Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
The Seroprevalence of SARS-CoV-2 Antibodies in Romania – First Prevalence Survey
Introduction
The infection with the new Coronavirus generated important socio-economic transformations, through social distancing measures, with profound economic implications, but also a lot of concern, due to evolutionary and clinical complications and lack of specific treatment. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) associated disease – 2019 (COVID-19) has spread globally, affecting in one year and half over 170 million people from more than 180 countries or regions, leading to a global pandemic with a fatality rate of 2.1% [1]. The laboratory diagnosis of suspected COVID-19 clinical / contact cases is based on the detection of SARS-CoV-2 viral genome by qRT-PCR assays. However, asymptomatic or mild COVID-19 infections remain undiagnosed, therefore the burden (incidence and spread) of SARS-CoV-2 infection can be underestimated, affecting the implementation and efficiency of infection control and prevention measures. Given this limitation, countries are seeking to assess the spread of the infection in the population through prevalence studies conducted on study groups which are representative for the general population [2,3].
The surveys conducted in the first half of the year 2020 in different countries or geographical regions on populations of different sizes revealed different seroprevalence rates, ranging from <0.1% to more than 20% and that it can increase over time during longitudinal follow-up. In Europe, the seroprevalence reported by different countries was in decreasing order Italy (11.0%) [4], Switzerland (weekly seroprevalence rate of 4.8% to 10.8% during five weeks) [5], France (between 3.8 and 10% in different regions) (2), Spain (4.6%) [6], Denmark (1.9%) [7], Greece (0.42%) [8]. In USA, a great variation of seroprevalence was reported for different geographical regions (1.0% – 31.5%) [9,10], while for Brazil the rate was 3.8% [11]. In South America, Chile reported a seroprevalence of 13,4 – 16% [12]. In Africa, Kenya reported a crude seroprevalence of 5,6% and a study done in Alzintan City of Libya presented a seroprevalence of 2,74% [13,14].
In Asia, the highest rates were reported for Pakistan (15.6- 37.7%) [15], Guilan province, Iran (22%) [16], in China different serological studies reported positivity rates ranging from 0.6% in Chengdu, Sichuan to 3.8% in Wuhan, Hubei [17], while the lowest rates were recorded in Malaysia (0.4 – 0.6%) [18] and South Korea (0.07%) [19]. Japan reported 3.3% seroprevalence in Kobe [20] and a cumulative case detection ratios (2.6 – 8.7%) at 3 prefecture-level seroprevalence (Tokyo, Osaka and Miyagi) [21]. All studies reported a higher seroprevalence rate in males, although the differences are not statistically significant [22]. Considering the large variation of seroprevalence among different populations, filling the gap with data from different geographical regions is needed in order to better evaluate the burden of COVID-19 pandemic. This study reports for the first time the results of a seroprevalence survey performed in the Romanian population, to estimate the degree of spread of SARSCoV- 2 infection and to substantiate the measures to respond to the COVID pandemic that will be adopted at the level of the Romanian health care system for the next period.
Material and Methods
In this study, people that presented themselves conjuncturally at selected laboratories have been invited to participate in the seroprevalence survey. The participating laboratories were selected from each of the 42 counties of Romania.
Study Design and Participants
A cross-sectional study was performed to assess the SARSCoV- 2 antibody seropositivity prevalence. The study used a nonprobability sampling method, known as convenience sampling. The sampling strategy had two steps: the selection of laboratories and the selection of persons. The inclusion criteria for the laboratories were the following: either public or private facilities, with high addressability (over 40000 samples per year) and serving ambulatory patients (non-hospitalized). Based on these criteria, each of the 42 County Public Health Directorates over the country selected between 3 and 5 laboratories to participate in the study (except Bucharest Public Health Directorate, which selected 9 laboratories). Inclusion and exclusion criteria for the enrolment of the study subjects were also defined. In order to be selected, people from all ages that presented themselves conjuncturally at the selected laboratories for check-ups were invited to participate in the study. They should not present signs of symptoms of respiratory infection or requested to be tested for Covid-19. The participants to the study were selected based on a sampling step, and only individuals who expressed their informed consent to participate in the study were enrolled.
If a person qualified in the sampling step did not agree to participate in the study, the next person was asked if willing to be enrolled. The data collection took place between July and October 2020. The participants had to sign an informed consent to be included in the study (for children the consent was signed by the parent/legal representative). The participants had also to provide their demographic information, that included age, gender, city of residence and personal pathologic history. The seroprevalence analysis involved residual serum obtained from these individuals. The size of the study sample was calculated using the EpiInfo 7 program, for obtaining regional and decadal age-group representation. The regional sample for a specific agegroup was proportionally allocated for the counties in the region, considering their total population for the corresponding age-group. The resident population of Romania from July 1, 2018, on decadal age groups was used, with an expected frequency of SARS-CoV-2 infection in Romania of 50% on each age group, an accuracy of 95% CI, error accepted 5 % and 5% losses accepted for each age group in the region.
Procedures
All the serum samples of the enrolled participants were analyzed by the National Institute of Public Health laboratory, using a chemiluminescent technology (CLIA) based assay to detect the anti-SARS CoV-2 antibodies of the IgG type. The samples were kept at temperatures between minus 12 and minus 20 degrees Celsius. Transportation of residual serum samples was done using refrigeration machines and, exceptionally, isothermal bags with ice packs. The quality criteria for the serum samples were the following: blood samples collected in biochemistry vacuums, without anticoagulant, with or without separating gel; samples with a serum volume of 0.5-1 ml for the age group 0-14 years and 1-2 ml in people over 14 years. The residual serum from people that were suspected of Covid-19 and those presenting jaundice, haemolysis or superinfection (with flakes or veil) were not considered.
Ethics Statement
The existing study protocol was reviewed and accepted by the Scientific Council of the National Institute of Public Health – Research Ethics Committee. The seroprevalence study was performed in full compliance with the principles of ethics and confidentiality of personal data. Written informed consent was obtained from all eligible for enrolment individuals, while all professionals involved in the collection, retrieval and storing of data have signed a confidentiality agreement.
Results
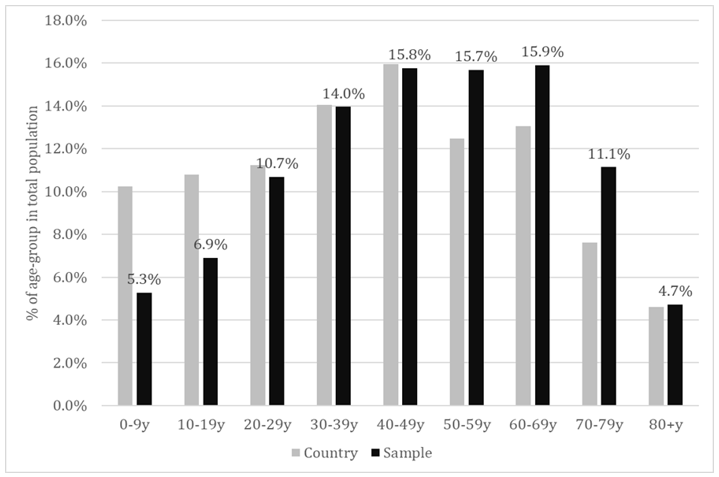
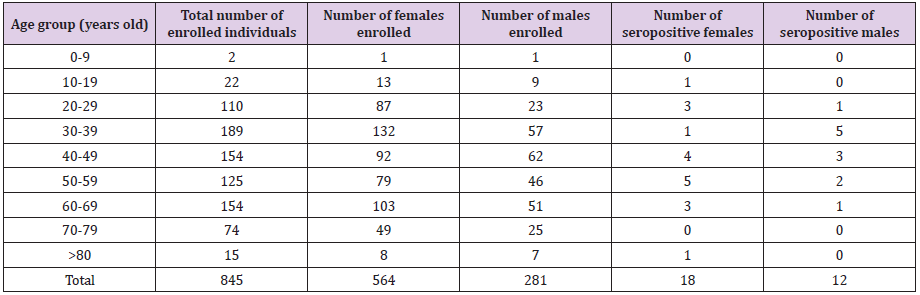
Of all the individuals that presented themselves at the selected laboratories across 8 regions of the country, 19738 agreed to participate in this study and 19597 provided a serum sample for which a CLIA result of anti-SARS-CoV-2 IgG specific antibodies was available. Males represented 36.2% of the total study population and this could be probably associated to the higher health-related concern of females in general, considering that the selection was conjunctural (people addressing themselves for different blood tests). The sample population had a mean age of 46.61±21.08 years and a median age of 48 years. The proportion of each decadal age-group is shown in Figure 1. As could be noticed, the young age-groups were seriously under-represented, meanwhile the agegroups 50-59y, 60-69y and 70-79 y were slightly over-represented (last-one in particular).
Figure 1: Proportion of the decadal age-groups in total population – sample versus country population.
Seroprevalence at National Level
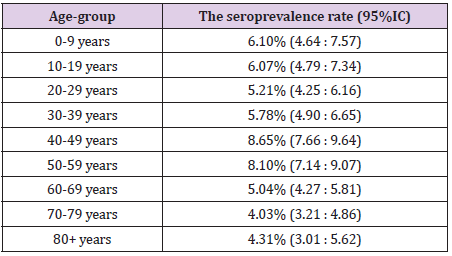
Overall, we found 1213 positive IgG samples in the study population, resulting in a seroprevalence rate of 6.19% (95%CI: 5.85:6.53). The seroprevalence rate by age-groups at national level is shown in Table 1. The level of protection was similar in children and young adults (slightly higher in children, but statistical significance was not met). The middle aged adults, especially the age-group 40-49 years showed a significantly higher level of protection. Population aged 60+ years seemed to be less protected compared to both adults and children. A statistically lower level of seroprevalence was revealed between each elderly age-group compared to middle-age adult population. A slight difference in seroprevalence was found compared to children and young adults, but this did not meet the statistical significance. We found also differences within the elderly groups. The seroprevalence seemed to be lower over the age of 70 years, compared to age-group 60 – 69, but, again, this difference did not meet the statistical significance.
Table 1: The seroprevalence rate by age-group.
Seroprevalence by Regions
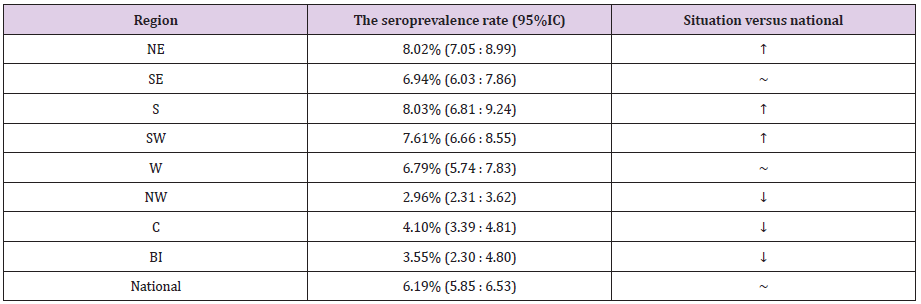
Romania is divided in eight region: North-East (NE), South- East (SE), South (S), South-West (SW), West (W), North-West (NW), Center (C) and Bucharest-Ilfov (BI) – the last-one including the capital city of Bucharest. By comparing the regions with the national rate, we found significantly higher prevalence in NE, S and SW, and significantly lower one in NW, C and BI (Table 2).
Table 2: The seroprevalence rate by regions.
Seroprevalence by Age-Groups – Regional Versus National Level
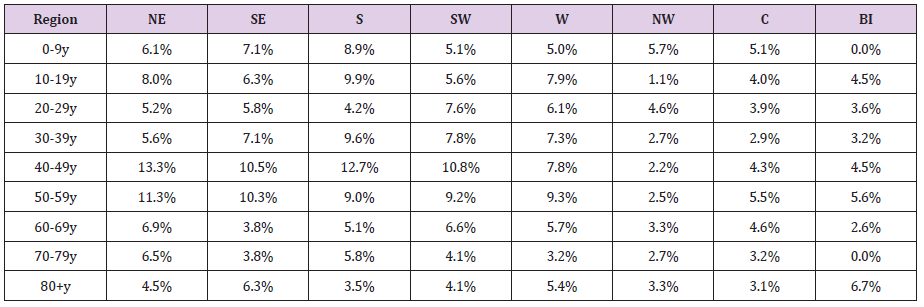
The seroprevalence by age-groups in the regions is shown in Table 3. Although the seroprevalence for each age group registered some variations among regions, significant differences compared to the national level were found only in limited cases. Thus, we found significantly lower seroprevalence rates compared to the national level in the regions NW (age-groups 10-19y and 30-59y) and Centre (age groups 30 – 39y and 40-49y). The only situation with a significantly higher level of protection was age-group 40-49y, in the NE region.
Table 3: Seroprevalence by age-groups in the regions.
Seroprevalence in the Capital Region (BI)
The enrolment rate in the Bucharest-Ilfov region was from far very poor (23% of planned). Table 4 provides details about the number and age of participants in Bucharest. Out of 845 participants, 30 tested positive for SARS-CoV-2-specific IgG antibodies, meaning a seroprevalence of 3.55% (2.30:4.80). A very limited number of cases was enrolled in the extreme age-groups (children and elderly population) and nonpositive case has been identified in age-groups 0-9y and 70-79y. The proportion of males was 33.3%, slightly lower compared to the national proportion (36.2%), but without statistical significance (p=0.081, Chi Square test). From the total positive cases, 18 were females and 12 were males. The enloled and positive cases are shown in Table 4.
Table 4: Seroprevalence by age-groups in the regions.
Discussion
Given that the vast majority of infection cases remains asymptomatic, countries are seeking to assess the spread of the infection in the population through seroprevalence studies with representation for the general public. The aim of this study was to estimate the degree of spread of SARS-CoV-2 infection in the Romanian population. In this purpose, we have assessed, using a chemiluminescence immunoassay, the anti-SARS-CoV-2 IgG antibodies, as they last longer than IgM and therefore, play a crucial role in assessing the real prevalence of the virus [23]. SARS-CoV-2 invades human cells by binding the spike protein to the membrane protein receptor of the cell. The genome of this virus encodes four key proteins – spike (S), nucleocapsid (N), envelope (E) and membrane (M) [24-27]. As the spike protein is involved in the first step of the infectious process, represented by the interaction with specific receptors, followed by virus internalization in the infected cells, there are many assays that detect the specific antibodies anti-S protein of SARS-CoV-2. Chemiluminescence immunoassay represents an indirect detection method of the anti-SARS-CoV-2 antibodies [28].
It can detect either IgM or IgG in serum [29]. Different countries tested the performance of CLIA, all indicating good specificity, sensitivity and its convenience for sampling [29-31]. Other studies used this method on a specific population to report the seroprevalence: private healthcare group in Fukushima Prefecture, Japan [32]; elite football players in Germany [33]; multicenter, primary care, and emergency care facilities in North Carolina [34]. The findings in this seroprevalence study for SARS-CoV-2 suggest that the prevalence of IgG antibodies against the Spike protein of SARS-CoV-2 is over 6% in Romania. However, according to the official data reported from the surveillance system, the cumulated notification rate for confirmed COVID-19 cases reached to 1.27% at end October 2020, when our study was finished. Our results support the data published regarding the lower proportion of COVID cases which are generally requiring health care, based on the severity of their symptoms The overall seroprevalence in Romania was lower than that recorded in Sweden, but higher than reported in Germany and Spain [2]. However, it should be noted that the specified studies presented a number of differences, regarding the number of participants, time frame and the methods that were used to evaluate the presence of antibodies.
The more modest seroprevalence rate among elderly could be a reason for consideration in the next planning phase for controlling the pandemic. Also we found interesting and significant geographical variations among regions, which could be an argument in favour of adopting public health interventions tailored to the epidemiological situation in the region, even with particularization for the smallest territorial units. Our study has a number of limitations. Although convenience sample is a common strategy used by many researchers, it can provide biased results because this method has the possibility to over/underrepresent a population [35]. The response rate to the study invite achieved lower levels in extreme age-groups. This is normal, because generally the parents could be reluctant or hesitant in agree the enrolment of their children in surveys. On the other hand, the children are less likely to perform blood tests compared to the adults, thus their enrolment was more difficult. As for the elderly, due to the epidemiological situation, they might avoid or postpone their usual blood tests. Women were represented in a higher proportion than men in this study, meaning that women could be more interested in participating in surveys, or more active in general, in investigating their health status.
Conclusion
Our study suggests that the real number of individuals infected with SARS-CoV-2 in Romania exceeds by around five times the number of reported cases confirmed by PCR. Therefore, data on seroprevalence are very important for understanding the magnitude and distribution of the pandemic at country level. Repeating the study after the vaccination campaign could provide strong indications about the further needs of public health interventions.
Opportunistic Diagnosis of Osteoporotic Vertebral Fractures on Imaging Studies performed for Alternative Clinical Indications
Introduction
In an era of increasing life expectancy, osteoporosis has become a major global health concern [1,2]. Osteoporosis is a skeletal disorder characterised by compromised bone strength which predisposes to increased fracture risk [2]. At least one third of all post-menopausal women, and one fifth of men older than 50 will suffer an osteoporotic fracture in his/her lifetime [3-5]. The National Osteoporosis Foundation (NOF) estimates that approximately 54 million Americans suffer from osteoporosis resulting in 2 million fractures annually [6]. Population-based studies have demonstrated an increasing prevalence of osteoporotic fractures resulting in hospitalisation, increased morbidity and mortality and placing increasing burden on healthcare systems [7-9]. Vertebral fractures (VF) account for up to 50% of osteoporotic fractures making them the most common fracture subtype [10]. The incidence of vertebral fractures increases with age [10,11]. Up to 26% of Scandinavian women are diagnosed with at least one VF in their lifetime [11]. VFs are a major cause of pain and reduced mobility. Many patients who have sustained a VF suffer with the psychological fear of isolation and loss of independence [12,13]. Additionally, sustaining a VF is an independent risk factor for mortality [14]. Studies show that patients with previous VFs are five times more likely to obtain an additional VF and are twice as likely to suffer a hip fracture with resulting morbidity and mortality [15,16]. Encouragingly, evidence has shown that early intervention with pharmacological agents such as bisphosphonates result in a relative risk reduction of up to 0.6 for vertebral fractures and up to 0.8 for non-vertebral fractures [17]. Therefore, it is vital that VFs are correctly diagnosed so that patients are investigated and treated appropriately. However, there is a discrepancy between best recommended management and real-life clinical practice studies concluding that many patients diagnosed with an osteoporotic fracture are never appropriately investigated or treated for osteoporosis [18-20].
Many imaging studies performed for alternative clinical indications fortuitously include the spine. Radiologists do not always systematically review the spinal vertebra when they are not the specific clinical area of concern [21,22]. This can lead to a missed opportunity to detect vertebral fractures and diagnose osteoporosis [21,22]. VFs are evident on various imaging modalities that are performed for alternative clinical indications but are frequently not reported by radiologists [23,24]. Use of terminology such as ‘wedging’, ‘endplate compression’ and ‘endplate concavity’ in radiology reports can be confusing and may not be clearly understood as vertebral fracture or implication of underlying osteoporosis by the ordering physician. Non-diagnosis or inappropriate reporting of VFs in this way is a missed opportunity to diagnose osteoporosis, to provide appropriate treatment and to reduce patients risk of further osteoporotic fractures [18]. In this paper, we discuss the radiological assessment of VFs and describe how fractures can be diagnosed on the most used imaging modalities including plain film, MRI, CT and bone scans (Figure 1A- 1B).
Figure 1A: Lateral lumbar spine radiograph of an 80-yearold female patient. The radiograph demonstrates several insufficiency compression fractures; severe anterior wedge fracture at T12, mild compression fracture of the L1 and L4 superior endplates and moderate compression fracture at L2.
Figure 1B: Lateral thoracic spine radiograph demonstrates a moderate compression fracture at T7 with secondary kyphosis.
Assessment of Fractures
Genant et al. devised the Semi-Quantitative (SQ) method for describing vertebral fractures [25]. This method has high inter- and intra-observer agreement, even amongst inexperienced reviewers [25]. The method is widely reproducible and is often used in research settings and clinical trials. The SQ method is a relatively straight-forward method to grade fractures and avoids otherwise confusing language which may be misinterpreted. First described on lateral radiographs, the SQ method employs visual inspection to grade vertebral fractures. Grade 0 is normal without loss of vertebral body height. Grade 0.5 are borderline vertebral fractures. Grade 1 fractures show mild deformity with approximately 20 % to 25 % loss of height and 10 % to 20 % reduction in area. Grade 2 fractures are moderately deformed with 25 % to 40 % loss of height and 20 % to 40 % loss of area. Grade 3 vertebral fractures have lost 40 % or more of their height and area. The SQ method is not without its limitations. Employing this method may inadvertently overdiagnoses VFs in patients with congenital or acquired vertebral anomalies [26]. Additionally, employing the SQ method alone would fail to diagnose minor endplate fractures which do not result in loss of vertebral body height. In response, Jiang et al devised the algorithm-based qualitative (ABQ) approach which focuses on vertebral endplate deformities [27]. Using this method, an experienced radiologist needs to assess various aspects of endplate abnormality before diagnosing it as a fracture. Jiang et al showed that using a stringent criteria-based algorithm in this way, the ABQ method is likely to diagnose only one third of fractures that would be diagnosed by the SQ method alone. Similarly, Black et al showed that the SQ method diagnosed three times the number of mild vertebral fractures compared to other quantitative methods [28].
Recognition of Fractures
Imaging Modalities:
A. Plain Films: For clinically suspected VFs, plain films including antero-posterior (AP) and lateral projections are usually the first line of investigation. The lateral film is particularly useful (Fig. 1A and 1B). The radiologist should carefully examine the vertebral body outline, especially the superior and inferior endplates to ensure VFs are not missed. The pedicles are examined for symmetry on the AP film. Subjectively identifying reduced bone density heightens the index of suspicion for VFs as these patients are at much greater risk. Dynamic radiographs of the vertebrae can increase the likelihood of correct diagnosis on plain radiography. This method allows the radiologist to compare supine images with lateral sitting radiographs to evaluate for changes in vertebral body height. The sensitivity and specificity of dynamic radiographs for diagnosing acute VFs is 66% and 96% respectively [29]. While moderate and severe VFs are rarely misdiagnosed, there are several conditions which can be mistaken for mild VFs leading to overdiagnosis. These include developmental short vertebral height, physiological wedging, Scheuermann’s disease, degenerative scoliosis, Schmorl’s nodes and Cupid’s bow deformity (smooth developmental curvature of the inferior endplate of lumbar vertebra) [30]. Possible reasons for underdiagnosis of VFs by non-musculoskeletal radiologists include focusing on other acute imaging findings, lack of specialist knowledge about osteoporosis/ osteoporotic VFs or simply ignoring osteoporotic VFs completely [31]. Vertebrae are included on many plain films when there is no clinical suspicion of VF. Examples include abdominal radiographs for patients with abdominal pain or chest radiographs in patients with cardio-respiratory symptoms. Less commonly, the vertebrae are incidentally imaged during barium investigations, interventional, cardiac, and fluoroscopic procedures. Even if not performed to out rule a VF, each imaged vertebra should be carefully evaluated to ensure no underlying occult VF. Despite the obvious opportunity to diagnose VFs in this way, there is a paucity of published literature in the area. The most studied radiographic technique to incidentally diagnose VFs is the chest radiograph. In a large study of over 10,000 post-menopausal women who underwent a lateral chest x-ray, 41% of radiologists who identified a VF failed to document it in the report summary, and only 36% were put on treatment for osteoporosis on discharge [32]. In a smaller retrospective review of chest x-rays of post-menopausal women, Gerlach showed that 14.1 % had a moderate or severe VF visible on chest radiograph [21]. Unfortunately, less than one quarter of visible VFs were referenced in the radiologists’ summary and only one seventh of these patients received a discharge diagnosis of VF. As a result, only 18% of patients were discharged with appropriate medical therapy for underlying osteoporosis. The lateral chest radiograph on elderly patients is an opportunity to incidentally diagnose VFs by assessing vertebral bodies and clearly reporting them in the final summary [33]. Despite their importance in the initial investigation for suspected VF, many patients with VFs will have no morphological change on plain films. It is important not to dismiss patient symptoms based on normal radiographs since many patients with normal plain films may only have acute changes detectable on MRI [34]. Loss of vertebral height may not be evident at time of acute symptoms but can be evident on subsequent follow-up radiograph. MRI: MRI is a time-intensive imaging modality with relative contraindications such as claustrophobia, presence of a nonconditional pacemaker and first trimester of pregnancy. MRI has a sensitivity of 100% in detecting spinal trauma and is an excellent method to diagnose and assess VFs [34]. MRI has a sensitivity and specificity of up to 82% and 98% respectively for distinguishing osteoporotic VFs from other types of fracture [35], (Figures 2A-2C). In addition to identifying a VF, MRI may also diagnose other uncommon causes for back pain such as infection or malignancy, and allows assessment of spinal ligaments, spinal cord, surrounding CSF and meninges. The Short Tau Inversion Recovery (STIR) sequence is particularly sensitive to acute fractures as it nullifies marrow fat signal over a large body area such as the entire vertebral column allowing increased visibility of acute pathology such as fracture. STIR sequences in combination with T1 weighted sequences are helpful to differentiate benign osteoporotic VFs from those caused by malignancy [36]. The presence of marrow oedema recognised as high signal on fluid sensitive STIR or T2-weighted fat saturated sequences indicates recent fracture. Marrow oedema is absent in a chronic vertebral fracture. Benign vertebral fractures typically are seen as linear low T1 signal. Malignancy or infection in contrast cause diffuse nonlinear replacement of the normal marrow of the vertebra. For every MRI study performed, initial localizer sequences are utilised by radiographers to plan image acquisition. These localizers are obtained from thick slices and are not suitable for diagnostic detail but do represent an opportunity to diagnose a VF when not suspected. Strong inter-observer agreement has been reported in detecting VFs in the thoracic and lumbar spine on localizer images [37]. In another study, musculoskeletal radiologists examined 856 localizers of patients undergoing breast MRI. The authors concluded that 8.9 % of patients had a VF visible on the MRI localizer, but none were documented in the final report [38]. MRI localizers are a quick and reliable method of diagnosing vertebral fractures when not suspected and may negate the necessity for further imaging or using ionising radiation.
Figure 2: MRI Lumbar Spine with T1, T2 & STIR sequences of an acute mild compression fracture at T10 in a 67-year-old female patient.
Computed Tomography (CT): CT uses high doses of ionising radiation to acquire images. CT imaging is available 24/7 in most tertiary hospitals and offers almost instant acquisition of images. CT has excellent sensitivity and specificity for identifying VFs;100% and 97% respectively [39]. CT of the spine may be requested when a VF is clinically suspected and when the radiograph is normal. Of note, a non-displaced vertebral fracture on a background of osteopenia, may not be evident on CT [39]. In patients with known VF, CT can help to provide additional information such as stability of the fracture and protrusion of bone fragments into the spinal canal. CT can also aid with clinical decisions such as patient suitability for surgical intervention or vertebroplasty. The majority of CTs are performed for clinical indications not specifically related to identification of VFs including Cardiac CT, CTPA and CT thorax to evaluate for thoracic pathology and CT KUB, CT abdomen/ pelvis, CT colonography and CT peripheral angiograms/venograms performed to identify intra-abdominal pathology. Vertebral morphology, particularly on sagittal reformats is well visualised on these CT studies. Modern CT scanners can display vertebrae in the region imaged in excellent bony detail in coronal, sagittal and axial reformats without the requirement for further imaging or radiation exposure to the patient. Of these, the sagittal reconstructions are particularly important to diagnose VFs (Figure 3) [40]. Despite the ability to utilize CT to diagnose occult VFs, CT is often not effectively exploited in this way. A New Zealand study retrospectively reviewed sagittal reconstructions of CT abdomen or thorax in patients over 65 years. 22 of 175 patients had a VF visible on sagittal reconstruction, and 77% of these had previously undiagnosed VF. The authors concluded that reviewing reformatted CT of the abdomen and pelvis improved diagnosis of VFs but are frequently not reported – thereby missing an opportunity to diagnose osteoporosis, treat with appropriate medical therapy and to reduce risk of future osteoporotic fractures and associated morbidity and mortality [41]. Similar to localizers in MRI, CT scout views are obtained prior to final image acquisition. These use low levels of radiation to acquire 2-Dimensional images which are used to plan the final CT image. Lateral CT scout views may show fractures not visible on axial CT images. One study of 300 CT scans involving the thoracic and lumbar spines demonstrated the sensitivity and specificity of diagnosing VFs on scout views to be 98.7% and 99.7% respectively. The authors concluded that scout views should be used to evaluate for VFs on CTs performed for other clinical indications [42].
Figure 3: Sagittal reformatted CT of the Lumbar Spine in an 83-year-old female demonstrating severe compression fracture at L1, moderate compression fracture of T11 and mild compression fracture of L2.
Skeletal Scintigraphy (Bone Scans)
Tc 99m is a radioisotope which can be bound to MDP and injected intravenously. The radioisotope travels through the patient’s bloodstream and binds to remodelling bone. Three hours after injection, patients are placed on a gamma camera which identifies bony hotspots where Tc99m has accumulated. 80% of VFs are visible as hotspots, usually linear in morphology, at 24 hours following injury and almost all return to normal within two years [43]. The major limitation of bone scans is their poor specificity. The most common indication for performing bone scans is to identify osseous metastatic disease in patients with known primary malignancy. However, bone scans are also utilized to identify occult fractures or osteomyelitis. Due to their non-specific nature, hotspots can also be caused by degenerative changes. For this reason, bone scans are often reported in conjunction with other available imaging such as MRI, CT, or plain films (Figures 4 & 5).
Figure 4: Bone scan for completion of staging in a 67-year-old female with non-small cell lung cancer. There are non-specific foci of increased radioisotope uptake in the mid thoracic spine. Comparison was then made to previous staging CT thorax (Fig. 5)
Figure 5: Review of the staging CT thorax confirmed the areas of uptake on bone scan in Fig 4 correlating to previous moderate wedge compression sclerotic vertebral fractures at T6 and T7 secondary to metastatic disease.
Discussion
Osteoporosis is an increasing public health concern and predisposes patients to VFs. Prompt diagnosis and early intervention with appropriate medical treatment is imperative. The literature shows that incidental VFs, on imaging studies performed for alternative clinical indications are underdiagnosed thereby missing an opportunity to diagnose vertebral fracture, diagnose osteoporosis if not previously diagnosed and treat patient appropriately. Untreated and undiagnosed VFs can significantly impact on a patient’s quality of life and life expectancy. Patients with osteoporotic fractures can endure intolerable pain, loss of independence and suffer psychologically due to fear of isolation. Many patients require polypharmacy for pain control, and all are at high risk of future osteoporotic fractures. The mid-thoracic region and thoraco-lumbar junction are the most frequently affected areas and may result in spinal kyphotic deformities. Kyphosis predisposes to loss of balance, muscle wasting, further degenerative changes at adjacent intervertebral joints, restrictive lung disease, inability to work and loss of earnings [44]. Fortuitously many imaging studies including plain radiography, CT, MRI and Bon scans include the thoracic and lumbar spine in the area of imaging. This provides an opportunity to diagnose unsuspected abnormalities of the spine when these imaging studies are performed for alternate clinical indications. Many radiologists however do not systematically review the vertebra in these studies and miss the opportunity to identify abnormalities such as vertebral fractures and osteoporosis. When vertebral morphological abnormalities are identified equivocal language such as ‘loss of height’ or ‘wedging’ to describe VFs can be misleading. This terminology is ambiguous for referring physicians who may not appreciate that these are vertebral fractures and imply underlying osteoporosis. There is no agreed gold standard for diagnosing VFs on imaging. As a result, many VFs are both under and over-diagnosed. One strategy is the semi-quantitative method for grading fractures. Even amongst inexperienced observers, the SQ method demonstrates high levels of agreement [21]. Alternatively, the ABQ method forces the radiologist to answer a number of questions before diagnosing a VF and is arguably more accurate [27]. Whichever method is employed, it remains imperative the reading radiologist clearly states the existence of a VF in the report summary to improve the proportion of patients discharged on appropriate medical therapy. A number of imaging techniques performed for various clinical indications may show VFs in the area imaged. There is under reporting of VFs which are clearly visible on lateral chest radiographs, MRI localizers and CT scout views. Unless sagittal reformats of CT studies are routinely performed often VFs are not visible on standard axial images even to experienced musculoskeletal radiologists. The term ‘inattentional blindness’ refers to an inability to notice unexpected events when immersed in an alternative task. In one experiment, 83% of expert radiologists failed to recognise a gorilla drawn onto a stack of CT images when they were focusing on finding pulmonary nodules [45]. Another phenomenon coined “satisfaction of search” refers to a relative difficulty in identifying further pathological findings following identification of another significant abnormality [46]. These factors are relevant to radiologists when searching for clinically significant pathology not related to the spine on x-ray, MRI, or CT and thus VFs can easily be overlooked. Dedicated education programmes delivered to radiologists and internal medical physicians may help to improve the diagnosis and management of VFs. In one study, recognition of VFs amongst internists almost doubled from 22% to 43% following provision of basic lectures, posters and flyers. The same study demonstrated a significant increase in patients discharged on osteoporosis treatment from 11% to 40% [47]. In another study, there was a marked improvement in the ability of a radiology resident to correctly identify VFs after undergoing specific teaching [48].
Conclusion
In conclusion, VFs are a major health concern in an era of aging population. Many factors have contributed to underdiagnosis and treatment of VFs. When identified by a radiologist ambiguous terminology should be avoided and the SQ method employed. The spine is included in many imaging studies performed for alternative clinical indications. This is a fortuitous opportunity to assess the spinal vertebrae and diagnose fractures when present. Irrespective of the clinical indication or imaging modality, a high index of suspicion for VFs should be always employed. Basic education programmes for radiologists and internists would serve to improve the diagnosis of VFs and treatment of osteoporosis.
New Approach to the Treatment of CoV-2 Infection by Means of Immune-modulators and Non-Steroid Anti- Inflammatory Drugs
Historical Background of the “COVID-19” Pandemic
The first known case of coronavirus was described as “severe acute respiratory syndrome” (SARS), which occurred on November 16, 2002, in Foshan, a city about 20 km from Guangzhou in China’s Guangdong province. Since November 2002, an unknown infectious agent had caused outbreaks of an atypical pneumonia that spread throughout Guangdong province in southern China. The disease usually started with high fever and mild respiratory symptoms, but rapidly progressed to pneumonia and within a few days new cases emerged in mainland China, so that by February 2003 more than 300 cases had been reported, about one-third of which involved health care workers [1]. Persons who became infected and subsequently traveled spread the outbreak to Hong Kong [2] and from there to Vietnam, Canada, and several other countries [3]. By the end of February 2003, the disease had spread to neighboring regions and countries, was severe, could be transmitted from person to person, and appeared to cause significant outbreaks in health care workers [3,4]. On March 13, 2003, WHO issued a global alert on the disease that it termed “severe acute respiratory syndrome” (SARS) [5], and a remarkable global effort led to the identification of the SARS coronavirus (SARS-CoV). In early April of the same year [4,6], 6 outbreaks occurred in Southeast Asia, North America and Europe and led to the first pandemic of the 21st century. In July 2003 and after a total of 8,096 reported cases, including 774 deaths in 27 countries [7], no further infections were detected and the SARS pandemic was declared to be over. Five additional cases of SARS, as a result of zoonosis, occurred between December 2003 and January 2004 [8], but no further human cases of SARS have been detected since then. Infection control measures, rather than medical interventions, then put an end to the first SARS-CoV pandemic of the 21st century. However, the possibility of transmission in a variety of ways was noted. It was later shown that certain viruses, similar to SARS-CoV found in bats, could infect human cells without prior adaptation [9,10], indicating that SARS could re-emerge [11]. Indeed, 10 years after the first occurrence of SARS-CoV, a man in Saudi Arabia died of “acute respiratory syndrome” and in his serum the “coronavirus” had been isolated, this syndrome was called “Middle East Respiratory Syndrome coronavirus” (MERS) because of its place of origin. In April 2012, several cases of “severe respiratory illness” had already occurred in a hospital in Jordan [12], these cases were retrospectively diagnosed, and considered to be human-to-human transmitted, furthermore in the United Kingdom, 3 cases of MERS were reported in September 2012 [13].
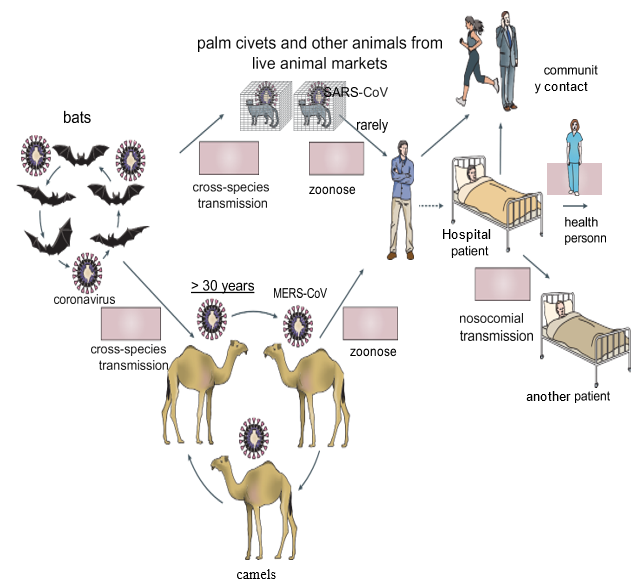
In May 2015, a single person, returning from the Middle East, initiated a nosocomial MERS outbreak in South Korea that affected 16 hospitals and 186 patients [14]. By April 26, 2016, 1,728 MERS cases, including 624 deaths, had been confirmed in 27 countries [15,16]. (Figure 1) In the accompanying figure, published in 2016 (copied from review paper: de Wit E, Doremalen VN, Falzarano D, et al. SARS and MERS: recent insights into emerging coronaviruses. Nat Rev Microbiol. (2016) 14: 523-34.doi: 10.1038/nrmicro.2016.81) shows as different ways of coronavirus transmission. Bats could have been the main reservoir of the coronavirus 30 years before passing to humans, due to “cross-species transmission” between bats and camels; these animals, through continuous contact with humans, could have produced the direct zoonosis that gave rise to MERS-CoV. Moreover, the detection of the virus in “palm civets” (Chinese species) and in a “raccoon dog” (Japanese raccoon), as well as the detection of antibodies to the virus in the Chinese ferretbadger (also known as small-toothed ferret- badger) observed at a live animal market in Shenzhen, China [17] alerted researchers to the possible transmission of the virus to humans. However, these animals were only incidental hosts, as there was no evidence of SARS-CoV-like virus circulation in “palm civets,” both in the wild and in breeding facilities [18]. Thus, the search for the MERSCoV reservoir initially focused on bats, but a serological study in dromedaries from Oman and the Canary Islands showed a high prevalence of MERS-CoV neutralizing antibodies in these animals [19]. In addition, MERS-CoV RNA was detected in swabs collected from dromedaries on a farm in Qatar that was associated with two human cases of MERS, and infectious virus was isolated from dromedaries in Saudi Arabia and Qatar [20-23], and serological tests also detected circulation of a MERS-CoV-like virus in dromedaries in the Middle East, East Africa, and North Africa. Dromedaries in Saudi Arabia harbor several viral genetic lineages [24], including those that have caused outbreaks in humans. Taken together, these data pointed to the role of dromedaries as a reservoir of MERS-CoV. The ubiquity of infected dromedaries near humans and the resulting zoonosis may explain why MERS-CoV continues to cause human infections, whereas SARS-CoV, without the continued presence of an infected intermediate host and with relatively infrequent human-bat interactions, had not caused further human infections.
Figure 1.
Person-to-person transmission of SARS-CoV and MERS-CoV occurred primarily through nosocomial transmission. Between 43.5 and 100% of MERS cases in individual outbreaks were hospital-related, and very similar observations were made for some of the SARS clusters [25-26]. Transmission among family members occurred in only 13 to 21% of MERS cases and 22 to 39% of SARS cases. Patient-to- patient transmission of MERSCoV was the most common route of infection (62-79% of cases), whereas for SARS-CoV, infection of health care workers by infected patients was very common (33-42%) [25]. The predominance of nosocomial transmission is probably due to the fact that substantial virus shedding occurs only after symptom onset [27-28], when most patients are already seeking medical care [29]. An analysis of hospital surfaces after treatment of patients with MERS showed the ubiquitous presence of viral RNA in the environment for several days after patients stopped testing positive [30]. In addition, many SARS or MERS patients were infected through “superpropagators” [25-27,31-33]. As of 2016, it had already been provided, in various publications, that the key features of these viruses are: the predominance of nosocomial transmission, pathogenesis driven by a combination of viral replication in the lower respiratory tract and an aberrant host immune response, and several potential treatments for SARS and MERS in animal models and “in vitro” had also been suggested, including small-molecule protease inhibitors, neutralizing antibodies and inhibitors of the host immune response.
Current Pandemic COVID-19
In December 2019, a new coronavirus (“nCoV”) emerged in Wuhan, Hubei province in China. Attention was focused on the Huanan food market, where in addition to fish, livestock animals were also traded. However, analysis of the first 41 hospitalized patients showed that the Wuhan seafood market might not be the main source for the spread of a new virus [34]. Nevertheless, an epidemic of severe pneumonia of unknown cause soon appeared [35], and genomic sequencing of viral isolates from five pneumonia patients hospitalized from December 18 to 29, 2019, indicated the presence of a previously unknown “b- CoV” strain in patients [36]. This “new” coronavirus (nCoV) subsequently spread from the original outbreak site in China and was designated as “SARS-CoV-2” by the World Health Organization (WHO) on January 12, 2020 and the disease as “COVID-19” on February 11, 2020 [37] and this virus was confirmed to have 75-80% similarity to the coronavirus that caused severe acute respiratory syndrome (SARS-CoV) [38]From February 2020 to April 2020, the disease “COVID-19” affected 188 countries worldwide. [38]and up to July 14, 2020 the cumulative number of confirmed cases was 13.1 million people and at least 572,426 people died from SARS-CoV-2 infection [39], the incidence of deaths ranged from less than 1% to 3.7% among the different countries [40], these figures were compared with the rate of deaths from influenza which was less than 0.1% [35].
After the first pandemic period, the incidence of COVID-2 infected cases declined during the summer months and then rose again significantly from September/October 2020 to date (31 January 2021), the increase in incidence is statistically shown as a “wave”, with 3/4 “waves” with “peaks”, “plateaus” and “valleys” in different countries; Most European Union countries, including Spain, have experienced high levels of incidence, but the highest number of infections has been observed in Great Britain, the USA, Brazil and India, up to this point. As of January 30, 2021, the number of cases in the world since the pandemic began at the end of 2019 has been: 102,000,000, and the number of deaths: 2,210,000.
The Acute Inflammatory Process
From the clinical point of view, the disease caused by CoV-2 presents 3 fundamental stages: in the first stage the patient shows signs and symptoms similar to infection by other viruses and/ or bacteria of the respiratory tract (e.g., Influenza), in this stage the symptoms are shown to a lesser degree and the patient may even be asymptomatic. In the second stage the patient feels worse and the signs and symptoms are more evident (fever, tiredness, general malaise, anosmia, hypoacusis, etc.); this stage is definitive for the patient, who may improve in the following days until cured or worsen until reaching the third stage, which may worsen to the point that the patient has to be admitted to the ICU, where intubation and assisted respiration may even be necessary; this moment is crucial for the patient since the feared “cytokine storm” may occur. From the immunological point of view, infections by bacteria and/or viruses, accidental or provoked trauma (e.g. surgical interventions), allograft rejection and the development of neoplasms have a common point: inflammation. Inflammation is the result of multiple interactions of the systems involved in the homeostasis of the organism, mainly the immune system, which have as their first objective the localization of the process and the elimination of the aggressor agent. When the infection is aggravated by a huge excess of antigen (due to the unstoppable and rapid replication of the virus), the inflammation reaches its climax and becomes a systemic process that affects the whole organism, it is called “systemic inflammatory response syndrome” (SIRS), and in the case of COVID-19, since the respiratory system is the main system affected, it is called “SARS-CoV-2” (“systemic acute respiratory syndrome”), the response of the immune system overflows and the “cytokine storm” appears, which can lead to “multiorgan failure” (MOF) and death of the patient. In fact, from a biological point of view, tissue injury and its sequelae are involved in most medical problems and the response of living tissues to aggression is the basis and foundation of the immune response. [41-45].
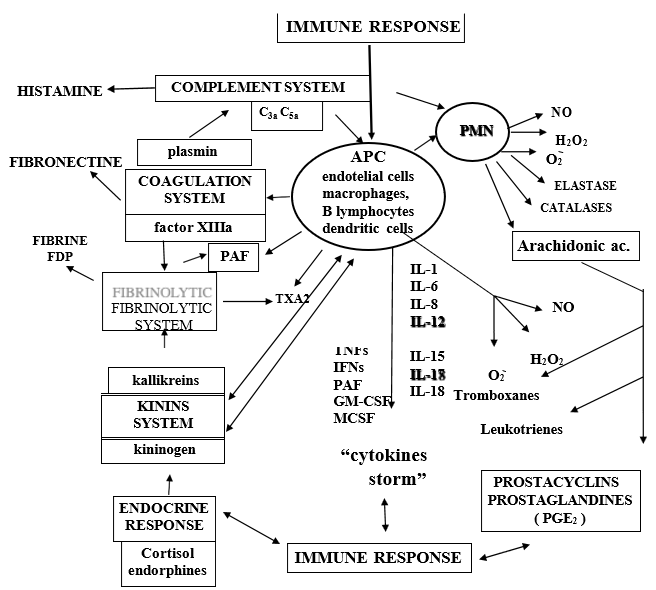
In addition to cytokine storming, COVID-19 viral particles can also directly induce multiple organ dysfunctions. In this regard viral particles from COVID-19 infection have been identified in bronchial and alveolar type 2 epithelial cells, and in fecal and urine samples [46,47]. Therefore, it is suggested that multiple organ dysfunction in patients with severe COVID-19 may also be caused by a direct attack by the virus. Many authors think that the synergistic effects of both effects contribute to the “multi-organ” failure of patients with severe COVID-19 however, we and some authors believe that in fatal COVID-19 cases, severe dysfunction of the immune response is responsible to a greater degree than the direct damaging effect of the virus itself [42,47]. (Figure 2) When macrophages or any other “antigen presenting cell” (APC) are stimulated, the “proinflammatory” cytokines par excellence are released: IL-1, IL-6, IL-8, IL-15, IL-17, IL-18, TNFs, IFN□ and PAF (platelet-activating factor). These cytokines play a relevant role in the inflammatory process and, in turn, can give rise to the so-called “cytokine storm”, the consequence of which is “systemic inflammatory response syndrome” (SIRS) and finally “multi-organ failure” (MOF), leading to death. On the other hand, as Niels Jerne (1974) said: “any stimulus capable of producing an immune response provokes a reaction comparable to the transmission of the ripples that can be observed in a pond when a stone is thrown, so that in the immune system the variation at the site of the stimulus receptor is transmitted everywhere”. In “SARS” this allegory reaches a dramatic expression and encompasses not only the network of signals, which cross and intersect within the immune system, but between the different systems (coagulation, fibrinolytics, cyanins, arachidonic acid, leukotrienes and thromboxanes, the immune system itself (complement system, circulating immune complexes ICC, ADCC, NK cells, adaptive immune response: CTL and cytokines) (Figure 2).
Figure 2: Navarro-Zorraquino M Immunologic response in shock and multiorgan failure. In: Navarro-Zorraquino M, editor. Immunological aspects of surgery. Zaragoza: Prensas Universitarias de Zaragoza; 1997. p. 261-300.
For this reason, the lack of control of the servomechanisms that maintain homeostasis in any of the mentioned systems can cause an unstoppable situation of mediator release leading irremediably to tissue damage [42]. From the pathophysiological point of view, inflammation is the result of multiple interactions between the various systems of the organism, which have as their first objective the localization of the process and the elimination of the aggressor agent; this is followed by a repair process. The main physical-chemical events that occur during inflammation are: increased blood supply to the site of the attack, increased capillary permeability – which allows larger molecules than usual, such as antibodies and fractions of the complement system and other enzyme systems, to pass through the vascular endothelium – and the activation of leukocytes: initially neutrophils and macrophages, then lymphocytes. The development of the inflammatory reaction is controlled by cytokines, which are the intercellular messengers of the “immunocompetent” molecules, the products of the plasma enzyme systems, the coagulation, fibrinolytic, cyanin and complement systems, vasoactive mediators released from mast cells, basophils and platelets, and endothelial adhesion molecules. Since CoV-2 exhibits tropism to the lung, the initiation of the immune response against coronavirus begins with direct infection of the bronchus and bronchiole epithelium. First, antigen-independent innate immunity provides the first line of defense of leukocytes against microorganisms. The “innate immune response involves several cell types, including leukocytes, neutrophils, eosinophils, eosinophils, basophils, monocytes, macrophages, lung epithelial cells, mast cells, and NK cells. After initial CoV-2 infection, dendritic cells (DCs) residing in the lungs become activated and change to “antigen presenting cells” (APCs).
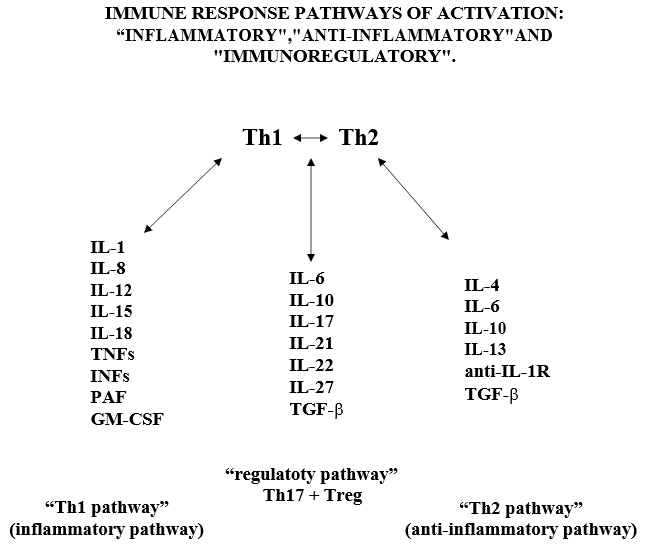
Figure 3.
In the lung, DCs reside within and beneath the airway epithelium, alveolar septa, pulmonary capillaries and airway spaces. Activated APCs” cells ingest and process the antigens and migrate to the lymph nodes, in the lymph nodes the “APC cells” present the antigen in the form of MHC/peptide complex to the “virgin circulating T helper cells” (Th0), inducing the immune response. Following activation of the Th0 receptor by the MHC/peptide complex, Th2 cells are activated, proliferate and differentiate into CD4+ (Th lymphocytes) and CD8+ (cytotoxic T lymphocytes) cells. Subsequently, Th lymphocytes further differentiate into Th1 and Th2 cells, which are capable of releasing different cytokine profiles: Th1 cells drive cell-mediated immunity and release pro- inflammatory cytokines such as IFN-γ, IL-1β, IL-12 and pro-inflammatory factors such as TNFs, IFNs, PAF, GM-CSF, MCSF; Th2 cells activate the production of antibody-producing B cells and release anti- inflammatory cytokines such as TGF-β, IL-4, IL-5, IL-9, IL-10 and IL-13 [42,47]. In the immune response of healthy adults with CoV-2 infection there is a balance between Th1 and Th2 lymphocyte activity. The inflammatory reaction initiated by the immune system, through the Th1 activation pathway and with the participation of Th17 cells and various cytokines, is regulated by the immune response itself through a “regulatory servo-mechanism” involving mainly Th2 cells (considered as the main pathway of the “anti-inflammatory response”), through sub-populations of Th2 cells, called “regulatory cells”: Treg (CD4+25+FOXp3 and CD8+25+FOXp3) and Th-17 cells (Figure 3). Th17 cells” regulate the response by increasing the release of “pro-inflammatory” cytokines and Treg cells” regulate the response towards the release of anti-inflammatory cytokines. (Figure 3) Navarro-Zorraquino M. Immunologic response in shock and multiorgan failure. In: Navarro-Zorraquino M, editor. Immunological aspects of surgery. Zaragoza: Prensas Universitarias de Zaragoza; 1997. p. 261- 300. We wish to emphasize here that the “regulatory pathway” exerts its role by responding to the needs of the immune response, at a given time, against the corresponding antigen, by increasing the inflammatory activity of the Th1 pathway, mainly by means of Th17 cells and IL-17A, or by increasing the anti-inflammatory activity of the Th2 pathway, mainly by means of transforming growth factor β (TGF-β). Since these 2 cytokines are going to be the key in the design of our research project, we will insist on them later.
Systems of the Human Organism Affected by the “Cytokine Storm”
It is important to remember here the influence and consequences that the immune response has on the most important systems of the human organism, especially when it overflows producing the “cytokine storm”. If we look at Fig. 2, we can see that this response is related to the release of histamine, activation of the coagulation, fibrinolysis and “kinins” systems, release of arachidonic acid metabolites, neuroendocrine response, release of free radicals and release of prostacyclins and prostaglandins [42]. When the complement system is activated, the different fractions are released (activation by the classical pathway begins with the C1 fraction, and activation by the alternative pathway begins with the C3 fraction), but the most important for their pathophysiological actions are the C3a and C5a fractions (called anaphylatoxins), which increase capillary permeability and produce smooth muscle contractionboth at the level of the bronchial tree and the gastrointestinal tract; the C3a fraction is capable of producing tachycardia, impairing cardiac function and inducing coronary vasoconstriction. The C3a and C5a fractions stimulate basophils and mast cells to release histamine, whose main action is to increase vascular permeability and smooth muscle contraction. When aggression to the organism occurs, activation of the enzymatic cascades of the complement system, kinins, coagulation and fibrinolysis occurs rapidly, as well as cell activation of PMN leukocytes, macrophages, endothelial cells and platelets. Tissue damage produced by viruses (the case of CoV- 2) induces platelet aggregation and adhesiveness on subendothelial collagen when the vascular endothelium is damaged, thus initiating an activation, by means of the so-called intrinsic pathway, through the activation of factor XII (Hageman’s factor), which gives rise to FXIIa [42] which is an active protease; this is a key factor that directly relates the coagulation system to the so-called “kinin system”, “kinins” or “kinins” (Figure 2). kinins” or “kinins” (Figure 2). FXIIa activates pre-kallikrein which becomes kallikrein and this, in turn, becomes kininogen, a high molecular weight substance, which together with factor XII and pre-kallikrein binds directly to sub- endothelial collagen, as do platelets through the mediation of Willebrand factor (Figure 2).
At the same time that activation of the coagulation system by the intrinsic pathway occurs, activation of the so-called “extrinsic pathway” can also occur, by means of tissue thromboplastin released by damaged cells; tissue thromboplastin activates the extrinsic pathway in collaboration with factor VIIa (FVIIa) causing factor X (FX) to also become an active protease -FXa-. The result of the activation of the coagulation system by both pathways is the conversion of prothrombin to thrombin, which increases platelet aggregation and induces the release of arachidonic acid metabolites, especially thromboxane A2 (TxA2) (Figure 2).This activation of the coagulation system would be implicated in the immune response to CoV-2 and the production of clots in patients with COVID-19, especially in the most severe stage of the disease, as well as in the finding of clots in the necropsies of deceased patients. The hypothalamic-pituitary-adrenal axis responds to stimuli that represent the release of mediators and the organism’s own aggressor agent in a given situation. At the present time there are numerous studies that attempt to relate different hormones, whose synthesis and release is regulated by the neuroendocrine system, with the immune response in various situations. We will refer here only to what seems to us most relevant in relation to the inflammatory response and in particular to the pathophysiology of the “cytokine response”[42].
Cortisol is the most important glucocorticoid secreted by the adrenal cortex in response to ACTH and corticotropin-releasing hormone (CRH). Cortisol plays a very important role in many aspects of the inflammatory response and shock (it increases the effect of catecholamines, increases protein catabolism at the muscular level, has action (together with epinephrine and norepinephrine) on vascular smooth muscle, on lipolysis and on neoglycogenesis). But here we try to emphasize that cortisol inhibits the release of “kinins” and that it is closely connected with the release of other mediators and with the systems of coagulation, fibrinolysis and the complement system in the inflammatory response. In addition, cortisol considerably reduces the number of lymphocytes, especially the number of T- lymphocytes, in patients with sepsis. in this regard, it is very noticeable that the majority of patients affected by COVID-19 show lymphopenia. Nitric oxide (NO) is synthesized in the body from L-arginine by an enzyme: nitric oxide synthase. There are two types of this enzyme: one is a constituent of the cytoplasm and is Ca++ and calmodulin dependent for NO release; the other enzyme is also a cytoplasmic component, but is Ca++ independent, however it requires tetrahydro-biopterin and other cofactors for its activation and is inhibited by glucocorticoids. Following the studies of Furchgott and Zawadzki, et al. [47-50] there is no doubt that NO is a very important neurotransmitter. The enzyme nitric oxide synthase is found in brain neurons, but is not present in glia; in the pituitary it is found in brain neurons, but is not present in glia; in the pituitary it is found mainly in neurons located in the posterior lobe (which are the neurons that synthesize and release vasopressin and oxytocin), it is also found in the adrenal medulla in neurons that stimulate the cells that release adrenaline or epinephrine), in the intestine it is found in the mesenteric plexuses, regulating peristaltic movements. In addition, nitric oxide synthase is present in numerous tissues, but especially in the cells of the endothelial layer of blood vessels, where it seems to play an important role in vasomotor phenomena, but also as a “messenger” molecule closely connected to the immune system. In all these tissues NO release by nitric oxide synthase appears to be Ca++ and calmodulin dependent (as described above), constituting the “physiological NO production pathway”.
The point of view that most interests us here is the relationship of NO with the immune response, not only because it is able to stimulate macrophages, endothelial and dendritic cells against bacteria, but also against viruses and rikettsias, and because it is actively involved in the inflammatory process. Its excess production may contribute to a high degree to the pathophysiology of SARS and multiorgan failure. Macrophages produce detectable levels of NO about 6 hours after activation by IFN-g, reaching the maximum level at 24h. However, there is a “servo-control mechanism” by which NO can regulate its own synthesis, inhibiting IFN-g production from Th1 cells and also that of nitric oxide synthase. In addition, some cytokines, including IL-4 and IL-10 and TGF-b, also have an inhibitory effect (apparently “dose-dependent”) on NO production. In this respect, antagonists of cytokine and NO production could be a therapeutic measure in the treatment of COVID-19, as evidenced by some in vitro studies.
Risk Factors Associated with COVID-19 Infection
Diseases associated with COVID-19 infection, mainly severe heart disease, chronic kidney disease, chronic obstructive pulmonary disease (COPD), cancer (patients undergoing active treatment), immunosuppression due to solid organ transplantation, obesity and type 2 diabetes mellitus, together with advanced age of the patients, can result in “immune dysregulation” leading to failure of the “system regulatory pathway” and “anti-inflammatory pathway” with an exaggerated shift towards the “inflammatory pathway”, can result in “immune dysregulation”, leading to failure of the “system regulatory pathway” and the “anti-inflammatory pathway” with an exaggerated shift to the “inflammatory pathway” which can develop into a huge release of cytokines and inflammatory factors called “cytokine storm”.
Advanced age is perhaps the most important factor in our century, since there are populations of people living in the world at very advanced ages of life (even people > 100 years), especially in developed countries. Overall, published work with respect to patient age shows that the COVID-19 pandemic is causing a large increase in mortality in the elderly population, relative to the mortality rate observed in patients under 70 years of age.” The mortality rate is dramatically alarming in the case of patients older than 80 years, about 30% compared to the total population of COVID-19 infected patients [44]. Some currently published statistical data show that the probability of death from COVID-19, compared with the age group of infected patients aged 18-29 years, can be summarized as follows: persons aged 30-39 years (2 times higher), 40-49 years (3 times higher), 50-64 years (4 times higher), and 50-64 years (4 times higher). higher). 65-74 years (5 times higher), 74-84 years (8 times higher), > 85 years (13 times higher) [51]. All of the above shows that the COVID-19 pandemic is causing a large increase in mortality in the elderly population, compared to the mortality rate observed in patients younger than 70 years of age. The mortality rate is dramatically alarming in the case of patients over 80 years of age, about 30% compared to the total population of CoV-2 infected patients.
Important Characteristics of Aging
Chronic inflammation in aging, described as “inflammatory aging, may occur in elderly patients, and may also be associated with other related disorders. with inflammation: diabetes mellitus, obesity, arthrosis, etc. Consequently, the increased generation of pro-inflammatory markers in “inflammatory aging” may have an impact on the severe inflammatory process that occurs in patients with COVID-19 and increased risk of mortality. Several factors, including altered ACE2 receptor expression, excess reactive oxygen species (ROS) production, senescent adipocyte activity, altered autophagy and mitophagy, “immunosenescence”, as well as severe vitamin D deficiency (VD) may be associated with “inflammatory aging” and contribute to the cytokine storm in elderly patients suffering from COVID-19 [52,53].
Alteration Of Ace2 Receptor Expression
SARS-CoV-2” uses the same receptor “angiotensin-converting enzyme 2” (ACE2) as “SARS-CoV” (the coronavirus associated with the SARS outbreak in 2003). The “renin-angiotensin system” (RAS) is an important regulator of several physiological events, including cardiovascular and blood volume, natriuresis, diabetes, chronic kidney disease and liver fibrosis. The study by Xudong and colleagues in 2006 observed in the rat lung that ACE2 expression is significantly reduced with aging; these authors suggest that ACE2, which is higher in young adults compared to older age groups, may contribute to the prevalence of SARS episodes in this age group. On the other hand, Chen and colleagues, in 2020, found a markedly higher expression of ACE2 in Asian women compared with men; they also found an age-dependent decrease in ACE2 expression, and a highly significant decrease in type II diabetic patients, and established a negative correlation between ACE2 expression and death from COVID-19 [54].
Excess Production of Reactive Oxygen Species (ROS)
The effects of reactive oxygen species (ROS) on cellular metabolism have been well documented in a wide variety of species. These include not only roles in programmed cell death and necrosis, but also positive effects, such as induction of defense genes and mobilization of ion transport systems. It is also frequently implicated in “redox signaling” or “oxidative signaling” functions. In particular, platelets involved in wound repair and blood homeostasis release reactive oxygen species to recruit more platelets to sites of injury. They also provide a link to [immune system] adaptation through white blood cell recruitment. Reactive oxygen species are involved in cellular activity in a variety of inflammatory responses including cardiovascular disease. They may also be involved in cochlear damage induced by elevated sound levels, ototoxicity of drugs such as cisplatin, and in congenital deafness in animals and humans. Redox signaling is also involved in mediating apoptosis or programmed cell death and in ischemic injury. Specific examples are strokes and heart attacks. Garrido, et al. [55] identified that immune cells from prematurely aging mice had lower values of antioxidant defenses and higher values of ROS and pro-inflammatory cytokines, thus suggesting that excessive ROS production during aging may activate the inflammatory response and subsequently increased release of pro-inflammatory cytokines, which include TNF-α, IL-1β, IL-2 and IL-6 and adhesion molecules. Therefore, excessive ROS production and inflammation are closely related, as they are involved in the pathogenesis of chronic inflammation and “inflammatory aging” in older adults.
Autophagy and Age
Autophagy is a conserved catabolic turnover pathway in eukaryotic cells by which cellular material is delivered to lysosomes for degradation. The autophagy process is related to the maintenance of cellular homeostasis, and its dysregulation could lead to the development of several pathophysiological diseases related to aging [56]. It has been shown that the autophagy process decreases during aging and leads to the accumulation of damaged macromolecules and organelles. Decreased autophagy during aging may also lead to dysfunctions in mitochondria and consequently to increased ROS production [57] (since mitochondria are the main source of ROS. On the other hand, mitophagy, which is characterized by autophagic degradation of mitochondria, decreases in aging the decrease in mitophagy, together with the decrease in antioxidant capacity during aging [58], may increase the levels of ROS in the human organism and also to the increased secretion of proinflammatory cytokines during aging [59-62].
Senescent Adipocytes and Age
Some studies on aging highlight the importance of adipose tissue inflammation in aged animals by elevated release of IL- 6, IL-8, IL-1β, and TNF-α. [63-65] Adipose tissue is a dynamic structure that plays an important role in modulating metabolism and inflammation. It is very likely that adipose tissue dysfunction (e.g., obesity during aging) is associated with chronic inflammation in elderly subjects [66]. The mortality rate of obese elderly patients with COVID-19 is approximately 14%. Covarrubias ,et al. [67] found that during aging senescent cells accumulate significantly in visceral adipose tissue and that “inflammatory cytokines” are found in the supernatant of senescent cells, Alicka et al. in 2020 found that “stem cells” derived from adipose tissue of old horses (older than 5 years) exhibited increased gene expression of pro-inflammatory and miRNA genes (such as IL-8, IL-1β, TNF-α, miR-203b-5p and miR-16-5p) and markers of apoptosis (such as p21, p53, caspase-3, caspase-9) [68]. Therefore, it is possible that elevated release of pro-inflammatory cytokines by senescing adipocytes carries an elevated risk of the “cytokine storm” in obese elderly patients with COVID-19.
Age and Immunosenescence
Immunological senescence” is characterized by alterations in both humoral and cell-mediated immune response. Dysregulation of the response severely impacts the pro-inflammatory/antiinflammatory balance when the organism is attacked by an infectious agent. It is known that NK cells and macrophages link the innate and cell-mediated immune systems. Some authors have described an increase in the number of circulating NK cells during aging [69]. One of the important cytokines for the cytotoxic activity of NK cells is IL-2, which increases the killing properties and proliferation of NK cells. In a young healthy individual, IL-2 can induce IFNg secretion by NK cells, but this effect is diminished in the elderly [70]. On the other hand, it has been observed that T cell numbers do not decrease during aging, but the T cell pool shows significant age-related alterations, including impaired responses to T cell stimulation by mitogens, an inverted CD4+/CD8+ T cell ratio, a reduced proportion of Th0 cells, and an increased proportion of “memory cells,” in animals and humans [71-73]. In addition, aging is associated with overproduction of pro-inflammatory cytokines by T cells, leading to immune pathology [74]. The proportion of Th17 cells increases during aging, resulting in an “inflammatory aging” state in adults [75]. The “Th17 regulatory” cells have the “pro-inflammatory” phenotype and are in balance with “antiinflammatory Th-reg cells.” Both cells are derived from a common precursor: Th0 cells [76]. During aging, the generation of several macrophage-induced factors, including fibroblast growth factor, vascular endothelial growth factor, epithelial growth factor, transforming growth factor (TGFβ), is reduced. TGFβ is one of the most important “cytokines” released by “anti-inflammatory regulatory cells”. Therefore, it is thought that the fragile and mildly overactive immune system in older adults cannot turn off proinflammatory response in COVID- infection. 19. The clinical findings in severe patients with COVID-19 infection are consistent with the literature mentioned above. In 2019, Schouten et al. identified that the increase in “pro-inflammatory cytokines” during aging also correlated with SARS severity and could explain, at least in part, the difference in COVID-19 severity between young adult patients and elderly patients [77].
Age and Vitamin D Deficiency
Older adults are at risk for vitamin D deficiency due to several factors, including decreased pre-vitamin D production, poor skin integrity, decreased dietary intake of vitamin D, increased adiposity, obesity, decreased kidney function, as well as less time outdoors [78].Vitamin D deficiency has been linked to various inflammatory diseases related to aging, such as rheumatoid arthritis, asthma, inflammatory bowel disease, multiple sclerosis, cardiovascular disease, hypertension, diabetes mellitus, and cancer [79].
Vitamin D together with the vitamin D receptor (VDR) have an important anti-inflammatory function, acting as “immunomodulators” by decreasing the release by Th1 cells of “proinflammatory cytokines” and increasing the release by Th2 cells of “anti-inflammatory cytokines”. Furthermore, vitamin D deficiency in elderly subjects is associated with the pro-inflammatory phenotype of immune cells, which probably increases the risk of “inflammatory aging” in older adults [80], and this chronic inflammatory condition could contribute to the “cytokine storm” in elderly patients with COVID-19. However, patients with renal failure or granulomatous disease are at high risk for side effects and should be excluded from being treated with vitamin D supplementation. Upcoming vitamin D supplementation trials will provide more clarity on the in vivo effects and the opportunities and possible limitations of vitamin D as an immuno-regulatory agent. In this regard, recent work by Murai, et. al [81] shows that high-dose vitamin D3 shows no significant difference among hospitalized patients with COVID-19, nor does it significantly reduce the length of hospital stay. These findings do not support the use of high- dose vitamin D3 for the treatment of moderate to severe COVID-19.
Influence of Sex
The higher COVID-19 case fatality rate and greater disease severity in men compared to women are likely due to a combination of behavioral/lifestyle risk factors, prevalence of comorbidities, aging, and underlying biological sex differences. However, the underlying biological sex differences and their effects on COVID-19 outcomes have received less attention. The recent review conducted by Haitao Tu, Vermunt JV et al. of the Mayo Clinic (October 2020) [82] summarizes the available literature regarding proposed molecular and cellular markers in COVID-19 infection, their associations with health outcomes, and any reported modifications by sex.
Biological sex differences characterized by such biomarkers exist within healthy populations and also differ with age- and sex-specific conditions, such as pregnancy and menopause. In the context of COVID-19, descriptive biomarker levels are often reported by sex, but data regarding the effect of patient sex on the relationship between biomarkers and COVID-19 disease severity/outcome are scarce. Such biomarkers may offer plausible explanations for the worse COVID- 19 outcomes observed in men. Larger studies with sex-specific reporting and robust analyses are needed to elucidate how sex modifies the cellular and molecular pathways associated with SARS-CoV-2. This would improve biomarker interpretation and clinical management of patients with COVID-19 by facilitating a personalized medical approach to risk stratification, prevention, and treatment. Several comorbidities, which occur disproportionately in men, likely contribute to worse COVID-19 outcomes, it is thought that perhaps ACE inhibitors are involved or that angiotensin receptor blockers may exert adverse effects on COVID-19. Experimental and epidemiological evidence is conflicting as to whether the use of ACE inhibitors and angiotensin receptor blockers upregulate ACE2 expression and affect susceptibility to infection and/or disease severity. Ongoing randomized clinical trials could inform whether this differs by sex and recommendations on the use of such therapy in patients with COVID-19.
Immunologically
It appears that women have a stronger immune response overall; however, men are more likely to develop the “cytokine storm associated with poor outcomes against COVID-19. Further research on immuno-modulation by sex hormones, age and X-linked gene expression could help explain the poorer survival of men and identify sex-specific risk factors for SARS-CoV-2 infection and the course, outcome and prognosis of COVID.
Current Treatment of COVID-19
Despite advances in the deterioration of the COVID-19 patient population, there is no approved drug that has considerable beneficial effects in the medical treatment of COVID-19 patients. Hydroxychloroquine was the first drug of choice for the treatment of the disease, but today it is being rejected because of its ineffectiveness and because in some cases it has aggravated the condition of the treated patient. At present, umifenovir, remdesivir and favipiravir are thought to be the most promising antiviral agents for improving the health of infected patients. Dexamethasone is being considered as the first known steroid drug that can save the lives of critically ill patients, as it was shown in a randomized clinical trial in the UK to reduce the death rate in patients with COVID-19. However, despite its increased use worldwide it is not a truly effective treatment over the current high mortality rate in severe cases.
Based on the evidence, the US Food and Drug Administration (FDA) approved some drugs that had already been used in the treatment of SARC-CoV and MERC-COV. The primary treatment chosen for COVID-19, lopinavir, is an antiretroviral (ARV) drug used for the treatment of HIV-1 and has been used for COVID- 19 in combination with ritonavir (potent anti-HIV drug). Currently, 64 clinical trials are underway with lopinavir-ritonavir along with other drug implications, and most of them are in the early stage of progress. The latest evidence for the management of COVID-19 will be uncovered shortly. No single drug may be superior or inferior, however, the use of a single drug may not be effective enough to control this deadly virus, considering PK and drug metabolism, the use of a combination of antivirals with different mechanisms of action may be more effective [83].
Antiviral Agents Used to Date
Remdesivir
Remdesivir (GS-5734) was developed by Gilead Sciences (Foster City, CA, USA). It is an adenosine triphosphate analog and has been used to treat coronavirus and Ebola virus. Remdesivir stops viral replication by inhibiting essential replication enzymes (RNA-dependent RNA polymerase). Currently, more than 24 clinical trials are underway in patients with COVID-19 [84].
Favipiravir
Favipiravir directly inhibits viral transcription by inhibiting RNA polymerase. Currently, 18 clinical trials in various stages of development are underway for the treatment of COVID-A Phase 3 clinical trial has recently been initiated in India, and full study results are expected to be published soon. Clearance for the clinical trial phase evaluation for the safety and efficacy of favipiravir in tablet form has been granted to Appili Therapeutics to monitor COVID-19 in long-term care services [85].
Lopinavir/ritonavir
Lopinavir (Kaletra) is a potent anti-HIV drug used to treat HIV infection in combination with ritonavir. Ritonavir inhibits the pharmacological metabolism of lopinavir to improve PK (half-life) and activity. The Infectious Diseases Society of America (IDSA) recommended ritonavir-boosted combination therapy for HCV patients as first-line therapy. Lopinavir / ritonavir have shown anti-SARS-CoV-2 activity “in vitro” by inhibiting protease in Vero E6 cells [86]. In addition, SARS patients revealed that lopinavirritonavir plays an important role in explaining clinical outcomes and in combination with IFN improved clinical outcomes in some MERS patients [87]. In India, the EMR division has recommended the dosing schedule of this drug combination for the clinical management of COVID-19.
Ribavirin
Ribavirin is a broad-spectrum antiviral drug developed by Bausch Health Companies (Bridgewater Township, New Jersey, USA). It is a guanosine analog used to treat several viral diseases. It showed a lower risk of death in ARDS (acute respiratory distress syndrome) infection in combination with lopinavir- ritonavir. In recent “in vitro” studies, ribavirin showed high efficacy against COVID-19; however, in other studies rivavirin showed an unexpected adverse effect, which was very detrimental to some patients with SARS. [88-89].
Umifenovir
Umifenovir, also known as Arbidolâ , is a broad-spectrum antiviral agent developed by the Russian Institute of Chemical and Pharmaceutical Research. Lopinavir-ritonavir and umifenovir were previously used to treat acute SARC-CoV in clinical practice; however, their efficacy remains debated. The clinical safety and efficacy of umifenovir monotherapy were analyzed in patients with COVID-19 and compared with lopinavir-ritonavir therapy. Umifenovir was found to be better than lopinavir-ritonavir for the treatment of COVID-19 [90]. This drug has obtained approval to proceed with the phase III clinical trial of umifenovir. This randomized, double-blind, placebo-controlled trial will test the efficacy, safety and tolerability of umifenovir. Results are expected to be reported soon [83].
Nitazoxanide
Nitazoxanide inhibits viral infection by potentiating the hostspecific mechanism. Although the “in vitro” activity of nitazoxanide against SARC-CoV-2 suggests that it is effective, more clinical data are needed to estimate efficacy and safety against CO-VID-19 [91]. Currently, many clinical trials of nitazoxanide are underway with various doses to treat patients with COVID-19. 969Although the results are not encouraging or available yet, the FDA has given approval to Azidus Brazil for nitazoxanide to continue with the Phase II clinical trial.
Ivermectin
Ivermectin, an FDA-approved antiparasitic agent as effective as Albendazoleâ, has shown activity against many viruses. Recently, an in vitro study has shown that ivermectin inhibits COVID-19 replication. Its antiviral activity may play a key role and be a potential candidate to treat COVID-19. Finally, the FDA announced a statement for the administration of ivermectin in patients with COVID-19 [92].
Interferons
Interferon (IFN) is a broad-spectrum antiviral agent that inhibits viral replication by interacting with the toll-like receptor (TLR Type III IFNs (IFN-λs) were identified in 2003 and were independently used to elicit antiviral resistances in cells. One member of this family (IFN-λ) [93] was shown to be effective in 2013. IFNs of this type have been used to treat patients critically ill with chronic hepatitis C virus and have also been effective in treating people infected with hepatitis B virus, so they are believed to have the ability to protect patients during outbreaks of other viruses. IFN-λ has also been shown to be more efficacious compared to IFNα-based therapies, also leading to less increase in inflammation and tissue damage, and potentially restricted viral spread from the nasal epithelium to the upper respiratory tract. Moreover, IFNα and β exhibited activity against SARS-CoV “in vitro”. IFNβ also showed potential action to decrease MERS-CoV replication. For the most part, type I IFN showed a rapid decrease in viral load in patients with mild or moderate COVID-19. In severe COVID- 19 infection, IFN showed an antiviral response, but with elevated pulmonary cytokine levels, and weakened T-cell response and acute clinical relapse [94].
Dexamethasone
The main synthetic glucocorticoids: dexamethasone, triancinolone and prednisone are used as immunosuppressants, but their therapeutic indications also include their anti-inflammatory action, and because of their qualities as anti-lymphocyte cytostatics they are used in oncology and in the treatment of allergic diseases. The immunological effects of these drugs are multiple and differ between experimental animals (rodents) and man. In man there is, within a few hours of administration, an increase in neutrophils and a decrease in all other white blood cells in peripheral blood, this decrease being more pronounced for B and T lymphocytes. Although a single dose of glucocorticoids has little effect on B lymphocytes, treatment for several days (3 to 10) may result in a decrease in IgG, IgA and IgM. The FDA approved dexamethasone as a spectrum immunosuppressant in 1958. It is 30 times more potent and longer lasting than cortisone and reduces the ability of B cells to synthesize antibodies [95]. However, a clinical trial showed that dexamethasone saved the lives of severely ill COVID-19-infected patients in the United Kingdom [96]. The UK government declared that dexamethasone was allowed as an immediate treatment option for hospitalized patients who were critically ill and on ventilators. WHO added dexamethasone to the list of life-saving drugs that are readily available at low cost. In the U.S., guidance was issued to recommend dexamethasone as a treatment option for patients infected with CO- VID-19. However, clinical evidence does not support the use of corticosteroids in COVID-19 infection [96]. Dexamethasone may regulate, to some extent, the damaging effects of cytokines by limiting their release, but it has not been shown to be able to inhibit the “cytokine storm”, when the antigen overwhelms the regulatory capacity of the immune response. In addition, dexamethasone prevents macrophages and NK cells from eliminating nosocomial pathogens associated with “coronavirus”.
Tetracyclines
Tetracycline can be used as a possible treatment option for patients with COVID-19 because of its known activity to decrease the level of inflammatory cytokines such as IL-1b and IL-6 [97]. Both IL-1b and IL-6 levels increase significantly in the body of patients during COVID-19 infection. Tetracycline has also been shown to decrease inflammatory factors in the circulation through activation of protein kinase C and induction of programmed cell death [98].
Tocilizumab
Tocilizumab (called Actemra) is a recombinant monoclonal antibody developed by Roche Pharmaceuticals (Basel, Switzerland). Tocilizumab is basically used to treat rheumatoid arthritis. It was designed as an IL-6 receptor blocker to inhibit the binding of IL-6 to its receptor, thus alleviating the “cytokine release” syndrome.
IL-6 is significantly increased in the body of patients when exposed to COVID-19 infection. This is why tocilizumab is used as a therapeutic option for the treatment of patients with COVID-19 [99]. In COVID- 19 infected patients, T lymphocytes and macrophages produce IL-6 and and help the “cytokine storm” and severe inflammatory responses in the lungs and other tissues. Tocilizumab has binding affinity for the IL- 6 receptor and renders the receptor unable to bind IL-6, decreasing the inflammatory response and ultimately decreasing the IL-6 signal transduction pathway [100]. Consequently, it may be essentially an effective therapeutic drug for the treatment of patients with severe COVID-19 infection [101]. The FDA has given Genentech approval to proceed with the Phase III clinical trial of intravenous tocilizumab to evaluate its safety and efficacy in adult patients infected with COVID- 19.
Itolizumab
Itolizumab (called Alzumab) is a recombinant monoclonal antibody against CD6 (IgG1 (Immunoglobulin G1) differentiation group. It was developed for the treatment of psoriatic patients [102]. It showed reduction of IL-6 in critically ill patients. Itolizumab has been shown to have the effect of regulating downstream activation pathways and reduction of inflammatory cytokines, such as IFN-γ, TNF- α and IL-6 [103]. Based on the mode of action, it could be used as a treatment option for COVID-19 infection [103].
Teicoplanin
Teicoplanin (called Targocid) was developed by Sanofi Pharmaceuticals (Paris, France). It is an antiviral drug that can inhibit replication and transcription of the competent virus. It also works against MERS and SARS [104]. Mechanistic investigations revealed that teicoplanin specifically inhibits the activity of host cell cathepsin L and cathepsin B; these proteins are responsible for cleaving the viral glycoprotein, allowing contact of the receptorbinding domain of its core genome and subsequent release into the host cell cytoplasm [105-106]. Since COVID-19 is also “virusdependent” on cathepsin L, some studies suggested that teicoplanin could be used as a therapeutic option to treat COVID-19. According to Ceccarelli, et al. [107], teicoplanin would have a possible therapeutic effect in COVID-19 infected subjects. At present, an in vivo study using teicoplanin in subjects affected by COVID-19 has already been performed for the first time and the results seem quite acceptable compared to a previous report from the same geographical area. Teicoplanin is now thought to be a promising option for the treatment of COVID-19 although more safety data in humans are still required.
Meplazumab
Meplazumab is a humanized monoclonal antibody that acts against the CD147 spike protein. In in vitro studies, it has been shown to effectively inhibit virus replication in Vero E6 cells [108]. Based on this evidence, a study has been conducted to determine the clinical outcomes with the use of meplazumab in treating patients infected with COVID-19. Meplazumab was previously reported to exhibit activity against “Chauge-Strauss syndrome” (characterized by eosinophilic vasculitis, pulmonary infiltration, sinusitis, neuropathy and asthma) [109].
The Phase I clinical trial (NCT0436369586) in healthy volunteers with maplazumab injection is currently being completed to find the safety, efficacy, tolerability, pharmacokinetic characteristics and dosing regimen for the Phase II clinical trial. In the U.S., an openlabel Phase I and Phase II clinical trial is underway to determine the safety and efficacy of meplazumab injection in patients infected with COVID- 19 (NCT04275245). Meplazumab could be used as a therapeutic option to treat patients with COVID-19.
Eculizumab
Eculizumab (Soliris, Alexion Pharma International, Zürich, Switzerland), a human monoclonal antibody, is a highly selective and effective C5-binding protein of the complement system with high affinity. It prevents cleavage to C5a and C5b and inhibits the production of the membrane attack complex (MAC) C5b- 9 to lyse cells. Interestingly, blockade of C5 reveals an indirect “immunoprotective” action by preserving early components of the complement system [110]. Consequently, eculizumab could function as an emergency therapy to treat patients with CO-VID-19 associated with SARS. Some studies have supported the use of eculizumab as a treatment for severe COVID-19. In addition, more clinical trials are approved, some already completed, studying the action of eculizumab in combination with ruxolitinib for efficacy in patients with severe COVID-19 [111].
AMY101
AMY101 is a highly selective inhibitor of the C3 fraction of the complement system that was developed by Amyndas Pharmaceuticals). AMY101 has successfully completed clinical phase I with acceptable safety and tolerability and is now in phase II clinical trial (NCT04395456) AMY101 could be a unique therapeutic option to overcome the complement-mediated inflammatory response in patients with COVID-19 [112-113].
ARDS-003
Cannabinoid (CBD) is also a potential treatment for patients with severe COVID-19. It was designed as an injectable form to treat a severe case of coronavirus with “acute respiratory distress syndrome” It may have the advantage of affecting several proinflammatory signaling pathways by enhancing the effectiveness of the drug to rapidly dampen cytokine release and prevent acute ARDS outcomes [114]. The cannabinoid drug named “ARDS-003” has been approved for a Phase I clinical trial, which is still being conducted by Tetra Bio-Pharma. Initially, the FDA emphasized that the results of the non-clinical studies were appropriate to begin the study in COVID-19 infected patients.
LCB1
CB1 has been shown to be the “SARS-CoV-2 neutralizing antibody”. It is a computer-engineered mini- protein that has been synthesized by researchers at the University of Washington School of Medicine. It binds tightly to SARS-CoV-2 spike proteins and prevents it from infecting cells. “LCB1” was shown to protect “Vero E6” cells from SARS-CoV-2 infection. Synthetic antiviral candidates were designed to stop infection by interfering with the mechanism used by the coronavirus to penetrate and enter cells. LCB1 is currently being evaluated in rodents [115]. These “hyperstable mini-agglutinants” provide a starting point for the most novel COVID-19) therapeutics.
Convalescent plasma
Convalescent plasma therapy has potential to cure COVID-19 (145). Clinical data are very limited to date, but suggest that it is safe, clinically effective, and reduces mortality. However, there is an urgent need for “multicenter clinical trial” studies to establish its efficacy in patients with COVID-19. The U.S. FDA has issued an “emergency use” clearance for “convalescent plasma”, currently under investigation, for the treatment of patients with COVID-19. In addition, polyclonal antibodies from convalescent individuals and immunoglobulin concentrates (human and bovine) may also be of interest in the treatment of COVID-19, at this moment a Spanish company is working on it.
Vaccine development
Coronaviruses are a family of single-stranded RNA viruses that infect many animal species, including bats and humans. Prior to 2003, only twelve animal or human coronaviruses were identified. In the last eighteen years, three new and deadly strains have spread to humans. In 2003, the severe acute respiratory syndrome coronavirus (SARS-CoV) had an official number of 8096 cases and 774 deaths, with people with pre- existing conditions suffering the highest mortality. The overall effect of COVID-19 vaccine development has been a massive invigoration of the field of pandemic vaccine development. The current vaccines are realizing the theoretical promise of antigen sequence-only platforms, such as mRNA and vector-based platforms, and have massively accelerated their development toward rapid “Phase 3 vaccination against COVID-19” evaluation in a timeframe never seen before for vaccines. However, it is important to note that, despite their rapid manufacturing timeline, these platforms encode an antigen that was developed over a timeline of many years through basic research on coronavirus biology and protein engineering. Largescale investment and unprecedented mobilization of the research community have generated insights into the design, manufacture, formulation, and deployment of candidate vaccines that may pay dividends in the future when society must cope with the next inevitable infectious disease outbreak [116-117,83].
Herbal Medicines
In China, during the COVID-19 outbreak, some traditional medicines were used, such as Astragali Radix (Huangqi), Saposhnikoviae Radix (Fangfeng), Glycyrrhizae Radix et Rhizoma (Gancao), Atractylodis Macrocephalae Rhizoma (Baizhu) [118]. Some cannabinoid products were also used [119]. As a treatment option to control the inflammatory response medicinal plants with proven antiviral effects and related beneficial effects could be considered as an alternative approach to prevent high-risk population from COVID-19. However, there are no randomized studies to know the true efficacy and side effects of these natural products obtained from plants. Currently, other researchers, and ourselves, are focusing our attention on the acute and systemic inflammatory process that leads to the activation of “damageassociated molecular patterns” (DAMPs), as well as the study of substances capable of preventing or decreasing cell damage by “suppressing/inhibiting DAMPs” (SAMPs), leading to the resolution of the “inflammatory disease”.
Authors such as Land WG (Laboratory of Excellence Transplantex, University of Strasbourg, Strasbourg, France and German Academy for Transplantation Medicine), think that current or future therapeutics will include the inhibition of “DAMPs” in hyper-inflammatory processes, e.g., “systemic inflammatory response syndrome” (SIRS), which is currently observed in Covid-19, as well as the application of “SAMPs” in chronic inflammatory diseases, in “hyperresolution” processes, systemic inflammatory response syndrome” (SIRS), currently observed in Covid-19, as well as the application of “SAMPs” in chronic inflammatory diseases, in “hyper-resolving” processes (e.g. compensatory anti-inflammatory response syndrome) and in the administration of “SAMPs” in the treatment of chronic inflammatory diseases. We are in full agreement with this author that controlled production of “DAMPs” and “SAMPs” is necessary to achieve complete homeostatic restoration and repair of tissue injury and tissue damage. On the other hand, we fully agree with this author that a controlled production of “DAMPs” and “SAMPs” is necessary to achieve complete homeostatic restoration and repair of tissue injury, and also with the need to identify and define “a priori” a context-dependent “homeostatic DAMPs/ SAMPs ratio” in each case and a “homeostatic window” of DAMP, and SAMP concentrations, to ensure a safe treatment modality in patients [120]. In this aspect, our research group has recently published the work: “Implant of mesenchymal cells decreases acute cellular rejection in small bowel transplantation”[121]in which the inhibition of acute cell-mediated rejection is observed in an experimental model of allogeneic small intestine transplantation, through the implantation of mesenchymal cells and the activation of the “immune-regulatory response”, with an increase in the percentage of Treg cells, a significant increase in TGFb-1 and a decrease in IL-17. This finding will serve as the basis for the project: “Treatment of coronavirus-19 infection using nonsteroidal immunomodulators”, where the DAMPs will be the proinflammatory cytokines and the SAMPs will be the “anti-IL17” and “TGF-β1” molecules.
TGF- β1
As we have described above, the “pathway of regulation of the immune response” exerts its role by responding to the needs of the immune response, at a given moment, against the corresponding antigen, increasing the inflammatory activity of the Th1 pathway, mainly by means of Th17 cells and IL-17A, or increasing the antiinflammatory activity of the Th2 pathway, mainly by means of the “transforming growth factor β” (TGF-β). In the scheme shown on page 7 of this paper, we can see that this factor already acts from the “immune-regulatory pathway” and is part of the “anti-inflammatory pathway”, tipping the balance towards this second pathway. In our previously cited work on the inhibition of acute cell-mediated rejection in intestinal transplantation, “TGFb-1” is shown to be the most important factor, in relation to the other cytokines studied, acting as an inhibitor of the inflammatory immune response in rejection. In 2000, the Canadian researchers Prud’homme GJ and Piccirillo CA already pointed out that the importance of the factor “TGF-β” in “immuno-regulation” and tolerance had been recognized once again [122].
Like us, the authors propose that there are regulatory T-cell (T-reg) populations, some called T-helper type 3 (Th3), exert their action mainly by secreting this cytokine, and furthermore these authors emphasize the following concepts: 1) TGF-β1 has multiple suppressive actions on T cells, B cells, macrophages and other cells, and increased TGF-β1 production correlates with protection and/ or recovery from autoimmune diseases; 2) TGF-β1 and CTLA-4 are molecules that work together to terminate immune responses; 3) Th0, Th1 and Th2 clones can secrete TGF-β1 following CTLA-4 cross-linking; 4) TGF-β1 may play a role in the switch from effector T cells to memory T cells; 5) TGF-β1 acts with some other inhibitory molecules to maintain a state of tolerance, which is most evident in immunologically privileged sites, but may also be important in other organs; 6) TGF-β1 is produced by many cell types, is always present in plasma (in its latent form) and permeates all organs, binding to matrix components and creating a reservoir of this immunosuppressive molecule; and 7) TGF-β1 has beneficial effects in several autoimmune diseases and shows that it can be effectively administered by a somatic gene therapy approach, resulting in depressed inflammatory cytokine production and increased production of endogenous regulatory cytokines.
Currently, March 2021, Aydemir MN, et al. [123] have published an interesting paper. The authors believe that despite the information obtained on the structure of the SARS-CoV-2 viral genome, many aspects of virus-host interactions during infection are still unknown; their purpose in this study has been to identify the “microRNAs” (“miRNAs”) encoded by SARS-CoV- 2” and their cellular targets. The authors have employed for this purpose a computational method to predict SARS-CoV-2-encoded miRNAs along with their putative targets in humans. The predicted miRNA targets were grouped into clusters according to their biological processes, molecular function and cellular compartments. Aydemir MN, et al. note that the “TGF-β1 pathway” has important functions in many cellular processes, and that it is often manipulated by viruses, as it is a simple pathway. The authors expose that proteins that play a crucial role in almost all steps of this pathway are targeted by SARS-CoV-2 miRNAs and demonstrate that the SARS-CoV “nucleocapsid protein” (“N”) inhibits the formation of the “SMAD” complex (family of inducing genes of this pathway), resulting in blocking TGF-β1-induced apoptosis of Cov-2-infected cells and, conversely, tissue fibrosis in SARS-CoV-infected “host cells” [124]. Finally, these authors performed an integrative pathway network analysis with target genes and identified 40 SARS-CoV-2 miRNAs and their regulated targets, the analysis shows that the targeted genes including NFKB1, NFKBIE, JAK1-2, STAT3-4, STAT5B, STAT6, SOCS1-6, IL2, IL8, IL10, IL17, TGFBR1-2, SMAD2-4, HDAC1-6 and JARID1A-C , JARID2 plays an important role in NFKB, JAK/STAT and TGFB signaling pathways as well as epigenetic regulatory pathways in cells and they believe that their results may help to understand the virus-host interaction and the role of viral miRNAs during SARS-CoV-2 infection. Since there is currently no drug or effective treatment available for COVID19, it may also help to develop new treatment strategies.
Monoclonal Antibody Against Il-17
COVID-19 is caused by SARS-CoV-2, a “beta-coronavirus” closely related to MERS-CoV and SARS- CoV, the causative agents of “Middle East respiratory syndrome (MERS)” and “severe acute respiratory syndrome” (SARS), respectively. COVID-19 appears to follow a similar pattern, with 81% of fatal cases diagnosed with SARS (2). In consideration of this, a recent publication in The Lancet [125] suggests that all patients with COVID-19 should be evaluated for “hyper-inflammation” in order to identify those who would benefit from targeted immunosuppression or immunomodulation to prevent acute lung disease. (“ALI”) (acute lung injury) [126]. IL-17 (formally IL-17A) is the best known member of a family of multifunctional cytokines. Its predominant role seems to depend on where the cytokine is expressed (gut, lung or skin) and what the trigger is. These two factors appear to influence whether the predominant effect of its expression is protective or whether it leads to a detrimental hyper-inflammatory state. For MERS-CoV, SARS-CoV and SARS-CoV-2, disease severity was shown to correlate positively with levels of IL-17 and other T helper 17 (Th17) cellrelated pro-inflammatory cytokines, such as IL-1, IL-6, IL-15, TNF and IFNγ. (see page 7 of this paper) Increased IL-17 levels in LPS-induced “ALI” (“acute lung injury”) mice correlated with increased lung injury scores, increased protein-rich inflammatory lung infiltration and decreased overall survival. Furthermore, the addition of exogenous IL- 17 further exacerbated LPS-induced production of TNF, IL-1β, IL-6 and CXCL2, revealing the role of IL- 17 as a key principal modulator of the inflammatory pathway. In the same study, mice genetically deficient in IL-17 or those that received anti-IL-17 antibodies demonstrated improved survival, less pulmonary infiltration, and improved lung pathology scores after LPS exposure [127] Taken together, analyses of patients with coronavirus-induced lung disease suggest that IL-17 may serve as a biomarker (“DAMP”) of disease severity and a potential target for therapy to mitigate SARS-CoV-2 damage, particularly in the lung. Of note, COVID-19 mortality is also associated with myocarditis in the context of SARS.
Zhao Y, et al. [128] in a very recent paper (February 2021) propose a model to understand the underlying mechanisms involved in lung pathology by investigating the role of the lungspecific immune response. The authors obtain immune cells in bronchoalveolar lavage fluid and in blood drawn from patients with COVID-19 with severe disease and patients with bacterial pneumonia not associated with viral infection. By tracing T-cell clones across tissues, they identify Th17 cells similar to clonally expanded “memory T cells” resident in lung tissue, which they term “Trm17 cells” and which reside in the lungs even after viral clearance. Analysis of the lung suggests that Trm17 cells may interact with lung macrophages and Tc/s (CD8+ cytotoxic) cells, and is associated with disease severity and lung damage. Ultimately, elevated serum IL-17A and GM-CSF protein levels in patients with COVID- 19 are associated with a more severe clinical course. Zhao Y, et al. suggest that lung Trm17 cells are a potential orchestrator of hyperinflammation in severe COVID-19. On the other hand, Trm17 cells become activated or reactivated as part of the ongoing cytokine storm, during which they may begin to produce pro-inflammatory cytokines such as GM-CSF. This could lead to increased activation of macrophages and cytotoxic CD8+ cells, which other authors have linked to disease severity and ultimately mediate lethal lung damage [42,45].
As related by Zhao Y, et al. To date there have been 2 small pilot studies that have indicated that targeting GM-CSF in patients with severe lung disease by COVID-19 using anti-GM-CSF receptor monoclonal antibodies mavrilimumab or lenzilumab, respectively, may be a strategy to improve clinical outcomes [3,4], although larger controlled clinical trials would be needed to determine the efficacy and biological impact of such approaches. This network of tissue-resident cells may persist in the lungs even after the initiating event, e.g., a viral infection, has been eliminated, contributing to chronic lung pathology. There are three commercially available options: secuquinumab (human monoclonal antibody against IL- 17), ixeki-zumab (humanized monoclonal antibody against IL-17) and brodalumab (human monoclonal antibody against the IL-17 receptor). Both secukinumab and ixekizumab are approved for psoriasis, psoriatic arthritis and ankylosing spondylitis; brodalumab is approved for the treatment of psoriasis alone. All three of these drugs come with warnings about an increased risk of infections. Compared to placebo, clinical trials showed a moderate increase in upper respiratory tract infections (“URIs”) for patients treated with secukinumab and a similar number of URIs for patients treated with ixekizumab, while treatment with brodalumab resulted in a lower rate of “URIs.” The risk of serious infections is unchanged or low in the short term. Therefore, the use of these drugs in the acute setting of COVID- 19 should not lead to an increased risk of secondary infections.
“NSAIDs” (Non-Steroidal Anti-Inflammatory Drugs)
Nonsteroidal anti-inflammatory drugs (NSAIDs) are a group of often chemically unrelated compounds that have potent antiinflammatory, analgesic and antipyretic activity and are among the most widely used drugs worldwide. It is generally thought that one of their main mechanisms of action is the inhibition of cyclooxygenase (COX), the enzyme responsible for the biosynthesis of prostaglandins (PGs) and thromboxane. NSAIDs are also associated with an increased risk of gastrointestinal, renal and cardiovascular adverse effects.
The review paper by Bacchi S et al., [129] describes the clinical pharmacology of “NSAIDs, their classification, molecular mechanisms of action and adverse effects, including their possible contribution to “neuro-inflammation” and carcinogenesis, as well as some recent developments aimed at designing effective antiinflammatory agents with improved safety and tolerability profiles. In the late 1980s, it was discovered that COX has two isoforms, each produced by a different gene. The COX-1 gene is located on chromosome 9 and functions as an internal gene that regulates numerous cellular functions, including the complex series of processes responsible for protecting the gastrointestinal mucosa from ulceration. The COX-2 gene, located on chromosome 1, is an early and immediately activated gene and is rapidly deregulated in response to a variety of inflammatory cytokines and cellular injury.
The COX-1 enzyme produces the prostaglandins responsible for gastrointestinal cytoprotection and platelet function, while the COX-2 enzyme produces the reactions responsible for pain perception and inflammation. Thus, COX-1 and CoX-2 enzymes can produce both beneficial and adverse effects due to inhibition of prostanoids, derived from arachidonic acid (AA), which is converted to prostaglandin G2 (PGG2) and H2 (PGH2) as a result of cyclooxygenase (COX) activity, and PGH2 is subsequently metabolized by terminal synthases into biologically active prostanoids. COX-2 expression is greatly restricted under basal conditions, but is greatly increased at inflammatory sites in response to cytokines such as interferon-gTNFa, IL-1, hormones, growth factors, and hypoxia. The pharmacological effects of NSAIDs are due to blockade of COX and consequent reduction of PG synthesis, leading to a decrease in inflammation, pain and fever. The anti-inflammatory action of “NSAIDs” is due to the decrease of vasodilator PGs (PGE2, PGI2), which indirectly reduces edema.
Within the group of non-steroidal anti-inflammatory molecules, the group of pyrazolones stands out and among them metamizole (dipyrone). In 2014, the research group of Jasiecka A et al, [130] published a paper on the pharmacological characteristics of “metamizole”: a popular, non-opioid analgesic drug commonly used in human and veterinary medicine. In some cases, this agent is still incorrectly classified as a non-steroidal anti-inflammatory drug. Metamizole is a “pro-drug” that spontaneously breaks down after oral administration into structurally related pyrazolone compounds. In addition to its analgesic effect, the drug is an antipyretic and spasmolytic agent. The mechanism responsible for the analgesic effect is complex and most likely based on inhibition of a central cyclooxygenase-3 and activation of the opioidergic and cannabinoid systems. Metamizole can block both PG-dependent and PG-independent LPS-induced fever pathways, suggesting that this drug has a distinctly different antipyretic action profile than the other NSAIDs. The mechanism responsible for the spasmolytic effect of metamizole is associated with inhibition of intracellular Ca2 + as a result of reduced inositol phosphate synthesis [130]. Metamizole is predominantly applied in the therapy of pain of different etiology, spastic conditions, especially affecting the digestive tract, and fever refractory to other treatments. Coadministration of morphine and metamizole produces super-additive anti-nociceptive effects [131]. On the other hand, metamizole is a relatively safe pharmaceutical preparation, although it is not completely free of undesirable effects. Among these side effects, the most serious and most controversial is the myelotoxic effect; however, it seems that in the past the risk of metamizole-induced agranulocytosis was exaggerated [132]. Today it is considered that the side effects of metamizole appear only in long periods of treatment of chronic inflammatory diseases. Our research team has studied the effects of “magnesium metamizole” marketed under the name of Nolotilâ and currently produced by Boehringer Laboratories (Germany).
The active ingredient of this drug is the “methylated oxyquinazine” molecule, whose chemical structure is included here: The complete structure of this synthetic drug corresponds to a phenyl-dimethyl pyrazolone derivative whose “R” root is magnesium methylene sulfonate. Its complete formula is dimethyl oxyquinazine methylene methylamine magnesium sulfonate. Since 1975, we have used this drug in the surgical clinic as an analgesic in the first days of the immediate postoperative period, due to its high analgesic power and also to its anti-adhesiveness and anti-platelet aggregation properties. These findings were obtained in “in vivo” and “in vitro” studies carried out by our research team in the 70’s of the last century. [132-134]. Our results have now been ratified by Pfrepper C et al. in 2019 [135]. It is very important to emphasize here that increased platelet adhesiveness and aggregation leads to initial thrombus formation and eventually to thrombosis. Methylated oxyquinazine by its anti- aggregating and antiadhesive action on platelets may contribute to prevent vascular thrombosis. When “CoV-2 antigens” stimulate macrophages or any other “antigen presenting cell” the “pro- inflammatory” cytokines par excellence are released: IL-1, IL-6, IL-8, IL-15, IL-17, IL-18, TNFs, IFNg and PAF (platelet activating factor) (and source of PF4). Through the release of PAF, the immune response acts on the coagulation and fibrinolytic systems, giving rise to signals that cross and intersect between the immune response and the different systems: coagulation, fibrinolytics, cyanins, arachidonic acid, leukotrienes and thromboxanes, etc. Thus, we believe that methylated oxyquinazine could contribute to inhibit or palliate the immune response overwhelmed by COVID-19 in the most severe stage of Cov-2 disease [42]. (see Figure 2) page 5 of this paper). It has recently been published those vaccines using adenovirus vectors can produce thrombosis by activation of PAF and PF4, resulting in increased platelet aggregation and adhesiveness accompanied by thrombocytopenia [136-143]. In this aspect, methylated oxyquinazine (metamizole) could also serve as a prophylaxis of thrombus formation when these vaccines are given (Figure 4).
Figure 4: The complete structure of this synthetic drug corresponds to a phenyl-dimethyl pyrazolone derivative whose “R” root is magnesium methylene sulfonate. Its complete formula is: dimethyl oxyquinazine methylene methylamine magnesium sulfonate [134-136].
Our research project is aimed at avoiding the “cytokine storm” by means of molecules that do not inhibit the response to the virus but can avoid the excessive inflammatory response, by activating the “immuno-regulatory pathway” of the immune system. The treatments applied to date fail when patients, especially the elderly or “immuno-compromised” people (suffering from severe heart disease, chronic kidney disease, chronic obstructive pulmonary disease, cancer –patients undergoing active treatment–, immunosuppression by transplantation of solid organs, obesity or type 2 diabetes mellitus, or elderly people who also suffer from any of these diseases, reach the most serious stage of the disease, and their body is not capable of avoiding the “cytokine storm” and the multi-organic failure that leads inexorably to death.
How COVID-19 Pandemic Indirectly Affected Orthopedic Patients: A Case Report of a Rescue Treatment For a Proximal Humerus Nonunion
Introduction
Humeral fractures account for 5% to 8% of all fractures, whereas proximal humerus fractures represent the seventh most frequent fractures in adults [1,2]. Nonunion is a complication that occurs in 15% of all the humeral fractures [3] and its incidence increases in case of proximal humerus fracture [4]. Risk factors are advanced age, osteoporosis, obesity, smoking, alcoholism, and infection. Comminution and impaction of fractures and loss of fixation also contribute to the develop of nonunion [5,6]. This condition results in pain and loss of shoulder function. The management of proximal humerus nonunion is challenging and often the results are disappointing. Treatment of these kind of complications include open reduction and internal fixation with bone grafting but often it is an unsuccessful treatment resulting in bad clinical outcomes and further surgery is required. Other options are fixation with tension wires or with intramedullary nail [7].
These are optimal options for bone of good quality such as in young patients and with no signs of gleno-humeral arthritis. Shoulder arthroplasty is a reasonable option in case of proximal humerus nonunion associated with a rotator cuff damage and osteoporosis [8]. This case-report describes a proximal humeral nonunion in a 69-year-old woman who was first treated with an external fixation before the advent of COVID-19 pandemic. After removing the external fixator (EF), she was lost at follow-up because of the closure of our department during the Italian lockdown. She came back after seven months with pain and functional limitation. X-Ray reported a nonunion of proximal humerus. In the end she underwent to reverse shoulder arthroplasty, recovering with a good result.
Case Report
A 69-year-old woman came to ER of Poliambulanza of Brescia in October 2019. X-rays were obtained. Fracture involved proximal humerus of the right, dominant, upper arm. The fracture was 11C3.1 according to AO classification. At first, the fracture was treated with an external. fixation using a Galaxy EF in the first twenty-four hours. The EF was removed after one month because of the loss of reduction with displacement of the fracture. Physio- kinesitherapy was indicated but she was unable to underwent to treatment. She was lost at follow -up for several months due to COVID-19 pandemic and the social limitations that resulted. After 7 months, Xrays showed a dislocated nonunion of proximal humerus with necrosis of the head. She complained shoulder pain with passive elevation of 40° and scapular dyskinesia. In March 2021 she was listed for a reverse shoulder arthroplasty. During the surgery, Synovasure test and white blood cell count were performed: both tested negatives. A cemented trauma stem “Equinoxe” by Exactech number 8 mm was applied with a standard baseplate fixed with three screws of 26, 18, 18 mm. External rotators were reinserted, and range of motion (ROM) was good at three months follow-up.
Discussion
The impact of COVID-19-related restrictions has resulted in changes in patients’ healthcare and follow-up. During the pandemic, injured patients have experienced difficulties in receiving medical assistance, due to the lack of healthcare personnel and fear of contagion. Lombardy was the most affected region of Italy and orthopedic surgeons were involved in the emergency as other specialists [9,10]. Our level-2-trauma center in Brescia (Lombardy) went on admitting injured patients unceasingly, since several domestic accidents happened during that time, despite reports out of Italy noted a 65% reduction in trauma services provided for shoulder and elbow injuries during the time residents were asked to stay in the home [11]. One of the effects of the pandemic was the loss of follow-up of outpatients [12]. It is hypothesized that the main causes of this issue were the isolation and the fear of contagion in hospital environment [10] (Figure 1).
Figure 1: First radiograph showing comminuted and dislocated fracture.
Figure 2: First treatment with EF.
Figure 3: Partial loss of reduction after the removal of the EF.
Figure 4: Nonunion and dislocation at 7 months after trauma.
Figure 5: Final treatment.
Figure 6: Range of motion at 3 months after arthroplasty.
Radiographic checks showed a partial loss of reduction and physio-kinesitherapy was indicated but she was unable to underwent to treatment because of the new social restrictions. Further radiographs showed gradual loss of reduction. Therefore, we started contemplating a definitive treatment by performing a ORIF with bone graft or a shoulder arthroplasty, but at that moment, the patient was lost at follow-up. Given the poor bone quality, after the removal of the EF, we would probably have implanted a hemiarthroplasty or a reverse prosthesis with a press-fit primary humeral stem fixation, considered an optimal choice because of the possible easier revision, decreased operative time, healing time, and resolution of the symptoms [16]. After 7 months, the patient came back to our department, suffering from pain and severe functional limitation, compounded by a preternatural movement of the joint. Radiographs showed evident dislocated nonunion with reabsorption of tuberosities and metaphysis.
Therefore, our choice has been to implant a reverse shoulder prosthesis with a cemented trauma stem “Equinoxe” by Exactech number 8 mm. This choice involved several compromises like technical difficulties due to the severe bone loss and higher risks of dislocations, infections, nerve injuries and thromboembolism due to the use of cement, compared to an arthroplasty with a pressfit stem [17-20]. At three-month follow-up, the patient showed no pain and a sufficient function of the joint. Since the exact amount of loss to follow-up is not valuable, there is a chance that cases of nonunion in longstanding fractures like this could increase in the near future. Our experience shows that cemented stem fixation can be an important choice of treatment for these patients. Other strategies, like telemedicine, should be considered and eventually implemented to prevent this kind of consequences resulting from the pandemic [21-23].
Duststorms and sandstorms are natural meteorological phenomena and severe weather condition frequently occurring in arid and semi-arid regions mainly during summer season when these regions are subjected to strong winds; and driven by different factors: availability and nature of source sediments, vegetation cover density, prevailing climatic conditions, and the textural characteristics of the surface deposits, environmental, geomorphological and relief variation factors. One of the major terrestrial sources of moving sand worldwide is the Arabian peninsula and Sahara desert, while minor sources come from Iran, Pakistan, and India which deposit dust in the Arabian sea, and from China depositing dust in the Pacific. According to [1], the recent surface deposits are the major source of duststorms in Kuwait which are potentially originated from: 1) Dry sabkhas muddy sediments in the lower Mesopotamian flood plain; 2) Old sandstone, limestone and dolostone sediments exposed in the western desert of Iraq; 3) Dibdibba Formation Paraconglomeratic sediments exposed in southern Iraq and northern Kuwait; and 4) Air locally picked up particles from playa, sabkhas, and finegrained mobile sand. Duststorms winds have variant local nomenclature. In Sahara desert they are named as Simoom, in some Africa Arabian countries like Egypt, Libya, Sudan, Morocco, and Tunisia, they are named Khamasine, Ghibli, Haboob, Sahel and Chili, respectively, while in Asian areas like India and the Arabian Gulf region they are named Loo and Shamal or Toze, respectively [2]. A duststorm is distinguished from a sandstorm on the basis of particle size. Dust storms are made up of a multitude of very fine particles while sandstorms have larger particle sizes that range from .08mm to 1mm [3]. The fine “dust” particles may be elevated as high as 3km or more while the “sand” particles are confined to the lowest 3.5m, rarely rise more than 15m above the ground. The term sandstorm is oftenly used in desert sandstorms context, especially in the Sahara Desert, or places where sand is a more prevalent soil type than dirt or rock, when, in addition to fine particles obscuring visibility, a considerable amount of larger sand particles are blown closer to the surface. The term duststorm is more likely to be used when finer particles are blown long distances, especially when the duststorm affects urban areas. A sandstorm can transport and carry large volumes of sand unexpectedly. Dust storms can carry large amounts of dust, with the leading edge being composed of a wall of thick dust as much as 1.6 km (0.99 mi) high. In desert areas, dust and sand storms are most commonly caused by either thunderstorm outflows, or by strong pressure gradients which cause an increase in wind velocity over a wide area. Drought and wind contribute to the emergence of dust storms, as do poor farming (e.g., dryland farming techniques) and grazing practices by exposing the dust and sand to the wind. In addition to the environmental factors including: wind speed, atmospheric stability, source region surface characteristics, surface heating, soil moisture, soil type and surface vegetation. Moreover, in Kuwait human activities in the desert contribute to duststorms occurrence including: extensive motor car movements, extensive urban development, environmentally uncontrolled quarrying activities, and overgrazing by cattle throughout the year. In Kuwait duststorms are more frequent during the Spring and Summer due to: 1) The dry fresh (15-24 m/s) northwesterly winds blowing from Iraq and local lands [4]; 2) The deserts surrounding Kuwait: Iraqi desert from N-NW and Saudi Arabian from W-S; 3) The loose sediments covering most of the surface area [5]. There are 3 types of dust in Kuwait [6,7]. Duststorms (wind speed ≈18 knots (33.336 km/h), horizontal visibility is <1 km (if < 200 m it is called a severe duststorm)); 2) Rising dust (wind speed is moderate, horizontal visibility is ≥ 1 km); and 3) Suspended dust (horizontal visibility is < 1 km but with moderate wind speed (6-14 m/s) it is in the range of 1-5 km). Dust and sandstorms may have impacts in different aspects; physical, environmental, economic, social, human health … etc. As physical and environmental sandstorm can possess a huge power that it can move whole sand dunes; Duststorms and suspended dust can reduce visibility to < 200 m; dust may block roads, damage materials and equipment and affect transportation and severely pollute the air. Dust particles can reflect and absorb solar radiation causing radioactive effect as they are tropospheric aerosols a significant component of the earth’s climatic system changing climate by their direct radiative scattering and absorption [8], and indirectly by their radiative effects through affecting on clouds microphysics [9] and affecting the processes of atmospheric chemistry. Dust can remarkably affect the soil characteristics, ocean productivity, and air chemistry by influencing the nutrient dynamics and biogeochemical cycling of ecosystems. Economically, duststorms lead to soil loss, which, in turn, will remove the organic matter and nutrient-rich particles reducing the soil fertility and by abrasion they damage the young crop plants and reduce the crop productivity. Moreover, duststorms reduce visibility affecting aircrafts and road transportation, that would have consequences of financial and human lives loss. Duststorms reduce the amount of sunlight that reaches the surface, and hence cause critical complications on plants photosynthesis and productivity and reduce the livestock forage. Increased clouds of dust and sandstorms can affect the ecosystem stability by increasing the heat blanket effect. Socially wise, by reduction of livestock forage, ecosystem biodiversity and increase hunger, water availability and farmland yields, the land resources will be lost which result in turn will spread poverty, the spread of poverty and hunger will increase, which eventually will result in migration in search of food and relief, and increasing the environmental refugees number that poses pressure on neighborhood areas and leading to enormous social problems. In relation to public health, duststorms have adverse shorttime impacts on the public health including immediate increased symptoms and worsening of the lung function in individuals with asthma, increased mortality and morbidity long-transported duststorm particles adversely affect the circulatory system. Prolonged and unprotected exposure of the respiratory system in a dust storm can also cause silicosis, which, if left untreated, will lead to asphyxiation; silicosis is an incurable condition that may also lead to lung cancer. It was found by [10] that the concentrations of all pollutants (including Particulate Matter (PM10)) in the ambient air of Kuwait in the residential areas is dependent on the meteorological conditions (PM10 and NOx). It was indicated by [11] that in Kuwait duststorms and fossil fuel combustion strongly contribute to the air pollutants (especially (PM)) which play a significant role in determination the symptoms of Rheumatoid Arthritis (RA) disease and worsening it on overall. It was stated by [12] that the chronic and long-term exposure to calcite and quartz particles (the major constituents of dustfallout in Kuwait) may produce alkalosis and hypercalcemia and can have potentially serious respiratory effects. There is also the danger of keratoconjunctivitis sicca (“dry eyes”) which, in severe cases without immediate and proper treatment, can lead to blindness. There are short-term approaches for dust and sand storm control (e.g., forecasting and early warning) and others are long-term (e.g., source area rehabilitation). In general, dust and sand storms can be controlled by applying different kinds of dust suppressants or wind breakers. Such suppressants may include physical covers, e.g., vegetation, aggregate, mulches or paving; and chemical compounds, e.g., water, either fresh, sea water or even reclaimed, especially on construction sites and unpaved roads; calcium and magnesium chloride and petroleum-based chemicals, which can stabilize the soil by absorbing the moisture from the atmosphere. This will change the soil surface physical properties as by applying the suppressant the soil particles will be coated and aggregated together becoming heavy to be airborne particles hence unsusceptible for wind erosion. Controlling the movement and sand encroachment by wind can be done by creating tree windbreakers, reducing ground level wind velocity by inserting straw bundles into the sand in a checkerboard pattern, or using creeping plants. Sand or dust encroachment can also be controlled by rehabilitating and improving the land surface by reducing barren land through reforesting and planting degraded land, and improving the environmental capacity of the soil by introducing water-saving and water management techniques for the efficient use of water and application of farm animal manure.
Keratoacanthoma and Well Differentiated Squamous Cell Carcinoma Have a Distinct Prognosis Running Head: Prognosis of Keratoacanthoma
Introduction
Keratoacanthoma (KA) is a rapidly growing skin tumor thought to originate from the hair follicle [1]. The exact classification of the tumor is still a matter of debate. Due to its ability to spontaneously regress some consider KA a benign lesion [2]. However, KA can also display perineural as well as venous invasion [3,4] and cases of metastatic KA were also reported [5,6] suggesting the classification as a subtype of well differentiated SCC is more appropriate. On a molecular level, the etiology of KA and Squamous Cell Carcinoma (SCC) seems to differ, since deletion of polarity proteins in mouse models can rescue SCC formation but promote KA formation [7]. Expression of tumor suppressors and promoters is also different in KA compared to SCC with a gain of 11q and subsequent amplification of the cyclin D1 locus being the most frequent aberration in KA [8]. Mutated p53 is more frequently found in SCC compared to KA and the cell cycle inhibitor p16 is expressed in KA but downregulated in SCC [9]. Additionally, the tumor microenvironment of KA and SCC is different providing a possible explanation for the ability of KA to regress [10].
The therapy of KA usually consists of complete excision since it is impossible to predict whether the tumor will regress or progress to invade the underlying tissue and even metastasize [5,6]. Since current guidelines on SCC do not take the KA histological subtype as a prognostic factor into account the question whether KA has a distinct prognosis compared SCC remains open. This question is particularly relevant since KA often have an increased tumor thickness due to rapid growth and may unnecessarily fall into the category of high risk SCC thereby burdening the financial system with frequent follow-up of these patients. In this study, we compared the prognosis of KA with that of well differentiated SCC without KA histology (wSCC) and found that KA histology favorably impacts metastasis-free survival but not local relapse-free survival.
Patients and Methods
A retrospective analysis of medical records of the Department of Dermatology, University Hospital of Cologne identified 403 KA and 905 wSCC. Tumors with an incomplete excision were excluded. The histopathologic criteria for KA were a crateriform tumor surrounding a central keratin plug showing epithelial lipping [1,11]. Solar elastosis was defined as a fibrillary basophilic material in the upper dermis [12]. Immunosuppression was defined as use of chemotherapy, other malignancies than non-melanoma skin cancer and use of immunosuppressive drugs. Diabetes was not considered immunosuppressive. Statistical evaluations were performed with the statistical software package IBM SPSS, version 20.0. Graphs were made using GraphPad Prism, version 5.0. Student’s t test was used with continuous variables, while the X2 test was used for categorical variables. Survival rates were calculated by the Kaplan– Meier method and compared using log-rank tests. A P-value of <0.05 was considered significant.
Results
A total of 403 KA and 905 wSCC were retrospectively analyzed. The median follow-up was 23 months. 8 Patients with KA (2%) developed metastasis after a median of 7 months (range 1-49) and 35 patients with wSCC (3.9%) developed metastasis after a median 8 of months (range 1-37). Except for 2 patients with wSCC, who developed lung metastasis all patients developed metastasis of skin and/or lymph nodes. The metastasis-free survival was significantly decreased in the wSCC groups compared to the KA group (p=0.042) (Figure 1). 9 KA (2.2%) recurred locally following complete excision after a median of 32 months, while after a median of 8 months 24 wSCC (2.7%) recurred locally. The local recurrence-free survival was not significantly different in the KA group compared to the wSCC group (p=0.426) (Figure 1).
Figure 1:
a) Metastasis-free survival in keratoacanthoma compared to well differentiated squamous cell carcinoma (SCC) (p=0.042). b) Local recurrence-free survival in keratoacanthoma compared to well differentiated SCC (p=0.436).
Patients with KA were more likely to be female (40.2% versus 27%, p<0.0001) and to have thicker lesions compared to patients with wSCC (tumor thickness 3.2 vs 2.7, p=0.012) (Table 1). Age was also significantly decreased in KA compared to wSCC (p<0.0001). Furthermore the patterns of tumor localization were different in KA compared to wSCC, with KA occurring more frequently on the lower extremity and to a lesser extent in the head and neck region. Since the difference in tumor location could be explained by sun exposure, we analyzed the presence of solar elastosis in the periphery of tumors and found that solar elastosis occurred more frequently in wSCC compared to KA (82% vs 60.7%, p<0.0001). In contrast, the presence of immunosuppression and tumor diameter was not significantly different in the KA group compared to the wSCC group (Table 1).
Table 1: Clinical data keratoacanthoma compared to well differentiated SCC.
Currently, no specific guideline for the follow-up of patients with KA exists and it is unclear whether the guidelines regarding the follow-up of SCC [13] can also be applied to KA. To our knowledge, this the first study comparing the prognosis of KA with wSCC. We found that the metastasis-free survival was significantly increased in KA compared to wSCC. 2% of KA developed metastasis in the skin and regional lymph node indicating that similar to SCC ultrasound of the regional lymph nodes is also important in patients with KA. Since local recurrence-free survival was not different in KA compared to wSCC we propose to use the same frequency of physical examinations of the skin in KA as in SCC [13]. In line with the hypothesis that SCC and KA have different etiologies our study could show that clinical and pathologic characteristics were also significantly different in the wSCC group compared to KA. As expected from a rapidly growing tumor, the tumor thickness of KA was significantly increased compared to wSCC. Interestingly, patients with KA were more likely to be female and were significantly younger compared to patients with wSCC further underlining the different etiology of the two tumors. In accordance with a previous study [14] we could show that the predominant distribution of KA is on the lower extremity while SCC were mostly localized in the head and neck region. Moreover, the presence of solar elastosis was significantly increased in the KA group suggesting sun exposure plays a more minor role in KA. Consistent with the hypothesis that UV plays a less important role in the etiology of KA the mutation burden of KA is lower compared to cutaneous SCC [15]. Further supporting a different etiology of KA and SCC the rate of HPV DNA detection was higher in KA compared to wSCC suggesting a possible viral etiology in the pathogenesis of KA [16]. This would then imply that immunosuppression would play a more important role in the etiology of KA compared to SCC, however the incidence of immunosuppression was not different in KA compared to the wSCC group in our study, suggesting other etiologic factors such as the tissue microenvironment could play a role.
Conclusion
We could show that KA histology favorably impacts metastasisfree survival but does not influence local relapse-free survival.
Comparison of Three Treatment Methods of Ⅰ-Ⅲ Degree Hemorrhoids: A Meta Analysis
Introduction
Hemorrhoids is a common clinical disease and its pathogenesis is not yet clear. The theory of anal cushion displacement is widely accepted at present, that is, supporting tissue degeneration, including fibrous tissue fragmentation, elastic connective tissue and submucosal muscle fiber weakening, which may be related to lack of dietary fiber, constipation, improper defecation habits and lifestyle. The main clinical manifestations of hemorrhoids are bleeding during defecation, pain, anal prolapse, swelling, pruritus and perianal secretions [1]. Depending on the location of the disease, hemorrhoids can be divided into internal hemorrhoids, external hemorrhoids and mixed (internal and external) hemorrhoids. Internal hemorrhoids are formed by tissue covered by columnar epithelium, and located above the dentate line; External hemorrhoids are formed by tissue covered by squamous epithelium, and located below the dentate [2]. Mixed hemorrhoids appear at the top and bottom of the dentate line. The staging of internal hemorrhoids is not completely unified in the world. Goligher’s classification is more commonly used, which divides internal hemorrhoids into gradeⅠ-Ⅳ.
i. Grade Ⅰ: Bleeding during defecation, but not prolapse, most patients have no obvious symptoms. ii. Grade Ⅱ: The hemorrhoids protrude out of the anus during defecation, and the prolapse can be returned by itself. iii. Grade III: Prolapse out of the anus during defecation, fatigue, long walking, or coughing. After prolapse, internal hemorrhoids cannot be repaid by themselves, and they need to be repaid by hand. iv. Grade Ⅳ: With external hemorrhoids, the hemorrhoids remain outside the anus for a long time and cannot be repaid or prolapse immediately after being repaid. The treatment methods of internal hemorrhoids include non-surgical treatment and surgical treatment. Most internal hemorrhoids of grade I-III can be alleviated by non-surgical treatment such as drug treatment, RBL, IS, and IRC; grade IV internal hemorrhoids, internal hemorrhoids that fail or have complications should undergo surgical treatment [3]. RBL is a simple, quick and effective method for treating patients with grade I-II and part of grade III internal hemorrhoids. The method is to ligate with ligator above the dentate line, and the internal hemorrhoids are necrotic due to blood flow blockade and fall off automatically [4]. IS is an endoscopic or anal endoscopic injection of sclerosis agent into the submucosal layer of internal hemorrhoids, forming fibrosis and scars. IRC is to coagulate the hemorrhoid blood vessels or cause fibrosis of the hemorrhoid submucosa through the instant high heat generated by infrared rays, to fix the anal cushion. IRC is mainly used for the treatment of internal hemorrhoids of grade I – III [2]. The purpose of this study was to compare the efficacy and safety of RBL, IS and IRC in the treatment of internal hemorrhoids. We evaluated the evidence from the random control trial (RCT) and the research data from the systematic review of the RCT, and performed a meta-analysis, which is reported below.
Materials and Methods
Search strategy
Use keywords such as “Hemorrhoids”, “Hemorrhoid sclerotherapy”, “Injection sclerotherapy”, “Rubber band ligation”, “Hemorrhoid ligation”, “Infrared coagulation”, “Hemorrhoid infrared coagulation”. Searched the literatures from PubMed, Cochrane Library, and Embase database up to 2021. The research method limited the RCT to improve the sensitivity and did not limit the language, and the related references in the included literature were manually searched, and consistent standards were used to determine the included and excluded literature.
Inclusion and Exclusion Criteria
• Participants of the study included patients ≥18 years of age who met the Goligher’s grading classification criteria and patients with grade I-Ⅲ internal hemorrhoids; patients diagnosed with grade IV hemorrhoids and patients with other anorectal diseases other than the study disease were excluded. • The original text is publicly published literature; it is limited to RCT, in which patients are randomly assigned to two or more treatment groups, clinical results are recorded, and follow-up time is at least 3 months. • The original literature provides corresponding indicators of effectiveness and safety: including effective rate, recurrence rate, complication rate, etc. • The type of literature is limited to treatises, and literatures with incomplete original data are excluded. reviews, conference reports, reviews, case reports, etc. are excluded. • The included RCTs are all evaluated by the Cochrane handbook to evaluate the quality of the literature.
Data Extraction
General data of the literature were extracted: including the first author, year of publication, number of patients included, observation data, etc. The extraction of all data was done independently by two researchers. For the controversial data, the third researcher participated in the discussion and decided.
Outcome Indicators
Main Outcomes: Effective Rate, Recurrence Rate. Secondary Outcome: Complications.
Statistical Analysis
Meta-analysis was conducted with Review Manager 5.4 software to study the effective rate, recurrence rate and complication rate of RBL, IS and IRC in the treatment of patients with internal hemorrhoids. As a dichotomous variable analysis, odds ratio (OR) was used as the effect index, and 95% confidence intervals (95%CI) is calculated. The Cochrane Q test was used to evaluate the heterogeneity among studies, and the magnitude of heterogeneity among studies was determined by combining the I2 value. Moderate to high heterogeneity was considered when I2 was greater than 50%, and the test level was α=0.1. The data were combined and analyzed for heterogeneity. If there was no heterogeneity (I2≤50% and P≥0.1), the fixed-effect model was selected for analysis; If there was heterogeneity (I2>50% and/or P<0.1), then analyze its sources and discuss, choose random effects model analysis. Meta analysis test level was α=0.05. For highly heterogeneous variables, the single study deletion method was used to conduct sensitivity analysis to find the source of heterogeneity. If the heterogeneity decreased after deleting the document, the document was the source of heterogeneity, and the forest figure was finally made. Regarding the analysis of publication bias, by observing whether the two sides of the funnel chart were symmetrical, if the two sides were symmetrical, there was no obvious publication bias, and if the two sides were asymmetric, there may be publication bias.
Meta Analysis Results
A total of 379 relevant literatures were retrieved, 159 duplicate literatures were excluded, 155 were excluded after reading the title, 39 were excluded after reading the abstract, and 14 were excluded after reading the full text. A total of 12 literatures were screened according to the inclusion criteria (Figure 1). A total of 1438 patients were included, including 592 patients in the RBL group, 350 patients in the IS group, and 496 patients in the IRC group. The detailed data of the included literatures were shown in Table 1 (Figure 2).
Figure 1: Literature retrieval process and results Table 1 Features of the included literatures.
Figure 2: Risk assessment of inclusion literature.
Effective Rate
a. RBL vs IRC: A total of 782 cases are included in 6 literatures, and heterogeneity analysis indicates no heterogeneity (P=0.60, I2=0%). The fixed-effect model analysis is carried out, and the results shows that there is no significant difference in the effective rate between the RBL group and the IRC group (OR=1.36, 95%CI:0.89-2.09, P=0.16), indicating that the treatment effect of the two groups is similar, as shown in Figure 3.
Figure 3: RBL vs IRC effective rate.
b. RBL vs IS8: A total of 480 patients are included in 5 literatures. Fixed effect model analysis is used, and the heterogeneity analysis indicates that there is heterogeneity (P=0.06, I2=55%). By eliminating literatures one by one, it is found that the heterogeneity decreases after eliminating literatures Greca.1981, with statistical difference (OR = 2.56, 95% CI: 1.53-4.27, I2 = 46%, P = 0.0003). It suggests that the effective rate of RBL group is better than that of IS group, as shown in Figure 4.
Figure 4: RBL vs IS effective rate.
c. IS vs IRC: A total of 267 patients are included in 2 literatures. Heterogeneity analysis shows that there is no heterogeneity (P = 0.77, I2 = 0%). Fixed effect model analysis is carried out. The results shows that there is no significant difference in the effective rate between IS group and IRC group (OR = 0.66, 95% CI: 0.37-1.19, P = 0.17), indicating that the treatment effect of the two groups is similar, as shown in Figure 5.
Figure 5: IS vs IRC effective rate.
The Recurrence Rate
a. RBL vs IRC: A total of 612 patients are included in 4 literatures. Fixed effect model analysis is used and the heterogeneity analysis indicates that there is heterogeneity (P=0.004, I2=77%). By eliminating literatures one by one, it is found that the heterogeneity decreases after eliminating literatures Walker.1990, with statistical difference.(OR=0.40, 95%CI:0.24-0.67, I2=44%, P=0.0003), suggesting that the recurrence rate of the RBL group is lower than that of the IRC group, as shown in Figure 6.
Figure 6: RBL vs IRC recurrence rate.
b. RBL vs IS: A total of 480 patients are included in 5 literatures. Fixed effect model analysis is used and the heterogeneity analysis indicates that there is heterogeneity (P=0.02, I2=67%). By eliminating literatures one by one, it is found that the heterogeneity decreases after eliminating literatures Walker.1990, with statistical difference (OR=0.34, 95%CI:0.19-0.61, I2=264%, P=0.0003), suggesting that the recurrence rate of the RBL group is lower than that of the IS group, as shown in Figure 7.
Figure 7: RBL vs IS recurrence rate.
c. IS vs IRC: A total of 267 patients are included in 2 literatures, and the heterogeneity analysis indicates that there is heterogeneity (P=0.04, I2=76%). Since there are only 2 literatures, random effect model analysis is carried out, and the results showed that there is no significant statistical difference in the recurrence rate between IS group and IRC group(OR=0.59,95%CI:0.14- 2.39,P=0.46), suggesting that the recurrence rate of IS group and IRC group is similar, as shown in Figure 8.
Figure 8: IS vs IRC recurrence.
Incidence of Complications
a. RBL vs IRC: A total of 782 patients are included in 6 literatures. Fixed-effects model is used and the heterogeneity analysis indicates that there is heterogeneity (P=0.03, I2=59%). By eliminating literatures one by one, it is found that the heterogeneity decreases after eliminating literatures Walker.1990, with statistical difference (OR=1.91, 95%CI: 1.15~3.16, I2=19%, P=0.01), suggesting that the incidence of complications in the RBL group is lower than that in the IRC group, as shown in Figure 9.
Figure 9: RBL vs IRC complication rate.
b. RBL vs IS: A total of 554 patients are included in 6 articles and heterogeneity analysis indicates no heterogeneity (P=0.49, I2=0%). The fixed-effect model analysis is carried, and the results shows that there is no significant difference in the incidence of complications between the RBL group and the IS group (OR =0.02, 95%CI: -0.03~0.07, P=0.42), as shown in Figure 10.
Figure 10: RBL vs IS complication rate.
Discussion
Hemorrhoid is a soft venous mass produced by the dilation and flexion of the submucosal and cutaneous inferior venous plexus at the end of the rectum, which contains normal spongy tissue structures such as minute arteriovenous anastomosis, connective tissue, and nerve tissue, thus playing an important role in assisting and controlling defecation. Hemorrhoids are the most common anorectal diseases in adults, accounting for 89.25% of all anorectal diseases, and treatment needs are huge. The main clinical manifestations of internal hemorrhoids include bleeding, prolapse, pain and perianal itching, and in several cases, it can be complicated with thrombosis, incarceration, strangulation and difficulty in defecation, which significantly affects the patient’s quality of life. The treatment of internal hemorrhoids focuses on the elimination of symptoms caused by internal hemorrhoids. The commonly used treatment methods for internal hemorrhoids include non-surgical treatment and surgical treatment, among which non-surgical treatment includes RBL, IS, and IRC. The national guidelines of the United States, Japan, France, and China countries recommend that the above methods are mainly used for the treatment of I-III degree internal hemorrhoids [1,5,6], but the efficacy and safety of various methods are still controversial. In this article, the efficacy, recurrence rate and complication rate of the above three methods for the treatment of internal hemorrhoids are analyzed and compared in order to comprehensively and objectively evaluate the efficacy and safety of RBL, IS and IRC in the treatment of internal hemorrhoids. The results of this study show that the efficiency of RBL group is better than that of IS group, which is consistent with the research results of Jacobs, D et al. it is mentioned in the research report that the long-term effective rate of RBL group is about 90% among patients with internal hemorrhoids of grade I-III, while the long-term remission rate of only one-third of the patients treated with IS, indicating that the long-term effective rate of RBL is superior to that of the IS group [7]. Similarly, the research results of MacRae HM et al. also show that for I-III degree internal hemorrhoids, it is recommended to use RBL as the first-line treatment, and its curative effect is better than IS. Compared with patients receiving IS or IRC treatment, the need for retreatment in RBL group is obviously reduced [8]. This study has shown that the efficacy of the RBL group was comparable to that of the IRC group. The research by Ricci MP et al. also reported that the success rate of 4 weeks after RBL was not different from that of IRC, that is, the short-term clinical efficacy of RBL was comparable to that of IRC [9]. This study shows that the efficiency of IS group is equivalent to that of IRC group, which is similar to the research results of MacRae, MD et al. . It is mentioned in the research report that there is no difference in any outcome index between IS group and IRC group [10]. IS is the most effective for I-II degree internal hemorrhoids, and postoperative bleeding is rare. For patients with high risk of bleeding, such as patients receiving anticoagulant therapy, this method should be considered [7]. This study suggests that the incidence of complications in RBL group is lower than that in IRC group. However, the research of Johanson JF et al. Showed that RBL has better long-term efficiency, but the incidence of pain after treatment is higher. In contrast, the complications of IRC are few and not serious [11]. The reason for the analysis may be that the current guidelines classify pain as a type of complication. This article does not analyze pain alone, but classifies it as a complication for analysis. This study shows that the recurrence rate of RBL group is lower than that of IS group and IRC group. A C Poen et al. reported that 18% of the patients receiving RBL treatment had symptomatic recurrence, while 20% of the patients receiving IRC treatment had symptomatic recurrence to the level before treatment [12], and the longer the follow-up time was, the higher the symptom recurrence rate was [13]. Meta-analysis of non-surgical treatment showed that the recurrence rate of Ⅰ-II internal hemorrhoids patients after IS was relatively high, while the discomfort caused by RBL was relatively high [14-24].
The Limitations of this Study
1) Although the research documents included in the systematic review are all RCTs, the follow-up time varies, and there is a lack of multi-center, large-scale, long-term follow-up RCT research results. 2) Some studies have a small sample size, and some evaluation indicators only have 2-3 literatures for effect combination, and the outcome indicators of the analysis are not fully mentioned, such as: surgical recovery time, cost-benefit ratio, patient satisfaction, etc. To systematically evaluate the three methods, there is still a lack of high-quality RCTs research. 3) The cases of internal hemorrhoids in some literatures are not classified. In conclusion, for the treatment of grade I – III internal hemorrhoids, the safety of RBL group is better than IS group and IRC group, and the efficacy is better than IS group or equivalent to IRC group. Therefore, RBL can be the first choice among the three treatment methods, but it still needs to be verified by multi-center, large-sample and high-quality RCTs.
Optimization of Ovulation Induction in Clomifene Resistant Patient with Infertility
Introduction
It has been proven that the induction of ovulation is the main method of treatment in infertile women with PCOS [1-3]. According to the WHO, from 10 to 15% of married couples suffer from infertility. In the conditions of Central Asia, where large families are common and this is traditionally encouraged, childlessness is considered a great misfortune and often leads to family disintegration [4,5]. Up to 20-25% of women with PCOS are resistant to clomiphene citrate [6,7].
Materials and Research Methods
Our randomized trials were carried out in the central polyclinic of Urgench from 2018 to 2020. It included 40 clomiphene-resistant women with PCOS. In group I (n = 20) women, we used clomiphene citrate 100mg + recombinant follicle-stimulating hormone p FSH 37.5 IU / day. Group II (n = 20) received only p FSH 37.5 using a low dose escalating protocol. Informed written consent was obtained from all patients. Women were considered clomiphene resistant if ovulation did not occur when taking CC at a dose of 150 mg / day. PCOS was diagnosed based on the Rotterdam criteria, in which at least 2 of the following three criteria were met: 1) Oligo menorrhea (a cycle lasting 35 or more days) and / or amenorrhea (absence of menstruation for 6 or more months); 2) Hyperandrogenism (defined as a Ferriman-Gallvi index of more than 8) which is clinically manifested by acne / hirsutism and / or biochemical – the determination of testosterone in the blood serum of more than 0.7ng / mg; 3) Sonographic manifestations of polycystic ovary: if the ovary contains 12 or more follicles with a diameter of 2 to 9 mm and / or the volume of the ovaries is more than 10 ml. Inclusion criteria are, clomiphene citrate resistant women with PCOS aged 20 to 38 years, BMI, no previous ovulation induction, partners with normal sperm counts according to WHO standards, opening of the fallopian tubes (confirmed by hysterosalpingography in the previous 6 months), without presence operations on the genitals. The exclusion criterion is the presence of any factors of infertility, except for CV-resistant women with PCOS. The study also included the measurement of blood pressure, abdominal circumference, hormonal study of the serum of patients such as basal FSH, LH / FSH ratio, free testosterone (T), insulin, progesterone, AMG on the 3rd day of the menstrual cycle. HDL High Density Lipoproteins, serum estradiol was determined on the day of ovulation trigger administration. Insulin resistance (HOMA-IR) was determined as follows: HOMA-IR = fasting insulin (IU / ml) x fasting glucose (mol / l) / 22.5. Ultrasound of the ovaries with a transvaginal sensor on the 2nd – 3rd day of the menstrual cycle to assess the number of antral follicles with a diameter of 2 to 9 mm (in an amount of 12 or more is considered polycystic) and an assessment of the volume of the ovary, which is determined by measuring three perpendicularly directed ovarian diameters and applying the formula: D1xD2xD3x0.5236.
Results of the Study
(Table 1) shows the results of clinical and laboratory studies of both groups, which reflects the average age of a woman, type of infertility, BMI, abdominal circumference, ovarian volume, type of menstruation disorder, hormonal and biochemical studies (Table 1). As our study showed, group I (CC + rFSH) received a lower dose of rFSH (532.5 ± 315) and the duration of stimulation days (12.34 ± 4.5) was less than in group II (18.42 ± 6.2 days of stimulation). The number of growth of the middle and dominant follicle, the thickness of the endometrium, the number of ovulations and the frequency of pregnancy are shown in (Table 2). The study showed that the dose of gonadotropin preparations for obtaining ovulation can be reduced by the simultaneous administration of CC + rFSH.
Table 1: Results of clinical and laboratory studies.
Table 2: Induction cycle indicators with results.
Conclusion
The combined administration of CC + rFSH in clomipheneresistant women with PCOS compared to the use of rFSH alone, gives higher ovulation rates and lower financial costs. The use of this protocol enables monofollicular growth and a decrease in the risk of multiple pregnancies and, in turn, is the prevention of ovarian hyper stimulation.
Coats Disease in Young Patient with Congenital Cataracts History
Case Report
He is 14-year-old boy, attended at the Ophthalmology Unit of High Specialty at Hospital Civil de Guadalajara Fray Antonio Alcalde since 2013. He had an ophthalmologic precedent of bilateral congenital cataract, treated with cataract faco aspiration and capsular bag implantation of intraocular lens (IOL) of both eyes in the same year, as well as correction of air lenses after the surgical procedure and visual therapy, with adequate evolution. Nevertheless, the patient loses his follow up as of 2018. Later, in May 2021 he requests a new assessment due to progressive visual loss of the right eye of 5 months of evolution, with no other association. Left eye reports no symptomatology. Other personal precedents without significant data.
Ophthalmologic Exploration
Best corrected VA OD 20/400, OS 20/30. No alterations in OU eyelids and annexes, eucromic conjunctiva, clear cornea, formed anterior chamber, isochoric pupils, nomoreflectic, Pseudofaquia, intraocular lens in capsular bag (Figures 1 and 2).
Figure 1: Clinical picture of IOL in situ, opacity of posterior capsule is observed, as well as fibrosis with free visual axis right eye (A), left eye (B).
Figure 2: fundus image: right eye (A), left eye (B).
Fundoscopy
OD clear vitreous, isochoric pupil, normochromic, retina with exudation at inferior and superior temporal arcade level with presence of vascular tortuosity, macular exudates. OS without alterations (Figures 3-5). In ultrasound of OD, we observe normal ocular globe contour, with intraocular lens of posterior chamber, vitreous with small mobile condensations of low reflection, thickened retina due to important cystic edema with macular involvement, thickened choroid secondary edema, irregular papilla. OS is reported without alterations (Figure 4). Macular spectral domain ocular coherence tomography of OD, where 242-micron central foveal thickness is observed, in presence of intra-retinal cysts and sub-retinal fluid.
Figure 3: Mode B ultrasound, right eye (A), left eye (B).
Figure 4: Macular SD- OCT.
OS with central foveal thickness of 286-micron, within normal parameters (Figure 4). In the fluorescein angiography (FA) of OD we observe retinal vessels with dilation and leaks, with telangiectasias in retina surrounded by hard exudates, in peripheric retina with hyperfluorescent zones corresponding with areas of capillary closure. FA of the OS is observed without alterations (Figure 5) In accordance with clinical characteristics of the patient, as well as findings in complementary studies, Coats disease is diagnosed. Treatment with scheme of intra vitreous anti-VEGF (Aflibercept) of OD, and with previous informed acceptance from his parents, first dose was applied on Aug 05, 2021. After three weeks he is evaluated, and patient refers recovery of visual quality. Nevertheless, BCVA of OD didn´t improve further than 20/400. A second dose of anti-VEGF was applied in September 2021. He was evaluated one week later presenting vision improvement, with a BCVA 20/200 and reduction of retinal exudation as shown in Figure 6.
Figure 5: Fundus images, right eye (A1), left eye (B1). Red-free images of the retina, right eye (A2), left eye (B2). Flouoresceine angiography of right eye (A3- A6), left eye (B3- B6).
Figure 6: Fundus image A) and macular SD OCT (B) of the right eye.
Discussion
Coats Disease is a retinal vascular disease, characterized by telangiectasias and vascular leaks that lead to exudation. It is typically found in young males, between the first and second decade of life, with a peak of incidence between 5 and 11 years old. In 85- 90% of patients, it is a unilateral affectation. In cases of bilateral disease, the other eye shows no symptoms with slight telangiectasic changes in the periphery. There is no preference for race, and is a sporadic non inherited condition, without systemic association; the gold standard for the diagnosis of this disease is the eye fundus clinical exploration through direct ophthalmoscopy [1,2] and as our patient fitted in the above-mentioned characteristics, the diagnosis of Coats has reached. However, there are very few reports regarding the association of this pathology with the presentation of Congenital cataracts, even less in a bilateral way, as is the case of our patient [3,4]. The etiology of Coats disease is not completely defined; however, it is well known that retinal vascular leak is one of the main pathologic processes found in this disease. Several studies have been recently found that where an increase of cytokines is evidenced in the aqueous humor of patients with Coats disease, mainly the vascular endothelial growth factor (VEGF) of the aqueous humor was strongly elevated in this entity and had correlation with the extension of the retinal exudation. Tingy Liang et al. analyzed the aqueous humor of two groups of patients. One of them had 36 patients with Coats disease and another one with 15 patients as a control group with congenital cataract. Concentrations of 22 different cytokines, of which, concentrations of 8 cytokines (VEGF, IL-6, IL-8, MCP-1, MIP-1α, IP-10, VCAM-1 e ICAM-1) were significantly higher in the group of Coats disease, however, significant differences were observed in bFGF, TNF-a and IFN-y between the group of Coats disease and the control group, being this of importance for our patient since he presented both diseases and thus the use of anti-VEGF drugs for his treatment is sustained [5]. Broadly speaking, the objective of the treatment for slight and moderate disease is preservation of the vision and prevention of progression of the disease as retinal detachment and all the other complications already mentioned. That is why treatment is focused in ablation of the actual abnormal vasculature of the retina by means of photocoagulation with laser and cryotherapy. However, the innovative therapy is the use of intra vitreous VEGF, which is also recommended as a contributory manner with the traditional therapies already mentioned, since it seems to reduce macular edema and exudates, stabilize visual acuity and enhance regression of abnormal vessels, as observed in our patient, with a vision improvement and reduction of posterior retinal exudation to the first dose of intra vitreous anti-VEGF. Even though a complete regression of the disease is not expected, our objective is to stop progression and avoid appearance of future complications. [2,6,7]. Even though association of the appearance of cataracts is reported, after presentation of Coats disease, as mentioned by Daruich A. et al. [7], inverse association (that means, late presentation of Coats disease with bilateral congenic cataracts background) without a syndromic association is very rare.
Overview of Carbapenem-Resistant Enterobacteriaceae
Introduction
Respiratory infection is one of the most common diseases in the world, with high incidence and mortality. Enterobacteriaceae is the most clinically important gram-negative pathogenic bacteria, which are increasingly being reported worldwide. Antimicrobial resistance is globally recognized as one of the greatest threats to public health. For years, carbapenems have been used successfully to treat infections due to resistant Enterobacteriaceae, such as Escherichia coli and Klebsiella pneumoniae. However, recently Carbapenem-resistant Enterobacteriaceae have emerged, which confer broad resistance to most ß-lactam antibiotics including lastline carbapenems. Carbapenem-resistant Enterobacteriaceae refers to Enterobacteriaceae that are resistant to any drug of ertapenem, Doripenem, imipenem, meropenem, or enterobacteriaceae that produce carbapenemase. Infection with Carbapenem-resistant Enterobacteriaceae is emerging as an important challenge in healthcare settings and a growing concern worldwide, it is very easy to spread in patients with long-term hospitalization or low immunity, leading to nosocomial infection, and may even cause a small- or large-scale outbreak [1-3]. Most Enterobacteriaceae belong to the normal flora in the intestinal tract and can become opportunistic pathogens once the body’s immunity declines. Enterobacteriaceae obtain genetic material mainly by horizontal gene transfer mediated by plasmids and transposons [4] Carbapenem-resistant Enterobacteriaceae can cause a number of serious infection types (such as pneumonia, abdominal cavity infection, urinary tract infections, Bloodstream infection, skin and soft tissue infection, central nervous system infection, and device-associated infections) or asymptomatic colonization, among which Ventilator-associated pneumonia (VAP) was the most common [5]. Severe pneumonia has always been a common respiratory disease, which can endanger life. Statistics [6] show that infectious diseases account for 30% of all deaths worldwide, with severe pneumonia leading the way. Carbapenem-resistant Enterobacteriaceae infection was reported in 68.8% of patients with hospital acquired bacterial pneumonia [7]. Consistent mortality rates of 40-50% are observed among inpatients with infections caused by CRE in hospitals worldwide, while the mortality rate from CRE infection in pneumonia patients is as high as 60% [8]. Carbapenem-resistant Enterobacteriaceae infection is a very difficult problem in clinical practice.
Risk Factors of Acquisition of CRE Infection
There are a number of factors that predispose persons to infections by CRE. Exposure to these resistant organisms can cause serious infections in patients with the following reported risk factors: immune-suppression, advanced age, admission to intensive care unit (ICU), mechanical ventilation, previous exposure to antimicrobials, organ or stem-cell transplantation and prolonged hospital stays. Healthcare associated infections caused by CRE, mainly Klebsiella pneumoniae, have been encountered most commonly in ventilator-associated pneumonia, bacteremia, urinary tract and surgical site infections. Growing evidence suggests early detection of CRE-colonized patients on admission to long-term care facilities may help to prevent institutional outbreaks and limit regional spread of this emerging public health threat. Respiratory disease is one of the risk factors for CRE infection, probably because a variety of bacteria grow in the respiratory tract and maintain a dynamic balance in the body. Elderly patients with respiratory diseases have low immunity and are vulnerable to infection. Moreover, most patients with respiratory diseases have a history of invasive operation. When tracheotomy or endotracheal intubation is performed, the respiratory mucosa will be damaged, resulting in a variety of complications. Some bacteria are easy to form biofilm in the open airway, which leads to abnormal expression of outer membrane pore protein and bacterial drug resistance. In particular, frequent aerosol inhalation and other operations change the airway environment, requiring frequent contact with patients by medical staff, which makes patients susceptible to colonization and infection by multi-resistant bacteria.
Prevention and Control measures for CRE Infections
2.1 There are reports which suggest that overuse of carbapenems is closely related to the incidence of CRE infection, and unreasonable use of carbapenems can easily induce bacterial resistance and spread [9]. One of the chief difficulties in the treatment of CRE is the excessive use of antibiotics, not only those acquired by the community but also in hospitals. On the one hand, the use of broad-spectrum antibiotics can kill the sensitive bacteria, and the resistant bacteria can survive and become the dominant growth, thus increasing the probability of CRE infection. On the other hand, drug resistance may occur due to the change of drug binding sites after drug use, resulting in carbapenemases and other drug resistance mechanisms [10]. Growing evidence suggests that carbapenem-resistant Gram-negative bacteria are sufficient to develop in the intestinal flora of intensive care patients just a few days of application of carbapenems antibiotics [11]. Therefore, it is necessary to strengthen the supervision and management of clinical application of carbapenems, and strictly implement the classification of antibiotics and the management of doctors’ prescribing rights, limiting the over-use and abuse of antibiotics in humans and agriculture.
Standardized Collection and Correct Interpretation of Microbial Test Reports
Specimens should be collected before antibiotic treatment, sterile site specimens should be collected as far as possible and microbial reports should be correctly interpreted, eliminating contamination and colonization and avoiding unnecessary use of antibiotics. Therefore, clinical microbiology laboratories at all levels of medical institutions should establish the ability to receive and process microbial specimens within 24 hours. There are reports which suggest that that patient carrying other multidrug-resistant bacteria are mostly in serious and complex conditions, with low immunity and relatively long stay in intensive care units, leading to the development of CRE. Therefore, it is necessary to strengthen the contact and isolation of MDR-resistant bacteria to avoid the spread of MDR-resistant bacteria in hospitals. Hand hygiene is the simplest, most effective, most convenient and economical method to control the infection in hospitals, which can significantly reduce the incidence of CRE infection. Mobile water sinks, non-contact faucets, hand sanitizers, hand drying facilities, quick-drying hand disinfectants, and related charts can reduce the colonization rate of CRE [12]. Studies show that the wash basin and its surrounding environment are seriously polluted, which is an important source of CRE pollution. Therefore, medical institutions should pay attention to the cleaning, disinfection and management of the location of the sink in the diagnosis and treatment area, taking anti-splash measures. Symptomatic colonized patients can become potential sources of infection. The significance of active screening lies in early identification of CRE colonized patients so that timely isolation measures can be taken to reduce the risk of transmission. Stool is the best specimen for active screening, and if not readily available, a rectal swab is taken. If the patient has a definite history of CRE infection, specimens from the infected site should be screened again. Patients with positive initial screening and hospitalized for less than 30 days do not need further screening, while patients hospitalized for more than 30 days were screened once a month. Those who have been screened negative for the first time should be screened regularly, either once a week or every two weeks, or twice a week, depending on the severity of the outbreak. Health care facilities should implement isolation of all CRE infected/colonized persons. Isolation refers not only to the establishment of physical spatial barriers, but also to the strict enforcement of isolation measures.
Treatment Options for CRE Infections
There are numerous different types of carbapenemase enzymes, each conferring varying spectrums of resistance. In general, the presence of a carbapenemase confers broad resistance to most ß-lactam antibiotics including penicillins, cephalosporins, and the monobactam aztreonam (excluding metallo-β-lactamases [MBLs] and oxacillinases [OXAs]) [13]. At present, the main drugs for the treatment of CRE in the world are polymyxins, Tigecycline, fosfomycin, Ceftazidime-Avibatam and aminoglycoside antibiotics. Polymyxins and tigecycline were highly sensitive to CRE in vitro and were not affected by the type of carbapenemases produced by bacteria. Due to heterogeneous drug resistance and positive correlation between dose and renal toxicity, polymyxins are often used in combination with other antibacterial agents. The conventional dose of tigecycline is difficult to reach sufficient concentration in the areas including the blood flow and alveolar lining fluid, so it is often necessary to increase the dose and use it in combination with other drugs. Ceftazidime-avibactam lacks effective antibacterial activity against metalloenzyme-producing CRE, so it may be an important choice for the treatment of nonmetalloenzyme- producing CRE infection. The most common adverse drug reactions of Ceftazidime-avibactam in trials were vomiting, nausea, constipation, and anxiety [14]. Combination therapy for CRE infections may decrease mortality compared with monotherapy. Benefits of combination therapy include reduction of initial inappropriate antimicrobial therapy, potential synergistic effects, and suppression of emerging resistance [15]. For patients who are critically ill or with deep-seated infections, consider empiric and antibiogram-directed combination therapy with 3 drugs, basing on antimicrobial sensitivity results. Polymyxins may be most effective as part of a combination for serious CRE infections [15,16].
Conclusion
In summary, the burden of carbapenem-resistant Enterobacteriaceae is increasing rapidly worldwide. CRE is widely spread and is now a major factor in morbidity and mortality in health-care settings. The results at present are still not good, especially in elderly patients with a history of CRE infection. The extremely high mortality rates of patients with CRE infections have driven efforts to prevent the acquisition and spread of these bacteria in hospitals. Although the above measures are simple, they can prevent the spread of CRE to some extent. However, continued research is desperately needed to determine the most appropriate treatment for serious CRE infections.