Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
The scientific results in Medical Education reveal the improvement in professional performance [1]. Ostgraduate education in the education system guarantees the permanent improvement of graduates’ college students Several training and development processes can concur in it, among which are: teaching-learning process (PEA), specialization, research, innovation, articulated in a relevant educational proposal [2]. Postgraduate education enables social development through continuous processes of creation, dissemination, transfers, adaptation and application of knowledge. Sustainable development through the training of professionals is closely linked with the practice that meets the demands of improvement with the in order to meet new challenges. The master’s degree is one of the ways of overcoming the academic postgraduate course that prioritizes the processes of productivity-focused learning. It aims to achieve a broad scientific culture in certain area of knowledge, greater capacity and development for teaching activity. in correspondence with the needs of production, services, economic, social, scientific, technological and culture of the country [1].
Health Technologies is a branch that contributes decisively to the solution of the problem health disease of Medical and Health Sciences. The technologist in the area in which he works has not received a continuous improvement that links this professional with the technological procedures, the technologies biomedical adjusted to the quality requirements that guarantee the epidemiological, clinical and social approach [3]. The results achieved in the area of technology are not at the desired level. They must provide a practical solution identified in the area in which they work. For this reason, the authors’ commitment to This publication is to define the scientific results of the training process of the master’s degrees in Information Technology Health.
Developing
The scientific results are the contributions that constitute products of the investigative activity. In them they have used scientific procedures and methods that allow solving problems of practice or theory. In general terms, world science is led by the great industrial powers such as: USA, Japan, UK and Germany. These countries are the largest producers of knowledge and scientific results [4]. In Latin America, they are dominated by large countries Brazil, Argentina and Mexico. The other countries in the region they barely contribute a small percentage of these results with international visibility. In general terms [5,6].
Latin America has Very Few Scientific Results in Relation to the World
In Cuba, the Science, Technology and Environment System is governed by the Ministry of Science, Technology and Environment (CITMA), in accordance with the methodological documents for the organization of science and technological innovation in the universities of the MES, 2017-2021. whose implementation consolidated scientific activity aimed at achieving scientific results linked to productivity and services [7,8]. The (CITMA), has worked, especially to fill the gap between knowledge and action. The scientific results in the health sector benefit population groups. The System of Sciences and Innovation Technology for Health (SCITS) is unique, it conceives the interdependence between teaching, services and research. As far as researchers have been able to systematize, the (CITMA) defines scientific results, it is the one that meets the requirements to be considered applicable. Features such as: novelty and contribution to the development of an activity, process or sphere of human knowledge that is supported by the technical commissions of experts constituted for this purpose [8].
Several authors have referred that scientific results are finished and measurable products. What do they contribute to from the material, human and available resources and the use of methods, techniques and procedures scientists. They achieve the specific objectives and contribute accordingly to the solution of the problem [6]. In the pedagogical area, the scientific result is the contribution to the solution of a research problem educational. Achieves from the available human resources the use of methods, techniques and procedures scientists to fulfill the objectives set and transform pedagogical practice or theory. The authors agree that the scientific results can constitute theoretical or practical contributions and should be meet certain requirements [9].
• Hat they are feasible: Real possibility of the use and of the resources that it requires; applicable clearly enough for implementation by others; generalizable, due to the condition of applicability and feasibility; that is valid: the result when it allows the achievement of the objectives for which it was conceived; clarity in the exposition, logic, coherence in the language used; rigor, the search for information, procedure and critical assessment; relevance, due to the social value and the needs to which it responds; novelty and originality. It reflects the creation of something that did not exist. Lazo M A, states that scientific results are “the product of a scientific activity, designed, planned and developed based on a social good, based on the use of scientific procedures, [10] directed to the search of solutions to the problems of the social historical practice”. Mastery is a scientific result “(…) the product of an activity in which they have been used scientific procedures, which allow us to offer a solution to something, is reflected in recommendations, descriptions, publications, containing scientific knowledge or material concrete production, or their combination and [9,10].
They solve a certain economic and social need. De Armas N, defined scientific results “(…) the contributions that constitute products of the activity investigation in which scientific procedures and methods have been used that allow to solve problems of practice or theory and that materialize in systems of knowledge about the essence of eleven object or its behavior in practice Travieso N, points out that the scientific results “(…) constitute products of the investigative activity in the which scientific procedures and methods have been used that allow solving problems of practice or [11] of theory and materialize in systems of knowledge about the essence of the object In this regard, they consider that in order to achieve a better understanding and application of scientific results, it must take into account that classification that divides them according to the aspect of reality that it transforms.
The theory or practice, although when the research is done the results are neither theoretical nor practical. They should be presented in a balanced way. The results express the achievements of the project, to what extent they reach the proposed objective. Must be concrete, measurable qualitatively and quantitatively. Related to indicators that verify it. I know verified through the presentation of publications of various types, presentations at scientific events, patents or registrations, prototypes, models, technologies, procedures or manuals. [11-14]. They also allow enriching, modifying or perfecting scientific theory. They provide knowledge about the object, the methods of science research, which can be classified into systems of knowledge and methodological on the other hand, the practical results have an instrumental character to transform the functioning of the object in reality making it more efficient, productive and viable.
They reach essential elements that characterize the effects and requirements that can be considered for determine the contributions in the practical theoretical plane of an investigation. It is used to provide pathways in the improvement of professional performance in the PEA. Show points of view, reflect on the eleven logical and methodological procedures underlying the construction of the proposal on the systematization carried out, the author identified the following regularities in the definitions of results scientists: finished and measurable products; scientific methods, techniques and procedures; problem solution; recommendations, descriptions; They solve certain economic and social needs. The application of results in the graduates of Health Technologies, for the improvement of the professional performance in the care areas where they provide services.
Allows to define the scientific result from the Sciences of Medical Education. The main author operationally defines scientific results from the Sciences of Medical Education and in particular the Health Technologies, product of the research process, which provides the solution of a scientific problem, which allows to identify, apply, process, make decisions for socialization and generalization of the results. It helps to transform reality.
Conclusion
The scientific results of the training process of the master’s degrees in Health Technology were defined, which enrich the epistemic bases of technologies as a branch of Medical Education, a science still in construction.
Experience of Laparoscopic Duodenum Preserving Pancreatic Head Resection
Case Report
Pancreaticoduodenectomy (PD) or pylorus preserving pancreaticoduodenectomy (PPPD)in the past was seen as a placeholder disease of traditional operation scheme of head of pancreas retrospectively. With the development of medicine, there are more and better surgical options. In 1972, Beger et al. proposed duodenum preserving pancreatic head resection (DPPHR)in the treatment of chronic pancreatitis [1], which has become one of the surgical options for benign or partial low-grade malignant tumors in the head of the pancreas. In the era of rapid development of laparoscopic technology, laparoscopic duodenum preserving pancreatic head resection(LDPPHR)was poorly reported due to its difficult operation. The department of hepatobiliary Surgery in our hospital successfully performed 1 case of this operation in March 2021. The relevant data are summarized as follows.
Clinical Data
A 37-year-old female patient was admitted to the hospital due to pancreatic head occupation. The patient had no jaundice before surgery, and no abnormalities in tumor markers CA19-9, CEA and CA125 were observed. Color ultrasound suggested slightly high echoic nodules in the pancreatic head area, which was considered to be occupied by the pancreatic head. CT showed: irregular mixed low-density shadow was observed on plain scan of the head of the pancreas, with an unclear boundary of about 3.1cm×2.8cm. The degree of enhancement of enhanced scan was lower than that of surrounding normal pancreas parenchyma, so more consideration was given to occupying space see (Figure 1). Magnetic resonance examination revealed space occupation at the head and neck junction of the pancreas see (Figure 2). After informing the patient and his family of the condition and treatment options, the patient signed and agreed to undergo laparoscopic duodenal and pancreatic head resection.
Figure 1.
Figure 2.
Sugure
Patients were placed in supine position, and towels were disinfected after anesthesia took effect. An incision was made at the upper margin of the umbilicus with a length of about 5.0cm and an incision of about 1.0cm at 2.0cm below the costal edge of the right side. The laparoscopic poke card poked holes into the abdomen in turn. Conventional abdominal exploration showed no tumor metastasis, and ultrasound scalpel was used to hit the aperitif colon ligament to expose the pancreas. There is a 3.0cm diameter mass at the neck of the pancreas near the head of the pancreas. The retropancreatic tunnel was opened above the portal vein, the Kocher incision was opened, and the branch vessels were ligated with a ligature pin clamp. The medial margin of the duodenum should be preserved at 0.5~1.0cm when the pancreatic neck is transected. The inferior pancreaticoduodenal artery and the first jejunal artery should be protected to prevent ischemia of the horizontal part of the duodenum. Ultrasound knife was used to transection the pancreas near the caudal side of the pancreatic body from the tumor, turn the pancreas to the cephalic side, and gradually strip the pancreas from the posterior peritoneum to preserve the posterior arterial arch on the dorsal membrane of the pancreas, so as to prevent the common bile duct and ampulla Vater from ischemia.
The branch vessels near the head of the pancreas and the main pancreatic duct of the head of the pancreas were ligated with a laparoscopic clamp, absorbable ligature clamp and a series of intracavitary clamps. Pancreatic tumor was resected and duodenal-preserving pancreatic head resection was performed. The intraoperative frozen pathological examination after family members’ examination suggested that the pancreatic head tumor was benign, and the tumor was paraffin waxed. Checking that no overflow, pancreatic juice, bile and intestinal juice under the common bile duct segment and duodenum without damage, about 15.0cm from the distal flexor tendon using electric nail straight cutting anastomat and warehouse transection of cavity mirrors jejunum, using ultrasonic knife in pancreatic body mesocolon line a diameter of about 3.0cm incision, pull distal jejunum to pancreatic tail section, looking for the pancreatic duct, A pancreatic duct drainage tube was placed in the distal main pancreatic duct, and an incision with a diameter of 0.5cm was made about 2.0cm away from the broken end of the distal jejunum. Adenotubulojejunostomy was performed with absorbable surgical sutures, and no bleeding, pancreatic leakage or intestinal leakage was detected. Jejune-jejunal anastomosis was performed at about 60cm from the pancreatic duct jejunal anastomosis using linear cutting stapler and nail bin. A drainage tube was placed at the Wentschner’s foramina and the pancreaticointestinal anastomosis, and the abdomen was closed layer by layer after checking the correct instruments and dressings.
Result
The operation duration was 290 minutes, the intraoperative blood loss was 50ml, and no blood transfusion was performed. Postoperative pathological report :(immunohistochemical results of pancreatic head tumor were microcystic serous cystadenoma). No serious complications such as hemorrhage, pancreatic leakage, biliary leakage, duodenal fistula, and common bile duct stenosis were found after operation.
Discussion
DPPHR is an important surgical procedure in the treatment of benign or partial low-grade malignant masses on the head of pancreas, with the premise of preserving the integrity of digestive tract and improving the prognosis and quality of life of patients. Therefore, a variety of improved procedures have been developed, such as Frey surgery, Beme surgery, Takada surgery, etc [2-4]. In this case, a modified Beger procedure was performed under a single hole. A little pancreatic tissue was retained at the stump of the medial margin of the duodenum, but pancreaticoenterostomy, electrocoagulation and ligation of the main pancreatic duct were not performed here [5]. LDPPHR is another advance of DPPHR. Indications of DPPHR:
1. Chronic pancreatitis and its resulting mass type on the head of the pancreas;
2. Pancreatic duct calculi at the head of the pancreas;
3. Benign mass, borderline or low grade malignant mass in the head of pancreas;
4. Pancreatic trauma;
5. Pancreatic mitosis deformity [6-9].
The therapeutic range of LDPPHR is similar to DPPHR. The key and difficulty of LDPPHR surgery is to ensure blood supply of duodenum and bile duct [10]. The anterior and posterior pancreatic duodenal arcs are crucial. Because it is bidirectional blood flow, theoretically retaining either side of the aortic arch can ensure the duodenum and bile duct function. The gastroduodenal artery often gives off the anterior duodenal artery, and the superior mesenteric artery gives off the inferior anterior pancreaticoduodenal artery [11]. The posterior pancreaticoduodenal aortic arch is located on the dorsal side of the head of the pancreas and can be shown by Kocher incision. In Berger method, pancreatic tissue of 0.5~1.0cm at the stump of the medial margin of the duodenum was subtotal resection of the pancreatic head to protect the anterior and posterior aortic arches. It is important to maintain the integrity of the posterior pancreatic fascia during operation. Although Kocher incision risks damage to the posterior aortic arch, it is suitable for surgical exploration and identification of the posterior pancreaticoduodenal aortic arch [12]. It is up to the surgeon to cut Kocher. In this operation, Kocher was opened without injury to the posterior pancreaticoduodenal arch. Advantages of LDPPHR surgery: safe and feasible, minimally invasive surgery with clear vision and fast recovery; The intact duodenum makes the physiological function of digestive tract unimpaired.
The tail of the pancreatic body and the intestine-pancreatic axis exist, and insulin secretion and blood glucose regulation are not infringed [13]. The surgical team should have rich knowledge of endoscopic anatomy theory and be skilled in operating endoscopic instruments. In conclusion, LDPPHR surgical resection scope is small, small trauma, although the operation is difficult, but patients benefit a lot. It is believed that with the continuous efforts of hepatobiliary surgeons, the operation of LDPPHR will become more skilled and more patients will benefit.
Carbon Dots as Antimicrobial and Antiviral Nanomaterials and Drug Delivery Applications
Introduction
Carbon Dots
CDs a novel class of carbon nanomaterials discovered in 2004 have gained considerable attention due to certain specific characteristics: excellent photoluminescence, high quantum yield (QY), low toxicity, biocompatibility, small size, chemical stability, and inexpensive and easy synthesis [1,2]. The size of CDs is less than 10 nm, made of carbon, an element abundant and generally nontoxic. CDs are particularly attractive in many applications such as bioimaging, biosensing, and nanocarriers for drug delivery [3] (Figure 1). CDs are mainly classified according to their different formation mechanism, surface functional groups, and properties: carbon quantum dots (CQDs), graphene quantum dots (GQDs), carbon nanodots (CNDs), and carbonized polymer dots (CPDs). In addition, associations can be built among them by changing the carbonization degree and graphene layer (4).
Structure and Properties
Carbon dots have been characterized to analyze their physic properties and to understand the mechanisms associated with their properties. Common techniques are transmission electron microscopy (TEM) to obtain morphology, size, and agglomeration by demonstrating that they are very small of approximately <10 nm and quasi-spherical form, Fourier-transform infrared spectroscopy (FTIR) to identify specific functional groups, X-ray diffraction for the evaluation of the crystalline nature of CDs. It is also known that CDs are usually the product of the carbonization of organic precursors, mainly consisting of sp2 /sp3 -hybrid carbon or sp2 -domains embedded in amorphous carbon [5,6]. They also have several functional groups on their surface such as carbonyl, carboxylic and hydroxyl groups, which provide a rich part in oxygen and favor it to be soluble in water, in this way it can be useful in a wide variety of applications [7]. Carbon dots offer the flexibility to be able to manipulate both their structure and their properties depending on what type of carbon and organic molecules are made [8]. CDs have great properties such as 1) Optical absorption depending on the method of synthesis, 2) Excitation-dependent photoluminescence. The fact that the emission color of the CDs can be adjusted according to the excitation wavelength makes it very attractive for various applications. 3) Photo induced electron transfer, 4) Electrochemoluminescence, 5) Proton adsorption and 6) Low toxicity [3,9].
Figure 1: Biomedical applications of Carbon Dots.
Synthesis of Carbon Dots
According to the strategies, there are two types of synthesis ‘‘top-down’’ and ‘‘bottom-up’’ [10]. The top-down approaches include arc discharge, acidic exfoliation, laser ablation electrochemical oxidation, and microwave-assisted hydrothermal synthesis, where CDs formed from a larger carbon structure. This advantage is abundant raw materials, large-scale production, and simple operation [7]. The obtained CDs generally present graphite-like structures with weak fluorescence luminescence is a synthetic process and requires complex steps [11]. In the bottom-up synthesis, it has been used small molecules carbonized as precursors for example citric acid. This technique is efficient to produce fluorescent CDs. It has been produced under simple and mild conditions through microwave or hydrothermal reactions [12].
CDs Antimicrobial Activity
One of the biggest public health problems that fear is antibiotic resistance. This is due to the abuse of antibiotics, which has allowed new mechanisms of Resistance to be generated that is why new strategies are needed that are fast, easy to produce, affordable. These strategies include Carbon dots since it has been reported to have antimicrobial activity, due to its photosensitizer properties to produce oxidative stress by ROS and attack a wide range of microbes in the following ways: with physical or mechanical damage to the cell wall, disrupting the EPS matrix, causing biofilm splitting, inhibiting growth and even killing [13] Heteroatoms in carbon dots enhance the generation of ROS due to extra free electron incorporation in carbon dots. The functional characteristics of Carbon dots depend strictly on the precursors from which they are made, solvents that are used, as well as the functional groups of their surface. It has been shown that depending on the load of the carbon dot interacts or not with the bacteria. Something more interesting is that when preparing the CDs they can incorporate heteroatoms; they are called doped CDs, to make their activity more powerful [14]. Another strategy is to combine CDs with antimicrobial agents for example sodium hypochlorite (NaOCl), hydrogen peroxide (H2O2) to reach the maximum antimicrobial effect [15].
CDs Antiviral Activity
Viral diseases continue affecting millions of people around the world causing serious problems, many alternatives have been proposed to try to avoid them, and one of the strategies is CDs based on different carbon sources and synthesis methods, which can bind to viral proteins to stop multiplication or blocking the entry of the virus into the cell. The studies that exist are very recent but this activity has already been demonstrated with CDs from different methods and precursors, for example, curcumin carbon dots to prevent the entering and replication of coronavirus, benzocaine carbon dots to prevent the attachatchment of dengue, and zika virus, carbon dots to inhibit the binding of human norovirus, glyzhyrric acid carbon dots to inhibit the replication of herpes virus, boronic acid functionalized carbon dots to prevent entry step of human immunodeficiency virus 1, etc. The action of the CDs depends on the size, Surface, and load [16,17]. Lin et al., 2019 have suggested that C-dots can act at different levels of infection [18]. Actually, with the SARS-COV2 coronavirus pandemic in which there are no drugs to completely cure, CDs have been proposed as alternatives to stop the infection inside people’s bodies or detect it [16]. In a study conducted by Lai-Di Xu et al 2021, they used a new lateral flow immunochromatography technology in which they used red emission-enhanced CDs based-silica spheres as signals to detect SARS-COV2. In addition, the incorporation of the desired functional groups with QDs could effectively interact with the virus input receptors and affect genomic replication [19].
There are already some analyses that suggest that the cationic surface charges of CQDs interact with the negative RNA chain of the virus-producing reactive oxygen species within SARS-COV2. Also incorporating some specific functional groups to these CQDs would interact with the virus receptors and thus inhibit replication. One of the areas of opportunity to attack the SARS-COV2 virus is to look for alternatives to make CDs more efficient, perhaps using natural compounds to make them such as curcumin [20]. In general, we are facing a new field of research because although it has been shown that CDs have antiviral activity, many of these are in vitro and in vivo there are few so it is necessary to do more to understand the mechanism of action and know the real potential of these.
Conclusion
CDs have emerged as a new type of Nano carrier, breaking down barriers of production methodologies using carbon abundant raw materials and have begun to take an important place as nanomaterials with great potential for applications in the field of biomedicine. The antimicrobial and antiviral properties of CDs give them a promising future as new nano-drugs against resistant and emerging pathogens.
A Case of Thoracic Disc Herniation Effectively Treated with Interventional Radiology Computed Tomography- Guided Percutaneous Endoscopic Radiofrequency Annuloplasty Using a Disc-Fx®
Introduction
In 1972, Hijikata et al. established percutaneous discectomy (PD), which is a procedure aiming at symptom relief for disc herniation through a reduction in nerve root irritation associated with a decrease in intervertebral disc pressure [1,2]. Furthermore, herniation reduction is achieved through secondary cicatricial contraction of the intervertebral discs. PD has subsequently been modified to be a safer, noninvasive procedure, and has been applied in various forms, such as with the use of laser, including the Disc- Fx®. The Disc-Fx® facilitates nucleus pulposus transpiration or fiber ring thermocoagulation in addition to conventional nucleus pulposus extenteration using forceps (Hijikata’s procedure) [3-5]. In this study, we report a patient for whom Interventional Radiology- Computed Tomography (IVR-CT)-guided Percutaneous Endoscopic Radiofrequency Annuloplasty (PERA) was performed for the thoracic disc herniation to reduce the incidence of complications and improve treatment results, leading to a favorable outcome [6].
Case Report
The patient was a 34-year-old man (height: 167cm; weight: 74.4 kg), with a chief complaint of lightning pain in the right flank. He had no significant medical history. The patient consulted the Department of Anesthesia of another hospital with bilateral dorsal lower back pain, which had persisted for 1 year, and was treated with medication for 5 months. However, he stopped consulting the outpatient clinic due to symptom relief. 6 days before visiting our hospital, he again experienced lightning pain in the right flank appeared. 3 days before visiting our hospital, he consulted the Emergency Outpatient Unit of another hospital owing to exacerbation of the pain. Under a tentative diagnosis of ureteral calculi, an anti-inflammatory analgesic agent (diclofenac sodium suppository) was prescribed 2 days before visiting our hospital, he consulted the same hospital again, because there was no symptom relief. The presence of ureteral calculi was ruled out based on abdominal CT data. He was admitted with severe pain, and detailed examination and treatment were started. However, the presence of a disease in the field of internal medicine was ruled out. 1 day before visiting our hospital, he was discharged based on his wishes to consult another hospital. Although he consulted another local clinic, a definitive diagnosis could not be made. Next day, he consulted the outpatient clinic of our department. Physical examination on admission showed tenderness at the Th9 to 12 level.
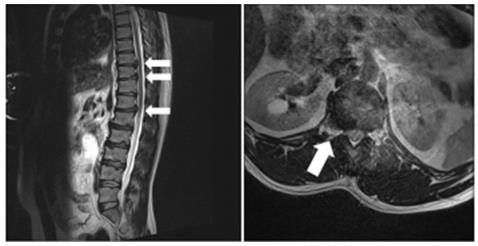
Figure 1: a. MRI of the thoracic/lumbar vertebrae displayed multiple disc herniation involving the thoracic vertebrae to thoracolumbar junction (Th9/10, Th10/11, and Th12/L1). (arrows) b. Coronal section of Th12/L1 showed a disc herniation (arrow).
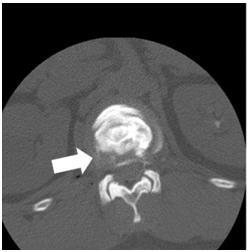
Figure 2: CT-discography led to a definitive diagnosis of lateral disc herniation at the Th12/L1 level (arrow).
In particular, there was marked pain at the Th12 level, and allodynia was noted at the site of the pain. Hematological analyses did not demonstrate any abnormalities. The Numerical Rating Scale (NRS) score was 10/10, and the Self-rating Depression Scale (SDS) score was 41. The EuroQol-5 Dimension (EQ-5D) score was -0.594. X-ray of the thoracic/lumbar vertebrae displayed osteophyte formation, leading to a diagnosis of thoracic spondylosis deformans. Magnetic Resonance Imaging (MRI) of the thoracic/ lumbar vertebrae displayed multiple disc herniation involving the thoracic vertebrae to thoracolumbar junction (Th9/10, Th10/11, and Th12/L1), suggesting thoracic disc herniation as an etiological factor for lightning pain of the right flank (Figure 1). Outpatient treatment was started. Intercostal nerve (right Th10, 11, and 12)/epidural (Th12/L1) blockade was performed, but there was no improvement. Blockade of the right Th12 nerve root was conducted under fluoroscopy, but the pain remained, with an NRS score of 5/10. Subsequently, during CT-discography, the patient felt irradiating pain which was consistent with the pain he felt constantly. CT-discography led to a definitive diagnosis of lateral disc herniation at the Th12/L1 level (Figure 2). Therefore, IVR-CTguided PERA with a Disc-Fx® that features a patented navigational device with bipolar system which was specifically designed to access and treat the diseased portion of the disc was scheduled.
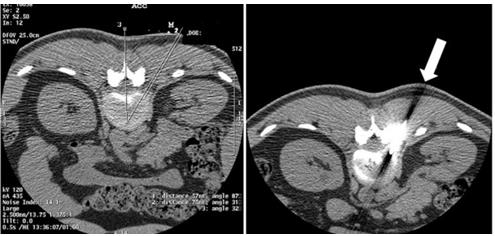
Under IVR-CT guidance, the point and route of insertion were determined, and a Disc-Fx® was inserted through an area 5 cm right to the spinous process at the Th12/L1 level to approach the intervertebral disc (Figure 3). Direct PD involving the herniated site was performed to treat the lateral herniation, and nucleus pulposus extenteration and thermocoagulation were conducted by DiscFx®. There were no complications, such as pneumothorax thoracic spinal nerve root injury and haemorrhage. After treatment, the NRS score was reduced to 1-2/10. Subsequently, follow-up was conducted by trigger point injection and drug therapy. 1 year after treatment, although there was a pain (NRS score was 2-3/10), there was no acute exacerbation of symptoms. The symptoms were calm, so it was decided to follow up at the clinic around the house, depending on the wishes of the patient.
Figure 3: a. Under IVR-CT guidance, the point and /route of insertion were determined. b. A Disc-Fx® was inserted through an area 5 cm right to the spinous process at the Th12/L1 level to directly treat the lateral herniation (arrow).
Discussion
PD is an intermediate treatment procedure between surgical and conservative therapies, which was proposed by Hijikata in 1972 [1]. It reduces pain by decreasing the intervertebral disc pressure and reducing stimulation-associated nerve root pressure, degeneration of the disc, and cicatricial contraction of the disc. Advantages of PD include low-level invasiveness, a low incidence of postoperative complications, and shortening of the admission period. Treatment as an outpatient is possible. As complications, persistent inflammation of the nerve root and intervertebral arthrosis associated with a decrease in the intervertebral space have been reported. Several studies indicated the efficacy of PD combined with epidural/nerve root/intervertebral joint blocking for persistent inflammation of the nerve root [7]. Recently, PD has been improved to become safer and less invasive, and various techniques, including the use of laser, have been applied. As one such technique, the Disc-Fx® was developed. This technique uses Trigger-Flex® and Surgi-Max® for nucleus pulposus transpiration by percutaneous high-frequency intervertebral disc decompression or fiber ring thermocoagulation in the process of intra-disc highfrequency thermocoagulation in addition to conventional nucleus pulposus extenteration with forceps (Hijikata’s procedure) [3,4,8]. In addition, this device facilitates the examination of the intra-disc nucleus pulposus and fiber ring under an endoscope.
Thoracic disc herniation is rare compared with cervical/lumbar disc herniation, accounting for 0.25% to 1.00% of all patients with disc herniation [8]. Symptoms of thoracic disc herniation vary, and include: dorsal chest pain, girdle pain, dysesthesia of the lower limbs (numbness, weakness), and myelopathy; therefore, an accurated diagnosis is difficult. In addition, treatment methods vary from conservative therapy to surgery. As this disease is rare, few studies have reported the results of treatment, and a consensus regarding treatment has not been reached. The present case was characterized by thoracic disc herniation and lateral herniation, which are rare. Therefore it was difficult to make a diagnosis. MRI of the thoracic/lumbar vertebrae, discography, and CT-discography led to a definitive diagnosis. The intervertebral foramens of the thoracic vertebrae are narrower than those of the lumbar vertebrae, and the lungs are present in the lateral regions; therefore, when performing PD for thoracic disc herniation, the risk of pneumothorax must be considered [9]. To reduce the risk of complications, we performed IVR-CT-guided PERA with a Disc-Fx®, although there are still few reports on this procedure. The point and route of insertion were determined under IVR-CT guidance, facilitating individualdifference- matched fine adjustment. Effective treatment could be administered while reducing the risk of pneumothorax by directly puncturing and extirpating the site of lateral herniation.
In addition, spinal canal operations and intervertebral joint drilling was not required, in contrast with surgical procedures; therefore, it was possible to reduce the risk of complications, such as spinal canal adhesion and thoracic vertebral instability. 1 year after treatment, although there was a pain (NRS score was 2-3/10), because the disc herniation other than lateral disc herniation at the Th12/L1 level remained. However, of course there was no acute exacerbation of symptoms in TH12/L1 level. In conclusion, although the long-term efficacy should be further investigated, the present case suggests that IVR-CT-guided PERA with a Disc-Fx® is useful for treating patients with thoracic disc herniation.
First Twin Live-Birth Deliver After Oocyte Cryopreservation in a Follicular Lymphoma Patient
Introduction
Many young patients diagnosed with lymphoma achieve durable remissions with current treatment strategies and become long-term survivors. However, chemo- and radiotherapy can determine a severe gonadotoxicity and compromise their reproductive potential [1]. Therefore, the demand for fertility preservation has greatly increased during the last decades and the matter is particularly challenging when female patients are concerned [2,3]. Oocyte freezing and thawing proved to be an efficient method for fertility preservation [4,5]. Nevertheless, small numbers of successful pregnancies and live births from oocyte cryopreservation have been reported in female cancer survivors, especially in patients with hematological malignancies [6-8]. This is the first report of a follicular lymphoma (FL) patient who carried out a healthy twin pregnancy through fertilization of the oocytes cryopreserved before chemotherapy.
Case Report
A 28-year-old nulliparous woman was diagnosed with non- Hodgkin FL, grade II, stage IIIA, in August 2014. She presented in good clinical conditions, asymptomatic, and objective examination only showed superficial lymphadenopathies, the largest ones measuring about 5 cm in her groin. Before starting hematologic chemo-immunotherapy, the young woman was referred to the fertility preservation specialists at our Institution and, after appropriate counselling regarding the available options, she decided to undergo oocyte cryopreservation. Since the patient’s hematologic condition did not contraindicate a moderate delay in the beginning of chemotherapy, controlled ovarian stimulation was performed: gonadotropins (follitropin α) associated with gonadotropin-releasing hormone agonist, namely leuprolide acetate. After 15 days of gonadotropin stimulation (the patient received a total dose of 1.575 IU), her estrogen level was 1.442 pg/ml and a transvaginal ultrasound showed 17 follicles ≥ 16 mm. Ovulation was triggered with α-chorionic gonadotropin (250 mcg). Fifteen oocytes were retrieved, 12 were cryopreserved through vitrification. No complications as ovarian hyperstimulation syndrome, bleeding or infection occurred after oocyte retrieval.
Ten days later, the patient started her hematologic treatment. She received 6 cycles of CHOP chemotherapy (cyclophosphamide, doxorubicin, vincristine and prednisone) associated with 8 administrations of rituximab, obtaining a complete response which was confirmed after 2 years of maintenance with rituximab.
In May 2015, after the end of chemotherapy, the patient’s menstrual cycle reappeared. She had fruitlessly tried to conceive for approximately 17 months when, in September 2018, she addressed the Infertility and In Vitro Fertilization Unit of our Hospital to research pregnancy with frozen oocytes. Endometrial preparation was performed with emiidrate estradiol patches, 300 mcg/day for 11 days. When the endometrial thickness reached 10 mm, 600 mg/ day of micronized progesterone were added. Four oocytes were thawed; two of them survived and were inseminated through intracytoplasmic sperm injection, resulting in normal fertilization with development of two embryos which were transferred into the uterus on day 2 after insemination. After 14 days the serum level of β-human chorionic gonadotropin was 537 IU/l. Two weeks later, transvaginal ultrasound examination revealed two intrauterine sacs with embryo heart activity. Gestational diabetes mellitus, treated with diet and exercise, was the only medical complication of pregnancy.
At week 36 of gestation, preterm prelabor rupture of membranes occurred. An urgent caesarean section was performed, which resulted in the birth of two healthy males weighing 2690 g and 2610 g, respectively. Uterine atony/postpartum hemorrhage occurred after caesarean section and was treated with Bakri balloon tamponade inserted within the uterine cavity. Patient gave written informed consent to publish her data.
Discussion
The increasingly prolonged survival of young lymphoma patients urges clinicians to focus on minimizing the long-term impact of antineoplastic treatment. An important issue is the potential toxicity of chemo- and radiotherapy on the gonadal function, which can lead young female patients to premature ovarian insufficiency and infertility [1]. Embryo cryopreservation is the most established option among assisted reproductive technologies, resulting in a pregnancy rate of approximately 30% [2]. More recently, oocyte cryopreservation has become a valid alternative for women who do not have a male partner and do not wish to resort to a sperm donor [3-5]. Overall, a small number of live births have been reported from fertilization of thawed oocytes in patients having received cancer therapies, most of them as single case reports or retrospective studies [6-8]. Some authors report that cancer patients tend to have a low ovarian reserve and an inadequate response to stimulation protocols, resulting in inferior numbers of oocytes retrieved when compared to age-matched non-oncologic women [9]. Others indicate that even the type of malignancy can influence the outcome of the procedure, with lymphoma patients showing lower levels of anti-mullerian hormone and needing higher doses of exogenous follicle-stimulating hormone compared to patients with solid tumors [10]. This aspect seems to be related to the high amounts of circulating inflammatory cytokines associated with this type of disease [10].
This topic is actually a matter of debate, since many other studies do not account for any significant difference in ovarian function among these categories of patients [11]. Another difference is that oocytes frozen for oncological reasons tend to face longer storage periods, due to the patient’s need for prolonged treatment; nevertheless, it was demonstrated that time of storage does not affect cryopreserved oocytes in terms of gene expression, provided the freezing is done correctly [12]. In fact, data show that no higher incidence of genetic aberrations or birth defects is associated with the procedure.
Conclusion
The case we described is, to our knowledge, the first twin live birth obtained through fertilization of frozen-thawed oocytes in a woman with a non-Hodgkin FL after first line treatment for the hematological malignancy. With this report, we aim to further stress the importance of oncofertility counseling in young women in need of antineoplastic therapy, in order to minimize the impact of gonadotoxic treatment on their future lives.
Management of Penile Fracture with Urethral Injury in Haiti
Penile fracture is a urological emergency requiring operative management [1,2]. Considered a rare and underreported traumatic injury [3-6], it has a reported incidence ranging from 0.29 to 1.36 per 100,000 people [1] and affects 1/175,000 men in the USA [6]. It is defined as a rupture of the tunica albuginea of the corpus cavernosum and occurs when the penis is erect [1,2,7] Erection causes thinning of the tunica, with its thickens reduced from 2 mm to 0.25-0.5 mm, and it becomes vulnerable to trauma [6]. The main cause of penile fracture is coital trauma, which represents 1/3 of all trauma to the penis. In very rare cases it is accompanied by rupture of the urethra which occurs in 1% to 38% of cases of penile fracture reported globally [1,2,8,9]. Some African studies revealed the main cause is masturbation [10]. Management of penile trauma has evolved over time. Initially, penile fractures were managed conservatively and non-operatively. However, due to the high complication rate observed, emergency surgical management has been the standard of care since 1980, which considerably reduces rates of long-term complications as erectile dysfunction [1,9,11-16]. To our knowledge this is the first described case from Haiti, we present a case of traumatic penile fracture and an associated urethral injury which presented to the emergency department at the State University Hospital of Haiti and managed operatively by the urology service.
Case Presentation
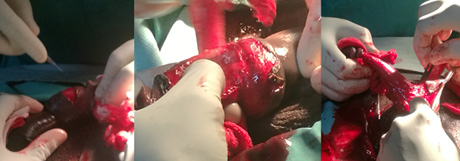
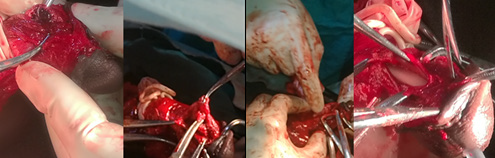
Our patient was a 49-year-old man with no known medical history. He presented to the emergency department with a six hours history of urethrorrhagia and difficulty of retracting the glans. He reported taking sexual stimulants and subsequently engaging in vigorous sexual intercourse during which he heard a sudden cracking noise at the penis after bumping the perineum of his female partner. He reported engaging in vigorous vaginal penetrative sex from the posterior position (i.e., doggy style). After the sound, he passed blood from the meatus, followed by pain and edema in the body of the penis. Given the increasing intensity of the pain and the persistent hemorrhage, the patient decided to come to the Urology Emergency Department. Initial clinical examination was remarkable for a leftward deformity of the penis, most markedly in the distal 1/3 of the organ, edema without apparent ecchymosis (Figure 1), and passage of blood via the urinary meatus. There was difficulty in retracting the glans and pain was most severe at the point of swelling. Examination of the scrotum and perineum was unremarkable. The diagnosis of penile corpora cavernosa fracture was made and the patient was consented and prepared for operative repair. The operation was initiated by the in ligature and section of frenulum artery followed by a circular incision was made through the balanopreputial groove to strip it down to the root (Figure 2). A tourniquet was placed for less than 30 minutes and exploration of the penis was initiated where clots were identified, hematoma was drained and wound was washed with 0.9% serum saline.
Figure 1: Description of the fractured penis with leftward deformation and edema of the penile shaft.
Figure 2: Circular incision and penile stripping.
Exploration of the penis revealed an injury in the corpora cavernosa on the right distal to the urethral meatus approximately 2.5 cm away. This was repaired with Vicryl 0, followed by a sealing test using 0.9% serum saline and removal of the tourniquet (Figure 3). After exploring the corpus cavernosum, we started the exploration of the urethra using a Nelaton catheter 16, which allowed us to identify and evaluate the anterior urethral injury which was approximately 3 cm in length and located at 5 cm from the urinary meatus. We proceeded to dissect the urethra circumferentially, then we proceeded to repair the urethral mucosal injury with (interrupted) Vicryl 4.0 suture over a 16 Fr. Foley catheter. A reassuring erection test with Nacl 0.9% was performed, and then we repaired the albuginea with (interrupted) Vicryl 2.0. Next, a second circular incision 5 cm (distal) from the first one was made, and we proceeded to repair the skin to the mucosa with a (interrupted) chromic 2.0, followed by the repair of the frenulum. At the conclusion of the procedure a sterile dressing was placed and the Foley catheter remained in place. The procedure which lasted approximately 2hr 45 min.
Figure 3: Circular incision and penile stripping.
Discussion
Penile fracture is the traumatic rupture of the albuginea attached to the corpus spongiosum [1,3,17]. This structure has a bi-layer of collagen, which provides a significant tensile force resisting the intracavernous pressure which can rise to1500 mm Hg. This tensile strength is essentially provided by the outer layer of the albuginea, the thickness of which decreases considerably during erection (2 mm to 0.2-1.5 mm) and thus weakens the corpora cavernosa [6,9]. Any situations or evens which elevate the intra-cavernous pressure above 1500 mm Hg are a risk factor for penile fracture due to the rupture of the albuginea and the corpus spongiosum [18]. These situations include the use of oral sexual stimulants and sex under psychological pressure, like extra-marital sex [2,6]. Our patient admitted to having used oral sexual stimulants prior sexual act. Diagnosis of penile fracture is essentially clinical [5,15,16]. The majority of cases involve a history of trauma, especially and more than a third of cases report coitus [1,2,19]. Other causes of trauma can lead to penile fractures, such as a fall from the top of the bed during sleep, direct blunt impact, and penetrating injuries such as that made by projectiles [1,2]. It is uncommon to see penile fracture with concurrent urethral rupture. The prevalence reported varies by region of the world. It is 3% in Asian and African countries, while it is around 38% in Western countries [6,8]. Furthermore, certain sexual positions favor the occurrence of penile fractures with or without rupture of the urethra.
Among these positions, the doggy style position and the position where the woman is on top are the most often described cases [14,20-22]. However, other positions can result in penile fractures as well. The most consistent clinical sign of penile fracture with urethral rupture is hematuria, followed by urethrorrhagia, dysuria, and urinary retention [5,18,23,24]. However, the absence of these signs does not exclude a penile fracture with urethral injury [13,18]. Furthermore, there are the classic signs of penile fracture such as pain, edema, ecchymosis, and the classic “eggplant” deformity [4,5,16,18]. Our patient presented with a similar picture; he had urethrorrhagia, edema, pain and an eggplant deformity. Imaging studies can be used in certain well-determined circumstances, among them sonography and cavernosography, retrograde urethrography, MRI, and cystourethroscopy [15]. These are not recommended in emergencies where the clinical exam is usually sufficient to make the diagnosis and to expedite emergent surgical management [12]. This was the case for our patient who had almost all the clinical signs, and thus we expedited his penile anesthetic block and operative repair. Since 1980, emergency surgery is recommended in all cases of penile fractures. The British Association of Urological Surgeons recommends surgery within the first 24 hours [14] in order to reduce the risk of longterm complications. Bozzini et al. observed a complication rate of 7.6% in patients operated before 24 hours and 68.7% in patients operated 24 hours after injury [12,14].
Our patient underwent the procedure approximately 12 hours after admission. The wound was approached by a coronal suture (Figure 2), the most commonly technique used, which gives better exposure, improved post-operative aesthetics, and facilitates dressing changes [2,9,18]. However, some studies have shown that this approach is associated with risks of infection and necrosis [9]. The rupture of the corpus cavernosum was partial as is the case in the majority of penile fractures [9,12] and measured 2.5 cm, while the urethral wound was mostly anterior and 3 cm in length. Studies have shown that urethral rupture is most common in bilateral fractures [12,14,19] and is often ventrolateral where the tunica albuginea is thinner [14]. Reports recommend the use of urethrography or retrograde cystography in cases of fracture with signs of urethral rupture [12,14,19]. In our case this was not available, so we have used a 16 Fr catheter a very common practice and highly recommended by some researchers and we proceeded to operative exploration with ultimate repair of the albuginea as recommended [4,19] with Vicryl 2.0. . Our patient has had a good clinical outcome. Post-operatively, he was followed for 2 days in the inpatient surgical ward. He received antibiotic coverage with ceftriaxone. After discharge on post-operative day, he was evaluated regularly at 3-day intervals with changes of the petroleum-based dressing and re-application of topical neomycin for the first 15 postoperative days. The patient was instructed not to wet the wound and to continue the neomycin application until complete healing. The foley was removed one month post-operatively, and the patient had satisfactory urinary function. Return to sexual intercourse was advised at 2 months post-operatively.
Conclusion
Any patients presenting with hematuria and/or urethrorrhagia in whom clinical history suggests penile fracture, an evaluation of urethral injury must be performed. The diagnosis is essentially clinical and requires surgical intervention within the first 24 hours after injury. After operative repair, return to sexual activity is recommended after 6-8 weeks. In developing country like Haiti, with limited resources like cystogram or retrograde urethrogram, clinical evaluation and surgical emergency is key to avoid long term complications.
Coronavirus disease (COVID-19) is caused by SARS-CoV, a highly infectious virus that has become a global health challenge since 2020 (Lai, et al. [1]). The virus effects on individual immune can be mild to moderate and severe to some. Immunity is the ability of organisms to protect the body from attacks from particular toxin infections (Yazdanpanah, et al. [2]). The emergence of the SARS-CoV into the human body affects the immunity system. Usually, the body immunity can detect foreign organisms and fight back by releasing antibodies that protect the entry (West, et al. [3]). However, Covid-19 emergence of Covid-19 has led to many research pieces to determine how the immune system and disease correspond. COVID-19 directly or indirectly affects the immune system through the hype inflammatory immune response in patients with underlying conditions. The virus leads to severe Acute Respiratory distress symptoms and organ failure (Abu-Izneid, et al. [4]). SARSCoV- 2 enters the cell through (ACE-2) that is detected by Toll-like receptor 7 (TLR7) (Ahmadpoor [5]). When the Coronavirus attacks the body, the immune system tries to fight through cytokine storms that have adverse effects and even cause death. The presence of two domains that is S1 and S2, in glycoprotein is responsible for attachment, invasion, and entry to the body (Barcena, et al. [6]). The SARS-CoV interacts with the host cell through the ACE2 and another host called protease TMPRSS2 (Davidson, et al. [7]). The interaction of coronavirus and host cells causes the non-structural proteins that utilize the virulence factors Kumar, et al. [8].
The increased rate of enzymes production within the kidneys, liver, and heart in patients suffering from anemia induces an underlying expression of tissues of the ACE2 receptor (Kuppusamy, et al. [9]). The entry mechanism of both SARS-CoV and SARS-CoV2 are almost similar, and the ACE2 receptor binds the glycoprotein with the virus (Yang, et al. [10]). The Toll-Like Receptor-7 senses the interaction and binding responsible for producing inflammatory cytokines (Dyavar, et al. [11]). The secretion of hyper-inflammatory cytokines in various body parts, such as the lungs, causes acute respiratory distress (Lin, et al. [12]). The ACE2 factors are present in some organs, such as the kidneys, the heart cells, epithelial lung cells, and the liver (Deshmukh, et al. [13]). When Coronavirus enters the body, it interferes with multiple receptors that sense the virus, blocking the Ribonucleic acid (RNA). The activation of TLR7 in endosomes secretes alpha-interferon that contributes to the production of antibodies and antigen B specific (Ahmadpoor, et al. [5]). The above action mechanism depends on the adaptive immune response that dominates virus infections and dictates recovery. The effects of Covid-19 on the immune system vary from the individual; some response of antibodies released by white blood cells determines the strength to fight the virus. The human body contains white blood cells that are the key player in maintaining the immune system (da Silveira, et al. [14]). The function of white blood cells is to block entry of harmful toxicity and detect any cell changes because it travels throughout the body in blood cells (Farahinia, et al. [15]).
According to (Wiig [16]) body exchange fluid and cells between the lymphatic and blood vessels to form the lymphatic system. Lymph nodes encounter antigens where foreign organisms, immune cells, and lymphatic vessels enter the nodes (Leong, et al. [17]). The immune cells, foreign antigens, and lymph vessels are transmitted throughout the bloodstream by the blood vessels surveying foreign antigens (Hickey, et al. [18]). The immune cells and the lymphatic vessels then drift back to lymph nodes, where they fight foreign antigens by stimulating antibodies (Chowdhury, et al. [19]). The immune system is ideal for fighting foreign antigens because of its natural body defense mechanism. The entry of the COVID-19 virus slowed down the body’s immunity because the virus is highly inflammatory, and it is the first time it attacks the body; hence, the virus becomes fatal and is likely to cause illness. The effects of the Coronavirus vary from individuals depending on the strength of immunity, the aged, children, and those with underlying conditions such as high blood pressure, pneumonia, and respiratory problems. Since the emergence of COVID-19, the appropriate treatment has not been determined; hence, many researchers have opted for natural cure and prevention measures to help reduce the effects of the virus. Nutrients and supplements perpetuate the healthy immunity from individual dietary patterns (Trujillo-Mayol, et al. [20]).
The individual is responsible for host metabolic status such as diet, lifestyle, and nutrition with the surrounding conditions fosters the clinical and recovery manifestation. Based on diet, there are specific nutrients that individuals should consider taking in plenty to help boost body immunity, such as Vitamins, iron, and other adequate nutrients status (Gasmi, et al. [21]). The Coronavirus less affects strong immunity (Brodin [22]). Proper nutrition and hydration are vital supplements during COVID -19. Eating well balanced makes the body healthier and ensures stronger immune systems that lower the risk of the infectious virus. Thus, individuals are encouraged to eat various fresh and unprocessed foods daily to get adequate vitamins, minerals, dietary fibre, protein and antioxidants that the body requires (WHO [23]). In addition, taking plenty of water is also critical in enabling the body to stay hydrated and speeds upmetabolic activities that require more energy. The consumption of a balanced diet and environmental toxins interact with the host (García Bayona, et al. [24]). The Microbiota speeds up the interaction between the host and the linings to various organs such as lungs, liver, heart etc. The barrier lining creates integrates antimicrobial peptides that protect the internal environment from microbial translocation and secretion of protective mucous. The other natural prevention of COVID-19 is regular exercise enhances the body’s physical fitness and eradicates the developing diseases that might speed up the virus infections (Matricardi, et al. [25]). COVID-19 is mild when it interacts with ill patients having underlying conditions; hence, physical exercise helps regulate blood sugar body pressure and enhance metabolic functions.
More than 25 years have passed since the term evidence-based medicine (EBM) was introduced into the medical literature [5]. EBM is a concept that has evolved over time, initially clinicians considered that the decisions were made based on evidence, a more systematic approach was created to identify the most appropriate evidence an individual patient. This new approach was defined as patient-oriented evidence, meaning that the decisions are based on the clinical judgment of a capable expert, resulting from relevant medical literature witch follows a set of defined steps [1-6]. The most well established clinical guidelines are developed using methods that incorporate the EBM principles [1]. The successful implementation of EBM allowed a departure from the classic empirical practice that dominated medical history, however, the EBM approach provides only partly adequate solutions. The reason being that it is based on the premise “one size fits all”, this means that the solution found for the patient derives from information from a similar population. Consequently, medicine deals essentially with fragmented data, so the experts cannot master all the required knowledge [3]. This era of groundbreaking scientific developments in high-resolution, high-throughput data generating technologies is allowing the cost-effective collection and analysis of huge datasets on individual health, commonly refer as Big Data. This knowledge, makes it possible to achieve a data-driven approach centering on the individual, also known as personalized medicine, however, its implementation presents several challenges [3]. The most critical difference between EBM and MP lays on the fact that computational tradition, Big Data, is driven by data rather than hypothesis testing. This method works with raw observations and does not incorporate context knowledge into evidence production [7]. The long-term goals of MP are focused on: providing better-adapted, personalized surveillance measures and therapies and to significantly delay disease onset and, whenever possible, to prevent it. To achieve these goals, it is necessary to create a connection between MP and EBM [3].
Evidence-Based Medicine (EBM)
EBM is not only the application of knowledge acquired through literature, it is also the use of a series of steps to obtain relevant information for the patient in question and the incorporation of system of values related to the patient, that is, the wishes and preferences of the patient [1,4]. The EBM stages are typically [1,8,9]: 1) Formulation of the EBM question; The questions must be specific to a population, the more specific the easier it will be found in the literature. In addition, it must be well designed.
2) Gathering Evidence to answer the clinical question; The selection of relevant studies to gather all evidence necessary must be performed through a literature review. It is important to identify and use high-quality sources, such as MEDLINE, Cochrane Collaboration, among others;
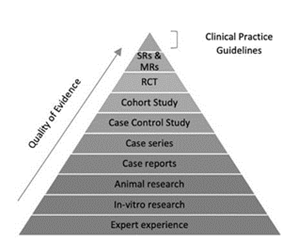
3) Evaluation of the quality and validity of the evidence: Not all scientific studies have the same value, they differ in terms of scientific strength and legitimacy, as defined in Figure 1. In addition to any type of study, individual examples vary in internal validity (quality of the methodology) and external validity (generalization of results). The levels of evidence are defined from 1 to 5 in decreasing order of quality. The types of study at each level vary in relation to the clinical issue but typically consist of:
Figure 1: Quality of evidence: traditional EBM (SRssystematic reviews; MRs- meta-analysis).
• Level 1: Systematic reviews or meta-analyzes of randomized controlled trials and single high-quality, randomized and controlled trials
• Level 2: Well-designed cohort studies.
• Level 3: Case control studies with systematic review.
• Level 4: Low quality cohorts and case control studies.
• Level 5: Expert opinion without critical evaluation, based on reasoning about physiology, bench research or its underlying principles [10].
4) Decision to apply the evidence to the patient’s treatment; Since the best available evidence can be derived from a population of patients with different characteristics from the patient in question, it is necessary to make a detailed analysis about the applicability of the evidence to the specific patient [1,8].
Big Data EMB
The explosion of big data has made the traditional research methodology obsolete [4]. Big data methods offer expanded research power. Classification algorithms can act as diagnostic tests, classifying a patient as having or as not having a disease [7]. Evidence – based personalized medicine is based on three pillars: responsible inter-institutional sharing of large clinical harmonized data sets; data on vital signs and behavior collected by empowered citizens; and clinical bioinformatics required to convert this complex information into clinically useful knowledge, which will be then returned by the medical practitioners to the individuals concerned [3]. For the clinicians today, the technology is already available but new concepts and ways of thinking are still lacking. Future clinicians will not be responsible for the storage of knowledge but rather, they will be responsible for knowledge administration. They will apply the knowledge acquired from a complete set of data to their daily clinical practice and serve the patients even better [4,11]. Some of the stages of Big Data EBM can be: [4,9,11]
1) Formulating Questions; Determining the research area: disease, treatment, tests, principle, group, characteristics, among others.
2) Research of data from real cases: hospitals, operators, etc. (preferably in a defined period of time )
3) Evidence analysis, advanced analytics tools are used to transform the data collected from the heterogeneous sources into the consumable units;
4) Evidence Grading and Calculation of Statistical Significance;
5) Analysis of the results with the objectives defined for the research, in order to support the best evidence;
6) Evidence Presentation, presentation of medical evidence;
While EBM continues to be the guiding principle, clinicians should be aware of potential tainted results. In the future, big data is likely going to offer us a new aspect of EBM and arm us with more comprehensive data when we make our clinical decisions [4].
EBM Big Data: An Example
Genomic and other related big data are leading a new era of precision medicine. Genomic medicine attempts to construct customized strategies for diagnostic or therapeutic decision making by using patients’ genomic information. The way this will impact population health depends on its ability to affect large segments of the population [6,12]. Next-generation sequencing (NGS) technologies, targeted sequencing, and other associated technologies, are increasingly applied to biomedical research and medical practice to identify diseases, drug- associated genetic variants, diagnostic markers. Genomic data generated by NGS technologies is a vital component support genomic medicine and therefor to advance precision medicine [13]. Nonevidence-based use of BGD may be harmful and result in major waste of healthcare resources [6]. Cancer is a complex genetic disease that results from the accumulation of genetic alterations and depends on the individual predisposition to cancer and the somatic alterations that initiate and trigger the progression of cancer. Genetic alterations could serve as effective biomarkers for early detection, monitoring and prognosis of cancer. Big Data EBM makes it possible to magnify screening from a single gene to the whole genome by using genomewide genotyping for genome wide association studies (GWAS) or next-generation sequencing (NGS) for cancer genome profiling studies. With the use of this technologies it is possible to provide the right dose of the right drug for the right patient at the right time, based on the genetic profiles of cancer and the individual [14].
Evidence-based Medicine and Precision Medicine: How to?
This combination will require worldwide and responsible data sharing, as well as regularly updated training programs responsible for the interpretation of the increasing amount and complexity of data, analyses and sharing of standardized medically relevant data globally, data for modeling disease and for issuing reports to support the decisions of clinical staff. Big data EMB will shift progressively from therapy to prevention, thus leading eventually to improved, clinician-to-patient communication, citizen-centered healthcare and sustained well-being [3]. EBM practitioners would benefit from seeking data science partners to exploit the availability of new, largescale, diverse data and to enlarge their tool kit with machine learning methods that may offer less expensive, quicker, and more powerful approaches to generating evidence in some circumstances. Big data scientists, who often come from outside the health field, would also benefit from partnering with clinical researchers who have the disease knowledge to adjust for sources of bias and to recognize spurious signals. Evidence-based medicine needs the computational power of big data, and big data needs the epistemological rigor of EBM. Combining these 2 types of knowledge offers the best path for enlarging and strengthening the knowledge base of clinical medicine [15].
Big Data EMB: Barriers and Solutions
One of Big Data EBM’s barriers is connected to the guidelines related to electronic health records and other clinical tools, that are overly restrictive [6]. Clinical tools are often built on representative patient population and may not reflect the individual patient. To overcome this barrier the guidelines can be adapted to the patient and use a shared decision making to help patients chose the most effective option [5]. Aggregation of heterogeneous data sets into electronic health records is important to achieve de goals of MP. The data is of multiple heterogeneous types, furthermore, storage and analysis of large data sets is not easily obtained by using current EHRs. There is a clear necessity for robust standardized procedures to ensure reliability, efficiency and an higher-level management of EBM. However, EHRs are not only heterogeneous but they can have incomplete, inconsistent, or inaccurate data, as well as additional limitations that further hinder their applicability, scalability, and semantic and technical interoperability [3,5]. Efforts to simplify the application of precision medicine into clinicians’ practice are improbable to be successful except if the EBM system became integrated into their Workflows [11]. Big Data EBM must be taught in an interactive and clinically based way, in order to fill the lack of knowledge of this practice. Even with the evolution of this concept, for many conditions, there is still no relevant evidence. In addition there is still incomplete evidence and conflicting evidence, so a set of guidelines with a low level of bias should be used in order to strengthen the clinical judgment. The clinician himself must keep abreast of the literature and be prepared for changes in practice due to changing evidence [5,6].
Conclusion
The paradigms of evidence-based medicine and personalized medicine both have strengths and weaknesses. The field of personalized medicine should advance with caution, avoiding overselling [3]. EBM´s success in providing a framework for fully integrating research evidence into the delivery of health care and raising awareness of the need for consideration of individual patient values and preferences. This framework has evolved over time in order to bridge the advances in medicine, so it may come to incorporate the era of big data that we live in and remain enduring contributions to clinical medicine and related fields [15].
How We Do It: – Making Local Anesthesia Safe and A Pleasant Experience
Introduction
Number of patients undergoing surgery under local anesthesia is about 13000 per year in the Department of Surgical disciplines at All India Institute of Medical Sciences (AIIMS), New Delhi, India. While performing minor surgical procedures under local anesthesia prevents unnecessary use of General Anesthesia and its inherent risks, it also allows patients to be discharged on the same day. This minimizes unnecessary use of hospital manpower and resources. However, do all the patients tolerate the procedure without pain? Do they have unpleasant experience during or after the procedure? In this era, when pain has been described as the FIFTH vital element for assessing patients’ well-being [1], every patient has the right to be pain-free. It’s the duty of every doctor to ensure this, more so in cases of procedure under local anesthesia. We as the Surgeons should do our best to make the procedure pain-free. Anxiety related to the procedure and fear of the operation theatre (OT) itself, conscious awareness of the procedure being performed, nausea, vomiting and palpitation are few of the so many important concerns that our patients go through and tolerate in the pursuit of getting surgical treatment. Therefore, it is the one and utmost responsibility of the operating Surgeon to perform the surgical procedure in a well-planned manner with all the precautions to avoid any problems related to the local anesthesia.
Challenges
In our daily practice, we see patients go through this phase in a varied and often apparently trivial manner which, nevertheless, means a great deal for any individual. Therefore, it’s very essential to be vigilant and expectant so as to prevent and / or to identify and address these concerns. How exactly can we overcome these problems? We intend to discuss some important strategies to minimize problems during local anesthesia and making it a pleasant experience.
Consent and Counseling
Every Individual has the right to be pain-free. There are various ways to minimize or abolish the perioperative pain. Overall being communicative with the patient and explaining them the progress of the procedure and getting their constant feedback will result in more compliance and satisfaction [2,3]. We do need well-trained Nursing staff and OT technician in this regard.
OT Set Up
Operation Theatre has its own standards to be met [4]. Minor OT settings are basically similar to the main OT settings. Besides all the standards that are usually met at the time of OT set up, adequate illumination is the key to any successful operative procedure. It saves time and prevents unnecessary tissue damage.
Patient Selection
It is a well-known paradigm to any medical care personnel that medical acumen has its success when proper treatment is given to suitable patient at the right time [5]. We need to select patients who are fit for local anesthesia. Patients with coronary artery disease or compromised respiratory status or even patients with high BMI though feasible might not be able to tolerate even the minor stress of pain during day care procedure [6-9]. Hence, those candidates would better undergo procedure under General anesthesia with specialized Anesthetists team. Therefore, we usually avoid local anesthesia in patients like in the extremes of ages, with obesity, patients with uncontrolled hypertension, other cardiovascular disease and those with compromised respiratory status.
Preparation
Before taking patient to the operation theatre, we should be cognizant of the comorbidities of the patients and any medications patients is taking like anticoagulants, antidiabetic, antihypertensive medications etc. We should be aware of any allergic reactions to Local Anesthesia (LA) in the past. We should always try to keep the Anesthesiologist in the loop for any immediate help that might be needed. Intravenous (IV) cannula, IV fluids, analgesics, oxygen supply and lifesaving drugs and intubation set should always be available in the vicinity, irrespective of the procedure we perform.
Pleasant Anesthesia
There are certain mechanisms by which we can prevent the pain cycle itself to start.
a) Dermal Analgesia
Eutectic Mixture of Local Anesthetics (EMLA) cream contains topical lidocaine and prilocaine as active ingredients [10,11]. This has been commonly practiced in plastic surgery before harvesting skin grafts. It should be used 30 minutes to 1 hour before surgery as topical anesthesia [12]. It works by stabilizing the neuronal membrane by suppression of the ionic fluxes providing dermal analgesia in the vicinity of pain receptor and nerve endings [10]. EMLA cream also decreases the dose of injectable local anesthetic drugs [13].
b) Infiltrating Needle
Wide bore needle causes more pain at the time of infiltration. In our set up, we usually use 26-gauge needle for infiltration. We have learnt from our experience at AIIMS that cold needle causes numbness, soothing effect and less pain during the procedure. We usually keep the needle in the freezer compartment an hour before use.
c) Pre-Oxygenation
Oxygen: – The aim of oxygen supplementation is to increase pulmonary oxygen reserve by raising the functional residual capacity. Thereby, in the event of a decrease in cardiovascular or respiratory function such as arrhythmia, hypotension or bronchospasm, oxygen transport is already optimal and there is enough time to secure the airway if the need arises [14].
Energy Sources
Various modalities of new energy sources are available. Judicious use of these energy sources can help in minimizing complications like intra-operative bleeding or post-operative hematoma. Energy sources are usually not used in minor procedure under local anesthesia. In cases operated under local anesthesia, incision is usually small and the limited exposure precludes easy control of hemorrhage lest the bleeding occurs. Therefore, we routinely use energy sources [monopolar or bipolar electrocautery] which helps to reduce the operative time, blood loss and excessive tissue damage which may occur in the struggle to secure bleeders [15].
Support and Conscious Awareness
It has been well-known fact that proper patient communication and assurance is the best way not only to best support the patient but also to avoid unnecessary medicolegal issues [2,3]. Counselling is also very important part of local anesthesia. We generally counsel the patient what to expect during and after the procedure including the expected pain during infiltration of local anesthesia. Occasionally, patients might feel little pain despite full analgesia. Patients might also feel some traction/tugging sensation during the procedure. The other important aspect is that patient may feel pressure effect. Patient remains awake throughout the procedure, and hence, they may feel undue pressure when the Surgeons or the assistants put their hand to rest on patient’s body around the operative site.
Regional Blocks
Majority of the procedures are better operated with regional block [16]. Regional block is usually indicated in local procedures requiring wider surgical field [17]. However, the procedure is technically demanding. At our center, we usually practice ankle block, wrist block and digital block.
a) Ankle block
Ankle block is essentially the block of four terminal branches of the sciatic nerve viz. deep & superficial peroneal nerve, tibial and sural nerve and one cutaneous branch of the femoral nerve [18]. Ankle block is very safe and highly effective for a wide variety of procedures on the feet and toes. In our centre we usually do dressing, debridement and amputation of gangrenous toes and forefoot, and skin grafting over raw area of foot and toes under ankle block. Blocks are done just proximal to the level of malleoli, above the ankle joint using surface anatomical landmarks for the respective nerves [18].
b) Wrist block
Wrist block is essentially a block of radial nerve, ulnar nerve and median nerve [19]. Wrist block is performed for surgery of hand and fingers.
c) Digital block
Digital block is the technique of blocking the nerve of the digits to achieve anesthesia of fingers. This technique is commonly used for a wide variety of minor surgical procedure of digits such as partial excision for ingrowing nail, excision of corn, excision of cyst, amputation of digits for gangrene of digit, dressing and debridement of wound over digits. Combination of LA with epinephrine has been found to be safe [20,21], however, it has to be used with extra precautions.
Know Your Drugs and Side Effects
Local anesthetic agents are broadly categorized into two groups; Benzoic acid esters that includes procaine, tetracaine etc. and Acid amides that include articaine, lidocaine, bupivacaine, prilocaine, ropivacaine etc [22]. At our center, lidocaine and bupivacaine are mainly used and will be the focus of further discussion.
a) Lidocaine [Xylocaine]
Lidocaine has rapid onset of action [< 2 minutes] and acts for medium duration of about 30-60 minutes (longer with epinephrine) [23]. Maximum safe dose without vasoconstrictor is 3mg/kg body weight [maximum up to 300mg]. Whereas, maximum safe dose with vasoconstrictor is 7mg/kg body weight [up to 500mg] [24]. We generally use 2% lidocaine at our center. One ml of 2% lidocaine contains 20 mg of lidocaine. So we can use 15 ml of 2% lidocaine as maximum safe dose without vasoconstrictor and 25 ml of 2% lidocaine with vasoconstrictors for a standard Indian male. We usually use xylocaine 2% with adrenaline 1: 2,00,000. One ml of this solution contains 20 mg of lidocaine and 5 micrograms of adrenaline.
b) Mechanism of Action
Lidocaine alters signal conduction in neurons by blocking the fast voltage gated sodium [Na+] channels in the neuronal cell membrane that are responsible for signal propagation [25]. With sufficient blockage, the membrane of postsynaptic neuron will not depolarize and will thus fail to transmit an action potential. This creates the anaesthetic effect by not merely preventing pain signal from propagating to the brain but by aborting their generation in the first place itself.
c) Side effects
Common side effects include nausea, dizziness, bruising, redness, Itching or swelling where the medication is injected. Unlikely but serious side effects include CNS related side effects such as drowsiness, mental/mood changes, ringing in the ears, vision changes, headache, tremors, numbness [24]. Cardiovascular related side effects are bradycardia, hypotention and cardiovascular collapse which may lead to cardiac arrest [26]. Allergic reactions have also been noted as characterized by cutaneous lesions such as urticaria, edema or anaphylactoid reaction [27].
d) Bupivacaine
Other commonly used local anesthetics is Bupivacaine. Its onset of action is about 5-10 minutes [23]. Duration of action of Bupivacaine without vasoconstrictor is about 200 minutes and with vasoconstrictor is about 540 minutes [23]. Maximum safe dose of plain Bupivacaine is 2mg/kg body weight and with vasoconstrictor it is 2.5 mg/kg body weight [28]. We generally use 0.5% bupivacaine. 1ml contains 5mg of bupivacaine. Its mechanism of action is essentially similar to that of Lidocaine. Common side effects of Bupivacaine includes nausea, vomiting, chills or shivering, headache, backache, dizziness, problems with sexual function, restlessness, anxiety, ringing in the ears, blurred vision, tremors, constipation, low blood pressure, etc [29]. We should avoid use of bupivacaine during pregnancy and lactation because it harms the fetus and also gets concentrated in breast milk and may harm the nursing baby. Overall precautions that we routinely take into consideration to avoid these preventable side effects of local anesthetics are proper dose calculation, prior testing of sensitivity and aspiration prior to injection so as to ensure local anaesthetics are not being injected into blood vessels.
Additional Medications
a) Non-Steroidal Anti-inflammatory Drugs (NSAIDS)
Non-Steroidal Anti-inflammatory Drugs can be used along with L.A. in the patients where LA alone is not sufficient to control pain despite administrating maximum safe dose [30] or situations where local anesthetics cannot be administered at the whole area of interest.
b) Bicarbonates
In case of abscess, cellulitis and inflamed tissues, the tissue pH is acidic. In acidic pH lidocaine and bupivacaine do not work [31]. Therefore, the use of bicarbonates along with lidocaine or bupivacaine helps to make the medium alkaline, so that the local anesthetics may be effective in such scenarios.
c) Anti-Emetics
Anti-emetics can be added pre-emptively or as on demand basis.
Essential Care
Any surgical procedures in the day care procedure under local anesthesia needs essential care. Besides the specific considerations mentioned previously, every patient needs special attention throughout the course of procedure to address their specific concerns. It’s essential that all the patients undergo vitals monitoring with at least pulse rate and saturation throughout the procedure. Oxygen supply can be provided to anxious patients or those with cardiovascular, respiratory or other comorbidities. Maintenance Intravenous fluid should be administered to replace insensible loss in day care procedures that are expected to take longer duration [32]. Even after the procedure it is essential to hold the patient and make her/him sit down or leave the patient to the attender to avoid any sudden hypotension or fall of the patient. On should never neglect patient’s complaints of any problems like dizziness following the procedure. One should always be aware of the possible side effects of local anesthetics. Therefore, Proper teamwork with the Nursing and OT staff with routine habit of taking into considerations the minute details during the surgery is the key to providing a safe and pleasurable local anesthesia for any day care procedures.
3D Screen Printing Enables Application of Integrated QR Codes on Pharmaceutical Dosage Forms in Mass Production – A Game Changer
Introduction
Quick Response (QR) codes have been in use since the 1990s. They were initially developed as a way to track components of vehicles at Denso Wave (a Japanese company and a subsidiary of Toyota) through the supply chain [1]. Since then, their use has steadily increased. The widespread availability and decreasing costs of entry for mobile devices such as smartphones and tablets that can quickly read QR codes have significantly contributed to their quick adoption. A QR code is simply a two-dimensional barcode. It looks like a crossword puzzle with black and white squares called modules. The square grid-like design allows for an increased storage of information compared to a standard one-dimensional bar code. QR codes can store about 7,000 digits (around 4,000 characters) of information such as linking to a specific website. It includes a high-level of integrated redundancy, allowing for the QR code to be readable even if a substantial portion (around 30%) of the code has been damaged. Today, QR codes are ubiquitous and can be found everywhere from construction through social media to banking. The flexibility of their design and the ability to quickly update their information makes them easily amenable to a wide range of applications, including healthcare.
QR codes have already proven to be highly beneficial in healthcare such as patient tracking, drug safety and many other use cases (Figure 1). They can be used to digitally store product safety, medication interactions, among others, as well the ability to update this information in real-time for patients and health care providers. Moreover, implementing QR codes directly on dosage forms is an efficient means for combating counterfeit medicines. This review investigates the potential for using QR codes in medicine, with a special focus on their application for pharmaceuticals using 3D printing technology, including screen printing.
Figure 1: Advantages of using QR codes for pharmaceutical dosage forms in mass production.
Tablet Level Labeling
Additive manufacturing is an increasingly disruptive force in pharmaceutical development [2-4]. 3D printing (3DP) approaches enable custom geometry, size, content, and release characteristics of active pharmaceutical ingredients (API). At the same time, digital modelling has allowed for a new level of freedom in drug design. These opportunities have led to a boom in 3DP technologies for pharmaceutical development. Although conceptually similar, each uses its own method to deposit each layer of material and cure it [5- 9]. There are two primary approaches for additive manufacturing: personalized drug development and production for the mass market. The ability to produce custom drugs for the mass market has a lot of appeal for responding to changing needs at scale and have been a major focus of recent technological developments.
However, concerns over scalability of 3DP technologies, low mechanical resistance, low printing resolution and limited material choices have so far limited their practical implementation [10,11]. Currently, only a single 3D printed pharmaceutical, the antiepileptic drug Spritam® is FDA approved and marketed [12]. The first types of 3DP pharmaceuticals were developed using continuous inkjet printing [13]. Since then, advances in inkjet printing [14,15] as well as newer technologies, most notably: extrusion-based printing (fused deposition modelling (FDM), and screen printing) [16-18], powder-based printing (powder bed and powder jetting) [19-21], selective laser sintering (SLS) printing [22], have aimed to print instead pharmaceuticals for the mass market. Among the 3DP technologies, extrusion-based printing, such as FDM, direct ink writing (DIW), and most recently 3D screen printing (3DSP), have shown the greatest promise due to their low cost and flexibility.
All extrusion-based 3D printers have two principal components 1. The extruder (which deposits the precise quantity of material over a specific distance) and 2. The positioning system. The pintable material (i.e., ink) in the form a viscous melt or liquid is extruded through a nozzle (in case of FDM and DIW) or through a tissue (in case of 3DSP). While the nozzle gets only a single printer, the tissue, as a function of its area, mediates extrusion of paste for multiple objects at the same time. The newkid on the extrusion-based printing block is 3DSP. 3DSP is a type of extrusion printing that uses a screen mesh to transfer a semisolid, API containing paste onto a substrate, except in areas made impermeable to the paste by a blocking stencil. The deposited layer is then dried. The next layer is printed precisely on top of the previous one after lifting the screen by the dried layer thickness. 3DSP has the potential for mass customization enabling the buildup of thousands of units per screen simultaneously. The number of units printed simultaneously is largely defined by the ratio of screen size to unit size. This differentiates screen printing from other 3DP technologies, whose capacity is limited by the number of printing heads [10,23]. Exentis Group [24], based in Switzerland has developed the patented 3DSP technology for a broad range of industrial applications, such as renewable energy sources, automotive industry, aerospace, and biotechnology. The Exentis 3DSP enables the production of several hundred items with the option for a mass production of an upscaling to several million a day. Laxxon Medical Corp holds the exclusive worldwide license to explore this 3DSP technology for all kind of pharmaceutical applications.
Laxxon Medical Corp. is developing a screen-printing approach for printing pharmaceuticals for the mass market. This approach is based on a classic flatbed screen printing that is widely used in industrial applications [25,26]. Proof-of-concept work with 3DSP (SPID®-Technology) has shown that it is possible inter alia to print QR codes directly on tablets as small as r = 5 mm during and as integrated part of the manufacturing process (Figure 2). Using this approach, the QR code is part of a one-stop manufacturing process of the tablet. 3DSP could also be used to print API containing QR codes and/or inks which make the tablet easier to identify, harder to counterfeit and increases product safety. There are at least two ways that a QR code can be printed directly on tablets. The first is to print the code on top of the tablet using different kinds of inks. Inkjet printing for example has previously been shown as a viable strategy for printing QR codes directly on oral dosage formulations. Work by Edinger et al. showed that it was possible to print specific amounts of the neuroleptic drug haloperidol as a QR code on an edible orodispersible substrate [27]. Here, researchers used the QR code to identify the API, dose, patient name, administration route, expiration date, manufacturer ID and batch number as a proof-ofconcept. Further work by Trenfield et al. combined both 2D and 3D inkjet printing technologies in a single-step manufacturing process to create drug-loaded tablets with a combined QR code identifier that used anti-counterfeit ink [28]. In both cases, a personalized medicine approach was investigated instead of a mass customization strategy, but there is clear potential for both strategies.
Figure 2: 3D Screen Printed Tablets with integrated QR Code. A. QR code screen with different sizes (diameter) and QR code designs used within the 3D Screen Printing Unit EX 301i. B. Tablets were printed with 92 levels of each 0.025 mm. Afterwards, at the end of the manufacturing process, 2 additional layers with the QR code pattern were applied. A mixture of black and blue (2:1) commercial food dye was utilized for coloring the QR-code. Example QR code printed on a 9.5 mm size tablet. C. More complex QR Code (allows larger amount of data) were printed on different sized tablets 14.5, 11.5, 9.5 mm (from left to right).
The ability to print a QR code directly on the tablet would be a major benefit for patients and health care professionals (HCPs). It would allow them to confidently identify the medication and access all relevant product information, even without the need of any secondary packing information. This could be helpful to older patients who may be taking multiple medications, and who may separate their pills into pill boxes without any identifying information. It is also of great interest to patients who may be visually impaired and have trouble identifying their medication even with the packaging information available [29]. Also, patient safety could increase through automated dispensing enabled through this QR code marking [30]. This is especially important in the hospital setting, a situation characterized by frequent medication changes and of increasing patient turnover. Checking drug data against patient data, both in an electronic format and at the point of dispense, could maximize patient safety.
An alternative to printing the QR code on the tablet itself is to embed the code into the tablet [31]. One such proposal used grooving to offset the surface inward to create light and dark regions resulting from ambient occlusion. This could allow for tablets with rough surface structures as well as a wide range of surface colors to have a readable QR code. While conceivable, the outlined solution is complex as its implementation requires the sequential application of two technically different processes. In contrast, 3DSP is capable of yielding tablets with embedded QR codes by applying two additional steps of the very same production process. First, a negative print is administered on top of the printed tablet’s body using the “negative” screen, then resulting recesses are filled using the “positive” screen and a colored paste. Requirements are well within the scope of the screen-printing technology, namely two more screens and two pastes with different colors. Where needed, the QR code could be sealed by applying a thin layer of transparent paste.
Improving Medication Safety
Product safety communication in medicines is an integral, interactive exchange among regulatory authority, HCPs, and patients, so that all parties understand the product risks. The backbone of this communication starts at the level of defining what a medicine is. The safety of pharmaceuticals, especially regarding the testing, approval and manufacture of drugs, pharmacovigilance, the distribution of drugs, and the monitoring of drug traffic for NCAs is defined in national laws, e.g., Section 1 of the German Medicines Act (AMG) [32]. This regulation covers what qualifies a product as a pharmaceutical, a generic, as well as counterfeit medicines.
Patients and HCPs are most often informed of product risks in statutory information such as that contained in the product information (i.e., the summary of product characteristics (SmPC), package leaflet (PL) and the labelling of the packaging) and public assessment reports [33]. A key limitation of this content is the speed for the implementation of updates. In this format, emerging safety issues discovered from NCAs and HCPs cannot be updated in real-time, leaving potentially vulnerable patients at a greater risk as a result of the inflexibility of this communication method for months, if not longer. Moreover, PLs and additional supplementary information provided with prescription medication can be easily lost or discarded by the patient.
Medication errors, incorrect dosages, and unintended drug interactions have reduced the effectivity of available care. Medication errors account for an estimated one-quarter of all healthcare errors [34], costing an estimated US$42 billion annually worldwide according to the World Health Organization (WHO) [35]. Errors may happen while prescribing, transcribing, dispensing and administrating medication. A combination of look-alike/sound-alike medications, overwhelmed doctors and nurses, and the increasing complexity of patient care all contribute to an increased rate of mistakes. Patient error resulting from misunderstanding medication labels contributes significantly to avoidable hospitalizations. Up to 25% of all medication errors can be attributed to name confusion and 33% to packaging and labeling confusion [36]. This issue is further complicated in older patients who may be taking prescription drugs and supplements simultaneously [37]. For example, warfarin, a common prescription blood anticoagulant, and Ginkgo biloba, a common herb supplement, can both reduce blood clotting. Taking these products together can increase chances of internal bleeding and stroke in some patients [38]. However, this level of information is very often missing from PL.
The European Union’s Innovative Medicines Initiative WEBRADR has spent the last three years investigating how the influx of mobile devices, such as smartphones, could offer an ideal platform to improve communication of emerging safety issues [39]. Based on the progress in this arena, the European Medicines Agency (EMA) published guidelines on the use of QR codes for labeling and packaging of authorized medications in 2018 [40]. An early study from 2015 found that adding QR codes to the labels reduced medication errors in older patients taking multiple medications [41]. Further studies have looked at how medication errors may be reduced across different age groups. Recent work from Arizona State University undergraduates and senior citizens over 70 for example, similarly, found statistically reductions in medication errors for both groups when a QR code from the label was scanned prior to taking the medication [42].
Automated dispensing of medications in pharmacies and in hospital settings is a common way to provide medications to patients on-demand and to fill prescriptions close to the pointof- care. Automated dispensing cabinets and similar technologies aim to increase efficiency and reduce medication errors. There are several systemic reviews [43-45] which have found that automated dispensing was an effective way to decrease medication errors and improve patient management. Barcodes, and in many cases QR codes, can be read by these technologies. This efficiency could be bolstered by the addition of a QR code on the tablet itself, as this would allow for control at the single tablet level.
Reliable Remote Patient Monitoring
Patient adherence to their medication remains a substantial barrier in getting the most out of their prescribed treatment. An estimated 50% of patients on long-term therapies do not take their medications as prescribed [46]. Tight medication monitoring is also critical for medications which may be prone to misuse, such as those which are highly addictive. One popular example is the widespread use of medical cannabis. The prescribed dose of medical cannabis is highly individual, and the medication is prone to misuse, requiring close supervision by HCPs [47]. Recent publications on data-enriched edible pharmaceuticals (DEEP) used QR codes containing lipophilic cannabinoids, i.e., cannabidiol (CBD) and delta-9-tetrahydrocannabinol (THC), that were printed using a desktop inkjet 3D printer [48,49]. They printed a customized dose that could be readable by standard smartphone applications which remained readable after 8 weeks of storage under standard conditions. This approach shows the ability to use the QR code to directly label the substance at the single dosage unit level and track the patient’s adherence to taking that prescribed dose. A further approach could be the development of specific apps for medication management that can scan QR encoded dosages prior to taking the medication [41,50-52]. Such apps have already shown promising results in improving compliance of elderly patients with heart disease [53] as well as for mental health interventions [54].
Combating Counterfeit Medicines
Counterfeit medicines make up an estimated US$200 billion of the pharmaceuticals market annually, making it the largest identified fraud market globally [55]. In the industrialized world, estimates suggest that less than 1% of medicines sold are counterfeit [56]. However, in developing countries, these can be as high as 30%. The statistics are further complicated by the increased number of consumers buying medication online, increasing the risk of obtaining counterfeit products from suppliers globally. In response, the United Nations (UN) under the auspices of the UN Office on Drugs and Crime (UNODC) started in 2014 a global campaign to raise awareness among consumers on the dangers of counterfeit goods and their link to organized crime [57].
The addition of QR codes to pharmaceuticals and pharmaceutical packaging has been suggested as a way to help reduce the number of counterfeit medicines in circulation at least as early as 2015 [58]. QR codes would be more difficult to replicate compared to standard text and image-based labeling used on pharmaceuticals. QR codes can be further equipped in anti-counterfeiting features, such as holograms [59] and fluorescent inks [60] which could help prevent falsified QR codes from appearing on the market. Drug-loaded biodegradable labels in the shape of QR codes have already been manufactured by casting the drug solution into prepared molds [59]. Although QR codes could be applied to both packaging and the drug dosage form, packaging labels are only an effective method if the drugs themselves are not repackaged. To decrease this risk there is an increased attention to “in-drug labeling” (i.e., direct tablet labeling) as an untapped tool to protect consumers from counterfeit medications [61]. Such in-drug labeling approaches would need to be ideally developed not only for solid drug formulations but also injectables and liquid formulations which may contain expensive and/or dangerous APIs that are high-interest targets for forgery.
Outlook
QR codes have a lot of potential to improve the way patients and HCPs interact with prescribed medications and treatments. Technical hurdles do remain for patients who may still be uncomfortable or have physical limitations with using QR codes and smart mobile devices. Additional training needs to be taken into consideration for these patients. It also should be remembered that the implementation of a QR code on pharmaceuticals would not be a complete replacement for existing patient leaflets. The basic information about the product still needs to be provided in a printed form to allow for patients to be able to access the information even if their smartphone is out of batteries. QR codes instead should be viewed as a way to augment this printed information with further details on medication interactions, explaining medical terms, and safety alerts that might be relevant to their specific treatment. The increased availability of 3D printing options for pharmaceuticals makes the addition of the QR code to the labeling and to the packing itself already within technical reach.
Safety concerns using QR codes could however continue to arise if the information linked to the QR code is either no longer in use or had been moved from its original online location. This can be mitigated by using dynamic QR codes instead of static QR codes. Regulations on the updating of online medical information must be in place to ensure that the information that is available to patients is the most accurate and up-to-date available. If there is one thing that has been highlighted by the COVID-19 pandemic more than anything, it is that the pace the medical information, including recommended treatments, can change overnight. Although this is an extreme example, all registered medications continue to be researched and have their safety information tracked after the patient information booklet has been printed. For all medicines, having the ability to update patients and doctors with this new information on-demand in an easy electronic way, would be invaluable.