Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Bio-Filtration as a Solution for the Detrimental Health Effect of Excess Fluoride in Drinking Water
Introduction
One of the main importance of water filtration is to prevent water-related illnesses and diseases. To this day, various explored methods were used in the remediation of water of different types of contaminants such as flocculation [1,2], coagulation [3], solventextraction [4], co-precipitation [5], precipitation [6], ion-exchange [7], photo catalysis [8], adsorption-desorption [9], reverse-osmosis [10], nano-membrane filtration [11]. The adsorption technique is considered one of the attractive and commercial options to eliminate of the most pollutant substances whether macro- or micro- organic/inorganic ions from water, due to its simplicity of steps and high activity. Moreover, the purification of water by using adsorption technique has been applied to several matter as absorbent such as agricultural residues and industrial residues, and biomaterials wastes, which are modified and applied in biosorption of contaminants from water [7,9-12]. Fluoride is an ionic form of fluorine and can be found in food and numerous sources of drinking water. It can be also purchased as a dietary supplement [12]. Many kinds of toothpastes contain fluoride because these ions serve as an armor against tooth decay [13]. Approximately 80% of the fluoride taken orally is absorbed. Humans retain around 50% of the fluoride they consume, and most of this amount is deposited in teeth and bones (Graphical Abstracts 1 & 2). The remaining 50% is excreted in the urine.
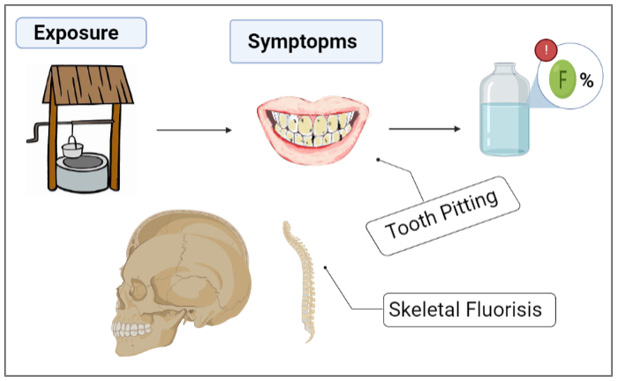
Graphical Abstract 1: Problem statement.
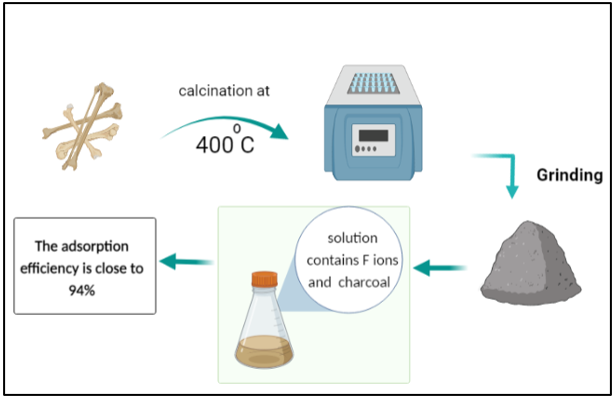
Graphical Abstract 2: Solution.
However, young children can retain an especially high percentage of the consumed fluoride, because their bones and teeth absorb more fluoride than those of adults [14]. The principle and mechanism of pollutants removal by adsorption technology from different types of water based on forms layer of condensate pollutants (called adsorbate) which is migrated from aqueous solution to the surface of solid (called adsorbent) as either in the form of liquid-solid interface [11,15]. Excess fluoride is harmful to human health. Groundwater wells worldwide have been reported to contain water with fluoride concentrations exceeding the acceptable level of 1.5 mg/L. This fact was attributed to local ground stones exhibiting high percentages of fluoride in their composition [14]. Excessive fluoride consumption can lead to several health issues, such as skeletal fluorosis, a disorder marked by bone and joint pain as well as joint tenderness. The overconsumption of fluoride during the formative years of tooth enamel can also lead to dental fluorosis, which leads to tooth discoloration, and/or tooth pitting [15]. Many researchers have attempted to develop water filtration strategies to lower the levels of fluoride or metals that contaminate water [16]. Biomaterials have shown great promise in water filtration because of their environmentally favorable properties, high filtering efficiency, and low cost [17].
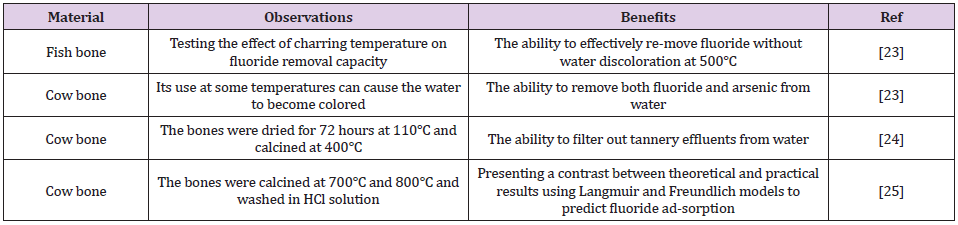
Charcoal, which may be manufactured from a variety of biomaterials, is one of the most commonly used bio-filters. Water contaminated with heavy metals can be treated using different processes, which include ion exchange, precipitation, reverse osmosis, catalysis, coagulation, and adsorption [18,19]. Heavy metal adsorption is dependent on the nature of the adsorbents, which can be composed of natural or man-made mate-rials including clay [10], sludge [11], industrial waste, activated carbon, and plants [12]. Bone char is an adsorbent made up of 90% calcium phosphate and 10% carbon. It can be created using one of the two methods: treatment with chemicals and physical treatment leading to carbonization of bones [20,21]. Cow bone char is com-monly used to purify water contaminated with heavy metals, as shown in (Table 1). The aim of the current study was to produce a lowcost, effective, and environmentally friendly biochar adsorbent from cow bone through physical activation (carbonization), and subsequently use it to remove fluoride from the polluted water [22]. Furthermore, it was also proposed to enhance this bio-filter by adding nanocomposites. Nanocomposites have very high surfaceto- volume ratios, which makes them ideal components for the adsorption process [23,24].
Table 1: Bone charcoal use based on the literature review.
Experiments
Cow bones were collected and processed by rinsing them several times with hot water to remove residual muscles and other joint tissues. Then the bones were allowed to dry in the open air. The dried bones were calcined in a furnace for 1 h at 400°C. The resultant charcoal adsorbent was crushed using a gate mortar and stabilized for further testing. It can be stated that the filters were produced with little to no expenses. A stock solution of CaF2 with a 100-ppm concentration of fluoride was prepared to test its adsorption in the cow bone sample. First, 1 g of charcoal was added to the 100 mL solution in a separate beaker, which was then placed in a shaker operated at room temperature and a 251 min-1 frequency for 5 h. Next, on the same day, the solution containing cow bone charcoal was filtered from impurities and charcoal leftovers using filter paper to prepare a sample for ionic chromatography (IC) [25]. IC was utilized for determining the concentrations of calcium and fluoride ions in the prepared CaF2 solution. Ion chromatographs can measure concentrations of important anions such as fluoride, chloride, nitrate, nitrite, and sulfate, as well as major cations such as lithium, sodium, ammonium, potassium, calcium, and magnesium in the parts-per-million (ppm) range. Ion chromatography can also be used to determine the concentrations of organic acid [26].
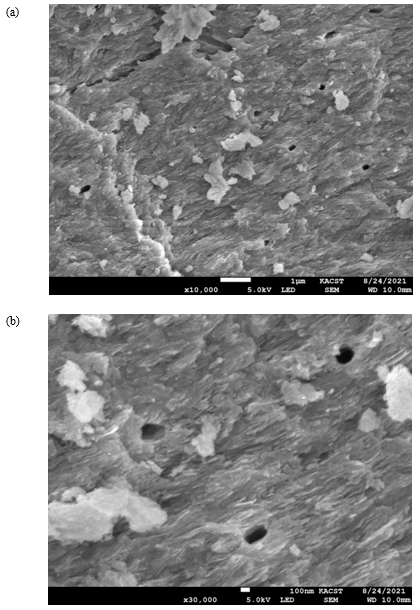
The surface structure of cow bone charcoal was studied by using a scanning electron microscope (SEM) (Model: JSM-7100F) at 10000 × magnification [27]. In conjunction with SEM, the energy dispersive X-ray (EDX) analysis technique was used to perform the elemental analysis and chemical characterization of the material. EDX utilizes an electron beam that strikes the surface of a conducting sample (placed under SEM) to determine its elemental content [28].
Results and Discussion
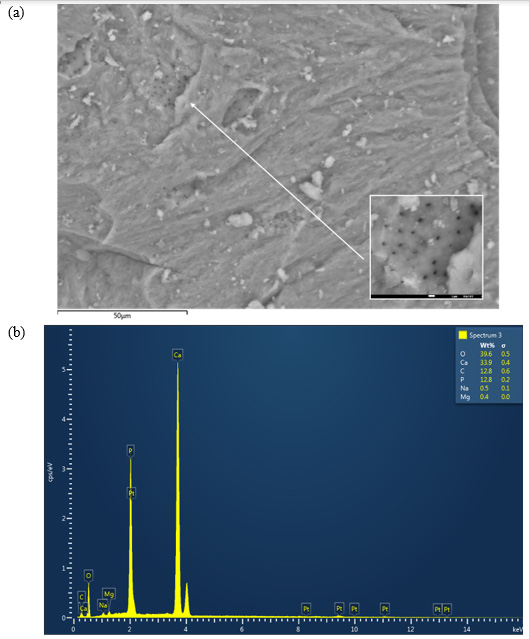
The SEM micrographs of the cow bone biochar explained the sample morphology by analyzing the microstructure of the bone powder, as shown in (Figure 1a). The corresponding EDX graph is presented in (Figure 1b). A close look at (Figure 1a) reveals cracks and irregular surfaces, as expected after grinding, where Vickers hardness can be determined (it is planned to be measured in the upcoming study). Furthermore, SEM micrographs showed that the studied samples had several heterogeneous porous layers, which represent a key feature relevant for fluoride adsorption. The pores appeared to be localized symmetrically in certain regions in the grooves on the surface of the bone. The sample composition revealed by EDX results was as follows: O2, 39.6 wt%; Ca, 33.9 wt%; C, 12.8 wt%; P, 12.8 wt%; Na and Mg, 0.9 wt%.
Figure 1: (a) Scanning electron microscope (SEM) micrograph of the cow bone charcoal shows several groups of symmetrically distributed pores. (b) The corresponding energy dispersive X-ray (EDX) graph of the bone constituents.
The surface morphology of the cow bone is particularly distinctive in terms of the hard appearance and the distribution of pores, which are of critical importance in filtering large species from water (Figure 2). Hence, the surface geometry and the source of adsorbent provided different types of active sites onto surface of adsorbent [29-35] (Table 2).
Figure 2: (a) SEM micrograph of cow bone charcoal shows symmetrically distributed pores on the surface (red arrows) with diameters in the range of several hundred nanometers, as shown in (b).
Table 2: The effect of bio-filtration with cow bone charcoal on fluoride removal.
Conclusion
The examined cow bone charcoal filter achieved maximal fluoride adsorption of 93.6%, which can be attributed to its porous nature. The prepared bio-filter has a very high adsorption capacity and is energy-efficient as it works at room temperature and does not require energy consumption. It means that using cow bone charcoal is a cost-effective filtration technique that should be further investigated to optimize the performance of nanocomposites and to set up measures for its widespread manufacturing.
Breast Cancer Prognosis: A Genetic Code for Personalized Therapy
Introduction
Today, breast cancer is distinguished into at least three different subtypes based on clinical and molecular parameters: luminal, erbB2, and basal type, which exhibit different biological behaviors and prognoses. Correctly identifying the molecular subtype of the tumor opens the door to new, increasingly adequate and targeted therapeutic possibilities for the treatment of the specific molecular subtype [1]. In this scenario, luminal carcinomas (which represent approximately 65% of the total) are distinguished by a particular heterogeneity of biological behavior, with recovery of disease in approximately 40-50% and death in approximately two-thirds of these patients 5 years after diagnosis, despite initial anatomopathological pictures of apparent low aggressiveness [2- 9]. Precisely for this diagnostic category, biomolecular parameters derived from the genome/transcriptome that are capable of orienting the therapeutic choices in a more precise and personalized way on the patient’s actual therapeutic needs are desirable [10,11]. Currently, the clinical (T, nodal status) and biopathological (hormonal status) parameters obtained from membrane receptor expression provide prognostic information and an indication of any adjuvant systemic chemoradiotherapy treatment [12-14]. However, adjuvant therapy reduces the risk of recurrence by only 25-30% [13]. These data are probably due to: 1. Clinicopathological parameters of stratification of the risk of disease recovery are not sufficiently adequate for the patient’s prognostic framework. 2. Adjuvant therapies are not specific enough toward the cells responsible for disease recovery [15,16]. Knowing the details of the mutations of every single tumor allows us to predict the biological behavior of that neoplasm and to adequately stratify the risk. Genetic tests, such as Mammaprint and Oncotype DX, EndoPredict [17,18], assist clinicians in choosing the most suitable adjuvant treatment by analyzing the expression profile of genes involved in the metastasis process (St Gallen 2017). These tests are very expensive and often have to be sent to foreign laboratories. The genetic profile is of the utmost importance in the evaluation of parameters already known as the expression of hormonal receptors and HER2; these are currently determined with immunohistochemistry (IHC) or FISH methods, which provide information about the morphological expression of the receptor but not about their functional state. In any case, knowing that the receptor is expressed at the membrane level is not sufficient information to guarantee the effectiveness of the drug addressed to it because that protein may not be functionally active. Therefore, it is necessary to ascertain the functional activation of the gene responsible for the synthesis of the protein to guarantee its functionality, more than its presence. Moreover, from the gene expression profile, additional information that specifically correlates the expression of some genes to the response to individual therapies can be obtained; for example, in HER2-positive patients, the high expression of IGF1R correlates with resistance to Herceptin, as well as the hyperexpression of CCNE1; instead, ER+ patients with high PDGFRA expression are resistant to tamoxifen treatment [14,19,20]. The use of gene profiling tests offers the opportunity for a more adequate risk stratification, an improvement of the therapeutic planning and the clinical outcome, avoiding what happens today, with the standard clinical-pathological criteria, namely, the undertreatment of approximately 20% of women with grade 1 breast cancer and overtreatment of approximately 15% of women with grade 3 breast cancer
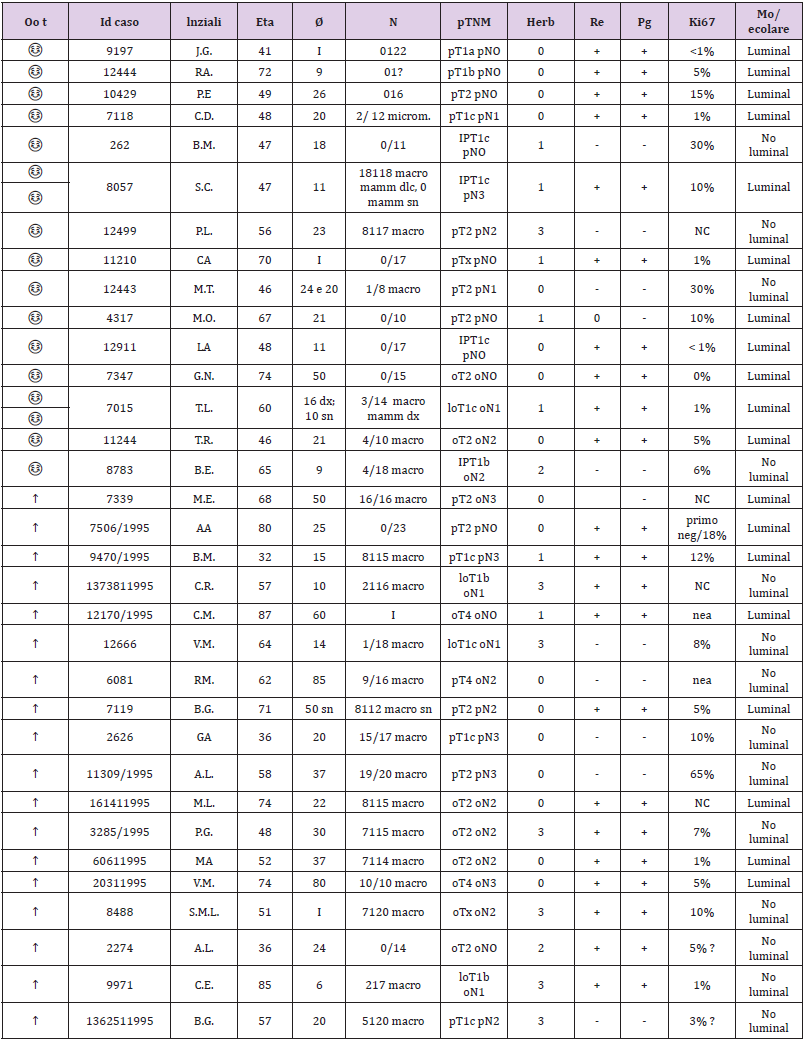
Methods
This retrospective study aimed to observe the difference in the receptor state obtained from the genome compared to that obtained with traditional immunohistochemistry. Analyzing biological material from formalin samples from 1994/1995 from two groups of selected patients with breast cancer, one consisting of patients still alive and the other of patients with a survival of less than 4 years. Survival data of a group of patients with a long follow-up period (RTUP) suffering from breast cancer diagnosed in the twoyear period 1994/1995 were obtained with the authorization of the Ethics Committee of Umbria (CEAS). The group, consisting of 55 patients, was then divided into 2 numerically balanced subgroups: the first of 30 patients staged alive on 31/12/2013 with survival of >20 years and the second of 25 patients staged in death with lower survival 4 years after diagnosis (Table 1). The relative tissue samples of the respective patients fixed in formalin and included in paraffin (FFPE) were subsequently collected and stored in the histoteca of the SC of Anatomy and Pathological Histology of the Hospital of Perugia. Twenty-two patients who had the respective tissue sample unsuitable for lack of biological material in the original inclusion block were excluded. The remaining samples, for a total of 33 cases, were all characterized again from a biopathological point of view through a dedicated immunohistochemical panel: ER, PgR, Ki67, HER2 and subjected to microscopic evaluation by a pathologist who was thus able to identify two groups of carcinomas: luminal and nonlluminal (according to the San Gallen criteria 2011 and following).
Table 1: The two-subgroup division of the 55 patients.
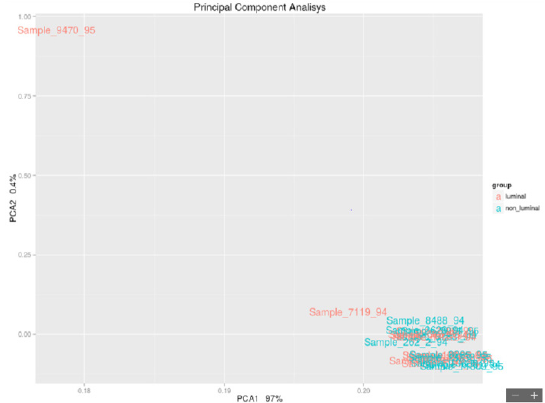
The recharacterization provided for the preparation of 1 slide for hematoxylin and 4 slides with blank sections necessary for the immunohistochemical panel for each sample. The pathologist made the diagnosis based on current guidelines and verified that in each section stained with the hematoxylin of each patient there were at least 30% of the neoplastic cells out of the total. This percentage figure is necessary to maximize the extractive yield of total RNA. In practice, for samples with a number of neoplastic cells ≥ 30% of the total, it was not necessary to proceed with macrodissection. In the first phase of the experimentation, so with the 33 starting samples, the enrichment of the sample was not necessary, but 2/4 sections of the FFPE fabric of 10 μm thickness were cut in sequence on microtome and placed in 1.5 ml safe look tubes ready to be extracted. Total RNA, after appropriate quantitative and qualitative evaluation, was used for the preparation of cDNA for sequencing purposes. The library used is Illumina’s TruSeq Total RNA. In the second phase of the experimentation, 2 pilot samples were used to validate the panel of genes obtained with the first phase; they were homogeneous both as biopathological characteristics of the lesion (early breast cancer; tumor diameter; lymph node status; state of HER2 and so on) and as the age of the patients. In the end, for each patient, we obtained 2 tubes of tumor tissue and 2 tubes of healthy tissue ready to be extracted. The extraction kit used to obtain total RNA was the same as that used in phase I of the trial. Total RNA, after appropriate quantitative and qualitative evaluation, was used for the preparation of cDNA for sequencing purposes. The library used was Illumina’s TruSeq RNA Access, suitable for processing RNA extracted from paraffin samples. Total RNA was extracted from sections of paraffin tissue using the “Tissue Preparation Reagents” kit – Sividon Diagnostic, from the Pathological Anatomy Section of the Santa Maria Della Misericordia Hospital. The chosen extraction method was previously “validated” on 2 samples with characteristics of “age of the sample”, “type of tissue” and “origin” identical to the samples to be used for this work. Validation test of the extraction method suitable for the preparation of the “TruSeq RNA Sample Prep” library from RNA for sequencing. For the deconvolution of the data from the HiSeq sequencer, to process them, the following steps were carried out: a. Demultiplexing: phase necessary to attribute to every single sample its respective data (1 sample = 1 fastq file). b. Fastqc: phase in which the quality control of the sequencing is carried out through the use of the “fastq file for reads quality” tool. c. Trimming: delicate but essential phase of the deconvolution process because it eliminates the reads and low-quality fragments from the Fast file. d. Mapping: important phase of the process because for each sample a same file (also called bam) is built which specifies how the reads align on the reference genome. e. Count table assembly: a final phase that includes all the information from the same file of the analyzed samples and related “count reads” in a single table. Based on the reference human genome, the following are the data of the number of reads that align: Human Genome Assembly (GRCh37/hg19). These data are used as a criterion for deciding which samples will be analysed. Samples with a low quantity of exons were excluded: a low number of reads mapped to exonic regions <12%. Two R/Bioconductor 3.2.2 packages were used for statistical analysis: 1. DESEq2 (Love MI, Huber W, Anders S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014; 15 (12): 550.) 2. edgeR (Robinson MD, McCarthy DJ, and Smyth GK (2010). “edgeR: a Bioconductor package for differential expression analysis of digital gene expression data.” Bioinformatics, 26, pp. -1) The edgeR package was used on the data analyzed with DESeq2 to confirm the results obtained with this calculation algorithm. Both are based on the negative binomial distribution but use different correction tests. The use of the two packages allows obtaining a list of genes that for both calculation algorithms are differentially expressed between the samples. The statistical significance that will be used in the two packages is shown below: 1. DESeq2: P-value <0.05; P adjusted value <0.1 2. edgeR: P-value <0.05; False Discovery Rate <0.1. An analysis of the network of genes significantly differentially expressed in the two groups was also conducted using GeneMania (http://www.genemania.org). This network was built based on the interactions between the genes, as reported by results published in the literature. Features such as gene coexpression, proteinprotein interactions, physical interactions between genes and other functions as described in the studies indicated in the table compared to the network figure are evaluated. Although paraffin introduced non negligible “background noise” in the analysis, the number of reads obtained was satisfactory to conduct a differential expression analysis using a “Read Counter” approach. It is possible to evaluate the formation of 2 small subclusters, and the analysis of differential expression with this dataset allows us to differentiate 25 genes differentially expressed between the 2 groups. The hierarchical cluster of significant genes shows a homogeneous trend among the 2 groups except for 2 luminal samples, which, although clustered with nonluminal samples, are very close to samples of the same stage (sample 7506 luminal staged due to death is very close to sample 2626 nonluminal staged due to death; sample 10429 luminal staged in life is close to sample 262 nonluminal staged in life). The IFIT3 and MX1 genes, among the 25 differentially expressed genes, have a strong interactome with other genes not present in the list but strongly correlated with each other in biological processes.From a careful observation of the PCA luminal vs nonluminal of the samples selected in Figure 1, it is possible to observe the formation of 2 groups of samples that do not comply with the luminal/nonluminal classification provided, as shown by the PCA. Although paraffin introduced nonnegligible “background noise” in the analysis, the number of reads obtained was satisfactory to conduct a differential expression analysis using a “Read Counter” approach. It is possible to evaluate the formation of 2 small subclusters, and the analysis of differential expression with this dataset allows us to differentiate 25 genes differentially expressed between the 2 groups. The hierarchical cluster of significant genes showed a homogeneous trend among the 2 groups. Among the genes, the FGFR3 gene is highlighted: a 2012 paper may be useful in which the following is stated: “FGFR3 activation in MCF7 cells stimulated activation of the mitogenactivated protein kinase (MAPK) and phosphoinositide 3-kinase (PI3K) signaling pathways, both of which have been implicated in tamoxifen resistance in breast cancer”. It should be considered that it is 4 times less expressed in “luminal” cases than in “nonluminal” cases.
Figure 1: Luminal vs Non-Luminal.
Results
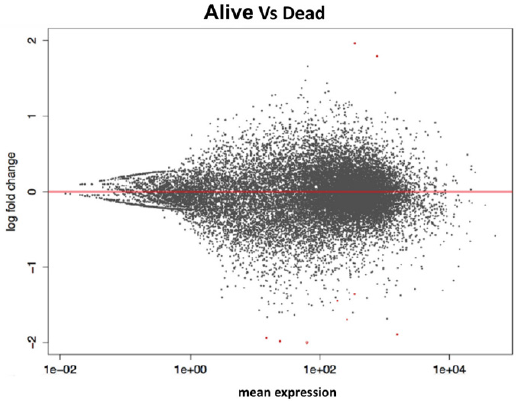
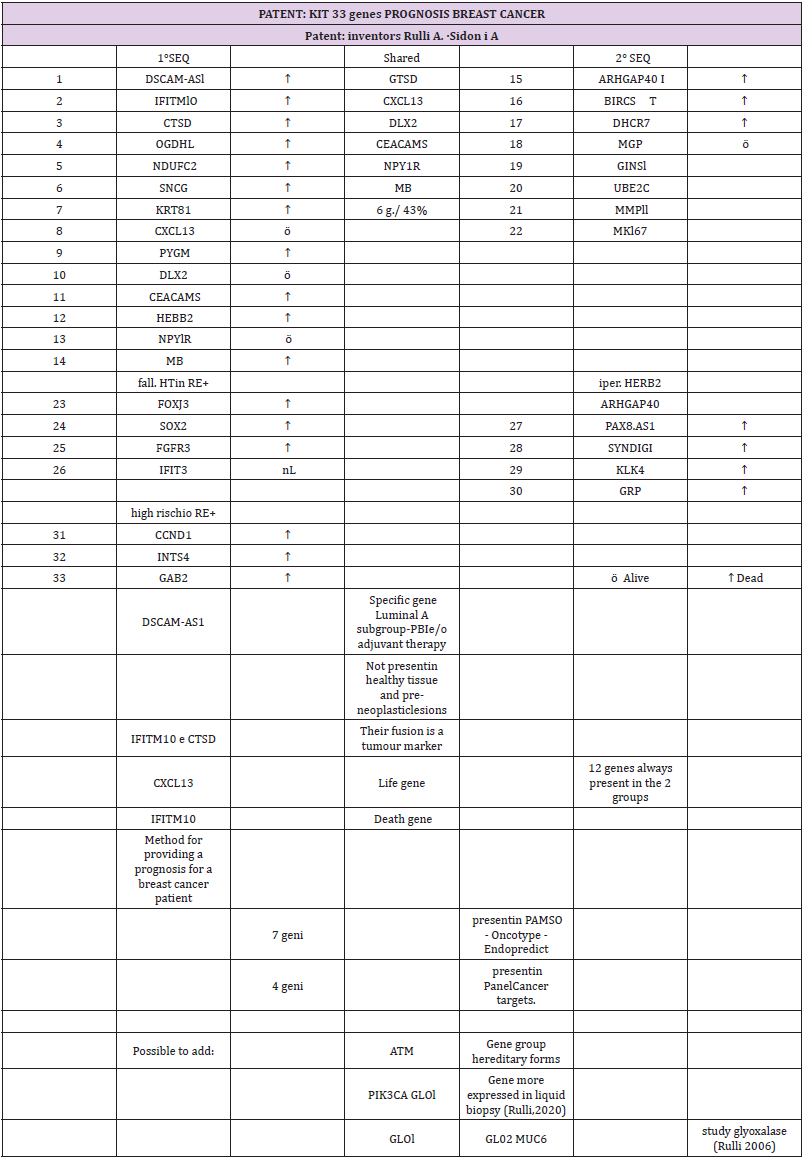
From the comparison of the results obtained with the two methods of statistical analysis, 62 significant genes emerged between living and deceased patients (Figure 2). In particular, 12 overexpressed genes emerged in live patients, and 50 overexpressed genes emerged in deceased patients. The 8 intersecting genes of the diagram are IFITM10, CEACAM7, KCNE4, OGDHL, NPY1R, SNCG, ARHGAP23, and PIEZO2. The unique DESeq 2 gene is RBFOX1. In this study, the data of the 26 samples (previous analysis) were analyzed again to highlight the genes that are differentially expressed in the luminal (life/death) and in the nonlluminal (life/ death) samples using the bioinformatic tools edgerR and DESeq2 in the R/Bioconductor environment using the following settings: DESeq2 pValue <0.05, P adjusted value 0.1; edgerR P-value 0.05, FDR 0.1. The parameters are those used in point 4.2 so that the results can be compared. The final result is divided into some innovative cornerstones: from the 28 overexpressed genes (23 in the luminal and 5 in the nonluminal), we found that 1. DSCAM-AS1 is a specific gene of the luminal A subtype that is not present in healthy tissue or preneoplastic lesions. If this gene is present, the patient could avoid standard PBI and adjuvant therapy. 2. ER+ patients (good prognosis) died because of a high risk for the overexpression of CCND1, INST4, and GAB2. 3. ER+ patients (good prognosis) died because the overexpression of FOXJ3, SOX2, and FGFR3 (4 times less expressed in the luminal region) correlated with the failure of endocrine therapy. 4. in HERB2+ patients, we found other genes, among which PAX8-AS1 was responsible for stem cell proliferation. 5. The fusion of IFITM10 and CTSD promotes cell proliferation of the tumor and is a tumor marker. The study highlighted a code of 33 genes that characterize breast cancer. Forty-three percent of the isolated genes were common between the 1st and 2nd sequences. Seven of our genes are found in the commercial genetic tests PAM50, Oncotype and Endopredict: four are present in the Panel Cancer targets 50 genes of the Ion AmpliSeq. The verification of the validation of the 28 genes selected from phase I in a more recent sample of women (2005) and characterized by the molecular split point (Endopredict®) allowed us to provide the study with greater consistency (Table 2).
Figure 2: Life vs Dead.
Table 2: The 28 genes characterized by the molecular split point (Endopredict®).
Conclusion
A very positive result was the ability to extract suitable RNA from 1994 samples in paraffin in good quantities and qualities to make the study possible. In this regard, experiments have been conducted to define the best protocol between RNA extraction and library preparation. The calculation of the RNA (RNA integrity number) and the concentration at Qubit allowed us to always “select” valid samples. The basic hypothesis of the study has been confirmed: the characterization of the luminal and nonluminal tumors is not real through IHC (surrogate St. Gallen), which is routinely used but must be read on a molecular basis. However, the most relevant data are represented by the 33 overexpressed genes: 28 genes (23 in the luminal and 5 in the nonluminal) and 5 genes (which confirm the premises of the study in wanting to find molecular markers capable of “personalizing” the therapy). Two of the 28 genes were always present in both groups: a CXCL13 life gene and an IFITM10 death gene. Moreover, IFITM10 and CTSD fusion promotes cell proliferation of the tumor and is a tumor marker. The DSCAM-AS1 gene is specific to the luminal A subtype. If this gene is present, the patient could avoid standard PBI and adjuvant therapy. The result obtained, which can be assumed to be transformed into a genetic panel, following validation on more recent samples (2005) and studied with Endopredict®, will help us to implement a personalization of the therapy: surgical and adjuvant. In the preoperative phase, with the core biopsy of the neoplasm, the histological diagnosis is obtained, and then the biopathological characterization and the presence of the genes described above are verified to evaluate the risk of local and/or systemic recurrence, which varies according to the molecular subtype. The hyperexpression of CCND1, INST4 and GAB2 changes the prognosis of ER+ patients from favorable to inaustic. Our work also revealed that ER+ patients died (in which we would have expected a good prognosis) because they had overexpressed FOXJ3, SOX2, and FGFR3 genes that correlate with the failure of endocrine therapy. In the postoperative phase, targeted therapy allows a better stratification of adjuvant therapies based on the amplification of the genes that regulate, for example, resistance to tamoxifen and/ or to trastuzumab.
Enhancing Patient Outcomes with Clinical Nutrition: The Effects of Supplementation in Orthopedics
Introduction
Each year more than half of people over the age of 18 in the US will develop a musculoskeletal injury that lasts more than 3 months. This is roughly 18% of all clinical visits and represents enormous costs, ~5.7% of US GDP and 216 million lost workdays [1]. Tens of millions of patients each year turn to orthopedic surgeons and physical therapists to treat their injuries and return to normal function as quickly as possible. There is an urgent need to utilize all of the latest techniques, tools and technologies to improve outcomes and enhance patient recovery to lower the cost burden on the health system and improve economic output due to lost workdays. New innovations continue to enhance the field of musculoskeletal injury treatment and management. One area that is showing considerable promise is in targeted nutrition.
Nutrition and Healing
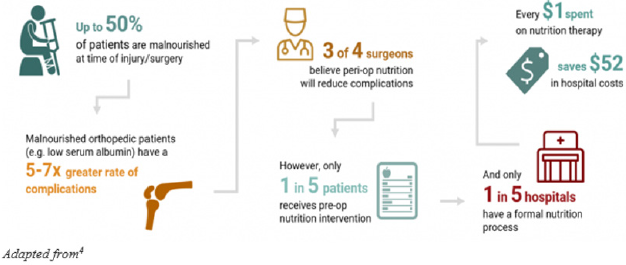
Science is increasingly showing just how critical nutrition is to healing and recovery. As we know during a state of trauma, such as injury or surgery, the body’s nutritional needs increase: a) The body enters a higher metabolic state and requires more energy b) Trauma and lack of use leads to muscle atrophy, which prolongs recovery c) The immune system is weakened due to stress and shock d) Risk of wound infection is increased e) Persistent inflammation delays return of function f) Trauma and physiological stress lead to increased fatigue Nutritional deficiencies impede the natural progression of healing, including elevating the risk of infection and lengthening recovery periods. A patient that is nutritionally optimized will heal better and faster and have better long-term outcomes. One that isn’t will heal more slowly and may have long-term complications. Unfortunately, most Americans are overfed and undernourished, meaning most Americans are not at optimal nutritional status to prevent complications post-trauma. Hospital studies have shown that as many as 50% of patients are undernourished or malnourished [2]. These patients face greater complications than properly nourished patients, including longer hospital stays, greater risk of infection, and increased mortality. One study, published in the Journal of Nutrition, studied over 16,000 individuals and found that many are not meeting the minimum recommended thresholds for micronutrient intake (Table 1): The combination of increased baseline nutritional needs post-trauma, from injury or surgery, and prevalent undernourishment means that most Americans are not well equipped nutritionally to heal Figure 1.
Table 1.
Adapted from3
Figure 1: The Impact of Malnourishment on Healing ().
Clinical Evidence – Nutrition as an Orthopedic Treatment Tool
The science of nutrition in orthopedics is advancing rapidly and a growing body of clinical trials are demonstrating convincingly that targeted nutrition can enhance outcomes, both for acute patients as well as for patients with chronic conditions. Wound healing, inflammation response, increasing muscle mass and strength, and decreasing muscle atrophy are crucial recovery objectives for orthopedic patients, and nutrition has been shown to support these healing processes. Below we look at a sampling of randomized trials from a larger set of published clinical trials in orthopedics. A randomized controlled study by Ekinci et al. [3]. included 75 older female patients with hip fractures and investigated the effects of Calcium HMB, vitamin D, and protein supplementation on wound healing and muscle strength. The study group received an enteral product containing 3g CaHMB, 1000 IU vitamin D, and 36 g protein, in addition to standard postoperative nutrition. They found that the patients on the nutritional supplement product had an acceleration of wound healing, shortening of immobilization period, and increased muscle strength without changing body mass index. This study also found a reduced dependence to bed and related complications after an orthopedic operation [4,5]. A study by Negro et al. found that twice daily consumption of a mix containing Essential Amino Acids (EAA), creatine, vitamin D and Muscle Restore Complex® (MRC®: Alpha Lipoic Acid (ALA), Coenzyme Q10 (CoQ10), resveratrol) for 12 weeks may aid in sarcopenia prevention without physical exercise by improving muscle aging-related outcomes, such as muscle mass, muscle strength and muscle power. In this study 38 healthy elderly subjects were randomized and allocated into the supplement or placebo group. Significant improvements were found in the supplement group compared to placebo in vitamin D blood levels, Legs Fat Free Mass, Appendicular Lean Mass, Maximal Voluntary Contraction, and Peak Power [6]. Dreyer et al. found in a double-blind, placebo-controlled, randomized trial on patients undergoing total knee arthroplasty (TKA), that EAA supplementation is safe and reduced the loss of muscle volume in older adults recovering from TKA [7]. These studies emphasize the importance of targeted nutritional supplements for muscle preservation and return to function – critical in any patient with a surgery that results in significant muscle atrophy such as ACL. Certain key ingredients are crucial to include to help support recovery. Liberman et al. found that thirteen weeks of nutritional supplementation with Vitamin D and leucine-enriched whey protein may attenuate the progression of chronic low- grade inflammatory profile in older sarcopenic persons with mobility limitations [8]. Another key study by Kim et al. found that in surgical patients, the addition of glutamine supplementation reduced infection rates and shortened the length of hospital stay. Glutamine also decreased the production of pro-inflammatory cytokines in this population [9]. By lowering inflammation, the healing process is greatly enhanced. β-hydroxy β-methylbutyrate (HMB) has been shown in many studies to promote wound healing and diminish muscle wasting Flakoll et al. found that elderly women treated with a nutritional supplement containing HMB, arginine, and lysine for 12 weeks had increased muscle mass and maximum strength [10]. HMB is also utilized and useful in combination therapies. This doubleblind controlled 12- month study by Rathmacher et al. found that HMB in combination with Vitamin D had a significant benefit on lean body mass and showed improvement in knee extension peak torque even with no exercise. Overall, their findings showed that even without exercise, the HMB+ Vitamin D supplemented group showed significant increases in functional outputs than those in controls [11]. Interestingly, HMB has also been shown to increase anabolic signaling [12].
Conclusions
A very significant proportion of the orthopedic patient population is nutritionally compromised and during trauma the body’s nutritional needs increase above baseline. Clinical studies are increasingly demonstrating that a patient’s nutritional status can directly impact outcomes and that modification through supplementation can enhance outcomes. The American Physical Therapy Association (APTA) has recognized the important role of nutrition in patient care and treatment and put it in scope of practice. APTA states: “Nutrition is part of the professional scope of practice for physical therapists”; further they state: “it is the role of the physical therapist to screen for and provide information on diet and nutritional issues to patients, clients, and the community within the scope of physical therapist practice.” (House of Delegates P06-15-22-17).” There remains work to be done to quantify the economic impact and savings to the healthcare system, but we suspect it is considerable. For example, large retrospective studies done by Novartis and Eli Lilly of more than 130 thousand patients shows that severe muscle atrophy and weakness (MAW) is common in joint replacement patients and that complications related to MAW cost roughly $10K per patient to treat13. Similarly, according to a study published by Mackenzie et al. [13]. in the Journal of Orthopedic Sports Medicine, revision costs in ACL patients range roughly in the $9K range [14]. Considering the sheer volume of orthopedic injuries and surgeries, we can extrapolate that there is billions of dollars of cost in the healthcare system that can be addressed through nutritional supplementation and optimization. In summary, an increasing body of science suggests that targeted supplementation should be utilized in patient care. By doing so, we can improve patient outcomes and reduce healthcare costs.
Teleconsultation is defined as synchronous or asynchronous consultation using information and communication technology to omit geographical and functional distance [1]. The WHO defines telemedicine as: “Delivery of health-care services, where distance is a critical factor, by all health-care professionals using information and communications technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and the continuing education of health-care workers, with the aim of advancing the health of individuals and communities” [2]. In the current COVID-19 pandemic, the use of telemedicine has increased by leaps and bounds- both by patients as well as health care providers. There are certain medical specialties where Teleconsults may be very useful, and maybe the way forward as well, viz. Dermatology, General Medicine, Diabetology, Endocrinology, Psychotherapy, to name a few. However, if we apply the same across all specialties- Oncology in general, and Surgical Oncology, in particular, seem to be the least efficacious towards “telemedicine”. The Cancer sufferers are caught on the ledge of a precipice- Cancer on one end, and COVID at the other. But, is telemedicine the way out? The pros would be – ability to allay anxiety, provide basic management and hope for a future “in person” consults. The cons include inability to manage any emergent situation or provide any definitive management to the patients. So- is there no role in Oncology? Effective teleoncology interventions may include cancer telegenetics, telepathology, bundling of cancer related teleapplications, remote chemotherapy supervision, symptom management, survivorship care, palliative care, and approaches to increase access to cancer clinical trials [3]. The Medical Council of India, in partnership with the NITI Aayog, has laid down certain guidelines for telemedicine, to provide Medical Practitioners to work within a specific framework. They have considered tele-consults to be equivalent to the “in –person” consults, both clinically, as well as economically. However, if we look at the satisfaction levels of patients, there seems to be a tremendous shortfall. The physician as well, faces several limitations, in accurately assessing the patients’ clinical condition. Moreover, “in person” consults allow a more humane, personal and confidential approach, which go a huge way, not only in building the “patientdoctor” relationship, but also enabling a more wholesome approach to disease management. In a nutshell, Teleconsultations are here to stay, but their appropriate usage for optimal patient outcomes and satisfaction is still debatable.
Development of Flexural Psoriasis Following COVID-19 Infection in an Infant
Introduction
A handful of rare and newly reported dermatoses have come into light following COVID-19 infection. While most manifestations are benign are transient, there are also a handful of reports of COVID-19 triggering a chronic dermatosis [1]. Although there are reports of triggers and flares of various morphological variants of psoriasis following COVID-19 infection, there is no such report of trigger of napkin psoriasis following the viral infection [2,3].
Case Report
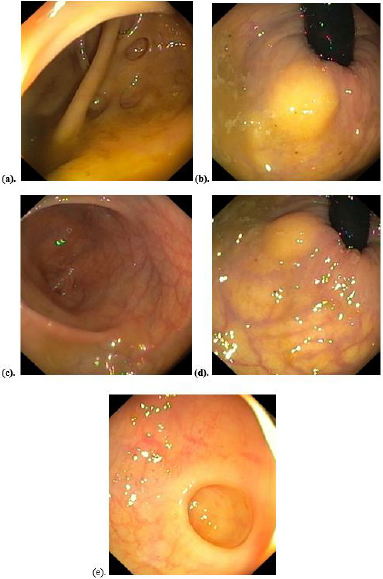
A 6 months old female child presented to our skin out patient department with the parents complaining of development of whitish pink macerated lesions in her groin since 3 weeks. On examination there was presence of well-defined bilaterally symmetrical fine scaly erythematous and slightly indurated plaques in intertriginous areas of groin, buttocks and anogenital region (Figure 1). The parents reported that the child had developed a lab proven COVID-19 infection 2 months back, which she presumably contracted from her infected mother. The onset of her cutaneous lesions had begun 5 weeks following the infection, while she experienced a respiratory flare in her symptoms. Current lab investigations revealed the girl to be RTPCR negative for COVID-19. Rest of the lab investigations were unremarkable. The child also had an optimum weight, height and milestones for her age. The KOH and fungal culture of lesional scraping and woods’ lamp was negative. The child was diagnosed with inverse or flexural psoriasis on the basis of striking clinical picture which further got confirmed by histopathological analysis. Biopsy findings included hyperkeratosis, fused rete ridged, suprapapillary thinning, and dilated tortuous dermal blood vessels. The child was prescribed hydrocortisone lotion and pemicrolimus ointment, along with oral antihistaminincs.
Figure 1: Napkin psoriasis in a 6-months-old female child 8 weeks after COVID-19 infection.
Discussion
The only variant of psoriasis presumed to have a definitive correlation following a systemic infection is guttate psoriasis. It is triggered following a staphylococcal infection and seen predominantly in children and young adults [4]. Various other genetic, environmental and idiopathic factors have also been reported to be responsible for triggering psoriasis. In fact. Even respiratory viral triggers, including COVID-19, are being reported. A viral infection can lead to immune dysregulation which stimulated TLR-3 which can stimulate CXCL8 and IL-36 [5]. As the novel COVID-19 evolves and unfolds it is only obvious that its myriad manifestations and complications will unravel. Skin being the largest organ has a great potential of being perhaps the greatest target of various immune deregulatory sequalae of this infection, especially in long haulers. Although our patient had a favourable clinical course with rapid recovery, the potential long term complications of COVID-19 are still unpredictable.
Conclusion
To the best of our knowledge this is the first such case of napkin psoriasis triggered by COVID-19. A dermatologist must always be on the look out to differentiate such presentation from other similar looking spotters like candida intertrigo, tinea cruris, and acrodermatitis enteropathica to name a few.
Electroanatomical Voltage Mapping Endomyocardial Biopsy-Guided Diagnosis and Therapy of Erythroparvovirus Myocarditis Presenting with Ventricular Arrhythmias: Case Series and Review of the Literature
Introduction
Myocarditis is an inflammation of the cardiac muscle caused by infiltration of immunogenic cells following different kinds of cardiac injury. It most commonly results from a viral illness; however, it can also be due to non-infectious etiologies. Given its variable clinical presentation, the diagnosis is frequently missed, making it difficult to quantify the true incidence of acute myocarditis. Infectious causes include a large number of viruses, as well as bacteria, protozoa and fungi; among these pathogens viruses are the most frequent cause of the myocardial inflammatory process. The most common forms of cardiotropic viruses found in endomyocardial biopsies (EMB) are erythroparvovirus B19 (B19V) and human herpes virus 6 (HHV6) and most recently Coronavirus (COVID19) [1-4]. We will now present two cases of 3 Dimensional electroanatomical mapping (3D-EAM) guided endomyocardial biopsy for the diagnosis and therapy of B19V myocarditis presenting with ventricular arrhythmias.
Case 1
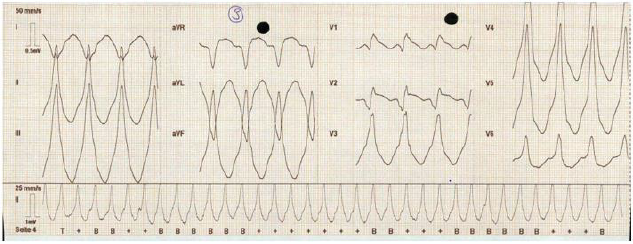
A 54-year-old woman presented to our emergency departement with a sustained monomorphic ventricular tachycardias (VTs) (inferior axis, RBBB, Figure 1), which, due to evolving haemodynamic instability, had to be cardioverted externally. She had no other known diseases except for a MTHFR mutation without clinical relevance and did not take any medications. On her arrival and after the external cardioversion she had no complaints. She had a normal blood work with no signs of an active infection and only a slightly elevated Troponin without elevation of CK as well as CKMB. Her ECG in sinus rhythm showed a minimal diffuse STelevation and relatively low voltages in the praecordial leads. The patient underwent a coronary-angiography, with no signs of coronary disease, an echocardiography which showed a normal left ventricular function with a slightly enlarged and dyskinetic right ventricle and finally a cardiac MRI (c-MRI) with evidence of preserved LV function and a RV dyskinesia as well as multiple RV aneurysms and areas of edema as well as multisegmental transmural late gadolinium enhancement on both ventricles, setting a differential diagnosis between sarcoidosis and myocarditis. The patient underwent a PET-CT which ruled out the sarcoidosis. We performed a 3DEAM-guided EMB to target areas of edema and fibrosis on the interventricular septum and avoid false negative results, which showed signs of an inflammatory cardiomyopathy with B19V with active replication and started the patient on a therapy with interferon Beta which is a well-tolerated and safe treatment option, leading to effective virus clearance or reduction of the virus load in patients with chronic viral cardiomyopathy [5]. After two months of therapy, we repeated a c-MRI which showed an almost complete resolution of the edema with persistence of late enhancement as scarred myocardial tissue. The patient underwent a secondary prophylactic implantation of an ICD and is stable ever since, without having experienced any new arrhythmias.
Figure 1: ECG: sustained monomorphic ventricular tachycardia with an inferior axis and a right bundle branch block, rhythm of presentation of the patient in case1.
Case 2
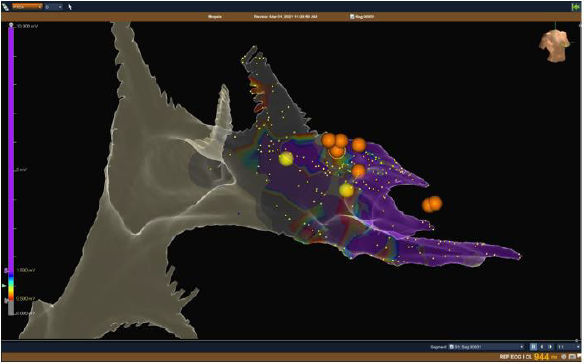
A 66-year-old woman was sent to our cardiology Department after a secondary prophylactic implantation of an ICD, due to sustained slow ventricular arrhythmias (LSB, inferior axis) after a probatory therapy with amiodarone as well as with sotalol. The echocardiography showed a mildly reduced EF (41%) with a diffuse hypocontractility, more evident in the basal segments. There were no echocardiographic signs for a dilated cardiomyopathy or for a hypetrophic cardiomyopathy and a coronaroangiography made in the first hospital had already ruled out any ischaemic cause of the reduced EF or the VTs. As the VTs were of incessant nature the patient underwent an emergency VT ablation of the RVOT-septal focus. Even if the procedure had an acute success with termination of the ventricular arrhythmias, one day after the ablation the VTs started again, and the patient was put on Mexiletine (Table 1). Because of the unclear diagnosis of the origin of the ventricular arrhythmias, their persistence after ablation, and the impossibility to run a c-MRI because of the implanted ICD, we decided to perform a 3DEAM-guided EMB which showed an active B19V replication. We then began an immunomodulating therapy with interferonbeta, under which a cessation of the ventricular arrhythmias was documented. At the follow-up, after six months of interferonbeta there were no sustained VTs anymore in the ICD-memory. No control MRI could be performed because of the device in situ (Figures 1 & 2).
Table 1: Endomyocardial biopsy results.
Figure 2: NavX Ensite Precision™ Image : bipolar voltage mapping of the right ventricle showing healthy ventricular tissue in purple (bipolar voltage > 1,5 mV) and scar ventricular tissue (grey, < 0,5 mV) with pathological area identified with the color coded scale. Right anterior oblique view with NavX Ensite Precision™ system. The yellow dots show the His Bundle And the right fascicle While the orange dots show the site in which the endomyocardial biopsy has been made, targetting the fibrotic or edematous tissue on the septal right ventricular wall.
Discussion
Even though for many years the medical research has failed to show a causative role of B19V in the genesis of heart failure confirming only an association [5-7], some more recent works have reported that chronic viral infections of the heart can be one antecedent event leading to progressive dysfunction of the myocardium, often with an impaired prognosis due to a virus- or immune-mediated myocardial injury [6]. Moreover, even if it is known that myocarditis can lead to cardiac dysfunction and to ventricular arrhythmias through the development of scars and therefore reentry circuits [8] no direct association between B19V persistence and those clinical pictures has been described. As the diagnosis of viral myocarditis can be problematic and the presentation can mimic other diseases such as sarcoidosis, arrhythmogenic cardiomyopathy as well as an evolution in dilated cardyomyopathy, the gold standard for the diagnosis and guide of the therapy is the EMB, an invasive but safe diagnostic tool that allows the quantification and identification of immune cell infiltrates, the quantification of viral loads and confirmation of virus subtypes via sequencing [9-14]. Hystorically, the EMB was performed under fluoroscopy guidance and was associated with potentially critical complications such as a cardiac tamponade. In the last years, there has been an evolving and promising use of EMB guided by 3D-electroanatomic voltage mapping, which could confere a higher specificity and sensitivity in targeting the involved tissue and in reducing false negative results, could reduce the radiation exposure of patients and operators in such procedures and present a higher safety profile compared with the mono-dimensional fluoroscopy images [15]. We described how two patients presenting with ventricular tachycardias of unknown cause could be successfully managed after a diagnostic 3D-EAM guided EMB after ruling out the most common causes of ventricular tachycardia. In our patients a subacute viral myocarditis caused by persistent erythroparvovirus, having sustained ventricular tachycardias as clinical presentation and demonstrating active replication of the virus, an immunomodulating therapy with interferon Beta was able to stabilize and resolve the ventricular arrhythmias. The 3D EAM guided EMB either combined with cMRI or not, can help to improve specificity and sensitivity in targeting the involved my-ocardial tissue and avoid false negative results, without increasing risks for the patients, as already shown in the literature [15,16].
Conclusion
To our knowledge this is the first case series described in the literature. Even if we will need a greater number of patients to confirm our observations, we hypothesize that B19V active replication could have a pivotal role in some forms of myocarditis which show an arrhythmogenic clinical presentation and that diagnosing and treating B19V in patients with a subacute myocarditis and ventricular arrhythmias could be determinant in solving the arrhythmias as well as the myocardial inflammation, although is not curative of the areas where the myocarditis has already produced a myocardial scar. We also described the emerging role of 3DEAM-guided endomyocardial biopsy in order to target the involved myocardial tissue and reduce complications as well as false negative results.
Family Counseling with a Child with Learning Disabilities or Disability
Introduction
Nowadays it is generally accepted the belief that counseling intervention in families with children either with disabilities or with learning difficulties or generally with special needs is necessary. It is therefore necessary to understand how essential the science of counseling psychology is and how long a counselor can stand by parents who have children with special needs, in order for them to provide the appropriate help to their child and finally to harmonize daily life. of their family.
Children with Special Needs
The term “special needs” refers to children with disabilities who are classified into categories according to the problems they face. These are a) Hearing problems b) Vision problems c) Special learning difficulties d) Autism e) Mental retardation f) Motor problems g) Behavioral disorders h) Speech disorders i) Personality disorders j) Chronic diseases [1]. Children with disabilities need in addition to special pedagogical treatment and psychological support, which can be achieved through the counseling process, so as to meet their personal, educational, social and professional needs [2]. There is no doubt that the role of counselor or psychologist is absolutely necessary so that children and adolescents feel supported and safe in the above areas. At the same time, however, prevention must be extended to the family system. In other words, it is necessary for the parents of children who face some problems to seek the appropriate counseling and psychological help, so that they can realize and at the same time understand early on the needs of their children, but also to support and unwind themselves psychologically.
Having a Child with Special Needs
Having a child without a doubt is one of the most important experiences of our lives. But it ends up being the most painful, when what we had dreamed of suddenly collapses because the child, we brought into the world does not live up to our dreams. As a result, completely unprepared parents view the event as a disaster, resulting in psychological shock, which determines their later life [3]. The treatment of this event by the parents is divided into two phases: a) The divisive phase according to which most parents are in a state of shock and subconsciously often have abominable thoughts such as for example thinking that they would prefer their child or even to die themselves. The most common reaction in the end is for parents to try to give birth to another child, to make their regrets more bearable and to restore their self-confidence and morale. b) The recovery phase of the relationship during which there is a variety of reactions. Most of the time the parents are too attached to the child and consciously conflict with his disability. In this second phase, it is necessary to be properly informed and supported by expert counselors, so that parents can more easily accept their child’s problem, feel relieved and therefore be able to function more effectively [4].
Defining Counseling
The term Counseling presupposes working with individuals but also with couples, during which the counselor manages to discover as well as to explore the methods that will bring him a more creative and satisfying life [5]. This type of counseling helps parents actually discover the extent of their child’s disability and assess their developmental prospects. It also enables them to be more decisive but also to implement their decisions more effectively. Also, during the sessions, the parents learn the ways that will help them to mobilize and offer their child more help. Still, through counseling they gain more courage and thus develop over time defense mechanisms of survival. The path of early counseling, that is, according to [6] offers long-term benefits to the whole family.
The Role of the Consultant
In order for a Counselor to implement a correct counseling intervention and to give accurately and without evasions a correct information, it is certain that he must possess the necessary theoretical and practical training so that he has the ability to guide correctly as well as to support them psychologically. parents of children with special needs. The counselor must possess the correct knowledge on the disorders he is called to deal with and of course on the counseling and psychology. The main roles of the Consultant are three. Primarily, they have a therapeutic role as their job is to help people cope with this difficult phase of their lives. Their second role is a preventive role as it prevents the anticipated difficulties that the family may face in the future. The third role of the counselor is educational and evolutionary because it enables people to plan how to get the most out of their experiences which will enable them to discover and accomplish everything, they are capable of achieving. He must also accept himself to be intelligent, to be dignified and above all to be possessed by humanity and compassion.
The Role of the Parent
Nowadays parents can play an active role during their children’s rehabilitation therapy. It is easily understood that parents have the ability to observe their children’s daily behaviors that do not manifest themselves during the examination or visit to a health professional. They can also be involved during their participation in psychological support and early intervention programs and most of the time manage to have amazing therapeutic results [7]. Parents who seek and receive special help are able to act therapeutically as far as their children’s behavior is concerned and by using the programs and treatment strategies, manage to successfully deal with the difficulties that their child faces during treatment and rehabilitation. Also, parents who are trained in counseling, are able to perceive inadequate behaviors, such as speech difficulties, difficulties in self-care and behavioral issues. Thanks to the knowledge they have acquired, they are able to judge which methods are appropriate and choose them, so that they can intervene and help immediately and prevent such behaviors, such as outbursts of laughter or anger and other outbursts. In addition, they know when it is necessary to support their child and how to reach the desired behavior slowly [8].
The Advisory Process
Throughout the counseling process, it is important for parents to be informed as clearly and accurately as possible about the report, the diagnosis, the prognosis and the ways to deal with the problem [8]. There are many counseling theories with similarities and differences between them and with their own counseling procedures. The following steps are followed in the counseling process in which the Counselor and the Counselor participate. 1) Stage 1: The Counseling process begins with the first contact of the counselor and the Counselor, who by creating a good psychological climate, set the desired goals. 2) 2nd Stage: In this stage, the relationship between the Consultant and the Consultant is built, which is the most important element that will lead to the success of the counseling process. Here the Consultant has the dominant role, since he is the one who with his correct behavior should facilitate the smooth outcome of the process. This will be achieved more easily, since it positively affects the Counselor, who, by adopting his personal way of thinking, now helps and believes in himself. The purpose of this second stage is to create the right climate of trust that will help parents express how they feel, express doubts and discuss the goals they have set for their child. 3) Stage 3: This stage leads through the development of a positive relationship between the Consultant and the Consultants in setting and delimiting the goals. 4) Stage 4: After setting the goals, the Consultant, taking into account the personalities of himself and the Consultant, applies his scientific knowledge in order to choose the appropriate consulting method. 5) 5th Stage: This stage is the end of the whole counseling process. This process is therefore considered successful when the initial goals have been achieved.
Conclusion
With the right guidance and support of families of children with special needs, it is possible in our time, as we saw above, for these families to find their own tactics for solving the problems they face as well as to use various techniques in their personal daily lives. You put more emphasis on these elements of the family that are considered more positive as well as on gaining in terms of selfconfidence [2]. In other words, counseling for families with children with special needs, whether it is some kind of disability or a special learning disability, can offer a better quality of life, peace of mind and clarity in order to help the child properly and effectively.
Abdominal Wall Metastasis without Primary Lesion or Definitive Diagnosis until Repeat Histology of Specimens from Laparoscopic Cholecystectomy: A Case Report
Background
Tumors located in the abdominal wall are often related to occupational and iatrogenic factors, and increased cases of abdominal wall metastases are reported along with increased removal of resected tumors by laparoscopy. Since the first laparoscopic cholecystectomy (LC) was performed in 1987, [1] LC has become the gold standard operation for benign disease of the gallbladder. With the explosive increase in LC rates, the incidence of incidental gallbladder carcinoma (IGBC), which has a more favorable prognosis than cancers presenting with symptoms, is found in 0.18-2.1% of patients during or after LC, diagnosed during or after cholecystectomy by pathology has increased [2-5]. Port-site metastasis (PSM) is a complication caused by the removal of IGBC using laparoscopic techniques, with an incidence of 14%–29% [6]. Several authors have reported cases of port-site adenocarcinoma metastasis of IGBC of unknown origin following LC. We present herein a case of PSM that was difficult to diagnose due to an incorrect histopathological examination and was discovered 3 years after LC was performed. The patient remained alive for 2 years without any treatment after the first sign of a recurrent tumor was found by the patient.
Case Presentation
A 57-year-old woman was admitted to our hospital because of aggravating pain in the right upper quadrant and a progressively enlarging mass with tenderness, measuring 20 cm × 4 cm, palpated at the right rectus abdominis region. The patient had undergone only one surgery, five years prior: she underwent LC using the threeport technique owing to symptomatic cholelithiasis diagnosed as chronic cholecystitis after a postoperative histological examination at an outside hospital. The patient first noticed the hard mass, measuring approximately 3 cm×3 cm, with intermittent pain in the right upper abdomen 2 years prior. Then, she underwent abdominal ultrasonography, which indicated only agenesis of the gallbladder. A wait-and-see policy was adopted, and the patient was discharged from the hospital and has not received any special treatment over these 2 years.
What Tests are Indicated to Narrow Down the Differential Diagnosis?
To determine the cause of abdominal pain and the mass at the uncommon location, relevant auxiliary examinations were performed. Abdominal contrast-enhanced computed tomography (CT) showed a thickened right rectus with uneven density whose enhancement was not obvious, indicating that the mass could be a benign lesion. Abdominal contrast-enhanced magnetic resonance imaging (MRI) also showed the mass as more likely a fibroma durum. Then, an ultrasound-guided needle biopsy of the mass was performed to further clarify the nature of the mass, and metastatic adenocarcinoma tissues were found. The mass was diagnosed as a metastatic adenocarcinoma.
What is the Origin of Adenocarcinoma?
As the carbohydrate antigen (CA) 19.9 level was 367.0 U/ml, above the normal range, the adenocarcinoma cell was believed to originate from the gastrointestinal tract, but no tumor foci were found on gastroscopy, colonoscopy, or whole-abdominal and pelvis enhanced CT. A positron emission tomography–computed tomography (PET-CT) scan was performed and primary lesion was not found, neither. According to abdominal MRI, the mass passed through the longitudinal section of the rectus abdominis and presented as a spindle shape near the subxiphoid laparoscopic scar. As tumors located in the skin are often related to occupational and iatrogenic factors, PMS could not be excluded. A repeat histopathologic examination of the gallbladder was performed at our hospital and revealed adenocarcinoma in the specimen. Therefore, the diagnosis was gallbladder adenocarcinoma with PMS.
What is the Most Suitable Treatment for the Patient?
On the basis of the PET-CT data and given the extensive metastases in the abdomen, a second operation to achieve radical resection was impossible, and the patient was initiated on the GP regimen (gemcitabine, cisplatin), the standard chemotherapy regimen for patients with advanced biliary tract cancer [7].
Discussion and Conclusion
Laparoscopic surgery has been widely accepted to treat benign diseases due to its desirable advantages, such as low blood loss, quick recovery, minimal pain, a short hospitalization time and few complications. Nowadays, a histological examination, which is often performed after surgery, is the gold standard for the diagnosis of benign or malignant tumors. Under these circumstances, the frequency of incidental gallbladder cancer is 0.25%-0.89%, as demonstrated by routine histopathological investigation after LC for benign disease [8-12]. In addition, 50%-70% of patients are diagnosed incidentally with gallbladder cancer based on cholecystectomy specimens for presumed benign indications [13]. The prognosis of IGBC (median OS 32.4 months) is better than that of non-IGBC (median OS 17.2 months), [13] and according to the current guidelines, reoperation, including complete portal lymphadenectomy and bile duct resection, is required for patients with T1b, T2 or T3 disease [14]. Since the first case of PSM was reported as an unusual complication of LC in 1991, [15] many centers have reported similar cases, and the incidence of PSM in IGBC is 10.3% [16]. Most of the metastases are found at the extraction site, [16] showing that few wound protection measures (avoiding bile spillage and using retrieval bags) may cause direct contamination and increase the risk of PSM due to the lack of awareness of possible metastases. Other factors related to laparoscopic techniques, including pneumoperitoneum and carbon dioxide, have been described as risk factors [17-19]. PSM, a manifestation of aggressive disease progression, is generally found 1 to 6 months and as late as 4 years after performing LC [6]. Port-site excision (PSE) has been considered a routine treatment, along with radical reoperation, but it has been demonstrated to have no benefits in improving survival, and recurrence at the wound site may be associated with aggressive tumor biology [20,21]. PSE has shown to benefit patients with PSM without other metastases [22,23]. Chemotherapy is now a common therapy [24]. While it is necessary to investigate a larger group of patients diagnosed with IGBC after LC is performed. PSM is thought to be associated with an advanced T stage and poor histopathological features [3]. The median survival duration is typically 10.3 months [16], while the patient described herein remained alive for 2 years without any treatment after the first sign of a recurrent tumor was found by the patient herself. Whether PSM indicates the aggressive nature of the tumor is still not clear. In addition, a longer follow-up study on patients with PSM is needed.
Activated Protein C (APC) Promotes A Healing Phenotype in Cultured Murine Tenocytes Via Protease- Activated Receptor (PAR)-2, but not PAR-1
Background
Tendon is the connective tissue that transmits the force from muscle to bone to facilitate joint movement. Healthy tendon is comprised of fibroblast-like tenocytes between parallel collagen fibres. Injury to a tendon triggers an ordered triphasic healing response: (i) Inflammation, (ii) Repair and (iii) Remodeling [1]. Hindrance to these sequential stages can halt the healing cascade, leading to tendinopathy.
‘Tendinopathy’ is a non-specific term used to describe pathology in, and/or pain arising from a tendon. Indications of tendinopathy include collagen disorganization, increased cellularity and a poor tendency to heal [2,3]. Tendon injuries cause considerable morbidity in the general adult population [4]. The ideal treatment for tendinopathy is yet to be elucidated and should be focused on elucidating the key functional pathways implicated in the disease [5]. Activated protein C (APC) is an endogenous serine protease of physiological importance due to its potent anti-coagulant, anti-inflammatory and cytoprotective properties [6]. Protein C is mostly produced by the liver and is secreted to the blood where it is activated to APC when bound to the thrombin-thrombomodulin complex. Endothelial protein C receptor (EPCR) can enhance this activation. Once activated, APC exerts either its anti-coagulant activity, or while still bound to EPCR it can cleave protease activated receptors (PARs) to elicit cytoprotective effects via numerous signaling pathways, including inhibition of the nuclear factor (NF)- κB, and activation of the mitogen-activated protein (MAP) kinase and glycogen synthase kinase (GSK)-β3 pathways [7]. PAR-1 and PAR-2 have been found to be vital to cell functions in various body systems including musculoskeletal system [8,9], the nervous system [10], cardiovascular system [11], respiratory system [12,13], as well as the integumentary system [14-24].
In a previous study, APC has been shown to stimulate a healing phenotype in sheep tenocytes via the EPCR [25]. APC increased tenocyte proliferation, matrix metalloproteinase (MMP)-2 activity and collagen type I deposition in a dose and time dependent manner [25]. Additionally, the MAP kinase pathway was proposed to be involved; APC dose-dependently stimulated phosphorylated (P)- extracellular signal-regulated kinase (ERK)-2 and inhibited P-p38 [25]. Whilst APC has been shown to exert some of these effects on tenocytes via EPCR, whether and how PARs are involved remains to be elucidated. Understanding the molecular mechanisms of APC is crucial in maximizing its therapeutic potential in tendinopathy.
Methods
Aim
The aim of this study was to determine whether APC stimulates murine tenocyte healing and if so, to assess the involvement of the receptors and underlying mechanisms in vitro.
Cell Isolation, Culture and Treatment
Three weeks old female wild type (WT), PAR-1 knock out (KO) or PAR-2 KO mice (all are with a C57 background) were bred and obtained from Kearns Facility, Kolling Institute, University of Sydney. 6 mice were used for each gene knockout with a total of 18 mice used. Mice were euthanized by a trained, individually; separate from animal room, in a visible chamber, with 100% carbon dioxide with a fill rate of 70% of the chamber volume per minute. Mice were observed for cessation of respiration within 2 minutes and carbon dioxide flow continued for another 1 minute thereafter. After euthanized, mouse-tail skin was physical peeled back; tendon stripped off and cut into an amorphous mass of small pieces. Tenocytes were extracted from the tail tendon using a 0.2 % Type 1 collagenase digestion medium and then cultured in Dulbecco’s modified Eagle’s medium (DMEM) containing 10 % foetal bovine serum (FBS), 100 U/mL penicillin and 100 μg/mL streptomycin. The unused mouse tissues were cremated and discarded. Confirmation of complete deletion of PAR-1 and PAR-2 at the gene level was further achieved by reverse transcription (RT)-PCR. After confluency, cells were trypsinized, reseeded into individual 24-well culture plates, and grew. When approximately 90 % confluency was reached, cells were switched to serum free DMEM overnight, then changed to fresh serum free DMEN and treated with recombinant human APC (Eli Lilly, Indianapolis, Indiana USA).
After treatment, culture supernatants were collected for zymography and cells were lysed by NET lysis buffer (100 mM NaCl, 1 mM EDTA, 20 mM Tris, 0.5 % Triton X100) supplemented with protease and phosphatase inhibitors (Roche, Sydney NSW Australia) for western blot. Cells from passages 1 to 4 were used in experiments. Royal North Shore Hospital Animal Ethics Committee approved usage of mouse tissues. All experiments were performed three times.
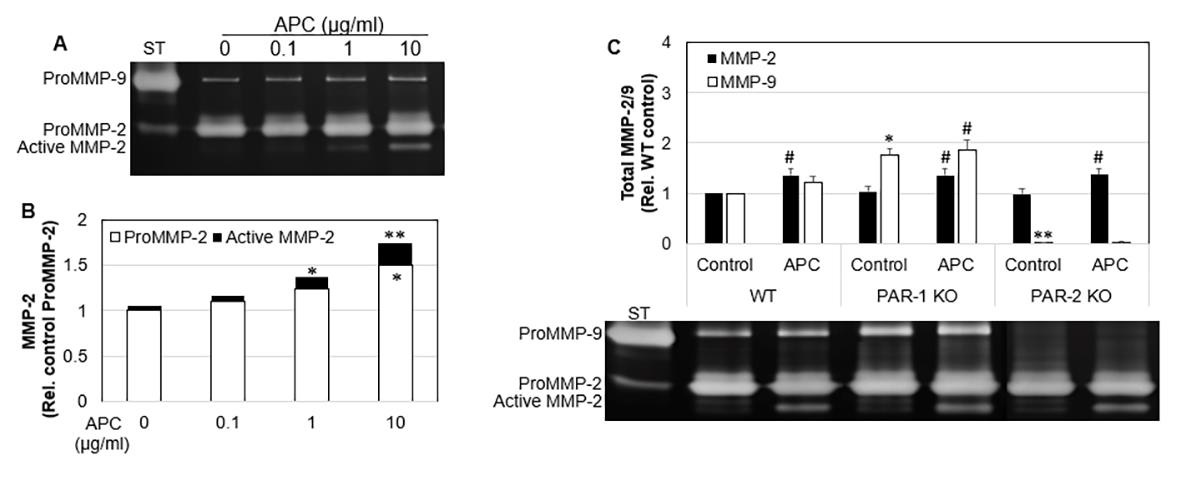
Gelatin Zymography
MMP-2 and MMP-9 protein secretion and activation in the cell culture supernatants were detected by gelatin zymography under non-reducing conditions, as described previously [26]. In brief, the proteins were separated by electrophoresis under non reducing conditions with gelatin retained in the gel. After electrophoresis, the gel was renatured with Triton® X-100, and subsequently developed in an appropriate activation buffer. During this development, the concentrated, renatured MMPs in the gel digested the substrate. After incubation, the gel was stained with Coomassie® Blue, and the MMPs were detected as clear bands against a blue background of undegraded substrate. The clear bands in the gel were then quantified by densitometry.
Western Blotting
The expression and activation of ERK1/2, AKT and GSK-β3 by tenocytes were investigated by Western blotting as described previous [25] β-actin was included to assess equal loading.
MTT Assay
Tenocyte proliferation was assessed by the 3- (4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay. Cells were counted and seeded in a 96-well plate with 200 μl of 10 % FBS in DMEM. After overnight attachment, the medium was replaced with fresh 2 % FCS DMEM and APC treatments were applied. Cells were incubated at 37 °C for a total of 72 hrs. Three hrs prior to termination of the experiment, 10 μl of 2 mg/mL MTT solution was added to each well. After 3 hrs incubation, the medium was removed and replaced with 100 μl of dimethyl sulfoxide. The colour change resulting from the solubilisation of formazan crystals was quantified using a microplate spectrophotometer (BioRad) operating at 570 nm. A baseline reading was also taken at 630 nm to minimize background interference.
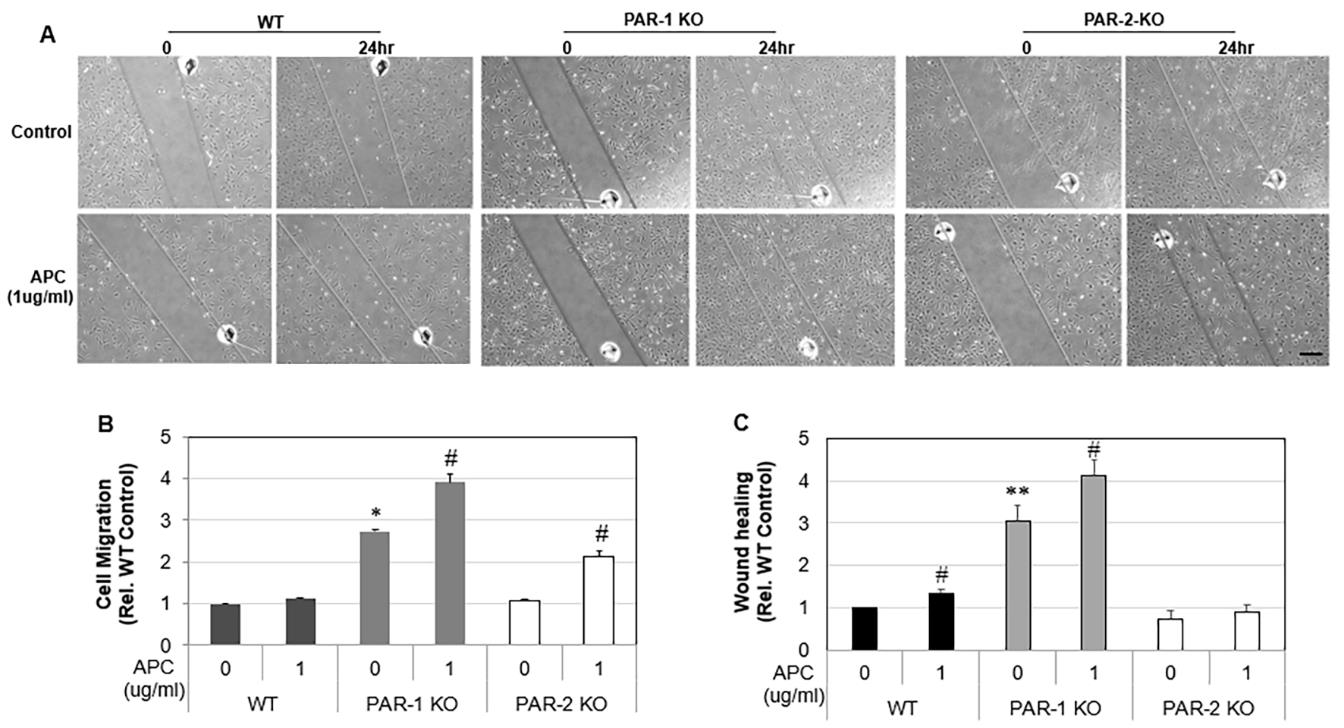
Scratch Wound Assay
Tenocyte migration was examined via a scratch assay. Cells were counted and seeded into 24-well plates and grown to 70% confluency. One vertical line was scratched down the center of each well using the point of a sterile 1 mL pipette tip, creating a cellfree “wound” area approximately 2 mm in width. To standardize the position of the wound when photographing, small indents were made in the well using a sterile 31G needle. Cells were washed twice with 1 mL of media to flush away any suspended cells. Cells were then starved in 2 % FBS DMEM and photos immediately taken. To distinguish the contribution of proliferation to the migration of tenocytes into the “wound” area, cells were pre-treated with mitomycin C (10 μg/mL, Sigma, Aldrich) 2 hrs before “wounding” to inhibit proliferation. Cells were then treated with 1 μg/mL APC and photos were taken again after 24 hr. Cell migration was determined by calculating the fold change of cells that migrated into wound areas in 24 hours by:
mRNA Isolation and Quantitative Real Time PCR
mRNA was isolated using RNAzol RT Isolation Reagent (Molecular Research Center, Cincinnati, OH USA). Primers for EPCR, PAR-1 and PAR-2 were designed and checked for specificity using the National Center for Biotechnology Information BLAST search tool [27]. The murine primer sequences for EPCR (NM_011171.2: 183bp) were 5ʹ′-ATCTGACCCAGTTCGAAAGC-3ʹ′ (forward) and 5ʹ′- GGCCGGAAACTTACAAAAGC-3ʹ′ (reverse); PAR-1 (NM_010169.3; 199bp) were 5ʹ′- ACTTCACTTGCGTGGTCATT -3ʹ′ (forward) and 5ʹ′- GAAACGATCAACGGCACAAG-3ʹ′ (reverse); PAR-2 (NM_007974.4; 164 bp) were 5ʹ′-CCTTACTGCATCTGCCTACG-3ʹ′ (forward) and 5ʹ′- AATGCACTACGAGCAGAAGG -3ʹ′ (reverse). RT Quantitative PCR was performed to determine the amounts of EPCR, PAR-1 and PAR- 2 gene expression in tenocytes from WT, PAR-1 KO and PAR-2 KO mice (The Rotor-Gene 6000 Real-Time PCR machine, Corbett Life Science, Mortlake Australia). Data were analysed using the relative quantification method, and results expressed as fold change (ΔRn) relative to wild type (WT) untreated samples. β-Actin housekeeping gene expression was used to normalize mRNA levels of PAR-1, PAR- 2 and EPCR.
Statistical Analysis
All data was expressed as mean ± standard deviation (SD). Results were analysed using one-way analysis of variance (ANOVA), in combination with and followed by Tukey post-hoc test. GraphPad Prism software was used for statistical computations. A p-value < 0.05 was considered statistically significant.
Results
Gene Expression of EPCR, PAR-1 or PAR-2 in WT, PAR-1 and PAR-2 KO Cells
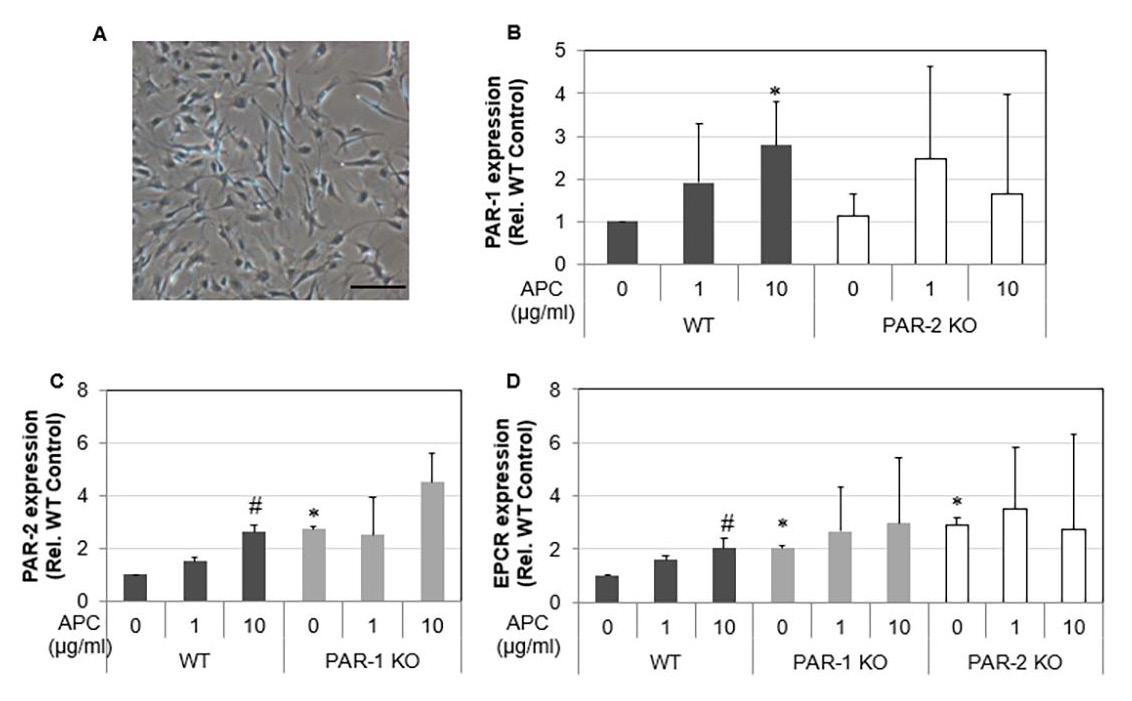
A homogenous cell population was obtained and morphologically identified as fibroblast-like cells. Spindle-shaped contours were observed using inverted phase-contrast microscopy (Figure 1A). Tenocytes from 3 w/o mice demonstrated that, as expected, PAR-1 KO cells had no expression of PAR-1 and PAR-2 KO cells had no expression of PAR-2 (data not shown). Interestingly, expression of PAR-1 by PAR-2 KO cells did not change whereas PAR-2 expression was increased 2.7 folds by PAR-1 KO cells. EPCR expression was stimulated in both PAR-1 KO and PAR-2 KO cells (Figures 1B-1D). In WT cells, EPCR, PAR-1 and PAR-2 expression showed a dose-dependent response to APC treatment. There were 1.6 and 2-fold increases (p<0.05) in EPCR expression in response to APC at 1 and 10 μg/mL, respectively (Figure 1D); a 2.7-fold increase in PAR-1 expression and a 2.7-fold increase (p<0.05) in PAR-2 expression at 10 μg/mL APC by WT tenocytes (Fig. 1B&C). However, the expression of PAR-2 and EPCR by PAR-1 KO tenocytes or the expression of PAR-1 and EPCR by PAR-2 KO tenocytes did not display a statistically significant response to APC treatment (Figures 1B-1D). This data indicates that APC can regulate its receptor expression, while knockout PAR-1 or PAR-2 abolishes this effect of APC.
Figure 1: The gene expression of EPCR, PAR-1 and PAR-2 in WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: Tenocytes at passage 1 from 3 w/o WT, PAR-1 KO and PAR-2 KO mice were treated with APC (1, 10 μg/ml) for 24 hrs. A) Micrograph of tenocytes growing from collagenase digestion tendon at passage 1. Scale bar: 100 μm. B) Gene expression of PAR-1 in WT and PAR-2 KO tenocytes. C) Gene Expression of PAR-2 in WT and PAR-1 KO tenocytes. D) Gene expression of EPCR in WT, PAR-1 KO and PAR-2 KO tenocytes. Quantitative RT-PCR of EPCR, PAR-1 and PAR-2 expression in tenocytes normalized to β-actin. Bars show mean ± SD (n=3). *p< 0.05 vs WT Control and #p< 0.05 vs their own controls, one-way ANOVA calculated using Tukey post-hoc analysis.
Proliferation and Migration of Tenocytes
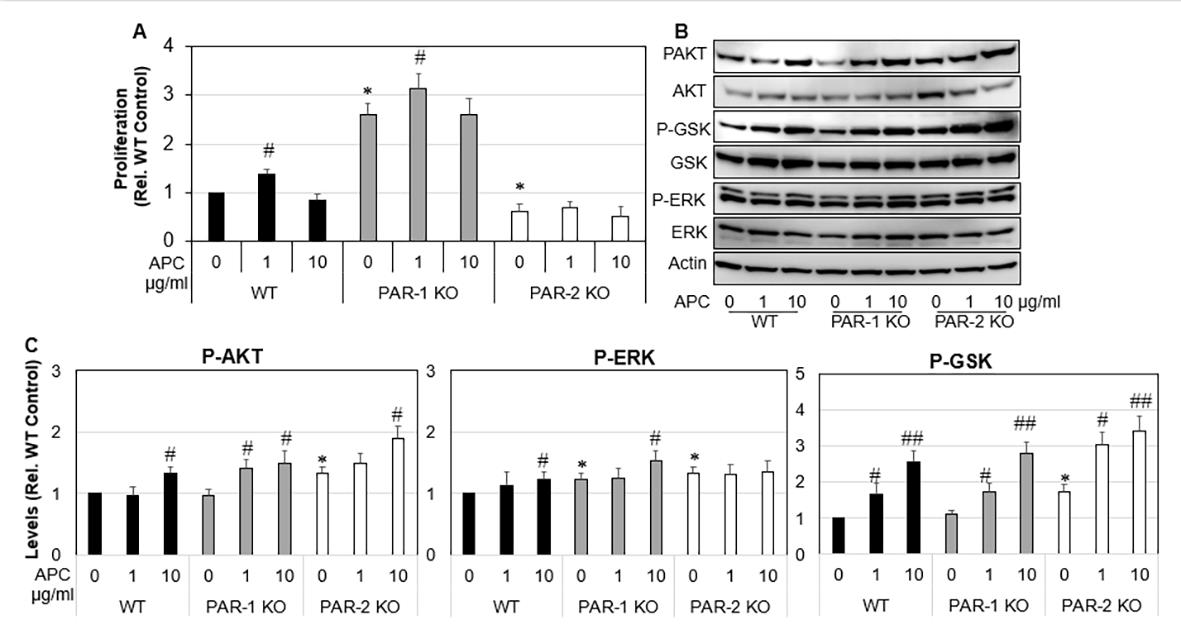
Figure 2: Proliferation and MAP Kinase expression of WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: WT, PAR-1 KO and PAR-2 KO tenocytes were treated with APC (1, 10 μg/ml) for either 24 hrs or 72 hrs. A) Tenocyte proliferation assessed 72 hrs after APC treatment by MTT assay. B) Expression and activation of ERK, AKT and GSK-β3 24hrs after APC treatment detected by Western blot. C) Data are semi-quantitation by Image J and depicted in the graph as fold change relative to control. Results shown are mean ± SD (n=3) *p< 0.05 vs WT Control and #p< 0.05 vs their own controls (no treatment), one-way ANOVA calculated using Tukey post-hoc analysis. ##P<0.01.
Cell proliferation and migration are vital for tendon healing. Under basal conditions, proliferation of PAR-1 KO tenocytes was increased by 3.3-fold compared WT tenocytes (Figure 2A), p<0.0001). In contrast, PAR-2 KO tenocytes showed a 0.6-fold decrease in proliferation when compared to WT control. APC promoted proliferation of WT tenocytes by ~1.3-fold (p<0.05), PAR- 1 KO tenocyte by 1.2-fold (p<0.05) (Figure 2A) at 1 μg/ml when compared to their own controls (Figure 2A). APC had no significant effect on the proliferation of PAR-2 KO tenocytes (Figure 2A). These results suggest that APC dose-dependently promotes tenocyte proliferation, similar to other cells showed previously [28], and this stimulating effect is likely via PAR-2. To investigate the underlying mechanisms, western blot was performed to examine the activation of ERK, AKT and GSK-β3, three intracellular molecules that associated with cell proliferation/survival [7,29-32]. Compared to WT, activated forms of ERK, AKT and GSK-β3 were significantly higher in PAR-2 KO cells (Figures 2B & 2C). APC stimulated the activation of AKT and GSK-β3 in all primary cells, and the activation of ERK in WT and PAR-1 KO cells (Figures 2B & 2C).
Similar to proliferation, unstimulated PAR-1 KO tenocytes showed a 2.7-fold (p<0.0001) increase in cell migration compared to WT cells, whereas PAR-2 KO tenocytes did not differ from WT control. APC (1 μg /mL) had no effect on WT tenocyte migration (Figures 3A & 3B), but stimulated PAR-1 KO tenocyte migration by 1.4-fold (p<0.0001) and PAR-2 KO tenocytes migration by 2.1- fold (p< 0.001), when compared to their own controls (Figures 3A & 3B). Wound healing is a combined effect of cell migration and proliferation. As expected, wounds created in PAR-1 KO cell monolayers healed 3-fold faster than WT cells (Figure 3C), whereas wounds on PAR-2 KO cell monolayers healed at a similar rate to that by WT control. APC at 1 μg/ml promoted ~1.3-fold increase in wound healing by PAR-1 KO and WT by not PAR-2 KO cells (Figure 3C).
Figure 3: Migration and wound healing of WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: WT, PAR-1 KO and PAR-2 KO Tenocytes were treated with APC for 24 hrs. A) Representative images of migration assay. B) Tenocyte migration assessed 24 hrs after APC treatment (1 μg/ml) by a scratch assay. C) Tenocyte wound healing assessed 24 hrs after APC treatment (1 μg/ml) by a scratch assay. Results are expressed as mean ± SD (n=2). Scale bar: 250 μm. *p< 0.05 vs WT Control and #p< 0.05 vs their own controls, one-way ANOVA calculated using Tukey post-hoc analysis. **p<0.01.
MMP-2 and MMP-9 Expression by Tenocytes
MMP-2 and MMP-9 aid the remodeling phase of healing by contributing to the turnover of collagen and extracellular matrix, and cell migration in many cell types [8,33-35]. Gelatin zymographical data showed that WT tenocytes displayed a dose response increase in MMP-2 expression and activation from 0.1 to 10 μg/mL of APC (Figure 4A). There was a 1.5-fold increase (p<0.05) in MMP-2 expression and 1.7-fold increase (p<0.01) in total MMP-2 at 10 μg/mL APC compared to the control (Figure 4A). APC increased MMP-2 in WT, PAR-1 KO and PAR-2 KO. APC had no effect on WT MMP-9, however, increased MMP-9 expression in PAR- 1 KO cells. PAR-2 KO cells showed decreased MMP-9 expression. These findings show APC increases MMP-2 by PAR-1 and PAR-2, however decreases MMP-9 via PAR-1 and increases MMP-9 via PAR- 2 in murine tenocytes.
Figure 4: The expression and activation of MMP-2 in WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: WT, PAR-1 KO and PAR-2 KO Tenocytes were treated with APC for 24 hrs. A) MMP-2 expression/activation in WT cell culture supernatants, detected by zonography. Data are semi-quantitation by Image J and depicted in the graph as fold change relative to control. B) Total MMP-2 and MMP-9 in cell culture supernatants, comparing treatment with APC, detected by zymography. Data are semi-quantitation by Image J and depicted in the graph as fold change relative to control. Results shown are mean ± SD (n=3) *p< 0.05 vs WT Control and #p< 0.05 vs their own controls, one-way ANOVA calculated using Tukey post-hoc analysis. **or ##p<0.01.
Discussion
APC is an endogenous serine protease of physiological importance. It has potent anti-coagulant, anti-inflammatory, antiapoptotic and cytoprotective properties. The therapeutic potential of APC has been demonstrated in wide variety of pathologies including sepsis, wound healing, ischemic stroke, lung disorders, kidney injury, diabetic nephropathy, inflammatory bowel disease, systemic lupus erythematosus, amyotrophic lateral sclerosis and cancer metastasis [36-41]. The therapeutic effects of APC on tendon healing have been far less studied. In the only previous study of tenocytes, APC increased tenocyte proliferation, MMP-2 activity, type I collagen deposition and stimulated a healing phenotype in sheep tenocytes [25]. The actions of APC are largely via binding to EPCR, which subsequently activates PAR-1 [42]. However, APC promoted murine skin wound healing via PAR-2, but not via PAR- 1 [43]. Whether and how APC via these receptors mediates the tenocyte healing phenotype has not previously been investigated. In the current study, we demonstrated that deletion of PAR-1 increased tenocyte proliferation, migration and wound healing, whereas deletion of PAR-2 decreased tenocyte proliferation and has no effect on cell migration or wound healing when compared to WT cells; PAR-1 KO and PAR-2 KO cells exhibit increased EPCR expression; APC enhances tenocyte proliferation, migration and wound healing in WT or PAR-1 KO cells, and had limited effect in PAR-2 KO cells. These data indicate that APC promotes tenocyte proliferation and migration by PAR-2, not PAR-1.
Tenocyte proliferation and migration are vital stages of tendon repair [1]. In this study, PAR-1 and PAR-2 displayed differential functions on these two events in mouse tenocytes. This is consistent with a previous study which showed that PAR-2 knockout mice healed significantly slower than wild-type mice and this delayed healing was not altered by adding APC, indicating that APC acts through PAR-2 to heal murine wounds [43]. Similarly, PAR-2 but not PAR-1 modulates synovial macrophage maturation in posttraumatic osteoarthritic mice and thus may play a critical role in the initiation of patient Osteoarthritis [8], and PAR-2 KO mouse synovial fibroblasts exhibited slower rates of proliferation and invasion of than normal cells [9]. These differential functions of PAR-1 and PAR- 2 have also been found in other types of cells or diseases. PAR-1 activation promotes proliferation of human keratinocytes [14] and dermal fibroblasts [15]. It has been shown blocking PAR-1 inhibits APC-induced proliferation in human keratinocytes and thus PAR- 1 appears to promote anti-apoptotic and neuroprotective effects [16,17]. In contrast, PAR-2 affects keratinocyte differentiation, maintains the epidermal barrier, regulates inflammation [18-22] and pain perception [23], and has a tumor-protective role in the skin [24]. In relation to the nervous system, PAR-1 has been shown to mediate mechanisms underlying astrogliosis, vital after brain injury [10].
In regards to the respiratory system, PAR-1 contributes to protective effects of APC on vascular barrier integrity [12] whereas PAR-2 increases ciliary beating which is vital against inhaled pathogens [13]. Additionally, for the cardiovascular system, PAR-1 KO mice have shown an absence of APC’s protective effects against myocardial ischemia/reperfusion injury via inhibition of apoptosis and inflammation [11]. It was found that APC stimulated murine ectopic bone volume and enhances angiogenesis in a model of Bone Morphogenetic Protein 2 induced bone formation. Mechanistically, APC enhances cell proliferation and activates a number of canonical kinase pathways in a PAR1-dependent manner [44]. In comparison, APC induced PAR-1 signaling was shown to regulate the retention and recruitment of EPCR expressing mice bone marrow hematopoietic stem cells [45]. APC was shown to suppress RANKL-induced human osteoclast differentiation mediated through EPCR, PAR-1, S1P receptor, and ApoER2 [46]. While the noted studies above describe different effects of PAR-1 and PAR-2, it must be highlighted that the outcome of PAR activation by the same protease or synthetic agonist can also vary between tissues and cell types [47]. Therefore, the therapeutic role of APC via PARs extends and differs thorough a number of different studies and cell types.
The remodeling stage of tendon healing is predominantly achieved by tissue-degrading enzymes, MMPs [33,48,49]. MMP-9 degrades the ECM days after injury, while MMP-2 participates in both the ECM degradation and remodeling throughout the healing process [34,50,51]. MMP-2 has been associated with increased angiogenesis in in vitro and in vivo studies, however the role of MMP-9 is less distinct [35]. As a result, APC increasing MMP-2/- 9 activity/expression in PAR-1 KO tenocytes may prove vital in stimulating extracellular matrix degradation, angiogenesis and ultimately tendon healing. Other studies [52] have suggested the APC pathway is a potential target for prevention of MMP-2/-9/-13 activation and cartilage extracellular matrix degradation in patients with OA.
The MAPK pathway is essential in regulating key cellular activities including mitogenesis, motility, and survival in many cell types [7]. Although associated with cancer development, distinct MAP kinases including ERK, AKT and GSK-β3 are essential for proliferation and the normal tissue repair process [30-32]. In previous studies, APC has been shown to cleave PARs to elicit cytoprotective effects via numerous signaling pathways, including the MAPK Pathways [29]. In this study, APC stimulated the activation of AKT and GSK in all 3 cell lines, and the activation of ERK in WT and PAR-1 KO cells. This may help explain why PAR- 1 KO mice showed greater cell proliferation. Another study Xue, et al. [25] found that APC dose-dependently stimulated/inhibited ERK/p38 signaling in sheep tenocytes at 24 hours, respectively. It is feasible that MAP kinase signaling in response to APC is different in different species and at different time frames post treatment, being 1hr in our study.
Since tendinopathy can be both hyper- or hypo-cellular [53], fine-tuning the balance between APC’s interaction between PAR-1 and PAR-2 could help regulate tenocyte equilibrium. These finding could be vital as a large body of evidence suggests the promise of regenerative medicine will be achieved by focusing on augmenting the natural healing response, where little is known about the synergistic and antagonistic interactions of growth factors and perhaps their receptors to produce the best effects [54,55].
Conclusion
We demonstrated that depletion of PAR-1 increased tenocyte proliferation, migration and wound healing, whereas depletion of PAR-2 only decreased cell proliferation and had no impact on cell migration or wound healing when compared to WT cells. Depletion of PAR-1 or PAR-2 increased EPCR expression, but has no effect on either PAR-2 or PAR-1 expression. APC enhanced tenocyte proliferation only in WT or PAR-1 KO cells, not in PAR-2 KO cells; promoted migration and wound healing in PAR-1 KO cells; and increased migration only in PAR-2 KO cells. These findings suggest that APC promotes tenocyte proliferation, migration and wound healing largely by PAR-2, and not PAR-1. APC increases MMP-2 by PAR-1 and PAR-2, however, decreased MMP-9 via PAR- 1 and increases MMP-9 via PAR-2 in murine tenocytes. Overall, APC promotes a healing phenotype in cultured murine tenocytes largely via PAR-2, no PAR-1. By shedding light on APC’s therapeutic mechanistic action through PARs, this work has laid the initial platform in maximizing APC’s potential in improving tenocyte healing and treating tendinopathy.
Asymptomatic Submucosal Lipoma of the Anal Canal: A Report of an Incidental Colonoscopic Finding in an Elderly Patient with Colonic Diverticuli
Background
Lipomas are benign adipose tissue tumors commoner between the ages 40 -60 years and have a preponderance in the male gender [1]. They may be solitary or multiple, superficial or deep in location and are usually asymptomatic. Cosmetic concerns (in larger lipomas), pain or discomfort are the common indications for removal of superficial lipomas and these commonly occur in the trunk, head and neck regions. Deep-seated lipomas are relatively uncommon; they occur in the thorax, retroperitoneum or abdominal cavity [2]. Intra-abdominal lipomas usually affect the omentum, mesentery, the submucosa and subserosa of the gastrointestinal tract (GIT) [3]. Lipomas are the second most common non-epithelial benign GIT tumours after leiomyomas [4]. The most commonly affected region of the GIT is the colon, with the highest incidence at the cecum, ascending colon, transverse colon, and the left colon (in decreasing order as one approaches the rectum) [4]. Occurrence of a lipoma in the anal canal is extremely rare with only one case reported so far by Porta et al in 1979! [5]. In diverticulosis of the colon, there is a transmural outpouching of the colonic mucosa through an area of weakness. This mural weakness-the primary pathology in diverticulosis-is of multifactorial aetiology and the predisposing factors include weakened points of vascular entry into the colonic wall, reduced dietary fiber, hereditary factor, reduced physical activity and obesity [6]. In ventral abdominal wall hernias, stretching of abdominal musculature (because of an increase in its content as seen in obesity) and separation of muscle fibers with weakening of aponeurosis are known to weaken the integrity of the fascia leading to herniation [7]. Whilst the role of mural adipose tissue in the development of GIT diverticula is yet to be established, Yekeler et al have however reported a case of two coexisting rarities- an oesophageal lipoma that resulted in an oesophageal diverticulum due to extramucosal impact of the lipoma [8]. We present an interesting incidental finding of a submucosal anal lipoma in an elderly man who had a concomitant presence of colonic diverticula with an increased submucosal adipose tissue in the vicinity of the diverticuli. This case is reported in line with the SCARE criteria for case reports [9].
Case Presentation
A 70-year-old male retiree was referred for colonoscopy on account of recurrent passage of bloody stool of three months duration, last episode being two weeks earlier. He had no history of anal pain, discomfort, or anal protrusion. There was no change in bowel habit, reduction in stool caliber, melaena, abdominal pain or tenesmus. There was no history of anorexia, haematemesis, early satiety and he does not have a history of peptic ulcer disease. He had no fever, weight loss or any comorbid illness. He had no history of anal trauma or previous anal surgery. No personal or family history of similar illness or malignancy in the past. He was not on any anticoagulation. On examination, he was pale, otherwise other aspects of his general and systemic examinations were normal with a body mass index of 23.1 kg/m2. A pre-procedural rectal examination did not reveal any abnormality. Colonoscopy revealed multiple diverticuli in the caecum, ascending colon and descending colon (Figure 1a) with a 5mm x 3mm sessile polyp in the descending colon. There was a yellowish, oval, submucosal sessile mass (about 10mm x 8mm in widest diameters) with a lobulated surface, about 3cm from the anal verge (Figure 1b). The mass exhibited positive pillow or cushion sign. The mucosa of the transverse colon, sigmoid colon (Figure 1c) and rectum was normal. However, there was an increased yellowish hue to the large bowel submucosa around the anal canal (Figure 1d) and the sites of diverticula (Figure 1e). No stigmata of recent bleeding were seen. The descending colonic polyp was removed with cold biopsy forceps (Figure 2a). The anal submucosal mass was biopsied revealing the characteristic naked fat sign (Figure 2b). The anal submucosal mass was reported to be benign at histology while the descending colonic polyp was reported as an adenomatous polyp with low grade dysplasia. He has been on conservative care for the colonic diverticulum and has remained asymptomatic both for the diverticulum and the anal submucosal lipoma 3 months post colonoscopy.
Figure 1: Colonoscopic findings: a) Caecal diverticuli b) Yellowish submucosal mass of the anal canal c) Sigmoid colon mucosa d) Increased submucosal adipose tissue around anal mass e) Increased submucosal adipose tissue around a sigmoid colon diverticulum.
Figure 2:
a) Site of descending colonic polypectomy
b) Anal mass showing spilling out of adipose tissue following biopsy (naked fat sign).
Discussion
Lipomas are common benign tumour of mature adipose tissue that usually occur in superficial locations – most common location being subcutaneous. The relatively uncommon deep-seated lipomas either present atypically or as incidental findings [10]. In the GIT, they are usually subserosal or submucosal in location, the colon being the most affected region. Involvement of the rest of the large bowel decreases anal-ward. We presented an extremely rare report of a submucosal lipoma of the anal canal with a curious finding of concomitant existence of divertculi at areas of increased submucosal adipose tissue. We discuss this case in terms of rarity and then, its peculiarities. The rarity of this case lies in the fact that it is a deep-seated lipoma occurring in the anal canal. The most distal GIT lipomas reported in the literature are those of the rectum and these presented as polypoid submucosal masses protruding through the anal canal or casuing rectal bleeding [11,12]. Beyond the rectoanal canal, the perianal region, lipomas are also rare with a report of a perianal lipoma occurring years after surgery for a perianal abdscess [13]. The aetiology of the perianal lipoma was likely traumatic, similar to the report by Uscilowska et al on para-anal lipoma resulting from perineal trauma [14]. Beyond trauma, the other risk factors for lipoma formation include genetic predisposition, obesity, hyperlipidaemia and diabetes mellitus [15]. There risk factor for lipoma in our patient was not apparent. This was not a surprise since such deep-seated lipomas are incidentalomas like in our patient. Colonic lipomas are usually asymptomatic except when they are larger than 2cm, torsed, or pendulated. The small size, submucosal location and sessile nature of the lipoma in our patient may explain the asymptomatic nature. The sigmoid colon is said to be the commonest site of colonic diverticulosis, although a study on our patient population by Akere et al revealed right colonic preponderance [16,17] The endoscopic appearance of most colonic diverticuli is that of an outpouching of the mucosa with an otherwise pink-looking mucosa/submucosa due to the rich vasculature of these layers. In diverticulitis, the mucosa of the diverticulum is reddened with or without a surrounding fibrinous slough [18]. The peculiarity of our report is the increased submucoal adiposis in the vicinity of colonic diverticuli, with a predominantly yellowish (than pink) hue to the mucosal color (Figure 1e). These diverticuli involved the caecum, ascending and descending colon with none in the sigmoid colon, the mucosa of which appeared normal (Figure 1c). It therefore stimulates curiosity as to a possible link between increased large bowel mural adiposi and a possible predisposition to subsequent diverticulum formation in the areas where these adipose tissues are located. The plausibility of this link may not be far-fetched if the underlying pathology of colonic diverticulum- mural weakness-is considered. It is therefore more compelling to associate increased submucosal adiposis in our patient with his colonic diverticuli considering the established effect of same adipose tissues on tougher tissues like aponeurosis in abdominal wall hernias. Whilst colonic diverticulosis is commoner in older patients like our patient, Brouland et al reported a large colonic diverticulum in a young male arising due to colonic mural weakness by multiple colonic lipomatosis [19]. The risk factors for colonic diverticulosis include comorbidities (like hypertension and diabetes mellitus), increased luminal pressure (from colonic dysmotility, reduced dietary fiber), genetic risk factors (like Ehlers-Danlos syndrome, Coffin-Lowry and renal polycystic disease), obesity/reduced physical activity, smoking and increasing age [20]. Age alone may not explain the diverticuli seen in our report and none of the other known risk factors was apparent. Although the endoscopic features of the submucosal anal mass we reported were in keeping with a lipoma, histological report did not show the presence of adipocytes. This is a common limitation of endoscopic biopsies where only the mucosal layer is usually biopsied except multiple biopsies are taken at the same spot to include deeper layers. A limitation of this report is our inability to do endoscopic ultrasound which would have confirmed the location of the lipoma. Facility for endoscopic ultrasound is not available in Nigeria as at the time of this report to the best of our understanding.
Conclusion
Lipomas of the anal canal are rare. Although an incidental endoscopic finding in this report, coexistence of large bowel lipomas with increased submucosal adiposis in the vicinity of colonic diverticuli may suggest an aetiological role of such lipomas in colonic diverticulosis.