Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Source-Induced Dissociation Vs Collision-Induced Dissociation Fragmentation Behavior of Four Antiviral Drugs in a Liquid Chromatography Ion-Trap Mass Spectrometry
Introduction
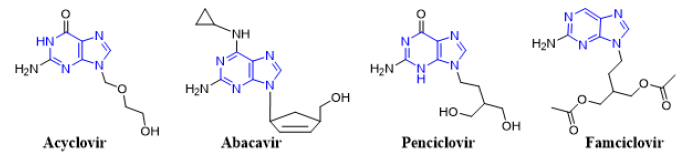
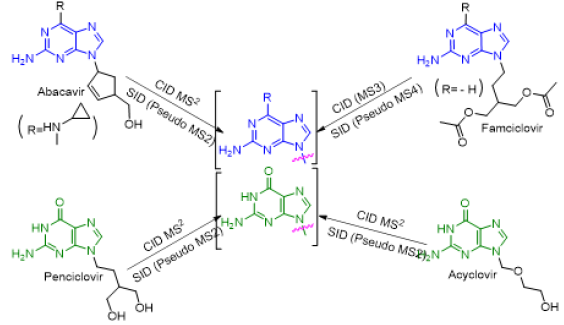
Mass spectrometry (MS) is an important tool for analyzing or detecting a wide range of organic, inorganic, natural, unnatural molecules, especially drugs, proteins, peptides are of interests beside routine analysis [1]. MS measures the mass-to-charge ratios of ions of an ionized sample, which may be gas, liquid or solids. Mass-to-charge ratios may obtain for a charged molecule or charged fragments. MS has both quantitative and qualitative uses. Numerous ionization methods are used in MS experiments, such as chemical ionization (CI), matrix assisted laser desorption ionization (MALDI), electron impact (EI), atmospheric pressure chemical ionization (APCI), and electrospray ionization (ESI). ESIMS has been applied to the analysis of oligonucleotides [2, 3] drugs and drug metabolites [4] oligosaccharides [5, 6] environmental contaminants [7, 8] glycoproteins [9] and many other types of compounds [10-15]. In atmospheric pressure ion sources, e.g., ESI or APCI, dissociation of ions can occur inside the ionization source (source induced dissociation; SID) before reaching the mass analyzer. SID has been used by several research groups [16-22]. Usually, SID is used to analyze single mass, whereas CID is used to analyze fragmentation. Both SID and CID techniques having advantages and disadvantages [23, 24]. While CID technique is very much effective to analyze pure sample with much more information about structural data [25]. Acyclovir, [26, 27] abacavir, [28, 29] famciclovir [30-33] and penciclovir [10] are the known antiviral medication used to prevent viral diseases. All of these antiviral drugs having common purine moiety [34] (Figure 1) and 9-position of purine are substituted with deferent alkyl chains. Mass spectrometric study of these structurally similar compounds may reveal lots of information for further analysis process during antiviral doses. As a medicinal chemist, it is our duty to develop drug molecules / administration procedures / toxicity evaluation process and / identification in a mixture or in biological matrixes. Therefore, there is always a room for extending such development using modern scientific methods such as mass spectrometry.
Figure 1: Chemical structures of antiviral acyclovir, abacavir, penciclovir and famciclovir showing a common purine nucleus.
Here, analysis of four antiviral drugs acyclovir, abacavir, penciclovir and famciclovir serves to figure out how to extend the qualitative power of ITMS and to maximize the benefit from this mass analyzer. These four drugs also were selected as they contain a common purine nucleus in their chemical structures which might generates a common fragmentation pattern. Above mentioned four known antiviral drugs were studied for their fragmentation pathways and data of SID and CID of ESI IT were compared. The detail fragmentation pathways of all ions observed in the in-source fragmentation spectrum of compounds were elucidated by further dissociation of each of these fragment ions using MS2, MS3 and MS4 fragmentation stages.
Experimental
An Agilent 6320 Ion-Trap connected (LC-MSn) mass spectrometer was used. Compounds were dissolved in DMSO and used as standard solution, then diluted with a mixture of HPLC grade water and acetonitrile (1:1). Fragmentation pattern of these four antiviral drugs by direct injection using infusion pump were performed. 10 μL of each sample was injected with direct injection, flow rate was 0.4 ml/min., run time was set to 5 minutes, drying gas was N2 (flow was 12 L/min), temperature was set to 350 °C, nebulizer pressure was 50 psi, smart target was 10,000, accumulation time 150 ms, scan range was 20- 400Da and Ion source was ESI, in positive mode with ultra-scan. There are several factors that can influence the fragmentation spectra, such as the collision energy, major precursor ion, electrospray mode (positive or negative) and capillary exit voltage. In IT, product ion scan was performed before the in-source fragmentation to determine each compound’s related fragment ions, the capillary exit voltage was optimized to produce adequate in-source fragmentation. The data compared to multistage fragmentation using CID. We made all default parameters except capillary exit voltage which was 100 V for CID and 200 V for SID.
Results and Discussion
CID MSn Fragmentation Pattern of Abacavir
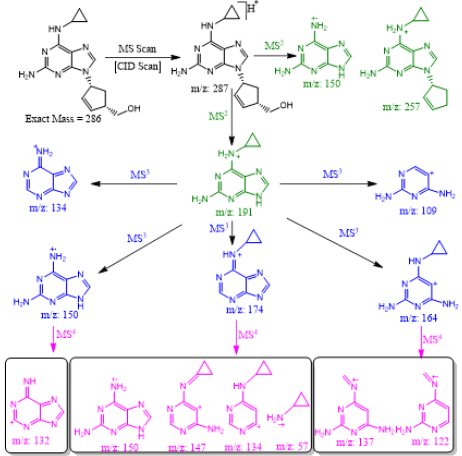
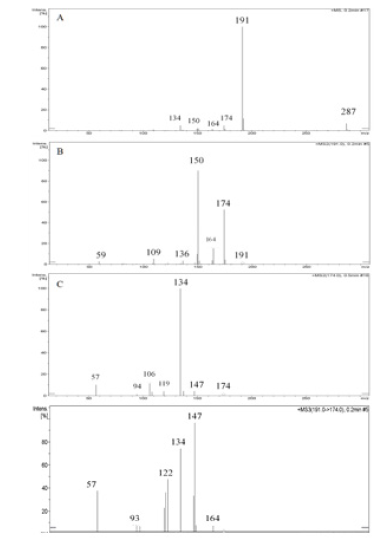
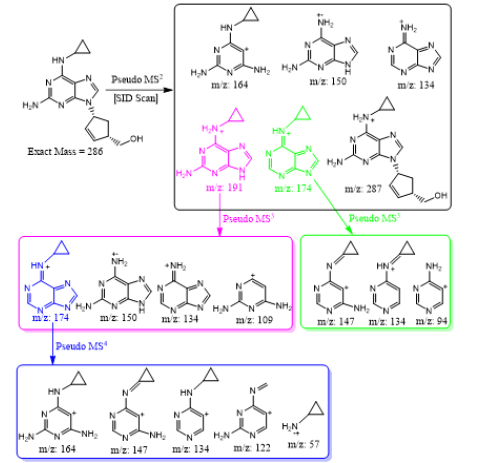
Abacavir was set for an example of comparing two fragmentation techniques. As shown in (Figures 2 & 3), full scan of abacavir gave m/z 287 (Figure 2A) and MS2 of abacavir gave three fragments at m/z 257, 191 and 150 (Figure 2B). Among three fragments, m/z 191 was a prominent peak which was further bombarded (MS3) and gave m/z 174, 164, 150, 134, 109, 83 and 59 (Figure 2C). Consequently, high intense three ions m/z 174, 164 and 150 were further bombarded (MS4) in which, m/z 174 gave four ions at m/z 159, 148, 132 and 157 (Figure 3A), m/z 164 gave two ions m/z 137 and 122 (Figure 3B), and m/z 150 gave a single ion at m/z 132 (Figure 3C).Based on (Figures 2& 3), we have drawn Scheme 1 for the fragmentation pattern of abacavir in CID mode. As shown in scheme 1, after four steps (MS4) fragmentation, abacavir gave maximum fragments at m/z 150, 147, 137, 134, 132, 122, and 57. SID pseudo-MSn fragmentation pattern of abacavir. As shown (Figure 4), pseudo MS2 of abacavir gave m/z 287, 191, 174, 164, 150 and 134 (Figure 4A), and pseudo MS3 of major two fragments, m/z 191 and 174 was further bombarded (MS3) and obtained m/z 191 gave m/z 174, 164, 150, 136, 109 and 59 (Figure 4B) and m/z 174 gave m/z 147, 134, 119, 106, 94 and 57 (Figure 4C), respectively. Pseudo MS4 of high intense m/z 174 gave m/z 164, 147, 134, 122, 93 and 57 (Figure 4D).
Scheme 1: CID MSn fragmentation pattern of protonated abacavir.
Figure 2: CID MSn fragmentation pattern of abacavir: A. MS scan for abacavir, B. MS2 of 287 and C. MS3 of 191.
Figure 3: CID MS4 fragmentation of three ions (174, 164 and 150): A. MS4 scan of 174 B. MS4 scan of 164 and C. MS4 scan of 150
Figure 4: SID pseudo-MSn fragmentation pattern of abacavir: A. MS scan for abacavir applying capillary exit voltage, B. product ion for 191 C. product ion for 174 and D. MS3 for 174.
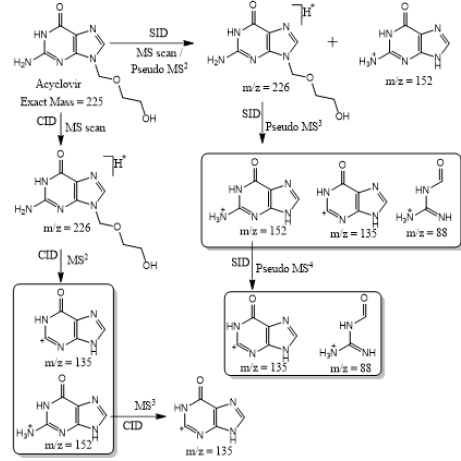
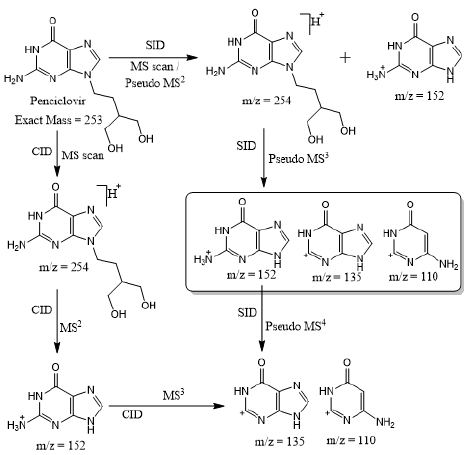
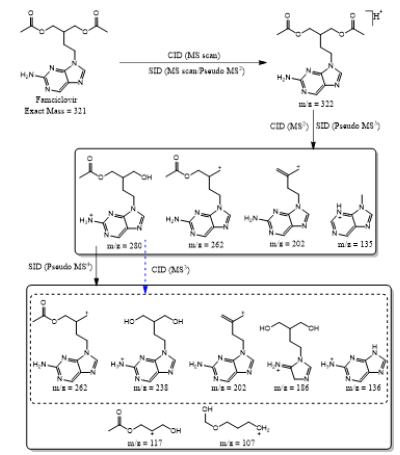
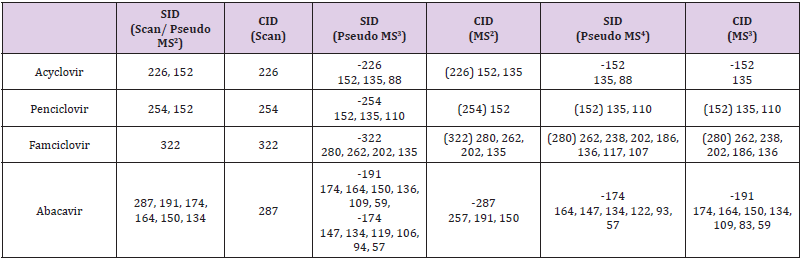
Based on (Figure 4), we have drawn Scheme 2 for the fragmentation pattern of abacavir in SID mode. As shown in scheme 2, in two steps (pseudo MS3) fragmentation, abacavir gave maximum fragments at m/z 174, 150, 147, 134, 132, 109 and 94 and pseudo MS4 of m/z 174 gave five fragments at m/z 164, 147, 134, 121 and 57. SID and CID of acyclovir, penciclovir and famciclovir. Other three antiviral drugs acyclovir, penciclovir and famciclovir mass spectrometric study in SID and CID results are summarized in Table 1 along with abacavir. As shown in Table 1 and depicted in Scheme 3, SID scan of acyclovir gave m/z 226 [M+H] + with 152 and MS2 of main peak m/z 226 gave three main fragment at m/z 152, 135 and 88. Among three fragments, m/z 152 was further bombarded and obtained m/z 135 and 88. On the other hand, in CID scan, acyclovir gave m/z = 226 [M+H] + only. Which was further bombarded for MS2 and obtained m/z 152 and 135 only. MS3 of m/z 152 gave only one fragment from SID at m/z 135.As shown in Table 1 and depicted in Scheme 4, SID scan of penciclovir gave m/z 254 [M+H] + with 152 and MS2 of main peak m/z 254 gave three main fragment at m/z 152, 135 and 110. Among three fragments, m/z 152 was further bombarded and obtained m/z 135 and 110. On the other hand, in CID scan, penciclovir gave m/z = 254 [M+H] + only. Which was further bombarded for MS2 and obtained m/z 152 only. MS3 of m/z 152 gave same fragments as we obtained from SID, which is m/z 135 and 110. As shown in Table 1 and depicted in Scheme 5, SID and CID scan of famciclovir gave only protonated peak at m/z 322 [M+H] +. MS2 of this m/z 322 also gave four same fragments at m/z 280, 262, 202 and 135. Among those peaks, a main peak m/z 280 was further bombarded and obtained seven fragments m/z 262, 238, 202, 186, 136, 117 and 107 in SID and 5 fragments m/z 262, 238, 202, 186 and 136 in CID. Common fragmentation paths of abacavir, acyclovir, penciclovir and famciclovir.
Scheme 2: In source fragmentation pattern of protonated abacavir.
Scheme 3: Fragmentation pattern of acyclovir.
Scheme 4: Fragmentation pattern of penciclovir.
Scheme 5: Fragmentation pattern of famciclovir.
Table 1: MSn fragmentation behavior of acyclovir, penciclovir, famciclovir and abacavir.
As depicted in Scheme 6, all four antiviral drugs gave similar fragmentation pathway. Abacavir, acyclovir and penciclovir gave purine moiety while SID / CID MS2 was applied, on the other hand, famciclovir gave similar pathway with purine moiety while SID (Pseudo MS4) / CID (MS3) was applied (Scheme 6).
Scheme 6: Fragmentation pathways of all antiviral drugs (abacavir, acyclovir, penciclovir and famciclovir).
Conclusion
Excellent qualitative information was obtained using sourceinduced dissociation (SID) comparing to collision-induced dissociation (CID) in an ITMS. Fragmentation pathways of four antiviral drugs abacavir, acyclovir, penciclovir and famciclovir gave similar information regardless fragmentation method as they contain purine nucleus in their building blocks. This method can be applied for the detection /identification of know/unknown drugs or their metabolites in-vitro / in-vivo or in biological matrixes by comparing their fragmentation pattern and using different possible fragmentation tools to maximize the benefit of ITMS in the process of drug development.
Microbial infections are still a challenge despite of the existing of numerous potent antibiotic drugs and other modern antimicrobial means, Bacterial infections are still a major cause of mortality. The problem is that major groups of antibiotics, currently in use, generally affect three bacterial targets: cell wall synthesis, translational machinery, and DNA replication. Unfortunately, bacterial resistance may develop against each one of these modes of action. In addition, the use of conventional antibiotics carries a major risk for resistance of viable bacteria. Nanoparticles as antibacterial agents complementary to antibiotics are highly promising and are gaining large interest as they might fill the gaps where antibiotics frequently fail. This includes combatting multidrug-resistant mutants and biofilm. Nanotechnology is a technology conducted at the nano-scale in the fields of fabric manufacturing, food processing, agricultural processing, and engineering, as well as in medical and medicinal applications. Over the present decade, several studies have suggested that nanoparticles are excellent antibacterial agents, thus nanomaterial applications for antimicrobial works have prime interest by many researchers. Several reports showed that some of the metal oxide nanoparticles have toxicity toward several microorganisms and they could successfully kill numerous bacteria. This new approach has been identified to deal with resistance of pathogenic microorganisms because of their inherent antimicrobial activity. The use of nanoparticles as antimicrobial components especially in the food additives and medical applications can be one of the new and considerable strategies for overcoming pathogenic microorganisms. Based on literature review there are some effective factors that can influence the ability of nano materials in reducing or killing the cells. Mechanisms for nanomaterial against bacteria, which are briefly listed as follows: surface charge of the metal nanomaterial, shape, type and material, concentration of nanomaterial, dispersion and contact of nanomaterial to the bacterial cell, presence of active oxygen, liberation of antimicrobial ions, medium components and pH, physicochemical properties, specific surface-area-to-volume ratios, size, role of growth rate, role of biofilm formation, and cell wall of bacteria. Nanoparticles as antimicrobial agents have become an emerging approach which can establish an effective nanostructure to deliver the antimicrobial agents for targeting the bacterial community efficiently. In addition, they are so potent that microbial pathogens cannot develop resistance towards them. On the other hand, most of the metal oxide nanoparticles have no toxicity toward humans at effective concentrations used to kill bacterial cells, which thus becomes an advantage for using them in a full scale. Metal, metal oxide and organic nanoparticles now are used show a diversity of intrinsic and modified chemical composition properties. Thus, it is not surprising that they have numerous modes of action as antimicrobial agents. In some cases the ratio between the bacteria and the nanoparticles is critical to the bacterial toxicity. In addition, many factors play a role and affect the lethal effect of nanoparticles to bacteria including aeration, pH, and temperature, size, shape, chemical modification and coating, and mixture in various ratios with other nanoparticles and solvent used. Lethal effect of nanoparticles is generally due to membrane damage occurs when nanoparticles bind electrostatically to the bacterial cell wall and membranes, leading to alteration of membrane potential, membrane depolarization, and loss of integrity which, in turn, result in an imbalance of transport, impaired respiration and cell death. Among inorganic metals silver nanoparticles have been widely used as an effective antimicrobial agent against bacteria, fungi, and viruses. The antimicrobial efficacy of silver (Ag), as of other metals and metal oxide nanoparticles, was reported to be size-dependent. Although the Ag nanoparticle mechanism of action is still not clear, small diameter Ag nanoparticles have a superior antimicrobial effect to those of a larger diameter In comparison to silver, gold- (Au-) nanoparticles are less potent and have almost no antibacterial effect by themselves. Except when they of an antibacterial approach, adopted from cancer treatments, gold nanoparticles bound to Fe3O4 and activated by photothermal means. In addition, Titanium oxide with its photocatalytic effect serves as an antimicrobial agent for both positive and negative bacteria. An interesting approach in the antimicrobial application of nano- metals and nano- metal oxides is the synergistic effect of the combination between two or more of them as Titanium and silver. Moreover, Zinc oxide nanoparticles were shown to have a wide range of antimicrobial activity. This metal oxide is characterized by its low cost and low toxicity to human cells, thus it was used as coating materials designated for medical and other devices. White color, UV-blocking, and ability to prevent biofilm formation made its nano particles suitable for fabric treatment. Zinc was approved by the FDA as a food additive. Another metal oxide used as an antibacterial agent is copper oxide nanoparticles have been shown to be effective against various bacterial pathogens especially gram positive Bacilli. In our lab we obtained excellent results by applying these approaches in many fields of polymers and textile.
The Texas Networking for Science Advancement (NSA) team formed in 2016. The team now consists of 15 faculty from 10 Texas universities. Five of the partnering universities are classified as Hispanic-Serving Institutions (at least 25% Hispanic enrollment) and the other five are considered as Hispanic-emerging (16- 24% Hispanic enrollment). Two of the 10 institutions are private universities, and the remaining are public. To date, the team has published results of eight studies (two currently in press) evaluating general chemistry students’ QR arithmetic automaticity skills (what students can do without a calculator) using the Math- Up Skills Test (MUST), a 20-question, 15-min, hand-graded, openended diagnostic instrument [1-3]. One of our carrots to encourage students to try this quiz without using their trusted calculating devices is that the MCAT is a calculator-free evaluation instrument and over 50% of our general chemistry students indicate an interest to enter the health professions.
The Good
From the very first observation, the team’s results provided a linear trend-the better students’ arithmetic skills the better their general chemistry averages in both first- and second-semesters. The results not expected are that there is a stronger relationship between what students can do without a calculator (their automaticity) than what they can do with a calculator. Yes, the students did better on the MUST with a calculator but the effect size without a calculator is stronger. The statistics consistently support that the MUST is highly reliable (KR-20 > .80), has good internal consistency (Cronbach’s alpha > .85), and the Cohen’s d for the MUST is consistently > 1.0 indicating a large effect size for a population of over 10,000 students. Using the MUST has provided the team with a diagnostic instrument that allows instructors the ability to identify at-risk students in 15 min the first week of classes. Being able to identify these students who will struggle with the course material early in the semester provides ample time for corrective measures to be employed in hopes that students will take advantage of the opportunity but herein lies the rub: it’s the rich that get richer! Pilot studies indicate that this trend carries onto lower-level organic chemistry courses.
The Bad
The original study came about because the team noticed that Texas students’ SAT scores were consistently declining below the national average. This trend coincided with the Texas Education Agency (TEA) mandated change from a 4×4 high stakes testing system consisting of a series of four exams per year in four subjects (mathematics, science, social studies and English) during the final four years of secondary school. TEA’s current testing-system focuses on only two STEM areas (biology and first-year algebra) along with first- and second-year English and US History. The TEA calculator policy states no calculators are permitted on STAARs (State of Texas Assessments of Academic Readiness) in grades 3-7, but districts must ensure that each student has a graphing calculator to use on all STAARs starting with 8th-grade mathematics (both paper and online versions) and biology. For the biology assessment, there should be one calculator (four-function, scientific, or graphing) for every five students. Students may bring their own calculators with them to the assessments, but internet capabilities must be disabled and calculation applications on smartphones are not allowed. Beginning in May 2018, the grade 8 science STAAR requires students to have access to calculators with four-functions, scientific or graphing capability. What is not obvious is how much these rules/ regulations are hurting the students’ future preparation for postsecondary success. Handheld calculators are generally accepted for classroom use and allow teachers to give beginning students realistic problems using tangible data gathered from the field. All is good but how many times do students calculate a negative mass or an unrealistic density and not have the quantitative-reasoning ability or basic number sense to know that the “calculator” answer is impossible or improbable.
The Future
When students enter post-secondary education with low automaticity ability, they lack the mental-math skills needed to succeed in general chemistry, a major gateway course to many STEM-major degrees. Adding more calculator-free instruction for all STEM and non-STEM majors in general chemistry (and other STEM courses) is advisable and will improve students’ mentalmath capability. Summer bridge programs, weekly recitations and the like should emphasize students’ automaticity skills to help prepare incoming students for success. However, quantitativereasoning (QR) skills (like those needed to understand how to read scientific data graphs and charts) are required to understand much of our current data-driven world needed to prepare global citizens for both STEM and non-STEM careers. Improving our students’ QR calculator-free skills is a place to start to attempt to improve retention and graduation rates for all students. Is this the answer? Maybe or maybe not, but what is obvious is that we are going in the wrong direction. Without a doubt, students need more quantitative-reasoning and quantitative-literacy skills to have a chance of succeeding in this data-driven world. To encourage students to use their calculator-free skills, teach part of your class without the use of a calculator. Ask students how they arrived at their answers, what is their logic-it might surprise you as to what they can and cannot do without using calculators, and as a result their automaticity abilities and MCAT scores might improve!
Acute Hyperuricemia Secondary to Epileptic Seizures Leading to Acute Urate Nephropathy: A Case report
Background
About two third of the body uric acid is produced endogenously while the rest of one third is from dietary products containing purines. Most of the uric acid is excreted through kidneys while the remaining through intestines. Hyperuricemia occurs either due to underexcretion of urate or overproduction of urate. Factors that predominantly effect uric acid excretion include tubular fluid Ph, tubular fluid flow rate and renal blood flow. Acute hyperuricemia can lead to acute uric acid nephropathy by renal tubular obstruction by urate and uric acid crystals which can lead to significant morbidity. Seizures is an exceedingly uncommon cause of acute hyperuricemia. This is one such case of a patient with Generalized tonic clonic fits leading to acute hyperuricemia which in turn caused acute urate nephropathy.
Case Presentation
A 35-year-old man with no premorbid presented in emergency department with generalized tonic clonic fits. At presentation patient had Bp of 130/70, Pulse 96, Temperature 98.7F, Oxygen saturation 97% with room air. Blood sugar random was 126mg/dl. He had two such episodes in last 30 minutes. Abortive therapy was given to control the fits. After initial management detail examination was done. Central nervous system examination was normal with no focal neurological deficit. Chest was clear bilaterally with rest of respiratory examination normal. Cardiovascular, Gastrointestinal and musculoskeletal examination was also normal. Complete blood picture showed leukocytosis with white blood cell count 22550/microliter with 80% neutrophils. Liver function tests, Renal function tests, C-reactive protein, Erythrocyte sedimentation rate, Serum electrolytes, Fasting lipid profile, Serum calcium, magnesium and phosphorus were also normal. Urine routine examination was normal with no myoglobinuria. CPK levels were 153 and serum prolactin levels were 404. Serum uric acid was 20.73 mg/dl. Chest x-ray, Electrocardiography and Echocardiography were normal. After 2 days his Renal function tests started deranging with Urea 45 mg/dl and creatinine 1.52 mg/dl. His previous renal function tests and uric acid were completely normal. Maximum urea and creatinine levels went up to 55 and 2.88mg/dl respectively. Patient was managed with intravenous hydration and allopurinol. His renal function tests and uric acid levels started declining and normalized after 5 days.
Discussion
In previous case studies it was noted that creatinine was deranged initially on the day of presentation. In our case unusual was that patient’s creatinine was normal at presentation and started rising after 2 days. So, it is important to follow patient’s Renal function tests for at least 4-5 days post seizure so that acute renal failure is not missed which can prove fatal if not managed early. Secondly in previous studies maximum level of high uric acid levels were up to 15mg/dl while in our case serum uric acid was extremely high with levels up to 20.73 mg/dl which was managed successfully with early intervention. Uric acid is the final insoluble waste product of purine breakdown [1]. Uricase enzyme which allows converts insoluble uric acid to soluble allantoin in absent in humans because of which it accumulates in the distal part of nephron particularly in acidic environment leading to toxicity [1,2]. Multiple studies have proven that high uric acid level is linked with many systemic illnesses including hypertension, chronic kidney disease, cardiovascular disease, diabetic nephropathy, stroke and acute kidney injury [3,4]. Tumor lysis syndrome is the most common cause of acute hyperuricemia through high cell turnover and cell lysis following aggressive chemotherapy for cancer particularly lymphoma [1,2]. When urinary uric acid surpasses solubility threshold, it is deposited and accumulated as crystals in renal tubule leading to acute renal failure [2]. High uric acid levels have been implicated to change the basic architecture of renal histology and have an important role in acute and chronic renal injury [5]. Acute uric acid nephropathy is characterized by raised creatinine levels; high uric acid levels raised urinary urate to creatinine ratio [6]. High uric acid causes acute urate nephropathy by various mechanisms including uric acid crystal formation and non-crystal mediated pathway [6]. Acute urate nephropathy must be suspected in high risk patients who develop acute renal failure with high serum uric acid levels and presence of urate crystals in urinary sediment [2]. Various mechanisms proposed in the development of acute kidney injury secondary to hyperuricemia include uric acid crystal formation in tubules, renal vasoconstriction, endothelial dysfunction, stimulation of inflammatory response, oxidative stress, antiangiogenic changes and direct microvascular injury [6]. Acute uric acid nephropathy is reversible [1]. Epileptic fits cause skeletal muscle breakdown which in turn causes life threatening rhabdomyolysis leading to acute kidney injury in 15% of patients [7]. Rhabdomyolysis releases high amount of myoglobin by breakdown of muscle cells which in turn results in high serum myoglobin levels. Raised serum myoglobin levels exceeds haptoglobin binding capacity resulting in myoglobinuria which causes cast formation and tubular obstruction leading to acute kidney injury [7]. Various metabolic abnormalities have been associated with severe epileptic seizures including lactic acidosis, raised ammonia, raised creatine phosphokinase and high prolactin levels [2]. Rare metabolic derangements associated with seizures include electrolyte changes, hyperuricemia and osmolality changes [2]. Fits induced hyperuricemia is one of the rarest complications described in literature even more rare when associated with acute urate nephropathy [2]. Seizures cause acute uric acid nephropathy by increasing uric acid levels and provide favorable environment for urate crystal formation [6]. It is speculated that acute hyperuricemia secondary to seizures occurs both due to overproduction and impaired tubular excretion of urate [1]. Muscle injury during seizures causes tissue breakdown which release nucleosides leading to its transport into liver and is converted into uric acid by urea cycle [6]. Factors that lead to hyperuricemia following fits include acidification of urine secondary to acidosis caused by lactate production and hypoventilation making urate less soluble, dehydration secondary to hyperthermia and profuse diaphoresis causing increase tubular water reabsorption leading to high tubular uric acid secretion and renal ischemia due to shunting of blood from viscera to muscles [2]. Most effective therapy to lower uric acid levels is Rasburicase which is a recombinant form of xanthine oxidase [2]. Allopurinol inhibits uric acid formation, but it does not remove already existing urate in the body and may also worsen acute renal injury by releasing xanthine [1]. Urinary alkalization can increase urate solubility but has not yet been proven to be effective in acute urate nephropathy [1]. Oliguria secondary to acute urate nephropathy have excellent response to hemodialysis [1].
Conclusion
In nutshell acute hyperuricemia is an uncommon manifestation following a seizure. Immediate necessary steps should be taken to lower uric acid levels. Acute uric acid nephropathy is a reversible condition and if early management is done to lower urate levels it can prevent progression to acute renal failure with excellent fruitful outcome.
Clozapine-Induced Acute Interstitial Nephritis: A Case Report
Introduction
Clozapine is nowadays the most effective treatment for refractory schizophrenia. It has proven to be superior in terms of efficacy compared with 1st generation antipsychotic and other 2nd generation antipsychotic [1]. Moreover, it does not cause extrapyramidal side effects nor tardive dyskinesia and its impact on prolactin level is negligible [2]. This atypical antipsychotic is also used to treat other conditions such as schizoaffective disorder. However, clozapine is underprescribed, due to potentially lifethreatening side effects such as neutropenia, agranulocytosis, myocarditis and myocardiopathy and other additional problems including weight gain, orthostatic hypotension, constipation and sialorrhea [3].
Among uncommon adverse reaction, acute interstitial nephritis (AIN) should also be taken into account. Very few cases have been described and the underlying mechanism is still unclear [4-6]. It could be related to a nonspecific inflammatory response, which is often observed in the early weeks of treatment with clozapine. This drug indeed exerts some immunomodulatory effects that have clinical implications [7]. We report a case of a patient who experienced acute renal failure twice. Both episodes followed initiation of treatment with clozapine.
Introduction
A 54-year-old woman with a known history of schizoaffective disorder was admitted to our hospital in November 2020. She was diagnosed with schizoaffective disorder in 1988, at the age of 22. She had been treated with different antipsychotics during the past 30 years (quetiapine, haloperidol, chlorpromazine, levomepromazine, clotiapine, lurasidone) and she has a history of repeated and prolonged hospitalizations. The patient is also affected by hypothyroidism treated with levothyroxine, type 2 diabetes in insulin therapy and gallstones. Furthermore it is reported in her clinical history an episode of acute renal failure in December 2017, probably due to carbolithium, and an episode of acute pancreatitis in October 2019. In November 2020 a new hospitalization was necessary because of the relapse of the psychotic symptoms with agitation and suspiciousness in spite of the antipsychotic therapy with lurasidone and clotiapine. In consideration of the antipsychotic resistance, the therapy was switched to clozapine on 17th November, commenced at 25 mg/day up to 50 mg/day. On 19th November there was the onset of fever, partially responsive to paracetamol. In the following days the progressive increase of fever up to 39.5°C and the onset of desaturation occurred: oxygen therapy and an empirical antibiotic therapy were necessary. Eventually, all the causes of an infective disorder were excluded.
On 23rd November we observed a PLT reduction (96.000/uL), so clozapine was suspended. From 5th December we observed a progressive increase of the creatinine value, from 2,95 mg/dl up to 3,90 mg/dl. Her previous creatinine value was 0,85 mg/dl on 19th November 2020. The main causes of acute renal failure were excluded. The abdomen CT showed kidneys of normal size and morphology, without parenchymal bulks, stones or distension of the urinary tract, with a minimal edema of the perirenal fat on the left . The patient was evaluated by a nephrologist, who suggested to move her in the Unit of Nephrology to find the cause of the renal failure and to treat it. The cause was not established, but the renal function values gradually normalized. On 22nd December the patient was re-admitted to the Unit of Psychiatry. The patient’s clinical and psychiatric conditions gradually improved, so she was dismissed on 28th January.
On 2nd February a new episode of psychomotor agitation and relapse of psychotic symptoms occurred and the hospitalization was necessary. The patient was suspicious and contentious and she had persecutory delusions. On 11th February, considering the patient’s psychopatological conditions, clozapine was reintroduced. Again fever occurred after a single tablet of clozapine, followed by renal failure (06/02: creatinine value 1,19 mg/dl; 13/02 creatinine value 2,14 mg/dl, progressively increased up to 3,65 mg/dl in few days).
Evaluated by the nephrologist, a steroid therapy was prescribed and, on 16th February, the patient was moved again to the Unit of Nephrology. The diagnosis of iatrogenic interstitial nephritis caused by Clozapine was confirmed as diagnosis by exclusion and, after the stabilization of the renal function, the patient was retransferred to the Unit of Psychiatry. The therapy was switched to brexpiprazole: the renal function progressively improved up to 1,15 mg/dl and the patient’s clinical conditions slowly improved, until the dismissing on 14th April. The case was followed up for 6 months and we observed a gradual recovery of the renal function: actually the creatinine value is 0,99 mg/dl.
Discussion
To the best of our knowledge, this is the first case of clozapine-induced nephrotoxicity ever described in Italy. Acute interstitial nephritis is an immune-mediated condition featuring tubulo-interstitial inflammation and oedema. It can be infective, autoimmune or even idiopathic but more commonly it is induced by various drugs, such as NSAIDs and antibiotics like aminoglycosides and vancomycin [8-9]. The diagnosis of drug-induced acute interstitial nephritis is based on its clinical and laboratory manifestations, characteristic morphologic features of the kidney on biopsy, and the identification of a causative agent. In practice, satisfying all three criteria is fraught with limitations, particularly in patients exposed to several potentially incriminated drugs [10]. In this regard, a possible limitation of our study is the lack of renal biopsy.
Our results are in agreement with previous evidence, reporting the importance of renal function monitoring prior to clozapine initiation and during titration. Moreover, it is fundamental when clozapine is prescribed together with other potentially nephrotoxic medications. Further, is it of great interest to remember that early recognition of this phenomenon, also involving nephrologists, leads to prompt intervention and adequate treatment.
Simulation of a Laparoscopic Major Vessel Injury in a Live Animal Model
Introduction
Iatrogenic injury to major vessels with the ensuing bleeding is a rare but potentially life-threatening complication during laparoscopic major HPB surgery. The most commonly injured vessels are aorta, the iliac vessels, and the inferior vena cava [1]. Contrary to traditional approach suggesting immediate conversion to open surgery it is suggested nowadays that this kind of injury and bleeding should be approached laparoscopically [2]. An obvious requirement for such an approach is an appropriate training [3]. Advanced laparoscopy training currently includes box-trainers [4], virtual reality training [5], live animal training [6] and training that combines all of the above [7]. Unfortunately, the majority of training modalities in laparoscopy concentrate on purely technical knowledge not considering psychological burden of a major intraoperative disaster. While obtaining and maintaining technical skills is clearly important [8] the possibility of testing these skills in a stressful environment imitating operating room disaster could be the way to prepare surgeons to adequately react to the unexpected [9]. In this study we have tried to create an environment as similar to real life laparoscopic disaster as possible and observe trainees’ reactions and their ability to use technical skills to control the situation.
Materials and Methods
During three editions of advanced laparoscopic training course 12 participants faced a task of controlling a major vessel damage. Training course was designed for both experienced surgeons and novices in advanced laparoscopy. Each course lasted for two days. At the beginning of the first day the tutors explained the methods of laparoscopy bleeding control with a video footage. Each day of the course there were 7 hours of live animal laparoscopy training. The first part of the training was designed to achieve technical abilities in various steps of advanced laparoscopy procedures depending on the level of experience of each participant. In the second part of the training during the last 60 minutes of each day the participants were exposed to iatrogenic injury of a major vessel performed with an electrocautery on an area of approximately 1cm and were asked to control the bleeding and repair the damage. During these maneuvers their Heart Rate (HR) was monitored, and their reactions were video recorded. After successfully completing the task and if time permitted the same animal was used for another iatrogenic injury with another participant operating. Animals used for training were pigs and sheep. During the whole procedure the animals were taken care of by an experienced veterinary anesthesiologist. At the end of each course participants were asked to evaluate their experience in controlling the bleeding in a stressful environment using Visual Analogue Scale from 1 (very bad experience with no value for training) to 5 (the best type of training one can imagine).
Results
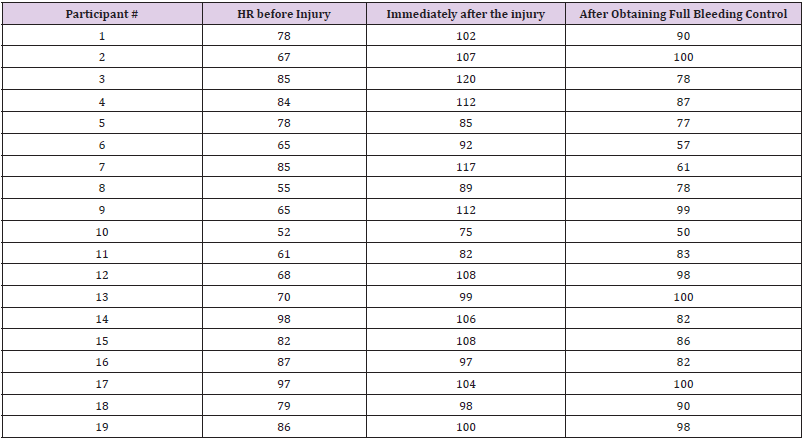
Altogether there were 19 episodes of iatrogenic injury in 10 animals controlled by 12 participants. One animal died after exsufflation due to relapse of bleeding after non-complete hemostasis. There were no conversions to open procedure. Temporary vessel control was obtained with a grasper, gauze, intraabdominal pressure elevation or temporary clip application. For final hemostatic purposes participants used Vicryl 2.0 or PDS II 3.0 suture. Heart rate of participants before the injury, during the repair and after obtaining a haemostasis is shown in Table 1. HR ranged from 52 to 97 per minute before the task and from 75 to 120 during the repair of injury. There was a tendency towards higher HR values before and during the task in experienced surgeons than in novices although this difference did not reach statistical significance. When evaluating this approach to training in disaster control eleven participants gave the exercise 5 points on a VAS scale and one participant gave it 3 points resulting in a total of 4.8 points for the whole group.
Table 1: Changes in participants’ heart rate before, during and after the vessel injury.
Discussion
With growing number of advanced laparoscopic HPB surgery worldwide there is a clear need for a structured laparoscopy training [3]. In order to prepare surgeons for these demanding procedures a variety of simulation models have been proposed so far. Advanced laparoscopy techniques can be taught in a simple boxtrainer. The box trainer however, apart from giving the opportunity to learn purely technical skills is much less effective in preparing for conditions in real life surgery [4]. A Virtual Reality (VR) training offers interesting approach to teaching without the need for the use of animal tissue and creating close to real life conditions. Unfortunately, at its current level of performance, it does not meet expectations. No additional benefit is observed from VR training in a multimodality laparoscopy training program [5]. A very interesting model with perfused pig liver can simulate almost lifelike conditions [7]. It is one of the few training modalities to offer trainees a highly simulated bleeding in order to acquire advanced laparoscopic suture skills and train under the pressure of bleeding [10]. The setting of such a training modality seems however too complex to be widely used for teaching laparoscopy. Also, contrary to the model described herein it does not offer the trainee the possibility to observe the effect of bleeding on a general status of the patients, concentrating only on the bleeding itself. In this sense, it seems closer to a box-trainer concentrating merely on a technical control of bleeding without the stress of observing worsening vital signs that clearly simulates real-life disaster. The closest to life experience can probably be achieved in live animal models [11]. It has been successfully used in creating a model for the intravascular treatment of IVC injury. In live anesthetized pigs after iatrogenic IVC injury a bleeding was controlled successfully by trainees using balloon insertion via femoral vein [12]. Live animal laparoscopy training using pigs has been shown to be useful in acquiring advanced liver laparoscopy skills [6]. While the benefits of this model over other approaches in teaching purely technical skills can be discussed it offers unique opportunity to create a simulation for a life-threatening intraoperative event. There are much less reports on the use of sheep as a model for advanced surgical training [12]. It is however known to be an interesting model for advanced colon resections [13]. During our study we have observed a higher level of stress measured as a rise in HR in more experienced trainees. While it was a bit surprising it can be explained by the fact that more senior surgeons are well aware of the potentially fatal complications of a major vessel injury during laparoscopy. Almost all participants including experienced and inexperienced surgeons agreed that this training modality was close to perfect in creating a stressful environment simulating reallife disastrous intraoperative event.
Conclusion
In-vivo pig and sheep models can be used for training in the management of major bleeding during HPB surgery. It is a modality that is highly appreciated by trainees. It seems that stress level during advanced exercises is higher in experienced surgeons than in newcomers.
Designing an Adjustable Head Frame for Surgery Using Mixed Reality Technology Hololens 2
Introduction
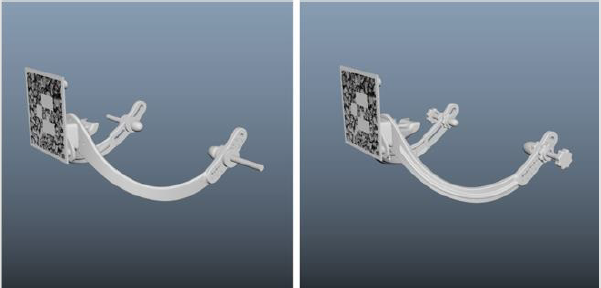
To position three-dimensional holograms to a strictly defined point in space, it is necessary to use special markers, which can be represented in the form of images [1], QR codes [2] or geometric objects [3]. In the case of using mixed reality technology in surgery, these markers must be rigidly linked to the patient’s anatomy in order to accurately position the 3D model of the anatomical structures. This can be achieved through the use of special frameholders of the marker [4], which are based on the individual anatomy of the patient and are made using the 3D printing method. The main disadvantage of such marker-holders is that for each patient it is necessary to design and manufacture a new marker-holder, which is time-consuming and expensive. To solve this problem, we have developed an adjustable frame (Figure 1), which is intended for performing operations on the head using mixed reality glasses [5]. This frame fits over the patient’s head and adjusts to his individual parameters. This device is entirely made of polyamide, which allows it to be sterilized before each procedure and used repeatedly in various operations related to neurosurgery and maxillofacial surgery [6].
Figure 1: Adjustable frame design.
Design and Basic Principle of Use
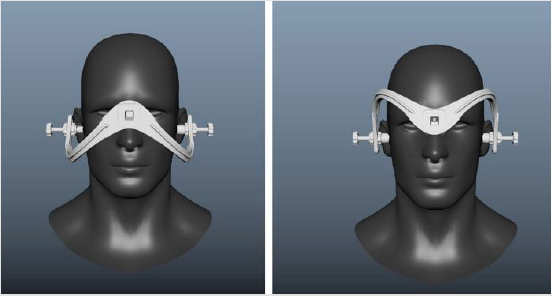
The design of the frame is designed in such a way that it rests on the fixed parts of the patient’s anatomy, namely the bridge of the nose and ear canals. All adjusting elements are near the ears. As a result of their adjustment, the frame is firmly adhered to the patient’s head due to the tension created between the support on the bridge of the nose and the ears. The original fitting position of the frame is designed neurosurgery, however it can be placed upside down in order to open access to the face for maxillofacial surgery (Figure 2). The frame also contains radiopaque markers, which can be used to compare the position of the frame relative to the CT scan and thus calculate the exact position and orientation of the hologram relative to the marker when using mixed reality glasses. The marker itself is inserted into a special slot in the frame, which allows you to set markers of various configurations depending on the surgical access and the position of the patient during surgery.
Figure 2: Two different fitting positions of the frame. For neurosurgery (left) and maxillofacial surgery(right).
Iterative Design Approach
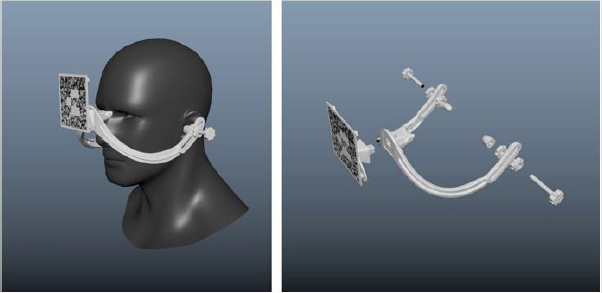
At the moment, the design of the frame has undergone 2 major development iterations. On each of them, various design changes were made to improve the ergonomics and quality of positioning of the holograms (Figure 3). The first version used plastic adjusting clips with metal rods. Despite the small length and size of the threads, they gave very strong interference in CT scans; as a result, the retainers were replaced with polyamide screws with nuts from the same material. In the second version, in addition to screws, polyamide plugs were made, which were put on over the screws and increased convenience in the process of adjusting the position of this frame. Also, the frame was reinforced with stiffening ribs to reduce possible deformation as a result of tightening the screws in the ears. In addition, the design of the installation of radiopaque markers has been revised. Now they are represented by small 2×2 mm set screws. This made it possible to significantly improve the quality of calibration and the positioning accuracy of the holograms. The result of using the frame during surgery with mixed reality glasses can be seen on the Figure 4.
Figure 3: Two versions of the frame. Old design (left) and new design (right).
Figure 4: Doctor wearing Hololens 2 glasses during the procedure (left) and picture from first point of view through glasses (right).
Conclusion
The adjustable frame allows surgeons to perform multiple surgeries using the same rig without creating custom system for each procedure. The latest version of the design is not final and requires some improvements. In particular, it is planned to revise the regulation mechanism to increase compactness in order to fit portable dental CT scans. We are also considering an option in which has an additional emphasis on the forehead to increase the rigidity of fixation.
From Traditional Braiding Methods to Additive Manufacturing for Fabricating Mckibben Artificial Muscles
Introduction
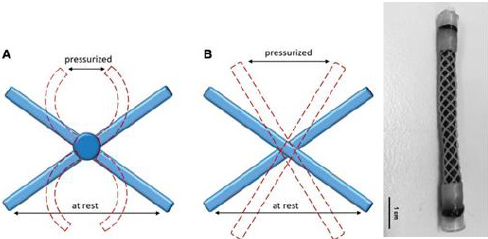
Mckibben artificial muscles [1-5] are of interest because of their practical engineering performances such as large contraction strains, high blocked forces and short response time. Since these performances are comparable to those of biological muscles, the demand for employing these muscles for robotic tools and medical devices is high. Mckibben artificial muscles are simply made of three essential parts: an inner elastomeric bladder, a braided sleeve and the fluid supply system [6]. The inner elastomeric bladder is surrounded by a braided sleeve which is connected to the fluid supply system. To activate the muscle, pressurized fluid is normally injected into the one end sealed inner bladder, once the inner bladder is fully pressurized, the volume of the inner bladder increases, and it produces force in radius direction against the braided sleeve. The braided sleeve subsequently transforms the generated radius force into the length direction along the braid axis [4]. The muscle, therefore, generates a length change or tensile blocked force depending on the experimental conditions. The magnitude of the generated force and length change significantly rely on the topology and mechanical properties of the braided sleeve. Previous literature described that the generated tensile blocked force normally decreases remarkably with increasing the initial angle of the braided sleeve up to the critical angle of 54.44 for a fixed input pressure. The amount of contraction strain also depends on the initial angle of the braided sleeve and for ideal systems is independent of internal pressure [3,7]. The amount of contraction strain usually declines with increasing initial braid angle and reaches zero contraction strain at the critical angle. Given the importance of the braided sleeve design to the performance of McKibben artificial muscles, here we review the trend of leading methods for manufacturing braided sleeves used in McKibben muscles and also suggest some design strategies for the future manufacturing.
Traditional Braided Sleeves
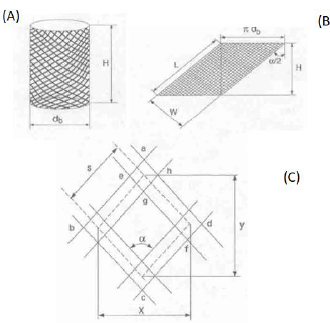
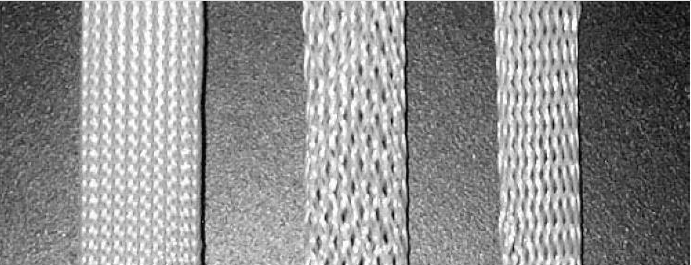
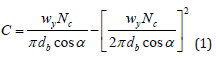
A braided sleeve is basically manufactured with several yarns interwoven with each other and fabricated around a mandrel [8,9]. There are important geometric variables that affect the final mechanical performance of the braided sleeve with an assumption that the braid is made of flat strip yarn. These variables include the braid angle, α, helical length. L, of one pitch of yarn, mandrel or braid diameter, db, yarn width, wy, and cover factor, C as shown in Figure 1. The cover actor is an essential property of the braid and is defined as the ratio of area occupied by yarn within a periodic pore unit to the total area of the pore unit, as shown in Figure 1. As derived by Zhang et al. [8], the cover factor is described by equation (1) and is a function of braid diameter, initial braid angle, yarn width, and the number of threads, Nc. Braided sleeves with the high cover factors are normally required in manufacturing McKibben artificial muscles due to the working conditions at high pressures. When fewer fibers are used in manufacturing of the braided sleeve this results in wider gaps between the fibers and consequently may result in muscle rupturing due to the internal bladder passing through the gaps at high pressures. Figure 2 illustrates the three different types of the braided sleeve with different cover factors.
Figure 1: Braided sleeve geometry (A) braided tube (B) Braid geometry of a helically slit tube of one pitch length (C) Unit-cell geometry used to determine cover factor; x and y are unit-cell height and width, respectively[8].
Figure 2: Three different types of braided sleeves designed with higher to less cover factor [9].
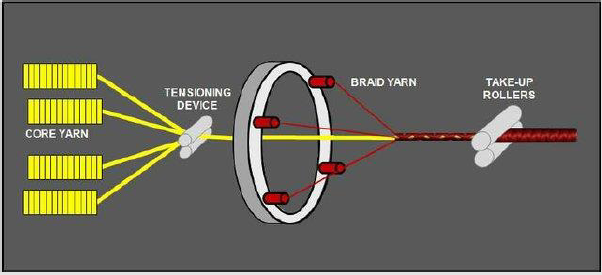
The traditionally two-dimensional made braided sleeves used in manufacturing conventional McKibben artificial muscles are sourced commercially and manufactured with industrial braiding machines [10]. As shown in Figure 3, the braiding machine assembles multiple individual fibers by using several rotary spools to produce a cylindrical hollow braided sleeve.
Figure 3: Typical set-up for a biaxial braid with core yarn.
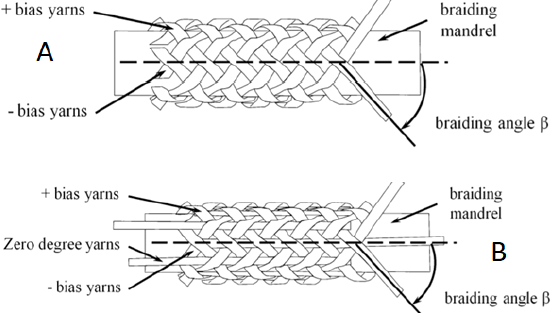
Two dimensional-braided sleeves are structurally divided into three categories. Biaxial-braided sleeve is the most widely used braid structure in industrial textiles, especially in the composite industry. A single yarn set are (generally orientated at an angle in the + θ and – θ directions) interlacing with each other around mandrel to form the braided fabric surface as shown schematically in Figure 2A. This structure, however, suffers from poor impact resistance because of crimp and low delamination strength due to the lack of binder fibers in the thickness. Triaxial-braided fabric normally consists of three sets of yarns and intertwine with each other around the axial yarns at about 45° angle as shown in Figure 2B. In this method, braiding very dense structure patterns is less feasible compared to biaxial-braided fabrics. Although the axial directional properties are improved in this method (Figure 4). Currently, various types of braids, made of nylon, polyester and carbon fibers are commercially available providing different advantages and disadvantages to the performance of the McKibben muscles.
Lab-scale braiding machines, however, suffer from several essential disadvantages. Firstly, the braiding machines are limited in generating only a narrow range of braid angles, where the braiding angle α is the angle between the longitudinal direction of the braided sleeve and the fibers that are helically wrapped to form the braid. Commercially available braids have a limited selection of braid angles typically in the range of 15o- 35o. Secondly, producing a consistent cover factor is limited due to the friction between fibers. The cover factor is defined as the ratio of area occupied by fibers to the total braid surface area and is a function of braid diameter, initial braid angle, fiber width, and the number of threads. Again, the variation in cover factor from commercially available braids is limited and most have a cover factor in excess of 85%. Third, long fiber lengths are needed to operate braiding machines, which limit the introduction of novel fiber materials for research-scale production especially when only short lengths of experimental fibers are available.
Smart Birded Sleeves for Contraction Sensing
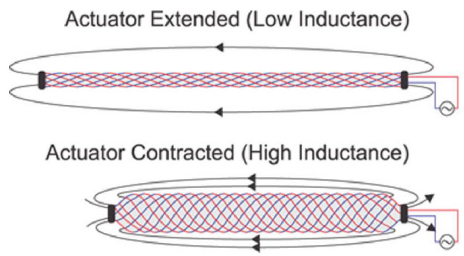
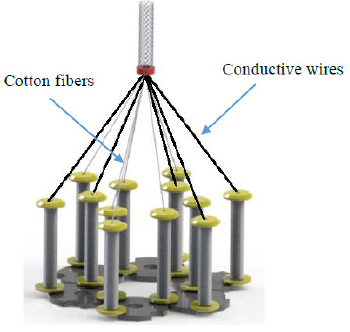
Using traditional or prismatic joints is generally required to precisely measure the motion of Mckibben muscles. Particularly in robotic applications using the Mckibben muscle with sensors is a normal practice to allow for closed-loop control of the generated motions. Research [11,12] has shown that measuring the motion is possible by using smart braided sleeves in manufacturing the McKibben muscles. The traditional braided sleeves of a pneumatic artificial muscle (PAM or McKibben muscle) were interlacing with conductive, insulated wires. Ultra-flexible wires with soft copper stranding and PVC insulations were utilized as conductive wires. This particular braid was assembled with 16 helices equally woven to the right and left directions. These wires acted as a solenoid-like circuit with an inductance that more than doubles over the PAM contraction. Following the actuator contraction, the direction of conductive fibers become more aligned therefore the inductance of the circuit increases. Figure 5 shows the schematic view of the smart braided sleeves used in manufacturing McKibben muscles.
Figure 4: Two dimensional-braided sleeves (A) Biaxial (B) Triaxial.
Figure 5: The smart braid sensors at (A) extended and (B) contracted motion[11].
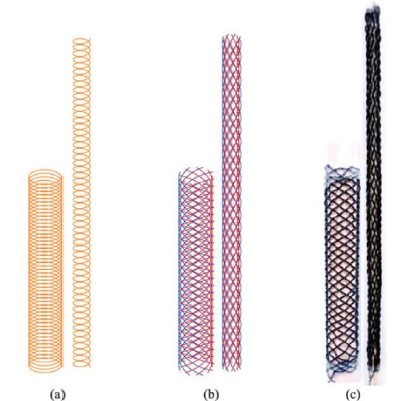
In this study, three structurally different braids were assembled to match the mathematical models. As shown in Figure 6 the authors modeled the inductance of the smart braid with either a simple long solenoid
a) or by using the Neumann formula on 16 helices
b) that are radially distributed about the actuator and electrically connected in series. The results then were compared with measurements from a smart braid stretched over dowels of different diameter
c) 4. Electrically conductive braided sleeves Conductive braided sleeves were used to manufactured miniature and bladderless McKibben artificial muscles [5]. As shown in Figure 7 the conductive braids were assembled with scale lab braiding machine using cotton fibers and steel wire in a parallel direction.
The resistivity of the conductive braid was reported to be ∼18 Ω. As mentioned earlier the cover factor of the braided sleeve is an important parameter and should be closely monitored the braid manufacturing process. In this study, the conductive braided sleeve was manufactured with different cover factors by independently decreasing the diameter of the braid yarn. The ultimate aim of this study was to keep the thermo-sensitive material (paraffin) inside the braided sleeve without using any inner bladder. The thermossensitive material was used to generate a sufficient pressure inside the conductive braided sleeve similar to air in pneumatic version. Adequate conductivity was required to electrically stimulate the thermos-sensitive material and consequently activate the muscle.
To manufacture the bladderless McKibben muscles, researches used the principles of breakthrough pressure [13]. The pressure needed to push a non-wetting liquid through the pores of a membrane is called the breakthrough pressure, P, and is related to the membrane and liquid properties by the following Young–Laplace equation where, r, is radius of the pores, σ and θ are the surface tension of the liquid and the contact angle, respectively. As shown in equation 2, for any pair of materials, the breakthrough pressure increase as the size of pores decreases. Pore sizes in a braid can be expressed in terms of the cover factor, C, which was defined earlier
Figure 6: Three structurally different types of smart braided sleeves[11].
Figure 7: The schematic illustration of the lab-scale braiding machine[5].
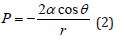
The muscle made of the conductive braided sleeve with the cover factor and average pore size of 0.73 and 0.27 mm was able to prevent the wax exuding through the pores during the actuation tests for many cycles. Figure 8 illustrates the microscopy images of two conductive braided sleeves with different cover factors packed with a thermos-sensitive material.
Figure 8: Microscopy images of conductive braided sleeves with high (A) and low (B) cover factors packed with thermossensitive materials (C and D). (E) the Entire conductive bladderless McKibben muscle[5].
Three-Dimensional Printed Braided Sleeve
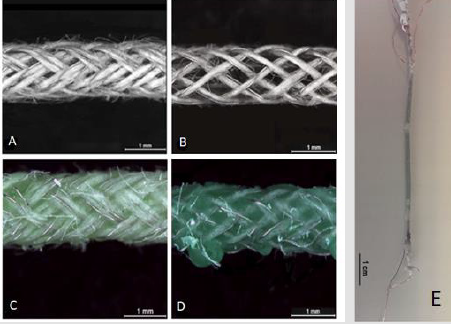
An alternative method was investigated to manufacture braided sleeves using a three-dimensional (3D) printing technique [14]. 3D printing method was chosen to achieve more versatility in controlling the geometry and the structure of the braids. This unique 3D printing technique is simple, fast, and accurate that can be easily modified to fabricate tools for small robotic systems where custom manufacturing is required. The braided sleeves in this study were made by employing an extrusion style threedimensional (3D) printing machine using a similar technique to that introduced recently. Each individual printed line was made of polycaprolactone (PCL) material and was precisely printed around a rotating cylindrical steel rod. An additional advantage of this method was the ability to incorporate the hydraulic end connectors directly into the braided sleeve structure. The end connectors are an integral part of the McKibben muscle system and achieving leak-free connection to the hydraulic fluid supply and robust mechanical connection to external loads is a challenge that can be uniquely addressed using 3D printing. As shown in Figure 9, the manufacturing process of 3D printed braids is a follow. The right to left printing direction was first performed as described above and then the entire mandrel with the printed helix was dip- coated in alginate solution and dried. The left to right printing direction was performed to form the second helical fiber on top of the dry alginate film. The mandrel was then immersed in the water bath to dissolve the alginate interlayer. By removing the alginate films from between the PCL helices the double-helix braids with disconnected fiber crossover points were successfully produced. The braided sleeves were then removed from the steel mandrel. The cover factor was constant at 0.47.
As shown in Figure 10C, the printed braids have integrated end connectors to simplify the assembly of the completed McKibben muscle. The effect of fiber connection in crossover points has been investigated. In this particular study, it has been found that the braided sleeves with connected fibers were unable to produce any actuation due to mechanical failure of the fibers (Figure 10A & 10B). Future directions in the future, it would be worthwhile to three-dimensionally print the braided sleeve using conductive materials. It would be then feasible to manufacture braided sleeves which contain conductive and non-conductive helices similar to those explained in sections 3 and 4 and pave the way for entirely printing the braided sleeves for in situ strain sensing applications. This task can be done via using conductive polymer composites with adequate viscosity for 3D printing applications.
Figure 9: (A) Photograph of printing set for manufacturing polymeric braided sleeve (B) Schematic illustration of the manufacturing process of 3D printed braids. All the manufacturing steps shown in the figure have been conducted around a mandrel[14].
Figure 10: Illustration of the deformed shape of one junction point unit (A) connected junction point before (blue ribbons) and after (red dotted lines) pressurization (B) disconnected junction point before (blue ribbons) and after (red dotted lines) pressurization (C) The entire McKibben muscles manufactured with 3D printed sleeve[14].
Analytical Platforms for Medical Diagnosis: A Study on the Performance and Recent Trends on Aptamer and Antibody Based Biosensors
Introduction
Advances in the field of molecular biology and chemistry have driven the studies in biosensing to an important and necessary level. The increasing attention of the population to healthcare summed to the alterations in their alimentary and social habits significantly changed the needs for personal health. Miotto, et al. [1] mentioned that the current context of healthcare demands to “ensure that the right treatment is delivered to the right patient at the right time”. In this scenario, the study of biosensors has provided sufficient tools, especially in the last decade, to advise the science of sensitive, rapid and accurate medical diagnostics. Clark and Lyons [2] were the pioneer in the field with the development of an enzymatic biosensor for detection of glucose. Their technology based on the oxidation of glucose by the enzyme glucose oxidase produced gluconic acid, hydrogen peroxide and electrons. This technology inspired unlimited researches up to nowadays and the more known commercial devices are still based on biosensing of glucose (being the first commercially available biosensor for glucose fabricated by the company Yellow Spring Instruments) [3].
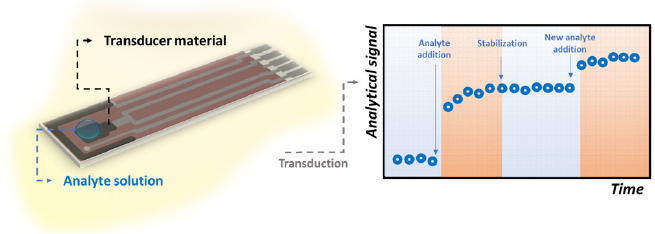
Once biological molecules are irreplaceable agents in living beings to make humans and animals to perfectly function, not surprisingly, scientists and research companies devote maximum efforts to mimic the biochemical reactions that naturally occur in the nature. This is the basis of a biosensor. A biological element of recognition is attached to the surface of an electrode material to detect a target molecule by means of their specific sites. Changings in chemical and/or physical properties of the transducer system are thus monitored and associated to the presence or to the concentration of the molecule of interest. Regardless the numerous possibilities of substrate materials, transduction modes and kind of molecules of interest, possibly the study of bioreceptors is represents the golden effort to achieve the two most important characteristics of a tool for diagnosis: sensitivity and selectivity. In light of this context, this work proposes a critical review of the literature on biosensing technologies for medical diagnosis with respect to two of the most important bioreceptors employed in highperformance sensors: antibodies and aptamers. A discussion on the global features of biosensors, their importance and application in medical diagnoses, key aspects of antibodies and aptamers to be employed as bioreceptors are provided herein. This knowledge is illustrated with the most recent trends in current works available in the specialized literature in order to contribute to the field of biosensors and clinical bioassays.
Biosensors and Units of Biorecognition
Sensors are part of our daily lives, inserted in the most diverse equipment’s with the most different functionalities. In general, a sensor is a device that transforms a certain physical or chemical property into an analytically measurable signal. In this way we can classify sensors where the variation of a biochemical property generates any signal, these devices we call biosensors, which can be defined according to IUPAC as being “device that uses specific biochemical reactions mediated by isolated enzymes, immune systems, tissues, organelles or whole cells to detect chemical compounds usually by electrical, thermal or optical signals” [4] A biosensor consists of two parts, one formed by the biological recognition element (receiver) and the other by the transducer, which can be electrochemical, optical, thermal, piezoelectric, capacitive and field effect. We can classify them, by the different methods of transduction, as well as according to the element’s receptor. Here, we will classify them only this. Bioreceptors can be selective or not, but recognition element plays a crucial role in the overall biosensor performance and selectivity toward a particular analyte [5]. Temperature, pH, contaminants, ionic strength, type of solution (buffer solution, body fluids, water) are factors that determine the performance of the biosensors [6,7].
Aptamers / Aptasensors
Aptamers are short and single-stranded nucleic acids (DNA or RNA) with capacity to bind to target molecules with high affinity and specificity [8]. First introduced in 1990, the process of selecting an aptamer is called Systematic Evolution of Ligands by Exponential enrichment (SELEX), from a large oligonucleotide library [9,10]. Aptamers can be selected for a variety of targets, including small molecules, proteins, nucleic acids, microorganisms, cells, tissues, metal ions and chemical compounds [11-13]. With the advantages of small size, high binding affinity, good stability and easy synthesis, aptamers show potential for various applications, such as targeted therapy, detection and clinical diagnoses [14-17]. After selection and characterization, aptamers can be customized for developing sensors [18]. A large variety of aptamer-based biosensors (aptasensors) with various detection strategies have been developed and reported in the literature [19]. In comparison to antibodies, aptamers are smaller units containing oligonucleotides with sizes over 30 oligos [20]. They are similar to monoclonal antibodies in terms of binding affinities, being called synthetic antibodies [21] in addition to other advantages, such as chemical stability and regeneration of its threedimensional structure even after several cycles of denaturation/ renaturation [22]. Its small size allows a greater density of immobilized molecules. They are chemically synthesized, which allows the flexibility of the conformation of their two-dimensional structure, so it can be built for the detection of any antigen, from small molecules, heavy metals, protein, enzymes, microorganisms and cells, with the possibility of adjusting the sensitivity and selectivity [23-28].
Antibodies / Immunosensors
Antibodies (Abs) are proteins that can be employed as valuable tools in laboratory and clinics [29]. Antibodies include those secreted by a single clone of B lymphocytes, termed monoclonal antibodies (mAbs), and those produced by a mixture of various B lymphocyte clones, the polyclonal antibodies (pAbs) [30-32]. In 1975, Kohler and Milstein developed a system for the production of monoclonal antibodies. Abs demonstrate high affinity and specificity to target molecules and have been frequently selected for a wide variety of applications including immunodiagnoses, biomarker detection, immunological research and vaccine quality control [33-35]. Abs can be used to develop a variety of sensors (immunosensors) upon the formation of an antibody-antigen complex [36]. Immunosensors are based on antigen-antibody affinity, where an immunochemical reaction forms a very stable complex. Every protein has an isoelectric point (point where the global electrical charge is equal to zero) that varies according to the composition of the amino acids, thus determining the magnitude and polarity of that point at a specific pH [37]. One can assume that any protein (Ag), with charge Ch1, and its antibody pair with charge Ch2, the reaction of that system (AgAb) results in a global charge Ch3 which can be described by the following equation:
where K is the binding constant for this complex. This change in electrical charges can ideally be detected, depending on the antigen concentration and the transduction technique used. The ambivalence of this system still allows the use of a biosensor for the detection of an antigen, regarding the possibility of immobilizing an antigen and the antibody becomes the analyte. Abs possess a “Y” shaped structure consisting of two heavy and two light polypeptidic chains bound by S-S bonds with approximately 150 kDa and dimensions of 14 nm x 10 nm x 4 nm [38,39]. The base of this “Y” structure is called fragment crystallizable region (Fc) and is composed by the heavy chains. On the other two extremities, there are the antigen-binding sites, or epitopes, comprising the fragment antigen binding (Fab). The Fab branches exhibit different characteristics (such as the chemical composition, the physical structure and the isoelectric point) as a natural consequence of their properties to bind different analytes [39,40]. At the same time it is advantageous to orientate the immobilization of Abs by the Fc portion because it keep frees the active specific sites (Fab) to bind analytes, the extra protocol to allow this orientation makes the fabrication of oriented antibodies-based sensors more laborious and frequently more expensive.
Key Features on the Performance of Biosensors
The most important characteristics of a biosensor are its selectivity, reproducibility, stability, sensitivity and linearity. The combination of these parameters has been the focus of many researchers specially in the last decade to develop high performance devices for diagnosing molecules of medical interests. These features can be defined as follows: a. Selectivity: represents the ability of a sensor to present an analytical signal exclusively due to the recognition of the target analyte, not suffering the influence of interfering species at a significant level. Morales and Halpern [41] mention that selectivity is essential in the development of point-of-care biosensors. This is because the testing biological samples are typically very complex and can possess various interfering molecules capable to compete for the bioreceptor sites of the sensor; b. Limit of Detection (LOD): is the minimum amount of analyte able to generate an output signal distinguishable from the blank signal (analyte absence) [42]. Depending on the level of affinity between the biorecognition element and the analyte, the biosensor can achieve low LODs and meets a broader window of applications in the field of clinical diagnosis. This affinity is expressed in terms of the dissociation constant “KD” (reciprocal of the association constant “KA”), which relates the concentration of free and bound molecules in a solution to provide a sense of strength of these interactions. In this regard, the lower KD is, the higher is the affinity between the bioreceptor and the analyte and, consequently, the lowest concentrations can be detected by the biosensor. IUPAC recommends the use of the equation LOD = 3S/m to calculate LOD, where “S” corresponds to the standard deviation derived from the black measurements and “m” represents the slope of the calibration curve; c. Sensitivity: despite it is still very common to observe the misuse of this term to designate the LOD, the sensitivity actually refers to the variation of the analytical signal due to the variation of the target analyte. In other words, it is calculated as the slope of the calibration curve and has the unit of the transduction signal (e.g. Ampères, Ohms, Volts, degrees, Celsius degrees, Hertz, etc) divided by the unit of concentration [43]. Briefly, the higher is the sensitivity, the higher is the response of a biosensor when it binds an analyte; d. Stability: capability of keeping the analytical signal robust enough to not suffer the influence of extrinsic agents, such as environmental disturbances, loss of bioreceptors’ affinity to the target, molecules degradation over time, etc [38]; e. Linearity: corresponds to the obeyance of the calibration curve to a mathematical expression. Once the linearity is set known, the concentration of the molecule of interest in a certain medium can be predicted and this is the working principle of quantitative accurate biosensors; f. Reproducibility: can be defined as the ability to provide similar responses under similar conditions of detection. In addition to those basic analytical properties, some authors also defend the evaluation of the linear range of detection and the response time to validate the performance of a biosensor. The former represents the concentration range of the analyte at which the sensor generates linear output signals, which is important to define whether the working range meets the requirement for a certain application besides helping to calculate the LOD and the sensitivity. The latter is an important reference mainly in medical applications. The response time of a sensor is the time required by the device to generate the analytical output signal as a consequence of the recognition of the target molecule. It is also frequent in the literature to find this definition as the time required to obtain 95% of the data resulting from the detection [38]. In the context of clinical diagnoses, fast responses of biosensors allow doctors to manage the diseases at early stages, avoiding the spreading of infections and the worsening of the clinical picture of patients. Within the scenario of the ongoing pandemic of coronavirus disease (COVID-19) for instance, authors defend that the importance of a quick diagnosis lies on fact that SARS-CoV-2 has exhibited higher contagiousness and infection rate if compared to other coronaviruses infections [44]. Furthermore, early diagnosis contributes to fast decisions on medical treatments and quarantine strategies to slow down the spread of the transmission rate.
Traditional Analytical Techniques for Diseases Diagnosis
Diagnosis, detection and prognosis techniques have been studied for several years and many methods for fault detection and diagnosis have been developed [45]. Molecular diagnostics assays use in vitro biological techniques for detection. Polymerase chain reaction (PCR) and quantitative PCR are performed to detect and amplify a genetic material (DNA or RNA) from a specific organism, for instance, a virus [46,47]. The advantages of PCR include the high sensitivity, quick performance and the ability to detect lesscommon organisms. On the other hand, its disadvantages include the supply costs, machinery fees and training expenses [48,49]. At present, PCR assay is regarded worldwide to as the most accurate and reliable test to detect active COVID-19 infections [50,51]. Immunoassays, such as enzyme-linked immunoassays (ELISA) and point-of-care (POC) techniques can be used for detection of antigens or specific antibodies [52]. Currently, immunoassays play a prominent role in the analysis of many clinical laboratory analytes such as proteins [53]. A broad variety of tests detecting specific SARS-CoV-2 antigens and IgA, IgM and/or IgG antibodies were developed [54,55]. Although the classic immunoassays can provide very sensitive and accurate diagnoses, many of them possess some important limitations: high cost, they are time consuming, demand sophisticated equipment and high skilled staff [56].
Recent Trends in Biosensors for Detection of Analytes of Medical Interest
It is worthy notable that the field of biosensing through the design of assays to detect molecules of medical interest has attracted huge attention specially in the last year with the outbreak of COVID-19 around the world. Not exclusively due to the current pandemic, though, numerous researches have been devoted to some special improvements in the analytical sciences in order to ameliorate the performance of the already known technologies. Within the recent literature in this domain, one can easily recognize some trends in the newest biosensors of medical interest: the fabrication of point-of-care devices, the label-free detection, realtime measurements and the advance of electrochemical transducer mechanisms. Under all these trends, the use of antibodies and aptamers as bioreceptor agents seem to properly match the needs and expectations of current diagnoses.
Point-of-Care Biosensors
Point-of-care diagnoses collect several unquestionable advantages over traditional laboratory setups. Not surprisingly, the golden characteristic refers to the possibility of running the test wherever the patient is, on-demand and onsite [57]. It makes the sensors amenable for bedside monitoring, analysis in pharmacies or even by the user himself. Consequently, this kind of device tends to gain increasing visibility in the market. Eguilaz et al. [58] highlight that these devices are even more relevant in resourcelimited regions where the access to medical centers is difficult to the majority of the population. Nonetheless, point-of-care devices combine other interesting characteristics, such as (generally) the rapid detection, fewer steps for data/results acquisition, friendly interface, easy transport due to the reduced dimensions and light weight and demand for small sample volumes [57,59]. Concerning this last characteristic, though, there is a strategic point to be taken in account. Depending on the application, the target molecule is present at very low concentrations in the sample of analysis. Thus, a small volume for testing can contain insufficient quantity of analyte in such a manner that the biosensor would not be able to detect it [58]. In this regard, antibody- and aptamer-based biosensors are widely employed to overcome this drawback because of their high sensitivity resultant from the high affinity and selectivity of these molecules. Searching for overcoming the limitations of conventional diagnoses, Ferreira, et al. [60] worked on the development of an aptasensor for detection of breast cancer in undiluted human serum. This kind of cancer is unfortunately responsible for thousands of deaths annually. According to the authors, the diagnosis is mostly based on the detection of tumor markers present in blood or other corporal fluids at concentrations from 15 ng/mL to 75 ng/ mL (over the regular healthy range of 2- 15 ng/mL). Ferreira, et al. [60] exploited two functionalization methods to attach Human Epidermal Growth Factor Receptor 2 (HER2) aptamers to the surface of screen-printed electrodes (SPEs). These devices are widely recognized in the literature to serve as useful substrates for designing portable electrochemical sensors, mainly because of their good conductivity, electrical stability in typical electrolytes and reduced dimensions [61]. In a list of 110 recent articles reviewed by Ranjan, et al. [62] on point-of-care biosensors for breast cancer diagnosis, 23% were described the use of antibodies and 5% the use of aptamers as bioreceptors, which symbolically represents the large employment of these biomolecules in biosensors of medical interests. In this same work, other elements of recognition were described, e.g. enzymes, inorganic probes, DNA, proteins, receptorligand complexes and molecular imprinting polymers (MIP).
Label-Free Detection
The topic of label-free sensing in the context of bioassays generally converges to two points: the advantage of reducing the consumption of reagents and the consequent lower number of fabrication steps of biosensors in comparison to golden standard techniques (e.g. ELISA and PCR). Label-free sensing mechanisms consist in the direct detection of target molecules by the bioreceptor attached to the transducer substrates, i.g., without the needs for fluorescent chemicals, enzymes and so on [63]. Thus, since the label-free biosensors do not demand extra labels to run the detection, this characteristic nicely meets the requirement of point-of-care biosensors for the simplest incubation protocols and allows the use of unprepared samples at working environments. Among other interesting features, Andryukov, et al. [63] point out the following advantages over label-based similar analytical assays: simpler pattern of detection, lower response time, lower cost of analysis, opportunity to detect small molecules and possibility of multiplexing. Zhang and Liu [64] mentioned that the success of using DNA in label-free devices based on optical biosensors has inspired the same approach in the aptamer field. However, the authors explain that aptamers can fold DNA and hide its bases, providing slow kinetics of target binding, especially when the target is a small molecule. Therefore and since aptamers possess lower affinity to small molecules (KD around low micromolar units) than DNA (KD approximately in picomolar or low nanomolar), the detection of aptasensors tends to be more challenging, justifying the efforts on label-free sensing to enhance its analytical response. On the other hand, numerous works can be easily found in the field of labelfree immunosensors for detection of analytes for highly sensitive diagnoses [65-68].
Real-Time Measurements
The key point of real-time biosensing is the necessity of the sensor to rapidly recognize the target molecule. If so, the output signal will be registered by the transducer source in short time intervals and a variation in its magnitude could be notable as illustrated in Figure 1. This need makes some important well recognized techniques such as ELISA and Luminex assay to fail as real-time methods for in vivo applications, since they require laborious and pre-defined longtime steps [69]. Cohen et al. [69] highlight that ELISA, for instance, depends on diffusion processes concerning the interaction between antibodies and antigens in a non-mixed solution, which is associated to a low binding equilibrium constant and makes the response time longer. Typically, this technique requires approximately 3 hours to be performed [70,71]. In this regard, Shengnan, et al. [72] reported the construction of an aptasensor for the real-time detection of vascular endothelial growth factor, one of the most important cytokines present in cancer patients (with average concentration of 434 pg/mL). The authors achieved a LOD of 0.1 pg/mL within a linear detection window from 2 pg/mL to 500 pg/mL. The mechanism of recognition was based on a Chronoamperometry test at the positive redox peak potential of ferrocene-labeled aptamer for 5,000 seconds.
Figure 1: Illustrative scheme referring to the fluctuations of the analytical signal of a biosensor as a consequence of rapid interaction between its bioreceptors and the target molecules.
Also taking advantages of the specificity of aptamers as bioreceptors, Soleimani, et al. [73] manufactured an aptasensor assisted by a computerized monitoring system to detect prostate specific antigen (PSA). To characterize their aptasensor and to construct the calibration curve towards PSA, the authors carried out Electrochemical Impedance Spectroscopy (EIS) and Cyclic Voltammetry (CV). Due to the steric hindrance of the analyte, the electrochemical signal of the transducer substrate increases over the time when aptamers bind the molecules of PSA. As a result, the findings showed that this kind of setup presented sensitive and rapid response fitting the real application aimed to the diagnosis of patients with prostate cancer.
Electrochemical Transducing
As per the examples of the previous sections, electrochemical mechanisms have progressively illustrated the transduction modes of many biosensors for medical applications. From 2017 to 2019, for example, these devices represented 45% of the published articles in the specialized literature of biosensors [74]. The reason is the collaboration that electrochemical reactions provide to enhance sensitivity, accuracy and response time. Briefly, in this kind of biosensor the electrical properties of biological molecules and their interaction with electro active surfaces are exploited for assessing the changes in current, potential, charge, impedance, conductivity, etc. Complementarily, depending even on the dimensions of target molecules, the distance from the electrode surface and needs for redox probes, the specific electrochemical technique can be chosen to achieve highest analytical performance [75]. The detection system consists of three (or two) electrodes, of which one is the sensing surface (named working electrode), one is the counter-electrode and the other is a reference. These electrodes must be immersed in a conductivity solution to allow redox processes to occur and charges transfer. When the detection of the analyte happens and the electrical properties of the surface is altered, an electronic system acts to amplify and manage the resultant data. Traditionally, this last step is performed by a potentiostat interfaced with a software for control of the required parameters. Mishra, et al. [75] pointed out details on the electrochemical aptasensors referring to design strategies and functionalization. The researchers reported that aptamers have been mostly immobilized to gold and carbon-based electrodes via chemical cross-linking with particular attention to ensure biochemical stability, surface coverture and optimal binding affinity. Most common electrochemical techniques used for fabrication of biosensors are CV [76,77], EIS [78-80], potentiometry [81,82] and amperometry [83,84]. When real-time performance is required, time-based assays (such as chronoamperometry, chronocoulometry and chronopotentiometry) well fits medical applications.
Efficiency of Immunosensors and Aptasensors
Cesewski and Johnson [85] point out that, in some cases, the high sensitivity of immunoassays are not enough to detect certain pathogens in the organism. In such circumstances, although these infectious agents are present, they do not generate enough available Abs in the blood, so the concentration of the Abs in the blood are lower than the LOD of the technique, failing the detection. According to the authors, this is a typical situation in which the employment of DNA-based systems is more useful. The biosensors consisting of nucleic acids, for instance, are usually able to recognize low concentrations of pathogens by themselves or through the indirect expression of toxins they release in the infected organism (e.g. toxins, other nucleic acids and raised cells. In this regard, Table 1 contains a list of recent researches in the literature of biosensors for medical applications using antibodies and aptamers as bioreceptors. It is worthy notable that these biomolecules facilitate the biosensing of analytes at concentrations as low as some femtograms per milliliter [86-90].
Table 1: Recent developments (from the last two years) in the field of aptasensors and immunosensor for assisting clinical diagnosis.
Note: *NPs = Nanoparticles
Regardless the obvious different protocols used to attach antibodies and aptamers to the different transducer substrates, it is worthy notable that the sensitivity of these devices are really high. Besides, in this recent literature is not rare to observe a trend in using label-free molecules to optimize the fabrication step and to allow accessible in-situ measurements [91-98]. Nonetheless, it is also evident that many authors have employed electrochemical techniques to ensure accuracy and high performance of biosensors, corroboration the previous discussion brought to this minireview in the section “Recent trends in biosensors for detection of analytes of medical interest”.
Conclusion
With the increasing humans needs for accurate, fast and friendly methods for health control, biosensors for medical applications have undergone important changes in the last decade. The immobilization of antibodies and aptamers on transducer substrates for high performance detection has been an exhaustive strategy for the production of biosensors, especially due to the high sensitivity of these bioreceptors. Articles published in the recent literature exhibit LODs in the order of femtograms per milliliter. To this end, added to the intrinsic advantages of antibodies and aptamers, there is a notable trend to search for label-free devices, with less functionalization steps, lower times for the formation of bioreceptor-analyte complexes, under selective and sensitive sensing modes. Thus, much is seen about the use of electrochemical techniques such as CV, EIS and amperometry, although optical and piezoelectric transduction techniques are also present in the field of biosensors for various applications including the ones for medical diagnostics. It is believed that this specific application demands advanced technologies, especially to shorten the detection time, since early diagnoses are essential for the administration of first aids and precise medications that can enhance the chances of cure and survival of patients (especially those who have less access to health centers). The main challenges in the area still seem to be related to the commercial viability of these devices. Likewise, quite possibly, the prospect of advances in technology is likely to be based on the study of alternative materials and methods to make immunosensors and aptensensors increasingly simple and inexpensive.
Empathy and Telepathy: Functional Imaging Psychiatric and Philosophic Correlates
Introduction
What is the Telepathy?
Objective data indicates that a significant percent of general population experience the feeling described as they had undefined communications with other persons who are not in contact with them. They define this exceptional perception in various visual or auditory modalities which are correlated with an altered consciousness state. ‘’Myers defined telepathy is as “the transmission of feelings, perceptions, experience and thoughts from one person to another, without using any of the recognized sensory channels or physical interaction’’ [1,2].
Are Telepathic Experiences Normal in Psychiatry?
Interestingly such perceptions are usually associated with stressful life situations that is a challenging situation for a psychiatrist to distinguish it from a real psychopathological situation. To make a precise diagnosis, the major psychiatric diagnostic algorithm necessitates to exclude all other possible organic causes, such as oxidative stress and internal and external traumatic conditions that predispose to mood and neurodegenerative disorders [3-7]. In this respect it is important to evaluate the functional or pathological correlates of such experience before we diagnose it as a psychiatric disorder. As in many psychiatric disorders the duration of symptoms and disease since the degree of the impairment of daily functionality is an important parameter that help us to make the psychiatric diagnosis [8,9]. This mean for example just as the diagnosis of a major depressive disorder where the depressive symptoms may result from normal, uncomplicated, situations which can be viewed as a simple reaction to stressful situation instead of evidence of mental disorder [9]. Interestingly many persons with telepathic experience are categorized as normal in psychiatry.
A Possible Link between Empathy and Telepathy
Telepathic communications usually occur between persons who share an emotional link instead of a physical, biological or genetic background. For example, such experiences have been reported between close friends although it can be not the case among members of the same biological family. There are also some interesting cases reporting that even physical symptoms especially pain have been experienced by telepathic communications. This has been occurred between twins, parents, and their children as well as some few psychiatrists who have reported telepathic experience with their patients. The well-known Swiss psychologist, Carl Gustav Jung also reported experiencing severe headache when his patient shot himself in the head [10]. All these above-mentioned data indicate that an emotional link rather than a physiological, biological or genetics play an important role in the communication of telepathic experience between emotionally linked persons. Regarding the background of emotional bound between person’s empathy has been reported as a significant indicator of their emotional dynamics that can be affected by various drugs [11]. Empathy is defined as the ability to sense other people’s emotions, and to imagine what someone else is thinking or feeling called also “Cognitive empathy” or “perspective taking”. If we look from this point of view, it can be hypothesized that there is a thin border between the empathic ability and telepathy [11]. Thus, it has been recently suggested that superior cognitive empathy is associated with special abilities, indicating that people with telepathy might be able to activate specific brain regions related to the empathy circuit. Studies have already shown that right hemispheric region of the brain plays an important role during the processes of both empathic and telepathic experience [1,12,13].
Non-Local Unconsciousness Theory and Real-Word Neural Correlates of Telepathy
In agreement with this, many studies in cognitive neuroscience indicate that the processing of symbolic and especially unconscious components are associated with the activity in the structures of the right hemisphere. This is especially important since both the telepathic experience and cognitive emphatic abilities are localized on the same hemispheric region suggesting that there might be a functional link between the activation of the unconscious part of the brain and these exceptional abilities [4]. Based on these data it can be assumed that activated specific brain regions might connect and collect the information from a common information network that is difficult to understand within the conventional time and space concept. This theory resembles us the theory of collective unconsciousness of Jung [10]. Jung’s collective unconscious theory is hypothesizing that human psyches are linked together via an unseen linkage that consists of basic shared perceptions, instincts, patterns of thinking, behavior and a pool of common knowledge which may function as a common information network enabling to connect and collect the information out of the time and space. Jung hypothesizes that each individual inherits a collective memory from past members of the species, that contributes to the collective memory and affects other members of the species in the future [10,14]. As opposed to the conservative functional neurobiology of the brain this window helps us to create a universal unconsciousness model including an enriched picture of causality. Despite these findings, Venkata Subramanian, et al. showed recently that successful telepathic session was associated with significant activation of the right limbic area in compared to the activated left frontal cortical region by the subject without telepathic ability [1,15] which is consistent with the multimodal role of fMRI. Moreover, other functional magnetic resonance imaging and magnetic field studies demonstrated that distant intentionality was related to the alterations of different brain functions in the isolated recipients which may be modulated with the artificial magnetic stimulation. Thus, there have been many studies suggesting the beneficial role of magnetic stimulation in various neuropsychiatric and neurodegenerative disorders characterized with empathy [8,9,16, 17].
Conclusion
Alternative paradigms including a universal and non-spatial nature of human consciousness could help us to understand the nature of telepathic experiences. Besides concrete rational findings where neurobiological and functional/metabolic correlations are still the only measurable macroscopic parameters in our real world, alternative consciousness models which seem out of space and time help us to expand the conservative consciousness model and understand the flexible cause-effect relationship in the human cognition.