The Baseline of the Patient’s Cohort Undergoing Bariatric Surgery in Chile
Introduction
The prevalence of obesity worldwide has reached pandemic levels in recent years, mainly due to profound changes in lifestyles, among which sedentary lifestyle and high calorie density diets stand out [1-3]. The Chilean population is not exempt from this reality, according to the latest data published by the Organization for Economic Cooperation and Development (OECD), 74% of the adult population in Chile are overweight or obese, making Chile the country of the OECD with the highest rate of obesity and overweight, above Mexico (72.5%) and the United States (71%) [4]. These data are reaffirmed with the 2016-2017 National Health Survey, which show that in Chile 42% of the adult population between 30 and 49 years of age are overweight, 31.2% are obese, and 3.2% of the population is morbidly obese [5]. Currently, obesity treatments include first-line lifestyle modification diet, physical activity, and behavioral therapy, and in some case pharmacotherapy [6]. However, only some patients achieve satisfactory weight loss or resolution of comorbidities associated with obesity with these conventional treatments. When patients do not respond favorably to these treatments, BC is considered. Strictly speaking, the term ‘bariatric surgery’ (BC) is applied to all surgical procedures that aim to reduce excess weight, and actually is considered as the most effective therapy available for significant and sustainable weight loss and control of obesity-related comorbidities in morbidly obese patients, improves the quality of life and reduces mortality in obese people [7-9].
Currently, it is estimated that in Chile there are about 500.000 morbidly obese people eventual candidates for BC. However, the National Health Fund (FONASA) provides treatment consistent in comprehensive care and BC to 400 people per year, an insufficient considering the morbidly obese people that currently exist in the country. The first published cases of BC in Chile date back to 1986 when González et al. described six jejunoileal shunts [10] and, in 1999 when the first horizontal gastroplasty in Roux-In-Y was described by Csendes, et al. [11], one year later, in the 2000, the first RYGB was performed at the public hospital San Juan de Dios Hospital of Curicó. BARCO is a cohort of obese patients operated for RYGB and SG procedures at the San Juan de Dios Hospital, in Curicó, Maule district, from January 2000 to May 2018. BARCO was created to support clinical, epidemiologic, and behavioral research to patients operated by BC in public regional health. This paper aims to report the baseline characteristics of BARCO´s patients, to provide a basic description of the sociodemographic, anthropometric measurements, principal comorbidities, mental health, lifestyle habits, clinical, and post-surgical complications of patients undergoing BC.
Materials and Methods
Data Collection
For data collection, a standard review file was created that included 46 variables with sociodemographic, clinical, mental health, main comorbidities diagnosed by a doctor, complications after the intervention, and lifestyle habits of patients undergoing BC. The data were collected through an exhaustive review of physical clinical records, two members of the BC team (one physical therapist and one nursing intern) were trained in data extraction from clinical records, to standardize the information collection method, while avoiding the reduction of systematic errors in their transcription. The information was entered into a database by two surgical interns who, in case of having any doubts regarding the values or data, reviewed the clinical file again for corroboration, in case of discrepancy the chief surgical team determined the inclusion or exclusion of the data. The compilation lasted 6 months.
Patients
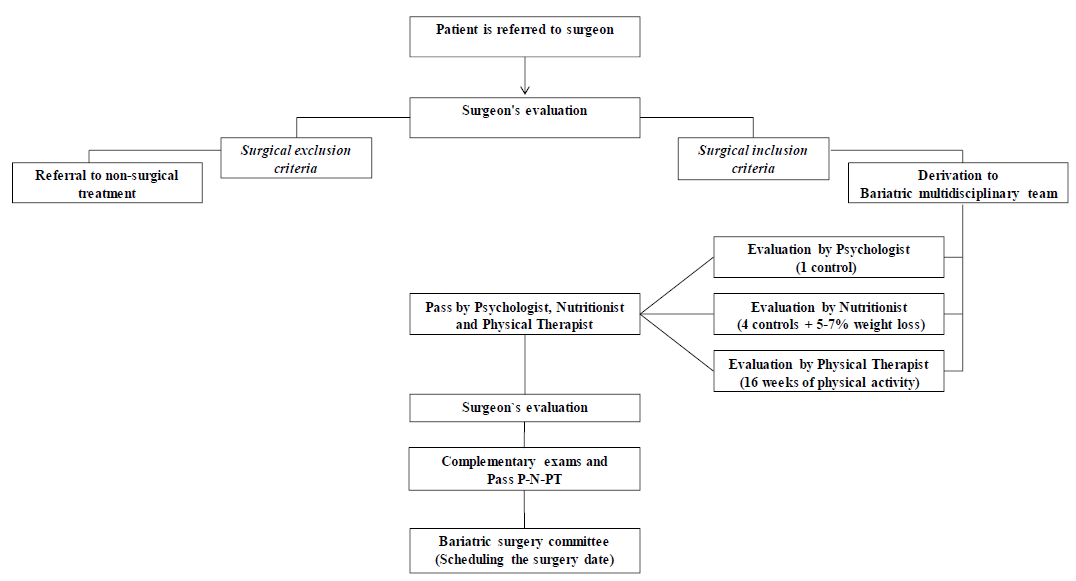
Figure 1: Diagram flow of the patients’ selection to bariatric surgery procedures. The patients’ selection to bariatric surgery procedures. Pass Psychologist = Pass P, Nutritionist = Pass N, Physical Therapist=Pass PT.
652 patients were operated on between January 1, 2000, to December 31, 2018, 3 adjustable gastric band, 5 deceased patients, and 19 patients whose clinical records were lost with the 2010 earthquake were excluded from this study. The remaining 625 patients, who were included, were older than 18 years with a BMI ≥ 35 kg / m2 in presence of at least one comorbidity, or BMI ≥ 40 kg / m2 without comorbidity, and who had undergone of RYGB or SG as the primary intervention. All patients had to be evaluated by the hospital’s BC multidisciplinary team, composed of bariatric surgeons, nurses, physical therapists, nutritionists, and psychologists (Figure 1).
Surgical Procedures Type
RYGB: For this procedure, a 5 cm gastric pouch with a 40-cc capacity was made with a 60 mm x 3.5 mm purple endo linear cutting stapler, between the 2nd and 3rd vessels of the lesser curvature, with 3 refills and 110 cm digestive loop and 150 cm biliopancreatic loop were used. SG: For this procedure, the greater curvature was dissected with a ligature from 4 cm proximal to the pylorus to the Hiss angle, and then the 36 F-calibration probe was installed under direct vision of the lesser curvature. Finally, an EndoGia 60 stapler was used for the section (5 purple loads). The Medtronic® kit was used for both procedures.
Variables
A database created included 46 variables referring to sociodemographic such as age, gender, occupation, and marital status: and the anthropometric measurements body weight, and BMI. The principal comorbidities like arterial hypertension, diabetes mellitus, insulin resistance, hypothyroidism, dyslipidemia, skeletal muscle diseases, obstructive sleep apnea, and gastroesophageal reflux, were included. Mental health including anxiety disorder, depression, bipolar disorder, and panic disorder were evaluated. Lifestyle habits such as alcohol, tobacco, and physical inactivity were also included. In the case of clinical parameters: pre-surgical exam results of upper gastrointestinal tract endoscopy and pulmonary evaluation by forced spirometry and rest EKG were evaluated. The number of RYGB and SG procedures between 2000 to 2018 years. Number of cholecystectomies during the surgical procedure and post-surgical complications. This study was approved by the Department of Teaching and Research of the San Juan de Dios Hospital of Curicó, complying with the criteria indicated in the Helsinki Declaration.
Data Analysis
Qualitative variables are presented as frequencies and percentages. The quantitative variables are presented as means, with standard deviations. It found that 34 were missing data, which were eliminated. The data observed mean in the case of continuous variables and use of the mode in the case of qualitative variables. To statistical analysis the data, the software SPSS version 2.4 was used.
Results
A total of 625 patients met the eligibility criteria of the study. SG was the most frequently reported procedure (85.6%) followed by RYGB (Table 1). Participants mean age was 39 years old and were predominantly female (85.9%). Most of the patients were homemakers (45.8%), professionals (21.3%), office workers (18.6%), 9.6% were students and 4.7% declared other kinds of occupation. Regarding marital status, 60.5% was married, 29% single, 6.1% divorced, 1.1% widows and 3.2% declared other. Regarding the anthropometric measurements, the mean of preoperative body weight was 110.6 kg and the mean of BMI was 42.2 kg / m². Most of the patients (87%) had a BMI ranged from <40 kg / m² to 49.9 kg / m², 11.4% 50 to 59.9 kg / m² and 1.6% have 60 kg / m² or more. The most prevalent comorbidities were hypertension (37.3%), type 2 diabetes (23.6%), insulin resistance (17.9%), hypothyroidism (17.5%), dyslipidemia (7.6%), the skeletal muscle diseases (3.3%), obstructive sleep apnoea (1%) and finally gastroesophageal reflux (0.6%). Regarding the total number of associated comorbidities, most of the patients (42.7%) did not present comorbidities at the time of surgery, 29.3% presented with one comorbidity, 17.6% presented with two comorbidities, 7.5% presented with three and 2.9% presented with four or more comorbidities.
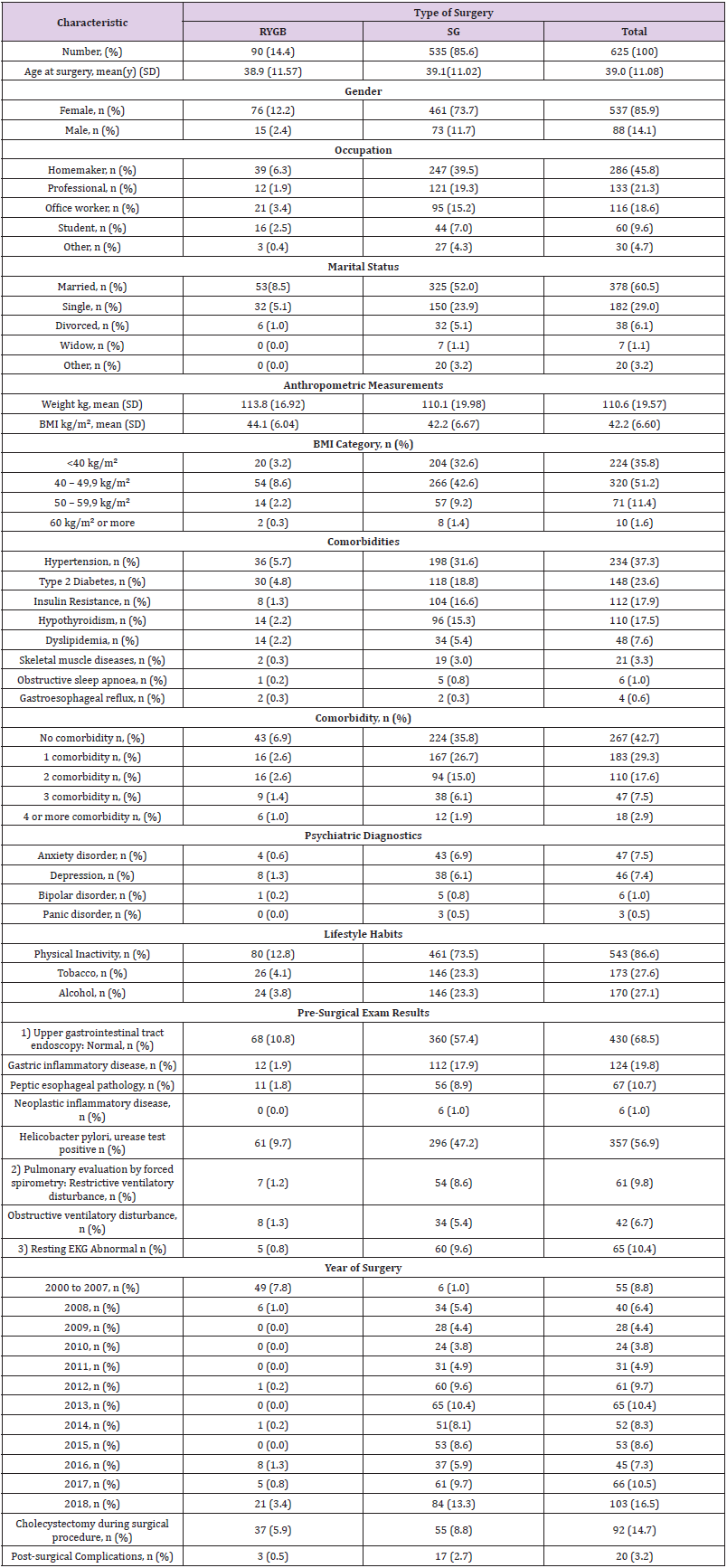
Table 1: Baseline summary of BARCO patients.
Between the psychiatric diagnostic, the most prevalent were anxiety disorder (7.5%) and depression (7.4%), followed by bipolar disorder (1%) and panic disorder (0.5%). During the clinical interview, the patients declared about their lifestyle habits, 86.6% were sedentary, 27.6% smoked tobacco and 27.1% drank alcohol. The pre-surgical exam results indicated that 68.5% of patients presented with a normal upper gastrointestinal tract endoscopy, 19.8% gastric inflammatory pathology, 10.7% peptic esophageal pathology, and 1% presented neoplastic inflammatory disease. Notably, 56.9% of patients presented with Helicobacter pylori (H. pylori), positive urease test. Pulmonary evaluation by forced spirometry indicated that 9.8% presented with restrictive ventilatory disturbance and 6.7% obstructive ventilatory disturbance. Regarding the rest EKG, 10.4% of patients presented abnormal results.
The number of bariatric procedures progressively increased, from 55 cases between 2000 and 2007, and over 100 cases in 2018. Regarding the type of surgery performed per year, between 2000 and 2007, RYGB was the most frequent procedure (49 of 55), however from 2008 to 2018, SG was the most reported procedure (528 of 568) used. During surgical procedures, 92 patients underwent a cholecystectomy, of which 55 were SG and 37 RYGB. Finally, the percentage of post-surgical complications was 3.2%, of which 2.7% corresponded to SG and 0.5% to RYGB. No patients died during the procedures (Table 1). The trends used from 2000 through 2018 are summarized by procedure types in Figure 2. The number of RYGB was higher compared to SG procedures between the years 2000 and 2008, and from 2008 onwards, the number of RYGB decreased and SG procedures had a significant increase. BMI distribution by bariatric procedure types is summarized in Figure 3. The mean BMI was 35 to 65 m/kg2 between both bariatric procedures, however, some patients operated with SG presented a BMI of over 60 m/kg2.
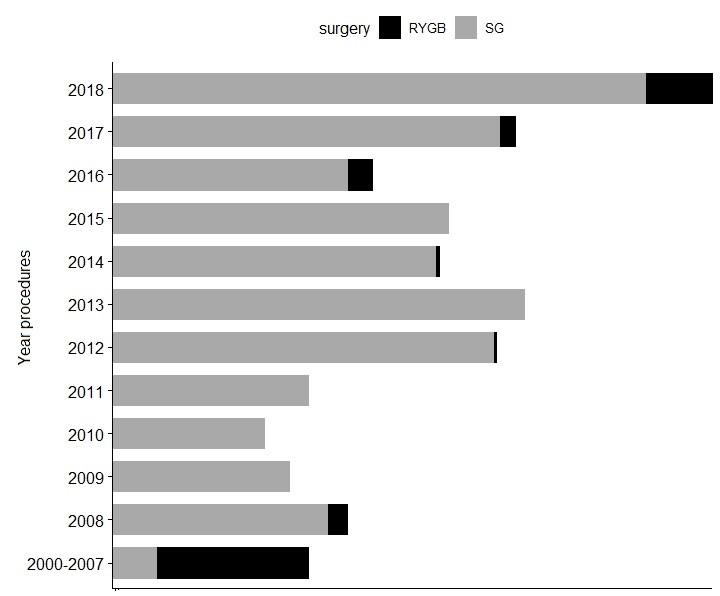
Figure 2: Bariatric surgery utilization trends over time, by procedures types.
Distribution of the number of bariatric surgery procedures from years 2000 to 2018. Roux-in-Y gastric bypass (RYGB) is show by the dark gray bars, and Sleeve gastrectomy (SG) by the light gray.
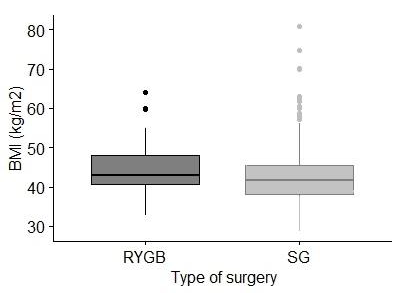
Figure 3: Body mass index by bariatric procedure types.
Box-and-whisker plots of body mass index (BMI) by surgery procedure types. Roux-in-Y gastric bypass (RYGB) is shown by the dark gray box and sleeve gastrectomy (SG) by the light gray box. The lines through the middle of the boxes are the means. The tops and bottoms of the boxes are the standard deviations.
Discussion
According to recent OECD data, Chile, a developing country, tops its list of obesity and overweight (74%), surpassing Mexico (72.5%) and the United States (71%) [4]. These data are reaffirmed with the latest National Health Survey, which shows an important increase of the obesity and morbid obesity from 21.9 % to 25.1 % and from 1.3 % to 2.3%, respectively, in the last 7 years [5,12]. Currently, it is estimated that in Chile there are about 500.000 morbidly obese people, who are eventual candidates for BC, an amount that according to projections is increasing. Although, the National Health Fund has annual coverage of 400 BC per year, it is insufficient considering the amount of morbidly obese people that currently exist in the country. It must be considered that, because BC is not routinely indicated for obese patients, the option of performing a SG versus RYGB was made according to a multidisciplinary team evaluation, considering comorbidities such as hypertension or type 2 diabetes. Effectively, as expected, SG patients had a higher prevalence of high-risk metabolic diseases as hypertension, type 2 diabetes, and insulin resistance. They also had higher rate of hypothyroidism, dyslipidemia and skeletal muscle diseases before surgery. As observed in this study, SG is the type of BC most performed followed by RYBG procedures, in public and private hospitals both in Chile [13] and in other countries [14,15].
However, in a recent article, Sun et al., indicated that RYGB was the BC type most frequently reported procedure in England followed by SG [16]. Despite these differences, it is important to note that both techniques are effective in the remission of the more prevalent comorbidities of the morbid obese, like type 2 diabetes, insulin resistance and hypertension [17,18]. In this study, it was observed that most of patients were female, which is consistent with other studies that point to a higher prevalence of surgical treatment for obesity among women [19]. This difference could be associated with the fact that in Chile, as well as in other countries such as the United States and Canada, the prevalence of obesity is higher in women than in men, and that women seek more health services compared to men, mainly because they have a greater concern for their health [20,21]. It can be assumed that this higher prevalence is due to the search for an ideal beauty and positive attributes, both associated with thinness, deriving from the many social demands that fall on women [22,23], although specific reasons for this disparity remain unclear. Considering the characteristics of the sample, it was observed that the majority ages of bariatric patients fluctuate between 39 to 46 years, are married or single, and BMI > 40 kg/m2, like other studies [13,21].
Most patients did not present comorbidities prior to surgery, and the prevalent comorbidities in patients are the same as those observed in other studies, type 2 diabetes, hypertension, insulin resistance, hypothyroidism, dyslipidemia and skeletal muscle diseases [21,24]. Interestingly, a higher prevalence of H.pylori (56%) diagnosed prior to surgery was observed, compared with similar studies that report 37.1% [25], and 22% [26] respectively. This difference may be due to the fact that the H. pylori infection is prevalent in 73% of the general Chilean population [27] and the social economic insecurity the patients face. However, the relationship between H.pylori and obesity is controversial, so further studies are needed in this area. It is known that obesity is a multifactorial disease that places individuals at risk for additional health compromising conditions such as biological, social consequences, psychological and psychopathology including depression and anxiety. In this study, it was observed that 93% of patients presented with psychiatric disorder including depression (47%) and anxiety (46%), higher than describe previously in another study of veteran women 60% (28% depression and 32% anxiety) [28].
One can also think that this higher prevalence is justified because most of patients were rural women, homemakers and sedentary. Therefore, it will be very interesting analyze the impact of BC procedure in these patients. Finally, none of the patients that died during the procedures were registered and only 3.2 % presented with immediate post-operative complications, which offers a satisfactory outcome when compared with other studies showing 5 to 10% [29]. These results obtained in the present study demonstrate that RYGB and SG BC procedures are feasible to be carried out in a public regional hospital with results comparable to those obtained in both public and private hospitals at the national and international levels. Although beyond the type of surgery applied, the therapeutic goals of surgery for morbid obesity are to improve quality of life and prolong life by counteracting the lifeshortening effect of obesity and its comorbidities, the future and ongoing investigations will provide evidence on the long-term benefits and risks of these most used bariatric procedures in current clinical practice.
This study presents some limitations, such as related to the external validity of our findings, because BARCO represents rural populations therefore, some results may not be applicable to residents of large urban areas. Here we report the baseline characteristics of BARCO´s patients, to provide a basic description of the sociodemographic, anthropometric measurements, principal comorbidities, mental health, lifestyle habits, clinical, and postsurgical complications of patients undergoing BC. In conclusion, given that BARCO is the largest cohort of the public health system patients operated of BC in Chile, these longitudinal data could be used to evaluate the effectiveness of the Chilean public policies related with the BC to treat the morbid obesity. Future and ongoing research will provide evidence on the long-term benefits, risks, and effectiveness of these bariatric procedures in reducing cardiometabolic morbidity, mortality related to obesity, and maintaining long-term weight loss. So, among the findings, the presence of Helicobacter pylori and the high prevalence of psychiatric disorders stand out as relevant factors for investigation in future studies.
For More Articles: Biomedical Journal Impact Factor: https://biomedres.us

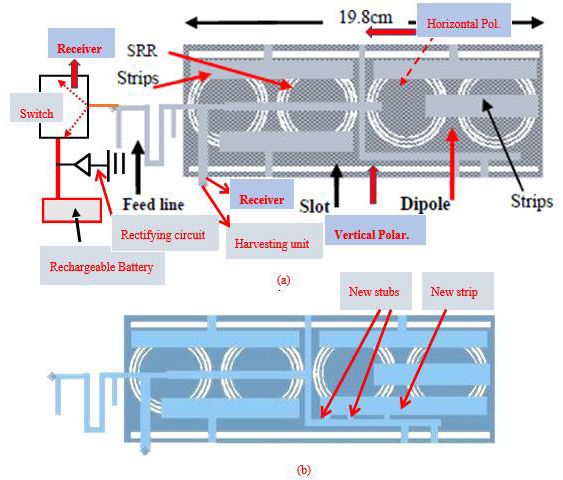
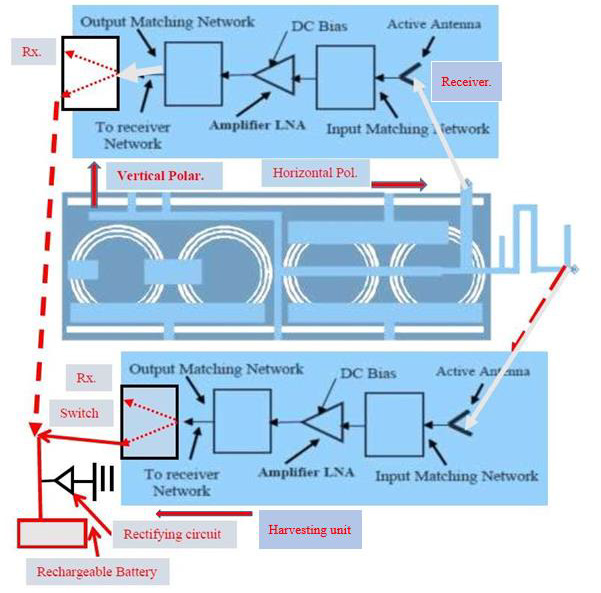

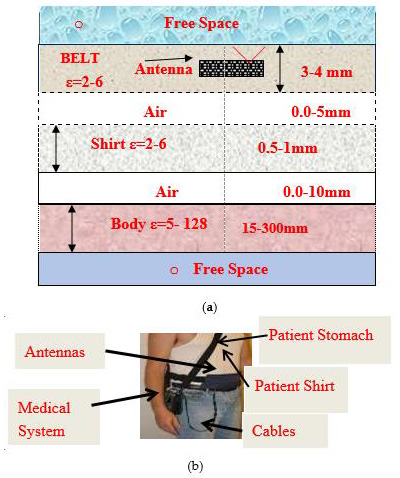

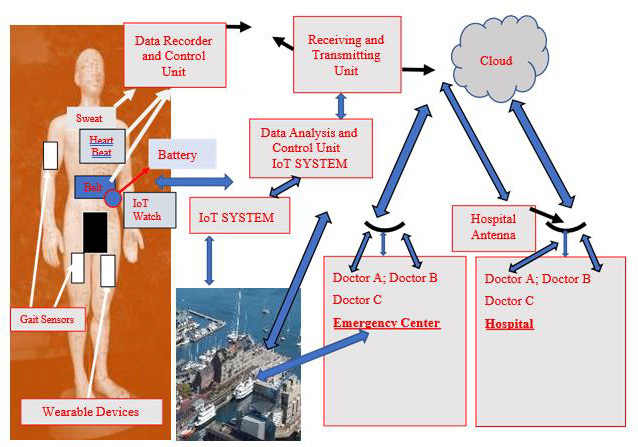
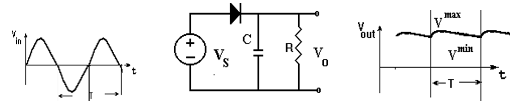
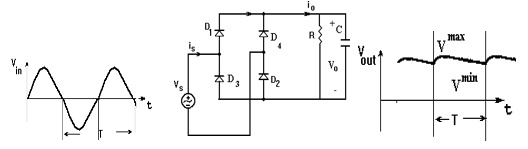
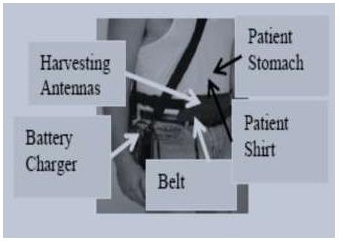
 The rectifier output voltage may be improved by connecting a capacitor in shunt to the resistor as presented in (Figure 19). The full wave rectifier efficiency is 81.2%. Energy harvesting systems provide green renewable energy and may eliminate the usage of power cords and the need to replace batteries frequently. Wearable RF System with energy harvesting unit for IoT, 5G, and healthcare devices is presented in (Figure 20). The wearable harvesting module with a compact battery charger is placed on the patient shirt as shown in (Figure 20) [46,47].
The rectifier output voltage may be improved by connecting a capacitor in shunt to the resistor as presented in (Figure 19). The full wave rectifier efficiency is 81.2%. Energy harvesting systems provide green renewable energy and may eliminate the usage of power cords and the need to replace batteries frequently. Wearable RF System with energy harvesting unit for IoT, 5G, and healthcare devices is presented in (Figure 20). The wearable harvesting module with a compact battery charger is placed on the patient shirt as shown in (Figure 20) [46,47].