Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Rectal Palpation Instead of Drug Administration: A Natural Approach to Induce Parturition in Delayed Dairy Cows
Method and Discussion
This case study report aimed to provide an innovative and practical approach to induce parturition in delayed pregnant dairy cattle. Chemical calving induction is a process in which parturition is induced by administrating exogenous hormones and corticosteroids. Having a natural calving, however, is important for optimal health and future productive and reproductive performance of dairy cows. In addition, neonatal calf survival and health can be negatively influenced by any disturbances in the natural calving process. Dystocia and premature calf birth can lead to calf morbidity and mortality due to hypoxia and metabolic acidosis. Chemical induction of parturition was initially performed in beef and sheep production systems [1]. Likewise, in some parts of Australia and New Zealand, calving induction is being used in pasture-based dairy systems with seasonal reproductive programs [2]. These programs are planned to maximize pasture use as an economical feed source. However, induced cows have produced 4% lower milk than those calved normally [2]. Retained fetal membranes is a common consequence of chemically induced calving, predisposing cows to postpartum uterine diseases such as metritis. Therefore, veterinary costs increase following postpartum disorders that may affect reproductive performance of early lactation cows. Health problems associated with chemical calving induction can also affect animal welfare negatively. Because of these issues, The Australian Veterinary Association (AVA) suggests that the induction of parturition should be cancelled in dairy herds with seasonal calving programs. Additionally, the AVA supports gradual remove of chemical calving induction by 2022. Natural calving process may be postponed in some dairy cows, causing oversized calves and dystocia. This is more noticeable in primiparous cows because they have more difficulty in delivering an oversized calf than do multiparous cows. As a result, heifers can be culled because of pelvic injuries during dystocia. Moreover, calf loss may occur during severe dystocia. To avoid these problems, induction of parturition may be a useful practice. In other cased such as downer, lamed, and under-conditioned cows that are unable to calve normally and timely, the induction of calving would be an appropriate way to reduce the risk of sever dystocia and calf loss. Intramuscular injection of corticosteroids such as dexamethasone alone or combined with prostaglandins (PGF2α) are routine ways to induce calving [3]. In the majority of cases, parturition will happen 45-75 hours after injection. However, these methods do possess undesirable health consequences for both calf and dam. As a herd protocol in our dairy herd (Behroozi dairy complex, Tehran, Iran), pregnant animals are allowed to naturally calve between 270-282 d of gestation for healthy calving with no manipulation and pulling of calf. After the above time period and if calving has not yet occurred, cows and heifers are monitored via rectal palpation to check calf survival and probably calf malposition. If the calf is still alive, one more day is given to allow a natural calving to occur. In delayed or prolonged calving (i.e., > 283 d of gestation) in both cows and heifers, induction of parturition will be necessary. Instead of chemical induction with administration of dexamethasone and PGF2α analogues that may cause retained placenta and metritis as well as calf health issues and mortality, rectal palpation and moderate stimulation is practiced inducing natural calving. In our experience, natural parturition usually occurs within one- or two-day of rectal palpation. With this feasible and natural method of calving induction, delayed cows are able to calve naturally without any artificial drug administration. It is necessary to emphasize that during palpation and manual stimulation, calf is modestly moved inside the uterus to induce initiation of the parturition process. In our experience, pushing digital part of calf hooves modestly and gently provide suitable stimuli to help the calf move. After this, calf delivery would be expected to occur within 24-48 hours. Rising cortisol levels immediately before calving has a pivotal role in initiating parturition. Fetal cortisol may be one of the most important physiological modulators that promote parturition in cattle [4]. In addition, maternal cortisol arises as a part of parturition process and stress-like response can be seen during labor [5]. As such, it seems that parturition induction by rectal palpation and manual stimulation of the calf can be a result of fetal cortisol secretion. In other words, we postulate that pushing calf digits in the uterus could induce some degree of stress to the calf which promotes cortisol secretion.
Conclusion
Therefore, to help optimize cow and calf health and productivity, we recommend that the above-explained practicalmanual- natural approach be practiced in delayed cows instead of drug administration.
Perioperative Management of Adolescent Idiopathic Scoliosis: Posterior Spinal Fusion of 14 Segments with a Foreseen Blood Loss of 2000 ML (57 % of Total Blood Volume of the Patient) without Transfusion
Introduction
Adolescent Idiopathic Scoliosis (AIS) is a disease of the spinal column characterized by a three dimensional deformity (coronal, sagital and axial). It has an incidence of 2-3% of the pediatrics population between the ages of 10 and 18 years old, and its treatment is internationally standardized depending on the degrees of the curves, their timeline progression and spinal maturity. The management of curves that have reached a pre-established severity (Cobb angle greater than 40º and have not responded to treatment with an orthesis) is surgical: an instrumental arthrodesis to correct the deformity and prevent deterioration of pulmonary and cardiac function. The most frequent complication of the operation is excessive blood loss. Different surgical and anesthetic techniques have been developed to reduce it. In the case report we present, we combined all the approaches of Patient Blood Management (PBM), starting at the moment of indication of surgery and continuing until the definitive discharge of the patient, to perform a procedure with aforeseen 57% total blood volume (TBV) (2000ml) loss, without recurring to allogenic blood product transfusion. Specific anesthetic and minimally invasive surgical techniques (MISS) were used.
Case Description
We present a 15 years old (50kg, 160cm, body mass index 19,5 kg/m2, total body surface 1.49m2), Latino male with AIS of the thoracolumbar spine (T2-L4) with curves of 78º and 42º respectively, associated with a moderate restrictive – obstructive respiratory insufficiency (FEV1 2,11L (61,5%), FVC 2,74L (62,5%), with a positive bronchodilator test (increase in FEV1 of 11,8% (250ml), whose instrumented posterior spinal fusion (PSF) of 14 segments was performed at our hospital (a national reference center) in March 2021. In May 2019, the patient who was 13 years old at that time, developed a 40º thoracic curve which was initially treated with a permanent plaster brace for 6 months. By November 2019 the curve had progressed to 60º and a new permanent plaster brace was applied. It was ill fitting and badly tolerated by the patient, causing him constant discomfort, and it was changed after three months. At this stage the thoracic curve had progressed to 72º and a 30º lumbar curve developed.
The patient was again braced for 6 months. At the next check up in September 2020, the curves progressed to 78º and 42º respectively. The patient´s orthopedic surgeon recommended to continue with conservative management until the patient turned 16 years old and reached skeletal mature, and then to be operated. The family sought a second opinion as the patient was severely limited in his physical and psychosocial development and was breathless with mild exertion which prevented him from participating in activities with his peers. He had pain when remaining in the same position for a period of time and had difficulties with daily hygiene as he lived in a hot climate. Photos of the patient at presentation to our hospital X-rays of the patient at presentation to our hospital When the patient presented at our hospital in January 2021, the orthopedic surgeon in charge deemed the futility of the brace and indicated preferrential surgical treatment.
The thoracic curve progressed to 100º, the patient had dispnoea with mild exercise and great discomfort and limitations because of the brace. He was placed on the waiting list and went through the first preanesthetic assessment. Of significance was a hemoglobin (Hb) 12,6g/dl, hematocrit (Hct) 38%, microcytosis, hypochromia and a total protein count of 5g/dl. Respiratory function tests revealed a moderate restrictive-obstructive component to his limitations which responded well to bronchodilators. Echocardiography and cardiac function testes were normal. We initiated PBM with oral Ferrous Sulphate 105 mg daily (to be taken on an empty stomach with a glass of orange juice 30 minutes before breakfast), supplementation with a multivitamin complex, vitamin B12, Folic Acid and a puffer of Salbutamol (inhalation suspension 100mcg/dose) as needed. Recommendations were also given to increase the overall caloric and protein intake and the patient was given instructions for prerhabilitation exercises.
There was a delay with the waiting list because of the COVID pandemic situation, with cancellation of physical presence consultations and all surgical procedures, except emergency and oncologic operations. Three months later, in March 2021, the patient came back for a second preanesthetic assessment (two weeks prior to his operation). He was tolerating the oral iron supplementation with no digestive issues and was using the bronchodilator two to three times a day. The blood test revealed Hb 15,7 g/dl, Hct 45,6%, Fe 126mcg/dl, Fe saturation index 36%, Transferrin 277mg, Ferritin 43ng/ml, Vitamin B12 442pg/ml, Folic Acid 5,65ng/ml. The rest of the consultation results were satisfactory. The patient was scheduled for a14 vertebrae instrumental arthrodesis via posterior approach with autologous and donor bone grafts and Ponte osteotomies. We calculated the foreseen intraoperative blood loss according to the orthopaedic surgeon´s predictions based on his 25 year experience with these operations: 80 +/- 40 ml per vertebral space fused and up to 150 ml for each Ponte osteotomy (approximately 2000ml total).
On the day of the operation a combination of Total Intravenous Anaesthesia (TIVA) (induction with Midazolam, Fentanyl, Atracurium and Propofol, maintenance with Propofol, Fentanyl and Remifentanyl, without muscle relaxant to permit neurophysiology monitoring) and a Morphine spinal for postoperative analgesia (due to an impossible lumbar puncture by the anesthesiologist, this was administered by the surgeon under direct vision during the operation: Morphine Chloride 3mcg/kg (total dose 150mcg). Antibiotic prophylaxis was administered with Cefazolin 1g IV at induction and repeated after 4 hours during the operation. This was continued at 8 hourly intervals for the first 48 hours postoperative. Preemptive analgesia was provided with the administration of IV Dexamethasone 8mg and Dexketoprophen 50mg. Full standard ASA monitorization was applied. After induction, and while the neurophysiology monitoring was being placed, acute hypervolemic hemodilution (AHH) was slowly started with 2000ml of Gelafundin®. Central venous access was secured by cannulation of the right internal jugular vein; the right radial artery was cannulated for close hemodynamic monitoring and frequent blood tests.
Bladder catheter was inserted for fluid balance control and a nasogastric tube was placed to empty the gastric chamber. The patient was placed in prone position on a special scoliosis operating table, taking care to protect all the pressure points and decompress the abdomen in order not to cause excessive filling of the epidural veins which would increase the intraoperative bleeding. Head (3kg) and lower limb (5kg) traction was applied and the table was placed in a mild Trendelenburg position. Strict normothermia was observed during the whole procedure by employing convective air blankets to exposed body parts and warmed IV fluids. Core temperature was monitored throughout surgical time. The first blood test was done before incision revealing Hb 13,2 g/dl and Hct 42% which reflected the results of the AHH. The fluid reposition and maintenance continued at the anaesthesiologist´s discretion (Lactated Ringer solution 2000ml). Intravenous Tranexamic Acid (TXA) was administered as a loading dose of 15mg/kg and continued with a 2mg/kg/h infusion for the duration of the operation.
The OrthoPAT® (Haemonetics), an autologous cellsalvage and transfusion system, was set in place. After skin incision (T2 to L4), subperiosteal dissection of the paravertebral muscles to the tips of the transverse processes of all the vertebrae to be fused was performed under controlled hypotension (mean arterial pressure (MAP) 55 mmHg). Once the curve correction stage was reached, the patient was returned to normal MAP (65-75 mmHg) to prevent ischemia of the neural tissues during distraction, rotation and stretching manoeuvres of the corrective screws and rods which were done under continuous neurophysiology monitoring (somatosensory evoked potentials, motor evoked potentials, screw placement potentials). Before closure, 1g of Vancomycin was mixed together with the bone graft shreds and distributed directly over the open operating field. Another blood test revealed Hb 11,2 g/dl, Hct 36%. An atmospheric pressure drain was placed.
At the end of the procedure which lasted 7 hours, a third blood test revealed Hb 10,2 g/dl and Hct 33%. The anaesthesiologist reinfused the blood recuperated by the OrthoPAT® (350ml). The patient was placed in the supine position and extubated before transfer to the Pediatric Critical Care Unit (PCCU). A loading dose of postoperative analgesia with Paracetamol 1g and Metamizol 2g IV was administered. There were no intraoperative complications. On admission to the PCCU the patient was hemodynamically stable and in sinus rhythm. Respiratory mechanics were correct with 100% SpO2 with Ventimask® O2 at 6L/min. The patient was fully conscious and had no pain. Post OrthoPAT® blood infusion test revealed Hb 12,6g/dL, Hct 36,4%. The following 24 hours were uneventful. Analgesia was continued with IV Paracetamol and Metamizol. On discharge from the PCCU at 24 hours postoperative Hb was 11,8 g/dL and Hct 35,9%, drain yield 170ml. He was transferred to the childrens´ orthopedic ward for further care.
The first dose of Patient Controlled Analgesia (PCA) with Morphine was required at 36 hours postoperative when patient mobilization was initiated. The drain was withdrawn at 48 hours with a 200 ml yield. The patient started early deambulation. The postoperative period was satisfactory, except for continued serohematic oozing from the lower third of the incision which required reinforcement with surgical stapling. There were no hemodynamic, respiratory, infectious or neurological complications. The patient was discharged home on day 8 with oral analgesia (Paracetamol and Metamizol). Blood workup before discharged revealed Hb 9,3 g/dl. A single dose of IV Ferrous Carboxymaltose 1000mg (20mg/kg) was administered.
On day 12 the patient presented to the Emergency Department because of sustained bleeding from the lower third of the wound. His Hb dropped to 8,9 g/dl (nadir) and he felt tired, weak and dizzy when standing up, with no syncopal episodes or breathlessness. He was admitted for surgical revision of the bleeding and bed rest. There were no signs of infection. When the wound was clean and the bleeding had stopped the patient was discharged home. Another dose of IV Ferrous Carboxymaltose (1000mg) was administered. On a revision visit two weeks later he was subjectively well, sitting and deambulating without pain, the wound looked clean and was healing well. Staples were removed. Blood test was Hb 11,1g/dl and Hct 35,4%, Iron 62mcg/dL, Transferrin 227mg/dL, Ferritin Saturation Index 19%, Total Iron Transport Capacity 320mcg/dL and Ferritin 838ng/mL. The patient was instructed to avoid sports for three months and was advised to start aerobic exercise after that. Contact sports were to be delayed six months. He was scheduled for follow up in 6 months. The surgical results were surgically and esthetically satisfactory, and the patient and his family were very happy with the outcome.
Discussion
AIS is a frequent disease of the pediatric population [1-3]. Most cases are managed conservatively with active observation. In progressive cases bracing is applied. When the pathological angles progress rapidly and significantly, surgical management is indicated. Different operative techniques and instrumentations are in use depending on the surgical team´s training. The most frequent complication of extensive AIS surgery is excessive perioperative blood loss, requiring transfusion in up to 70% of the cases [4]. Attempts have been made to standardise the estimation of and predict the perioperative blood loss [5-8]. An exact formula is elusive as many factors are involved. The ultimate volume differs depending on the surgical and anaesthetic teams´ techniques and experience. The RBC transfusion rate is higher in males, lower preoperative Hb, greater deformity angles, larger numbers of vertebrae to be fused and duration of the operation. Our patient had all of the risk factors.
Knowing this and planning appropriately can help avoid blood product transfusion. It is well known that although blood transfusions are life saving in many cases, this however comes with a high price (immunomodulation side effects, metabolic disorders, induced coagulopathy, increased surgical site infections, pulmonary complications, increased length of hospital stay and overall costs per case, as well as complications associated with transfusion errors, adverse reactions and the possibility of infective agent transmission) [9-14]. PBM addresses all these issues and was scrupulously applied by our team as soon as the patient was placed on the waiting list for surgery. We had 3 months of preparation time and we used all techniques available pre, intra and postoperatively. Careful calculation of the predicted perioperative blood loss, taking into consideration hemorrhagic complications and possible contingencies.
• Perioperative red blood cell (RBC) mass optimization [15] with oral and IV iron supplementation. The use of bone marrow stimulating agents such as human recombinant erythropoietin was considered but deemed unnecessary in this case.
• Restrictive RBC transfusion trigger (in healthy ASA I pediatric patients a Hb nadir of 7g/dl, depending on anemia tolerance, can be accepted).
• AHH [16-20] to decrease the RBC loss by lowering the Hct of the blood lost from the operating field. Clinical studies support improved hemodynamic stability and optimization of central venous pressures in patients who undergo this technique under general anaesthesia. AHH promotes an increased heart preload, improves the rheological properties of the circulating blood and coagulation is not affected when the technique is done properly. Employing gelatins in the process maintains the effects for an estimated t½ of 6 hours, which is appropriate for the duration of the surgical procedure.
• TXA [21-25] (an antifibrinolytic) counteracts the hyperfibrinolysis that develops during the surgery due to extensive bone and muscle tissue trauma.
• Controlled hypotension during the dissection phase to decrease the blood lost during the bloodiest stage of the operation. It is important to return the patient to normotension during the traction and torsion stage to prevent possible ischemic damage to delicate neural tissues. The controlled hypotension technique has been shown to safely and significantly decrease autologous transfusion rate [26,27].
• Proper patient positioning on the operative table (decompressing the abdomen to avoid epidural vein engorgement, applying protection to pressure sites and placing the table in moderate Trendelenburg to favour adequate venous drainage and prevent the blood pooling in the operative field).
• Maintaince of normothermia with convective air blankets and warmed IV fluids to prevent hypothermia induced coagulopathy during prolonged surgery times (in our case 7 hours duration).
• The use of intraoperative cell salvage [28-30] with a system like the Harmonics OrthoPAT® system which is able to recuperate up to 70% of the blood in the intraoperative field, wash and concentrate the blood recovered and make it safe for returning it to the patient via the IV route.
• Careful hemodynamic and bispectral index monitoring to aid appropriate anaesthetic dosage.
• Neurophysiological monitoring to prevent possible neurological complications
• Meticulous hemostatic surgical strategy, MISS and experienced surgeons [31,32].
At our institution, the use of expensive OrthoPAT® technology is authorised for surgical procedures where the foreseen blood loss exceeds 30% of the total blood volume (TBV) of the patient as only then does it become cost effective compared to autologous blood product transfusions. In our case we calculated our patient´s TBV by using the 70ml/kg estimation (adolescent 50kg male: 3500ml TBV). The predicted blood loss was 2000ml, corresponding with 57% of TBV. We calculated the allowable blood loss (ABL) for a minimal Hb of 7g/dl according to the formula:
ABL = TBV.( preopHb − nadirHb) / preopHb
Where TBV = 3500 ml
Preop Hb = 15,7g/dl
Nadir Hb = 7g/dl
The ABL result was 1940ml.
We took into consideration the reinfusion of RBC recuperated from the operative field by the OrthoPAT® to allow for a margin of hemorrhagic complications and contingencies. Finally, 350ml of concentrated RBC was generated and reinfused at the end of the operation when Hb of 10,2g/dl was reached, raising the post infusion Hb to 12,6 g/dl. PBM was continued until the definite discharge of the patient. Because of persistent wound serohematic discharge, the patient´s Hb decreased leading to mild anaemia symptoms but never reaching the preestablished transfusion trigger. IV iron supplementation was used to speed up the recovery of RBC mass and aid in symptom tolerance.
Conclusion
With careful planning and conscientious application of PBM strategies, we were able to perform this complex and high risk surgical procedure without recurring to autologous RBC transfusion. The experience of the managing team and continued close communication between surgeons and anesthesiologists makes bloodless surgery of difficult AIS cases possible. The reporting and dissemination of Case Studies such as this one, may help in the management of similar situations by other teams at health institutions worldwide.
Minimally Invasive Rehabilitation Techniques for the Endodontically Treated Tooth – A Case Report
Introduction
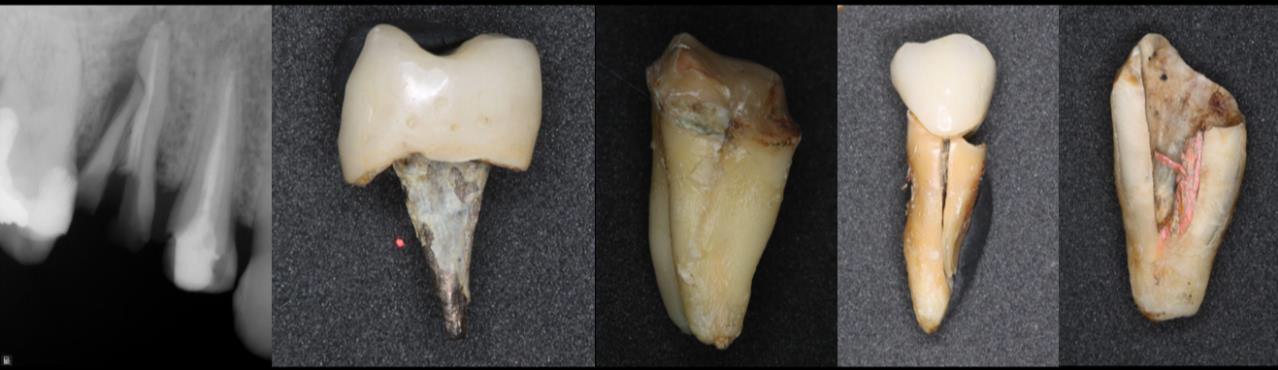
Today, the options available to restore an endodontically treated tooth with great loss of dental structure are limited. In most cases, the traditional approach is chosen to rehabilitate the remanent with the use of a post and crown. However, it is necessary to prepare the tooth prior to treatment, which reduces the amount of already limited dental structure. The objective of this case report is to describe a minimally invasive rehabilitation treatment option in an endodontically treated anterior tooth (ETT).
Case Report
Figure 1: Example of catastrophic failure.
Female patient, 54 years old, was referred for the rehabilitation of ETT 2.2. The tooth was endodontically treated, restored, and double sealed 2 weeks prior.After removing the previous restoration, the Clearfill SE® 2-step self-etching adhesive protocol was used (Figures 1-6). Then, EverX Flow® flow resin with a 2mm x 6mm piece of Interlig® reinforced fiber were used. The coronal area was restored with z350 resin using a silicone key layering technique (Putty speedex®). Control and polishing were later carried out (Figures 7-11).
Figure 2: Initial.
Figure 3: Rx Initial.
Figure 4: Isolation Split Dam.
Figure 5: Resin Removal.
Figure 6: Materials.
Figure 7: Interlig.
Figure 8: EverX Flow Resin.
Figure 9: Silicon matrix.
Figure 10: Restauración Final.
Figure 11: Rx Control.
Discussion
evidence shows that the use of cast or fiber posts to rehabilitate ETTs presents a high risk of medium- to long-term biomechanical failures, due to the great loss of dental structure [1]. In addition, cast posts have a greater tendency to microleakage [2]. Fiber posts are preferred over cast posts owing to their lower risk of catastrophic type fractures [3].Multiple studies reach consensus that the ferrule effect is one of the most important factors in determining the rehabilitative success of endodontically treated teeth, and that the posts material choice does not show statistically significant differences when a ferrule effect exists [4-7].
It has been reported that ETTs treated with reinforced glass fibers can have an increased fracture resistance compared to the ones rehabilitated with fiber posts at different lengths. However, it is not yet possible to guarantee more favorable fracture patterns with the use of reinforced glass fibers over conventional techniques due to the limited amount of evidence available.
Conclusion
1. It is essential that dental professionals are familiar with the different treatment options available in order to carry out the most effective treatment for the case. The judicious use of posts in ETTs should be emphasized in order to preserve healthy dental tissue when possible.
2. The restoration after fiber reconstruction can be either direct or indirect, which will be determined by the clinical situation and the individual characteristics of the case at hand. There is need for more evidence considering rehabilitative alternatives on fiberglass stumps in ETTs.
3. It is advised that long-term studies be conducted evaluating clinical performance of fiber-reinforced ETTs, as well as shortterm ones comparing fracture types in ETTs that have been either fiber-reinforced or rehabilitated with a fiber-glass post.
Chiropractic Instrumental Manipulation in the Lower Back: A Systematic Review
Introduction
Low back pain (LBP) is defined in the literature as pain located below the ribs that goes to the inferior gluteal folds [1]. LBP is pragmatically classified as non-specific or specific. Nonspecific LBP is defined as low back pain when there is no clear relationship between symptoms, physical findings and imaging findings [2], and represents 90-95% of low back pain cases [3]. The estimated point prevalence of nonspecific LBP is 18% [4], affects people of all ages and is a major contributor to the burden of disease worldwide [5]. As nonspecific LBP has no known pathoanatomical cause, treatment focuses on pain reduction and its consequences [6]. Pain management approaches vary widely [7]. Non-steroidal anti-inflammatory drugs, opioids and neurotropic drugs or steroid injections and surgery are the main tools used in treatment [8]. Another approach method for the treatment of non-specific low back pain is chiropractic instrumental manipulation therapy [9]. This technique is a chiropractic method that uses an instrument to replace the therapist’s hand, being the second most used technique in the world, which provides the same results and benefits as the manual method, with the advantage of being more comfortable and safer for the patient [10]. Chiropractic instrumental manipulation is used by chiropractors for the treatment of acute pain in the lumbar and sacral region [11].
The literature has a limited amount of information about the role of chiropractic in treating LBP. Appropriate and carefully performed manual manipulation of the spine has been used to care for many of these patients [12]. However, depending on the nature and extent of the patient’s pain, the high velocity, low amplitude (HVLA) force of manual manipulation, may present an undesired risk of aggravation or be completely inappropriate [13]. Chiropractic Instrumental Adjustment may offer an adequate and effective therapeutic approach in certain types of these cases due to the low strength and site-specific nature of the manipulative impulses that can be delivered to the spine with a manual adjustment instrument [14]. This instrument allows chiropractors to provide a quick, low strength thrust at specific points [15]. This systematic review aims to assess the result of the instrumental manipulation chiropractic therapy in LBP.
Methodology
Search Strategy
(((Chiropractic[mh] OR Chiropractic[tiab]) AND (Back Pain[mh] OR Low Back Pain[mh] OR Back Pain*[tiab] OR Backache*[tiab] OR Low Back Pain*[tiab] OR Lower Back Pain*[tiab])) AND (Effectiveness[tiab] OR Efficiency[tiab] OR Treatment Outcome[mh] OR Treatment Outcome[tiab] OR Efficacy[tiab] OR Effect*[tiab] OR Assessment[tiab] OR Evaluation[tiab])) AND (English [lang] OR Portuguese [lang] OR Spanish [lang]) AND (“2016/01/01”[PDAT]: “2021/04/20”[PDAT]
Eligibility Criteria
The studies included in this review must: (i) Use instrumental manipulation chiropractic therapy, (ii) Written in English, Spanish, and Portuguese, and (iii) That speak of the Low back pain. Excluded articles that were duplicates, comments, letters, abstracts of congresses, books, book chapters, systematic reviews, and meta-analyses or narrative reviews and that do not use instrumental for manipulation. Also besides, articles that do not address pain in the low back spine.
Methodological Quality
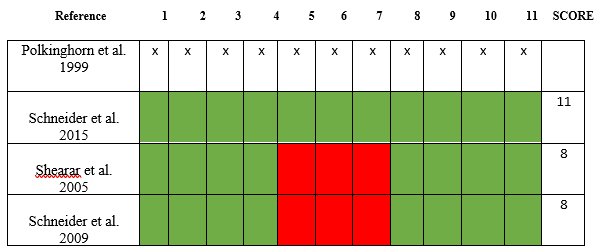
The methodological quality of the articles assessed using the PEDro scale (Physiotherapy Evidence Database) which tests the effectiveness of therapy interventions. On this scale, there are 10 criteria established based on an “expert consensus” and not on empirical data. The score awarded only when a criterion is satisfied. Publications with a score of seven or more on the PEDro scale considered to be of ‘high’ methodological quality, those with a score of five to six would be of ‘regular’ quality, and a score of four or less classified as “poor” quality [16].
Risk of Bias
The risk of bias was assessed in the studies selected according to the Cochrane risk of the bias assessment tool [17]. According to the instrument, for each work, different domains related to the risk of bias were assessed independently.
Case Report (CARE)
The CAse REport (CARE) guidelines checklist is structured to correspond with key components of a case report and capture useful clinical information. This 13-item checklist provides a framework to satisfy the need for completeness and transparency for published case reports [18].
Results
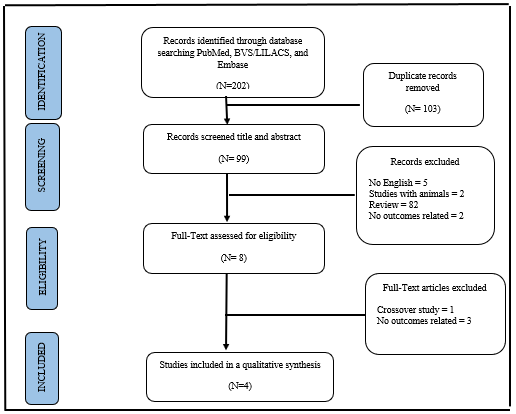
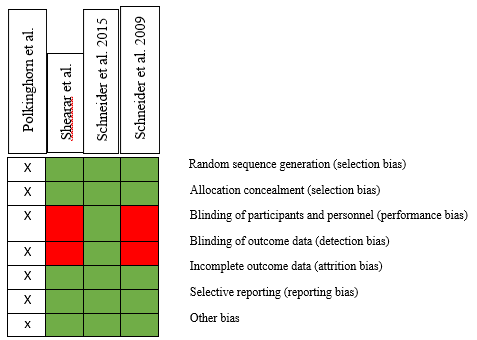
A total of 202 studies were identified through a database search and, after the removal of duplicates, 99 studies were identified. During the screening process, 189 publications were excluded for not being related to the research question and the full text of nine studies was reviewed in detail. Finally, four randomized control studies were included in the systematic review. The selection process is schematized in (Figure 1). The included studies had a mean score of six when assessing the methodological quality with the PEDro scale (Figure 2), with a minimum of 5 points and a maximum of seven, evidencing moderate methodological quality. Detailed description and results of the included studies are presented in Table 1. All studies [19-21] were designed as randomized controlled trials. The risk of bias of included studies was assessed with the Cochrane risk of bias tool (Figure 3). To analyze the case study article, we used The CAse REport (CARE) guidelines checklist (Figure 4).
Figure 1: PRISMA flowchart with the different stages of the current systematic review.
Figure 2: (1) Methodological quality assessment of the included studies with PEDro scale. (2) Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received); (3) Allocation was concealed; (4) The groups were similar at baseline regarding the most important prognostic indicators; (5) There was blinding of all subjects; (6) There was blinding of all therapists who administered the therapy; (7) There was blinding of all assessors who measured at least one key outcome; (8) Measures of at least one key outcome were obtained from more than 85%; of the subjects initially allocated to groups; (9) All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat”; (10) The results of between-group statistical comparisons are reported for at least one key outcome; (11) The study provides both point measures and measures of variability for at least one key outcome. The Polkinghorn et al. 1999 as a case study, it does not fit this criterion.
Figure 3: Risk of bias summary: authors assessment for each risk of bias criterion. The Polkinghorn et al. 1999 as a case study, it does not fit this criterion.
Figure 4: Case Report (CARE) guidelines.
Discussion
The aim of this review was to analyze the results of the treatment of patients with pain in the lower region of the spine (lumbar, sacroiliac and coccyx) using chiropractic instrumental manipulation technique. For this, we selected a case study [21], a cohort study, a randomized trial and a randomized clinical trial [21]. The Polkinghorn et al. because it is a case study, it was not evaluated using the PEDro methodological quality scales and the Cochrane risk of bias tool. The other three articles were evaluated and their methodological quality by the PEDro scale obtained a score of 8 and 15 for Schneider et al. 2015. Due to the risk of bias, Schneider et al. Obtained the low-risk result, and the other 2 articles obtained a medium risk of bias with a score of 7. In CAse REport (CARE) guidelines, Polkinghorn et al. got a good evaluation with a score of 12. Although there are several articles [22-24] in the literature that present studies on this technique, there is still a need for more research on this method. In this review, we were able to assess that in terms of clinical efficacy, chiropractic instrumental manipulation found statistically positive results for pain, although the differences between the protocol and the application of the technique were not the same in the four studies addressed. In summary, the articles that investigated the use of the instrument in manipulation only reported that it brought clinically significant benefits to patients. The results of this study may provide useful information for clinicians and patients in terms of therapeutic efficacy for treating patients with back pain without the risk of manipulation of the lumbar spine, sacro-coccygeal.
Level of Adherence to COVID-19 Preventive Measures: Case Study of FUTA Shuttle Bus
Introduction
Since the beginning of the 20th century, the world has witnessed several crises which are epidemic and endemic. In the year 1918- 1920, the Spanish Flu is popularly known as Influenza occurred and affected about one-third of the world population. In the 21st century, there were disruptive events such as the 9/11 terrorist attack that occurred at Pentagon, the SARS outbreak that occurred in the year 2003, the global economic and financial crisis that occurred between 2008–2009, the Middle East Respiratory Syndrome (MERS) outbreak that occurred in the year 2015, and the latest Covid-19 are known to have negatively affected the world economy. The recent novel (2019-2020) Coronavirus (Covid-19) endemic was originated from Wuhan, China in December 2019. It is an acute respiratory infectious disease. Qiu et al. (2017) noted that it was confirmed an endemic by the World Health Organization (WHO, 2019) because of its rising human-to-human infection resulting in more than 200,000 deaths within three months ever since the beginning of the outbreak WHO [1]. As of 2nd September 2020, it has been reported in 213 countries and has resulted in approximately 862,234 deaths Worldometers 2020. Liu, et al. [2] noted that surprisingly, the Covid-19 infection and deaths recorded the highest rate when numerically compared to other coronavirus outbreaks like SARS-CoV, MERS-CoV, and Influenza.
Previous studies of Sohrabi, et al. (2020), Chinazzi, et al. (2020), Smith and Freedman (2020), and others have disputed that movement restriction and control is the best method to managing and curbing the spread of such diseases. Therefore, many countries including Nigeria enforced social distancing, travel restrictions, and rescheduling of events (such as a wedding, burial) for at least 2 weeks in their respective countries. In many countries, the emergency unit also referred to as a quarantine unit was set up for curbing the spread of coronavirus. The aftermath of this order was felt on human psychology such as anxiety, stress, and depression (Ghani, 2020), and on socioeconomic activities such as the temporary shutting down of retail shops, retail premises, and interruption of product delivery (Karabag, 2020). In Nigeria, the 14th day’s travel /movement restriction order which started from 30th March 2020 till 27th July, disrupted the operation of many small and medium enterprises including the agriculture, retails, food and beverages, construction, tourism, and transport sectors. Before focusing on the impact and strategies for reducing the impact of Covid-19 on the operations of the FUTA shuttle bus operation, it is pertinent to be aware and conscious of the explanation of the crisis. According to Booth (1993), a crisis is a condition that is experienced by an individual, or group which they find difficult to cope with using normal habitual measures. Booth further identified three types of crises, which are: Gradual threat, Periodic threat, and sudden threat.
The Covid-19 crisis can be known to be a sudden threat because the crisis came up suddenly and affected all organizations and sectors of the economy including the bus operators. Hence, they must be able to manage the crisis. Nonetheless, little is acknowledged and evaluated about the adherence to Covid-19 safety rules and personal preventive measures, such as physical distancing, use of mask, hand and cough hygiene, in bus operation. Understanding the level of adherence is essential for the containment of the Covid-19 epidemic in the long term. On this note, this study assessed the level of adherence regarding the Covid-19 preventive measures suggested by the government. The Covid-19 endemic has up till now had a significant impact on people’s mobility at the local, national, and international levels. As a result of the endemic, stringent interventions, such as travel restrictions, remote work, lockdowns, and sensitization were imposed, and have affected the operation of passenger transport. Research reveals that physical distancing policies are effective in minimizing the spread of the virus Islam, et al. [3]. Nonetheless, distancing has been established to be indeed challenging in some situations and for some groups of people. This is undeniably the case with public transport, especially the FUTA shuttle bus.
The brisk spread of the Covid-19 virus, which became a worldwide endemic as of the year 2020, was attributed to the hypermobility, globalization, recent lifestyles, and the accessibility and connectivity of citizens in Wuhan, the first epicenter Musselwhite, et al. [4]. Since then, the Covid-19 endemic swiftly evolved into a condition that is labeled with profound effects on spatial interaction (mobility dynamics), lifestyle, and social integration. Most of the long, medium and short distant movements were minimized worldwide, leading to an unprecedented increase in tele-working. These impacts emanated from governmental measures (majorly travel restrictions) as well as individual choices to refrain from traveling to minimize exposure to other people and the risk of contamination. There is a drastic reduction in urban travel across the world, though not uniformly for all modes, as the hardest blow of the endemic was felt on public transportation (Molloy et al., 2020; Astroza et al., 2020). Because of the unavoidability of public transportation especially for the low-income earners and the fact that it provides door-to-door service, there is a perception that public transportation has more risk than private means of transport. In Nigeria, after the ease of lockdown and the provision of the necessary equipment that is necessary for preventing the spread of Covid-19, the tertiary education resumed activities and students travelled down from their respective locations. Also, shuttle bus operators resume operations on various campuses, but assessment level of adherence to and satisfaction of passengers to shuttle bus operations in the tertiary institutions regarding the Covid-19 preventive measures have not been well-researched, and none have been conducted on the campus shuttle of the Federal University of Akure (FUTA).
FUTA shuttle bus operation’s purpose is to provide an affordable, accessible, and sustainable transport mode for most people in the FUTA community which be jeopardized by the need to guarantee physical distancing. In this context, FUTA shuttle bus authorities and operators face the unprecedented challenge of maintaining adequate levels of service while upholding the health of users and workers and, at the same time, dealing with harsh economic instability. This study assessed the level of adherence to the Covid-19 preventive measures suggested by the government on the campus shuttle of FUTA. It addressed these main questions: What is the level of adherence of FUTA shuttle bus operators to compulsory hand rinsing, physical distancing preventive measures, and passengers’ wearing of a nose mask and or face mask in FUTA shuttle bus? There is no sureness that new waves of extensive infection will not emerge after the first crisis; hence, there is a need for proper management of preventive measures especially in the situation that involves gathering of a group of people. The study is pertinent because it gives room for a better understanding of the level of adherence regarding the covid-19 preventive measures suggested by the government on the campus shuttle of FUTA. Furthermore, the study will reveal the extent to which the FUTA shuttle buses were able to adhere to the covid-19 measures after the movement lockdown due to the Covid-19 outbreak, and those strategies that will be impactful on the performance of the shuttle bus operation. The outcome of this study will enhance a basis for policy recommendation by the University authority regarding the covid-19 preventive measures on bus operations.
Literature Review
Public Transport Operations in Nigeria During the Covid-19 Endemic
In Nigeria, bus services are the major means of transport for intercity travel while minicab services are the major means of transport for intra-city travel among the majority of commuters because of the relative affordability Adeniran, et al. [5]. These services which are run by the informal sector have seats between 15 and 21 passengers for bus services while 5 and 8 for minicab services, depending on the size of the bus or car, and several seats fabricated for a vehicle by local metal smiths Tetteh, et. al. [6]. The vehicles are, nonetheless, usually overloaded, presenting a potential health hazard for the spread of infectious diseases Adeniran, et al. [5,7] such as Covid-19. Minicabs, motorcycles, tricycle services, Acheampong, et al. [8-10], and bus rapid transit services Adeniran, et al. [5] exist in most Nigeria cities, for intracity movement because of their cheap fares, and large vehicle fleets that ply most roads. As a result of their informal natures, operators of bus services and some minicab services are unionized under the National Union of Road Transport Workers (NURTW), a member of the Trade Union Congress. This enhances the commercial drivers to be able to represent their interest with the government, such that their services will be regulated through government directives, especially in times where public transport management requires a collaborative effort between the operators and government.
The ministry of transport in conjunction with the ministry of health and ministry of information issue directives for intercity and intra-city bus operators during covid-19, which included the use of veronica buckets in bus terminal; compulsory rinsing of hands and regular washing of vehicles before boarding vehicles; reducing the number of occupants per vehicle; opening of windows for ventilation; and recording of passenger cell phone numbers for contact tracing. Appropriate use of a nose mask and or face mask was also provided on the ministry’s website. According to FUTA (2020), intra-state travel is doable by public transport- buses, tricycles, and taxis. The covid-19 rules guiding the intra-state travel in Nigeria, which is applicable to shuttle bus operation in all the tertiary institutions, were related to the provision of hand sanitizers for hand washing, and the earlier points. This study focused on the level of adherence between passengers and bus operators to the covid-19 preventive measures as suggested by the government on the campus shuttle of FUTA.
Empirical Review
During the Covid-19 lockdown period, it was generally agreed that travel must be minimized, allowing only essential or unavoidable trips. As activities resume in the post-lockdown period, it gives rise to the question of physical distancing in public transport. The sparse empirical studies available hitherto do not provide conclusive evidence on the effect of physical distancing in closed environments such as public transportation facilities and vehicles. There is, although limited, evidence depicting the significance of physical distancing in public transport can be wholly minimized if other non-pharmaceutical measures are enforced, such as the correct use of nose masks and or face masks, enhanced hygiene, or even a prohibition of talking (Singapore case) Cao, et al. [11-13], then there is still a risk of the virus spreading without wearing a nose mask and or face mask. In the presence of an infected passenger, physical distancing can help minimize the number of people infected but not prevent infection altogether when passengers do not wear masks. On the other hand, the latest epidemiological research shows that masks are effective in preventing or at least significantly reducing covid-19 virus spread Leung, et al. [14,12,15]. There are public transportation systems currently running large occupancies with passenger spacing below the two-meter physical distance rule and no covid-19 outbreaks attributed to public transportation when everyone wears masks, as recently reported for Japan.
In that country, it was recently found that most covid-19 contagion clusters originated in places where people gather, eat, drink, chat, and sing, such as live music venues, gyms, pubs, and karaoke rooms. There is no link between clusters and commuter trains. The fact that close-range conversation among strangers in public transportation is infrequent has been hypothesized by virologist Hitoshi Oshitani as one of the explanations for these findings Normile [16]. This type of result led Singapore to its decision of not enforcing strict physical distancing rules in public transportation but requiring passengers to wear nose masks and or face masks and not talk to each other. Even though the safety gains from the universal adoption of a nose mask and or face masks are potentially large, it is unknown how much safer a public vehicle or station is if all passengers wear different types of masks (surgical, cloth, ₦95) at different stages of the endemic, versus if only a subset of them does it. This is a matter of utmost relevance because it can help in defining a “reasonable” occupancy level for public transport, an element that has significant economic, operational, and social implications. Put differently, if a physical distance of two meters does not properly work in public vehicles when people do not wear masks, what should be the maximum passenger capacity of vehicles if all people use masks properly? The current experience in large cities in Asia, such as Tokyo and Seoul, shows that a physical distance shorter than 1 meter in public transportation seems to work well under general usage of masks and high hygiene standards; however, the current prevalence of the virus in those places is unknown.
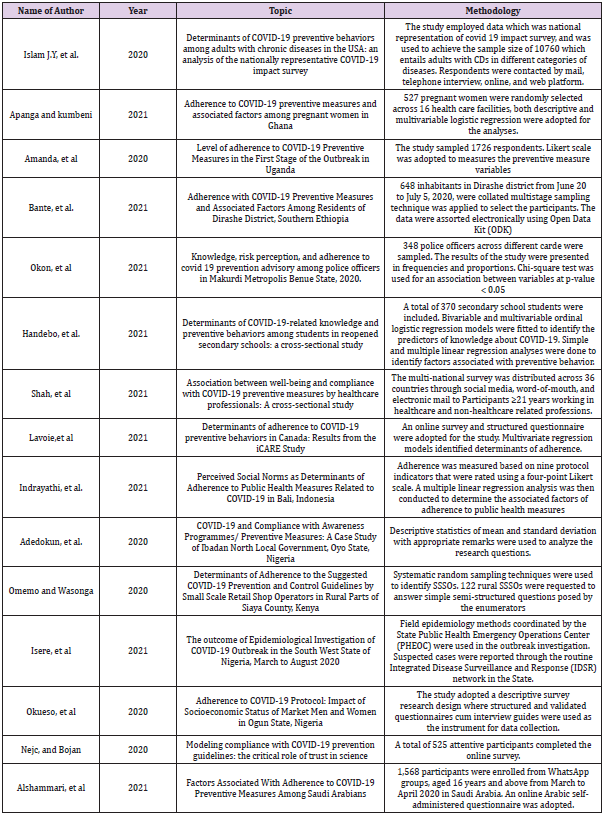
The evolution of such a method to public transportation use, without setting strong physical distancing rules, should be closely followed shortly to understand the conditions that would allow for its replication in other cities around the world. The problem of new maximum occupancy standards due to new physical distancing requirements is a multifaceted challenge that depends on the use of nose masks and or face masks, sanitization, and ventilation, among other factors. However, conditions are likely to be less clear-cut with some passengers that are not (properly) wearing masks. It is therefore assumed that some form of physical distancing may be needed, which is the current reality in many countries. From the empirical review shown in (Table 1), there were not many related studies on the adherence of covid-19 preventive measures by public transport operators, and there were no related studies conducted in FUTA. This study focused on the level of adherence regarding the covid-19 preventive measures as suggested by the government on the FUTA campus shuttle bus operation.
Table 1: Yield of intermediate products of grinding and flour of the initial wheat-triticale grain mixture without peeling.
Note: Authors’ compilation (2021)
Materials and Methods
This study adopts a survey research design through personal observation as a research instrument to collect primary data which was used to achieve descriptive statistics. The study is designed in such a way to assess the adherence of FUTA shuttle bus operators to covid-19 preventive measures during operation. The observation lasted for one week in the FUTA bus park. The survey is a technique that involves the use of other trained observers to categorize respondents’ behavior. This survey enhanced a fair appraisal of passengers’ and operators’ compliance in real-time Beutel, et al. [17]. The most suitable study populations were the shuttle bus operators and the passengers that were observed during the bus operation; passengers were selected because they do patronize the shuttle bus for departure. The assessment was best conducted at the bus park and the bus operators together with passengers are best to assess the adherence of shuttle bus operators to covid-19 preventive measures based on the indicators set by the Federal Ministry of Health. Primary data were collected through a structured survey of personal observations. The observation was conducted on shuttle bus passengers in the FUTA shuttle park using research assistants before takeoff. The three variables of frequent hand rinsing, wearing nose masks and or face masks and physical distancing was considered the most effective covid-19 prevention measures in FUTA shuttle bus operation. To determine the level of adherence of FUTA shuttle bus operators to compulsory hand rinsing, personal observation was conducted by the researcher within the period of study.
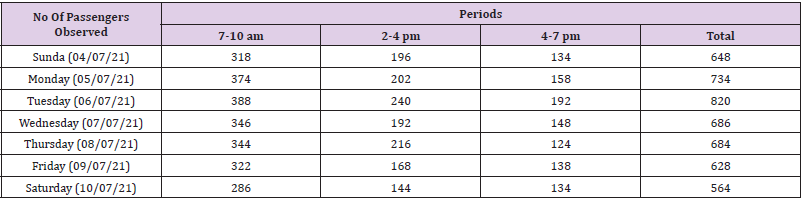
To assess the level of adherence of FUTA shuttle bus operators to physical distancing preventive measures, the category of buses (whether 18-passengers bus or 14-passengers bus) were identified, and the number of passengers that occupied each of these shuttle buses from Sunday (04/07/21) to Saturday (10/07/21) between the specific hours of 7-10 am, 2-4 pm, and 4-7 pm were numerically identified and summed. To assess the level of adherence of passengers to nose mask and or face mask-wearing in FUTA shuttle bus, the number of passengers that wear nose mask and or face mask in each of these shuttle buses from Sunday (04/07/21) to Saturday (10/07/21) between the specific hours of 7-10 am, 2-4 pm, and 4-7 pm were numerically identified and summed.
Results and Discussion
From the sample size calculated to seven hundred (700) which equals to the total number of passengers that were interviewed by the researcher and assistants in FUTA shuttle bus, only six hundred and eighty-seven (687) which is about 98.14 percent respondents provided valid responses for data analysis and reporting (Table 2).
Table 2: A response rate of respondents.
Note: Field Survey (2021).
Adherence of Futa Shuttle Bus Operators to Compulsory Hand Rinsing
To assess the adherence of FUTA shuttle bus operators to compulsory hand rinsing by passengers, personal observations were carried out in the Bus Park from Sunday (04/07/21) to Saturday (10/07/21) between the specific hours of 7-10 am, 2-4 pm, and 4-7 pm. It was revealed that there was the presence of Veronica buckets, but the passengers did not make use of it.
Adherence of Futa Shuttle Bus Operators to Physical Distancing
From the observations that were carried out regarding the adherence of FUTA shuttle bus operators to the covid-19 measures from Sunday (04/07/21) to Saturday (10/07/21) between the specific hours of 7-10 am, 2-4 pm, and 4-7 pm, it was revealed that all the shuttle bus operators adhered strictly to physical distancing measures by reducing the number of passengers apportioned to the seats. In the 18-passengers shuttle buses, the passengers were minimized to 14 as a result of physical distancing. Also, in the 14-passenger shuttle buses, the passengers were minimized to 10 as a result of physical distancing (Table 3).
Adherence of Passengers to Wearing of Nose Mask and or Face Mask in Futa Shuttle Bus
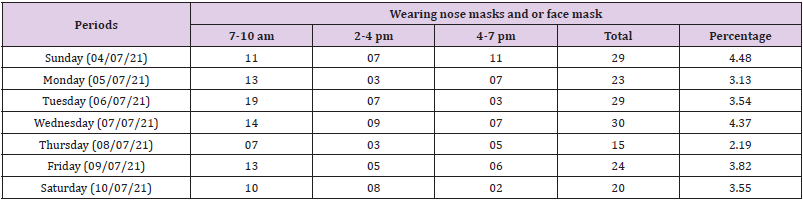
From the observations that were carried out regarding the adherence of passengers to the wearing of a nose mask and or face mask in FUTA shuttle bus from Sunday (04/07/21) to Saturday (10/07/21) between the specific hours of 7-10 am 2-4 pm, and 4-7 pm, it was revealed that fewer passengers adhered to the nose mask and or face mask-wearing in FUTA shuttle bus. When comparing (Table 3) with (Table 4), it was discovered that among 648 passengers that were examined, only 29 passengers wear nose masks and or face mask on Sunday which implies 4.48 percent. Among 734 passengers that were examined, only 23 passengers wear a nose mask and or face mask on Monday which implies 3.13 percent. Among 820 passengers that were examined, only 29 passengers wear a nose mask and or face mask on Tuesday which implies 3.54 percent. Among 686 passengers that were examined, only 30 passengers wear a nose mask and or face mask on Wednesday which implies 4.37 percent. Among 684 passengers that were examined, only 15 passengers wear nose masks and or face masks on Thursday which implies 2.19 percent. Among 628 that were examined, only 25 passengers wear a nose mask and or face mask on Friday which implies 3.82 percent. Among 564 passengers that were examined only 20 passengers wear a nose mask and or face mask on Saturday which implies 3.55 percent. Despite the fact the all the shuttle bus operators adhered strictly to physical distancing measures, the majority of the passengers did not adhere strictly to the nose mask and or face mask-wearing in the FUTA shuttle bus (Table 4).
Table 3: Adherence of FUTA shuttle bus operators to physical distancing.
Note: Author’s survey (2021)
Table 4: Adherence of Passengers to Wearing of Nose mask and or face mask in FUTA Shuttle Bus.
Note: Author’s survey (2021)
Discussion
Regarding the adherence of FUTA shuttle bus operators to compulsory hand rinsing, the study found that there was the presence of Veronica buckets, but the passengers did not make use of it. This corroborates the findings of Bonful, et al. [18] in Ghana which found that majority of bus stations in Accra have at least one Veronica Bucket, but few passengers make use of it. This implies that the practice of hand washing was either not observed. Regarding the adherence of FUTA shuttle bus operators to physical distancing; it was revealed that all the shuttle bus operators adhered strictly to physical distancing measures by reducing the number of passengers apportioned to the seats. This agrees with the findings of Emmanuel, et al. [19-25] which found that there was physical distancing in paratransit (trotro) buses in Kumasi, Ghana. However, this does not agree with the findings of Bonful, et al. [18,26-35] in Ghana which found that social/physical distancing was rarely practiced in Ghana. Regarding the adherence of passengers to wearing of a nose mask and or face mask in FUTA shuttle bus, it was revealed that fewer passengers adhered to the nose mask and or face mask-wearing in FUTA shuttle bus.
The adherence to nose mask and or face mask was dominant on Sunday. This finding is similar to the findings of Bonful, et al. [18,35-45] in Ghana which found that face masks were either not worn or only worn by a few passengers in the selected bus stations, but not similar to that finding of Emmanuel, et al. [19,45-61] which found that passengers wear nose mask in paratransit (trotro) buses in Kumasi, Ghana. Lack of hand washing practice, and failure to use nose mask and or face mask at the FUTA bus stations could be as a result of many factors. It could be as a result of inadequate relevant public sensitization about the pertinence of hand washing to guide against the spread of Covid-19 infection. Another likely factor could be as a result of socio-cultural factor that may influence people not be used to wearing of face and or nose mask and washing of hands regularly in public, especially at bus stations. Lack of adequate communication by transport operators could be another factor that influences people not to wear face and or nose mask and not to wash hands regularly in bus stations.
Conclusion
This study assessed the level of adherence of FUTA shuttle bus operators and passengers to the covid-19 preventive measures suggested by the government, regarding assessing the level of adherence of FUTA shuttle bus operators to compulsory hand rinsing; assessing the level of adherence of FUTA shuttle bus operators to physical distancing preventive measures; and assessing the level of adherence of passengers to wearing of a nose mask and or face mask in FUTA shuttle bus. This study adopts a survey research design through personal observation as research instruments to collect primary data which was used to achieve descriptive statistics. The study is designed in such a way to assess the adherence of FUTA shuttle bus operators to covid-19 preventive measures during operation. The observation lasted seven which entails a seven-day peak and off-peak hour count within the specified hours of 7-10am, 2-4pm and 4-7pm from Sunday to Saturday. Of the three hours designated for each of morning, afternoon, and evening sessions, there seems to be no rinsing of hands by passengers, although there were provisions of veronica buckets in the Bus Park. Also, there seems to be a low level of adherence to nose mask and or face mask-wearing among the passengers, however, the FUTA shuttle bus operators were keen on ensuring physical distance in the sitting arrangement of passengers as this was discovered in all the shuttle buses that were studied. Based on the specific findings, it was suggested that there should be a strict monitoring and enforcement of hand rinsing by passengers in FUTA before the departure of shuttle bus; and the enforcement of nose mask and or face mask-wearing was a bit relaxed; hence the university management should be more strict in her enforcement of nose mask and or face mask-wearing especially in the FUTA shuttle bus.
Influence of Abrasive Peeling of Wheat-Tritical Grinding Grain Mixture on the Yield of Intermediate Grinding Products and Flour
Introduction
Current directions of development of one of the most important branches of the processing industry – flour milling is both the improvement of technologies for processing traditional crops (wheat and rye), and the development of new technologies for processing non-traditional crops, such as triticale [1-2]. One of the main directions of development of the industry is the development of new and improvement of traditional technologies and the creation of processed products of various types of grain with a given composition and properties, including products of deep processing [3-5,6,7]. In addition, the direction of joint processing of grain of various crops, including wheat and triticale, is very promising. Triticale is the first grain crop created by man and obtained by crossing wheat (Latin Triticum) and rye (Latin Secale). The use of triticale as a food crop is an interesting, promising direction not only for the flour milling, but also for other branches of the food and processing industries. This is confirmed by the increased interest in this culture, both from researchers and from food producers not only in our country, but also abroad. Bakery products using processed products from the central part of the endosperm of triticale grain are characterized by increased nutrition due to a higher protein content and essential amino acids, in particular the main limiting acid – lysine [8-11]. The combination of positive properties of rye – a high content of biologically active aromatic substances and wheat – the rheological properties of the dough, allow making food products of mass consumption from processed products of triticale grain and mixtures based on it.
At the same time, the technological properties of baking flour obtained from various grain mixtures, including wheat-triticale grain grinding mixture, remain poorly understood. Peeling of the wheat-triticale grain mixture during varietal bakery grinding is carried out for maximum cleaning of the grain surface from dust, dirt, mold, bacteria, as well as reducing and simplifying the length of the technological scheme [12-14]. Removal of surface shells with the use of peeling machines allows, in addition, to reduce the number of peeling and grinding systems and reduce the technological process of processing the milling wheat-triticale grain mixture into flour.
When using abrasive peeling in the finished product, the number of shell particles is reduced, and its appearance is improved [15,16]. The ash content of the milling grain mixture of wheat and triticale decreases after peeling. Removal of membranes allows: – get a more solid and hygienic clean product; – to obtain from the stripped systems bakery flour with a higher index of whiteness; – significantly reduce the number of grinding and sieve systems, simplify the technological scheme of grinding. In addition, it should be noted that in the process of peeling from the surface of the grain, not only impurities are removed, but also part of the fruit and seed shells. This, on the one hand, has a positive effect on reducing the process of moistening the grain, but on the other, due to the exposure of the endosperm and injury to the germ of the grain, it can lead to a loss of its viability, which is not given enough attention.
In this regard, additional studies of the peeling process and its effect on the properties of wheat grain are required [14]. The purpose of our research is to determine the effect of abrasive peeling on the yield of intermediate products of grinding and flour in the processing of peeled wheat-tritical grain mixture in varietal bakery grinding.
Research Materials and Methods
In studies conducted at the Department of Grains, Bakery and Confectionery Technologies of the Federal State Budgetary Educational Institution of Higher Education “MSUPP” and at the Department of Food Technologies and Organization of Restaurant Business at the I.S. Turgenev Oryol State University, experiments were conducted to determine the effect of the degree of peeling of the wheat-triticale grain mixture on the output of intermediate grinding products. The objects of research were wheat of the “Radmira” variety and triticale of the “Nemchinovsky 56” variety, bred by breeders of the Federal Research Center “Nemchinovka” and differing from other wheat varieties by the increased protein content of the 2020 harvest. The main physical, chemical and chemical parameters of the initial wheat-triticale grain mixture are as follows: humidity – 11.2%, ash content – 1.83%, protein content – 13.2%, gluten content – 23.8%, gluten quality – 79 units of the device, vitreousness – 46% and drop rate – 354 seconds. When preparing the wheat-tritical grain mixture for laboratory grinding as a hydrothermal treatment (GTO), a mandatory operation for varietal grinding, cold conditioning was used as the most common method and the cheapest method. After hydrothermal treatment, abrasive peeling was carried out before grinding wheat-tritical grain mixtures. For grinding, a laboratory grinding mill MLP-4 with rifled rollers with a groove arrangement of the back along the back was used.
The main mechanical and kinematic indicators of the mill MLP- 4 with rifled rollers are as follows: productivity – up to 100 kg / h, the speed of the fast-rotating roller is 4.5 m / s, the differential is 1.75, the location of the backrest grooves, the number of grooves on the 1st linear centimeter – 8 pieces, the slope of the grooves is 8%.
The intervalian clearance on the I drain system was 700 μm, on the II drana system – 300 μm, on the III drana system – 150 μm and on the IV dranaya system – 100 μm. When conducting studies to determine the effect of the number of removed shells in abrasive peeling of wheat-triticale grain mixtures on the yield of intermediate products of grinding, laboratory grindings of shelled wheat-triticale grain mixtures were carried out with preliminary removal of shells in the amount of 2.5%, 5.0%, 7.5%, 10% and a control sample without peeling.
Next, laboratory grindings were carried out and 4 of the 5 main, cereal-forming dredge systems were modeled when grinding the initial wheat-triticale mixture and peeled wheat-triticale grain mixtures. The data obtained to determine the effect of abrasive peeling on the grain-forming ability of peeled wheat-triticale grain mixtures are presented in (Tables 1-5).
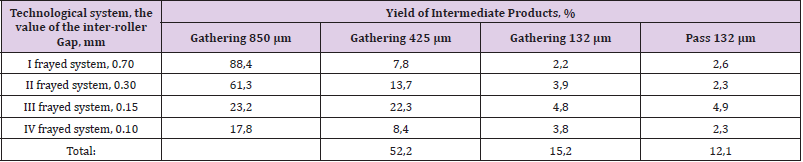
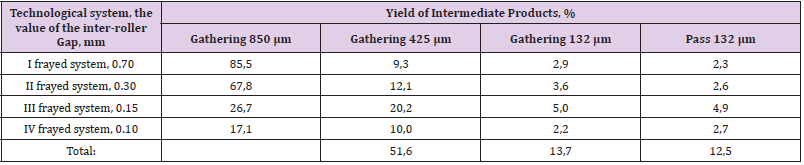
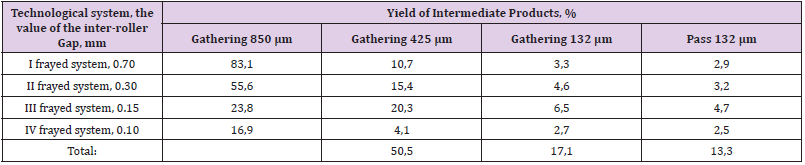
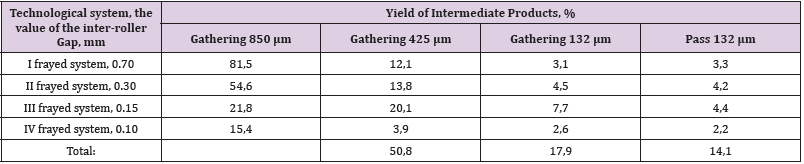
As can be seen from (Table 1), the yield of intermediate grinding products during the processing of the initial wheat-triticale grain mixture without peeling, sent for grinding to grinding systems, was 63.6%, the yield of wheat-triticale flour was 12.0%, the yield of a similar product sent to the V draught system was 19.3%. As can be seen from Table 2, the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 2.5%, sent for grinding to grinding systems was 67.4%, the yield of wheat-triticale flour was 12.1%, the yield of a similar product sent to the V strip system was 17.8%.As can be seen from (Table 3), the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 5.0%, sent for grinding to grinding systems was 65.3%, the yield of wheat-triticale flour was 12.5%, the yield of a similar product sent to the V strip system was 17.1%. As can be seen from (Table 4), the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 7.5%, sent for grinding to grinding systems was 67.6%, the yield of wheat-triticale flour was 13.3%, the yield of a similar product sent to the V draught system was 16.9%. As can be seen from (Table 5), the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 10.0%, sent for grinding to grinding systems was 68.7%, the yield of wheat-triticale flour was 14.1%, the yield of a similar product sent to the V strip system was 15.4%. Thus, according to the results of the studies, it was found that the greatest yield of intermediate products of grinding and flour during the processing of the wheattriticale grain mixture is obtained by removing 10% of the shells and is 82.8%, which is 6.9% more compared to the original nonpeeled grain.
Table 1: Yield of intermediate products of grinding and flour of the initial wheat-triticale grain mixture without peeling.
Table 2: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grainmixtures with the removal of 2.5% of the shells.
Table 3: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grain mixtures with the removal of 5.0% of the shells.
Table 4: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grain mixtures with the removal of 7.5% of the shells.
Table 5: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grain mixtures with 10% shell removal.
Findings
Thus, according to the results of the studies, it was found that abrasive peeling with the removal of up to 10% of the shells of wheat-tritical grain mixtures before grinding into varietal baking flour has a positive effect on the cereal-forming ability and leads to an increase in the yield of intermediate cereal grinding products and an increase in the yield of flour on the pulled systems. The greatest yield of intermediate products of grinding and flour during the processing of the initial wheat-tritical grain mixture is obtained by removing 10% of the shells and is 82.8%, which is 6.9% more compared to the original non-peeled wheat-tritical grain mixture.
Evaluation of Clinical Transfusion Practices in Neonatal Intensive Care Unit
Introduction
Appropriate transfusion of neonates is vital to balance the transfusion benefits against risk. Sick neonates are heavily transfused groups of patients in critical care medicine. The rational utilization of blood components is very consequential in this age group. It, consequently, remains an important tool to continuously improve, amend and implement the most appropriate transfusion protocols for blood components utilized in neonates within the constraint of the evidence-based guidelines. Because of the length of their stay in the neonatal intensive care unit (NICU) and the frequent monitoring of parameters through blood sampling neonates experience iatrogenic blood loss and may require multiple transfusions. Majority of the neonatal transfusions are often prescribed on expert clinical opinion rather than concrete documented guidelines [1]. Lack of perspective patient blood management (PBM) program in neonates accentuates the blood management and best transfusion practices in the neonatal intensive care unit (NICU). Due to the lack of sufficient data from India focusing on transfusion needs, patterns, indications, and short-term outcomes in preterm neonates prompted the requisite for this study.
Materials & Methods
Study data were collected retrospectively over 19 months from June 2019 to December 2020. All preterm and term neonates admitted to the Neonatal Intensive Care Unit (NICU) at All India Institute of Medical Sciences (AIIMS) Jodhpur, Rajasthan, India, for whom blood requisition form was sent for component transfusion, i.e., Packed Red Blood Cells (PRBC), Random Donor Platelets (RDP), Fresh Frozen Plasma (FFP), Cryoprecipitate, Reconstituted Whole Blood, were included in the study. Data was collected from NICU medical records and review of the NICU blood order forms at the AIIMS Jodhpur blood center. According to British Society for Hematology (BSH) guidelines [2]. Those blood order forms were considered appropriate and satisfied all the transfusion criteria required to evaluate transfusion needs according to the BSH guidelines [2]. Inappropriate blood order forms are those which deviate from the guidelines and include incomplete documentation (i) for PRBC transfusion missing Hemoglobin (Hb), Weight of newborn (wt.), Saturation status (SpO2), (ii) for RDP transfusion missing platelet count, comorbidity or surgical or invasive procedure patient is undergoing, and (iii) for FFP transfusion coagulation parameter, bleeding at present and patient is undergoing some invasive procedure. Data analysis was done with descriptive statistics. Perpetual variables will be summarized as mean & standard deviation. Nominal/categorical variables will be summarized as the proportion (percentage) and analyzed by utilizing the Chi-Square test/Fisher exact test. P-value < 0.05 was considered as significant (Tables 1-4).
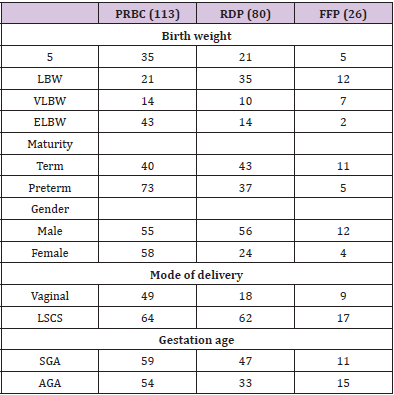
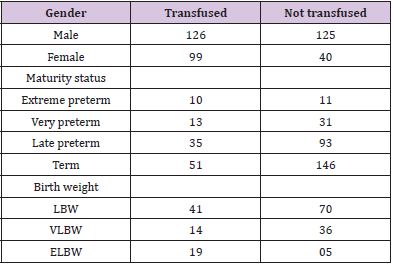
Table 1: Blood component issued as per Birth weight, maturity, gender, mode of delivery & gestational age.
Table 2: Transfusion Parameter of neonates.
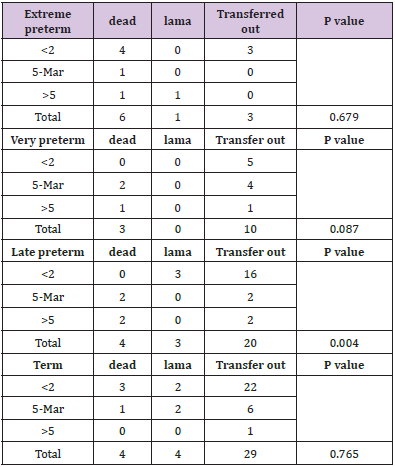
Table 3: Outcome assessed based on no of transfusion.
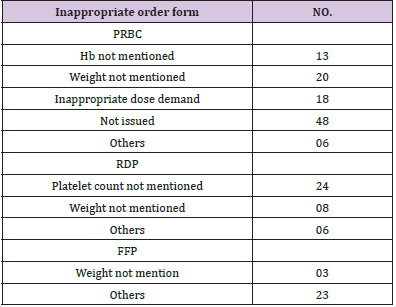
Table 4: Reason for inappropriate request order form.
Results
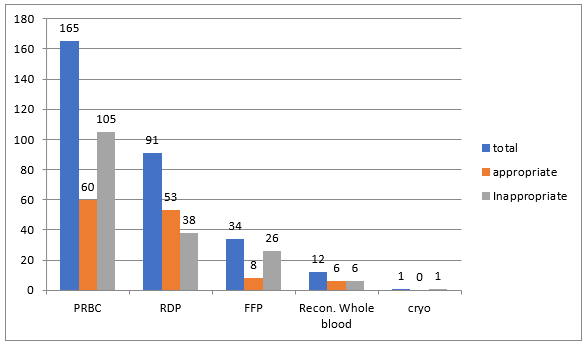
Data were analyzed retrospectively from June 2019 to December 2020. There were 390 NICU admissions during the study period, and 303 blood order forms were received. PRBC was the most frequently ordered blood component (165), followed by RDP (91), FFP (34), reconstituted whole blood (12), and cryoprecipitate (1) (Figure 1). Out of 303 received blood order forms, blood was issued for 225 requisitions (74%). Most frequent blood component issued was PRBC (113/225, 50%) followed by RDP (80/225, 35.5%), FFP (26/225, 11.5%) and reconstituted whole blood (6/225, 0.02%). NICU’s overall crossmatch to transfusion ratio (CT ratio) was 1.46 suggesting a significant utilization of blood components. During the study period, male admissions outnumber female admissions (251 vs. 139 respectively), and male requisitions received outnumber females (166 vs. 137 respectively). Females received more transfusions (p-value 0.000, chi-square 16.2), with PRBC accounting for the majority of transfusions in terms of gender predisposition. Out of the 303 requisitions received, the majority of the neonates were born through lower segment cesarean section (LSCS) compared with vaginal delivery and required frequent PRBC transfusions (166 v/s 137).
Out of the 390 NICU admissions, 187 were preterm (<37 weeks), and the rest were term. Requisitions received were higher for preterm neonates than term neonates (163 vs. 140 respectively). Out of the 163 preterm requisitions, 125 were issued and transfused (125/163; 77%), while for term babies, out of 140 requisitions, 94 were issued and transfused (94/140; 67%). Out of all the preterm transfusions, PRBC was the most frequent blood component transfused (73/125; 58%), followed by RDP (37/125; 30%) and FFP (15/125; 12%). While in term babies, RDP was the most frequent blood component transfused (43/94; 46%), followed by PRBC (40/94; 43%) and FFP (11/94; 12%). However, no significant association between transfusion requirement and maturity status (extreme preterm, very preterm, late preterm, and term patients) was seen (p-value 0.210).
Figure 1: Component order form appropriateness ( p value 0.001).
In terms of birth weight, out of the 390 NICU admissions, LBW (birth weight 2500 to 1500 gm) were 111, VLBW (birth weight 1500 to 1000 gm) was 50, while ELBW (birth weight <1000 gm) were 24. Out of the 303 requisitions 101 (33%) were received from LBW neonates, 94 (31%) form NBW, 68 (23%) ELBW and 40 (13%) from VLBW neonates. In our study, ELBW neonates were more transfusion-dependent (Chi-square 18.8, p-value 0.000), and the most frequent blood component transfused was PRBC.
The outcome was assessed only for 87 patients (Chi-square 12.7, p-value 0.005), and the extremely premature neonate mortality was higher. In terms of maturity, mortality was higher in late preterm neonates when the number of transfusions increased by more than 2 (p-value =0.004). As per the gestational age, out of 303 requisitions, 140 (46%) were from small for gestational age neonates (SGA) while 163 (54%) were from appropriate for gestational age neonates (AGA). PRBC and RDP transfusions requirement were more in SGA neonates compared with AGA with mean number of transfusions being 2.92 for preterm neonate and 3.45 for SGA. Out of 303 blood requisitions 127 were found to be appropriate while rest 176 were inappropriate. Most frequent inappropriate component requested was FFP 76.4% (26/34), followed by PRBC 63.6% (105/165), reconstituted whole blood 50% (6/12) and RDP 41.75% (38/91) (Figure 1) Chi square =17.8, p value 0.001. A single request was received for cryoprecipitate for deranged coagulopathy during study period but component was not issued. Most frequent reason for inappropriate blood order forms demanding FFP was missing indication for transfusion (n=23;88%) and information against dose directed transfusion (n=3;12%). Similarly for inappropriate blood order forms received for RDP, majority (n=24;63%) do not have pre transfusion platelet count (needed to calculate percentage recovery and corrected count increment), 21% (n=8) do not have Weight mentioned and for rest 16% (n=6) order forms patient had no indication for transfusion.
Most common indication for reconstituted whole blood was exchange transfusion for the management of hyperbilirubinemia. Exchange transfusion was done only when serum bilirubin exceeds its target limit based on maturity status of newborn and live days. Out of 12 blood order forms received, 50% required the transfusion support and in rest jaundice was subsided by use of phototherapy. Out of 105 inappropriate blood order forms received for PRBC transfusion 12% (n=13) have missing Hb, 19% (n=20) have missing Weight, 17% (n=18) demand for inappropriate volume and 6% (n=6) can’t justify the transfusion need because of missing other parameters like comorbidity and saturation status. Forty six percent (n=48) blood order forms were those which were not issued and where transfusion was not needed. Most common indication for PRBC transfusion was anemia (63/113: 56%), for RDP transfusion thrombocytopenia and for FFP transfusion deranged coagulopathy with bleeding tendencies. Other indication for PRBC transfusion were during surgery (21/113:19%), shock (12/113:11%), blood loss (11/113: 10%), pathological jaundice (6/113: 0.05%) in decreasing order.
Discussion
Blood transfusion has a pivotal role in modern medicine. Despite being a lifesaving drug, it has deleterious effects also. This becomes important in neonates who have small blood volume and immature organ system. Both restrictive and liberal transfusion are well described in literature. Because of the lack of National Clinical Transfusion guidelines and varied transfusion practices among clinicians, most transfusions are based on expert clinical opinion. We advocate that neonate transfusions should be critically analyzed in terms of maturity, gestational age, disease effect, blood volume, appropriateness and clinician’s transfusion practice which is neglected in majority of the times. Between June 2019 and December 2020, 390 neonates were hospitalized with 225 requiring transfusions and 303 blood order forms received. In our study, the incidence of transfusion was 58.4 % (225/384) with PRBC being the most frequently requested blood component (113/303; 37.29 percent). Several studies have found that the incidence of neonatal transfusion ranges from 20% to 90% [3,4]. The fact that some studies included only extremely low birth weight newborns while others included term neonates explains the wide variance in transfusion. The majority of preterm and extremely low birth weight neonates in the NICU are transfused based on laboratory criteria. It should be emphasized that while transfusions offer an instant benefit in tissue oxygenation, it also inhibits the neonate’s immature bone marrow, delay newborn neurodevelopment outcomes, and lengthen hospital stays [5-9]. In our study, we observed that ELBW neonates are an extensively transfused patient population, with PRBC being the most often requested component. Thus, it may be concluded that frequent transfusion to maintain a higher hemoglobin level in ELBW infants gives no further benefit [5-9]. As a result, a restricted transfusion approach may be adopted. In our study, we found that the mortality was more in extremely preterm newborns than the term neonates (p value 0.005). The association is significant when frequency of transfusion is more than 2 and mortality was higher in late preterm neonates (p value 0.004). Thus, RBC transfusions may have a negative impact on neonatal survival.
In our study, we found that SGA neonates required more transfusions than AGA neonates (mean of 3.45). Conti et al. found similar findings, with the majority of transfused newborns being between 24 and 29 weeks of gestation and weighing less than 1000g [10]. Iatrogenic anemia occurring due to repeated blood sampling in the NICU is a leading cause of anemia [11,12]. It is estimated that in NICU mean sample volume range between 0.8-3.1 ml/kg/day which corresponds to 30%-300% of neonates blood volume [11]. Phlebotomy loss alone in first 24 hours of NICU admission is around 3-10ml corresponding up to 25% of the blood volume [12]. For us establishing a temporal relationship between iatrogenic blood loss and requirement for PRBC transfusion is difficult because no documentation ever made regarding the number and amount of neonatal blood samples collected.
Necrotizing Enterocolitis (NEC), a complication of red cell transfusion, is one of the leading causes of newborn death. Marin et al. found that alterations in mesenteric oxygenation during PRBC transfusion might be linked to transfusion-related NEC. In our study we report NEC in 3 patients, one having single episode of transfusion and rest had 7 and 19 transfusion episodes. All the patients were preterm and mortality was found only in one patient received multiple transfusions and had long hospital stay. Though we haven’t found any relation of NEC with transfusion but several other studies have found that PRBC transfusions are an independent risk factor for NEC with VLBW neonates being more vulnerable as early as 48 hours after the transfusion [13]. As a result, it is necessary to explore pharmacological agents to reduce the need for transfusions. The use of erythroid stimulating agents, such as recombinant erythropoietin or longer acting darbepoetin, might potentially reduce the need for transfusions. Recently, the PENUT study shown that erythropoietin treatment can maintain a much higher Hb level, reduce the need for transfusions, and expose fewer donors [13]. Our findings are consistent with other research that show anemia is the most prevalent reason for PRBC transfusion. A review of the literature reveals that a greater blood transfusion/ unit volume ratio in newborns puts them at risk of metabolic derangement. This is due to immature liver’s decreased ability to metabolize anticoagulant and sense hypoxia, and the immature kidney’s inability to handle electrolytes, leads to hypocalcemia, hyperkalemia, acidosis, and hypomagnesaemia. With multiple or large transfusions, these potential hazards are compounded. Though it is uncommon with top-up transfusions, hyperkalemia can develop if the neonate receives more than 20 ml/kg of transfusion volume, has underlying hyperkalemia, or has renal disease.
Potassium levels in these patients should be regularly checked. Cardiac arrest has been observed after receiving a large blood volume transfusion due to hyperkalemia, particularly in neonates receiving exchange transfusion. Because of the stored blood and high body surface area, exchange transfusion can potentially cause hypothermia. Hypothermia can aggravate coagulopathy and result in a fatal triad [14]. We found no negative effects from transfusion in our study. This might be because patient blood management is tightly enforced at our center, and every transfusion is scrutinized. The amount of coagulation protein in the neonate varies with gestational age. Premature babies have prolonged prothrombin time and activated partial prothrombin time (PT/aPTT) due to underdeveloped hepatic function. Unless there are bleeding symptoms, FFP is not recommended to restore a prolonged international normalized ratio (INR). The development of disseminated intravascular coagulation (DIC) in the absence of current bleeding does not warrant the use of FFP. The use of FFP in liver disease is also debatable, because FFP may not always result in a complete correction of the coagulation abnormality [15]. In our study we analyzed that FFP was the most inappropriately requested component. This can be explained by the fact that parameters required for assessing the FFP transfusions were missing on the requisition form. Majority of the platelet transfusions in neonates were done prophylactically as neonatal guideline have higher platelet transfusion threshold as compared to adult. Improved outcome was seen with platelet transfusions for hemorrhage secondary to thrombocytopenia [15].
Conclusion
Evaluation of clinical transfusion practices is intended to bring a realization among clinicians’ expert in their field about the need to evaluate their own practices regularly. The two primary risk factors identified that lead to numerous blood transfusions are low birth weight and preterm. Transfusion has been linked to an increase in mortality, therefore studies towards reducing newborn transfusion needs, particularly PRBC, which is commonly prescribed for anaemia correction, is necessary. The most inappropriately requested component was fresh frozen plasma, and the indication was abnormal coagulation profile; however, there is no basis for using FFP for coagulation profile correction in neonates except bleeding.
Study of the Hypothalamic Pituitary Adrenal Axis Stress Effect on Spiny Projection Neurons by Pathophysiological Computing Modelling of Basement Metabolism, An in Silico Study
Introduction
Medium spiny neurons (MSNs) are a type of inhibitory neuron of the GABAergic type that plays a key role in initiating and controlling body movements so that today these neurons play an important role in the development of neurogenic diseases. Despite the importance of these neurons, there is no accurate information about the effect of stress on them. The subject of this research is a study on the effect of seven stresses include; hypoxia stresses, thermal stress, mTOR stress, oxidative stress, HPA axis stress, aging stress, and electrochemical stress on MSNs by modeling the pathophysiology of these neurons at the system biology level.
Materials and Method
This research can be divided into five stages (Figure 1). In the First step, prefabricated models related to MSN-related stresses, structures, and pathways were reviewed and extracted from biomodel, Vcell, and Reactome databases, and then screened, selected, and archived in SBML format. In the second stage, pathways were merged by COPASI software and a united model was created. In the third stage, the model was implemented on the Vcell platform and the results of the simulation were archived in SBML (level 3, version 1) format. At this stage, the variables were determined to simulate normal and stressed conditions, according to Table 1, and finally, after running the simulator based on solver stiff, the results were plotted by WPS office spreadsheet software and analyzed manually.
Figure 1: Simulation steps.
Table 1: Initial concentrations.
Results & Discussion
Figure 2: Results of model implementation under Vcell software.
According to Figure2(C), CYP RNA in stress increased. Cytochrome P450 3A4 (EC 1.14.13.97) is an important enzyme in humans, found mainly in the liver and intestines. This Cytochrome oxidizes small foreign organic molecules (xenobiotics) such as toxins or drugs so that they can be eliminated from the body. While many drugs are inactivated by CYP3A4, some drugs are activated by this enzyme. Some substances, such as grapefruit juice, and some medications interfere with the function of CYP3A4. Use of these drugs with drugs that are modified and enhanced or attenuated by CYP3A4. CYP3A4 is a member of the Cytochrome P450 family. Several other members of this family are also involved in mixed metabolism, but CYP3A4 is the most common [1]. According Figure 2(A,B,F,H,I,P) Dexamethasone metabolites in stress increased. Dexamethasone is a corticosteroid drug. It is used to treat many conditions, including rheumatic problems, some skin conditions, severe allergies, asthma, chronic obstructive pulmonary disease, croup, brain swelling, eye pain following eye surgery, and in combination with antibiotics for tuberculosis.
In adrenergic insufficiency, it should be used with a drug that has more mineral effects (including fludrocortisone). In preterm labor, it may be used to improve outcomes in the baby. It may be taken orally, by injection into a muscle, or intravenously. The effects of Dexamethasone often last for a day and last for about three days. Prolonged use of Dexamethasone may lead to thrush, osteoporosis, cataracts, bruising, and muscle weakness. It should not be consumed while breastfeeding. Dexamethasone has antiinflammatory and immunosuppressive effects [2].
According to Figure 2(G, M, N, O), cortisol metabolites in stress increased. Cortisol is a steroid hormone, a type of glucocorticoid hormone. When used as a medicine, it is known as hydrocortisone. In many animals, it is produced mainly by the adrenal cortex in the adrenal gland [3]. This substance is produced in smaller quantities in other tissues [4]. It is released during the circadian cycle and its release increases in response to stress and low blood glucose concentrations. It also reduces bone formation [5]. This gene encodes the alpha globulin protein with the corticosteroid-binding property. This protein is the major transporter for glucocorticoid hormones in the blood of most vertebrates [6]. PXR (Pregnane X receptor & Glucocorticoid receptor) is a nuclear receptor whose main function is to monitor the presence of foreign toxins and belongs to a family of nuclear receptors whose members are transcription factors that are transcribed by a domain into a ligand and by a Domains are attached to DNA. PXR is a transcription regulator of the Cytochrome P450 CYP3A4 gene.
It is activated by a combination of compounds including Dexamethasone and rifampicin and stimulates CYP3A4 [7,8] The glucocorticoid receptor (GR), also known as NR3C1, is a receptor to cortisol and other glucocorticoid GR is expressed in almost every cell in the body and regulates genes that control growth, metabolism, and the immune response, and because the receptor gene is expressed in different ways, it has different effects in different parts of the body. (Pleutropic) When glucocorticoid hormones bind to GR, the main mechanism of action is to regulate gene transcription [9,10]. After binding to the glucocorticoid, the activated glucocorticoid receptor complex expresses anti-inflammatory proteins in the nucleus. Regulates and suppresses the expression of inflammatory proteins in the cytosol (by preventing the transfer of other transcription factors from the cytosol to the nucleus [11,12]. Steroid Hormone Receptors (SHRs) are transcription factors that are activated in the presence of steroid hormones.
While estrogen receptors are predominantly nuclear, unbound Glucocorticoid (GR) and Androgen (AR) receptors are mostly located in the cytoplasm and are transported to the nucleus only after hormone binding. This Progesterone Receptor (PR ) in humans is encoded by a gene (PGR) on chromosome 11, which has two forms (PRA) and (PRB), that (PRA) is more in the cytoplasm and the form (PRB) in both the cytoplasm and There is in the core. Understanding the mechanism of ATPase activity of HSP90 is largely derived from structural and functional studies of Saccharomyces cerevisiae complexes. Binding of PTGES3 (p23) to the HSP90 complex and, finally, its combination stabilizes the hormone. It is worth noting that GR-importin interactions can be ligand-dependent or independent. In nuclear ligand-activated SHR, specific sequences in DNA called Hormone Responsive Elements (HRE) are created [13]. Albumin is a family of globulin, the most common of which is serum albumin.
All proteins in the albumin family are soluble in water and relatively soluble in concentrated saline. Albumin is usually found in the blood plasma and is not glycosylated. Albumin-containing substances are called albuminoids. Some transfusion proteins are evolutionary linked to the albumin family (including serum albumin, alpha-photo protein, and vitamin D-binding proteins. This family is found only in vertebrates [14-16].
Tyrosine aminotransferase (or tyrosine transaminase) is an enzyme present in the liver that catalyzes the conversion of tyrosine to 4-hydroxyphenylpyruvate [17]. Deficiency of this enzyme in humans can lead to what is known as type II tyrosinemia, in which there is an accumulation of tyrosine (resulting in accumulation of tyrosine due to a lack of aminotransferase reaction) [18].
Conclusion
According to their results and analysis, in general, it can be said that stress caused by the Hypothalamic-pituitary-adrenal axis increases Dexamethasone and cortisol metabolites and increases cellular metabolism and catabolism over anabolism, and therefore can It has a destructive effect on MSNs and other similar cells and thus aggravates the symptoms of MSN-related diseases. It is suggested that researchers investigate various aspects of the destruction of these neurons by researching this subject, and therefore future research could be a follow-up to this research. In this study, we examined only part of the basal metabolism on MSNs, so it is recommended
a) Examine other metabolic pathways not only on MSNs but also on other neurons.
b) Use other bioinformatics software to simulate stress on MSNs and other neurons.
c) Simulation of the effects of different drugs on cell metabolism using relevant software
d) Design of different drugs based on the feedback we receive from the simulator.
Investigation of bio transformation using Biomodel and Vcell.
ABO Blood Group Profile Frequencies and Relationship in COVID-19 Disease Susceptibility and Severity in Lagos, Nigeria
Introduction
COVID-19 caused by the Severe Acute Respiratory Syndrome Coronavirus-2 [SARS-CoV-2] was first described as a serious infection leading to significant morbidity and mortality in Wuhan, China in January 2020 Zhou, et al. [1]. The number of deaths was increasing due to the catastrophic effect of the emerging new strains. Research has shown that there are predicting factors of COVID-19 severity such as demographic, clinical, immunologic, haematological, biochemical, and radiographic factors Benjamin, et al. [2]. According to Samra, et al. [3] ABO groups can play a role in COVID-19 severity and susceptibility. The rapid global spread of the novel coronavirus SARS-CoV-2 has strained existing healthcare and testing resources, and it is causing COVID-19 severe cases in some people than in others. While some people experience only mild symptoms, others are being hospitalized Samra, et al. [3]. The pathogenesis of severe COVID-19 and the associated respiratory failure are still unclear, but the higher mortality rate is consistently associated with older age and being male Samra, et al. [3]. Many studies have shown that the ABO blood type is a potential risk for various diseases such as cancer, myocardial infarction, acute kidney injury, and venous thromboembolism Dentali, et al. [4,5] Apart from comorbidities and other predicting factors, findings have shown that the ABO blood group has a correlation with COVID-19 susceptibility and severity. Biological factors that determine susceptibility to SARS-CoV-2 and severity of COVID-19 are yet to be fully understood Samra, et al. [3]. The ABO blood grouping may influence the susceptibility of COVID-19 and severity of the disease Zhao, et al. [6]. As reported by Nagla, et al [7], patients from three hospitals in Wuhan, Shenzhen, and China showed the likelihood of association between ABO blood groups and the susceptibility to COVID-19 exposure after the outbreak of the COVID-19 infection. The study results showed that individuals with blood group A had a markedly greater risk of COVID-19 exposure, while those with blood group O had a significantly reduced risk of COVID-19 infection. In a meta-analysis of two different case-control cohorts, blood group A was reported to confer a greater risk of aggravated COVID-19, while blood group O offer protection against COVID-19 infection WU, et al. [8]. However, A, B and O blood group are antigenic complex oligosaccharide molecules located on the extracellular surface of the red blood cell membrane Storry JR, et al. [9]. ABO blood group are also expressed on the surface of other human cells and tissues, including the epithelium, sensory neurons, platelets, and the vascular endothelium Eastlund [10]. The ABO blood group have been reported to play a key role in various human diseases such as diabetes, cardiovascular, neoplastic, carcinoma and other infectious disorders Cheng et al. [11-13]. ABO and Rh blood groups polymorphism are valuable and indispensable tools in contemporary medicine, population genetics and anthropology. The distribution of these two blood groups has been reported different populations of the world and they showed considerable variation in different geographic locations, reflecting the underlying genetic and ethnic diversity of human populations Garratty ,et al. [14,15] reported the distribution and gene frequencies of ABO and Rh [D] blood group systems in six geopolitical zones of Nigeria. Their data revealed that the ABO blood group frequencies were found in the order O [52.93%] A [22.77%] B [20.64%] and AB [3.66%] respectively among Nigeria population. This was in agreement with other studies from other parts of the world from different race and ethnic groups in USA having [O; 46.6%, A; 37.1%, B; 12.2% and AB; 4.1%] Garratty, et al [14]. Another report from a study done in Mauritania, Morocco, Cameroun, Tunisia, Ethiopia and Iran is also consistent with the Nigerian study showing [O > A > B > AB] Hamed, et al. [16-21]. The report from Madagascar and Guinea showed slightly different result [O > B > A > AB]. However, Nigerian ABO blood group results are slightly different from the study in Madagascar and Guinea that reported this trend [O > B > A > AB] Randriamanantany, et al. [22,23]. Reports from studies in India and Bangladesh showed blood group B having highest prevalence followed by O and the least was AB [B > O > A > AB] Dewan, et al. [24,25]. In Nigeria, there is a limited information of association between ABO blood groups and the susceptibility to COVID-19 in Nigeria. This study therefore, evaluated the role of ABO blood group in SARS-CoV- 2 infection susceptibility and disease severity in Lagos, Nigeria.
Methods
Study Design and Participants
This study is a case series that includes patients that are evaluated between June and August 30, 2020, and diagnosed with COVID-19.With ethical approval obtained from the Institutional Review Board [IRB] at the Nigerian Institute of Medical Research [NIMR], Yaba, Lagos, Nigeria, patient data were obtained and reviewed at the Mainland Infectious Disease Hospital and the Nigerian Institute of Medical Research, Yaba. Informed consent was also obtained from the study participants before their health records were obtained. They were confirmed to have been infected with SARS-CoV-2 by a positive reverse transcriptase polymerase chain reaction test [Qpcr] of nasopharyngeal, throat and blood samples. Clinical outcomes were also monitored and recorded. Data Collection and Statistical Analysis: Clinicians and trained research assistants retrospectively reviewed and copied patients’ health records out to a standardized data collection form. Health records copied out include demographic information, signs and symptoms presented with, co-morbidities, and patient outcome. A formal sample size was not calculated for this study because the objective of the study was to describe the clinical characteristics of the patients and their Blood group profile of participants who had enough information in their health records for analysis. Records were double entered into the forms before merging to reduce errors during data entry. Descriptive analyses were performed using Statistical Package for the Social Science [SPSS] version 25 [IBM, USA].
Results
A total of 697 COVID-19 patients were included in this study. The mean age [S.D] of the study participants is 41.32 [12.917]. COVID-19 was common in males [66.1%] than in females [33.9%]. Out of the 697 participants, 43.6% were asymptomatic while 56.4% were symptomatic showing symptoms like breathing difficulty, fever, dry cough, running nose, sore throat and others as shown on Tables 1 & 2. The most frequently detected blood group in the population was O accounting for [59.2%], followed by A 155[22.2%], B 105[15.10%] and the least is AB 24[3.4%]. Figure 1 showed the blood groups that accounted for COVID-19 severity: blood group B 11 [10.5%] followed by A 14 [9.0%], O 35 [8.5%] and AB 1 [4.2%]. There was no significant statistical difference between the blood groups in relation to COVID-19 severity [p=0.358].
Table 1: Baseline Characteristics and Symptoms of COVID-19 among the Patients.
Figure 1: Profile of Blood Groups and Percentage of SARS-CoV-2 Disease Conditions.
Table 2: Symptomatic patients (56.4%). The most common symptoms were: dry cough (27.5%), Fever 185 (26.5) and breathing difficulty (18.5%).
Tables 3 & 4 showed five [5] persons having blood group O were among the deceased [55.6%]. Four out of the 5 deceased had severe COVID-19 and were males. Their age, ranged from 53 to 65 years. The youngest being 53years was a woman who had a mild symptom of COVID-19. Three [3] women having blood group A were among the deceased [33.3%]. Aged ranged 66-75 years. Two out of these three women had mild cases and one severe COVID-19 case. This is a proof to show that old age and co morbidities are risk factors to COVID-19 disease complications and death. Five [5/ 55.6%] persons having blood group O were among the deceased four out of the 5 deceased had severe COVID-19 and were males and aged 53 to 65 years. The youngest being 53 years was a woman who had a mild symptom of COVID-19. Three [3/ 33.3%] women having blood group A were among the deceased. Their age ranged from 66 to 75.
Table 3: Co-Morbidities in covid-19 patients at presentation, N = 697.
Table 4: Blood Group Disease Condition Cross Tabulation and Percentages.
Discussion
A person’s blood group [A, B, AB and O] is determined by the presence or absence of specific antigens on red blood cells which trigger an immune response. Reports from some recent studies, suggests that ABO blood group may play a role in the immunopathogenesis of COVID-19 disease with group A conferring a higher susceptibility to infection and or severe disease and group O individuals less likely to test positive (Geol, et al. [26]) and Fan, et al. [27]. However, reports are in contrast to our current study which shows no statistical ssignificant evidence [p = 0.358] that individuals with the blood group profile A were associated with increased risk to severe cases of COVID-19. Furthermore, in moderate cases of Covid-19 infection, group B [41.9%] individuals were more represented and may have increased risk to COVID -19 susceptibility when compared to other blood groups. We also observed that most of the deceased persons [5/ 55.6%] had blood group O, were males and age 53 to 65 years. Three [3/ 33.3%] women having blood group A were equally among the deceased aged 66 to 75 years with co-morbidities which include Pneumonia, Diabetes, LRTI , Hypertension in both severe and mild cases confirming that both age and comorbidities can lead to death with COVID-19 disease. A recent study that supported our data reported that a significantly increased risk was associated with blood group B Almadhi, et al. [28], which is also comparable to findings by Latz, et al. [29] and meta-analysis by Liu, et al. [30]. In Nigeria and other parts of the globe, blood group O Rhesus positive has consistently been the most common, followed by A, then B, and AB being the least [Anifoweshe et al 2016]. According to [Geol et al 2021], group O originated in Africa before early human migration, and has anti‐A and/or anti‐B antibodies present in group O individuals which binds to the corresponding antigens on the viral envelope and contribute to viral neutralization, thereby conferring some protection by preventing target cell infection. However, our data proposed that group B and or O individuals may be more likely to be infected with COVID-19 disease suggesting that COVID -19 in Nigeria and few other studies from other parts of the world may not be affected by the anti A or B that has been proposed to confer protection to these that have it. Furthermore, ABO blood group is determined by inheritance, natural selection, showing underlying genetic and ethnic diversity which may have influenced the current frequencies of ABO types among Nigerian populations based on susceptibility to particular diseases or disorders. Hospitalization, higher infection chances, and death were found among those with blood group A and O, and ethnicity was also a factor considered to weigh COVID-19 risks in this study.
Conclusion
The ABO blood group was not associated with the presentation and recovery period of COVID-19 disease during the period of this study. However, the patients of blood group B profile seem to have higher risk of COVID-19 disease susceptibility. To further detect the susceptibility and severity of COVID-19 infection, more samples of individuals with confirmed exposure to COVID-19 infection should be conducted.
Jaundice Clinical Manifestation and Pathophysiology: A Review Article
Introduction
Jaundice is when clinically there is an increase in the amount of bilirubin in the serum rising above 85mmol/l (5mg/dl). When in utero, unconjugated bilirubin is cleared in the placenta to produce cord serum bilirubin of approximately 35mmol/L (2mg/ dl). After birth, jaundice is a reflection of the bilirubin present in the liver, the rate of hepatic excretion and the ability to bind to serum proteins to retain the bilirubin present in the plasma. Many variations in individual responses to bilirubin load prevent specific levels of psychological jaundice [1]. Therapy has proven that the benefits outweigh the harm. The physiological pattern of jaundice also varies with other factors such as prematurity and ethnicity. In hemolytic jaundice, serum bilirubin exceeds physiologic levels and can be caused by sepsis and inherited hemolytic diseases such as glucose 6-phosphate dehyrogenase (G6PD) deficiency, ABO and Rh isoimmunization [2]. Prolonged jaundice refers to jaundice that persists beyond the first two weeks of long neonatal life, and is caused by other diseases, including lateonset jaundice of the breast, congenital hypothyroidism and rare inherited disease conditions. Infants with breast milk jaundice have prolonged levels of unconjugated bilirubin in other healthy infants, and glucuronidase b in breast milk appears to be an important factor in this condition. There are two types of neonatal jaundice associated with breastfeeding, the first known as lactational jaundice associated with treatment of the breast which results in dehydration and causes the jaundice to become more intense [3]. The second is breast milk jaundice which is associated with prolonged jaundice in infants with the first two weeks of life. One or more substances such as enzymes (glucoronidase), 3 alpha, beta and 20 pregnanediol in breast milk although to be possible cause of breast milk jaundice. Jaundice is influenced by several factors, namely dehydration, weight loss after birth, bleeding, cephalohaematoma, contusions, babies in mothers with diabetes, acidosis, apixia, and gastrointestinal obstruction [4].
Discussion
Clinical Manifestation and Etiology
Patients with jaundice may not experience any symptoms, although some present with a life-threatening condition. Patients who present with acute illness, which is usually due to infection, may present with fever, chills, abdominal pain, and flu-like symptoms. In these patients, skin discoloration may not be their chief complaint. Patients with non-infectious jaundice may complain of weight loss or pruritus. Abdominal pain is a symptom that usually appears in pancreatic or biliary tract carcinomas. Occasionally patients present with jaundice and accompanying extrahepatic manifestations of liver disease
Jaundice can be caused by a number of things, including [4,5]:
a. Haemolysis due to ABO or Rh isoimmunisation, resulting in G6PD. deficiency
b. Hereditary spherocytosis, drugs
c. Sepsis – septicaemia, meningitis, UTI and intra-uterine infections
d. Polycythaemia
e. Psychological and idiopathic jaundice f. Breastfeeding and Breastmilk jaundice.
There is a reduction in the erythrocyte cycle in normal newborns (70 to 80 days in infants and 120 days in adults) increasing the amount of bilirubin in neonates. Hereditary hemolytic changes lead to increased RBC turnover and increased risk of hyperbilirubinemia. This causes hemolysis in newborns which is divided into several causes, namely first, damage to RBC metabolism resulting in G6PD and pyruvate kinase deficiency. The second is RBC membrane damage, of which congenital sporocytosis is an important factor. The third is impaired hemoglobin production where alpha thalassemia syndrome is the main cause in newborns. Fourth is an inherited immune hemolytic disease called medelian trait [6] (Figure 1). Schematic drawing of bilirubin production in neonates [7]. Bilirubin metabolism occurs in three phases, including the prehepatic, intrahepatic and posthepatic phases. Dysfunction in one or more of these phases can lead to jaundice [8].
Figure 1.
a. Prehepatic jaundice
The human body produces approximately 4 mg/kg of bilirubin per day from heme metabolism. Approximately 80% of heme is the result of erythrocyte catabolism, with the remaining 20% resulting from ineffective erythropoiesis and the breakdown of muscle myoglobin and cytochromes. Bilirub that is formed will be transported from the plasma to the liver to be conjugated and excreted.
b. Intrahepatic jaundice
Unconjugated bilirubin is both fat soluble and water insoluble, and therefore can easily cross the blood-brain barrier or cross the placenta. In hepatocytes, unconjugated bilirubin will be conjugated with sugar catalyzed by the glucuronosyltransferase enzyme and finally dissolved in bile.
In the intrahepatic phase, disorders associated with bilirubin can be divided into three subgroups [5,9]:
1. Excessive production of bilirubin
2. Disturbance in the conjugation process
3. Impaired excretory function
c. Posthepatic Jaundice
After dissolving in bile, bilirubin is transported through the bile duct and cystic duct for temporary storage in the gallbladder, or through the ampulla of Vater and into the duodenum. In the intestine, some bilirubin will be excreted in the feces, while the rest is metabolized by the normal intestinal flora into urobilinogen and will then be reabsorbed. Most of the urobilinogen will be filtered from the blood by the kidneys and excreted in the urine. A small amount of urobilinogen is absorbed in the intestine and excreted into the bile [8,9].
Jaundice can be classified into three main groups. This division is based on the presence of bilirubin found in serum [10]:
a. Unconjugated (indirect)
Albumin is insoluble in blood, therefore albumin is bound to blood. The free bilirubin is then combined with albumin and transported to the liver. In the liver there is an uptake mechanism, so that bilirubin is bound by liver cell membrane receptors and enters the liver. As soon as it is present in the liver cells, ligandin (Y protein), Z protein and other hepatic glutathione compounds occur which carry it to the hepatic endoplasmic reticulum, where conjugation occurs 4.
b. Conjugated (direct)
Conjugated bilirubin is formed in the rough and smooth ER, where it is conjugated with glucuronic acid. The result is water-soluble bilirubin (monoglucuronide and diglucuronide) a process that catalyzes glucoridation by uridine diphosphateglucuronosyltransferase, which occurs with the help of two isoenzymes. Excretion of bilirubin into bile is actively carried out by ATP-dependent transporters. Billirubin is transported into the stomach by the help of cells. Apolar glycuronide bacteria produce water-soluble unconjugated bilirubin, which can be converted to urobilinogen by reducing bacteria.
c. Albumin and bilirubin binding (indirect) [11,12].
Conclusion
Delta bilirubin is a small amount of conjugated illirubin. In serum irreversibly bound to albumin by covalent bonds. In laboratory tests to determine albumin levels, directly conjugated delta albumin is usually referred to as jaundice and is protracted, in which delta bilirubin levels rise proportionally and results jaundice.