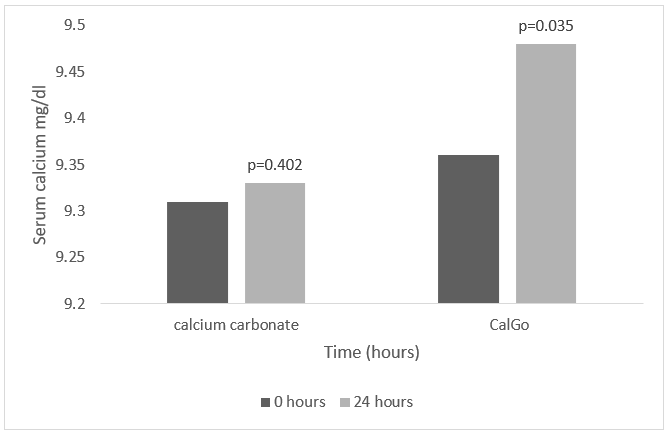
Figure 1: Serum calcium changes over 24 hrs.
Group B was given 4×250 mg calcium carbonate at the visit 2 (day 1), and then blood samples at visit 3 (day 2). At visit 4, after 7 days of washout (day 8) they were given 4×500 mg CalGo™, and the last visit 4 (day 9) the second blood samples were collected. All subjects were fasting 8 hours before visit 2 and 4. Blood samples were collected at baseline and at each follow visit, and the samples analyzed for serum calcium (Arsenazo method), serum creatinine and serum calcefidiol. Safety was assessed at every visit, and each subject was specifically asked about nausea, headache, and racing pulse at every visit. All subjects were provided with information of the purpose, procedures and risks with the study, and informed consent was obtained.
Statistics
The statistical analysis of the data was performed using a paired one-tailed Student t-test. All values are reported based on paired, one-tailed significance with p < 0.05 being statistically significant (95% confidence level).
Statement of Compliance
This study was conducted in compliance with the “Guideline for Clinical trials on Pharmaceutical Products in India-GCP Guideline” issued by the Central Drug Standard Control Organization, Ministry of Health and Government of India.
Results
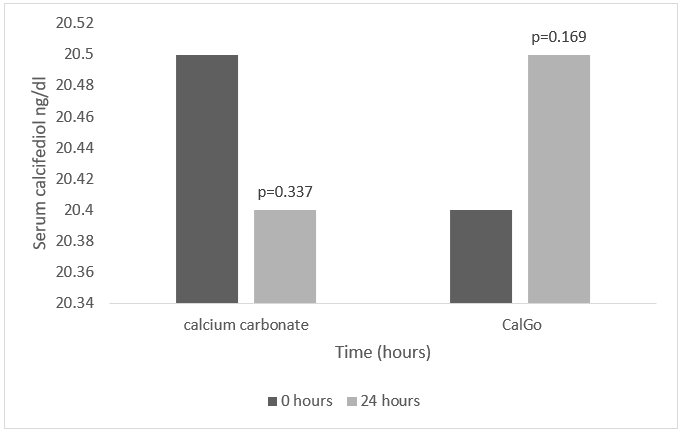
Baseline demographics were typical for a postmenopausal patient group. Mean age was 65 years (SD+/-5.2), BMI 25 (SD +/-2.9) and almost 60% were non-smokers. Two thirds were on concomitant medication. (Figure 2) shows the changes in serum values in calcium, calcifediol and creatinine after CalGo™ and calcium carbonate. The mean serum calcium level 24 h after calcium carbonate oral dosing did not show a statistically significant change at 95% confidence level (9.31 to 9.33 mg/dL, SD ± 0.8). The mean serum calcium level 24 h after CalGo™ oral dosing showed a statistically significant 1.28% increase at 95% confidence level (9.36 to 9.48 mg/dL, SD ± 0.9, p < 0.05). Laboratory reference range was 8.5-10.0mg/dL. The changes in serum calcifediol are also shown in (Figure 3). The mean serum calcifediol level 24 h after oral dosing of either calcium carbonate or CalGo™ was 20 ng/mL, SD ± 2.65. We used a serum calcifediol cutoff level of < 20 ng/mL as an indicator of the body responding to an increased uptake of calcium with a corresponding reduction in calciferol levels. Neither the calcium carbonate dosed subjects nor the CalGo™ dosed subjects showed a correlation between 25-OH Vitamin D (calcifediol) levels and serum calcium increase in this study. Changes in serum creatinine levels were used as a measure of renal safety. No change in mean serum levels was seen across the study treatments for the duration of the study.
Figure 2: Serum calcifediol changes over 24 hours.
Figure 3.
Discussion
In the present study we show that a natural form of calcium hydroxyapatite, CalGo™, significantly increased serum calcium compared to baseline values. Importantly, serum calcium levels remained within the normal reference range. In contrast, no significant increase was seen after the ingestion of calcium carbonate. There was no correlation between serum calcium change and vitamin D (calcifediol) in this study. No change in creatinine was observed. Similar findings are described in other studies, which have investigated the amount of calcium absorbed in bone meal products from fish, both in humans and animal models [9,13]. The positive impact of ingesting calcium derived from bone meal has received more research attention in the last decade. In clinical studies, natural hydroxyapatite appears to be more effective in building bone than traditional supplementation with calcium carbonate [14,15]. Bone meal also has a high collagen content, which appears to confer osteo-inductive properties, as indicated by several studies, both in-vitro and in-vivo [10].
The higher availability of serum calcium after intake of CalGo™ would suggest that this natural form of bone calcium is more easily absorbed by the gastrointestinal tract. As noted above, calcium levels remained within normal limits and no impact was seen on calcifediol levels. This lack of activation of a feedback mechanism used to control calcium uptake suggests that this increase in calcium is a positive outturn for the body. Therefore, CalGo™ looks to hold significant promise as a supplement for the treatment of postmenopausal osteoporosis. However, calcium metabolism is only one of many factors that need to be considered in treatment of osteoporosis. Numerous other factors influence the development of osteoporosis, including vit-D status, concomitant medication (for instance long-term treatment with corticosteroids), hormonal and nutritional factors [16]. There is a clear need to improve the current calcium supplementation strategies and deliver formats that supplement all the key elements of living bone: calcium hydroxyapatite, collagen and trace elements. Traditional supplementation with non-hydroxyapatite calcium salts has focused on delivering high levels of elemental calcium but this has resulted in a rather limited impact on bone density and strength. In summary, CalGo™ is derived from the off-cuts of salmon filet production thereby utilizing fish bones which would previously have been discarded as a waste product. This study builds further on the profile of this sustainable resource for the benefit of health. The findings in the present study suggest that bone meal from Norwegian Atlantic salmon is easily absorbed by the body and combined with previous data which indicated a potential to increase bone formation, CalGo™ looks to be a promising ingredient for supplementation to sustain bone health.
The NRH: Quinone Oxidoreductase Enzyme (QR2) has a Particular Distribution in Avian Retina
Introduction
The cytosolic detoxifying enzyme Ribosyldihidronicotinamide dehydrogenase (quinone), EC 1.10.99.2 (NRH: Quinone Reductase, QR2) is among the phase II detoxifying enzymes. Mice lack QR2 presents reduced sensitivity to menadione and myeloid hyperplasia of the bone marrow in comparison with the wild mice, proving that this enzyme is naturally active [1]. Regarding QR2 substrate, the para-quinone menadione is the most used in in vitro assays [2], but ortho-quinones such as dopamine quinone and estrogen quinone appear to be preferentially QR2 substrates in activity assays in vitro [3-5] and in situ [4,6]. The ability of the QR2 to retrieve dopamine from dopamine quinone is important in the retina because dopamine is the main modulator of the light-adapting events that are related to forming-image vision, besides dopamine has others trophic and circadian effects [7]. Therefore, a little change in dopamine levels can alter the retinal physiology.
In the retina, dopamine synthesis is triggered by light [4] and inhibited by melatonin [8]. The rate-limiting enzyme for dopamine synthesis is tyrosine hydroxylase, EC 1.14.16.2 (TH), which converts tyrosine to L-dopa, which is the substrate of the Aromatic L-amino acid decarboxylase, EC 4.1.1.28 (DOPA decarboxylase) in dopamine synthesis. DOPA decarboxylase and TH are in the type I amacrine cells, but in chick retina DOPA decarboxylase was also located in the type II amacrine cells and in photoreceptors [9]. The dopamine extracellular cleaner is done by the selective dopamine transporters that are located in dopaminergic amacrine cells [10]. However, a recent study in mammalian shows that the dopamine uptake and re-uptake also occur by non-selective transporters located in ganglion cells, in horizontal cells, in photoreceptors and in retinal pigment epithelial cells [11]. An interesting QR2 ligand is melatonin, which is the neurohormone produced in the dark phase of the circadian rhythm, mainly in the pineal gland and in the retinal photoreceptors [12,13]. Melatonin is the main modulator of the dark-adapting events in the retinal physiology [14]. The rate limiting enzyme in the melatonin synthesis is the Arylalkylamine N-acetyltransferase, (AANAT, EC 2.3.1.87), which is self-controlled by local molecular clocks and inhibited by dopamine [15]. Regarding non-neural retina, human retinal pigment epithelial cells in culture express functional melatonin synthesis machinery [16].
Melatonin has at least two binding modes in the QR2 pocket. The most common binding mode is that where melatonin is in parallel with FAD cofactor, matching well with the position of the inhibitors in the QR2 active site [17,18]. This observation is in accord with melatonin inhibiting QR2 in in vitro studies [19], suggesting that the same behaviour occurs in situ. On the other hand, the melatonin role in the QR2 activity in situ is very difficult to ascertain first because melatonin has membrane receptors and other binding sites in the retina [20], and second because the melatonin behaviour in the QR2 catalyses is dependent on its binding mode into QR2 active site [21]. In the chick retina, our previously published results showed that the differentiation of the retinal cells in culture is not completed in the absence of the melatonin [21,22]. Melatonin action on membrane receptors results in the inhibition of the cAMP accumulation [23], while the accumulation of this nucleotide is increased in this tissue by incubation with 5-MCA-NAT, which is a melatonin analogue and QR2 ligand [9]. The rising in cAMP levels by 5-MCA-NAT is a consequence of the QR2 recovering endogenous dopamine in developing and early PH retinas. In fact, the endogenous dopamine levels are increased by 5-MCA-NAT and by the QR2 cosubstrate N-methyl-dihydronicotinamide, while the QR2 inhibitor benzo[e] pyrene inhibits the endogenous dopamine levels in both control and stimulate retinas [6]. Regarding morphological data about QR2 in the retina, dense immunoreactivity for this enzyme has been shown in the whole neural retinas of the embryonic and early PH chicks [24] and in the whole neural retinas of the developing and juvenile turtles [18]. Thus, the current morphological studies do not show the QR2 distribution in the retinal layers. For that reason, these investigations offer limited insights concerning both the role of the melatonin into the QR2 binding site and the QR2 dopamine quinone activity in situ. As never was accomplished a study showing the distribution of the QR2 in the retina, the present aim was to investigate by immunohistochemistry the localization of the QR2 in retinal layers of the early PH chicks.
Material and Methods
Experimental Animals
Three early (3-5 day old) post-hatched (PH) chicks (male and female) were maintained at the equatorial photoperiod (12 h light/ 12 h dark, without annual variation) and sacrificed by decapitation in the morning. All possible efforts were made to avoid animal suffering and distress. All experimental procedures were carried out in accordance with the Brazilian laws for animal experiments, under license of the Ethics Committee on Experimental Animals of the Federal University of Pará (CEPAE-UFPA: BIO021-11).
Materials
NQO2 (N-15) polyclonal goat primary antibody (sc-18574) and chicken anti-goat Ig-G Texas Red (sc-3923) antibody were purchased from Santa Cruz Biotechnology Inc., CA, USA. Horse normal serum (S-2000), biotinylated horse anti-goat IgG antibody (BA-9500), Vectastain ABC Kit (PK-4005) and 3,3’Diaminobenzidine (DAB) peroxidase substrate (SK-4100) were purchased from Vector Laboratories, Burlingame, CA, USA. 4,6-Diamino-2-phenylindole dihydrochloride (DAPI) (D8417), Chicken serum (C5405) and Tween 20 (P2287) were purchased from Sigma Chemical Co., Saint Louis, MO, USA.
Tissue Preparation
Eyes of the PH chicks were enucleated and put in calcium magnesium free saline solution at 4°C. The anterior portion of the eye was removed. The cup containing the whole retina was immediately post-fixed for 24 hours in 4% paraformaldehyde, after the cup was put under different gradients of sucrose-glycerol solutions over 7 days. All solutions were at pH 7.4. The cup was frozen in Tissue Tek, and 30 μm [25] vertical and oblique sections were cut using a cryostat (Carl Zeiss Micron, Germany). An assortment of sections were mounted onto gelatinized slides and stored in a freezer at -20°C.
Immunohistochemistry
Texas Red Immunofluorescence: We used a commercial primary polyclonal goat antibody against avian QR2 enzyme, NQO2: N15 (sc-18574), previously validated for detection of the QR2 by immunofluorescence. The non-specific binding of the secondary immunofluorescent antibody chicken anti-goat Ig-G Texas Red (sc-3923) was prevented by including normal chicken serum (0.2%) in the emulsifying solution performed with Tween 20 (0.5%) in PBS. Negative controls of the secondary antibody binding were performed incubating retinal slices for 24 h at 4°C in a PBS solution devoid of the QR2 primary antibody. All solutions were at pH 7.4. Sections were incubated in the PBS solution containing Tween 20 (0.5%) and chicken serum (0.2%) for 30 minutes at room temperature. Then, the sections were rinsed (PBS, 3 times, 10 minutes) and incubated in the PBS solution containing 1:250 NQO2 primary antibody, for 24 h at 4°C. The negative controls were incubated for 24 h at 4°C in a simple PBS solution. After incubation, all sections were washed (PBS, 3 times, 10 min) and incubated in the PBS solution containing 1:400 Texas Red secondary antibody (anti-goat, done in chicken) for 2 h at 4°C. The secondary antibody reaction was stopped by exhaustive wash with PBS solution in room temperature. In some sections, cell’s nucleus were counterstaining with 0.001% DAPI for 15 seconds. The mounting medium (ibidi GmbH, Martinsried, Germany) was applied in the sections that were covered and analysed using a Nikon fluorescence microscopy. No immunoreactivity was observed in the negative controls.
Avidin-Biotin-Peroxidase Complex Reaction Revealed with DAB (DAB reaction): The slide-mounted vertical and oblique sections were removed from the freezer, kept in a heating oven at 37°C for 30 minutes, rinsed once in 0.1 M PBS (5 minutes) and pretreated by incubation in a solution of the 0.2 M boric acid (pH 9.0, 65°C) for 25 minutes. After freshening, the sections were incubated under constant agitation in a solution containing 1% hydrogen peroxide in methanol for 20 minutes. Sections were rinsed 3 times (5 minutes each) in a 0.05% PBS/Tween 20 solution and incubated with horse normal serum in PBS for 1 h. Without further rinsing, sections were then incubated in a PBS solution containing 1:500 of the commercial primary polyclonal goat antibody against avian QR2 enzyme, NQO2: N15 (sc-18574) overnight. As a negative control to check the non-specific binding of the secondary antibody, 10% horse serum, rather than the primary antibody, was used in this step. After, sections were rinsed in PBS/Tween 20 solution for 5 minutes (3 times), and incubated in a PBS solution containing the horse anti-goat biotinylated secondary antibody (1:100) for 2 h. Both primary and secondary antibodies were incubated at room temperature (20 °C). Sections were rinsed again for 5 min (3 times) in the PBS/Tween 20 solution under agitation, and incubated with the developed Avidin-Biotin-Peroxidase Complex (Vectastain ABC Kit, PK-4005) for 60 minutes. The peroxidase was visualised incubating the sections in a PB solution containing 0.05% DAB, 0.08% imidazole and 0.05% hydrogen peroxide. After the DAB reaction, sections were rinsed 3 times (3 minutes each) in 0.1 M phosphate buffer, dehydrated using alcohols and xylene, and cover slipped. Some sections were also counterstained or stained with cresyl violet for visualization of the nucleus. All sections stained with the different histological methods were surveyed by light microscopy (Nikon Eclipse 50i). No immunoreactivity was observed in the negative controls.
Data Analysis
A result was considered significant when repeated at least three times. The software Image J® was used only for slight adjusts in bright and contrast.
Results and Discussion
The Retina of the Early PH Chicks
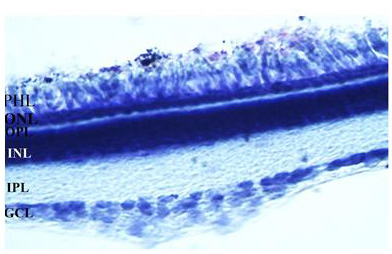
In this study, the distribution of the QR2 was investigated in the retinal layers of the early PH chick. The same development stage was used in the previous morphological and biochemical studies that showed the QR2 presence in these retinas [9,18,26]. The chick retina is avascular and its layers are well-demarcated in the early PH chicks used in this research (Figure 1).
Figure 1: The image of a 30 μm vertical retina section stained with cresyl violet is showing retinal layers of the early PH chicks. GCL: ganglion cell layer, IPL: Inner plexiform layer, INL: Inner nuclear layer, OPL: Outer plexiform layer, PHL: Photoreceptor layer. The magnification was 400xs.
The QR2 Enzyme Distribution in the Retinal Layers of the Early PH Chicks Visualized by Immunofluorescence
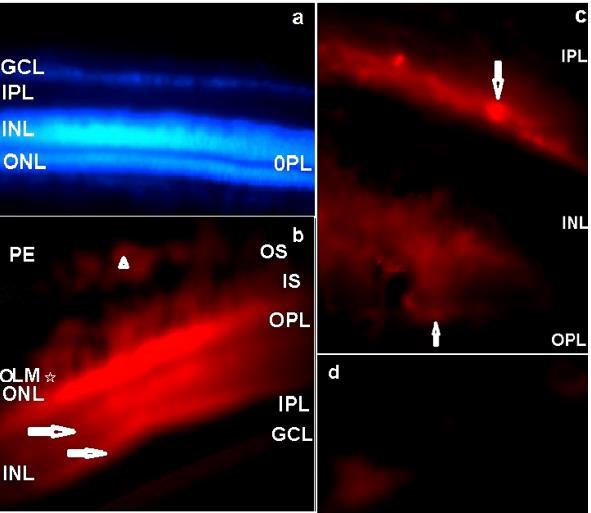
In the central retina, the QR2 enzyme was mainly localized by immunofluorescence in the Retinal Pigment Epithelium (RPE), in the Outer Nuclear Layer (ONL), in the Inner Segments (IS) and in the Outer Segments (OS) of the photoreceptors. QR2 immunoreactivity was also observed in the inner and outer borders of the Inner Nuclear Layer (INL). The ganglion cells and neural fiber layers (GCL/NFL) were also QR2 positive. On the other hand, the inner and the outer plexiform layers (IPL and OPL) were not positive to QR2 immunofluorescence in this study. Absence of the immunoreactivity was also observed in the Outer Limiting Membrane (OLM) (Figures 2a&2b). The OLM is localized between the body and the inner segment of the photoreceptors. This membrane is a semipermeable barrier with very important structural functions. A confocal microscopy analysis of the OLM is required to discard definitively the presence of the QR2 [27].
Figure 2: The distribution of the QR2 enzyme in a vertical retinal section of the early PH chick is shown by Texas Red immunofluorescence. a) Texas Red negative control counterstained with DAPI. No Texas red immunofluorescence was observed when the blue filter was replaced by the red filter. The magnification was 400xs. b) QR2 immunoreactivity in the PE, OS, IS, ONL and in the GCL. Arrowhead indicates QR2 immunoreactivity in a non-neural cell in the PE. Arrows point to bright linear bands localized in the outermost part and in the innermost part of the INL. The magnification was 400xs. c) The amplified image of the areas pointed with horizontal arrows in the innermost and in the outermost parts of the INL in “b”, showing amacrine-like cells (down arrow) and horizontal-like cells (up arrow). The magnification was 1000xs. d) QR2 immunopositive ganglion cells (magnification 1000xs). PE: pigment epithelium; OS: Outer segments of the photoreceptors; IS: Inner segments of the photoreceptors; OLM: Outer limiting membrane; ONL: Outer nuclear layer; OPL: Outer plexiform layer; INL: Inner nuclear layer; IPL: Inner plexiform layer, GCL: Ganglion cells layer.
The QR2 immunofluorescence pattern observed in this study was in accord with the cytosolic localisation of this enzyme showed by other authors [28]. In addition, the QR2 localization in bodies of the retinal cells is in agreement with the previously published results in the cerebral cortex of the human and rodent, in the hippocampus formation of the human and rodent [29], and in whole neural retinas of the early PH chick [24] and of the juvenile turtle [18]. The observed pattern of the QR2 immunofluorescence in the ONL presented herein (Figure 2b) suggests that QR2 is present in both cones and rods photoreceptors, because in chick retina cones are in superior quantity relative to rods, but rods have longer OS that touch to RPE [30], as showed herein (Figure 2b). The QR2 presence in photoreceptors is a found that links this enzyme with melatonin and dopamine synthesis because these cells are both the main place of the melatonin synthesis [15] and an alternative place of the dopamine synthesis, as showed by the presence of the DOPA decarboxylase in photoreceptors since early developmental stages in the chick retina [31]. The QR2 presence in the OS of the photoreceptors also is a link between this enzyme with melatonin and dopamine functions. This occurs because the photoreceptor strength is dependent on of the renewal of the OS, which is a melatonin effect, and of the phagocytosis of these OS by the RPE cells, which is an effect mediated by dopamine [32]. As the presence of the QR2 mRNA in the human pigment retinal cells in culture was previously showed by other authors [16], it is possible to suppose that the presence of the QR2 in the non-neural retina has evolutionary importance.
In general, bipolar-photoreceptors synapses are modulated by horizontal neurons located in the outmost part of the retinal INL, while bipolar-ganglion cells synapses are modulated by amacrine cells located in the innermost part of the INL, which encloses bodies of the bipolar, horizontal, amacrine and Muller glia cells. The characterization of these retinal cells can be done by their proper morphology and positioning in the retinal layers [33], furthermore the width of the INL is progressively smaller from central to peripheral retina [34]. In this study, highly immunoreactive parallel linear bands were respectively located in the outmost part and in the innermost part of the INL of the central retina, but they were not localized in the periphery of the retina (data not shown). These bright areas were also parallel to another linear band highly immunoreactive in photoreceptor layer, nearby the OPL (Figure 2b). Higher magnification of the linear bright bands located along of the outermost and of the innermost borders of the INL showed respectively horizontal-like cells and rounded and elongated amacrine-like cells (Figure 2c). These clustered QR2-positive cells are related to modulation of the synapses in the central retina, but it is not possible to infer the role of the QR2 in this because the type of the amacrine and horizontal cells were not characterized.
The dopamine synthesis and the dopamine selective transporter are located in amacrine cells [7]. Additionally, a recent study in the mammalian retina shows that the dopamine uptake and re-uptake also occur by non-selective transporters located in ganglion cells, in horizontal cells, in photoreceptors and in retinal pigment epithelial cells [26]. A more advanced investigation using double-staining immunofluorescence protocols is necessary to show the type of the amacrine-like cells that were QR2 positive in chick retina, and the presence of the non-selective dopamine transporters in the QR2 positive retinal cells shown herein. Ganglion cells presenting QR2 immunoreactivity were also observed by immunofluorescence in this study (Figure 2d). Regarding the characterization of the ganglion cells positive to QR2 as melatoninergic cells, it is another interesting point for further investigation because some ganglion cells have melatonin synthesis machinery in chick retina [35].
QR2 Enzyme Distribution in Retina Sections of the Early PH Chick Visualized by DAB Reaction
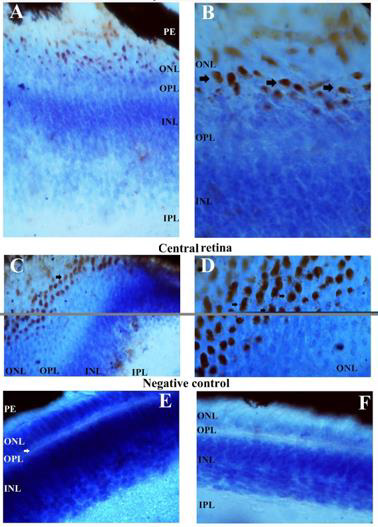
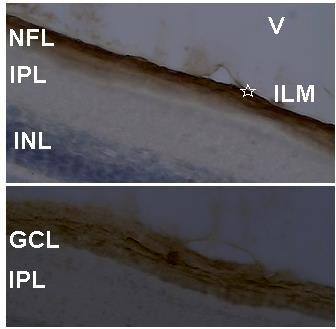
The QR2 enzyme distribution was previously investigated by DAB reaction in vertical and oblique retinal sections of the early PH chick. The results found in the vertical sections match well with those obtained using Texas Red immunofluorescence. The exception was the presence of the QR2 immunosignal in amacrine- and in horizontal- like cells only in sections assayed by immunofluorescence. This difference occurred either due to the retinal sections analysed or due to the DAB protocol utilized in this study. The main results obtained using DAB in vertical sections were the QR2 distribution in the RPE, in the photoreceptors layer, in the GCL and in the NFL (data not shown). Oblique sections were used to better visualize the QR2 presence in the non-neural retina, in the ONL, in the GCL, in the NFL and in the Inner Limiting Membrane (ILM) ( Figure 4). The distribution of the QR2-positive photoreceptors was higher in the central than in the peripheral areas of the retina (Figure 3). This distribution was in accord with the expected for the density of these cells in each area investigated [34].
The presence of the QR2 in the photoreceptor (Figure 3) is important to be highlighted because they are the second place of the melatonin synthesis in both avian retina [36]and mammalian retina [37], losing only to the melatonin production in the pineal gland [12]. Thus, the melatonin concentration into citosol of the QR2-positive photoreceptors must reach suitable levels to modulate the QR2 activity as in mammalian as in avian retinas. However, the DOPA-decarboxylase is present in photoreceptors in the chick [32], while in the mammalian photoreceptors never was noticed the presence of this enzyme. The NFL and ILM were also QR2 positive in the central retina and in the peripheral retina (Figure 4). The QR2 immunoreactivity in the area corresponding to ILM was visualized only in oblique sections in this study (Figure 4). The ILM is a basement membrane attached to the Muller cells footplates on the inner surface of the retina and to the cortical vitreous gel on the other side. It is composed of the structural macromolecules, having mainly structural functions [38]. Therefore, it is unexpected the presence of the QR2 in this region. Thus, this result will be subject of the future investigation.
Figure 3: QR2 localization in the most external part of the early PH chick retina, as it appears in an oblique section staining by DAB and counterstained with cresyl violet. Immunoreactivity in the bodies of the photoreceptors is present in both peripheral and central retina, as explained in the figure. The magnification was 400xs in the images A and C, while in the images B and D the magnification was 1000xs. Images E and F are the negative controls of the secondary antibody, in the central and peripheral regions of the retina (magnification 400xs). PE: retinal pigment epithelium; OS: outer segments of the photoreceptors; ONL: outer nuclear layer; OPL: outer plexiform layer; INL: inner nuclear layer; IPL: inner plexiform layer.
Figure 4: QR2 localization in an oblique section of the most internal part of the early PH chick retina. Sections were stained by DAB and counterstained with cresyl violet. Above, the QR2 presence in the NFL and in the ILM (star) is showed. Below, the QR2 presence in a ganglion cell (middle of the figure) and in neural fibers at GCL is showed. The magnification was 400xs. V: vitreous; ILM: inner limiting membrane; NFL: neural fiber layer; GCL: ganglion cell layer; IPL: inner plexiform layer; INL: inner nuclear layer.
Immunoreactivity for QR2 was not showed to occur in the thinner OLM (Figures 2b, 3b&3d). This point is highlighted because the OLM is the place of the traffic of the substances between the retina and non-neural ocular tissues, functioning as a semipermeable barrier that appear to be communicating with the main retinal barriers located in the RPE [27]. The present results showing QR2 presence in the RPE are in agreement with QR2 functioning as a detoxification enzyme in the retina [39,40].
Conclusion
We conclude that QR2 has a specific distribution in retinal layers. The observed distribution in photoreceptors suggests that melatonin can be a natural QR2 modulator in the retina. As well, the canonical QR2 detoxification activity must be occurring in this tissue by the presence of this enzyme in RPE. On the other hand, QR2-positive horizontal, amacrine and ganglion cells still were not characterized regarding dopamine containing, and this should be important to reinforce the previous pharmacological results showing dopamine quinone as a natural QR2 cosubstrate.
Prevalence of Diabetes Insipidus and Other Complications in Early Period After Pituitary Surgery: Analysis of 259 Patients
Introduction
Pituitary adenomas constitute about 10-12% of all intracranial tumors [1,2]. They are benign tumors growing from adenohypophyseal cells. All adenomas are classified according to their hormonal activity as non-secreting and secreting (prolactinoma, growth hormone-secreting, ACTH-secreting and thyroid stimulation hormone-producing) adenomas. The treatment of choice for most patients with secreting adenomas is surgical removal. In case of prolactinomas, dopamine agonists can be prescribed first. Surgery can be an option in this case if the conservative treatment is unsuccessful [1]. Patients with nonsecreting adenomas and any neurological or vision deficit are also candidates for surgery. The most common surgical technique for pituitary adenomas is the endoscopic transnasal transsphenoidal approach. This technique is becoming more popular and refined due to better lighting and endoscope’s superior visualization [3-5]. These factors have significantly reduced surgical complications and improved tumor removal. The aim of this study was to determine the relation between postoperative central diabetes insipidus (DI) and the characteristics of adenomas, tumor removal extent and surgical complications. Central DI has been one of the most common forms of transient or permanent disorder of fluid homeostasis after transsphenoidal surgery. Any disturbance of the posterior pituitary, pituitary stalk or neurons originating in the paraventricular or supraoptic hypothalamic nuclei can lead to DI [6,7].
Material and Methods
This study was a retrospective analysis of 259 patients with pituitary adenoma who were surgically operated at Federal Center of Neurosurgery of Ministry of Public Health of Russian Federation in Novosibirsk from July 2014 to December 2018. Patients who had been operated in our hospital before July 2014 using the microsurgical transsphenoidal technique and patients with DI before operation were excluded from this study. Only histologically verified pituitary adenomas were included. The following patient characteristics were recorded preoperatively: type of adenoma (non-secreting or hormone-producing), age of patient, gender, size of tumor (microadenoma (<10 mm), macroadenoma (10- 39 mm), giant adenoma (≥40 mm)), preoperative visual deficit (loss of visual fields or decreased visual acuity), preoperative hormone insufficiency, number of previous surgeries for pituitary adenoma. At the postoperative period, the following complications were evaluated: postoperative cerebrospinal fluid (CSF) leakage, meningitis, neurological deterioration, new visual deficit, hematoma, epistaxis, deep vein thrombosis (DVT), pulmonary embolism (PE) and DI. Other endocrinological complications were excluded from this study.
Surgical Technique
All the operations had been planned using the data collected from preoperative CT, contrast-enhanced MRI and MR-angiography. In every case intraoperative navigation (Integra, Radionics) was used. All the patients underwent a fully endoscopic endonasal approach. The operations took place with the patient’s head fixed in a three-pin Mayfield holder. Both nostrils were prepared with a topical vasoconstrictor. Between July 2014 and July 2015, we used a mononostril approach. Generally, the approach was through the right nostril, the left one was used only in a case of major septal deviation to the right. The initial step included lateralization of middle turbinate, but not resection. We removed the rostrum and small back part of the septum. At that moment the endoscope irrigating system (ClearVision system, Karl Storz) was additionally used as the monomanual technique was performed. In cases of intraoperative CSF-leakage, a fat-graft and fibrin-glue were applied for skull base reconstruction. After July 2015 we have begun applying a binostril approach, using the bimanual technique with an assistant surgeon holding the endoscope. The middle turbinate was lateralized on the left side and resected on the right side after injection in mucosa a solution of 2% lidocain and adrenalin. On the right side a nasal septal flap was formed using unipolar coagulation.
The anterior wall of the sphenoid sinus was opened bilateraly. Nasal cavity and sinus were disinfected with Octenisept. The septum and mucosa from sphenoid sinus were removed totally and then the bone of floor of sella turcica was removed rather wide. In all the cases we used a high-speed drill (2 or 4 mm in diameter). The dura was opened with a telescopic knife and microscissors under direct visual control. Before July 2015, the tumor was removed with curettes and after July 2015 – with suction and microforceps or using the two-suction technic. In all the cases the Karl Storz hard endoscopes (180/4 mm) with 0°, 30°, 45° angulations attached to high-definition cameras was used. In the case of unimanual technique the surgeon held the endoscope in his left hand and the instrument – in the right one, while an assistant held a suction tube, but in the case of bimanual technique the assistant held an endoscope and the surgeon – one suction tube in his left hand and in right hand – a second suction tube or any other instrument. In a case of high bleeding the assistant could help, holding one more suction tube. For skull base reconstruction vascularized flaps or mucosa from the resected middle turbinate were used. In presence of middle-flow intraoperative CSF-leakage, a fascia lata graft was applied. In some cases, we used a fat graft or a bone part or suture on dura mater for reconstruction, as well as artificial dura (Duraform), fibrin glue and a Foley catheter. The patients were not routinely given corticosteroids before surgery. Antibiotics administration continued for 24 hours.
Postoperative Evaluation
In 48 hours after surgery a full endocrinological assessment was performed. Within 72 hours postoperatively all the patients underwent MRI brain scans to assess the volume of removal. In cases of non-functional adenomas our main interest was control of cortisol, thyroxin, prolactin and testosterone. In case of growthhormone secreting adenomas, we additionally controlled the patients’ growth hormone, in case of ACTH-hormone secreting – adrenocorticotropic hormone, and in case of TSH-hormon secreting adenomas – thyroid stimulating hormone and threeiodthyronin. For evaluation of DI postoperatively the level of electrolytes, urine-specific gravity and production of excessive volumes of urine were controlled. All the patients underwent postoperative ENT inspection. Every patient with any preoperative visual deficit underwent neuro-ophthalmological evaluation postoperatively.
Statistical Analysis
Data analysis was performed using the R 3.3.3 statistical package [8]. Bivariate analysis was performed to identify the predictive factors of DI among the collected variables. It included Fisher’s exact test (asymptotic implementation) for qualitative variables and Wilcoxon rank sum test for quantitative variables. All the tests were 2-sided. Univariate analysis was carried out to test the covariates predictive of outcome (DI onset). The factors predictive in the univariate analysis (p<0.25) were entered into stepwise logistic regression analysis. Additionally based on some clinical considerations and graphical analysis, we tested a number of hypotheses about the nonlinear entry of variables into the logit function [9]. To select the final model AUC and ANOVA were used.
Results
All the 259 patients were operated at the same hospital by the same two surgeons from July 2014 to December 2018. The mean age at the time of surgery was 52.4 years, median – 55 (ranged from 14 to 79). The interquartile range was from 42 to 62. Women prevailed over men (155 versus 104). All the pituitary adenomas were divided by size into microadenomas (32 cases), adenomas of 11-39 mm in size (176 cases) and giant adenomas over 40 mm in size (51 cases). There were 159 non-secreting, 5 prolactinsecreting, 83 growth hormone-secreting, 9 ACTH-secreting, 2 thyroid stimulation hormone-secreting adenomas, and 1 patient had a mixed adenoma (growth-hormone and ACTH-secreting). Preoperatively 172 patients had visual deficit (66.4%). 230 patients were operated for the first time, 29 patients were reoperated due to tumor recurrence. As possible predictors of DI onset, the following factors were considered: gender (p=0.69), age (p=0.10), presence of prior surgery (p=0.53), hormone secretion (p=0.71), adenoma size (p=0.03), its consistency (p=0.01) and extent of tumor removal (p=0.71). The final model of logistic regression included factors interaction (Table 1): In the group of microadenomas, the influence of age was OR=0.963, CI= [0.94; 0.987], in macroadenomas – OR=0.977, CI= [0.957; 0.997], in giant adenomas – OR=0.99, CI= [0.971; 1.01]. The greatest impact the age rendered in increasing DI had in the group of microadenomas, but in the case of giant ones it was about 0.
Estimated OR and 95 CI for Size controlling for Age are shown in (Table 2). The size effect depended on the patients’ age. In young patients (30-year-old) the risk of DI was 1.51 times higher with increasing of tumor size by one grade in while in elder patients (60-year-old) it was 2.3 times higher. The transition from suctionable to unsuctionable increased the risk of DI 2.89 times (CI= [1.18; 7.07], p=0.020). In our opinion, the main cause of DI was changes in the shape and size of the pituitary gland in presence of giant and macroadenomas that determined bad visualization of the gland during surgery (Table 3). One of the most important surgical characteristics of an adenoma is its consistency. More dense and unsuctionable tumors have a higher risk (2.89 times) of post-op DI, because of worse identification of pituitary gland (p=0.020). No significant difference was found between the patients with and without surgical complications. The hormonal activity of adenomas had no effect associated with DI development (p=0.71) as well. In our study patients with prior surgery did not have a higher DI incidence (p=0.53). Smith et al. indicate that percentage of permanent DI after a first operation was 2.6% and while rate of transient DI after second surgery was 37.9% [10]. Also, patients with gross totally, subtotally or partially removed tumors had no differences in DI development (p=0.71).
Table 2: Estimated OR and 95 CI for Size controlling for Age.
Table 3: Extent of resection.
Note: *Tr DI – Transient Diabetes Insipidus; P DI – Permanent Diabetes Insipidus
Extent of Tumor Removal
The radicality of tumor removal was evaluated using contrastenhanced MRI within the first 72 hours. The resection extent is presented in (Table 4). Gross total resection was achieved in 74% (191/259) of cases. This group included all microadenomas and a part of macro- and giant adenomas, which were easily suctionable. A group of patients with subtotal (22%, 58/259) or partial removal (4%, 10/259) had unsuctionable macro- or giant adenomas, and giant adenomas with big antesellar part. The radicality of tumor removal depended on a tumor’s consistency (р=0.009) and size (р <0.001) (Table 3).
Table 4: Surgical complications in 259 procedures.
Visual Outcome
Of the 146 patients with preoperative visual deficit, impaired visual acuity improved postoperatively in 61%, visual fields normalized in 61.6% Postoperative deterioration of visual function was detected in 6 patients including 3 cases of visual acuity deterioration and 3 cases of deterioration of both visual acuity and fields. These patients had macro and giant adenomas with a large suprasellar part and had already been suffering from severe visual impairment. Fifty-three patients did not have any changes in their visual fields. The visual acuity stayed the same after surgery in 51 patients.
Overall Complication Rate
34 patients developed different complications in the early postoperative period, while the remaining 225 patients had no complications whatsoever (Table 4).
Postoperative CSF leakage
In 8 patients (3.1%) a postoperative CSF leakage occurred. One of the patients had microadenoma, 4 patients had macroadenomas and 3 patients – giant adenomas. In 4 cases we did not use vascularized or mucosal flaps. Artificial dura or a fat graft was used instead. In two cases necrotization of the vascularized flap was observed. One patient developed CSF leakage after skull base reconstruction due to necrosis of the vascularized flap. Another patient developed hydrocephalus of normal pressure. In that case, we first performed a ventriculoperitoneal shunting and then did a reoperation.
Meningitis
8 patients (3.1%) developed meningitis. All of them were patients with intraoperative CSF leakage. Six of them had CSF leakage postoperatively. They were treated with ceftriaxone (4.0 per day) or vancomycin (2.0 per day) and meropenem (6.0 per day). The treatment was successful and no neurological deficit after meningitis was observed.
Epistaxis
One patient (0.4%) developed postoperative epistaxis in 6 hours after surgery and required reoperation. This patient was operated using a unonostril approach. The sphenoidal sinus was opened on both sides but the mucosa on the opposite side was left intact. The bleeding originated from the opposite – side ramus of sphenopalatina artery.
New Visual Deficit
6 patients (2.3%) (2 had a macroadenoma and 4 – giant adenomas) developed a new visual deficit after surgery. In 3 cases of giant adenoma, the patients had both vision and visual fields impairment. The other patients had only visual acuity deterioration. In 5 cases, these new symptoms were gone after treatment. One patient did not have any improvement despite of the treatment.
Hemorrhage/Swelling of Residual Tumor
There was one case of thalamus hemorrhage that required external ventricular drainage. This patient developed a new neurological deficit (diencephalon syndrome), which regressed after the treatment. One more patient developed an asymptomatic ventricular hemorrhage after total removal of the macroadenoma that did not require any additional treatment. A third patient had swelling of residual tumor after partial resection and was reoperated.
Surgical Mortality
The surgical mortality rate was 0.8% (2 patients). The first patient had macroadenoma and Cushing’s disease. The tumor had an invasive growth. It was almost unsuctionable and therefore was not totally removed. After the operation, the patient developed hemiparesis followed in 8 days by deep vein thrombosis and cavafilter implantation. Within the next 7 days, the patient developed pulmonary embolism and on the 34th day after the operation he died. The second patient was a 54-year-old woman with a nonfunctional macroadenoma. During the operation we had no difficulties, and the tumor was removed gross totally. The first day after the surgery she was verticalized and developed pulmonary embolism. A cavafilter was implanted, and thrombus fragmentation was performed. The patient died on the 4th day after the surgery.
Diabetes Insipidus
The DI diagnostics was based on the level of electrolytes (serum Na >145 mmol/L), urine-specific gravity (1.004 or less) and excessive volumes of urine (quantified as more than 300 mL of urine per hour for 3 consecutive hours). In this study there were no patients with preoperative DI. After DI was diagnosed all the patients were treated with desmopressin (the dose was titrated by the level of diuresis). In this series of 259 patients, 111 cases of postoperative DI (42.9%) were diagnosed. 21 patients (8.1%) had transient DI and 90 (34.8%) – permanent DI. Since only the early postoperative period had been analyzed we considered transient DI to be the one that regressed during hospital admission. The patients’ data and tumor characteristics are summarized in (Table 5).
Table 5: Demographic characteristics and tumor characteristics in patients with or without postoperative DI.
Discussion
According to the literature, the rate of surgical complications after removing pituitary adenomas varies between 9% [11] and 35.8% [12] (in average 12.1%). The incidence of CSF leakage is about 3.1-4.7% [3,11-20] (minimal is 1.8% [20], maximal is 19.5% [21]). Smith et al. report 0% of CSF leakage in surgery of microadenomas. Contrariwise, in the study of giant adenomas (Koutourousiou M. et al.) rate of CSF leakage is 16.7%. Based on these data, we can conclude that percentage of postoperative CSF leakage depends on a tumor’s size. Another possible complication after endoscopic surgery is meningitis whose mean rate is 2.0-2.7% [21-24]. In most cases, it has been successfully treated by antibacterial therapy [25- 27]. Hemorrhage inside the residual tumor or its swelling occurs in 0.4-4.0% of patients [28,29] and can lead to new visual (0.9-4.4%) [30] or neurological deficit (0.4-2.3%) [31]. The most common are cranial nerve (III, IV, VI) dysfunction, hemiparesis (0.2-1.0%) and diencephalon syndrome [32]. The incidence of epistaxis in the studies rates from 0.4 to 2.9% [32]. In most cases nasal cavity tamponade is effective, but some cases require a revision surgery.
The rate of surgical mortality varies from 0.6 to 1.8% [33]. The main reasons of mortality are hemorrhage, somatic pathology (cardio-vascular disease, acute pancreatitis etc.), meningitis, ischemic stroke due to the damage of internal carotid artery, hard electrolytes irregularities (because of involvement of diencephalon region), pulmonary embolism, subarachnoid hemorrhage (in case of undiagnosed aneurism) [33]. In our study we did not find any difference between complications and DI postoperatively. DI belongs to a group of hereditary or acquired polyuria and polydipsia diseases. It is associated with inadequate arginine vasopressin (AVP) or antidiuretic hormone (ADH) secretion or renal response to AVP, resulting in hypotonic polyuria and a compensatory/ underlying polydipsia. The characteristics of DI polyuria include polyuria (>50 mL/kg), diluteurine (osmolality <300 mOsm/L), and increased thirst (water intake of up to 20 L/day). Untreated DI can cause hypovolemia, dehydration, and electrolyte imbalances. There are different types of DI such are central, nephrogenic, gestational and primary polydypsya. This paper refers only to central DI (CDI) [34].
CDI or neurogenic DI is the most common form of DI, occurring equally in both sexes and at any age. It is caused by inadequate synthesis/release of AVP, often secondary to surgery or to a head injury causing traumatic injury to the hypothalamus or posterior pituitary gland and destruction/degeneration of neurons originating in the supraoptic and paraventricular nuclei of the hypothalamus. DI Symptoms manifest themselves after 80–90% of the magnocellular neurons in the hypothalamus are damaged. Damage to the proximal part of the hypothalamo-neurohypophyseal region kills more neurons than do injuries to the distal region. However, proximal injuries account for 30–40% of posttraumatic and postoperative CDI, while distal injuries account for 50–60% of cases. Acquired CDI is more common than congenital one, and about 25% of adult CDI cases are idiopathic. Children with acute injury to the nervous system and CDI have a high mortality rate. Traumatic brain injury is associated with high mortality and acute and chronic morbidity [34]. Pituitary surgery results in CDI with a wide range of incidence (1–67%). Minimally invasive surgery has a low incidence of postoperative CDI (transient CDI 13.6% and permanent CDI 2.7%). Abnormalities in the secretion of AVP usually begin during the intraoperative period. The incidence of immediate postoperative DI is higher among the patient’s undergoing surgery by the traditional method than by the endoscopic transsphenoidal method (36% vs. 15%). The incidence of long-term DI did not vary significantly between the groups [34].
The history of desmopressin started from the first use of vasopressin to treat CDI in 1913. That time it was pituitary extracts containing oxytocin and vasopressin. Pitressin (vasopressin tannate in oil) became available for clinical use in the 1930s and was the principal drug for DI treatment almost until the 1970s when desmopressin was introduced. Substitution of the 8th residue of vasopressin with the D-isomer of arginine diminished the pressor effect of vasopressin. This synthetic analog of vasopressin, 1‑deamino‑8‑D‑AVP (DDAVP), or desmopressin, has increased and prolonged antidiuretic effect, decreased vasoconstrictive and oxytocic effects, reduced side effects (hyponatremia and convulsions), and enhanced resistance to vasopressinase. It can be administered in the form of intranasal spray, oral tablets, and orally disintegrating tablets (ODT) [34]. In our study, the patients received only the oral tables. The minimal initial dose of desmopessin is 0.1 mg. The titration control included blood electrolytes, urine-specific gravity and production of excessive volumes of urine. The maximum dose is 0.2 mg twice a day. In this study an attempt was made to determine the relation between postoperative DI frequency and different characteristics of adenomas, surgical complications and extent of resection.
In the literature, the rate of DI is estimated to be between 8.7% and 18.3%. In their study of giant adenomas M. Koutourousiou et al. have reported 9.6% rate of permanent DI, and PG Campbell et al. in their study of growth hormone secreting adenomas have detected no cases of permanent DI while transient DI have occurred in 7.7% of patients. Multivariate analysis of our cases showed the predictors of DI were patient’s age, size and consistence of tumor. In our study, we revealed the influence of adenomas size relative to a patient’s age. For older patients the size of the adenoma was a stronger factor than for the younger ones. In other words, in the elderly patients the tumor size has a greater effect on the risk of DI development. These data contradict to the results obtained by Sigounas et al. in 2008 who has not revealed any correlation between DI and tumor size. In our opinion our findings are related to the anatomy of a pituitary gland. The older a patient the more prone the gland is to hypoplasia while the risk its injury is lower, especially in case of microadenomas. Macroadenomas and giant adenomas are often found in close proximity to the pituitary gland that increases the risk of its injury and DI development after surgery. In case of giant adenomas, the last squeeze the gland a lot, but in case of microadenomas, when we usually observe healthy hypophysis tissue, the hypoplasia will play a major role.
The second important factor was consistence of tumor. The unsuctionable adenomas increased the risk of DI 2.89 times. This dependency also can be related to the tumor’s intimacy to the gland making the last more prone to injury and increasing the risk of DI development. The rate of all complications also depends on the surgeon’s experience. Ciric et al. analyzed complications in three groups of patients who were operated by surgeons with experience less than 200, 200-500 and more than 500 cases respectively. It has been demonstrated that those patients who were operated by surgeons with experience less than 200 surgeries (as in our study) had higher incidence of not only surgical complications, but also higher rate of DI (19%).
Conclusion
The endoscopic transsphenoidal surgery is the treatment of choice for patients with pituitary adenomas. Complications are rather common after endoscopic surgery and include two big groups that are surgical and endocrine complications. Further studies into the incidence and causes of postoperative diabetes insipidus and other complications can contribute to the reduction of both types. We can conclude that the predictors of DI include the patient’s age, size and consistence of adenomas. The influence of adenomas size depends on the age of a patient. The risk of DI in 30-year-old patients has been 1.51 times higher with increasing of the size group by one grade (micro, macro, giant), while in the elder patients (60-year-old) it has increased 2.3 times. Nevertheless, in case of giant adenomas the age has not been the impact factor to trigger DI after surgery. The tight consistence of tumor has been another important factor to provoke DI after surgery. The unsustainable consistency increases the risk of DI 2.89 times. The hormone activity of adenomas, prior surgery, extent of surgery have not been associated with DI development. The DI rate after endoscopic resection is 42.9% (in 8.1% of cases the patients developed transient DI and 34.8% – its permanent form).
Prevalence of Diabetes Insipidus and Other Complications in Early Period After Pituitary Surgery: Analysis of 259 Patients
Introduction
Pituitary adenomas constitute about 10-12% of all intracranial tumors [1,2]. They are benign tumors growing from adenohypophyseal cells. All adenomas are classified according to their hormonal activity as non-secreting and secreting (prolactinoma, growth hormone-secreting, ACTH-secreting and thyroid stimulation hormone-producing) adenomas. The treatment of choice for most patients with secreting adenomas is surgical removal. In case of prolactinomas, dopamine agonists can be prescribed first. Surgery can be an option in this case if the conservative treatment is unsuccessful [1]. Patients with nonsecreting adenomas and any neurological or vision deficit are also candidates for surgery. The most common surgical technique for pituitary adenomas is the endoscopic transnasal transsphenoidal approach. This technique is becoming more popular and refined due to better lighting and endoscope’s superior visualization [3-5]. These factors have significantly reduced surgical complications and improved tumor removal. The aim of this study was to determine the relation between postoperative central diabetes insipidus (DI) and the characteristics of adenomas, tumor removal extent and surgical complications. Central DI has been one of the most common forms of transient or permanent disorder of fluid homeostasis after transsphenoidal surgery. Any disturbance of the posterior pituitary, pituitary stalk or neurons originating in the paraventricular or supraoptic hypothalamic nuclei can lead to DI [6,7].
Material and Methods
This study was a retrospective analysis of 259 patients with pituitary adenoma who were surgically operated at Federal Center of Neurosurgery of Ministry of Public Health of Russian Federation in Novosibirsk from July 2014 to December 2018. Patients who had been operated in our hospital before July 2014 using the microsurgical transsphenoidal technique and patients with DI before operation were excluded from this study. Only histologically verified pituitary adenomas were included. The following patient characteristics were recorded preoperatively: type of adenoma (non-secreting or hormone-producing), age of patient, gender, size of tumor (microadenoma (<10 mm), macroadenoma (10- 39 mm), giant adenoma (≥40 mm)), preoperative visual deficit (loss of visual fields or decreased visual acuity), preoperative hormone insufficiency, number of previous surgeries for pituitary adenoma. At the postoperative period, the following complications were evaluated: postoperative cerebrospinal fluid (CSF) leakage, meningitis, neurological deterioration, new visual deficit, hematoma, epistaxis, deep vein thrombosis (DVT), pulmonary embolism (PE) and DI. Other endocrinological complications were excluded from this study.
Surgical Technique
All the operations had been planned using the data collected from preoperative CT, contrast-enhanced MRI and MR-angiography. In every case intraoperative navigation (Integra, Radionics) was used. All the patients underwent a fully endoscopic endonasal approach. The operations took place with the patient’s head fixed in a three-pin Mayfield holder. Both nostrils were prepared with a topical vasoconstrictor. Between July 2014 and July 2015, we used a mononostril approach. Generally, the approach was through the right nostril, the left one was used only in a case of major septal deviation to the right. The initial step included lateralization of middle turbinate, but not resection. We removed the rostrum and small back part of the septum. At that moment the endoscope irrigating system (ClearVision system, Karl Storz) was additionally used as the monomanual technique was performed. In cases of intraoperative CSF-leakage, a fat-graft and fibrin-glue were applied for skull base reconstruction. After July 2015 we have begun applying a binostril approach, using the bimanual technique with an assistant surgeon holding the endoscope. The middle turbinate was lateralized on the left side and resected on the right side after injection in mucosa a solution of 2% lidocain and adrenalin. On the right side a nasal septal flap was formed using unipolar coagulation.
The anterior wall of the sphenoid sinus was opened bilateraly. Nasal cavity and sinus were disinfected with Octenisept. The septum and mucosa from sphenoid sinus were removed totally and then the bone of floor of sella turcica was removed rather wide. In all the cases we used a high-speed drill (2 or 4 mm in diameter). The dura was opened with a telescopic knife and microscissors under direct visual control. Before July 2015, the tumor was removed with curettes and after July 2015 – with suction and microforceps or using the two-suction technic. In all the cases the Karl Storz hard endoscopes (180/4 mm) with 0°, 30°, 45° angulations attached to high-definition cameras was used. In the case of unimanual technique the surgeon held the endoscope in his left hand and the instrument – in the right one, while an assistant held a suction tube, but in the case of bimanual technique the assistant held an endoscope and the surgeon – one suction tube in his left hand and in right hand – a second suction tube or any other instrument. In a case of high bleeding the assistant could help, holding one more suction tube. For skull base reconstruction vascularized flaps or mucosa from the resected middle turbinate were used. In presence of middle-flow intraoperative CSF-leakage, a fascia lata graft was applied. In some cases, we used a fat graft or a bone part or suture on dura mater for reconstruction, as well as artificial dura (Duraform), fibrin glue and a Foley catheter. The patients were not routinely given corticosteroids before surgery. Antibiotics administration continued for 24 hours.
Postoperative Evaluation
In 48 hours after surgery a full endocrinological assessment was performed. Within 72 hours postoperatively all the patients underwent MRI brain scans to assess the volume of removal. In cases of non-functional adenomas our main interest was control of cortisol, thyroxin, prolactin and testosterone. In case of growthhormone secreting adenomas, we additionally controlled the patients’ growth hormone, in case of ACTH-hormone secreting – adrenocorticotropic hormone, and in case of TSH-hormon secreting adenomas – thyroid stimulating hormone and threeiodthyronin. For evaluation of DI postoperatively the level of electrolytes, urine-specific gravity and production of excessive volumes of urine were controlled. All the patients underwent postoperative ENT inspection. Every patient with any preoperative visual deficit underwent neuro-ophthalmological evaluation postoperatively.
Statistical Analysis
Data analysis was performed using the R 3.3.3 statistical package [8]. Bivariate analysis was performed to identify the predictive factors of DI among the collected variables. It included Fisher’s exact test (asymptotic implementation) for qualitative variables and Wilcoxon rank sum test for quantitative variables. All the tests were 2-sided. Univariate analysis was carried out to test the covariates predictive of outcome (DI onset). The factors predictive in the univariate analysis (p<0.25) were entered into stepwise logistic regression analysis. Additionally based on some clinical considerations and graphical analysis, we tested a number of hypotheses about the nonlinear entry of variables into the logit function [9]. To select the final model AUC and ANOVA were used.
Results
All the 259 patients were operated at the same hospital by the same two surgeons from July 2014 to December 2018. The mean age at the time of surgery was 52.4 years, median – 55 (ranged from 14 to 79). The interquartile range was from 42 to 62. Women prevailed over men (155 versus 104). All the pituitary adenomas were divided by size into microadenomas (32 cases), adenomas of 11-39 mm in size (176 cases) and giant adenomas over 40 mm in size (51 cases). There were 159 non-secreting, 5 prolactinsecreting, 83 growth hormone-secreting, 9 ACTH-secreting, 2 thyroid stimulation hormone-secreting adenomas, and 1 patient had a mixed adenoma (growth-hormone and ACTH-secreting). Preoperatively 172 patients had visual deficit (66.4%). 230 patients were operated for the first time, 29 patients were reoperated due to tumor recurrence. As possible predictors of DI onset, the following factors were considered: gender (p=0.69), age (p=0.10), presence of prior surgery (p=0.53), hormone secretion (p=0.71), adenoma size (p=0.03), its consistency (p=0.01) and extent of tumor removal (p=0.71). The final model of logistic regression included factors interaction (Table 1): In the group of microadenomas, the influence of age was OR=0.963, CI= [0.94; 0.987], in macroadenomas – OR=0.977, CI= [0.957; 0.997], in giant adenomas – OR=0.99, CI= [0.971; 1.01]. The greatest impact the age rendered in increasing DI had in the group of microadenomas, but in the case of giant ones it was about 0.
Estimated OR and 95 CI for Size controlling for Age are shown in (Table 2). The size effect depended on the patients’ age. In young patients (30-year-old) the risk of DI was 1.51 times higher with increasing of tumor size by one grade in while in elder patients (60-year-old) it was 2.3 times higher. The transition from suctionable to unsuctionable increased the risk of DI 2.89 times (CI= [1.18; 7.07], p=0.020). In our opinion, the main cause of DI was changes in the shape and size of the pituitary gland in presence of giant and macroadenomas that determined bad visualization of the gland during surgery (Table 3). One of the most important surgical characteristics of an adenoma is its consistency. More dense and unsuctionable tumors have a higher risk (2.89 times) of post-op DI, because of worse identification of pituitary gland (p=0.020). No significant difference was found between the patients with and without surgical complications. The hormonal activity of adenomas had no effect associated with DI development (p=0.71) as well. In our study patients with prior surgery did not have a higher DI incidence (p=0.53). Smith et al. indicate that percentage of permanent DI after a first operation was 2.6% and while rate of transient DI after second surgery was 37.9% [10]. Also, patients with gross totally, subtotally or partially removed tumors had no differences in DI development (p=0.71).
Table 2: Estimated OR and 95 CI for Size controlling for Age.
Table 3: Extent of resection.
Note: *Tr DI – Transient Diabetes Insipidus; P DI – Permanent Diabetes Insipidus
Extent of Tumor Removal
The radicality of tumor removal was evaluated using contrastenhanced MRI within the first 72 hours. The resection extent is presented in (Table 4). Gross total resection was achieved in 74% (191/259) of cases. This group included all microadenomas and a part of macro- and giant adenomas, which were easily suctionable. A group of patients with subtotal (22%, 58/259) or partial removal (4%, 10/259) had unsuctionable macro- or giant adenomas, and giant adenomas with big antesellar part. The radicality of tumor removal depended on a tumor’s consistency (р=0.009) and size (р <0.001) (Table 3).
Table 4: Surgical complications in 259 procedures.
Visual Outcome
Of the 146 patients with preoperative visual deficit, impaired visual acuity improved postoperatively in 61%, visual fields normalized in 61.6% Postoperative deterioration of visual function was detected in 6 patients including 3 cases of visual acuity deterioration and 3 cases of deterioration of both visual acuity and fields. These patients had macro and giant adenomas with a large suprasellar part and had already been suffering from severe visual impairment. Fifty-three patients did not have any changes in their visual fields. The visual acuity stayed the same after surgery in 51 patients.
Overall Complication Rate
34 patients developed different complications in the early postoperative period, while the remaining 225 patients had no complications whatsoever (Table 4).
Postoperative CSF leakage
In 8 patients (3.1%) a postoperative CSF leakage occurred. One of the patients had microadenoma, 4 patients had macroadenomas and 3 patients – giant adenomas. In 4 cases we did not use vascularized or mucosal flaps. Artificial dura or a fat graft was used instead. In two cases necrotization of the vascularized flap was observed. One patient developed CSF leakage after skull base reconstruction due to necrosis of the vascularized flap. Another patient developed hydrocephalus of normal pressure. In that case, we first performed a ventriculoperitoneal shunting and then did a reoperation.
Meningitis
8 patients (3.1%) developed meningitis. All of them were patients with intraoperative CSF leakage. Six of them had CSF leakage postoperatively. They were treated with ceftriaxone (4.0 per day) or vancomycin (2.0 per day) and meropenem (6.0 per day). The treatment was successful and no neurological deficit after meningitis was observed.
Epistaxis
One patient (0.4%) developed postoperative epistaxis in 6 hours after surgery and required reoperation. This patient was operated using a unonostril approach. The sphenoidal sinus was opened on both sides but the mucosa on the opposite side was left intact. The bleeding originated from the opposite – side ramus of sphenopalatina artery.
New Visual Deficit
6 patients (2.3%) (2 had a macroadenoma and 4 – giant adenomas) developed a new visual deficit after surgery. In 3 cases of giant adenoma, the patients had both vision and visual fields impairment. The other patients had only visual acuity deterioration. In 5 cases, these new symptoms were gone after treatment. One patient did not have any improvement despite of the treatment.
Hemorrhage/Swelling of Residual Tumor
There was one case of thalamus hemorrhage that required external ventricular drainage. This patient developed a new neurological deficit (diencephalon syndrome), which regressed after the treatment. One more patient developed an asymptomatic ventricular hemorrhage after total removal of the macroadenoma that did not require any additional treatment. A third patient had swelling of residual tumor after partial resection and was reoperated.
Surgical Mortality
The surgical mortality rate was 0.8% (2 patients). The first patient had macroadenoma and Cushing’s disease. The tumor had an invasive growth. It was almost unsuctionable and therefore was not totally removed. After the operation, the patient developed hemiparesis followed in 8 days by deep vein thrombosis and cavafilter implantation. Within the next 7 days, the patient developed pulmonary embolism and on the 34th day after the operation he died. The second patient was a 54-year-old woman with a nonfunctional macroadenoma. During the operation we had no difficulties, and the tumor was removed gross totally. The first day after the surgery she was verticalized and developed pulmonary embolism. A cavafilter was implanted, and thrombus fragmentation was performed. The patient died on the 4th day after the surgery.
Diabetes Insipidus
The DI diagnostics was based on the level of electrolytes (serum Na >145 mmol/L), urine-specific gravity (1.004 or less) and excessive volumes of urine (quantified as more than 300 mL of urine per hour for 3 consecutive hours). In this study there were no patients with preoperative DI. After DI was diagnosed all the patients were treated with desmopressin (the dose was titrated by the level of diuresis). In this series of 259 patients, 111 cases of postoperative DI (42.9%) were diagnosed. 21 patients (8.1%) had transient DI and 90 (34.8%) – permanent DI. Since only the early postoperative period had been analyzed we considered transient DI to be the one that regressed during hospital admission. The patients’ data and tumor characteristics are summarized in (Table 5).
Table 5: Demographic characteristics and tumor characteristics in patients with or without postoperative DI.
Discussion
According to the literature, the rate of surgical complications after removing pituitary adenomas varies between 9% [11] and 35.8% [12] (in average 12.1%). The incidence of CSF leakage is about 3.1-4.7% [3,11-20] (minimal is 1.8% [20], maximal is 19.5% [21]). Smith et al. report 0% of CSF leakage in surgery of microadenomas. Contrariwise, in the study of giant adenomas (Koutourousiou M. et al.) rate of CSF leakage is 16.7%. Based on these data, we can conclude that percentage of postoperative CSF leakage depends on a tumor’s size. Another possible complication after endoscopic surgery is meningitis whose mean rate is 2.0-2.7% [21-24]. In most cases, it has been successfully treated by antibacterial therapy [25- 27]. Hemorrhage inside the residual tumor or its swelling occurs in 0.4-4.0% of patients [28,29] and can lead to new visual (0.9-4.4%) [30] or neurological deficit (0.4-2.3%) [31]. The most common are cranial nerve (III, IV, VI) dysfunction, hemiparesis (0.2-1.0%) and diencephalon syndrome [32]. The incidence of epistaxis in the studies rates from 0.4 to 2.9% [32]. In most cases nasal cavity tamponade is effective, but some cases require a revision surgery.
The rate of surgical mortality varies from 0.6 to 1.8% [33]. The main reasons of mortality are hemorrhage, somatic pathology (cardio-vascular disease, acute pancreatitis etc.), meningitis, ischemic stroke due to the damage of internal carotid artery, hard electrolytes irregularities (because of involvement of diencephalon region), pulmonary embolism, subarachnoid hemorrhage (in case of undiagnosed aneurism) [33]. In our study we did not find any difference between complications and DI postoperatively. DI belongs to a group of hereditary or acquired polyuria and polydipsia diseases. It is associated with inadequate arginine vasopressin (AVP) or antidiuretic hormone (ADH) secretion or renal response to AVP, resulting in hypotonic polyuria and a compensatory/ underlying polydipsia. The characteristics of DI polyuria include polyuria (>50 mL/kg), diluteurine (osmolality <300 mOsm/L), and increased thirst (water intake of up to 20 L/day). Untreated DI can cause hypovolemia, dehydration, and electrolyte imbalances. There are different types of DI such are central, nephrogenic, gestational and primary polydypsya. This paper refers only to central DI (CDI) [34].
CDI or neurogenic DI is the most common form of DI, occurring equally in both sexes and at any age. It is caused by inadequate synthesis/release of AVP, often secondary to surgery or to a head injury causing traumatic injury to the hypothalamus or posterior pituitary gland and destruction/degeneration of neurons originating in the supraoptic and paraventricular nuclei of the hypothalamus. DI Symptoms manifest themselves after 80–90% of the magnocellular neurons in the hypothalamus are damaged. Damage to the proximal part of the hypothalamo-neurohypophyseal region kills more neurons than do injuries to the distal region. However, proximal injuries account for 30–40% of posttraumatic and postoperative CDI, while distal injuries account for 50–60% of cases. Acquired CDI is more common than congenital one, and about 25% of adult CDI cases are idiopathic. Children with acute injury to the nervous system and CDI have a high mortality rate. Traumatic brain injury is associated with high mortality and acute and chronic morbidity [34]. Pituitary surgery results in CDI with a wide range of incidence (1–67%). Minimally invasive surgery has a low incidence of postoperative CDI (transient CDI 13.6% and permanent CDI 2.7%). Abnormalities in the secretion of AVP usually begin during the intraoperative period. The incidence of immediate postoperative DI is higher among the patient’s undergoing surgery by the traditional method than by the endoscopic transsphenoidal method (36% vs. 15%). The incidence of long-term DI did not vary significantly between the groups [34].
The history of desmopressin started from the first use of vasopressin to treat CDI in 1913. That time it was pituitary extracts containing oxytocin and vasopressin. Pitressin (vasopressin tannate in oil) became available for clinical use in the 1930s and was the principal drug for DI treatment almost until the 1970s when desmopressin was introduced. Substitution of the 8th residue of vasopressin with the D-isomer of arginine diminished the pressor effect of vasopressin. This synthetic analog of vasopressin, 1‑deamino‑8‑D‑AVP (DDAVP), or desmopressin, has increased and prolonged antidiuretic effect, decreased vasoconstrictive and oxytocic effects, reduced side effects (hyponatremia and convulsions), and enhanced resistance to vasopressinase. It can be administered in the form of intranasal spray, oral tablets, and orally disintegrating tablets (ODT) [34]. In our study, the patients received only the oral tables. The minimal initial dose of desmopessin is 0.1 mg. The titration control included blood electrolytes, urine-specific gravity and production of excessive volumes of urine. The maximum dose is 0.2 mg twice a day. In this study an attempt was made to determine the relation between postoperative DI frequency and different characteristics of adenomas, surgical complications and extent of resection.
In the literature, the rate of DI is estimated to be between 8.7% and 18.3%. In their study of giant adenomas M. Koutourousiou et al. have reported 9.6% rate of permanent DI, and PG Campbell et al. in their study of growth hormone secreting adenomas have detected no cases of permanent DI while transient DI have occurred in 7.7% of patients. Multivariate analysis of our cases showed the predictors of DI were patient’s age, size and consistence of tumor. In our study, we revealed the influence of adenomas size relative to a patient’s age. For older patients the size of the adenoma was a stronger factor than for the younger ones. In other words, in the elderly patients the tumor size has a greater effect on the risk of DI development. These data contradict to the results obtained by Sigounas et al. in 2008 who has not revealed any correlation between DI and tumor size. In our opinion our findings are related to the anatomy of a pituitary gland. The older a patient the more prone the gland is to hypoplasia while the risk its injury is lower, especially in case of microadenomas. Macroadenomas and giant adenomas are often found in close proximity to the pituitary gland that increases the risk of its injury and DI development after surgery. In case of giant adenomas, the last squeeze the gland a lot, but in case of microadenomas, when we usually observe healthy hypophysis tissue, the hypoplasia will play a major role.
The second important factor was consistence of tumor. The unsuctionable adenomas increased the risk of DI 2.89 times. This dependency also can be related to the tumor’s intimacy to the gland making the last more prone to injury and increasing the risk of DI development. The rate of all complications also depends on the surgeon’s experience. Ciric et al. analyzed complications in three groups of patients who were operated by surgeons with experience less than 200, 200-500 and more than 500 cases respectively. It has been demonstrated that those patients who were operated by surgeons with experience less than 200 surgeries (as in our study) had higher incidence of not only surgical complications, but also higher rate of DI (19%).
Conclusion
The endoscopic transsphenoidal surgery is the treatment of choice for patients with pituitary adenomas. Complications are rather common after endoscopic surgery and include two big groups that are surgical and endocrine complications. Further studies into the incidence and causes of postoperative diabetes insipidus and other complications can contribute to the reduction of both types. We can conclude that the predictors of DI include the patient’s age, size and consistence of adenomas. The influence of adenomas size depends on the age of a patient. The risk of DI in 30-year-old patients has been 1.51 times higher with increasing of the size group by one grade (micro, macro, giant), while in the elder patients (60-year-old) it has increased 2.3 times. Nevertheless, in case of giant adenomas the age has not been the impact factor to trigger DI after surgery. The tight consistence of tumor has been another important factor to provoke DI after surgery. The unsustainable consistency increases the risk of DI 2.89 times. The hormone activity of adenomas, prior surgery, extent of surgery have not been associated with DI development. The DI rate after endoscopic resection is 42.9% (in 8.1% of cases the patients developed transient DI and 34.8% – its permanent form).