Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
New Significant Remarks on Bekesy’s Theory of Hearing
Mini Review
The remarks concern the reception of speech perfectly modeled in the organ of speech. Discussing these procedures requires separate paper. A huge amount of information is encoded in the generated sound wave and sent to the hearing receptor, where it is received and transmitted to the hair cell. This is where the initial analysis takes place and the transmission to the centers in the brain [1]. The path of the signal is long, complicated, and the transmission must be fast and accurate [2]. There are several ambiguities in the description of this path according to Bekesy’s traveling wave theory. Many of these have already been discussed in previous papers on hearing [3]. In this work, I would like to draw attention to facts that have so far been overlooked. Voice recognition consists of many elements encoded in a sound wave. The smallest element heard is a sound, which is divided into vowels and consonants. Sounds form words. There are gaps between sounds and words. The consonants have different durations: plosives – voiceless – 70-95 ms, fricatives – 65 ms, plosive-fricative – 67 ms, voiced – 82 ms. The duration of vowels depends on the position of a given vowel. Vowels before a syllable are on average 60-80 ms.
Vowels before a pause last on average 95-118 ms. The sound properties of speech overlap with the word sequence of speech. This gives language an emotional meaning. It is the accent, intonation, length of sound and melody that express emotions by changing the modulation of the voice. Accent is achieved by pronouncing a given phrase louder, increasing its duration, or increasing or decreasing the frequency. Accent can be dynamic, rhythmic, or melodic. In Polish language, the penultimate syllable is usually stressed. Long words sometimes have double stress. The main stress is on the first syllable and the second stress is on the penultimate syllable, e.g. in the Polish word “prawdopodobnie” (probably). A given syllable can be strengthened by increasing its frequency or by increasing its duration. In an interrogative sentence, the ascending melody is important – it is a change in voice modulation to express emotion. This information is stored in the sound wave. Can it all be encoded in the way that was mapped out 96 years ago? According to Bekesy’s theory, thanks to wave resonance, information is transferred to the basilar membrane and forms a traveling wave, growing from the oval window to the cap.
There are a few problems emerging here: The sound wave is a longitudinal wave and the wave on the basilar membrane is a transverse wave. If we draw the vectors of the forces of these waves, then the addition of vectors is not so obvious. The natural vibrations of the basilar membrane were incorrectly determined. The load on the basilar membrane caused by the massive organ of Corti lying on it was not taken into account. The resonant frequency depends on the magnitude of the resistance forces in the system. Damping increases with vibration frequency, and also increases with vibration amplitude. If the fluid in the tympanic cavity – on one side of the eardrum causes an attenuation of about 30 dB [4], how much attenuation does the fluid on both sides of the basilar membrane adhering to the basilar membrane 24 hours a day cause? Bekesy erroneously assumed for his calculations that the sound wave travels on both sides of the basilar membrane and pressure differences give rise to a traveling wave. He did not take into account the Reissner’s membrane, connecting the atrial duct to the cochlear duct. There is also the problem of the difference in the speed of the sound wave in the cochlear fluids – 1450 m/s and the speed of the traveling wave on the basilar membrane – 8-100 m/s, depending on the frequency.
If the average speed of the wave traveling on the basilar membrane is assumed to be 50 m/s, then in 1 ms the sound wave travels 1450 mm, and the wave on the basilar membrane moves 50 mm. New information is recorded on every millimeter of sound wave. Is it possible to accurately record on a wave 30 times slower? How is this information encoded by the traveling wave crest? [5]. We hear female and male voices at the same time, differing in frequency and intensity – how strongly damped resonance works in such a case. How does the basilar membrane encode this? How does the enormous package of information occurring simultaneously encode the endolymph fluid driven by basilar membrane movements consistent with the amplitude and frequency of sound? A greater difficulty arises in the case of polytones. The possibility of amplifying quiet tones by the contraction of outer hair cells seems unlikely. A sound wave is not a simple harmonic wave of constant intensity and constant frequency. The mechanism of mechanical signal amplification is time-consuming and energy-intensive.
After many milliseconds, there is a completely different wave on the basilar membrane, it may not require amplification, but the new energy added disrupts the transmission of the wave that is on the basilar membrane at that time. A wave below the auditory threshold cannot be amplified by this method, because the wave does not have the energy necessary to depolarize the hair cell. If quiet sounds are amplified by 30 dB, why do we still hear them as quiet? The amplification of the auditory signal at the molecular level in the hair cell is described. It refers to a signal that has been received, but with too little energy to reach the brain [5]. In the case of a cochlear implant due to partial deafness, the insertion of electrodes into the tympanic canal immobilizes the basilar membrane. This prevents the formation of a traveling wave, cochlear fluid flow, tilting or bending of the hairs of hair cells, and the tip-link mechanism is completely disabled. Hearing is still as it was before the surgery. This indicates the existence of a different pathway for the auditory signal to the receptor. This issue was discussed in the paper “Submolecular theory of hearing” [5]. The sound wave’s resonance with the transverse wave of the basilar membrane is opposed to hearing sounds lasting tenths of a millisecond, when one or two periods of the sound wave are unable to transmit information to the basilar membrane [6,7].
Acupuncture for the Treatment of Male Infertility: A Systematic Review and Meta-Analysis
Introduction
Male infertility refers to a condition where a couple, living together for more than a year and having regular, unprotected sexual intercourse for over a year, is unable to conceive due to factors originating from the male partner [1]. Survey results show that the proportion of couples worldwide suffering from infertility reaches 15%, and in some areas, it’s as high as 30%. The incidence of infertility caused by male factors is 30% to 50% [2]. In China, the male infertility rate has reached 10% to 15%, accounting for 25% to 37% of married couples [3]. Factors such as environmental pollution, sexually transmitted diseases, drug abuse, excessive alcohol consumption, heavy smoking, mental stress, and medication misuse can all contribute to the decline in male fertility. The increasing number of male infertility patients not only affects the physical and mental health of the patients themselves but also exacerbates family relationships and adds stress to both partners. Helping infertility patients and their families improve their situation is vital for promoting China’s population structure optimization, consolidating the comprehensive establishment of a well-off society, and achieving a harmonious coexistence between humans and nature [4].
Modern medical treatments for male infertility mainly include etiological treatments such as medication, surgery, and assisted reproductive techniques, which are the mainstream methods but also come with high costs and varying degrees of limitations and risks. Traditional Chinese medicine has a long history of treating male infertility, with extensive clinical applications that can effectively compensate for the limitations of Western medicine [5]. It also has low treatment costs, increasing patients’ treatment compliance and success rates of assisted reproductive techniques [6]. The development history of traditional Chinese medicine reproductive therapy is extensive, forming unique theoretical systems such as “the kidney dominates reproduction,” “the liver as the pivot of reproduction,” “the essence chamber theory,” and “the Tian Gui theory” [7]. Traditional Chinese medicine offers various treatments for male infertility [8], including acupuncture, moxibustion, acupoint catgut embedding, acupoint injection, massage, auricular acupressure, herbal fumigation, and herbal enema.
As a treasure of traditional Chinese medicine, the traditional Chinese acupuncture therapy has a clinical history of nearly a thousand years [9]. Through long-term practice, a rigorous treatment theory system based on the basic principles of acupoint selection, such as syndrome differentiation, meridian-based acupoint selection, and proximal and distal acupoint selection, has been developed. Acupuncture has a significant effect on treating male infertility, with simple operation, minimal side effects, and significantly reduced patient suffering. When combined with moxibustion, electrotherapy, and herbal medicine, the treatment efficacy for male infertility is further enhanced [10]. Traditional Chinese medicine believes that the main causes of male infertility are the imbalance of the five internal organs, a decline of essence and qi, irregular storage and leakage, and obstruction of qi transformation.
Its treatment of male infertility is based on the theory of the “kidney stores essence and dominates reproduction,” focusing on the basic principle of “nourishing the kidney, replenishing essence, and benefiting the marrow” for acupoint selection and needle manipulation; at the same time, it selects acupoints from meridians such as the liver and spleen based on the holistic concept of traditional Chinese medicine, and also employs experience-based acupoint treatment [11]. In reviewing past randomized controlled trials on male infertility, we found that systematic review articles on acupuncture treatment for male infertility are outdated, and updating such literature would help us better assist male infertility patients in developing the latest treatment measures. Therefore, it is necessary to research the literature and conduct a systematic review and meta-analysis of the studies on acupuncture treatment for male infertility.
Methods
Literature Search Strategy
A computerized search was performed in Chinese databases: CNKI, VIP Information Resource System, CBM, and Wan Fang Data; English databases: PubMed, MEDLINE, Cochrane Library, Web of Science, and EMBASE. We searched for randomized controlled trials related to traditional Chinese acupuncture treatment for male infertility. The search was limited to Chinese and English languages, and the search period covered the time from the inception of each database until December 2022. The following keywords were used for the search: for English keywords, (“acupuncture” OR “acupuncture and moxibustion” OR “electroacupuncture”) and (Male) and (Infertility) and (Randomized Controlled Trial). For a sample search strategy, please refer to the appendix.
Inclusion and Exclusion Criteria for Literature
Inclusion Criteria for Literature: (a) Study subjects: Male infertility patients with a clear diagnosis, aged ≥18 years, without restrictions on ethnicity, education level, disease course, and severity; (b) Study type: Randomized controlled trials, without restrictions on blinding and publication type; (c) Intervention measures (experimental group VS control group): The experimental group received acupuncture at acupoints or acupuncture combined with traditional Chinese medicine therapy, or acupoint stimulation, or acupoint stimulation combined with traditional Chinese medicine therapy, or electroacupuncture combined with traditional Chinese medicine, or electroacupuncture treatment mainly based on Shu-source point combination; The control group received conventional Western medicine treatment or traditional Chinese medicine, such as herbal decoctions, traditional Chinese medicine pills, or Jiaofu Fangxuanju capsules. The baseline data of the experimental and control groups should be balanced, and the treatment courses should be consistent. (d) Relevant outcome indicators reported: The primary outcome indicator is the total effective rate, and the secondary outcome indicators are sperm density, sperm survival rate, semen volume, sperm motility (grade a and grade a+b sperm count), etc.,
Exclusion Criteria for Literature: (a) Patients with other diseases requiring treatment outside of the intervention measures; (b) Duplicate publications; (c) Inability to extract valid data, and the original author cannot be contacted for information; (d) Non-Chinese and non-English literature.,
Literature Screening, Data Extraction, and Bias Risk Assessment of Included Studies: All literature screening and data extraction were independently performed by two reviewers and crosschecked. In case of disagreement, the reviewers discussed the issue, and if no consensus could be reached, a third-party reviewer was consulted. The data extraction of included literature was conducted according to a pre-designed data extraction table, including title, author, publication time, sample size, patient gender, patient age, intervention measures, treatment duration, and outcome indicators, etc. The Cochrane ROB2 tool was used for the quality assessment of RCTs, covering five domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. Each domain is evaluated as high risk, some risk, or low risk, and a final overall assessment is produced after considering all domains.,
Statistical Methods,
Rev Man 5.4 (Cochrane Collaboration) was used for statistical analysis. For a specific outcome indicator, if at least two studies were reported on it, a meta-analysis was performed. The Q-test and I2 were used to assess the heterogeneity of the studies, and if I2 ≥50% (P≤0.1), a random-effects model was applied; otherwise, a fixed-effects model was used. The outcome of this study was a binary variable, with the odds ratio (OR) as the effect indicator. For outcome indicators measured using the same scale, the mean difference (MD) and 95% CI were used as effect statistics for analysis. If a study had multiple measurement time points, only the last time point data were included in the analysis. If the required data were not reported in the study, the available data in the article were used for conversion. For data that could not be included in a meta-analysis, a textual description was used for summarization. A P-value of <0.05 was considered statistically significant.
Results
Search Results
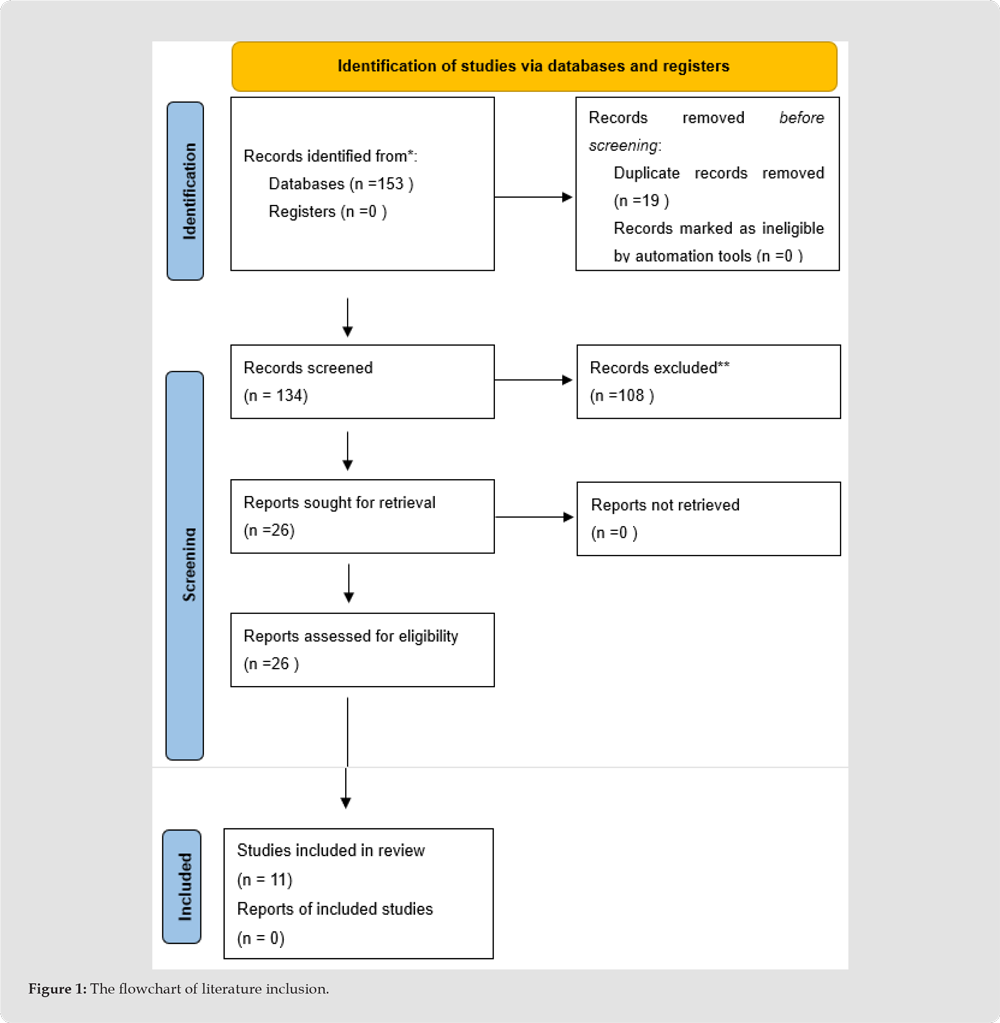
A total of 153 articles were retrieved, with 102 from Chinese databases and 51 from English databases. After removing duplicates using Note Express software, 19 articles were removed; after reading keywords and abstracts, 108 articles were removed; after carefully reading the full text, 15 articles were removed. Finally, 11 RCT studies [12-22] met the inclusion criteria. The flowchart of literature inclusion is shown in Figure 1.
Figure 1
Basic Characteristics of the Included Studies
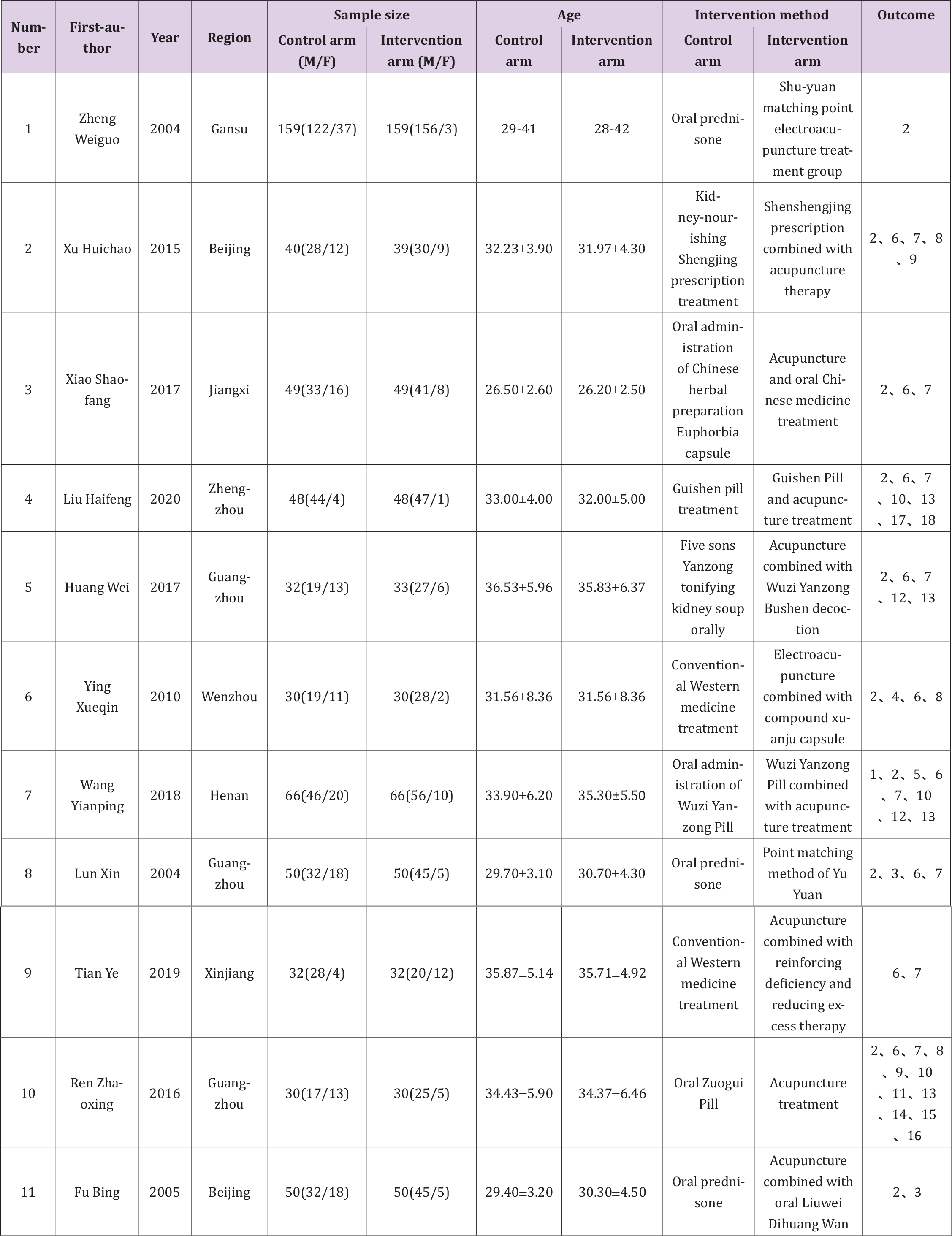
These include experimental design, researchers, intervention measures, and outcome measurement indicators. See Table 1.
Design and Intervention Measures of the Included Studies:
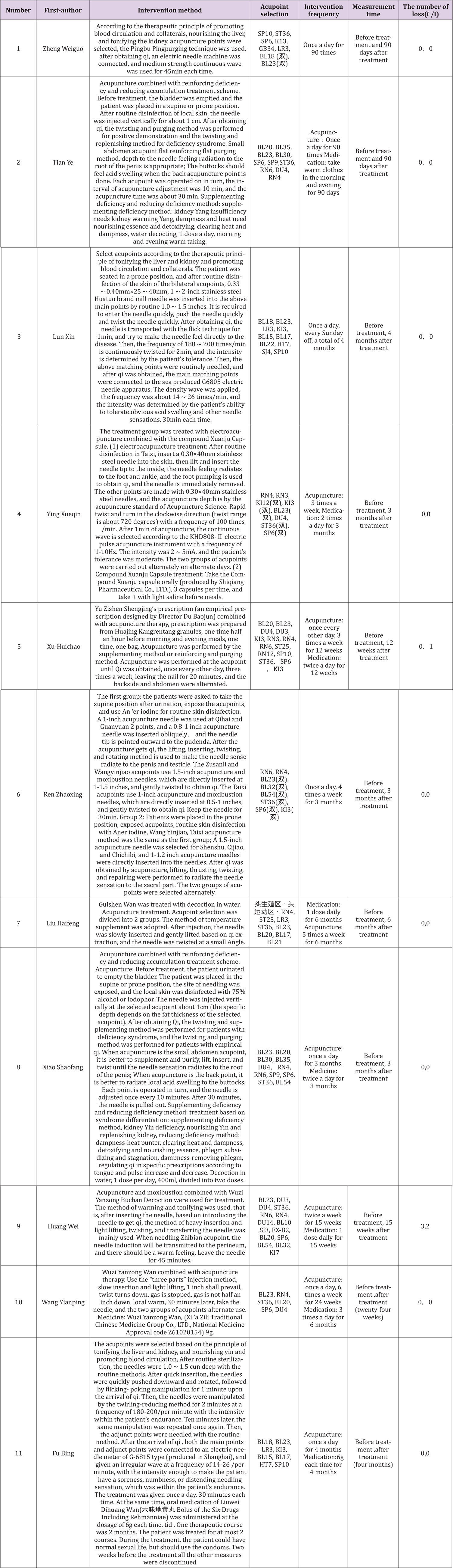
All 11 included studies were randomized controlled trials, conducted in China. The studies covered Gansu Province (1), Guangzhou Province (3), Wenzhou City (1), Beijing (2), Zhengzhou City (1), Jiangxi Province (1), Henan Province (1), and Xinjiang Uygur Autonomous Region (1). The number of cases included in the studies ranged from 60 to 318, totaling 1,172 cases. Among them, 3 studies compared acupuncture with other measures (including Western medicine or other traditional Chinese medicine therapies) for treatment, and 8 studies compared acupuncture combined with other therapies (including Western medicine or other traditional Chinese medicine therapies) with other measures (including Western medicine or other traditional Chinese medicine therapies) for treatment. Specific intervention methods are shown in Table 2.
Table 1: Characteristics of included studies.
Note: 1、serum testosterone levels before and after treatment; 2、therapeutic efficacy comparison; 3、changes in serum and/or semen AsAb positivity before and after treatment in both groups; 4、comparison of semen liquefaction efficacy between the two groups; 5、abnormal sperm morphology; 6、sperm density before and after treatment in both groups; 7、PR value before and after treatment in both groups; 8、PR+NP of patients’ sperm before and after treatment; 9 、traditional Chinese medicine symptom score before and after treatment in both groups; 10、semen volume before and after treatment in both groups; 11、total number of sperm before and after treatment in both groups; 12、motility a (%) before and after treatment in both groups; 13、sperm survival rate before and after treatment in both groups; 14、normal sperm morphology before and after treatment in both groups; 15、semen pH value before and after treatment in both groups; 16、semen liquefaction time before and after treatment in both groups; 17、comparison of kidney yang deficiency syndrome scores before and after treatment in both groups; 18、comparison of sexual function before and after treatment in both groups.
Table 2: Characteristics of each.
Outcome Measurement Indicators of the Included Studies: Ten studies compared the clinical effects before and after treatment between the two groups; nine studies compared sperm density before and after treatment between the two groups; eight studies compared PR values before and after treatment between the two groups; two studies compared grade a sperm motility before and after treatment between the two groups; two studies compared semen volume before and after treatment between the two groups; three studies compared sperm survival rate before and after treatment between the two groups; two studies compared PR+NP values before and after treatment between the two groups.
Quality Assessment and Bias Risk Evaluation
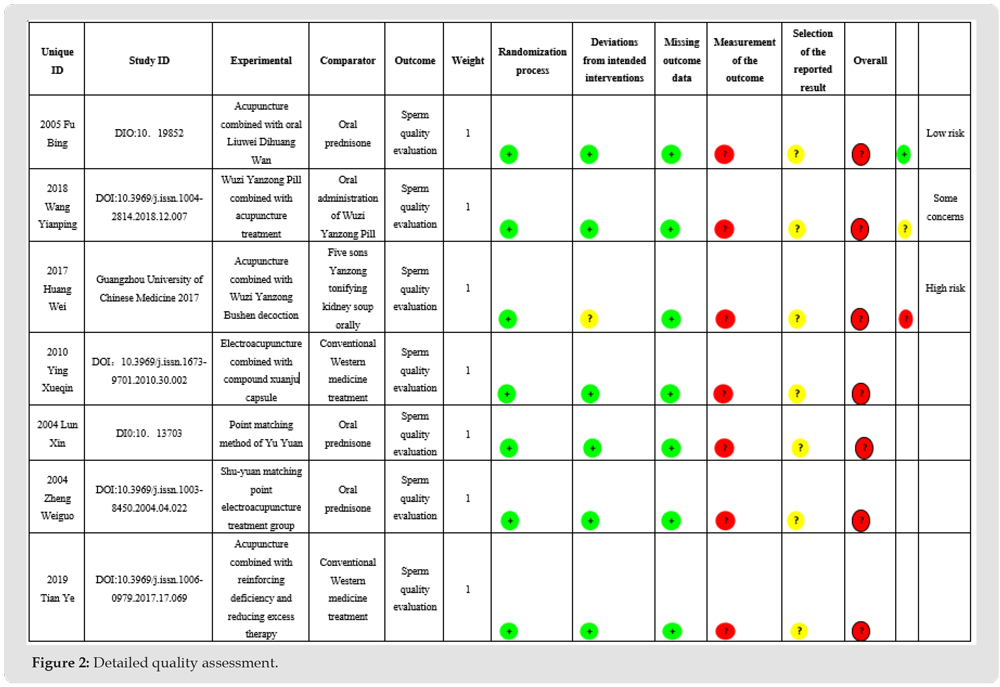
All 11 included studies mentioned randomization, with 2 using computer-generated random number tables for grouping, 3 using opaque envelopes for grouping, 2 using randomization by the order of visit, and 4 using random patient selection for grouping. All 11 studies had no selective reporting bias or other biased sources. Detailed quality assessment is shown in Figure 2. Due to the Good Similarity of the Included Studies, A Meta-Analysis was Conducted
Figure 2
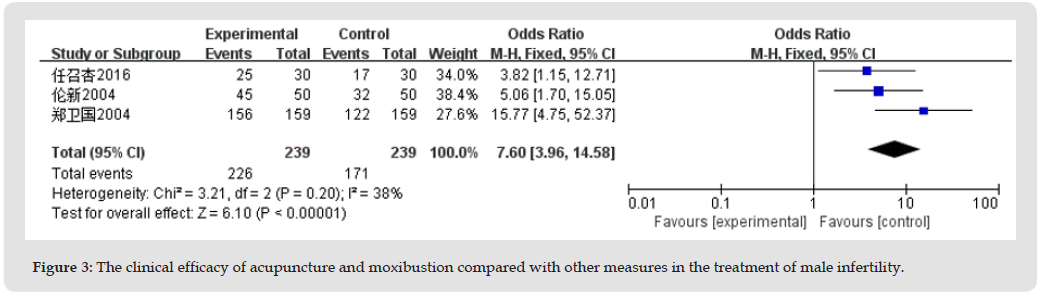
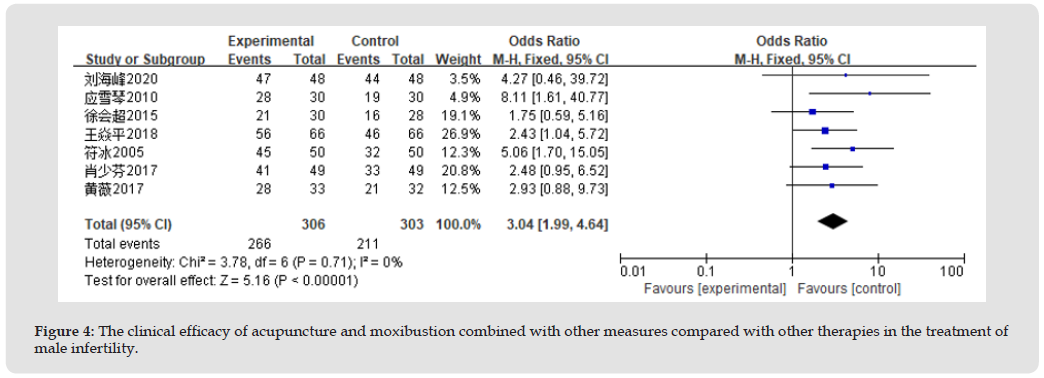
Clinical Efficacy: A total of 10 studies analyzed the clinical efficacy of acupuncture in treating male infertility, with a total sample size of 1087. Among them, three studies analyzed the effect of acupuncture compared to other measures, with certain heterogeneity between studies (I2=38%, P=0.20), using a fixed-effects model. Meta- analysis results showed that the clinical efficacy of acupuncture in treating male infertility was better than that of other measures (OR=7.60, 95% CI: 3.96-14.58), as shown in Figure 3. Seven studies analyzed the combination of acupuncture and other measures compared to other treatments, with no significant heterogeneity between studies (I2=0%, P=0.71), using a fixed-effects model. Meta-analysis results showed that the clinical efficacy of acupuncture combined with other measures in treating male infertility was superior to the control group (OR=3.04, 95% CI: 1.99-4.64), as shown in Figure 4.
Figure 3
Figure 4
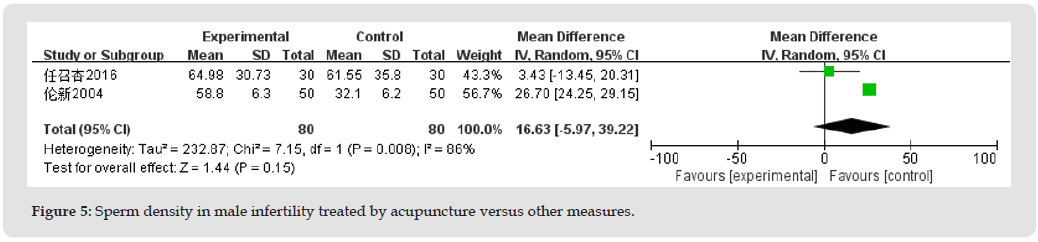
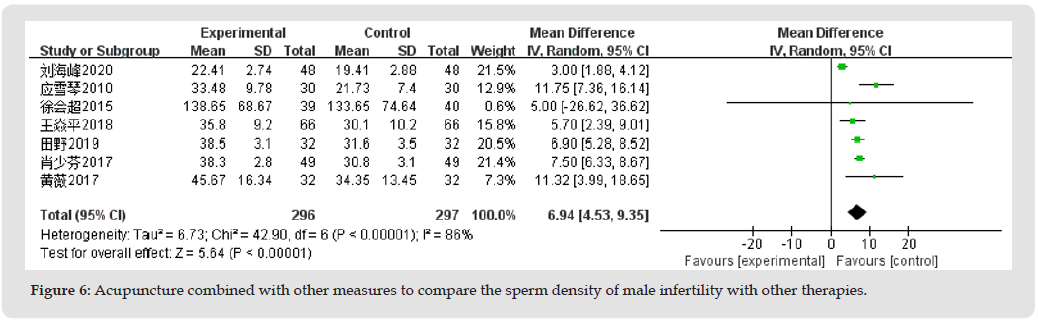
Sperm Density: Nine studies analyzed the sperm density of male infertility treated with acupuncture, with a total sample size of 753. Among them, two studies analyzed acupuncture compared to other measures, with certain heterogeneity between studies (I2=86%, P<0.008), using a random-effects model. The meta-analysis results demonstrate that acupuncture therapy improves sperm density in male infertility patients compared to the control group. (MD=16.63, 95% CI: -5.97-39.22), as shown in Figure 5. Seven studies analyzed the combination of acupuncture and other measures compared to other treatments, with certain heterogeneity between studies (I2=86%, P<0.00001), using a random-effects model. Meta-analysis results showed that the combination of acupuncture and other measures improved sperm density in male infertility better than the control group (MD=6.94, 95% CI: 4.53-9.35), as shown in Figure 6.
Figure 5
Figure 6
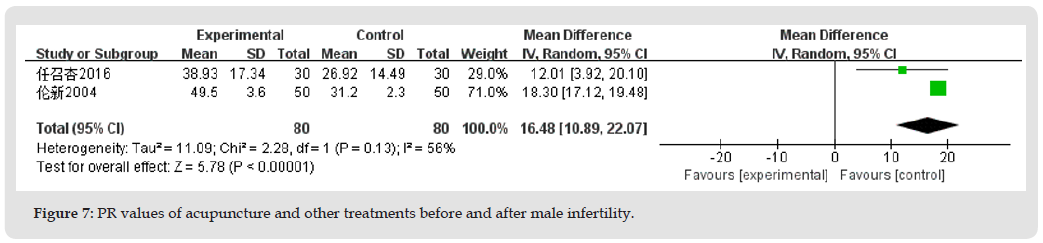
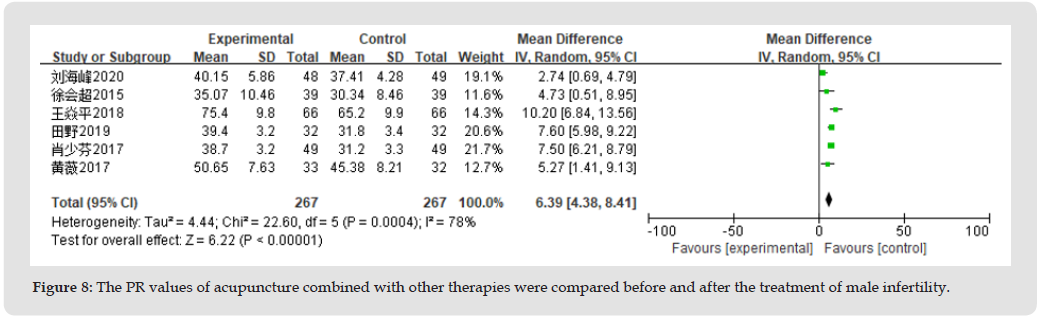
Progressive Motility (PR): Eight studies analyzed the PR value before and after acupuncture treatment for male infertility, with a total sample size of 694. Among them, two studies analyzed acupuncture compared to other treatments, with certain heterogeneity between studies (I2=56%, P=0.13), using a random-effects model. Meta-analysis results showed that acupuncture treatment improved PR values in male infertility better than the control group (MD=16.48, 95% CI: 10.89-22.07), as shown in Figure 7. Six studies analyzed the combination of acupuncture and other treatments compared to other treatments, with certain heterogeneity between studies (I2=78%, P=0.0004), using a random-effects model. Meta-analysis results showed that the combination of acupuncture and other treatments improved PR values in male infertility better than the control group (MD=6.39, 95% CI: 4.38-8.41), as shown in Figure 8.
Figure 7
Figure 8
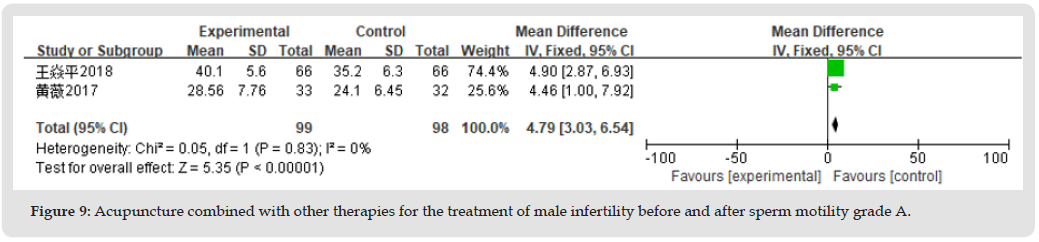
Sperm Motility Grade A: Two studies analyzed sperm motility grade A before and after acupuncture treatment for male infertility, with a total sample size of 197. No significant heterogeneity was found between studies (I2=0%, P=0.83), using a fixed-effects model. Meta-analysis results showed that the combination of acupuncture and other treatments improved sperm motility grade A in male infertility better than the control group (MD=4.79, 95% CI: 3.03-6.54), as shown in Figure 9.
Figure 9
Semen Volume: Two studies analyzed the effect of acupuncture combined with other therapies compared to other therapies alone on semen volume before and after treatment for male infertility, with a total sample size of 228. There was significant heterogeneity between the studies (I2=84%, P=0.01), and a random-effect model was used. Meta-analysis results showed no significant difference between acupuncture combined with other therapies and the control group in improving semen volume in male infertility (MD=0.30, 95% CI:-0.23- 0.82). See Figure 10.
Figure 10
Sperm Viability: Three studies analyzed the sperm viability of acupuncture combined with other therapies compared to other therapies alone for male infertility, with a total sample size of 293. There was some heterogeneity between the studies (I2=39%, P=0.19), and a fixed-effects model was used. Meta-analysis results showed that acupuncture combined with other therapies was more effective in improving sperm viability in male infertility compared to the control group (MD=8.68, 95%CI:6.82-10.53). See Figure 11. PR+Non-progressive (NP) Value: Two studies analyzed the PR+NP value of acupuncture combined with other therapies compared to other therapies alone for male infertility, with a total sample size of 139. There was significant heterogeneity between the studies (I2=80%, P=0.03), and a random-effects model was used. Meta-analysis results showed that acupuncture combined with other therapies was more effective in improving the PR+NP value in male infertility compared to the control group (MD=9.87, 95%CI:-1.69-21.42). See Figure 12.
Figure 11
Figure 12
Publication Bias Assessment
Due to the inclusion of fewer than 10 articles in this study, a publication bias assessment was not performed.
Discussion
The meta-analysis of 11 articles included in this study showed that acupuncture treatment for male infertility is diverse and has a significant positive effect on clinical outcomes in patients with male infertility, with all prognostic indicators better than using Western medicine or traditional Chinese medicine alone. Male infertility in traditional Chinese medicine falls under the categories of “infertility” and “sterility,” with complex etiology [23,24]. Some studies believe that kidney essence deficiency is the key pathogenesis of the disease, and the basic treatment method is to tonify the kidney and replenish the essence [25]. As Feng’s Golden Prescriptions Secret Record states, “If the essence is sufficient, a hundred diseases will not occur; if the essence is exhausted, all evils will arise.” External evils invade due to essence deficiency, first affecting sperm quality. Other studies point out that blood stasis is an essential factor in the occurrence of infertility and consider kidney deficiency and blood stasis as the core pathogenesis of male infertility [26]. Additionally, damp heat pouring downward can cause dead sperm and blood stasis to block the essence channels, which is also one of the main reasons for infertility [27]. Furthermore, the liver and kidney share the same origin, and when the liver fire is excessive, it scorches kidney water, and water cannot nourish the wood, which can also affect reproductive function.
In a review of previous literature, it was found that various acupuncture techniques have been used in different studies. In the included studies of this research, acupuncture techniques such as twisting and reinforcing-reducing manipulation, even-reinforcing-even-reducing manipulation, burning heavenly fire, and penetrating heavenly coolness were applied, with twisting and reinforcing-reducing manipulation being the most common. The reinforcing method involved smaller twisting angles (around 180°), slower frequency, and fewer repetitions, while the reducing method involved larger twisting angles (over 360°), faster frequency, and more repetitions. This is in line with the reinforcing-reducing rules along the meridians. After obtaining the sensation of qi during acupuncture, a smaller twisting angle, lighter force, slower frequency, and shorter operation time indicate the reinforcing method, while a larger twisting angle, heavier force, faster frequency, and longer operation time indicate the reducing method. For patients with excess syndrome, the reducing method is used, and for patients with deficiency syndrome, the reinforcing method is applied, following the principle of “tonify the deficiency and reduce the excess”[28].
In terms of acupoint selection, this study found that the most frequently used acupoints were Shenshu, Guanyuan, Zusanli, Qihai, and Sanyinjiao. Research by Zhao Yu, et al. [29] indicated that the common acupoint combinations include Guanyuan-Qihai-Sanyinjiao on the front side and Shenshu-Ciliao on the back side, with Zusanli as an additional point. This is consistent with the findings of this study. The “Compendium of Acupuncture and Moxibustion” states that Guanyuan can treat conditions such as spermatorrhea and sterility. Guanyuan belongs to the Ren Meridian, which is where essence is stored in men. It is the meeting point of the Ren Meridian and the three Yin meridians of the foot and the gathering point of the Small Intestine Meridian. It can regulate Chong and Ren channels, warm Yang, tonify the Kidney, and consolidate the foundation. Sanyinjiao is the meeting point of the three Yin meridians of the foot, governing the Qi of the liver, spleen, and kidneys. It mainly functions to invigorate the spleen, soothe the liver, nourish blood, and activate blood circulation. When reduced, it can regulate the essence chamber, dispel pathogenic factors, and promote the generation of new essence. It is an essential acupoint for treating male reproductive diseases. Shenshu is located on the back and waist area of the Bladder Meridian, corresponding to the kidneys and the perfusion of Qi and blood, and is indicated for diseases such as exhaustion, emaciation, deafness due to kidney deficiency, and chronic coldness in the water organs [30].
In recent years, acupuncture treatment for male infertility has been widely used in clinical practice, providing an alternative for patients who are unwilling to undergo drug therapy or for whom drug therapy has not effectively alleviated their condition. The results of this study suggest that acupuncture, either as a standalone treatment or in combination with other therapies, may play a positive role in improving male infertility. Compared to previous systematic reviews on the same subject, the effect of acupuncture in treating male infertility is found to be very significant. It was found in this study that the treatment effect of acupuncture combined with other therapies is better than that of acupuncture alone, suggesting that the combination of acupuncture with other therapies has potential application value in the clinical treatment of male infertility.
Limitations
All the included literature in this study comes from China, which may result in regional bias. Some studies only mention the word “random” without specifying the randomization method. Most studies have issues with allocation concealment and blinding, which may affect the quality of the evidence in the research results. Due to the unique nature of acupuncture, it is difficult to implement blinding for researchers and patients, but blinding should be implemented in data collection, efficacy evaluation, and statistical analysis. This study includes a relatively small number of studies, which may impact the strength of the conclusions drawn from the research results. More high-quality evidence is needed to supplement these findings.
Conclusion
In summary, the results of this study suggest that acupuncture, whether used as a standalone therapy or as an adjunct therapy, is safe and effective in the treatment of male infertility and is superior to Western medicine. It has particular clinical advantages in improving clinical symptoms and can be used as a supplementary treatment for Western medicine in the treatment of male infertility without increasing the risk of adverse reactions.
Declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Competing Interests
The authors declare that they have no competing interests.
Funding
This work was supported by the National Natural Science Foundation of China(No:82260967), Key Research and Development Plan of Ningxia Hui Autonomous Region(No:2022BEG02040), Natural Science Foundation of Ningxia Hui Autonomous Region (No:2022AAC05030), Key Research and Development Plan of Ningxia Hui Autonomous Region( No:2021BEB04023), Key Research and Development Plan of Ningxia Hui Autonomous Region(No:2021BEG02041) and School-level project of Ningxia Medical University(No:XZ2021004).
Authors’ Contributions
ZAZ, FW, MYL and XLJ performed the meta-analysis and wrote the first draft of manuscript, ZAZ, LX, ZDL, Mireayati Miredili and ZTG systematically searched and selected the literature, ZAZ, XXX, LJM, SZ and BG revised the final manuscript. All authors read and approved the final manuscript.
GATA Transcription Factors in Hematological System
Introduction
The GATA transcription factors are evolutionarily conserved among animals, plants flies, worms and fungi (Kudla [1-5]). The GATA family of vertebrate DNA binding regulatory proteins is expressed in diverse tissues and at different times of development. Up to date, six members of the GATA family have been characterized (GATA1-6) which are homologous in mammals, avians and amphibians (Laverriere, et al. [6]). Among these GATAs, GATA1/2/3 are expressed in both hematopoietic lineage and non-hematopoietic cells where their pattern of expression is complicated and may exhibit some minor species variation (Orkin, et al. [7-8]). Several findings reported that GATA2 and GATA3 also exhibited significant functions in the central nervous system, skin, prostate, mammary gland and kidney (Grote, et al. [9-13]). The GATA 4/5/6 are expressed in non-hematotopoietic cells, particularly in the development of heart and gut (Orkin, et al. [6,7,14]).
GATA is a zinc finger protein that contains a set of cysteines and/ or histidines within a short region of polypeptide chain and binds to a recognition sequence (A/T) GATA(A/G) via the highly conserved C-terminal zinc finger (Wall et al. [7,15,16]). The Zinc finger domain in transcription factors was first discovered in the Xenopus transcription factor IIIA (TFIIIA) (Brown, et al. [17]). In general, transcription factors in this family contain an antiparallel -sheet and -helix. Two cysteines, which are near the turn in the -sheet region and two histidines which are in the -helix, coordinate a central zinc ion in the form of Zn2+ and hold these secondary structures together to form a compact globular domain. A single zinc finger domain binds DNA via a short -helix in the major groove of the B-DNA and wrap around the double helix of DNA (Pevletich [18]). Each finger has a similar way of binding the DNA and makes base contacts with a three-base-pair subside. All GATA transcription factors have a zinc finger in the form Cys-X2-Cys-X17-Cys-X2-Cys. Among the GATA factors, the N-terminal finger exhibits a variety of functional roles. However, the common role of N-terminal in all GATAs is that it is able to interact with Friend Of GATA (FOG) protein (FOX, et al. [19).
GATA-1
The transcription GATA-1 is a key regulator of erythroid and megakaryocytic commitment during hematopoiesis. In contrast, GATA-1 prevents granulocyte-monocyte and lymphoid development (Orkin, et al. [7,20,21]). GATA-1 also expresses in mast cell, megakaryocytes and multipotential myeloid lines (Crotta, et al. [22-24]). Interaction of GATA-1 to FOG-1 (Friend of GATA) via the N-terminal zinc finger cofactors is necessary for erythroid or negative development. However, there is down regulation of the cofactors that are necessary for granulocyte- monocyte and lymphoid commitment such as PU. 1, PAX5 and IL-7. GATA1 is also involved directly in the survival of the erythroid precursors. Target genes that are involved in cell cycle regulation or proliferation and differentiation are activated by GATA1 (Chang, et al. [25-27]). Human diseases have been linked to mutations in the GATA1 N-terminal activation domain and the N-zinc finger. Acquired mutations in GATA1 are associated with acute megakaryoblastic leukaemia (AMKL) and transient abnormal myelopoiesis (TAM) in children with Down syndrome (DS). In fact, GATA1 is essential for megakaryocyte and platelet development. Therefore, dysregulation of GATA1 expression may lead to thrombocytopenia or platelet disorders. (Wechsler, et al. [21,28]).
GATA-2
The gene of GATA-2 is located in mouse chromosome 6 (Ciciotte, et al. [29]) and is highly expressed in the ventral region of the embryo by the end of gastrulation and later is expressed in the blood island region and the central nervous system (Kelly, et al. [30]). GATA- 2 mRNA is expressed in both hematopoietic cells, e.g. hematopoietic stem cells, mast cells, megakaryocytes, erythroblasts and neutrophils, and other cell types, e.g. embryonic brain cells and endothelial cells (Yamamoto, et al. [12,31-35]). GATA-2 transcription factor also exhibited crucial functions in organogenesis including gonad, placenta, kidney, prostate, ear, tissue, pituitary and thyroid gland (Tremblay, et al. [5]). In the hematopoietic lineage, the transcription factors GATA-1 and GATA-2 show restricted and largely overlapping expression profiles, but GATA-2 is uniquely expressed in early hemopoietic progenitors and mast cells. GATA-2 plays role in early murine hematopoiesis and is consistent with its expression both in early Xenopus embryos and in mammalian hematopoietic progenitors (Zon, et al. 32,36-38]). GATA-2 also has been found to appear as a phosphoprotein in hematopoietic progenitor cells, and stimulation of progenitors with interleukin- 3 (IL-3) results in enhanced phosphorylation of GATA-2 which occur within 5 min (Towatari, et al. 39]).
GATA2 is critical for the maintenance and function of hematopoietic stem cells. Mutations in GATA2 have been linked to familial predisposition to myelodysplastic syndromes (MDS) and AML. These mutations often affect the self-renewal capacity and differentiation potential of hematopoietic stem cells (HSCs) (Wlodarski, et al. [21,40]). Up to date, GATA2 mutation have been involved in some complex clinical syndromes overlapping features which include familial myelodysplastic syndrome (MDS), AML, Mono MAC syndrome characterized by peripheral monocytopenia, Emberger syndrome (primary lymphedema with MDS), and B- and NIC-cell lymphocytopenia, increased susceptibility to mycobacterium infection and a predisposition to acute myeloid leukaemia and myelodysplastic syndrome. Patients with familial AML-MDS associated with GATA2 mutation have increased risks for severe infections, particular intracellular organisms. (Abunimye, et al. [21]).
GATA-2 and Mast Cells
Mast cells are derived from hematopoietic stem cells and need GATA-2 for maintenance of their early progenitors (Tsai, et al. [41]). GATA-2 appears at high levels in hematopoietic stem cells and mast cells, especially proliferating mast cells (Martin, et al. [42-45]). In general, the C-terminal zinc finger protein is required for binding while the N-terminal finger assists with it to provide full stability and specificity of binding (Leonard, et al. [46]). In mast cells, there are several GATA-binding sites in cis regulatory elements in promoters and in enhancers of expressed genes including the IgE receptor chain enhancer and chain promoter, the mast cell chymase promoter, mouse mast cell protease (MMCP) promoters, the mast cell specific IL-4 enhancer and carboxypeptidase A promoter (Weiss, et al. [32,47,48]). Although GATA-1 and GATA-2 have been reported to co-express in mature mast cells (Zon, et al. [32-33]), GATA-1 cells derived from yolk sac or fetal liver of GATA-1+/- chimeric mice can differentiate into mast cells at normal frequency and with a similar phenotype as the wild type mast cells suggesting that GATA-1 is largely dispensable for mast cell development (Pevny, et al. [49]). Introduction of GATA-2 antisense in ES cells abrogated erythromyeloid colony-forming ability and this hematopoiesis-deficient phenotype could be rescued by ectopic expression of full-length GATA-2. In addition, GATA-2 knock out embryonic stem cells show a profound deficiency of mast cell colonies, and GATA-2 knock out embryos die with severe anemia. These studies suggest the important role of GATA-2 in early hematopoiesis and mast cell development (Tsai, et al. [41,50,51]). Recently, GATA2 promotes robust gene transcription to maintain mast cell identity and respond to antigenic stimulation by binding to super-enhancer regions with dense GATA2 binding sites available at key mast cell genes (Li, at al. [52]).
GATA-3
GATA-3 is found exclusively in the commitment to early T cell durring T cell lineage development of hematopoietic lineage and immune regulation. GATA-3 also plays a role in the long-term self-renewal of HSCs through the control of cell cycle entry (Frelin, et al. [53,54]). In addition, the development of CD4+ Th2 cells can be promoted by GATA3. Increased expression of GATA3 identifies a biologically distinct subgroup in peripheral T cell lymphoma associated with overall poor prognosis (Abunimye, et al. [21]). The gene expression profile of the GATA3 subset of peripheral T cell lymphoma also identifies increase expression of Th2 associated transcripts. This observation provides insight in understanding the pathogenesis and potential oncogenic pathways for the peripheral T cell lymphoma. Interestingly, aberrant expression of the T cell transcription factor GATA3 is observed in B cell-derived Hodgkin Reed-Sternberg tumor cells. The dysregulated GATA3 expression is likely due to constitutive binding of NFkB and Notch-1 pathways to GATA3 promoter elements (Abunimye, et al. [21]).
Aberrant expression or dysregulation of GATA3 has been implicated in T-ALL. In some cases of T-ALL, GATA3 expression levels may be altered or mutations affecting GATA3 function can contribute to leukemogenesis. These alterations could disrupt normal T-cell development and differentiation, leading to the uncontrolled proliferation of leukemic T cells. GATA3 is crucial for directing T-cell differentiation towards the T-helper 2 (Th2) cell lineage. Its dysregulation might influence the balance of T-cell subsets, potentially impacting immune responses and contributing to leukemic transformations (Hosoya, et al. [21,55]).
Conclusion
GATA1/2/3 exhibit many biological roles in both functions in hematological system and leukemogenesis which affect human health and diseases. Understanding the normal biological functions and its crucial roles in leukemogenesis of the GATA transcription factors (GATA-1, GATA-2, GATA-3) in blood system could have implications for diagnosis and potential future therapeutic interventions.
Acknowledgement
We would like to thank Suranaree University of Technology, Thailand for supporting this manuscript.
Unraveling the Mystique: Augmented Insights into Stem Cell Biology and Nanogenomic Engineering
Introduction
Introduction to the Revolutionary Impact of Stem Cell Biology
Stem cell biology represents a transformative shift in medical science, revolutionizing our understanding and treatment methodologies for a myriad of diseases [1-3]. Stem cells, with their unique propensity to differentiate into various cell types, have become the linchpin of regenerative medicine [4]. This offers unprecedented prospects for tissue and organ repair and potential remedies for diseases once deemed incurable [5]. Notably, the advent of induced pluripotent stem cells (iPSCs) has marked a significant advancement by mitigating immune rejection and ethical dilemmas, while the integration of nanotechnology has refined the precision and effectiveness of stem cell-based therapies [6]. The influence of stem cell biology extends beyond conventional therapeutic boundaries, particularly in immunology, where engineered immune cells are designed to target and eliminate cancer, and in tissue engineering, which aspires to cultivate lab-grown organs [7-9]. Despite the promise, the path is fraught with challenges, including ethical quandaries, genomic stability, and potential tumorigenicity [10]. These complexities necessitate comprehensive research and strict regulatory oversight. Moreover, the intricate interplay between stem cells and the immune system presents both opportunities and obstacles, underscoring the need for ensuring the safety and efficacy of these therapies [11,12].
The Quest for Understanding: Deciphering the Molecular and Genomic Foundations of Stem Cells: Embarking on a quest to decode the molecular and genomic complexities of stem cells is akin to exploring the fundamental codes of life [13,14]. This journey, at the intersection of regenerative medicine, immunology, and nanotechnology, seeks to understand the signaling pathways, transcription factors, and epigenetic mechanisms that dictates stem cell behavior and potential [15]. At the molecular level, stem cells are paradigms of biological finesse, boasting remarkable self-renewal capabilities and the ability to differentiate into a diverse spectrum of specialized cells [16]. Central to this process are the signaling pathways, transcription factors, and epigenetic modifications that collectively direct cellular fate [17]. Advanced techniques like CRISPR-Cas9 and RNA sequencing have become instrumental in mapping the transcriptomic landscape, illuminating the molecular switches crucial for stem cell behavior [18].
Concurrently, the genomic landscape of stem cells presents a vast reservoir of information, revealing regulatory networks essential for maintaining pluripotency and guiding differentiation [19]. Addressing issues of genomic instability and mutations is critical for the secure application of stem cell therapies [20]. The use of sophisticated tools like single-cell genomics is imperative for detailed monitoring and understanding [21]. The incorporation of nanotechnology has catalyzed a paradigm shift in stem cell research, providing precise tools to manipulate and understand cells at both molecular and genomic scales [22]. Nanoscale technologies enable the targeted delivery of genetic material, real-time tracking of cellular dynamics, and the potential to modulate cell behavior through external stimuli [23,24].
The Molecular Architecture of Stem Cells
Architectural Complexity of Stem Cells: Balancing Self-Renewal and Differentiation: The molecular architecture of stem cells epitomizes the intricate balance between self-renewal and differentiation, fundamental to their therapeutic potential [25]. These dual properties define stem cells’ unique role in regenerative medicine. Self-renewal is orchestrated by a complex interplay of signaling pathways such as Wnt, Notch, and Hedgehog, and transcription factors such as Oct4, Sox2, and Nanog [26]. These elements meticulously maintain the equilibrium between proliferation and pluripotency [27]. Conversely, differentiation is the transformative journey from stem cells to specialized cell types, driven by a synergy of extrinsic signals and intrinsic epigenetic alterations [28]. This process intricately directs specific gene expression patterns and cell fates, pivotal for regenerative applications. The advent of nanotechnology has refined this domain, providing unprecedented control over the cellular microenvironment and behavior, enhancing our ability to direct these fundamental processes with precision [29].
Epigenetic Mastery in Stem Cell Fate and Function: Epigenetics emerges as a cardinal regulator in stem cells, dictating gene expression beyond the genetic code [30]. Modifications like DNA methylation and histone alteration, alongside non-coding RNA dynamics, are instrumental in maintaining pluripotency and orchestrating differentiation [31]. DNA methylation serves as a pivotal regulatory sentinel, either repressing or activating gene expression, thereby guiding gene expression patterns that are critical for establishing stem cell identity and determining lineage commitment. Concurrently, histone modifications, along with the actions of non-coding RNAs such as microRNAs and long non-coding RNAs, intricately modulate the epigenetic landscape. This modulation ensures a delicate equilibrium is maintained between the processes of self-renewal and differentiation [32,33]. Emerging technologies such as CRISPR/Cas9-mediated epigenome editing and advanced sequencing methods are revolutionizing our capacity to map and manipulate this epigenetic terrain. Despite the potential, challenges in specificity, stability, and ethical implications persist, necessitating a nuanced approach to harnessing these mechanisms for clinical application [34-36].
Unraveling Transcriptomic Diversity: Elucidating Cellular Potentials: Exploring the transcriptomic diversity of stem cells offers a profound window into their cellular potentials and underlying molecular narratives [37]. This diversity, captured through advanced single-cell transcriptomic analyses, reveals the intricate regulatory networks and intermediate states pivotal for understanding pluripotency and lineage specificity. Key transcription factors and a plethora of non-coding RNAs contribute to a complex transcriptomic landscape, governing stem cell fate and function [38-41]. These insights are crucial for regenerative medicine as they provide a foundation for enhancing disease modeling, facilitating the identification of potential drug targets, and informing the development of therapeutic cell engineering strategies. By integrating transcriptomic data with other omics layers, such as genomics, proteomics, and metabolomics, we can achieve a holistic understanding of stem cell biology. This integration reveals novel regulatory circuits and pathways essential for stem cell function and differentiation. However, the challenge lies in deciphering the vast and complex data sets to extract meaningful insights, which necessitates the application of sophisticated computational strategies and analytical tools.
Nanogenomic Engineering a Convergence of Nanotechnology and Genomic Engineering for Precision Medicine
Nanogenomic engineering is an interdisciplinary field that melds nanotechnology with genomic engineering to manipulate and edit the genome at the nanoscale level. This innovative approach employs nanoscale tools and devices to precisely target and modify genetic sequences, facilitating advanced applications in gene therapy, precision medicine, and synthetic biology. Through the integration of nanotechnology’s unparalleled precision and the vast potential for genomic modifications, nanogenomic engineering aspires to revolutionize our capacity to understand, diagnose, and treat genetic disorders. Additionally, it aims to engineer biological systems for novel functionalities.
CRISPR-Cas9: Catalyzing a Revolution in Genome Editing: Nanogenomic engineering, a pioneering domain at the nexus of nanotechnology and genomics, has ushered in a new era of medical innovation with the advent of CRISPR-Cas9 [42]. This technology, renowned for its precision and versatility, has reshaped the landscape of genome editing, opening novel pathways for gene therapy and the potential eradication of genetic diseases. CRISPR-Cas9’s ability to accurately target and modify specific genomic sequences has shifted the therapeutic paradigm from symptomatic management to the potential for targeted, curative interventions [43-46]. Nanotechnology plays a crucial role in augmenting the delivery and specificity of CRISPR-Cas9 gene editing systems, a pivotal advancement in genetic engineering. Nanocarriers, which are minute vehicles designed at the nanoscale, serve to transport CRISPR-Cas9 components directly to specific cells or tissues. This targeted delivery system optimizes gene editing efficiency by ensuring that the gene-editing tools reach their intended destinations within the body more effectively. Additionally, nanocarriers help in reducing off-target effects—a significant concern in gene editing—by enhancing the precision with which these tools edit the genome, thus mitigating unintended modifications [47-50]. However, the profound capabilities of this technology necessitate a comprehensive ethical and regulatory framework to ensure its safe and equitable application. As research progresses, the potential of nanogenomic engineering continues to expand, promising a future of precision medicine tailored to individual genetic profiles.
Precision and Potentials: Advancing Nanogenomic Engineering in Stem Cell Manipulation: Nanogenomic engineering represents a frontier in stem cell research, combining the precision of nanotechnology with the transformative potential of genomic engineering. Techniques such as CRISPR-Cas9 have revolutionized our capacity to edit the genome with unprecedented accuracy, offering new insights into the genetic underpinnings of stem cell pluripotency and differentiation [51-53]. This precision enables the correction of genetic defects and the introduction of beneficial alterations, significantly advancing the potential for targeted therapies. Nanocarriers play a crucial role in this paradigm, enhancing the targeted (drugs) delivery and monitoring of genomic editing tools [54-56]. Despite the advancements, this field navigates a landscape fraught with ethical and safety challenges. The pursuit of a holistic understanding of stem cell biology through an integrated multi-omics approach promises to transform our capacity for personalized and effective medical treatments, fundamentally altering our understanding of life’s fundamental units [57-60].
Navigating Challenges and Ethical Considerations in Nanogenomic Engineering: The expansion of nanogenomic engineering brings a spectrum of challenges and ethical considerations. Technical challenges include ensuring precision, mitigating off-target effects, and addressing the toxicity of nanocarriers. Ethically, the ability to alter genomes raises critical questions regarding consent, privacy, and the implications of heritable modifications [61]. Establishing robust ethical guidelines and fostering public discourse is essential in navigating these complexities [62,63]. The integration of this field with emerging technologies such as artificial intelligence and big data analytics introduces new possibilities and complexities. Cultivating a culture of responsible innovation is crucial, ensuring that the advancement of nanogenomic engineering is not only scientifically progressive but also ethically sound and socially beneficial [64-66]. This approach will guide the field towards realizing its full potential in a manner that is responsible and advantageous to society.
Single-Cell Genomics: Dissecting the Complex Tapestry of Life
The Power of Single-Cell Resolution: Unveiling the Intricacies of Cellular Functions and States: Single-cell genomics, a trailblazing field in contemporary biology, provides profound insights into the nuanced functions and states of individual cells, previously masked by bulk analyses [67]. By characterizing the genomic, transcriptomic, and epigenomic landscapes at an unprecedented single-cell resolution, this approach reveals cellular heterogeneity and dynamics critical for understanding development, disease, and therapeutic outcomes [68-70]. Technological innovations in high-throughput sequencing and microfluidics have significantly expanded the capabilities of single- cell analyses, enabling large-scale, detailed studies that were previously unimaginable. These advancements have revolutionized our understanding of cellular diversity and the mechanisms underlying various diseases by allowing us to examine the genomic and transcriptomic profiles of individual cells in their native environments. In the fields of regenerative medicine and complex disease research, single-cell genomics has become indispensable for pinpointing disease- associated cells, uncovering novel biomarkers, and refining stem cell-based therapies with unprecedented precision. Despite these advances, the challenges of managing and interpreting massive datasets, coupled with ethical considerations surrounding the use of genetic information, necessitate the development of advanced bioinformatics tools and the establishment of rigorous ethical frameworks to ensure responsible use of this powerful technology [71-73].
Exploring Cellular Heterogeneity and Dynamic Responses in Stem Cell Populations: Single-cell genomics has revolutionized stem cell research by enabling the dissection of cellular heterogeneity and dynamic responses at an unparalleled resolution [68,74]. This technology characterizes diverse cellular states within stem cell niches, shedding light on differentiation pathways and tissue functions [75]. The enhanced understanding of signaling networks and adaptive mechanisms through individual cell tracking informs the optimization of stem cell cultures and therapies [76]. As the field advances, it faces ethical and analytical challenges, including consent and privacy issues and the complexity of data interpretation [70,77-79]. Future prospects involve integrating single-cell genomics with multi-omics approaches, providing a comprehensive understanding of stem cell biology and unlocking new therapeutic avenues in regenerative medicine. Implications for Disease Modeling and Regenerative Medicine: Single-cell genomics holds transformative implications for disease modeling and regenerative medicine, offering insights into cellular mechanisms and tissue regeneration processes [80]. In disease modeling, it identifies diverse cellular signatures, contributing to an in-depth understanding of disease mechanisms and the development of targeted therapies [81]. In regenerative medicine, it elucidates gene expression patterns and signaling pathways, enhancing stem cell therapy development and tissue regeneration strategies [82].
Pathways to Personalized Therapeutics
Bench to Bedside: Translating Molecular Insights into Clinical Realities: The trajectory of personalized therapeutics represents a fundamental shift in medical treatment, pivoting toward a model that is acutely attuned to the individual nuances of patients, propelled by molecular medicine, genomics, and nanotechnology [83]. This paradigm is revolutionizing the translational journey from bench to bedside, as detailed molecular insights guide the development of targeted clinical applications. The ability to discern intricate genetic mutations and biomolecular interactions informs the pinpointing of precise intervention targets. Single-cell genomics, by offering a granular view of cellular heterogeneity, unveils novel therapeutic targets, advancing disease understanding and treatment strategies [84-87]. Patient-specific stem cell insights and nanotechnology-driven drug delivery systems are critical in this revolution, enhancing the precision and reducing the systemic side effects of therapeutic interventions [88- 90]. This molecularly informed approach necessitates a multifaceted translational process, underscored by interdisciplinary collaboration, yet is encumbered by ethical, regulatory, and implementation challenges [91]. The future of personalized medicine is a mosaic of molecular insights, technological advancements, and a nuanced understanding of individual patient profiles, promising a new epoch of tailored, effective, and accessible medical treatment.
Tailoring Regenerative Protocols to Individual Genetic Profiles: The advent of personalized therapeutics in regenerative medicine represents a transformative shift from one-size-fits-all remedies to customized strategies meticulously aligned with individual genetic blueprints [92]. This approach leverages the power of molecular medicine, single-cell genomics, and nanotechnology, aligning regenerative protocols with patients’ unique genetic, cellular, and molecular signatures. Advancements in single-cell genomics provide an unprecedented understanding of genetic diversity, enabling the prediction and customization of therapies for optimized efficacy and minimized adverse effects [93-97]. The integration of patient-derived stem cells and precision nanocarriers stands as a pinnacle in therapy personalization, promising enhanced treatment efficacy and safety. However, the journey from bench to bedside is fraught with challenges, including ensuring the robustness of tailored treatments and addressing ethical and regulatory considerations. The horizon of personalized regenerative medicine is expansive, promising a future where treatments are not only disease-specific but also patient-specific, fundamentally altering the landscape of medical science and healthcare [98-101].
Overcoming Safety, Efficacy, and Regulatory Hurdles in Personalized Therapeutics: The ascent of personalized therapeutics heralds a new era of targeted and effective medical interventions, yet it is beset with significant safety, efficacy, and regulatory challenges. Ensuring safety in personalized treatments requires a deep understanding of individual biological profiles, leveraging molecular medicine and single-cell genomics to navigate the complex biological pathways unique to each patient. The role of nanotechnology in enhancing precision and mitigating toxicity is paramount, yet it demands stringent validation through comprehensive testing and monitoring [102-105]. Assessing the efficacy of personalized interventions necessitates robust methodologies capable of evaluating treatment outcomes across diverse genetic and environmental landscapes. Regulatory frameworks, too, must evolve to accommodate the unique aspects of personalized medicine, fostering international collaboration and standardization. The trajectory of personalized therapeutics is one of promise and complexity, with the integration of advanced technologies and systems biology poised to refine and revolutionize patient care, marking a new paradigm in healthcare and medical science [106-109].
Ethical and Biosafety Paradigms in Cutting-Edge Biomedical Research
Navigating the Ethical Terrain: Balancing Innovation and Moral Imperatives: The ethical landscape in biomedical research, particularly within the realms of stem cells, genomics, and regenerative medicine, requires a balanced approach that aligns rapid innovation with moral imperatives. The ethical framework guiding this field must offer comprehensive guidance to stakeholders, ensuring scientific exploration adheres to the highest ethical standards [110, 111]. Central to ethical discourse are issues such as informed consent, privacy, and moral considerations surrounding human embryos, especially with the potential for genetic enhancement and designer traits [112]. Developing robust biosafety and biosecurity measures is crucial for managing risks associated with genetic manipulation and biohazard containment [113, 114]. Engagement with the public and policymaking processes is essential to foster understanding, trust, and regulations that are ethically sound and resonate with diverse societal values [115]. International cooperation is pivotal in harmonizing ethical standards, biosafety, and biosecurity protocols, ensuring global benefits and respect for cultural diversity [116]. As biomedical research advances, ethical and safety paradigms must also evolve, requiring ongoing adaptation, reflection, and dialogue.
Ensuring Biosafety Rigor: The Cornerstone of Responsible Research: Rigorous biosafety standards are essential in the rapidly advancing domains of stem cell research, genomics, and regenerative medicine [97,117]. The establishment of comprehensive safety protocols addresses the unique risks inherent in biological material handling [118]. Risk assessment and management, together with fostering a culture of safety consciousness among researchers, are fundamental to preemptive and preventive safety strategies [119-121]. Regular monitoring, reporting, and the international standardization of biosafety protocols ensure consistency and reliability in research practices [122]. As the field progresses, biosafety paradigms must remain dynamic and responsive, adapting to new challenges and technologies through continuous research, evaluation, and community commitment [123,124].
Public Engagement and Policy Development: Steering the Future of Stem Cell Research: Proactive public engagement and informed policy development are crucial for guiding the future of stem cell research and therapy [125]. Effective communication strategies are key to demystifying the complexities of this field, building public trust, and shaping ethical and policy frameworks [126]. Policy development must address sourcing, consent, distribution, and longterm implications, such as genetic privacy, while integrating ethical and safety considerations [127-129]. International collaboration is vital for ethical standardization and ensuring global access to therapies [130]. Adaptable public engagement strategies and agile policy frameworks are paramount in responding to scientific advancements and societal shifts [131,132]. A proactive, informed approach ensures that stem cell research progresses with both innovation and moral integrity, realizing its potential in a responsible and beneficial manner [133].
Envisioning the Future: Transformative Trajectories in Stem Cell Research and Regenerative Medicine The Horizon of Stem Cell Research: At the Brink of Revolutionary Breakthroughs: As we stand on the precipice of transformative breakthroughs, stem cell research is poised to redefine the medical and scientific landscapes. This horizon is illuminated by emerging trends and cutting-edge technologies that are converging to propel significant advancements. The refinement of stem cell applications in regenerative medicine is leading to enhanced treatment efficacies for a multitude of conditions [95,134,135]. The development of organoids and advances in single-cell genomics are providing profound insights, heralding a new era of personalized therapeutics [136-138]. However, the evolution of this field necessitates parallel advancements in ethical, social, and regulatory frameworks, ensuring that progress is underpinned by ethical integrity and international cooperation [139,140]. The future beckons with the promise of transformative medical advancements, contingent upon our ability to navigate the complex interplay of innovation, ethics, and societal impact [141,142].
Synergizing Molecular Biology and Genomics for Advanced Diagnostics and Therapeutics: The synergy between molecular biology and genomics is forging a future of advanced, precise, and personalized diagnostic and therapeutic strategies [143,144]. This evolution is characterized by a shift from broad disease categorizations to individualized molecular profiles, enhancing the sensitivity and specificity of diagnostics [145,146]. Therapeutic strategies are undergoing a radical transformation, with the integration of single-cell genomics and nanotechnology playing pivotal roles [85]. These advances are accompanied by ethical considerations and societal implications, necessitating ongoing dialogue and international collaboration to ensure responsible advancements [147,148]. The future of diagnostics and therapeutics promises unprecedented precision and personalization, reshaping healthcare and heralding a new era of medical excellence [149-152].
Conclusion
Envisioning a future where advancements in stem cell biology, nanogenomics, and CRISPR-Cas9 technology drive significant breakthroughs in medical science, it is crucial to address the accompanying ethical, safety, and regulatory challenges. Doing so will fully realize the potential of these technologies in personalized therapeutics and regenerative medicine, thereby transforming healthcare and improving patient outcomes.
Acknowledgements
We are thankful to Irwina Eka Deraya for editing and technical assistance.
Core Tip
There is a lot of research about integrating stem cells and nanotechnology for therapy that uses CRISPR-Cas 9. However, this is a new insight and innovation in nanogenomic engineering applications integrated into stem cells for regenerative medicine. Furthermore, these innovations are feasible to fundamentally alter medical approaches and enhance human health.
Footnotes
Conflict-of-Interest Statement
There is no conflict of interest.
Author Contributions
Dito Anurogo conceived the idea for the manuscript, reviewed the literature and drafted the manuscript.
Intracoronary Streptokinase for Acute Anterior STEMI with a Superimposed Thrombus. 12 Months Follow up.
Introduction
Intracoronary heavy thrombus burden during PCI frequently caused management decision difficulties for the interventionist and was a major factor in the reduced post-PCI myocardial blush, distal embolization, and slow or no-reflow phenomenon, all of which increased the risk of myocardial infarction after PCI. As a result, selecting the best course of action for dealing with this issue during primary PCI in acute STEMI patients has frequently proven difficult [1]. Heavy thrombus burden was graded into five grades: G0, G1, G2, G3, G4, and G5 based on its size and angiographic description. Angiographically, it can appear as a cut-off pattern of occlusion in the IRA, presence of a floating thrombus, accumulated thrombus proximal to the occlusion, persistent dye stasis distal to the occlusion, incomplete occlusion with accumulated thrombus greater than three times the reference lumen diameter (RLD), and RLD of the IRA of ≥ 4.0 mm [2]. High thrombus burden lesions were managed using a variety of techniques during PCI: pharmacological treatments included anticoagulants, glycoprotein IIb IIIa inhibitors, vasodilators, and thrombus aspiration; mechanical treatments included embolic protection devices, rheolytic thrombectomy, and ischemic preconditioning [3].
Aim of the Work
This study aims to evaluate the impact of low dose intracoronary streptokinase (ICSK) on clinical, angiographic, and echocardiographic outcomes during primary PCI in patients presenting with acute anterior wall S-T segment elevation myocardial infarction with a definite thrombus in the left anterior descending artery.
Patients and Methods
The ethical committee at our institute gave its approval to this randomized controlled study. All eligible patients gave their written informed permission. 176 patients who had an acute anterior S-T elevation myocardial infarction (STEMI) within 12 hours after the start of chest discomfort were included in the study. Acute anterior STEMI patients were included in the study if their coronary angiography revealed a left anterior descending artery (LAD) with a thrombus grading > thrombus grade 2 (G2), which is defined by the TIMI thrombus grading score as a definite thrombus with greatest dimensions < ½ the vessel diameter and no history of coronary angioplasty or myocardial infarction. Exclusion criteria included a history of coronary artery bypass grafting (CABG), a history of coronary angioplasty or LAD infarction, patients with a history of recent stroke or gastrointestinal bleeding that precludes the use of streptokinase, patients with coagulopathy, renal impairment, dye allergy, or cardiogenic shock, as well as patients with suspected mechanical complications. All patients received 300 mg of aspirin, 600 mg of clopidogrel, and 100 I.U./ kg of unfractionated heparin after completing the history taking, clinical examination, 12-lead ECG, admission, and peak CK-MB. Following this, they underwent coronary angiography via percutaneous access into the femoral or radial arteries using the Seldinger technique. Only patients with thrombus grading > grade 2 (G2) were included after the coronary angiography. Following primary PCI, patients were randomly assigned to one of two groups: the study group (n = 77) received low dose (250 KU) intracoronary streptokinase (ICSK) during primary intervention (250 000 IU of streptokinase diluted in 15 ml of normal saline, with two thirds (2/3) of the dose infused); the control group (n = 90) underwent conventional primary intervention without receiving intracoronary thrombolytic.
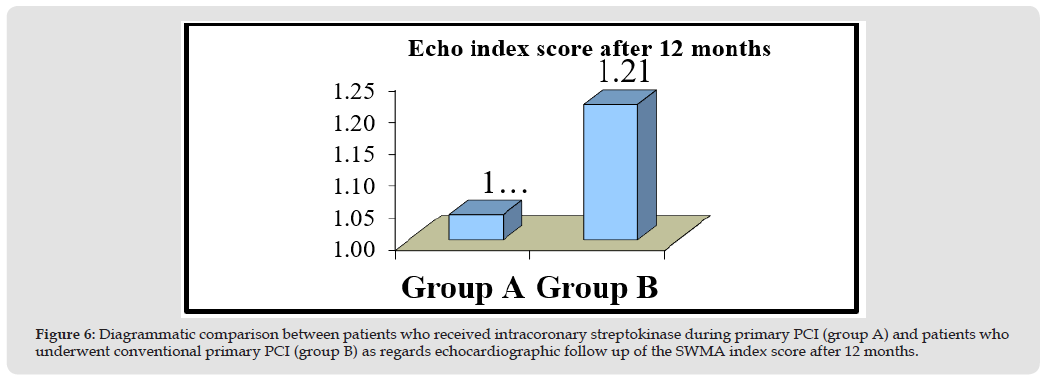
In certain circumstances, the operator may decide to employ additional techniques, such as an aspiration device or glycoprotein IIb/ IIIa inhibitors, to finish the treatment since the patients’ angiographic findings were not adequate. Following primary PCI, the quality of reperfusion and the efficacy of revascularization were evaluated electrocardiographically using the S-T elevation resolution score, angiographically using the TIMI flow grading method, myocardial blush grade (MBG), and corrected TIMI frame count (cTFC). The patients had echocardiography and serial evaluation of serum biomarkers while they were in the hospital. Six and twelve-month follow-up appointments comprised clinical examination and repeat echocardiogram to measure segmental wall motion abnormalities (SWMA), left ventricular ejection fraction (LVEF), and SWMA index score. Transthoracic echocardiography was used to calculate the SWMA index score. Each myocardial segment is given a score between 1 and 4, with 1 denoting normokinetic, 2 hypokinetic, 3 akinetic, or 4 dyskinetic. Then, the total of the previously indicated segmental values is divided by 16 (the number of myocardial segments) to obtain the wall motion score index; hence, a SWMA index score of 1.0 (16/16) is regarded as normokinetic.
Statistics
SPSS (statistical package version sixteen) was used for the collection, verification, revision, and statistical analysis of the data. While continuous variables were displayed as mean values ± standard deviation (SD), categorical variables were portrayed as absolute and relative frequencies (%). The chi-square test and Pearson correlation coefficient were used for categorical variables, while the t-test was used for continuous data when comparing the two groups. A P value of less than 0.05 indicated statistical significance, while a P value less than 0.01 indicated extremely significant differences.
Results
The study population consisted of 167 patients who had undergone primary PCI to LAD after having anterior STEMI. Patients were divided into 2 groups:
Group A (Study Group)
This comprised 77 patients who underwent primary PCI and were administered intracoronary streptokinase (of which two thirds were administered immediately following the achievement of at least TIMI 1 flow, following the guiding wire’s passage and the injection of 200 μg of nitroglycerin to prepare the microvasculature, and the remaining third after the stent was deployed).
Group B (Control Group)
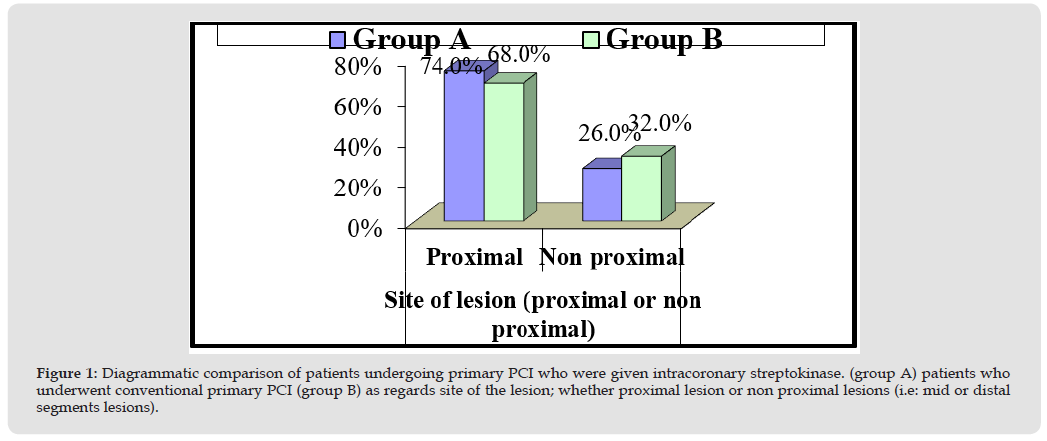
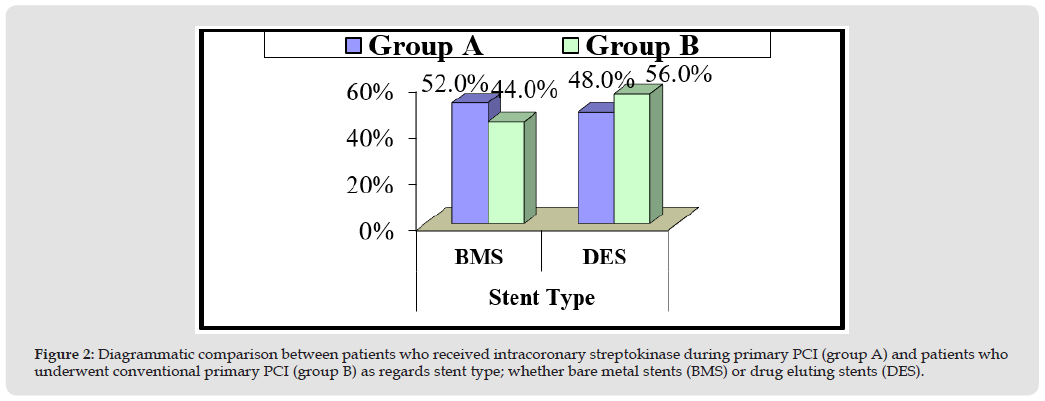
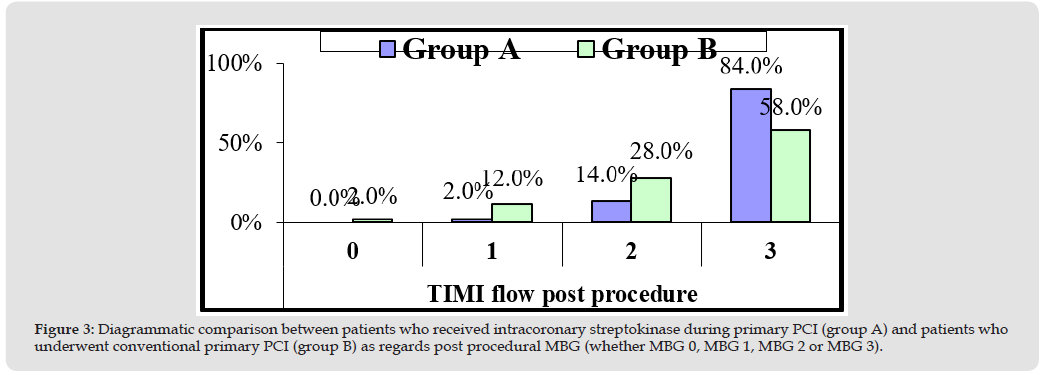
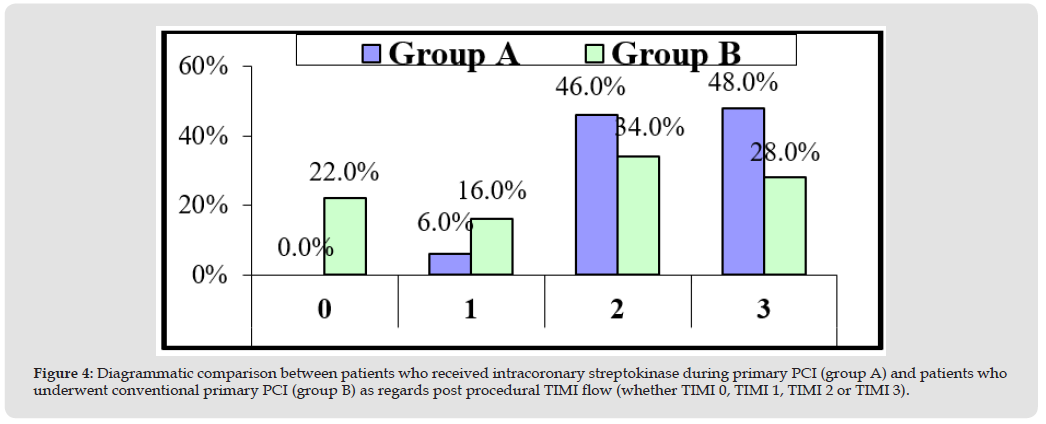
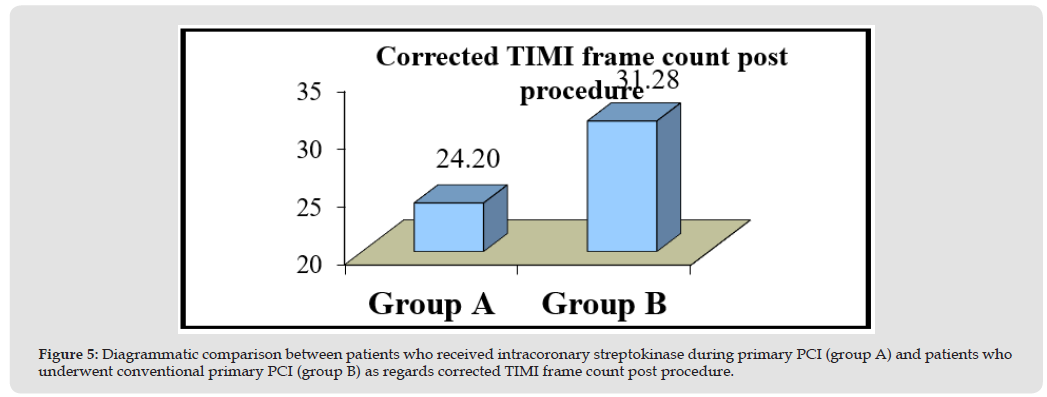
It included 90 patients who underwent conventional primary PCI without receiving intracoronary thrombolytic (Figures 1 & 2). Then, both groups were compared as regards the primary end points (angiographically: post procedural TIMI flow, post procedural MBG and corrected TIMI frame count and electrocardiographically: S-T segment resolution score) as shown in Figure 3, and represented diagrammatically in Figures 3-5. Both post procedural TIMI 3 flow and MBG 3 were statistically significantly higher among patients of group A (P-values = 0.026 and 0.001 respectively), mean corrected TIMI frame count was statistically significantly lower among patients of group A (P-value= 0.000), while S-T segment resolution score > 70% was yet higher among patients of group A, but not statistically significant (P-value=0.22) (Figure 6).
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
Group A showed statistically higher incidence of TIMI flow 3 and MBG 3, together with statistically significant lower mean cTFC. ST segment resolution was yet numerically better in group A, but still not statistically significant. Then, both groups were compared regarding the secondary end points: Major adverse cardiac events at follow-up: Group A showed a case of re-infarction and another with cerebrovascular stroke, while group B showed a case of re-infarction and another case of cardiac death. (P value= 0.572). Bleeding complications as a safety end point: Group A showed two cases of local minimal bleeding and a third case with local small haematoma, while group B had two cases of local small easily controlled haematomas (P value= 0.483).
Discussion
Over the past several decades, the prognosis for patients with acute STEMI has significantly improved because to PCI’s restoration of epicardial coronary blood flow. However, intra-coronary thrombus, which frequently results in microvascular dysfunction due to distal embolization after mechanical reperfusion, may impede the effectiveness of PCI [4]. Selecting the best course of action for acute STEMI patients’ large thrombus load lesions during initial PCI has always been difficult. Thus, to address this issue, pharmacological approaches such as glycoprotein IIb IIIa inhibitors, vasodilators, thrombus aspiration, embolic protection devices, rheolytic thrombectomy, and ischemic preconditioning, or mechanical approaches such as anticoagulants, were employed [5].
In this work, we aimed to do a randomized controlled trial evaluating the advantages and disadvantages of intracoronary (IC) thrombolytic as a main PCI adjunctive therapy in anterior STEMI patients. Our study was conducted on 176 patients who had undergone primary PCI to LAD after presenting with anterior STEMI. Patients were divided into a study group (n=77) who received intracoronary streptokinase during primary PCI and a control group (n=90) who underwent conventional primary PCI. The results of our study indicated that patients in the study group had significantly higher post procedural TIMI 3 flow and MBG 3 (P-values = 0.026 and 0.001, respectively), significantly lower mean corrected TIMI frame count (P-value = 0.000), and significantly higher S-T segment resolution score > 70% (P-value = 0.22), though not statistically significant. These results are consistent with research conducted in Istanbul in 2007 as a pilot study including 41 patients receiving primary PCI by Sezer and his colleagues. Patients were randomized to receive either no further treatment or intracoronary streptokinase at a dosage comparable to that of our research (250 kU). All microvascular function measurements, including corrected TIMI frame count, were considerably lower in the streptokinase group two days after PCI, which was consistent with our study’s findings [6].
Additionally, these results are consistent with the 2015 study conducted by Bainey and associates. They compared the advantages and disadvantages of IC thrombolytic as an adjuvant medication during primary PCI in STEMI patients in a meta-analysis. There were 131 patients from three randomized trials (71 IC thrombolytic and 60 IC placebo). Comparing IC thrombolytic to placebo, TIMI flow 2 and flow 3 were more frequently seen (P-value=0.004), which was consistent with our study’s findings (P-value= 0.026) [7]. A 12-month echocardiographic follow-up in our investigation showed that the study group’s SWMA index score was considerably lower than the control group’s (1.21±0.30 vs. 1.04±0.08, P value= 0.000). This result was at odds with Sezer’s initial pilot study, which found no evidence of a difference in left ventricular (LV) size or function between the two study groups. This implied that IC administration of SK did not improve left ventricular size or function over the long term. Since Sezer’s study was a pilot, its small study sample (n=41) may have contributed to this discrepancy and rendered its findings less definitive [6].
On the other hand, the final results of Sezer’s 2009 main study demonstrated significantly smaller LV volumes and higher echocardiographic LV ejection fraction in the ICSK group over the long term (57.2% vs. 51.8%, p = 0.018), which was similar to the findings of this study (as opposed to the first pilot study). Apart from the results of the echocardiographic follow-up, Sezer’s study also demonstrated that the ICSK group’s infarct size was substantially less than that of the control group, as indicated by the SPECT imaging results (22.7% vs. 32.9%, p=0.003) [8]. In terms of secondary study objectives, there was no significant difference between the two groups for major adverse cardiac events (MACE); re-infarction and cerebrovascular stroke were reported in the study group, while cardiac death and re-infarction were reported in the control group (P value = 0.572). However, Sezer’s trial produced nearly identical findings: two patients in the control group and one in the ICSK group required surgical revascularization, and one patient in the ICSK group experienced a reinfarction after a month. During the follow-up period, there were three cardiac fatalities in the control group and two in the ICSK group. Furthermore, Bainey’s study found no difference in mortality between study group and control group [9,10].
Conclusion
Administration of low dose ICSK during primary PCI in acute anterior STEMI patients with definite coronary thrombi improved coronary perfusion and caused improvement of LV function during follow-up.
Cancer cells are characterized by changing in cellular metabolism as compared to normal cells. Reprogramming of glucose metabolism is one of the characteristic features of the metabolic disorder in cancer cells. Accelerated glucose metabolism is required to supply enough high-energy intermediates necessary to support biosynthetic processes in rapidly proliferating cancer cells [1,2]. High glucose consumption causes an increasing level of lactate excretion in cancer cells even in the presence of oxygen (Figure 1). This phenomenon is known as the “Warburg effect” or “aerobic glycolysis” [3]. Aerobic glycolysis is a less energy-efficient metabolism than oxidative phosphorylation. A higher rate of glycolysis in cancer cells in comparison to their healthy cells has been observed in many types of cancer, including colon, breast, lung, pancreatic, head and neck, prostate cancer, melanoma, and glioblastoma [1-4]. This abnormal glucose metabolism may be explained by the increased demand for precursors for the synthesis of cell components like fatty acids, amino acids, and nucleic acids in rapidly growing cell tumours [5]. Glycolysis of glucose to pyruvate involves several enzymes. Inhibition of these enzymes can retain the generation of energy in cancer cells. A key role plays hexokinase (HK), an enzyme participating in the first limiting stage of glycolysis, the phosphorylation of glucose to glucose-6-phosphate (G6P) (Scheme 1). Glucose-6-phosphate opens the anabolic activity in cancer cells [6]. Hexokinase, due to its key role in glycolysis is considered, among others, as an important target for anticancer therapy.
Figure 1
Scheme 1
Isozymes of Mammalian Hexokinase
There are four mammalian hexokinase isozymes with different subcellular locations, physiological functions, and glucose affinity [7- 9]. These are hexokinase 1 (HK1), hexokinase 2 (HK2), hexokinase 3 (HK3), and hexokinase 4 (glucokinase, HK4). HK1 interacts with the outer membrane of mitochondria [10,11]. HK2 is usually placed on the outer membrane of mitochondria but is also located in the cytosol [10,12]. Both HK1 and HK2 bind to the outer mitochondrial membrane through a N-terminal hydrophobic region [11-13]. These two isoforms are structurally like each other. HK1 and HK2 are in 73% identical and 87% similar [9]. HK3 is present in the perinuclear compartment [8,14], however, HK4 operates in the cytosol [13,14]. HK1, HK2, and HK3 have two similar homologous with molecular masses of 50 kDa with high affinity for glucose (Table 1) [10,15]. The reaction product-G6P inhibits by negative feedback three isoforms namely HK1, HK2, and HK3 [10,15]. An elevated level of inorganic phosphate (PO43-) also inhibits HK1, HK2 and HK3. In the case of HK1 was observed that a low level of PO43- stimulating this isoform [16]. HK4, called glucokinase, has 50 kDa domains and has a lower affinity for glucose (Table 1) [10]. Isoforms are different by the number of catalytic domains, HK1 and HK3 have a single active catalytic domain, while HK2 and HK4 have two active sites [15,17]. All hexokinase isoenzymes have other mechanisms of regulation that lead to different distribution in tissues and cell types [8-18] (Table 1).
Table 1: Reported parameters of mammalian hexokinase isozymes [8-18].
HK2 as a Target in Anticancer Therapy
Among the four isoforms of hexokinase, HK2 is rarely expressed in normal tissues, except for some insulin-sensitive tissues. In contrast, this hexokinase isoform is overexpressed in tumour cells [12,14,19]. HK2 is required for the initiation and maintenance glycolysis process (Patra, et al. [20]) showed that HK2 deletion in the mouse models of KRas-driven lung cancer and ErbB2-driven breast cancer is therapeutic for cancer. Furthermore, elevated levels of HK2 are significantly associated with some tumour aggressiveness, promoting the development of metastasis in some rapidly growing tumours or resistance in therapy [4,12,14,15,19,21,22]. HK2 is a marker for poor prognosis tumours such as breast, lung, prostate, glioblastoma, hepatocellular, gastric, and liver cancer [4,15,19,21,22]. In solid tumours, there are hypoxia zones where oxygen levels are much lower than in normal tissues. Reprogramming the cancer metabolism allows maintenance of the redox homeostasis associated with hypoxia-induced factors such as HIF-1α. HIF-1α promotes the transcription of several genes, including the HK2 gene encoding. HIF-1α and HK2 overexpression are associated with a lethal cancer phenotype characterized by invasion and metastasis, and resistance to chemotherapy and radiation therapy [23,24]. Sparse reports suggest a connection of HK1 with cancer cell growth [25,26].
HK2–VDAC Complex
Mitochondria are intracellular multifunctional organelles present in eukaryotic cells. They engage in energy production, cell metabolism, and programmed cell death. The key role of mitochondria is the production of adenosine-5′-triphosphate (ATP), a key source of energy and phosphate groups in a cell. The mitochondria in cancer cells differ from normal mitochondria; they prefer changes in bioenergetics and biosynthesis shifting metabolic processes from oxidative phosphorylation to anaerobic glycolysis. It is assumed that the Permeability Transition Pore (PTP) complex in mitochondria regulates the release of pro-apoptotic factors. Furthermore, regulation of the PTP opening protects against the loss of membrane potential, leading to the disintegration of the outer mitochondrial membrane. The regulation of PTP components is different in cancer cells. Studies have shown that the PTP complex is associated with components such as HK2 and Voltage-Dependent Anion (VDAC), a transporter of mitochondrial metabolites, which are specific for cancer (Figure 2) [27].
Figure 2
Mitochondria-associated HK2 plays a crucial role in the aerobic glycolysis of tumour cells [15]. HK2 binds to the voltage-dependent anion channel 1 (VDAC1) located on the outer mitochondrial membrane [15,25,28,29]. VDAC1 allows the diffusion of ATP between mitochondria and cytosol; in this way, cell HK2 has direct access to intramitochondrial ATP used for glucose phosphorylation. The binding of HK2 to VDAC1 allows the defection of G6P, the phosphorylation product, resulting in protection from inhibition by negative feedback [28]. The interaction of HK2 with the outer membrane of the mitochondria forces cancer cells to have a high rate of glycolysis [14,28]. Mitochondria- associated HK2 cooperation with VDAC1 also interferes with the cell’s apoptotic pathways by preventing the delivery of apoptotic factors to the mitochondria and the release of apoptotic regulators by mitochondria to the cytoplasm (such as cytochrome c), protecting the tumour cell from apoptosis [15,25]. VDAC1 is often overexpressed in many types of cancer [9,25].
Factors Regulating HK2
The intracellular environment has a strong influence on HK2 activity and its association with the outer mitochondrial membrane. The increase a glucose uptake interferes with the induction of glucose transporter (GLUT) expression hence increasing hexokinase activity. Another factor, such as protein kinase B (Akt), plays a key role in the localization and regulation of HK2 activity. Activation of this factor induces the activity of the hypoxia-inducible transcription factor HIF-1α that promotes the expression of GLUT and HK2 [30]. Other factors regulating HK2 expression are c-MYC, protein p53 mutations, and insulin [15]. Protein kinase B, known as Akt, affects different signaling pathways and engages in glucose metabolism in cancer cells. The Akt protects cells from apoptosis by maintaining normal mitochondrial function and the correct state of PTP opening, which maintains hexokinase association with the outer mitochondrial membrane (Gottlob, et al. [31,32]). demonstrated that activated Akt increases mitochondria-associated hexokinase activity by approximately 50%. It has been confirmed that Akt causes HK2 disconnection from mitochondria and sometimes translocation of HK2 from the mitochondrion to the nucleus [30]. Magalhães, et al. [10] investigated changes in HK2 intracellular localization from mitochondria to cytosol under different concentrations of G6P, glucose, and Akt. Another study confirmed that the translocation of HK2 is dependent on its enzymatic activity [33].
Classes of Agents Affecting HK2 in Cancer Treatment
Competitive and/or Non-Competitive HK2 Inhibitors
Several potential HK2 inhibitors that directly affect HK2 activity (Figure 3) have been described in the literature [9,29]. They have shown insufficient effectiveness and limited selectivity in their practical application in cancer treatment. The search for new potential anticancer drugs requires further and more thorough and further research in the HK2 inhibitors field. Herein, the most promising HK2 inhibitors that mimic G6P binding or bind to the glucose binding site are described (Figure 3).
Figure 3
Metformin (Met): Metformin (Met) is a biguanide derivative used in therapy for type 2 diabetes. Met, like a drug approved by the FDA, is characterized by its safety profile. Common side effects of Met include gastrointestinal complaints and, very rarely, lactic acidosis. Moreover, long-term metformin treatment leads to vitamin B12 deficiency [34]. According to the meta-analysis, patients treated with Met showed a reduced risk of cancer incidence and mortality [35]. To date, several mechanisms of Met action have been demonstrated. One is that Met occupies the binding site of the phosphorylation product, G6P, changing the conformation of HK2 and directly reducing HK2 activity. Additionally, it also indirectly dissociates the enzyme from the mitochondria, leading to the activation of apoptotic cell death [36]. The study of (Salani, et al. [37]) demonstrated that Met inhibits (at a mM concentration of 0.0375 mM to 10 mM) both purified HK1 and HK2 as well as cell lysates in a dose-dependent fashion but does not have any effect on HK4. Preclinical studies have revealed that Met has the efficacy of standard chemotherapy in a variety of cancer cells and accelerates tumour regression and prolonged remission as an effect of combined treatment with Met and individual chemotherapeutic agents [38].
Lonidamine (LD): Lonidamine (LD) 1-(2,4-dichlorobenzyl)- 1-H-indazol-3-carboxylic acid is a known antispermatogenic agent with anticancer properties. (Florldl, et al. [39,40]) reported LD as an HK2 inhibitor. LD directly inhibits HK2 activity and interferes with HK2 binding of HK2 to VDAC. Tests performed on Ehrlich ascites tumour cells indicated that 20 μM LD reduced more than 50% amount of G6P formed by mitochondria, which is related to the effect on mitochondrial HK2. The antitumour activity of LD was assessed in Cholangiocarcinoma cell lines with characteristic overexpression of HK2. LD significantly suppressed the growth of Cholangiocarcinoma cell lines with an average IC50 value of 137 μM [41]. LD exhibits selective intracellular activity against tumour cells, resulting in low toxicity to normal cells, provided the doses do not exceed 400 mg/m2 (intravenous and oral) [42]. Due to its promising anticancer effects, clinical studies were performed using LD. A phase II clinical trial with LD was conducted in the treatment of malignant glioma that overexpresses HK2.
The data obtained confirmed limited therapeutic activity, 2 responses, and 3 stable diseases obtained in the 10 evaluable patients [43]. Clinical research on LD has demonstrated that combination of LD with chemotherapy and radiation is safe and potentially effective [44]. LD treatment does not cause the typical side effects of traditional anticancer drugs such as germ cell mutation, alopecia, and gastrointestinal mucosal necrosis. Phase II clinical trials demonstrated that the most common side effects of oral LD were myalgia, testicular pain, and lethargy [45]. The LD is used in few European countries for the treatment of cancer as a glycolysis inhibitor but has not yet been approved by the FDA [46]. Although LD tends to extend median survival in cancer patients with low toxicity, more clinical trials are necessary to determine the toxicity and benefits of this drug.
Recent research has shown that the mechanism of LD’s anticancer action is not just through HK2 inhibition. LD has multiple targets activity, such as Permeability Transition (PT) pore complex, Monocarboxylate Transporter (MCT), Mitochondrial Pyruvate Carrier (MPC), and anion channel VDAC [47]. The modification of lonidamine obtained by combining lonidamine with 7-hydroxy-4-methylcoumarin led to the discovery of a new promising anticancer agent (Figure 4). Measurements of the cytotoxic effect of LD and hybrid lonidamine- coumarin in the MCF-7 and A549 cell lines gave IC50 values for LD and hybrid lonidamine-coumarin as 239.4 μM, 33.12 μM for MCF-7 and 444 μM and 222.8 μM for A549, respectively. Based on molecular docking studies, a good binding affinity to HK2 was identified for hybrid lonidamine-coumarin, so this may confirm HK2 as a molecular target for this agent [48].
Figure 4
2-Deoxy-D-Glucose (2-DG): As early as the 1950s, 2-DG was proven to inhibit anaerobic glycolysis [49]. 2-DG is a glucose analog in which the hydroxyl group at position 2 is replaced by hydrogen. 2 DG is a glucose mimetic, so it has a high affinity for hexokinase (Km=27 μM) and competes with glucose for the active site of HK [49]. The mechanism of the 2-DG antitumour action involves inhibition of anaerobic glycolysis (Figure 5). It is known that cells relying on glycolysis are more susceptible to 2-DG. Overexpression of glucose transporters and glycolytic enzymes in cancer cells increases 2-DG uptake in cancer cells compared to normal cells. 2-DG is non-toxic to humans and animals. The safety of 2-DG as a single agent for a dose of 63 mg/kg/day has been confirmed in clinical studies [50]. However, the administration of 2-DG for a long time in high doses could be toxic, as it reduces glucose consumption in normal tissues, especially the brain. The most common reported side effect is reversible hyperglycemia [50]. Due to its efficient cytotoxicity in a wide variety of tumour cells, 2-DG has the potential for use in anticancer therapy and combination therapy with standard chemotherapeutics as confirmed by clinical studies [5]. However, the poor pharmacokinetic and pharmacodynamic profile of 2-DG is a major reason for the lack of 2-DG therapeutic activity. To improve 2-DG activity, its derivatives were synthesized. 3,6-Di-O-acetyl-2-deoxy-D-glucose possesses improved pharmacokinetic and pharmacodynamic properties, allowing two orders of higher maximum concentration of 2-DG in plasma cells compared to an equal molar dose of pure 2 DG [51]. The 2-DG derivative, namely, 2-[18F]-fluoro-2-deoxy-D-glucose has been used in positron emission tomography (PET) as a diagnostic agent in cancer. Interestingly, during the pandemic in recent years, 2-DG was approved in India for the treatment of patients with COVID-19 in severe cases [52].
Figure 5
Other Glucose Analogs: (Machado de Domenech, et al. [53]) conducted studies on the effect of glucose analogs on hexokinase. In this research, they used isozymes 1 and 2 of yeast hexokinase and brain hexokinase and studied the affinity for the enzyme and the rate of the phosphorylation reaction. Mannosamine and 5-thioglucose (5-TG) were shown to be the most promising competitive inhibitors [53]. 5-TG is a D-glucose derivative in which the sulfur atom replaced the oxygen in the ring and was first synthesized in 1962 [54]. 5-TG was found to inhibit glucose phosphorylation and is slowly phosphorylated. The reaction of 5 TG phosphorylation by hexokinase is not as effective with Vmax 0.3% in comparison to glucose [53]. Another research group confirmed that 5-TG as a competitive inhibitor has a moderate affinity for brain hexokinase with a similar Ki of 0.17 mM [55]. They also showed that this compound is an ATP inhibitor at the active site of the HK with estimated Ki values of 0.31 and 0.48 mM. In addition, 5-thioglucose phosphorylation gives 5-thioglucose 6 phosphate.
It was evaluated as glucose-6-phosphate analogs to inhibit soluble (HK1) and mitochondria-bound hexokinase (HK2). 5-Thioglucose- 6-phosphate at a concentration of 2.5 μM inhibited mitochondria- bound soluble hexokinase HK1 and HK2 mitochondria-bound hexokinase by 60% and 20%, respectively [55]. Mannoheptulose (MH), a 7-carbon monosaccharide, is a nonselective, competitive, and non-competitive inhibitor of various isoforms of hexokinase such as HK1, HK2, and HK4 [56,57]. However, on the other hand, the safety profile for animal treatment with MH is satisfactory. In studies of Energy Expenditure (EE) in healthy adult dogs, MH was used as an avocado extract. All dogs showed good general health without side effects [58].
(Al-Ziaydi, et al. [59]) conducted an in vitro study on the proliferation of the effect of MH on breast cancer cells (AMJ13 and MCF7) due to inhibition of the biochemical pathway. They determined IC50 for AMJ13 and MCF7 using the MTT cytotoxicity assay with values of 124,7 μg/mL and 122,6 μg/mL, respectively. These results were compared with a study on normal Embryonic Fibroblasts (REF), which confirmed the low toxicity of MH in normal cells (IC50 = 486,9 μg/mL). An MH concentration of 62.5 μg/mL slightly inhibited hexokinase activity in a normal cell, while it significantly inhibited hexokinase activity in breast cancer cells. Furthermore, MH induced a reduction in ATP concentration, pyruvate, and acidity levels in cancer cells, which is associated with hexokinase inhibition [59]. According to a study by (Malaisse, et al. [60]), D mannoheptulose hexaacetate increased biological efficiency by effectively crossing the cell membrane with subsequent intracellular hydrolysis. The ester itself did not affect D-glucose phosphorylation but allowed inhibition of glycolysis by the unesterified sugar [60]. This fact may be useful for designing new glucose hexokinase inhibitors and improving their pharmacokinetic properties.
Glucosamine Derivatives: Derivatives of glucose in which the hydroxyl group in position 2 has been replaced by an amino group, glucosamine derivatives, have been reported as anticancer agents with potential HK2 inhibitory activities (Figure 6) [61]. According to a High-Throughput Study (HTS hits), glucosamine derivatives were identified as potential selective hexokinase 2 inhibitors (HK2 IC50 = 6,3 μM; HK1 IC50 = 2,0 μM) (1) [62]. Based on SAR studies, optimization of their structure leads to the discovery of new and more selective HK2 inhibitors (Figure 7). The most promising glucosamine derivative 4’-chloro-N-((2S,3R,4R,5S,6S)6((2,3,dichlorophenylsulfonyl) methyl)2,4,5-trihydroxytetrahydro-2H-pyran-3-yl)biphenyl-3-sulfonamide (2) showed more than 100-fold higher selectivity against HK2 compared to HK1 with an average value of IC50 = 0,0079 μM and 1,0 μM, for HK2 and HK1, respectively. The inhibitory activity of glucosamine derivatives was evaluated in the UM-UC-3 cancer cells line, which had over-expressed HK2 and minimal HK1 expression [62]. Crystallographic studies confirmed the flexibility of the HK2 binding site to adopt an “induced-fit” conformation with inhibitors. (Lin, et al. [62]) demonstrated a dual mechanism of inhibition of this novel inhibitor, which binds to both the G6P binding pocket and the glucose- binding pocket.
Figure 6
Figure 7
Benserazide (BENZ): BENZ is a well-known drug for the treatment of Parkinson’s disease. BENZ is a decarboxylase inhibitor approved by the FDA but has been recently identified as a hexokinase 2 inhibitor. In silico studies have shown that BENZ occupies the active binding pocket in HK2, and the pyrogallol part of the BENZ structure interacts with the substrate (glucose) binding site. BENZ shows reasonable selectivity because it prefers one isoform of this enzyme, such as HK2 [63]. The inhibition measurement data demonstrated that the IC50 values for the HK2, HK1, and HK4 isoenzymes are 5.52 ± 0.17 μM, 25.13 ± 0.24 μM and 40.53 ± 2.94 μM, respectively. Their MST binding assay demonstrated that BENZ shows a high affinity for HK2 with a value of equilibrium dissociation constant (Kd) of 149 ± 4.95 μM. A comparison of the MTS results for BENZ with three reported HK2 inhibitors (3-BrPA, 2-DG, Met) indicated that BENZ was a compound with the highest affinity for glucose (Table 2). (Li, et al. [63]) postulate competitive and non-competitive inhibition of BENZ to HK2 by binding BENZ to the active site of the enzyme by changing the HK2 conformation. The kinetic enzyme assay showed that the Km value of glucose increased in a dose-dependent manner, whereas the Vmax value of glucose decreased after BENZ treatment. According to the data from Li, BENZ has shown cytotoxicity to various tumour cells such as SW480, Lovo, HCT116, MCF-7, and SMMC-7721, showing cytotoxic effects only in cancer cells, particularly SW480 (IC50 = 143 ± 7.0 μM). Furthermore, an in vivo test using a mouse xenograft model showed strong cell growth inhibitory activity under BENZ treatment. Experiments have confirmed that HK2 was a target of BENZ and this drug affected glucose metabolism [63]. But recent studies [64] have shown that BENZ reduced tumour growth and progression through a different mechanism than targeting HK2. In these studies, BENZ is DNA repair activating agent and it may prevent or retain the progression of breast tumours and their metastases.
Table 2: Kd parameter values obtained from the MST assay.
Benitrobenrazide BNBZ: Recently, a new compound benitrobenrazide ((E)-4-Nitro-N′-(2,3,4-trihydroxybenzylidene, BNBZ) has been reported as a promising HK2 inhibitor. BNBZ was identified by structure-based virtual ligand screening as a strong HK inhibitor. In vitro and in vivo studies confirmed the inhibitory effect on HK2 and promising antitumour activity. BNBZ displayed inhibition of HK2, HK1, and HK4 activity with IC50 values of 0.53 ± 0.13 μM, 2.20 ± 0.12 μM, 4.17 ± 0.16 μM, respectively. The enzyme kinetic measurements indicated competitive inhibition of the glucose substrate by BNBZ with high affinity for the substrate with a Km value of 4.99 ± 0.41μM [65,66]. In its structure, BNBZ has an aromatic hydrophobic substituent and a highly polar fragment, which allows greater affinity for the active site and more effective pharmacokinetic properties (Figure 8). The prediction of molecular coupling demonstrated that BNBZ exhibits competitive inhibition occupying the same binding pocket as glucose [65]. According to the structure-activity research, the trihydroxybenzene fragment in BNBZ is required for its HK2 inhibitory activity [67]. The affinity of BNBZ dihydroxybenzylidene derivatives with other locations of hydroxyl groups toward the inhibitory effect on HK2 was investigated in vitro using HepG2 and HUH7 cell lines as a biological model.
Figure 8
A comparison of the results with those of the parent BNBZ indicates that only BNBZ exhibited satisfactory inhibitory activity in vitro and within the cell. None of the BNBZ derivatives showed inhibition of the enzyme in vitro, but some showed HK2 inhibitory activity in cell lines. The reason for this may be the tendency of derivatives to form aggregates. MST studies demonstrated that only one of the BNBZ derivatives (2,4-dihydroxy derivative) showed moderate affinity for HK2 (Km=58.9 μM), while other BNBZ derivatives did not show binding affinity to HK2 [67]. According to cell viability tests of four pancreatic cancer cell lines expressing HK2, BNBZ has the strongest effect on cancer cells with high overexpression of HK, such as SW1990 and MIApaca-2 cells with an IC50 value of approximately 25 μM. Moreover, BNBZ has shown no obvious toxicity to normal cells LO2, L929, and Vero with an IC50 value above 400 μM [66]. Studies by (Zheng, et al. [66]) have shown that the anticancer effects of BNBZ involve inhibition of HK2 activity as a factor that causes a decrease in glucose uptake and lactate production and an increase in the production of Reactive Oxygen Species (ROS), resulting in inhibition of cancer cell proliferation and inducing apoptosis.
Steroid from Ganoderma: Ganoderma sinense are important wood-decaying fungi occurring throughout the world. Their strains are a source of steroids which are a natural inhibitor of hexokinase. Ganoderma species are characterized by a wide biological activity and have been used for thousands of years in folk Chinese medicine [68]. One of the main active components from Ganoderma was sterols selected as inhibitors of HK2. According to the structure-based virtual ligand screening, the highest binding affinity to HK2 was shown by one of the thirteen sterols from Ganoderma such as (22E,24R)-6-β- methoxyergosta7,9(11),22-triene-3β,5α-diol. The MST assay showed the equilibrium dissociation constant Kd equal to 114.5 ± 2.7 μM, which means a strong binding affinity. This steroid exhibited strong enzyme inhibitory effects against HK2 with IC50 values of 2.06 ± 0.15 μM, with non-competitive inhibition [68]. On the other hand, no inhibitory effect on other isoforms of HK was shown in these studies [68], which hinders conclusions on the selectivity of the compound. According to the cytotoxicity test, this steroid exhibited 4-fold selectivity against cancer cells SW1990 (IC50 = 5.05 ± 0.17 μM) versus normal cells Vero (IC50 = 22.59 ± 1.24 μM) and strongly inhibited cancer cell growth compared to known inhibitors: Benserazide and Metformin [63].
Germicidins: Other natural compounds such as new α-pyrone derivatives and their known analogues, named germicidins were screened for HK2 inhibition activity in vitro. These compounds were discovered from Streptomyces sp. 18A01 isolated from a sponge specimen collected from the sea area in Yongxing island of the South China Sea. One of these germicides exhibited significant inhibitory effects against HK2 with an IC50 value of 5.13 ± 0.53 μM. It was approximately the same result compared to the IC50 value of the known benserazide inhibitor used in the positive control (IC50 = 5.52 μM) [69]. Benzimidazoles: Benzimidazoles exhibit a wide spectrum of biological activities, including antihypertensive, anti-inflammatory, anti-ulcer, anthelmintic, antimalarial, antibacterial, antioxidant, and anticancer [70]. Benzimidazoles such as Fenbendazole, Albendazole, and Mebendazole are popular drugs used in the treatment of parasites in both human and veterinary medicine [70-72]. All three compounds have shown potent selective inhibitory effects on the growth of various cancer cells through modulation of multiple cellular pathways and depolymerizing microtubules. [71-75]. Benzimidazoles have been observed to reduce the expression of enzymes involved in glycolysis, including HK2 [71-75]. Molecular Docking Analysis demonstrates that Fenbendazole (FZ), Albendazole, and Mebendazole have binding interactions with HK2. In vitro analysis results showed inhibition of hexokinase activity by Fenbendazole, Albendazole, and Mebendazole with IC50 values of 0.25 ± 0.1 μM, 2.5 ± 0.8 μM and 10.0 ± 1.2 μM, respectively. The most promising benzimidazole as a potential HK2 inhibitor is an FZ, drug used against parasites in the digestive tract in animals [73]. Albendazole and mebendazole are drugs used for the treatment of parasitic diseases in humans. Many benzimidazole derivatives were evaluated in clinical trials for different anticancer cures.
Ongoing clinical trials do not have enough data to assess whether benzimidazole antibiotics can be used to treat cancer in humans [74]. Fenbendazole was applied in the in vitro and in vivo treatment of human Non-Small Cell Lung Carcinoma (NSCLC) [75]. FZ causes reduced glucose uptake in H460 and A549 cell lines after treatment with a drug concentration of 1 μM. The same concentration of FZ results in a significant reduction of HK2 expression. In silico studies suggested that FZ can bind to the glucose pocket in HK2 and thus mimic a substrate or a product of HK2. Inhibition of the activity of the HK2 assay in H460 cells and lysates of H460 and A549 cell lysates at a dose of 1 μM confirms the inhibitory activity of FZ. Fenbendazole inhibits purified HK2 in a dose-dependent manner (5-10 μM) [75]. This is in contradiction to the (Jang, et al. [76]), report in which FZ and other benzimidazole, such as oxibendazole, have been shown to have no effect on HK2 activity (in vitro) at a concentration of 1 and 10 μM. Poor pharmacokinetic parameters of benzimidazoles [76] and lack of a fully understood mechanism of action prompt further research on the potential of benzimidazoles as anticancer drugs.
Compounds that Disrupt the VDAC1-HK2 Complex
(Figure 9) The interaction of HK2 with VDAC1 is important for the regulation of glucose metabolism and the apoptosis process in cancer cells. Disrupting the HK2–VDAC1 binding complex by small molecules could inhibit the growth and survival of cancer cells. In this review, compounds with HK2-VDAC1 activity are reported to inhibit the activity in cell lines by dissociating HK2 from VDAC1 (Figure 10). Inhibitors such as LD and Met have been shown to directly affect HK, as well as disrupt the HK2-VDAC1 complex. When designing new drugs based on HK2-VDAC1 interference, attention should be paid to their cardiotoxic effects; it was reported that disruption of HK2 from mitochondria causes detrimental effects on myocardial function [77].
Figure 9
Figure 10
Bromopyruvate (3-BrPa): Investigation of the influence of key glycolytic enzymes on hepatocellular carcinomas led to the discovery of 3-BrPa as an inhibitor of the glycolysis pathway [78]. This compound has shown promising anticancer activity both in vivo and in vitro [78-83]. Studies show that 3-BrPa induces covalent modification of the enzyme dissociates HK2 from VDAC and releases the apoptosis- inducing factor. Incubation of HL-60 cells with 100.0 μM of 3-BrPa results in a significant dissociation of HK2 from mitochondria [80]. In cells treated with 3-BrPa, a decrease in HK2 expression is also a decrease in HIF-1α expression [81]. 3-BrPa is known as an alkylating agent and it can react with the cysteine residue in the protein chain, thus inhibiting hexokinase enzymatic activity [80]. Moreover, 3-BrPA has shown dose-dependent toxicity to the liver and duodenum [82]. (Hwan Jun Jae, et al. [83]) conducted studies on the evaluation of the anticancer effect and hepatotoxicity in a rabbit VX2 hepatoma model administrating 3 BrPA intravenously in small-doses 3-BrPA (25 mL at a 1 mM concentration, n = 10) and high-dose (25 mL in at 5 mM concentration, n = 10) and doxorubicin as a positive control (1.6 mg doxorubicin/0.4 mL lipiodol, n = 10). The tumour necrosis rate values were 93% ± 7.6 (high dose 3-BrPa), 62% ± 20.0 (low dose 3-BrPa), and 99% ± 2.7 (lipiodol-doxorubicin), respectively. The hepatotoxicity observed in the 3-BrPA group was comparable to that in the lipiodol- doxorubicin group. These results indicated limited efficacy of 3-BrPa application compared to conventional methods.
Methyl Jasmonate (MJ): Methyl Jasmonate (MJ), the plant stress hormone, is a natural cyclopentanone lipid. MJ exhibited anticancer activity through multiple mechanisms [84]. The main targets of MJ treatment in cancer cells are HK2-VDAC complex, Reactive Oxygen Species (ROS), 5 lipoxygenase (5-LOX) pathway, MAPK signaling pathway and NF-κB pathway. The anticancer effects of MJ have been assessed in many types of various human and mouse cancer cell lines such as melanoma, lymphoma cells, prostate, melanoma, lymphoblastic leukemia, and breast [85]. All cytotoxic effects of MJ on cells were observed at millimolar concentrations [84]. It is worth noticing that MJ induces ATP depletion in cancer cells but not in normal cells [86]. A number of MJ toxicity studies have shown that the compound is non-toxic to normal cells. The U.S. Federal Environmental Protection Agency has confirmed that MJ is non-toxic to humans and is a substance commonly consumed in fruits and is safe for humans. In addition, MJ as a food additive has been approved by the Food and Agriculture Organisation/World Health Organisation (FAO/WHO) [84]. According to (Goldin, et al. [27]), the proposed mechanism of MJ inhibitory effect on the hexokinase activity involves MJ binding to HK, which interferes with the HK-VDAC complex, hence enabling dissociation of HK from VDAC. Hexokinase released from the HK-VDAC complex is inhibited by G6P and has a lower affinity for ATP. MJ influences two other hexokinase isoforms: mitochondria-associated hexokinases HK1 and HK2. Destruction of the HK2-VDAC1 complex by MJ resulted in loss of mitochondrial function, among others, by inducing the transition of mitochondrial permeability and subsequent release of cytochrome c from mitochondria, leading to cell necrosis and apoptosis [86,87]. The discovery of MJ as a candidate for cancer treatment has resulted in the design and synthesis of derivatives of MJ [85]. In vitro studies of therapeutic effects of new MJ derivatives on glioblastoma brain tumours that are aggressive and malignant and highly lethal are due to overexpression of HK2. One of the novel analogs of MJ (Figure 11) more effectively reduces glioblastoma cell viability than MJ [85]. This 1,2,4-oxadiazole derivative inhibited HK2 more strongly and irreversibly than MJ with a value IC50 of 0.27 μM, and 7.47 μM, respectively [88]. The mechanism of action involved dissociation of the HK2-VDAC complex associated with mitochondria [85].
Figure 11
Clotrimazole (CTZ) and Bifnazole: Clotrimazole-an azole derivative is a popular antifungal drug. Investigations suggest that it is a promising agent for other disease treatments such as sickle cell disease and malaria. A number of reports have suggested that clotrimazole may be a drug for cancer treatment [89]. The mechanism of action of CTZ in cancer cells reported by (Pastorino, et al. [90]) involves the dissociation of HK2 from VDAC. Dissociation of HK2-VDAC complex increases pro-apoptotic BAX binding to the mitochondrion, mitochondrial membrane porosity associated with the release of cytochrome c, and subsequent cell death. This mechanism of action of CTZ has been confirmed by other groups [30,91]. Another antifungal agent, such as bifonazole, affects hexokinase activity by disconnecting it from the mitochondria of B16 melanoma cells. The IC50 in the detachment of HK2 from mitochondria by bifonazole and clotrimazole was equal to 10–15 μM [91]. Recent research by Cristiane M. Furtado and co-workers [92] suggested that clotrimazole affects the activity of glucose 6-phosphate dehydrogenase and glycolytic enzymes such as hexokinase, pyruvate kinase and phosphofructokinase in breast cells and dysregulates glycolysis, which can reduce of tumour progression. Treatment of metastatic cell lines MCF 7, MDA-MB-231, and normal breast cells MCF10A with different concentrations of clotrimazole (0– 100μM) under 24 h incubation time showed inhibition of cancer cell growth, especially in the more aggressive lines such as MDA-MB-231. CTZ has been established to inhibit the activity of HK2 in a dose-dependent manner. Moreover, CTZ showed a more pronounced inhibitory effect on HK2 activity in cancer cell lines in comparison with normal cells [92]. The 100 μM CTZ dose inhibited the activity in normal cells (MCF10A cells), in 46% HK, while the HK activity in MCF-7 and MDA-MB-231 cells was inhibited in 90% and 96%, respectively, by the same concentration of CTZ. Alternatively, (Carpi, et al. [93]) proposed the mechanism of action of CTZ through direct inhibition of enzymes [93]. Their investigation suggests that clotrimazole causes cell-cycle arrest and apoptosis in human melanoma cells in correlation with inhibition of HK2. Their study shows that clotrimazole induced cell death in A375 melanoma cells and caused a reduction in HK expression and activity under treatment with 10 μM of CTZ. Moreover, their report suggested the selectivity of clotrimazole against cancer cells because this drug significantly inhibited the activity of the HK and induced apoptosis in cancer cells without major changes in proliferating human keratinocytes. This effect depends on the higher rate of glycolysis in melanoma cells in comparison to normal cells. The high activity of CTZ against multiple targets makes its selectivity low. Clinical studies have shown that oral use of CTZ causes cytochrome P450 enzyme inhibition-thereby limiting its therapeutic value [94].
Flavonoids: Flavonoids are natural polyphenolic compounds that exhibit anticancer activity by inhibiting glycolysis. According to the anticancer effect of oroxylin A on non-small cell lung carcinoma, this flavonoid influences the c-Src / AKT / HK II pathway and interferes with HK2 binding to VDAC. [95] Synthetic modification of another flavonoid, genistein, resulted in novel polyphenolic derivatives: (5-hydroxy- 7-(2-hydroxy-3-(piperidin-1-yl)propoxy)-3-(4-(2-hydroxy-3- (piperidin-1-yl)propoxy)phenyl)-4H chromen-4-one), gen-27 (Figure 12) [96]. In vitro and in vivo studies have demonstrated promising anticancer effects of Gen-27 on human breast cancer. Inhibition of breast cancer cell growth by Gen-27 is concentration- and time-dependent (10-30 μM) and shows stronger effects than its parent compound, genistein. The mechanism of action of Gen-27 is to reduce the expression of mitochondrial HK2. It was confirmed that gen-27 dissociated HK2 from VDAC1 and changed the translocation of HK2 from the mitochondria to the cytosol [96].
Figure 12
Another Class of Potential Anticancer Approaches: Reducing Expression HK2
Trastuzumab, an approved anticancer drug, is a monoclonal antibody that targets the HER2 receptor. HER2 overexpression occurs in some types of breast cancer with a poor prognosis. The binding of trastuzumab to HER2 receptors affects the Akt/PI3K and MAPK pathways, which influence glycolysis. Treatment with antiHER2 compounds in xenografts derived from MDA-MB-453 breast tumour cells resulted in a significant decrease in the expression of HK2 and GLUT1, which may be related to the inhibition of tumour growth [97]. In vitro studies on the effects of Trastuzumab on breast cancer cells showed that the drug causes a decrease in HK activity [98]. In a novel approach to cancer treatment, the usage of siRNA (Small Interfering RNA) to silence specific gene expression is considered [99]. Under treatment, anaplastic thyroid cancer cells with lentiviral Small Hairpin RNA (shRNA) reduction of HK2 expression and inhibition of cell proliferation were observed. Lenti-HK2 shRNA treatment is a method of prolonged repression of the expression of a targeted HK2 gene [100]. shRNA gene knockdown is characterized by high specificity because it interferes with the expression of one HK isoform [101]. Small hairpin RNA can stay in cells much longer than siRNA, so shRNA exhibits long-term effects. The vector expressing shRNA against HK2 decreased glucose uptake and total HK activity. Combination therapy using lenti-HK2 shRNA and 131I Human Sodium Iodide Symporter (HNIS) to treat anaplastic thyroid cancer cells in an animal model showed a significantly stronger antitumour effect than single therapy [100]. Another study showed that down-regulation of HK2 gene expression by shRNA inhibited LoVo colon cancer cell proliferation in vitro and tumour growth in vivo [101].
Combination Therapy
Chemotherapy and radiation therapy are most used for cancer treatment. The major challenge in the treatment of cancer is the chemo- and radiation-resistance of cancer cells, in factors related to disease progression and therapy failure. It is assumed that HK2 overexpression is associated with chemo- and radiation-resistant phenotypes [102,103]. HK2 inhibitors as potential adjuvant agents have been shown to restore the sensitivity of cancer cells to drugs available on the market. The selected studies presented in Table 3 confirm that HK2 inhibitors synergistically enhance the therapeutic effect of known anticancer drugs [102-121].
Table 3: Synergistic effect in cancer treatment in combinatorial therapy with HK2 inhibitors and commercially available anticancer drugs.
Chemoresistance
Drug resistance is often associated with higher energy requirements and increased glycolysis rates. By comparing human breast cancer cells MCF-7 and a drug-resistant cell line derived from them, data proved that the drug-resistant cell line showed a 3-fold higher rate of glycolysis and, consequently, a higher demand for ATP [103]. The complete depletion of ATP in cancer cells mediated by HK2 inhibition may be one of the main reasons for overcoming drug resistance in cancer. In addition, the reduction of ATP levels by HK2 inhibitors has shown a synergistic effect in combination therapy on growth inhibition and prevention of recurrence in several types of cancer cells [106,108,109,110]. In solid tumours, the expression of specific proteins like HIF-1α, GLUT1, HK2, and LDH significantly increased [106,108]. Cell hypoxia is considered a key factor in drug resistance. Therefore, combining HK2 inhibitors with typical anticancer agents may be a way to simultaneously target hypoxic and aerobic cells in tumours [110].
(Valera, et al. [110]) assumed that the synergistic effect of combination therapy with docetaxel and 2-DG is a result of effective targeting of rapidly growing tumours in normoxia by docetaxel, while 2-DG targets tumour cells in hypoxia. Cells treated with drugs such as cisplatin, which cause DNA damage, can become resistant to treatment by switching on DNA repair mechanisms. HK2 inhibitors usage and subsequent glycolysis inhibition retained repair mechanisms in cancer cells, and damages cannot be easily removed because their ATP level is reduced [105]. Lonidamine has been reported to interfere with the repair process of damaged DNA during combinatory therapy with cisplatin [114].
Radioresistance
Radioresistance can result from a variety of mechanisms. Low oxygen levels in solid tumours are one of the factors responsible for radioresistance. It is believed that a hypoxia-induced decreasing in the amount of reactive oxygen species, and consequently a reduction of DNA damage, is due to radiation therapy. Further defense mechanisms against radiation include detoxification of Reactive Oxygen Species (ROS) and repair of DNA damage after ionizing irradiation. Glucose metabolism plays a significant role in these processes because energy is required to activate repair mechanisms [122]. The use of HK2 inhibitors can prevent or reverse these effects. One of the HK2 inhibitors, 2 DG, has been used in clinical trials I/II phase as an adjunct to radiotherapy. The results showed an increased survival while improving the quality of life and selective sensitivity to radiation [108,109]. In phase III of clinical trials, LD usage improved the efficacy of radiotherapy. Potentially Lethal Damage (PLD) repair has been reported to be an energy-dependent process of repairing DNA damage after radiation therapy. It has been assumed that LD disturbs this process, and enhances the effect of radiation without toxic effects to normal tissues [111].
Sensitization
The main problem with the use of high doses of radiation and anticancer drugs is the wide range of side effects during and after treatment. According to some reports, it has been proven that the use of HK2 inhibitors during anticancer therapy with known pharmaceuticals or radiation allows the use of lower doses of these agents which are effective in inhibiting growth [111,115,116]. Preclinical studies by (Iliopoulos et al. [118]) on mouse xenografts have revealed that combined treatment with metformin and doxorubicin allows reduced dosage of doxorubicin. Treatment with an oral dose of 200 μg/mL metformin with 1g/kg doxorubicin injection caused complete tumour regression and no detectable recurrence for at least 65 days. Comparable effects were observed under 4g/kg injection treatment, which is associated with a 4-fold reduced dose of doxorubicin in cancer treatment.
Conclusion
Physiological features of cancer cells, such as uncontrolled growth, weak specialization of organelles, and different metabolism of glucose under aerobic conditions, distinguish them from normal cells. HK2 is the first enzyme involved in the glycolysis pathway, converting glucose to glucose-6-phosphate and its overexpression in cancer cells, and this has been confirmed in many studies. In addition to glucose phosphorylation, the function of mitochondrial HK2, which is associated with VDAC, is to protect cancer cells from apoptosis. Therefore, HK2 is a potent target in cancer treatment. This review presents the actual knowledge about hexokinase 2 inhibitors as potential agents in cancer therapies. These compounds have shown anticancer activity both in vitro and in vivo. The promising anticancer effects of HK2 inhibitors have been discussed in many studies. Only one HK2 inhibitor has been approved for clinical use in humans, namely, Lonidamine (LD); so much more research is needed to determine safe, highly specific, and efficient inhibitors. An important aspect in the design of HK2 inhibitors is selectivity toward other isoforms, which is related to the safety of these drugs. HK2 inhibitors should not affect HK1, HK3, and HK4 isozymes, which are needed to maintain normal cell functions High-specificity inhibitors for one HK2 isoform have been found to reduce the side effects of cancer therapy. Conducting studies on distinct functions, structural characteristics, and expression of HK2 from other isoforms can be used for preferential inhibition of HK2 over other isoforms in cancer. The review suggests that modification of already known inhibitors may be the way to find novel, selective, and effective inhibitors with good pharmacokinetic properties. The HK2 inhibitors discovered are characterized by selective activity against many cancers with insignificant effects on normal tissues. However, its use as a single anticancer agent is not effective enough. HK2 inhibitors appear to be promising as an adjuvant in combined therapies. The effects of HK2 inhibitors on drug-sensitive and drug-resistant cancer cells are a key area of research. Novel approaches awaiting further development could help us evolve novel research strategies and anticancer therapies.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Funding Statement
The research was financially supported by BKM-638/RCH- 2/2022.
Artificial Intelligence in Echocardiography and Cardiac POCUS (Point-of-Care-Ultrasound) during the COVID-19 Pandemic: A New Paradigm?
Introduction & Background
Since the beginning of the coronavirus disease-19 (COVID-19) pandemic in Wuhan, China several technological developments have had to be enhanced to adapt to our new reality. The use of artificial intelligence (AI) has had significant development in recent years with widespread applications being used in medicine [1]. Consequently, the implementation of AI for the identification, classification, and diagnosis of echocardiographic images during the pandemic grew exponentially in medical centers around the world [2]. Moreover, cardiac point-of-care-ultrasound (POCUS) is a type of echocardiographic assessment that guides a clinician in the initial evaluation and management of select patients. Its continuous use since it was first described in the 1990s, prompted a useful tool that has aided in the management of the complex COVID-19 patient with cardiovascular complications. However, both echocardiography and POCUS are operator-dependent and in inexperienced hands, they may skew the appropriate diagnostic assessment [1]. The use of AI in cardiac imaging has reduced the risk of misdiagnosis in certain cases and has proven especially useful in COVID-19 due to reduced exposure to the virus. This review will help researchers and clinicians expand on the current utility of AI in cardiac imaging during the COVID-19 pandemic.
Artificial Intelligence in Medicine
AI in medicine refers to the utilization of software to aid human cognition in the analyzing, presenting, and comprehending complex medical data [1,2]. AI comprises computer tools that replicate human intelligence processes including, learning, reasoning, and self-correction [1,2]. Through various algorithms, machines learn and can make decisions [2]. However, nowadays it is difficult to establish a universal definition to what is known as AI. The term itself is often applied to the field of computer science, which endeavors to mimic human cognitive processes, learning capacity, knowledge, memory storage, and improvement through trial and error [1-7]. The term AI was first used in the 1950s [2-4]. It emerged to name computer systems that emulated certain processes of the human mind. However, early models faced several limitations, hindering widespread acceptance and application in medicine [2,3]. In the 1970s, the first experience in the health sector was shared with a new software called Mycin [4]. This system was aimed to detect infectious blood diseases and communicate with users in natural language. It also prescribed medications individually tethered to each patient [4]. This software is considered one of the most significant early uses of AI in medicine. Other systems such as INTERNIST-1 and CASNET were also employed in the early days of AI but were discontinued due to inaccurate results [4]. Furthermore, in the 1980s and 1990s, modern, high processing computers positively impacted medicine after microchips further improved automated software [5].
The advances in computer science prompted new levels of connectivity, and with the use of worldwide networks, exponentialize AI’s advancement [5]. During this time, researchers and developers recognized that AI systems in healthcare must be designed to accommodate and improve data and aid, rather than replace, the expertise of clinicians [3-5]. Currently, these new technologies have allowed the growth of AI applications in healthcare [2-6]. Faster collection and processing capacity of clinical data, improvements in computer vision processing time, have allowed machines to replicate human perceptual processes exponentially. High-specificity robot-assisted surgery, better insight and data records on rare diseases, electronic medical record systems, increasing knowledge in the genomic sequencing, and software that recognizes pathological abnormalities during medical procedures have already successfully applied this type of robotic intelligence [2-7]. The applications of AI in medicine are based on several principles, such as improving accurate diagnosis and treatment, utilizing of robotic tools, relieving the burden on doctors, and drug development [5-7]. Nowadays, there is virtually no branch of medicine that does not actively research AI to enhance diagnostic and therapeutic methods. In Radiology and Infectious diseases, more accurate and detailed methods through computerized tomography and magnetic resonance imaging have been developed, significantly improving the diagnostic accuracy. In Oncology, there is ongoing research into the early detection of cancer and the identification of the most effective treatments. Likewise, in Cardiology, several groundbreaking applications have been developed [2-13].
Current Applications of Artificial Intelligence in Cardiology
Machine learning (ML) and deep learning, integral parts of AI, can assist healthcare providers in automating various tasks in echocardiography, serving as a valuable diagnostic tool [14] (Figure 1). It can help expand research capabilities and discover alternative paths in medical management in an automated manner pre-established by a software [14] (Figure 2). Moreover, several advances have already been made to implement fully automatic interpretation of echocardiographic images [15]. This has been accomplished through automated identification of views, image segmentation, quantification of structures and functions, as well as the detection of cardiac conditions [15]. One of the most developed applications of ML in Cardiology is the prediction of cardiac arrhythmias [16]. Numerous studies describe algorithmic models for atrial fibrillation development, using ML predictive systems composed of different threads: signal processing, extraction of significant variables, and classification algorithms [15]. Another application is the use of AI to identify phenotypes and classify hypertrophic cardiomyopathies [17]. Additionally, the software and algorithmic management of the ML system could help avoid hospitalizations for heart failure and recognize patients susceptible to cardiac decompensation after hospital discharge [15]. Studies have indicated that ML could improve the clinical outcomes of these patients [14]. Another noteworthy area is heart transplantation, with ML systems applied to predict the probability of death or the option of heart transplantation [14].
Figure 1
Figure 2
Basics of Ultrasound
Sound, as defined in physics, is mechanical energy that propagates through matter, taking advantage of its elastic properties [18,19]. It carries vibrational and longitudinal movements that spread parallel to the direction of the vibration [18,19]. Ultrasound (US) technology uses the aforementioned principles to generate images [19]. It produces high frequency sounds, imperceptible to the human ear, which are subsequently interpreted by a machine’s algorithm to produce real- time images. Echocardiography employs US to assess the structural components of the heart [20]. Since the first recording of an echocardiogram in 1953 by Edler and Hertz, the technological advancements in echocardiography have profoundly influenced modern cardiology [20]. Point-of-Care Ultrasound (POCUS) echocardiography adopts a practical approach to obtain necessary images for clinical decisions in the least amount of time [21,22]. It is not as profound or detailed as an echocardiographic assessment performed by Cardiologists, but it provides sufficient information to make clinical decisions at the bedside [22]. Widely accepted since the 1990s, POCUS echocardiography has been embraced by numerous hospitals worldwide as a routine diagnostic measure [22].
Point-of-Care Ultrasound
POCUS is a diagnostic and procedural guidance ultrasound tool performed by a clinician during a patient encounter to help guide the evaluation and management of the patient [23]. It is an evolving outpatient, inpatient, and urgent care diagnostic tool which is performed and interpreted at the bedside [24]. Interest in POCUS has grown steadily over the last few decades since it provides immediate availability and real-time images that can guide medical decision making [25]. Frontline physicians, mostly surgeons, and emergency medicine physicians, began assessing trauma patients with ultrasound in the 1970s [25]. Following this trend, in the early 1990s, the term FAST exam, or Focused Assessment with Sonography in Trauma, was coined [25]. From its early description in the 1970s in Europe to its incorporation into (ATLS) guidelines in the 1990s in the United States, the FAST exam set a precedent for incorporation of POCUS into routine clinical practice [25]. Additionally, POCUS has been used to aid in the diagnosis of multiple medical conditions ranging from acute appendicitis, small bowel obstruction, heart failure, pericardial effusions, airway compromise, abdominal aortic aneurysm, traumatic injury assessment to COVID-19 [26-29]. Although the gold standard diagnostic test for COVID-19 is reverse transcription-PCR (RT-PCR), POCUS has proven to be a safe and quick first-line bedside diagnostic alternative for COVID-19 lung, cardiac, and thromboembolic manifestations [27,29].
In addition to disinfection being faster and easier and improved portability, POCUS is an invaluable first-line diagnostic tool for COVID-19 patients [27-29]. Because of its ease of use, it has emerged as a viable option in cases where a formal radiological study would cause a delay in diagnosis and/or treatment [29]. Additionally, COVID-19 undoubtedly causes several cardiovascular manifestations. Acute heart failure, myocarditis, and pulmonary embolisms with thrombus are a few of the cardiovascular complications of COVID-19 where cardiac POCUS has proven useful during the pandemic [29]. However, no technology comes without pitfalls [21]. The operator-dependency on producing and interpreting accurate and precise images is a common problem frequently encountered in clinical practice [21,23]. This has made way for new technological and practical solutions to this dilemma.
Limitation of 2D Echocardiography
One of the principal indications for echocardiography in clinical practice is the assessment of the LV chamber size and the systolic function [30]. Typically, this assessment involves direct visualization and interpretation of the dynamic ultrasound to estimate the LVEF. If these interpretations were to be done using 2D echocardiography, certain assumptions regarding geometric remodeling of the left ventricle would be necessary [30-32]. One of the limitations of standard 2D echocardiography is referred to as the missing “third dimension”. The difficulty of endocardial visualization is most challenging in the apical-lateral segments, which can be compensated for by certain maneuvers with the transducer (i.e., lifting). Furthermore, 3D technology allows for frame-by-frame detection of the endocardial surface from real-time 3D datasets. Numerous studies have shown that compared to 3D echocardiography, 2D echocardiography may underestimate left ventricular volumes [32]. In a study of patients with LV dysfunction due to previous myocardial infarction, patients underwent serial real-time 3D echocardiographic measurements and had low test-retest variability but, they were able to detect small changes in LV volumes that could not be detected by standard 2D echocardiography [33]. The Disparity in measurements between 2D and 3D echocardiography has been different between various studies, suggesting a probable error in the measurement methodology.
A large multi-center study focused on identifying potential errors in the measurements, found that the major source of underestimation of volume was the tracing method and the limited spatial resolution of real-time 3D echocardiographic imaging [33]. There was a correlation between RT3DE-derived LV volumes and CMR imaging (EDV: r=91, ESV: R=0.93), but were found to be 26% and 29% lower consistency across different institutions. The reason for this was found to be that RT3DE cannot differentiate between the myocardium and the trabeculae [33].
AI in Echocardiography and POCUS Interpretation
Although concrete recommendations are available for interpretating echocardiography and cardiac POCUS, these techniques are still prone to a considerable number of subjective errors [34,35]. Besides the fact that there can be interpersonal differences in the initial imaging interpretation, interpretation differences can also exist for the same person upon repeated readings [36]. This frequently encountered pitfall has prompted the use of different technologies to avoid misdiagnosis. AI has the potential to obtain images, process them and accurately interpret them constantly and repeatedly. AI also has the ability to improve diagnostic accuracy, clinical management, and patient care accuracy [36]. Besides accuracy, AI also reduces human strain, especially for inexperienced echocardiographers. It typically takes a sonographer approximately 1-2 years to comprehend and accurately put into practice the basic concepts and techniques of echocardiography [36]. With AI, programmed standardization can reduce assessment time and improve beginner’s accuracy. Additionally, this technology has the potential to improve operational efficiency in non-echocardiographic settings, such as emergency departments, and can also be used by resident physicians as a rescue measure in the appropriate clinical scenarios [37]. Furthermore, time restraints may prove challenging, particularly if the patient presents with an infectious pathology or due to the sheer volume of patients at a medical center.
This may cause a delay in the diagnosis and skew prompt medical management. According to a single-blinded, nonrandomized, cross-sectional investigation involving clinicians with varying POCUS expertise, non-cardiologists practicing cardiac POCUS can reliably detect common causes of heart failure [38]. POCUS is increasingly recognized as a paramount technique, especially in the training of resident physicians for monitoring cardiac function. POCUS has achieved some of the most significant advances in the management of critically unstable patients due to its capacity to evaluate pathology in real-time at the bedside [38]. POCUS is also frequently utilized to investigate unexplained hypotension, arrhythmia, or difficulties with equipment such as ventricular support devices or extracorporeal membrane oxygenation [38]. Despite its accomplishments, POCUS has operator restrictions, principally as it is often performed by non-cardiologists and non-expert physicians [37,38]. As patients decompensate and the window for accurate medical management closes, these restrictions become increasingly important. The integration of AI intends to address some of these pitfalls, allowing doctors to create faster evaluations with more input data and obtain accurate diagnostic and treatment recommendations ultimately aiming to improve patient outcomes [39].
Consequently, when discussing AI in cardiac ultrasound (US), several techniques have emerged to improve outcomes.
For example, the use of AI for global longitudinal strain (GLS) assessment has significantly enhanced results [40]. The AI software was able to accurately identify cardiac images, conduct precise timing of cardiac events without human input, assesses the myocardium, estimates motion and eventually quantifies GLS, irrespective of a wide range of left ventricular (LV) function and picture quality [40]. The most extensively used semi-automatic speckle-tracking algorithms require multiple phases of operator input, with a single GLS analysis is said to take between 5 and 10 minutes to complete. On the other hand, AI assessment takes less than 15 seconds [40]. Left ventricular (LV) function, including ejection fraction (EF) quantification, is accurately conducted [40]. Other assessments performed during cardiac US have also been positively influenced by AI. AI-driven echocardiographic imaging analysis approaches done by automated contour-based segmentation have proven incredibly useful [41,42]. Asch et al. utilized a software called AutoEF and Baylabs to perform automated left ventricular ejection fraction (LVEF) calculations [43]. The approach demonstrated similar accuracy to measures taken by cardiologists with more than 20 years of expertise, as shown in a study of 99 patients [43]. Additionally, human experts trained the AI with a database of over 50,000 echocardiographic studies from the Minneapolis Heart Institute spanning a period of 10 years. Expert readers’ visual EF corresponded highly with the AI response (r r=0.95 (P<0.001; CI, 0.938-0.960), ICC =0.92 (CI, 0.90-0.936) [43].
This was comparable to the accuracy of three board-certified, expert readers: r=0.94 (P<0.001; CI, 0.925-0.952), ICC =0.90 (CI, 0.876-0.920) [43]. The AI completed the analysis in 1 to 5 seconds per patient with a high level of consistency [43]. Without extensive operator expertise, distinct physiological and pathological situations may exhibit similar characteristics that are challenging to differentiate. For instance, left ventricular hypertrophy is common among athletes, but it can also be detected in hypertrophic cardiomyopathy (HCM). Because hereditary cardiac illness has a higher risk of sudden cardiac death, a precise distinction is crucial [35]. After adjusting for age, Narula et al. developed an ensemble technique using support vector machines and artificial neural networks to accurately distinguish between these two conditions, achieving a sensitivity of 96% [44]. Additionally, the assessment of regional wall motion abnormalities (RWMA) for the treatment of ischemic coronary artery disease is a common examination in echocardiography [40]. Recently, a study examined a deep learning method to construct automated diagnostic models for myocardial infarction. The area under the receiver-operating characteristic curve (AUC) of a deep learning system for detecting the presence of RWMA was comparable to that of a cardiologist/ sonographer interpretation and significantly higher than that of resident readers. Except for the left anterior descending coronary artery, deep learning demonstrated relatively low rates of misclassification of the right coronary artery, left circumflex coronary artery, and control groups [32].
Zhang et al., using PLAX- and A4c-view videos, trained a multilayer technique to identify HCM using a cohort of patients with HCM (with varied patterns of LV thickness) and technically matched controls [45]. Instead of constructing a discriminative model based on hand-selected features, the technique establishes a black-box model wherein the training algorithm manages all the feature derivation and selection. With a C statistic (area under the receiver operating characteristic curve) of 0.93 (95% CI, 0.91-0.94), the model accurately detects HCM. Subsequently, they developed a model to identify cardiac amyloidosis, a disease with similar morphologic characteristics, but different in etiology. They trained an AI model to detect cardiac amyloidosis using amyloid patients and matched controls and obtained outstanding results, with a C statistic of 0.87 (95 percent CI, 0.83- 0.91) [45]. Similar to HCM, they observed that subjects with a greater projected risk of amyloid had larger LV mass (ρ=0.36, P=0.002) but did not exhibit increased left atrial volumes (ρ=0.12, P=0.31) [45]. These technologies have the potential to be applied in cardiac US for increased precision, removing the need for an expert operator in select cases. Additionally, by alleviating time constraints, physicians have increased safety precautions especially when dealing with unstable, combative, or highly infectious patients. Artificial intelligence algorithms can provide extreme value in capturing high-dimensional information that is not easily perceptible to the human eye, as well as maximizing the extraction of image features.
Through this process, AI can help to identify crucial cardiac anatomical structures, improve the accuracy of cardiac segmentation, and help with the assessment of cardiac functioning [46]. Therefore, the cardiac imaging assessment of COVID-19 patients should be performed promptly without compromising diagnostic accuracy. AI has the potential to expedite this process by providing more consistent analysis for echocardiographic images [47]. Additionally, according to a prospective study which compared the cardiorespiratory parameters and time duration for assessment between Vscan Extend and the conventional US machine, this modality proved incredibly useful during the pandemic [48]. Vscan Extend is a handheld ultrasound device with a dual probe and an AI application software to precisely detect EF. In COVID-19 patients, the Vscan Extend portable US instrument aided in the quick detection, evaluation, and diagnosis of cardiopulmonary complications due to COVID-19 [48]. The Vscan Extend handheld US device’s agreement with the traditional approach demonstrated its efficacy and safety [48]. On a large scale, integrating this device into daily practice, both in COVID-19 patients and different clinical settings, could alleviate the load on the healthcare system by aiding in quick diagnosis and requiring fewer resources for an initial cardiopulmonary examination [47]. However, many questions remain unanswered due to the lack of randomized control trials. More clinical data in the upcoming years will elucidate additional potential applications for AI in cardiac ultrasonography and the validity of current utilization trends.
Ultrasonographic Assessment in COVID-19 Patients
POCUS can play a crucial role in the clinical setting by assisting in the diagnosis of common causes of poor oxygenation and hemodynamic instability in critically ill COVID-19 patients, including cardiac arrest [49]. Common findings that can be identified using POCUS in COVID-19 patients include confluent and inferior lung field lesions, thickened/irregular pleural lines, subpleural consolidations, and air bronchograms [50]. Huang et al. used lung ultrasound to evaluate pulmonary lesions in 20 patients who were not critical at the time in a hospital in China. They concluded that ultrasound may be superior to computed tomography in detecting small peri pulmonary lesions and effusions [51]. Lung ultrasound proves invaluable in practical setting for managing COVID-19 patients, allowing for the assessment of pulmonary complications/abnormalities, assess perioperative pulmonary status evaluation and guide ventilation management. Ultrasound can also confirm adequate endotracheal tube positioning, assessing for proper central venous catheter (CVC) placement, and rule out pneumothorax after CVC insertion [52]. Lung ultrasound has demonstrated high overall diagnostic sensitivity and specificity in COVID pneumonia [53]. While COVID pneumonia predominantly affects the posterior-basal lung zones, POCUS/LUS provides an effective view of the lung’s peripheries [54]. Particularly in Covid-19, B-Lines are most commonly visualized in the posterior-lateral lung zones in the early stages of the disease [55].
POCUS is particularly useful in evaluating cardiac involvement in COVID-19 cases. It is well-established that COVID-19 can damage the myocardium either by activating the immune cascade or via primary viral infection, affecting cardiac function by myocarditis or pulmonary embolisms [56]. The highest accuracy of POCUS in these settings is obtained when used to evaluate left and right ventricular function, valvular dysfunction, pericardial effusion and to calculate stroke volume [56].
Use of AI beyond the COVID-19 Era
In addition, AI in echocardiography and POCUS, can be used to calculate LV systolic function, and will continue to be of the most important uses of this technology. Knackstedt et al. tested a fully automatic software employing machine learning-enabled image analysis [57]. The autoLV can provide biplane end-diastolic and end-systolic volumes in a more feasible way in 98% of studies with an estimated time of 8 seconds/ patient. This means that automated analysis can provide quick and reliable EF measurements via LVEF and LV strain [57]. Cannesson et al. also explored the use of AI in calculating EF in 218 patients, demonstrating strong correlation with manual measurements (r= 0.98%), with far less time (48.2 s vs 102.2; p<0.01). When compared to visual estimates by expert readers, it correlated well (r= 0.96; p<0.01) [58]. A newly released Venue platform that can calculate velocity time integral and cardiac output in real time. Real-time visualization of this data can be time saving and improve prompt adequate decision making by clinicians [59]. Bobbia et al. determined in an experimental study that the Venue Auto-VTI tool had a better correlation with cardiac output measurement by thermodilution than any manual measurement [59]. The new echocardiographic techniques allow for the accurate assessment of mechanical properties of the myocardium, especially strain or deformation. Moreover, myocardial strain has been shown to offer more accurate measurement of systolic function compared to manual cavity measurement parameters.
These methods have been used in various clinical scenarios including cardiomyopathies, oncologic cardiology and to detect the presence of cardiac remodeling. These techniques also allow clinicians to recognize various myocardial strain patterns that can correspond to different disease processes [60]. Furthermore, machine learning-augmented interpretation aids in distinguishing between diseases with similar echocardiographic characteristics. Sengupta et al. used clinical and echocardiographic data of patients with constrictive pericarditis and restrictive cardiomyopathy to develop an associative memory classifier (AMC) based algorithm. This was possible with the addition of speckle tracking echocardiography, obtaining the diagnostic area under the curve of 89.2% [61]. Another potential advantage of employing AI in echocardiography is the assessment of valvular pathology. In a study by Moghadassi et al., mitral regurgitation severity was approached by utilizing binary patterns as image descriptors which include details from different viewpoints of the heart using KNN (k-nearest neighbors) clustering and SVM (support vector machine), with an accuracy of 99.52%, 99.38%, 99.31% respectively. These findings corresponded to a sensitivity and specificity of 99.38% and 99.63% [62]. Lastly, many of the common cardiovascular diseases have been called heterogenous, with many genetic, pathological and socioeconomic factors in effect [63].
There can be many ML algorithms that can be utilized to identify the numerous subtypes using databases in echocardiography. Sachez- Martinez et al. conducted a study in 150 patients aged >60 years old to evaluate for measurement of LV function at rest and during stress echocardiography in order to assess for differences between heart failure with preserved ejection fraction and healthy patients. The data that was utilized was acquired from the MEDIA study (metabolic road to diastolic heart failure). The machine learning algorithm was used to categorize patients, with a clinical validation performed afterwards. The correlation gave encouraging results (72.6%; 95% confidence interval, 58.1-87.0) [64].
Conclusion
Artificial intelligence (AI) has become an essential tool in modern medicine, particularly in the field of echocardiography. The use of AI is paramount in contexts characterized by time constraints, limited resources or patients with infectious comorbidities where fast and accurate cardiovascular evaluations are imperative. Undoubtedly, AI algorithms improve the interpretation of echocardiograms and point-of-care cardiac ultrasounds (POCUS), offering timely diagnosis and optimization of the management of cardiovascular complications related to COVID-19. Although its utility is evident, further comprehensive research is needed to validate, generalize and refine its use in various clinical settings. Additionally, its application in the post-covid era is still an exciting prospect. Artificial intelligence is here to stay and revolutionize cardiovascular healthcare, improving diagnostic accuracy and improving patient outcomes, which is at the heart of our medical practice.
Conflict of Interests
We hereby attest that all authors included in this manuscript have no conflict of interests
Survey of Knowledge about Fracture Prevention Among Patients and their Relatives at Department of Orthopaedic Trauma An Binh Hospital
Introduction
Fracture is a condition in which bones are broken due to external forces from domestic accidents, traffic accidents, etc. Fractures are divided into closed fractures (the outer part of the skin where the fracture is not damaged), open fractures (the outer skin damaged by the fracture head) most often occur in the hands and feet; Subsidence fractures (two bones colliding causing the broken bone to be shortened) usually occur in the spine. Signs of fracture are swelling, pain, bruising, deformity, loss of function of the injured area, protruding bones… In addition, osteoporosis is now a disease that can cause fractures due to weakened bone force and impaired bone structure, leading to a condition where the bones become brittle, easily broken when colliding with an opposing force, such as a fall for example [1]. Important bones that are often fractured are the vertebrae, hip, femoral neck and arm bones. Fractures of the ribs and pelvis are also common in older patients, and can also be considered a consequence of osteoporosis. In many cases, the bone is broken but has no superficial manifestations, and the sufferer is unaware of it. Therefore, osteoporosis is also known as a “silent disease”. Partly because of this “silent” property, osteoporosis is therefore a very common disease in the community, especially among the elderly. In Vietnam, statistics show that about 20% of women over 60 years old have symptoms of osteoporosis [2]. One of the leading causes of fractures is too low bone density in people [3].
According to epidemiological studies among Caucasians, 1 in 2 women who live to the age of 85 will have a fracture, and 1 in 3 men living in the same age group will have a fracture. These frequencies are equivalent to the frequency of carrying heart disease and cancer. Indeed, the risk of femur fracture in women is comparable to the risk of breast cancer. A fracture, which can occur in any location, is also a warning sign for a subsequent fracture with a relative risk (RR) ranging from 1.4 to 4.9 depending on the fracture site (hip fracture increases the risk of a second fracture by 2.8 times in women and 4.9 times in men) [4]. The serious consequence of a fracture is a decrease in life expectancy, the risk of death is higher in men (1.8 times) than in women (1.4 times). Research by Syroid, et al. [5] shows that up to 24% of women and 38% of men die in the first 3 months after hip fractures; the rest often have chronic pain, reduced quality of life, and depend on the care of others. At the community level, fractures are a significant socio-medical burden, as the disease is very common and has a high cost. An Binh Hospital, Ho Chi Minh City with more than 500 patient beds, bed occupancy rate is more than 90%, on average receiving more than 3000 outpatients per day. The orthopedic department at the hospital with 37 beds, receives about 60 patients per day for examination and treatment. In particular, the number of hospitalizations for bone fractures has been increasing in recent years. Therefore, the research objective of this project is to assess the knowledge of relatives and patients on fracture risk prevention at the Department of Orthopaedic Trauma, An Binh Hospital in 2022.
Research Methodology
Study Design
Cross-sectional descriptive study.
Time and Location
The data collection period is from 06/2022 to 08/2022 at the Department of Orthopaedic Trauma, An Binh Hospital.
Sample Size
For Z 1-α/2: Confidence coefficient, corresponding to 95% confidence, the confidence coefficient is 1.96 p = 0.5 (For the largest sample size, p = 0.5 should be selected); d: The allowable deviation between the ratio of the studied sample and the rate of implementation (d = 0.1). Using the above sample size formula, the basic sample required for the study is n = 97, plus the error and rounded to 129.
Study Subjects
Sample Selection Criteria: All relatives and patients are treated for fractures at the Department of Orthopaedic Trauma and agree to participate in the study.
Exclusion Criteria: relatives who are dumb, deaf, unable to give interviews, relatives who are not direct caregivers.
Data Collection Method
The data collection group has 4 nurses will be divided into 2 groups to provide a list of patients being treated at the department and directly interview relatives and patients with a set of prepared questions designed on Google Forms within 10 minutes.
Data Analysis and Processing
SPSS software version 22.0 is used for data entry, analysis and data processing. Frequency, ratio, average values are used to represent variables.
Medical Ethics
The topic is approved by the Review Council according to Decision No. 658/QD-BVAB, dated 07/09/2022 of An Binh Hospital.
Results
The results showed that the majority of patients and relatives in the study were between the ages of 19 and 79 years old, of which 59.7% of the study participants were over the age of 35 years (Table 1). In terms of gender, participants in the study were quite even in the proportion of men and women, of which women accounted for 56.6% and men accounted for 43.4%. Over 80% of study participants were Kinh ethnic group (80.6%) and lived in urban areas (84.5%). The majority of study participants had occupations in the manual labor group with 72.1%. Regarding the causes of fractures, study participants answered that the causes of fractures were mainly traffic accidents (38.8%), domestic accidents (37.2%) and occupational accidents (24%) (Table 2). Regarding the time from fracture to surgery, nearly half of the study participants were operated within 6 hours of the fracture (49.6%), nearly a quarter of the study participants had surgery from 6-24 hours (24.8%) and over a quarter of the study participants were operated within 24 hours of the fracture (25.6%). Regarding the history of osteoporosis treatment, only 17.1% of patients and relatives responded that they had ever received drugs including drugs such as Aclasta, Fosamax, Protelos, and traditional drugs. Regarding the history of falls, 93.6% of study participants had fallen at least 1 time, of which 15.5% of study participants had fallen 2 or more times. Regarding the family history of someone prone to fractures, 50.4% of relatives and patients responded that there was a family history of someone prone to bone fractures. The results showed that 11.6% of the study participants smoked from 2 to 15 cigarettes / day, 13.2% of people reported drinking alcohol from 0.3 to 1 liter / day.
Table 1: Socio-demographic characteristics of the participants (N=129).
Table 2: Cause of fracture and history of drug treatment, history of fracture of relatives and patients (N=129).
In addition, 19.4% of relatives and patients said they had used corticosteroid medications. In terms of current fitness status, only 2.7% of study participants practiced physical exercise and the sports listed such as walking, football, volleyball, basketball, badminton and dance. The results showed that most of the study participants had a high rate of correct knowledge, including 93% of the study participants with knowledge of osteoporosis prevention, so they walked briskly every 10 minutes, 3 times a day (Table 3). 93.8% of study participants had the correct knowledge that smoking had a higher risk of osteoporosis and fractures, and that underweight people had lower total bone mass, so a small extra weight loss was enough to increase the risk of fractures. 97.7% of the study participants had the correct knowledge that women were 4 times more likely than men to have their estrogen levels drop after menopause, and the same rate said that older people need to actively check for potential hazards such as obstacles, etc carpets or slippery floors. The majority of participants recognized the need to check for osteoporosis level (99.2%). However, only 93.8% plan to design crossbars with handrails in bathrooms or toilets to prevent falls. The results also showed that 18.6% of patients and their relatives had planned or had undergone examination and treatment with Chinese, oriental and traditional medicines prior to admission (Table 4).
Table 3: Study participants’ smoking, drinking, corticosteroid use, and exercise status (=129).
Table 4: Knowledge of osteoporosis prevention of relatives and patients (N=129).
Discussion
We conducted research on 129 patients and relatives of patients with bone fractures, of which 53 patients and relatives of patients were male, accounting for 43.4%, 73 patients and relatives of patients were female, accounting for 56.6%. The gender distribution of patients and relatives of patients with broken bones is more common in women than in men. This result is in contrast to the research of the group of authors Tran Trung Dung and Do Van Minh from Hanoi Medical University on 66 patients with two forearm fractures undergoing bone and screw fusion surgery, showing that the proportion of males, females is 71.4%, 28.6% [6].
Besides, working age and participation in traffic activities are also factors that increase bone fractures. The age group from > 35 years old accounts for 59.7% while the age group from 19 – 23 years old accounts for 14%. This result is similar to the study of Hanoi Medical University in 2014 with the average age of patients being 34.73±13.54 [6]. The result is also consistent with the study of Nguyen Lam Minh Tam and colleagues (2022), the age group with the highest proportion is from 31 to 45 years old with 17 cases (accounting for 40.47%) [7]. This is the age group that participates more in labor and is more active than other ages, so this happens more accidents; The occupations of patients and their relatives are also different, with nearly three-quarters of the study subjects being manual laborers and working conditions being different. Research results show that fractures due to traffic accidents account for 38.8%, higher than the causes of work accidents (24.0%) and daily life accidents (37.2%). This result is equivalent to the study of Hanoi Medical University with the main cause of traffic accidents [6]. Our research results are lower than the main cause of traffic accidents accounting for 71.4% by Nguyen Lam Minh Tam [7]. This shows that awareness of traffic participation and the traffic order and safety situation in our country are still weak.
In addition, the cultural level is still low, the understanding of traffic laws is also low. Furthermore, safety at work is not considered important. From there, it is consistent with the injury model in our country when the dense traffic of two-wheeled vehicles makes the group of patients whose injury cause is traffic accidents account for a high rate [7]. Our research shows that the time from injury to surgery is less than 6 hours accounting for 49.6%, from 6 to 24 hours accounting for 24.8%, over 24 hours accounting for 25.6%. From there, it was found that the time of less than 6 hours accounts for the highest rate because of early assessment and intervention, reducing the risk of complications in bone fractures. This is consistent with the research of Pham Ngoc Thang and colleagues; orthopedic traumatologists consider bone surgery from the beginning to be a reasonable choice in cases of bone body arm fractures. The reason for early surgery is to expose the nerves for examination, which is necessary to assess the damage and treat appropriately [8]. From the above analysis results, the main cause of bone fracture is a previous fall, accounting for a high rate of 78.3%, and no previous fall accounting for a very low rate of 6.2%. A history of falls increases the fear of falling, and people who are afraid of falling tend to shy away from physical activity, a reduction in movement that increases their risk of falling. Therefore, it is necessary to strengthen health education and communication on fall prevention for patients and their relatives; raising awareness about increasing activity for the elderly needs to be considered when implementing fall prevention programs [9].
The majority of people with broken bones often do not exercise, accounting for 78.3%, while in cases of walking, playing football, basketball, etc., the fracture rate is very low, 2.7%. The golden rule of preventing and treating osteoporosis and fractures early is that in addition to a complete diet rich in calcium and minerals necessary for bones, maintaining a healthy, active lifestyle, harmoniously combining physical activity from young age to old age, avoid bad habits that affect bone health such as drinking too much alcohol, smoking, excessive dieting, lack of exercise,…[10]. Most believe that the reason women are 4 times more likely to have osteoporosis than men is because their estrogen levels decrease after menopause, accounting for 97.7%, and that older people need to proactively check these potential hazards such as obstacles, carpets or slippery floors also account for the same proportion (97.7%). This result suggests that we should learn and detect the potential risks of fall-related risk factors in the home itself to improve safety in the daily lives of the elderly and help reduce falls in house [9].
Conclusion
The rate of correct knowledge about preventing bone fractures is quite high: 93% of study participants had knowledge about preventing osteoporosis and should walk briskly 10 minutes/time, 3 times/ day; 93.8% had correct knowledge that smoking has a high risk of osteoporosis and bone fractures, and that people who are underweight have an increased risk of bone fractures; 97.7% of study participants had correct knowledge that women are four times more at risk than men because their estrogen levels decline after menopause, and 97.7% believed that for those older adults need to proactively check for potential hazards such as obstacles, carpets or slippery floors. The majority of participants recognized the need to check the level of osteoporosis (99.2%). However, only 93.8% planned to design horizontal bars with handrails in the bathroom or toilet to prevent the risk of falls and 18.6% of patients and relatives planned or had gone for examination and treatment with chinese medicine, oriental medicine and traditional medicine before admission to the hospital.
Sponsorship Statement
The Scientific Council approved the research with project code: CS/BVAB/22/04, An Binh Hospital, Ho Chi Minh City.
Conflict of Interest Declaration
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of the article.
Research Progress on Insulin-Like Growth Factor 1 in Pain
Introduction
The 2020 revised definition of pain by the International Association for the Study of Pain (IASP) characterizes it as an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage. Pain is a specific physiological response to noxious stimuli and it is also considered a disease in itself, categorized by its etiology into traumatic pain, inflammatory pain, neuropathic pain, cancer pain and psychological pain. When the body experiences noxious stimuli, pain receptors detect signals generated by tissue damage. Action potentials are then generated and transmitted via nerve fibers to the central nervous system, resulting in the perception of pain. Insulin-Like Growth Factor (IGF) is a polypeptide that exerts physiological effects when it binds to its receptors. While it plays a significant role in various physiological processes such as cell proliferation, growth, metabolism and so on, there are a limited number of reviews and reports on the role of IGF in pain. This article briefly summarizes existing research on IGF-1 in pain-related conditions, providing potential insights for future pain diagnosis and treatment.
IGF Family
Discovered in 1957, the IGF family comprises IGF-1, IGF-2, IGF-1 receptors (IGF-1R), IGF-2 receptors (IGF-2R), and insulin-like growth factor binding proteins (IGFBPs). Due to its high genetic similarity to insulin and similar functions, the IGF was named “insulin-like growth factor.” The primary ligands for IGF are IGF-1 and IGF-2, which exert physiological effects by binding to their respective receptors. IGF1 is synthesized in multiple tissues including liver, skeletal muscle, bone and cartilage. The changes in blood concentrations of IGF1 reflect changes in its synthesis and secretion from the liver, which accounts for 80% of the total serum IGF1 in experimental animals. The remainder of the IGF1 is synthesized in the periphery, usually by connective tissue cell types, such as stromal cells that are present in most tissues [1]. IGF-1 is a member of the insulin gene family. It is a 70 amino acid long growth factor hormone with potent anabolic effects during development. The hypothesis that IGF-1 is not only implicated in the regulation of cell growth, differentiation, and apoptosis, but it is also a potential and useful marker of malnutrition status, by defect or by excess, is supported by the U-shape relationship existing between IGF-1 serum concentrations and body mass index. [2,3].
The liver is the main source of circulating insulin-Like Growth Factor-1 (IGF-1) (more than 75%). The variety of IGF-1 activities can be partly summarized as cell proliferation and differentiation; tissue growth and development; insulin-like activity; anti-inflammatory; and antioxidant, mitochondrial protection, and prosuivival/antiaging. On the other hand, a specific and not well-understood IGF-1 activity might consist of contributing to cell polarity, acting on cytoskeleton [4,5]. As a key cytokine in the nervous system, IGF-1 produced in the tissue in response to injury sensitizes the primary afferent neurons via IGF1R and produces tissue injury-induced pain hypersensitivity [6,7]. Several studies have suggested that IGF-1 enhances T-type channel currents through the activation of IGF-1R that is coupled to a G protein–dependent PKCα pathway, thereby increasing the excitability of DRG neurons and the sensitivity to pain [8]. The research findings by Lin and colleagues provided morphological evidence that T-type Cav3.2 channel, at least partially, mediates the pain facilitation of IGF-1/IGF-1R signaling in chronic inflammatory pain condition [9]. Given the association of IGF-1 with pain, numerous studies have been conducted both domestically and internationally. Miura et al. proposed that IGF-1 produced in the tissue in response to injury sensitizes the primary afferent neurons via IGF1R and produces tissue injury-induced pain hypersensitivity [10]. Some studies have indicated a relationship between the hypothalamus-pituitary-target organ secretion axis and pain generation. Bálint et al. found that retrograde endocannabinoid is involved in the effect of IGF-1, the endocannabinoid 2-AG, tonically secreted from the GnRH neuron, decreases the excitatory GABA release from the presynaptic axon terminals and thus, suppression of the endocannabinoid production results in an increased GABA release and fine-tuning the hypothalamus-pituitary- gonadal axis [11]. In conclusion, IGF-1 is closely associated with neuropathic pain, inflammatory pain, and cancer pain.
IGF Family and Pain
IGF Family and Neuropathic Pain: Neuropathic pain refers to pain caused by nerve damage and lesions occurring anywhere in the nervous system, including peripheral nerves and the central nervous system. Chen et al. found that IGF1 (derived from astrocytes) in the lumbar cord increased along with the neuropathic pain induced by CCI. IGF1R was predominantly expressed on neurons. IGF1R antagonism or IGF1 neutralization attenuated pain behaviors induced by CCI, relieved mTOR-related suppression of autophagy, and mitigated neuroinflammation in the spinal cord. These findings reveal that the abnormal IGF1/IGF1R signaling contributes to neuropathic pain by exacerbating autophagy dysfunction and neuroinflammation [12]. Elevated IGF-1 expression is closely related to neuropathic pain, and it enhances T-type channel currents through the activation of IGF-1R that is coupled to a G protein–dependent PKCα pathway, thereby increasing the excitability of DRG neurons and the sensitivity to pain [13]. Several studies provide practical evidence for the treatment of neuropathic pain with IGF-1R antagonists.
IGF Family and Inflammatory Pain: Inflammatory pain results from biological or chemical inflammation in peripheral tissues, eliciting discomfort associated with sensory receptors and signaling pathways. There has been extensive research on inflammatory pain, both domestically and internationally, focusing on receptors, ion channels, growth factors, neurotrophic factors, prostaglandins, and more. Mayumi Miura suggested that increased tissue IGF-1 production sensitizes primary afferent neurons via the IGF1R/Akt pathway to facilitate pain hypersensitivity after tissue damage [14].
IGF Family and Cancer Pain: Cancer pain arises from tumor-induced tissue ischemia, tumor infiltration of surrounding organs, or nerve compression. It has a severe impact on patients’ daily life, selfcare abilities, and overall quality of life. Tas et al. found that elevated serum level of IGF-1 is associated with favorable progression-free and overall survivals in EOC patients [15]. In breast cancer, the adjuvant hormonal treatment of choice for postmenopausal estrogen-receptor- positive breast cancer, and (原文 although) the pain is usually attributed to the estrogen depletion associated with Ais. Gallicchio et al. suggested the IGF axis in the development of AI-associated musculoskeletal pain, a first step in developing effective interventions [16]. In cancer-related bone pain, Wan proposed that when the cancer cells metastasized into bone marrow, the elevated endogenous formaldehyde induced bone cancer pain through activation on the transient receptor potential vanilloid subfamily member 1 (TRPV1) in the peripheral nerve fibers. More interestingly, TRPV1 expressions in the peripheral fibers were upregulated by the local insulin-like growth factor I (IGF-I) produced by the activated osteoblasts [17]. Similarly, in a rat breast cancer model, Li and colleagues found that TRPV1 current density was significantly increased in the acutely isolated DRG neurons from bone cancer pain rats. At the same time, there was an increase in the expression of insulin-like growth factor 1 (IGF-1) in the tibial cavity [18]. This suggests that in cancer pain, IGF-1 production is mediated through the expression of TRPV1.
Conclusion and Outlook
As the fifth vital sign, pain is increasingly receiving attention and insulin-like growth factor 1 (IGF-1) plays a crucial role in the development and manifestation of pain. Given the significant impact of pain on patients’ quality of life, further elucidating the mechanisms and pathophysiological processes of IGF-1 in pain is crucial. Exploring therapeutic approaches targeting the mechanisms of IGF-1 in pain management will be a focal point in research, with the aim of improving the quality of life for individuals experiencing pain.
Nutritional Profile of Annona Muricata and Ageratum Conyzoides Based Herbal Teas for the Management of a Precancerous Lesion: Atypical Hyperplasia of the Mammary Gland
Introduction
Hyperplasia, a term for an abnormally large volume of a tissue or organ due to an increase in the number of its cells [1], is characterized by the proliferation of epithelial cells of a specific tissue. It becomes atypical when the proliferating cells are abnormal or in an unusual way. When this abnormal proliferation attacks the cells that line the ducts or lobules of the breast it is called Atypical Mammary Hyperplasia (AMH) [2]. The prevalence of AMH is increasing every year and it is one of the leading breast disorders in women of childbearing age [3]. AMH is considered a potential precancerous lesion that can progress to breast cancer if left undiagnosed and untreated [4,5]. Breast cancer is a heterogeneous disease in which normal cells of the mammary gland adopt a malignant phenotype and proliferate indefinitely and uncontrollably, destroying breast tissue [6]. According to a report by the World Health Organization (WHO) and the International Agency for Research on Cancer (IARC), approximately 22 million people will be annually affected by cancer by 2030: 8 million more than in 2012 [7]. In 2021, cancer was the leading cause of death worldwide, accounting for about 10 million deaths: the most common in terms of new cases being breast cancer with 2.26 million cases [8]. In Cameroon, the figures are even more alarming and breast cancer is the most common in terms of prevalence and mortality. According to several studies, 70-80% of patients are diagnosed at advanced stages and nearly 2000 women die from it each year [9]. In addition to the delay in diagnosis, other risk factors for cancer include gender, age, family history, reproductive risk factors and obesity [10]. Obesity is particularly characterized by an abundance of adipose tissue where oestrogen synthesis takes place, and it plays a major role in both abnormal cell proliferation in the mammary gland and in the uterus, and that can progress to malignancy and metastasis [11]. There is an association between high fat, protein and carbohydrate diets and the increased risk of breast cancer through increased oestrogen production, hyperinsulinaemia and insulin resistance. High fat and protein diets play a role in the increase in oestrogen production by adipose tissues [12,13].
Polyphenols are good in slowing down cell proliferation; they are particularly good in the development of blood vessels and in inactivating carcinogenic products through their antioxidant activities. Plants, taken in form of herbal tea, are used by about 80% of the world’s population for their curative virtues [14,15]. They can help female populations to reduce the risk of developing gynaecological cancers. Annona muricata and Ageratum conyzoides are two plants from the Annonaceae and Asteraceae families respectively, which have shown convincing results in previous studies. Nutritionally, Annona muricata leaves are rich in protein (25 ± 0.06 g/100g), lipid (21.22 ± 1.01 g/100g), carbohydrate (16.62 ± 0.09 g/100g), Potassium (363.05 mg/kg), Calcium (11183.50 mg/kg), Sodium (694.86 mg/kg), Magnesium (9619 mg/kg) and Iron (139.50 mg/kg) [16,17]. Ageratum Conyzoides leaves contain crude protein (24.53 ± 0.104), lipid (3.78 ± 0.069), carbohydrate (36.81 ± 0.006), Sodium (88.50 ± 0.346), Potassium (139.10 ± 0.006), Calcium (220.60 ± 0.173), Magnesium (110.13 ± 0.115), Iron (22.73 ± 0.289), Zinc (43.50 ± 0.173) and Phosphorus (380.13 ± 0.173) [18]. The rich nutritional composition of these plants is responsible for their medicinal effects, including antibacterial, antiproliferative and even anticancer activities. Referring to their antiproliferative and anticancer effects, Annona muricata has shown convincing results on breast cells with 98% efficacy in previous studies [19]. Adebayo, et al. [20] demonstrated that the in vitro anticancer activity of aqueous extracts of Ageratum Conyzoides is more effective on lung, uterine, breast and liver cells. Based on these results, a combination of the two plants in the form of formulas proved to have more interesting properties leading to promising conclusions on slowing down AMH (Publication in progress). The main objective of this work was to evaluate the nutritional properties of formulations made by combining Annona muricata and Ageratum Conyzoides.
Materials and Methods
Plant Material
Annona muricata and Ageratum Conyzoides were collected in Yaoundé, Centre region in October and November 2019 between 5:30 and 6:30 am. They were identified by comparison at the National Herbarium of Cameroon against the numbers 6575 SRFK (YA) and 18681/ SRF/Cam (YA) respectively. The collected plants were weighed and spread out for 24 hours on large trays in a room (20-21°C) for wilting.
Preparation of Extracts
The wilted leaves were dried at 40°C in a ventilated oven for 24 hours. Once dry, they were milled using a blender and then sieved using a 150 μm mesh size sieve. The obtained powders were infused in boiling water in the ratios of 1/5 and 1/6 g/mL for Annona muricata and Ageratum Conyzoides respectively for 2 hours, stirring every 30 minutes. The solution was filtered, and the residue was rinsed twice. The obtained solution was freeze-dried, and a mixing plan used in industrial research and development studies [21,22] helped to have five combinations of the freeze-dried extracts in the proportions 100/0; 75/25; 50/50; 25/75 and 0/100 corresponding to C100Rh; C75Rh; C50Rh; C25Rh and C0Rh respectively (C for Annona muricata and Rh for Ageratum Conyzoides).
Crude Protein Content
Crude protein content was determined according to the method described by Devani and al (1989) [23]: it is a spectrophotometric method based on the conversion of total organic nitrogen to ammonium sulphate.
Carbohydrate Content
The determination of soluble carbohydrates was carried out using the Chronolab assay kit based on the oxidation of glucose to gluconic acid catalysed by glucose oxidase (GOD). The hydrogen peroxide (H2O2) produced is detached using a chromogenic oxygen acceptor, phenol ampirone in the presence of peroxidase (POD).
Lipid Content
Total lipids were extracted with Soxhlet according to the Russian method as described by Bourely, (1982) [24] based on the differential solubility of lipids in organic solvents (hexane) at high temperatures about 12 hours.
Mineral Content
The minerals Ca, Na, Mg and K were analysed according to the method described by Horwitz, (2000) [25] based on the separation of the minerals from the sample matrix by wet digestion of the organic matter. The separated minerals were diluted in acid and their content determined by atomic absorption spectrophotometry.
Statistical Analysis
Statistical analyses were performed using IBM SPSS 20.0 software for Windows. The data were analysed by 1-way ANOVA and Tukey’s multiple range test was used to determine the differences among samples. Significant levels were defined as probabilities of 0.05 or less. The obtained results were presented as mean ± standard error of the mean (SEM). Excel 2016 software was used for graphical representations.
Results and Discussion
Crude Protein, Fat and Soluble Carbohydrate Content
Table 1 shows the macronutrient content of the different combinations (formulations). Protein content ranged from 25.07 g/100g DM to 12.01 g/100g DM: fat content from 22.42 g/100g DM to 20.65 g/100g DM and carbohydrate content from 0.63 g/100g DM to 0.23 g/100g DM with statistical significant difference (p< 0.05) between the protein content of the different herbal tea combinations. Ageratum Conyzoides leaf tea C0Rh had the lowest protein content (12.01 g/100 g DM) compared to Annona muricata leaf tea C100Rh (25.07 g/100 g DM) and the combinations C75Rh, C50Rh, C25Rh of 17.65 g/100 g; 17.30 g/100 g and 16.42 g/100 g DM respectively. A significant difference (p< 0.05) was also observed between the lipid content of the different combinations. Ageratum Conyzoides leaf tea C0Rh had the highest lipid content (22.41 g/100 g DM) compared to Annona muricata leaf tea C100Rh (21.57 g/100g DM). Of the three combinations, the lipid content of the C50Rh herbal tea combination was the highest (22.42 g/100g DM) followed by the C75Rh and C25Rh formula. Ageratum Conyzoides leaf tea C0Rh had the lowest soluble carbohydrate content 0.23 g/100 g DM, followed by C75Rh, C100Rh, C25Rhand C50Rh.
Table 1: Protein, lipid, and soluble carbohydrate contents (g/100g DM) of herbal tea formulations based on Ageratum Conyzoides and Annona muricata leaves.
Note: Means assigned with different letters in the same rows are significantly different (p<0.05). C100Rh: 100% Annona muricata leaf powder; C75Rh: 75% Annona muricata leaf powder and 25% Ageratum conyzoides leaf powder; C50Rh: 50% Annona muricata leaf powder and 50% Ageratum conyzoides leaf powder; C25Rh: 25% Annona muricata leaf powder and 75% Ageratum conyzoides leaf powder; C0Rh: 100% Ageratum conyzoides leaf powder.
The protein content of A. muricata in the present study was approximately equal to 25 ± 0.06 g/100g DM, same value obtained by Usunobun and al. (2012) [26] in Nigeria; higher than 24.3 ± 0.1 g/100g DM and 15.74 ± 1.01 g/100g DM obtained by Rosemary and al. (2017) [27] and Ogbonna and al. (2019) [28] respectively. The protein content of A. conyzoides was lower than 14.73 g/100g DM and 15.67 g/100g DM respectively obtained by Agbafor and al. (2015) [29] and Agunbiande and al. (2012) [30]. These differences could be explained by various parameters such as the age of the plant before harvesting, the application of chemical or natural fertilizers on the harvesting land, the nature of the soil [31], and the different treatments carried out on the plant material such as drying. The combination of 75% A. muricata and 25% A. conyzoides tea had the highest protein content after the 100% A. muricata formula at 17.65 g/100 g DM. According to the Agence Nationale de Sécurité Sanitaire de l’Alimentation de l’Environnement et du Travail (ANSES) the average daily protein intake of a woman is 0.9 g/kg body weight. This means that a woman weighing 60 kg should have a protein intake of 54 g per day. The average protein content of 100 g of herbal tea dry matter (average of the five contents obtained) is 17.69 g/100g. Therefore, consumption of 100g of herbal tea per day provides 5.08 g of protein, thereby contributing approximately 10% of the protein RDA for a 60 kg woman. The protein intake of the tea (depending on the quantity) can be subtracted from the food intake. A high protein intake can lead to a rapid proliferation of tumour cells due to the stimulation of growth hormone (GH), which itself promotes the synthesis of IGF 1, another factor in the proliferation of tumour cells [32]. A lipid-rich diet has a higher energy density than one rich in other macronutrients. The role of lipids has been discussed in the development of overweight and obesity. When fatty acids are involved in energy production, the polyunsaturated fatty acids are oxidised, leaving the saturated fatty acids to accumulate in adipose tissue, where they trigger abundant oestrogen production [32].
As breast cancer prevention is a major public health objective, the quantification of lipids in our herbal tea samples was of paramount importance. The lipid content of A. muricata C100Rh tea (21.57 g/100g DM) was slightly higher than 21.22 ± 1.01 g/100 g DM obtained by Usunobun et al. (2015) [33] in Nigeria. That of A. conyzoides C0Rh tea (22.41 g/100g DM) was significantly higher than 5.67 g/100 g DM obtained by Agubiande, et al. (2012) [30]. The combination of 75% A. muricata and 25% A. conyzoides C75Rh had an average lipid content of 21.13 g/100 g DM. ANSES recommends an average daily lipid intake of 1 g/kg body weight for a woman. This means that a 60 kg woman should consume 60 g of fat per day. The average fat content of 100g dry mass is 21.63g, contributing 36% of a 60kg woman’s requirement. The fat intake from the tea (depending on the amount) can be subtracted from the food intake as too much fat can lead to increased fatty tissue in the body which is a source of abundant oestrogen production and thus increases the risk of developing cancer of the primary oestrogen targets [34]. Carbohydrates, when consumed in large quantities and in absence of balanced caloric expenditure, can be considered as risk factors for several diseases such as cancer. The combination of 50% A. muricata and 50% A. conyzoides (C50Rh) showed the highest soluble carbohydrate content 0.63g/100g DM followed by the combination of 25% A. muricata and 75% A. conyzoides (C75Rh) 0.61g/100g DM which is not very advantageous in this case. The soluble carbohydrate content of the combination of 75% A. muricata and 25% A. conyzoides (C75Rh) was 0.33g/100g DM, which would be an advantage for the management of people at risk.
Mineral Contents (Na, Ca, K, Mg)
Table 2 shows the mineral (Na, K, Mg and Ca) content of the herbal tea formulations based on Ageratum conyzoides and Annona muricata leaf powder. Minerals have various roles in cell proliferation. Of the three intermediate combinations, the tea combination with 75% Annona muricata and 25% Ageratum conyzoides (C75Rh) had the highest Na content (63.03 mg/100 g DM), followed by C50Rh (56.53 mg/100g DM) and C25Rh (48.46 mg/100g DM). This C75Rh combination also had the highest K content (467.09 mg/100 g DM). Sodium is frequently ingested in food in the form of naturally occurring sodium chloride (table salt). It is stimulated by growth factors and ensures the alkalinisation of the intracellular environment, a process essential for the activation of DNA synthesis and thus the initiation of the mitotic cycle. Potassium is nutritionally important for pH regulation and the proper functioning of carbohydrate and protein metabolism. Most people with cancer generally have too much sodium, not enough potassium, and a pH of 4, which leads to tissue damage and weakening of organs [35]. The potassium content of the tea would regulate the pH of the body by filling the potassium deficiency in people at risk. The combination of 75% Annona muricata and 25% Ageratum conyzoides herbal tea had the lowest calcium content of 18.19 mg/100 g DM; calcium is known to be a macro element required for hormone release [36]. Hypercalcaemia would lead to the deposition of calcium salts in the ducts of the breast, exposing the woman to precancerous connections [37].
Table 2: Content of mineral elements (Na, K, Mg and Ca) (mg/100g DM).
Note: Means assigned with different letters in the same rows are significantly different (p<0.05). C100Rh: 100% Annona muricata leaf powder; C75Rh: 75% Annona muricata leaf powder and 25% Ageratum conyzoides leaf powder; C50Rh: 50% Annona muricata leaf powder and 50% Ageratum conyzoides leaf powder; C25Rh: 25% Annona muricata leaf powder and 75% Ageratum conyzoides leaf powder; C0Rh: 100% Ageratum conyzoides leaf powder.
This low Ca content would be an asset as it would solve the problems of mammary calcifications, since high concentrations of calcium salts puts the individual at risk of developing benign tumours. The Magnesium content of the combination of Annona muricata and Ageratum Conyzoides herbal tea was 27.53 mg/100 g. Magnesium is a mineral required in hormone metabolism. It is also important for the release and action of insulin [38]. The higher the amount of magnesium in women at increased risk of cancer, the more it will lead to hyperinsulinemia, a factor that promotes the development of cancerous disease. According to WHO, the recommended daily intake of sodium is not more than 2000 mg/day [39]. Consumption of 100 g of C75Rh herbal tea meets 3.15% of the daily sodium requirement. For potassium, the European Food Safety Authority (EFSA) recommends an intake of 3500 mg/day for adult women (EFSA, 2016). C75Rh herbal tea meets 13.34% of the daily potassium requirement. The intake of potassium will promote the proper functioning of carbohydrate and protein metabolism. As for magnesium, the recommended intake for adults is 6 mg/kg/day [40] and the lowest magnesium content was that of the C25Rh formulation (4.87mg/100g DM). Finally, for calcium, the recommended nutritional intake for adults is 900 mg, for women over 55 and the elderly the requirement is 1200 mg/day. The highest calcium content was found in C50Rh (570.56 mg/100g DM) and the lowest in C75Rh (18.19 mg/100g DM). Calcium is known to be a macro element necessary for the release of hormones. The higher its content in the body, the more calcium salts will be deposited in the ducts of the breast exposing the woman to precancerous connections, the C75Rh formulation with a content of 18.19 mg/100g DM would be an asset for women at risk.
Conclusion
The objective of this study was to study the nutritional profile of herbal teas made from leaf powder of Annona muricata and Ageratum Conyzoides leaves combined in various proportions for the treatment of atypical hyperplasia. It was found that of the five combinations, the one with 75% Annona muricata and 25% Ageratum Conyzoides presented a better nutritional profile because of its low nutrient content (proteins and carbohydrates) and medium mineral content (Na, K and Ca). These results suggest a real asset for the dietary management of young women at risk of developing breast cancer or not. Furthermore, due to the high content of phenolic compounds in the C75Rh combination, its antiproliferative activity on mammary precancerous lesions induced in Wistar rats was studied and it showed an inhibitory effect on the disordered proliferation of mammary gland cells. As this work is in the process of being published, there are questions about the nature of the bioactive compounds present in the tea and mainly responsible for its antiproliferative activity.
Acknowledgments
The authors are thankful to all those who contributed to this work. Special thanks to Pr. Fokom Raymond, Mr. Jean Pierre and Mr. Jean Paul for the supply of some reagents.
Conflict of Interest
The authors declare no conflicts of interest for this study.
Data Availability
The datas analyzed during the current study are available from the corresponding author upon reasonable request.
Author’s Contribution
Fokou Elie, Mbacham Wilfred and Mercy Tah-Monunde conceived the study, edited and reviewed the manuscript; Mono Anne Sophie prepared the proposal and conducted laboratory analysis under the guidance of Djouhou Michelle and drafted the manuscript. Djouhou Michelle and Maptououm Laure were involved in data analysis and reviewing of the manuscript. All authors read and approved the final manuscript.