Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Recent Trends in Analytical Techniques for Impurity Profiling
Quality and purity parameters remain under the spotlight while focusing on the safety of the drug product. The imp urities have been defined by the International Conference on Harmonization (ICH) guidelines to be the component of a new drug product, which is not the drug substance, nor the excipient added in the formulation. However, no drug substance and product is 100% pure, if one looks into depth for the analysis of impurities in the product. Considering this, guidelines have established the limits of impurity identification according to the daily dose of the drug products [1]. Three types of impurities are known and are classified by ICH as; organic, inorganic, and residual solvent impurity based on the nature and source of origin. Toxicity of impurities is the reason behind the continuing approach to detect and control them in pharmaceutical drug products. Interestingly, a smattering of impurities does not pose health risks while some have the potential to cause significant damage to human health including physiological damage, organ- and genotoxicity [2]. Consequential toxicities of impurities have been continuously investigated and reported in the active pharmaceutical ingredient (API) and synthesis materials of numerous drugs including pantoprazole [3], ceritinib [4], ranitidine [5], metformin [6], atorvastatin [7] and many more. Impurity profiling is the principal step towards controlling impurities in pharmaceuticals. The process of identification refers to) and qualification (acquiring and evaluating biosafety data) of impurities are the two main components ascertained during impurity profiling.
Outstanding advances have been observed in the development of analytical instruments for impurity profiling of pharmaceuticals. A brief overview of recently emerged and increasingly used techniques are covered in this editorial. Mass spectrometry (MS) has found significantly increasing applications in the analytical field including analysis of impurities, proteomics, pollutants, and polymers. The different forms of MS including inductively-coupled plasma MS (ICP-MS), ultra-performance liquid chromatography – MS (UPLC-MS), liquid chromatography-quadrupole time-offlight high-resolution MS (LC-Q-TOF-HRMS), vacuum outlet gas chromatography MS (GC-MS), Fourier transform ion cyclotron resonance MS (FT-ICR-MS), and other sophisticated techniques were used in impurity profiling purposes. Drugs including alfentanil hydrochloride [8], arginine vasopressin [9], difluprednate [10], cefteram pivoxil [11], alalevonadifloxacin [12] and many other have been recently profiled for impurities by MS techniques. On the other hand, electrophoretic and spectrometric techniques have also been brought into use for impurity analysis. [13] has employed nuclear magnetic resonance (NMR) for the impurity analysis in rat urine and feces. Interestingly, analytical methods for impurity profiling have also been developed using capillary electrophoresis. Impurity profiling of drug products containing biomolecules, drugs with stereochemical centers, and biopharmaceuticals can be performed using capillary electrophoresis [14].
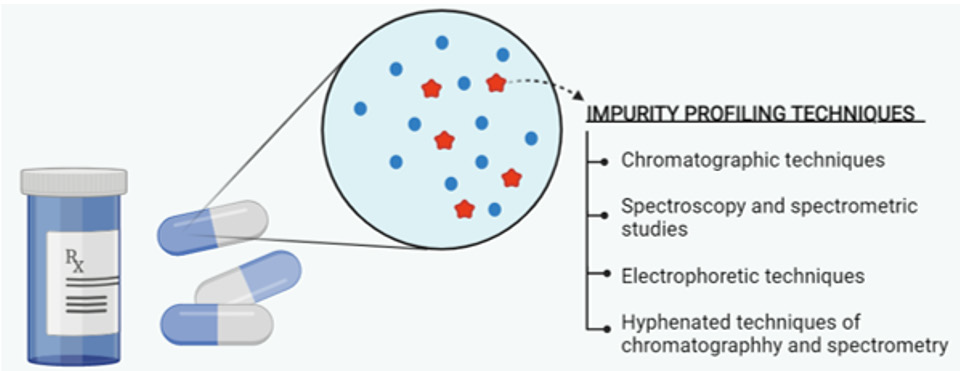
The technologies employed in impurity profiling are depicted in (Figure 1). Besides, maturing updates in chromatographic separation have been developed to efficiently execute a broad range of functions. Chromatographic techniques including hightemperature liquid chromatography (HTLC), hydrophilic interaction liquid chromatography (HILIC), supercritical fluid chromatography (SFC), UPLC, GC, and size exclusion chromatography (SEC) have established their scope of utilization in impurity profiling of drug products. Moreover, the hyphenation of chromatography with spectrometric techniques is also practiced. The equipment update in chromatographies for column and detector systems has also been observed. The control of impurities in drug products can be done if analysed. The methods of analysis have got significant advancements in recent years. The chromatographic and spectrometric systems are continuously getting new updates and being merged to expand their scope of applications. Observing at a large scale, the hyphenation of chromatographic and spectrometric methods is mostly used for impurity profiling. However, specific analytical methods for impurity profiling of drugs need to be developed.
Figure 1: Overview of techniques employed in impurity profiling.
A Case of Portal System Formation by Direct Joining of the Inferior Mesenteric Vein with the Superior Mesenteric Vein Observed in Anatomy Practice
Introduction
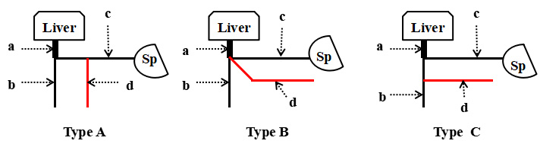
The inferior mesenteric vein (IMV) in humans flows into the portal vein (PV). In addition to the IMV, major veins constituting the portal system flowing into the PV include the superior mesenteric vein (SMV) and splenic vein (SV), and anomalies are frequently observed upon the joining of each vein. Anomalies have been also reported in gross anatomical studies [1,2,3] and on computed tomography (CT) [4-8]. Normally, the IMV ascends on the dorsal surface of the parietal peritoneum, distributes in the dorsal surface of the transverse colic attachment site, and enters the inferior margin of the pancreas, from where it flows into the SV, connecting to the PV. Regarding anomaly of this inflow region, there are 3 types: Type A directly flowing into the SV, Type B flowing into the SV/SMV junction, and Type C directly flowing into the SMV (Figure 1).
Figure 1: Inferior mesenteric vein 3 variations
• Type A) Variation of the venous drainage pattern of the inferior mesenteric vein into the splenic vein
• Type B) Variation of the venous drainage pattern of the inferior mesenteric vein into the junction between the splenic vein and the superior mesenteric vein
• Type C) Variation of the venous drainage pattern of the inferior mesenteric vein into the supeiror mesenteric vein.
a. Portal vein
b. Superior mesenteric vein,
c. Splenic vein
d. Inferior mesenteric vein
e. Sp: Spleen
In gross anatomical reports, Types A, B, and C accounted for 37, 21, and 42% of 112 autopsied bodies, respectively, in a report from Weinhaus [1], 65, 18, and 12% of 85 autopsied bodies, respectively, reported by Zilaie [2], and 73, 20, and 6% of 11 autopsied bodies reported by Kaur [3]. In CT reports, Types A, B, and C accounted for 54, 17, and 27% of 300 cases, respectively, in a report from Papavasiliou [4], 56, 18, and 26% of 54 cases, respectively, reported by Graf [5], 68.5, 7.60, and 18.50% of 102 cases, respectively, reported by Sakaguchi [6], 48.5, 10.6, and 40.9% of 66 cases, respectively, reported by Arimoto [7], and 40, 30, and 20% of 916 cases, respectively, reported by Krumm [8], demonstrating a slight difference in the frequency of each type (Table 1).
Table 1: Drainage site of IMV and frequency of occurrence. IMV= inferior mesnteric vein, SV= splenic vein, SMV= superior mesenteric vein, GA= gross anatomy, CT= computed tomography.
We report a case of direct joining of the SMV constituting the portal system in a corpse observed during anatomy practice. Embryologically, partial atrophy and disappearance of the venous system occur from the bilateral vitelline veins and their anastomotic branches as the intestine rotates at approximately 6 weeks of embryogenic age [9-12]. At this time point, a certain abnormality may have occurred when the distribution of bilateral vitelline veins started to become that observed in adults around the intestine through their development and regression, forming an anomaly in the IMV inflow region.
Case Report, Observed Body and Methods
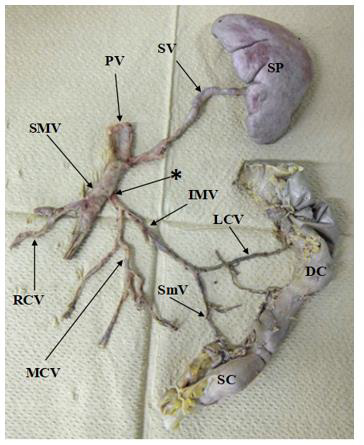
The anomaly of the IMV noted in an 89-year-old female (autopsy number 1989: senility) donated to Kanagawa Dental University for anatomy practice in the fiscal year of 2019 was excised using gross anatomical techniques, and the SMV, IMV, SV, and spleen were excised while connected to the PV (Figure 2). This report was prepared based on the ethical codes of the Japanese Association of Anatomists after approval (approval number: 557) by the Kanagawa Dental University Research Ethics Committee. There was no COI-related organization or institution.
Figure 2: Anatomic variants of the inferior mesentric vein (IMV): reaely drainage of the IMV into the superior mesentric vein (SMV) can be found. SP= Spleen, DC= Descending colon, SC= Sigmoid colon, PV= Portal vein, SV= Splenic vein, SMV= Superior mesenteric vein, IMV= Inferior mesenteric vein, MCV= Middle colic vein, RCV= Right colonic vein, LCV= Left colonic vein, SmV= Sigmoidl vein, *= Location of the IMV drained into SMV.
Results
The SV from the splenic hilum ran on the top surface of the pancreas on the posterior surface of the gastric corpus and flowed into the PV. The right and middle colic veins joined the SMV and flowed into the portal vein. In addition, the IMV joined by the jejunoileal vein joined at a site approximately 2 cm distal to the SPV from the region of the SMV and SV flowing into the PV (Figure 2).
Discussion
The portal vein is a functional blood vessel related to functions, such as detoxification and metabolism in the liver and bile production. The main veins constituting the portal system are the SMV, which transports nutrients absorbed in the jejunum and ileum, and water absorbed in a part of the ascending and transverse colon to the portal vein, the IMV, which transports water absorbed in the rest of the transverse, descending, and sigmoid colon and upper rectum, and the SV, which transports a component of red blood cells destroyed in the spleen, indirect bilirubin. Nutrients ingested by humans start from the oral cavity, are absorbed in the small and large intestine, and stored in the liver through the portal system. The portal system plays an important clinical role in absorption, metabolism, and storage of nutrients [13,14]. In addition, an increase in venous blood flow of the portal system was suggested to alter intrahepatic blood flow components of the portal vein, reducing the hepatic functional reserve. An anomaly was noted in this gross anatomical observation, in which the IMV joined the SMV and flowed into the portal vein. Anomalies of blood vessels constituting the portal system slightly differ among reports [1-8] but as shown in Table 1, the mean frequency of Type C in which the IMV directly joins the SMV was 24.1%.
Many veins constituting the digestive system gather in the portal vein and congenital abnormality in the distribution of the portal vein is considered markedly rare, even though the embryological timing is the same as that of the bile duct and celiac artery system. During development of the portal vein, 2 vitelline veins that develop from the yolk sac at 4 weeks of embryogenic age distribute to be positioned on the bilateral sides of the archenteron, which becomes the future duodenum, and then join the main vein and umbilical vein, and flow into the venous sinus. At 5 weeks of embryogenic age, 3 anastomotic branches of the bilateral vitelline veins on the cranial side, middle anastomotic branches, and anastomotic branches on the caudal side are formed on the ventral or dorsal side of the archenteron. At 6 weeks of embryogenic age, the venous system partially starts to atrophy, and disappears from the bilateral vitelline veins and their anastomotic branches as the intestine rotates [9-12]. At this time point, a certain abnormality may have occurred when the distribution of the bilateral vitelline veins around the intestine started to become that observed in adults through development and regression and formed an anomaly in the IMV inflow region. It has recently become possible to acquire detailed information before surgery due to the development of imaging diagnostic methods, including angiography, in all fields, thus increasing the frequency of surgical approach to the portal system in the digestive field. By identifying abnormalities in the distribution of the portal system before surgery, decisions regarding the surgical approach to the portal system can be easily made and its limitations are known.
For digestive surgery, CT is essential for treatment, and abnormality of the portal system distribution can be accurately diagnosed by ultrasonography and angiography in addition to CT, being a promising auxiliary diagnosis. Moreover, there are many case reports of abnormality of the portal system distribution based on imaging diagnosis [4-8]. It is necessary to identify the venous system from venules originating in the jejunoileum and colon that join the main veins of the portal system, i.e., the SMV, IMV, and SV, to investigate not only approaches in digestive surgery, but also the states of liver function and nutrition in patients in all fields. For anomalies of the portal system, confirmation on imaging, and gross and clinical anatomical information are desired.
Successful Mobile ECMO In COVID-19 and Varicella Patient: Case Report
Up to this date the World Health Organization had recorded more than 270 million confirmed cases of SARS CoV-2 infection, with over than 5 million deaths. Many hospitalized patients developed critical illness, requiring extracorporeal membrane support. In Serbia, there is only one center with experience in this technique. Some patients develop severe form of acute respiratory distress syndrome and cannot be transferred to reference hospital just by using conventional mechanical ventilation. This case reported successful treatment and first interhospital transport in Serbia of severe SARS CoV-2 and primary varicella co-infection using extracorporeal membrane oxygenation.
Last year declaration of the coronavirus outbreak as pandemic by World Health Organization was followed by rising number of patients infected with SARS-CoV-2 requiring hospitalization and intensive care unit (ICU) admission [1]. Although mechanically ventilated patients fulfilled criteria for acute respiratory distress syndrome (ARDS) by Berlin definition of ARDS [2], some distinctive features of SARS-CoV-2 infection made this ARDS more difficult to treat [3]. The Surviving Sepsis Campaign Guidelines released in January this year suggested to use venovenous ECMO in mechanically ventilated adults with COVID-19 and refractory hypoxemia despite optimized ventilation, use of rescue therapies and proning [4].
Case Presentation
We present the case of thirty-nine-year-old male patient, without other pre-existing conditions, who was admitted to remote University Hospital due to the bilateral covid pneumonia, proven by PCR analysis of nasopharyngeal swab. During the sixteendays hospitalization period he was treated with oxygen therapy, corticosteroids, tocilizumab, and other supportive therapy. On the day of the planned hospital discharge, fever appeared as well as maculopapular rash on the skin of the face and in the oral cavity. Additional anamnestic data revealed that a few days prior to the hospital admission the patient’s children suffered from chickenpox. Serological enzyme-linked immunosorbent assay confirmed high levels of Varicella Zoster IgM antibodies and acyclovir treatment was initiated. The patient’s condition rapidly deteriorated, respiratory failure required invasive mechanical ventilation, including the trial of prone position, with PaO2/FiO2 ratio of 85. Hypotension was bridged with the use of vasopressors. Severe refractory hypoxemia with Murray Score for Acute Lung Injury of 3.5 was the indication for VV-ECMO.
ECMO circuit was set by ultrasound guided placing of stiff wires in the right jugular vein and right femoral vein, followed by radiographic confirmation of adequate wire positions. Next, the cannulas were placed and the ECMO procedure with ultraprotective mechanical ventilation (Volume Control Ventilation, Tidal Volume 280ml, PEEP 12cmH2O, RR 12, FiO2 0.6, plateau pressure 22cmH2O) was started. On Day 3, after the hemodynamic stabilization was achieved, the patient was transferred to our ICU. Although ECMO transports are considered as high-risk and complex, this was the first interhospital transport on ECMO in Serbia and it went neatly. Team members included an anesthesiologist accompanied by ICU physician and ICU nurse. No staff has been proven infected during transport. The duration of the transport, defined by the time of leaving the hospital until arriving to our ICU, was not greater than 15 minutes. Potential ECMO transport complications were reduced by using our previously made ECMO checklists for interhospital transport.
For the time while VV-ECMO was performed the patient tailored anticoagulation was done with use of heparin, with targeted APPT-R of 1.5-2.0. Functional antithrombin III level was always above 80%. We did not observe any thrombotic circuit complication, nor bleeding. Platelet count were at the bottom level of normal range. Native lung shunt was 37% at the beginning, while membrane lung shunt was 23% and there were no major deviations in shunt percentages during the procedure. On the eleventh day of ECMO procedure, ECMO weaning was successfully done. Specimens submitted for microbiological testing at admission were negative. However, ICU stay was accompanied by Acinetobacter cloaceticus ventilator associated pneumonia treated with combined intravenous and nebulized colistin. Direct therapy led to significant clinical improvement within 24 hours. The day after ECMO weaning the patient was extubated. Nevertheless, severe ICU delirium along with urosepsis appeared so the patient was reintubated.
Bacteriological analysis of urine confirmed the presence of Enterococcus faecalis, wherefore carbapenem was added to the therapy. After three days the patient was successfully weaned from mechanical ventilation again. Three weeks after ICU admission he was transferred to the step-down unit. Further hospital stay was accompanied with intensified respiratory rehabilitation, cough, and expectoration stimulation. With the help of a physiotherapist the patient managed to start walking and preform active exercises a week after ECMO weaning. A color duplex scan of veins and arteries of the lower extremities was performed and was described as normal, while a color duplex scan of the neck and arms showed partial thrombosis in the jugular vein where ECMO cannula was placed. After thirty days of hospital treatment the patient was discharged home. He was recommended to use a home oxygen concentrator until the scheduled check-up as well as apixaban.
Discussion
In this paper we reported a case of SARS-CoV-2 and primary varicella co-infection resulting in bilateral pneumonia which progressed to acute respiratory distress syndrome requiring mechanical ventilation and ECMO. To our knowledge, this is the first reported case of the kind in adults with such devastating consequences. We searched PubMed, Cochrane database, Toxnet, Cinahl. Key words were varicella, COVID-19, coinfection, ARDS, ECMO. Coronaviruses belongs to a family of enveloped positivesense single-stranded RNA viruses [5]. A novel coronavirus named Severe Acute Respiratory Syndrome Coronavirus 2 causes COVID19 [6]. As of January 2020, more than 270 million people were tested positive for SARS CoV-2, with more than 4 million deaths worldwide [7]. It was first described in Wuhan, China, and soon it led to a global health crisis. There is a long list of symptoms and signs associated with COVID-19 such as fever, dry cough, aches and pains, diarrhea, headache, loss of taste and smell, skin rash, etc. Varicella-zoster virus is highly contagious a -stranded DNA virus that belongs to Herpesviridae family. It causes varicella (chickenpox) as a primary infection, which usually affects children under age of ten in parts of the world where vaccine against varicella is not available. Reactivation of the virus causes zoster (shingles) [8,9].
Interaction between these viruses is unknown. The immunological features of COVID19 and varicella separately are complex enough and adding tocilizumab in that equation makes pathophysiological mechanism of this case even more difficult to understand and explain. Cell-mediated immunity is necessary for fighting against viruses and bacteria. However, SARS-CoV-2 infection affects T lymphocytes, leading to immunosuppressed state [10]. Data from other study described functional exhaustion of NK and CD8+ T cells with the increased expression of inhibitory receptor NKG2A [11]. In addition to the above, humoral immune response have important role in COVID-19 infections [12].
VZV sets off robust innate and acquired immune responses [13]. While it causes mild disease in most children and healthy adults, immunocompromised patients are in risk of developing complications like pneumonia, secondary bacterial infections [14,15]. Latest published data confirmed that T-Cell mediated immune response is essential for preventing life-threatening VZV infections [16]. Other mechanisms causing immunosuppression include use of corticosteroids and IL-6-receptor-blocker (Tocilizumab) for COVID19 treatment which occurred in early phase of hospitalization. Tocilizumab is a humanized, monoclonal, antihuman interleukin-6 (IL-6) receptor antibody. It is approved for treatment of rheumatoid arthritis, giant-cell arteritis, cytokine releasing syndrome [17-21]. Based on preliminary non-peer reviewed report from Recovery trial group Tocilizumab may improve the course of COVID-19 [22]. However, in our case, this therapy probably additionally altered immune response and enabled VZV to cause severe pneumonia. Another risk factor for severe form of disease in our patient is cigarette smoking.
Our patient did not have history of chickenpox, and he was not vaccinated against varicella. Latency time between last contact with his children and development of skin lesions was almost three weeks. Alternative diagnosis of insect bite was ruled out because he was hospitalized at the moment of appearance of skin lesions, and continuously monitored during treatment for COVID-19. Also, patient did not report any insect bites. Type and distribution of skin and mucosa lesions was typical for varicella. In adult patients admitted in ICU requiring mechanical ventilation due to respiratory failure caused by varicella mortality rate is up to 50% [23]. Treatment options are antiviral therapy (acyclovir, valaciclovir, famciclovir, brivudine, foscarnet), corticosteroids, and respiratory support. Antiviral agents have been associated with reduction of severity of the disease, but there are no large, randomized control trials to confirm this. Benefit is greater in patients who receive antiviral drugs in first 24h of skin rash appearance.
Role of corticosteroids is controversial. In some studies utilization of steroids was not associated with mortality reduction but was associated with increased risk of superinfection [24,25]. Alternative treatment option in patients who develop severe ARDS refractory to optimized conventional care is ECMO. Based on what we know today ECMO is worth of considering in patients ARDS associated with COVID-19 [23]. Also, there are several case reports on ECMO procedure in patients with severe ARDS caused by varicella. They showed that ECMO was safe and effective [26,27]. Still there is not enough data on this topic to conclude whether ECMO should be used in these patients with more confident if needed. Interhospital transport of patients on ECMO is complex and associated with great risks. Therefore, it should be done by specialized teams with most experience to avoid complications. There are different models of organizing transportation of ECMO patients which can be considered [28]. In Serbia there are no specialized teams for interhospital transport patients on ECMO. In our case transport was organized by team of medical experts who is responsible for treatment ECMO patients in our hospital with technical help of colleagues from Institute for emergency medical aid Novi Sad. This case demonstrates that ECMO should be considered as rescue therapy in patients with profound respiratory failure caused by varicella refractory to standard care. Despite being complex and risky, interhospital transport patients on VVECMO is feasible if necessary.
Cancer CGH+SNP Unmasked Multiple Noncontiguous Deletions on Chromosome 7q and Cryptic Genomic Imbalances in a CMML Patient with an Apparently Balanced t(4;12) Translocation. A Case Report and Literature Re-View
Chronic myelomonocytic leukemia (CMML) is a clonal hematopoietic stem cell disorder with overlapping features between myelodysplastic syndromes (MDS) and myeloproliferative neoplasms and an inherent leukemic risk of ~15% over 3-5 years [1,2]. The 2017 WHO classification has recommended its partitioning into three categories based on peripheral blood and bone marrow (BM) blasts percentage [2]. In addition, the previously used 1994 FAB Cooperative Leukemia Group subdivision into a “dysplastic” (MD) and a “proliferative” CMML variant has been revived. Median age at diagnosis is 70 years, with a male preponderance. In many cases the diagnosis is occasional, with a median survival of 24-36 months [3]. Over the years several studies aimed to identify clinical and biological features associated with CMML survival outcomes, leading to the development of different prognostic models for individual patients’ treatment decision-making [4]. Like acute myeloid leukemia, CMML patients demonstrate ~10-15 mutations per kilobase of coding DNA regions, [5] while clonal cytogenetic abnormalities are observed in 20-30% of cases, including +8, -Y, chromosome 7 abnormalities, +21, and complex karyotypes [1]. In 2014 an international collaborative study between Mayo clinic and French consortium stratified CMML patients into three cytogenetic risk groups: high: complex karyotype, chromosome 7 abnormalities, monosomal karyotype; intermediate: +8, +21, others; and low: normal karyotype, -Y, der(3q) [3].
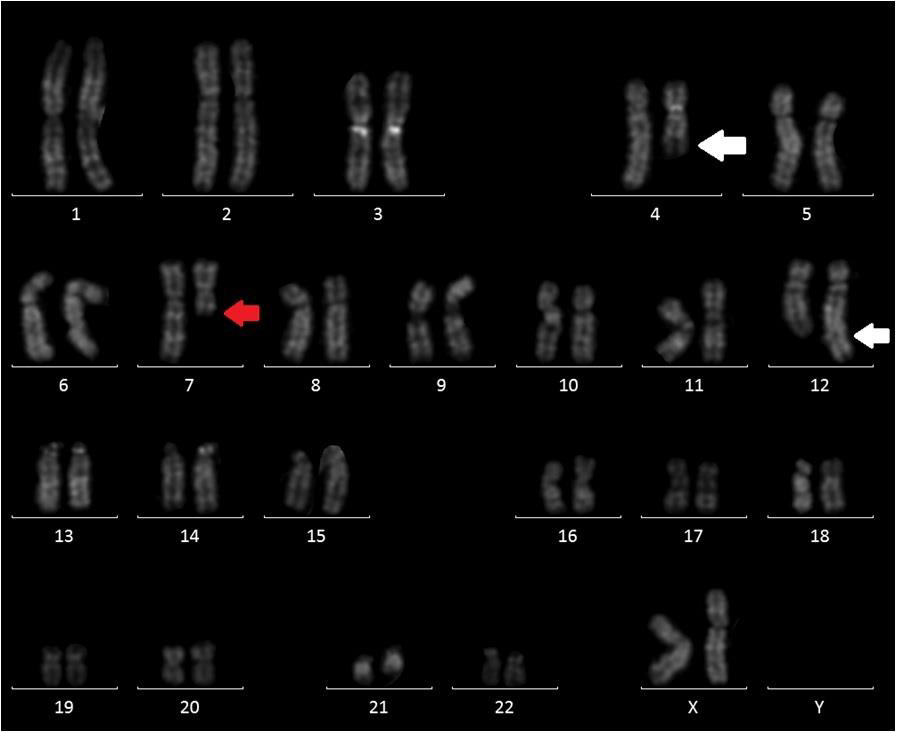
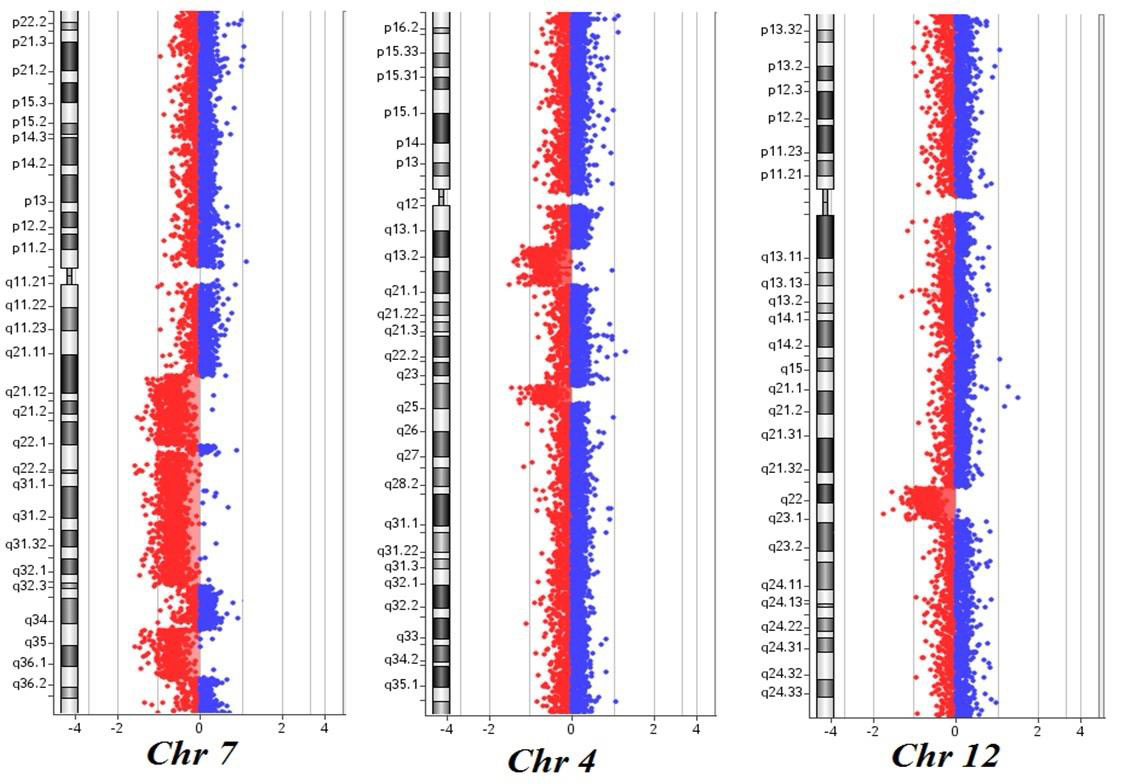
Here, we describe the case of a 76-year-old patient who was admitted to our hospital because of suspected CMML and for whom an array CGH was performed to better define the genomic imbalances at submicroscopic level and identify involved genes. In November 2018, a 76-year-old woman was referred to our hospital because of persistent monocytosis. A BM biopsy was then performed, showing increased age-adjusted cellularity and granulocytic proliferation associated with dyserithropoiesis and dysmegakaryopoiesis. A diagnosis of CMML-1, MD-subtype, was made according to the 2017 WHO classification. BM cytogenetic analysis revealed a karyotype characterized by the presence of two different cell lines, the largest one [18/20 metaphases] with an interstitial deletion of chromosome 7q at the bands q21-q36 and an apparently balanced translocation between chromosomes 4q24 and 12q15. Altogether, the karyotype was 46,XX,del(7)(q21q36),t(4;12) (q24;q15)[18]/46,XX[2] (Figure 1). A Cancer CGH+SNP array was then performed to define the real nature of the translocation. Array CGH analysis unveiled the t(4;12) unbalanced nature with three cryptic genomic imbalances: two deletions on chromosome 4 (one of 4.7Mb at band q24 spanning the bases 101944715-106679408, and one deletion of 10Mb at bands q13.1-q13.3, spanning the bases 64116915-74323464) and one deletion of 6Mb on chromosome 12 at bands q21.33-q23.1, spanning the bases 90077323-96215823 (Figure 2).
Figure 1: QFQ-banding abnormal karyotype of patient: white arrow showing the t(4;12) and red arrow the interstitial deletion of chromosome 7.
Figure 2: Cancer CGH+SNP array results of the patient: three noncontiguous deletions on chromosome 7q at bands q21.11-q22.1, q22.1-q32.2 and q34-q36.1; two deletions on chromosome 4 at bands q13.1-q13.3 and q24; one deletion on chromosome 12 at bands q21.33-q23.1. The breakpoints are according to the 37 build (March 2009) of the Human Genome Reference Consortium (GRch37/hg19).
Furthermore, the 7q deletion was composed of three noncontiguous deletions: a 15Mb loss at bands q21.11-q22.1, spanning the bases 82769585-98521920, a 30Mb loss at bands q22.1-q32.2, spanning the bases 100139536-130148949, and a 11Mb loss at bands q34-q36.1, spanning the bases 140529849- 151559567. Finally, the analysis did not detect any copy number neutral loss of heterozygosity. Based on these results, NGS analysis was then performed, showing the presence of TET2 c1870 (VAF 25.4%) and c3344 mutations (VAF 38.9%). These results are consistent with the presence of a normal cell line together with an abnormal one. As already reported in the literature, chromosome 7 aberrations are found in about 20% of CMML patients harboring cytogenetic abnormalities, classifying these cases as at high cytogenetic risk. On the long arm of chromosome 7 map several tumor suppressor genes and their loss of function via monoallelic deletion may play a role in CMML pathogenesis and progression. At present, tumor suppressor genes in 7q are believed to operate in a haplo insufficient manner, and new powerful technologies such as microarray comparative genomic hybridization allows to overcome this limit and new genes located in bands 7q22 and 7q34-36 have been discovered [6,7]. While chromosome 7q cytogenetic analysis could not detect the precise intervals and the genes involved in the deletion, with array CGH we identified five genes already known to have a potential role in tumorigenesis.
In details, EZH2 is a component of the polycomb repressive complex-2 and encodes for a methyltransferase, initiating epigenetic silencing of many genes involved in different cell pathways. CUX1 encodes for a homeobox transcription factor involving in tumorigenesis, with a possible role as a tumor suppressor gene. SAMD9 and SAMD9L compound heterozygous deletions with high frequency in adult and childhood myeloid leukemia. In contrast with previous reports, KMT2C/MLL3, despite being an epigenetic regulator acting as a gene silencer, is not involved in our deletion. In our patient, together with a del7q, we found an apparently balanced t(4;12) translocation, which was proved to be unbalanced by array CGH. The three deletions found on chromosome 4 involve many OMIM genes, with TET2 and NFKB1 playing an important role in disease progression. Somatic TET2 mutations occur in ~60% of CMML, even if they are not specific for the disease and can also be detected as a part of age-related clonal hematopoiesis. Moreover, they have not proven to negatively impact either on overall (OS) or leukemia-free survival [8,9]. On the contrary, in the absence of clonal ASXL1 involvement, TET2 mutations were shown to favorably impact on OS [10]. Interestingly, we found the coexistent loss of EZH2 due to the 11Mb deletion at bands q34-q36.1 of chromosome 7. Indeed, its deletion is known to contribute to myeloid tumorigenesis in association with TET2 variations. The 6Mb deletion of chromosome 12q involving 25 OMIM genes was not commonly described in association with hematological malignancies, so that its biological significance remains unclear. At the same time, we cannot exclude that some of the involved genes could play a minor role in disease onset or progression.
In conclusion, this case shows both common recurrent rearrangements and rare copy number alterations. Clarifying the role of these alterations could contribute to elucidate the mechanisms involved in CMML leukemogenic network, possibly contributing to define a more accurate prognosis. This case also underlines the importance of including different molecular cytogenetic tests in CMML diagnostic workup, so providing prognostic information and a strategy to develop personalized therapies, especially considering that NGS analysis is not always available.
Perception of the Quality of Life of People with Kidney Transplants and Transplant Candidates in Mérida, Yucatán, México
Introduction
Chronic kidney disease (CKD) affects around 11% of the population over 20 years of age worldwide, with an increase in incidence in recent years [1]. Peritoneal dialysis, hemodialysis, and kidney transplantation are treatments that have been effective in increasing the life expectancy of people with CKD [1,2]. In the last three decades, the analysis of quality of life has been integrated as an indicator of the evolution of the state of health in patients with CKD to see beyond the number of years of survival. The quality of life is, according to the WHO, “the perception that an individual has of his place in existence, in the context of the culture and value system in which he lives and in relation to his objectives, his expectations, his standards, your concerns. It is a concept that is influenced by the physical health of the subject, their psychological state, their level of independence, their social relationships, as well as their relationship with the environment ”. This concept encompasses both objective and subjective aspects that reflect the degree of physical, emotional, social and economic well-being of each individual. The analysis of the quality of life in people with CKD allows us to understand the impact of the disease and its treatment, to know more about the patients, how they evolve and how they adapt to the organic alteration [3,4].
At present, the analysis of the quality of life in people with CKD seeks to generate evidence, qualitative and quantitative, to facilitate: the process of assessing human needs and the implementation of quality interventions in healthcare sectors [5]. In health sciences, phenomenological research, and those with a qualitative approach in general, generate evidence that serves as a guide to practice that is sensitive to the realities of the people to whom care is directed, their cultural diversity and the contexts in which their lives unfold [6,7]. In studies related to quality of life in transplanted people and candidates for kidney transplantation, the participants manifest as the main human responses: recurrent hospitalizations, uncertainty about the work situation, deterioration of body image, deterioration of sexual functionality, dependence on third parties, stress and guilt [2,8-12]. Specifically, people who are candidates for kidney transplantation show anxiety and depression as the main human responses. Transplants report acute rejections, side effects of medication, and emotional instability; [12-14] immediately, after transplantation, they can perceive liberation with respect to dependence on renal replacement therapy, but as time passes they have to face various adaptation problems: side effects of medications, medical and social complications, among the latter the reincorporation of work, social and family life [12,13,15].
The analysis of quality of life, with its respective components and human responses in patients with a history of CKD is recent. Therefore, the inherent needs of the nursing care process may go unnoticed when directing care for people with these characteristics. Although there are numerous studies that quantitatively address health-related quality of life, [4,16,17] qualitative studies such as this one provide particular evidence to integrate it into the holistic process of the nurse-patient relationship at different levels of care [18,19]. Therefore, the objective of this study is to analyze the perception of quality of life of people with kidney transplants and candidates for kidney transplants treated at the High Specialty Medical Unit of Mérida, to identify related human responses through a phenomenological approach. interpretative.
Methodology
Design
A qualitative study with an interpretive phenomenological approach was carried out. From this design it is possible to understand the experiences and the articulation of similarities and differences in the meanings and human experiences of people with kidney transplants and kidney transplant candidates. Although it is not possible to make generalizations from the results of this study, particular data are achieved with transferability to other populations with similar characteristics [6,7,20]. This article followed the COREQ criteria (Consolidated criteria for reporting qualitative research) to enhance its quality and clarity [21].
Study and Sampling Population
An intentional sampling was carried out, obtaining a final sample was made up of 11 people with a history of CRI: 7 candidates for kidney transplantation and 4 transplants, who received health services at the High Specialty Medical Unit of Mérida (UMAE) of the Mexican Institute of Social Security (IMSS) during the period from November 2019 to February 2020.
Data Collection
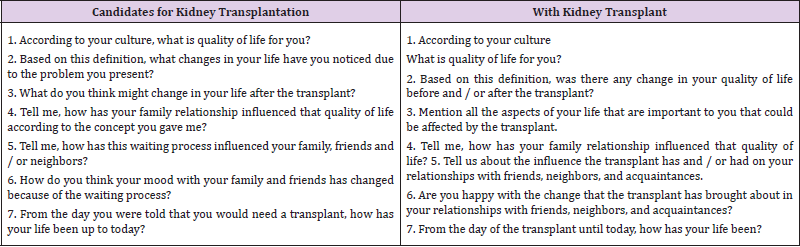
The data were collected through semi-structured interviews conducted during their follow-up consultations. Interviews lasted 30 to 40 minutes, were recorded in audio format and field notes were taken. Table 1 presents the questions asked during the semistructured interviews.
Table 1: Questions from the semi-structured interviews.
Ethical Considerations
The study respects the ethical principles: beneficence, nonmaleficence, justice and autonomy. The study research protocol, with folio R-2018-785-129, was approved by the ethics committee of the High Specialty Medical Unit of the Mexican Institute of Social Security. The testimonies presented herein are referenced with codes to safeguard the identity of the participants.
Information Processing
The semi-structured interviews were transcribed verbatim and then analyzed through content analysis. This analysis process consisted of:
1) Coding the data and establishing a data index;
2) Categorize data content into meaningful categories; and
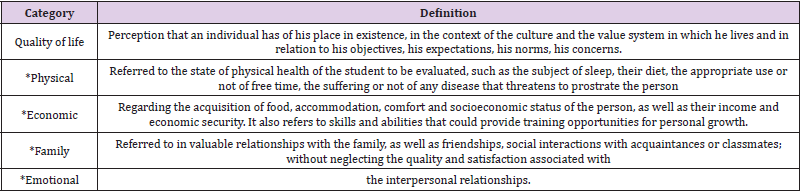
3) Determine the issues related, in this case human responses, with the previously defined categories. [7,22]. In the results section, tables are presented that allow the visualization of the analysis categories delimited in table 2 based on Urzúa and Caqueo [23], the human responses within the categories and, finally, the testimonies of the participants; all of the above accompanied by an interpretive narrative.
Table 2: Categories for grouping and analysis of qualitative data.
Note: *Categories of the concept of quality of life from Urzúa and Caqueo
Quality Criteria
Once the transcription of the interviews was completed, the 11 participants were asked to verify that the interpreted information was correct. Also the protocol related to the organization of the data, the detailed and meticulous description of the selection of the sample and the context in which the study is carried out, facilitate the possibility of transfer and reproducibility of the same under similar conditions, providing this otherwise qualitative quality criterion.
Results
Participant Characteristics
The years of age resulted with a median of 37 (mean 39) and SD = 13 in the 11 participants. In people who were candidates to receive KT, the median was 37 (mean 41) and in those with KT it was 35.7 years (mean 41), respectively. In this last group, two people were 6 months or less after having received RT, one was 1 year old and one person was 10 years after receiving this treatment. Table 3 shows that the majority of the total sample was made up of men who worked as employees.
Table 3: Sociodemographic characteristics of the 11 participants included in the study.
Quality
Once the transcription of the interviews was completed, the 11 participants were asked to verify that the interpreted information was correct. Also the protocol related to the organization of the data, the detailed and meticulous description of the selection of the sample and the context in which the study is carried out, facilitate the possibility of transfer and reproducibility of the same under similar conditions, providing this otherwise qualitative quality criterion.
Quality of Life: Perception in People who are Candidates for Kidney Transplantation
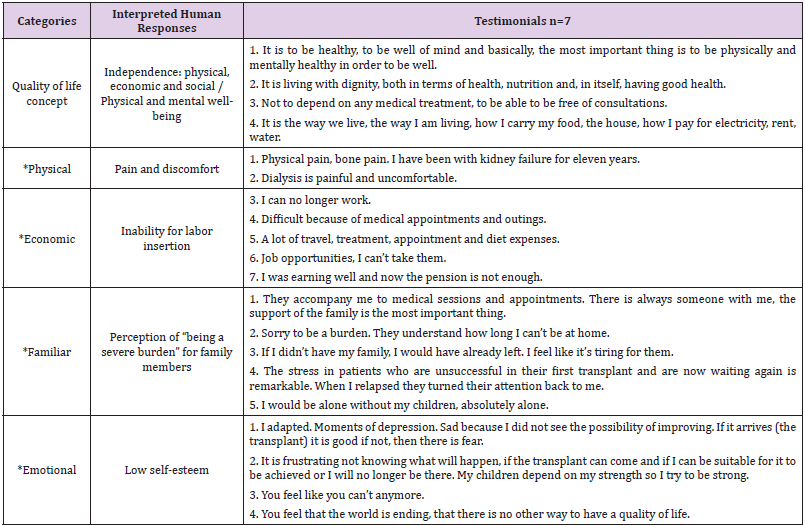
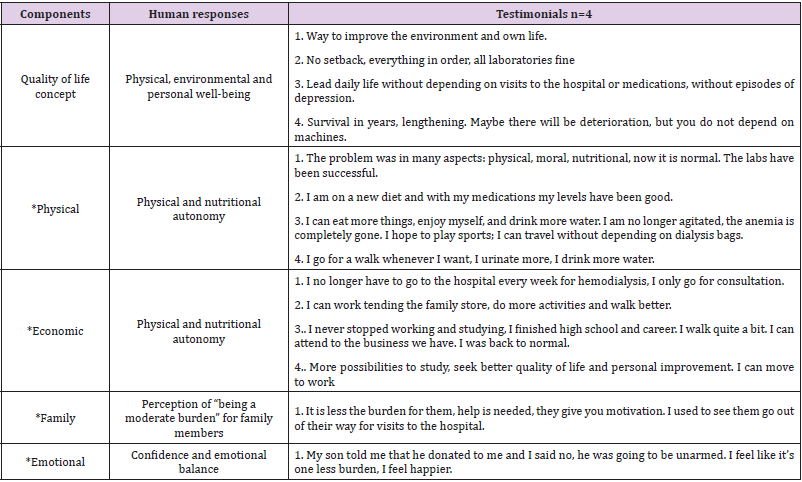
Table 3 shows the interpretations related to the categories: concept of quality of life with their respective domains: physical, economic, family and social, then the identified human responses are presented. Most of the participants stated that quality of life is to be well physically, mentally and emotionally, as well as having all the basic services and not depending on kidney replacement treatments: dialysis or hemodialysis. In the physical domain, people highlight discomforts, pain and discomfort related to the procedures of renal replacement therapies or of the body itself: chronic or bone pain, for example. These human responses largely condition the inability to enter the labor field. In the economic domain, the participants report that they are unable to carry out the activities of any job due to physical disability, and therefore, they consider that their monetary income from a trade or job is limited, scarce or nil. In addition, they highlighted that the economic resources are focused on financing the management of one’s own health: laboratory tests, transportation, extraordinary treatments, medical appointments and consultations, among others; These efforts are complicated precisely by the lack of monetary inputs. In the family domain, people identify the importance of the support, attention and understanding that they receive, received and expect to receive from their family in the ups and downs related to their state of health and well-being. In this regard, some express feelings of feeling a burden for their relatives due to the extra activities that the latter carry out in health care, which generates tension and uncertainty. However, the interviewees expressed the motivation generated by their family environment: mothers, children and grandchildren, among other ties, drive the desire to want to get out of their problem and be patients while waiting for the transplant.
In the emotional domain, each of the people interviewed expressed their affectation at different points that leads them to present low self-esteem: fear, frustration, depression, sadness and uncertainty are some of the emotions they expressed in their testimonies. Participants follow a continuous coping process, because not every day they feel with all the energy and motivation to continue with daily life. The emotional perception of the interviewees was reflected in their features during the interviews, points were touched that led them to tears, they expressed how difficult it is to live with a dysfunctional organ, the uncertainty before latent complications that can even lead them to lose life (Table 4).
Table 4: Quality of life: perception of kidney transplant candidates.
Note: *Categories of the concept of quality of life from Urzúa and Caqueo.
Quality of Life: Perception in People with Kidney Transplantation
Table 5 shows that most of the participants consider that quality of life involves physical, environmental and personal well-being as components. For one of the interviewees it means no longer depending on external factors to maintain life; another considered that the longer he can extend his life the better for its quality, he considered that discomforts are companions of life. In the physical domain, the interviewees expressed the freedom to carry out various activities and eat food without affecting their quality of life. They expressed that they can move and travel without thinking about the need to carry too many supplies related to their treatment. They also stated that they can eat food without causing discomfort or altering their clinical parameters, especially water, which was previously restricted. In the economic domain, the participants report that they have time and autonomy to build opportunities for insertion to trades, jobs and professional or educational training. One case mentioned that the ability to acquire economic resources improves their quality of life, another participant refers that they can work freely without thinking about the times of any kidney therapy, finally, one case reports that they returned to normal by taking fully these opportunities than before approached discreetly.
Table 5: Quality of life: perception of kidney transplants.
Note: *Categories of the concept of quality of life from Urzúa and Caqueo
In the family domain, the perception and feelings of being considered a burden for their families has decreased along with the amount of care related to kidney replacement therapies from which transplant participants are already exempt; People mentioned that despite the constant support of their relatives there was a physical distancing seeking to reduce the cross-infection of infections, a situation that has recently ended and they can share more time and experiences together. In the emotional domain, confidence and emotional balance were interpreted in the participants. Two people mentioned that they feel they have a new opportunity in life, to restart it and have new experiences that they previously did not consider possible. Two people mentioned the need to have confidence and know how to take the advice of health personnel: doctors and nurses. Finally, a participant described that he was overwhelmed by living a few days in isolation after his transplant, necessary to prevent infections, but at the same time accepting that it is necessary to improve his quality of life.
Discussion
The quality of life of people with a history of kidney disease is affected from the first clinical manifestations, QoL in this sector has shown deficiencies, low levels or areas of opportunity compared to the rest of the population [24]. Physical, environmental and personal well-being are part of the conception of quality of life in people with kidney disease, whether they have been transplanted or not. In the early stages of the disease, a series of negative perceptions of the disease and its immediate and intermediate quality of life are experienced that, ultimately, can influence their coping actions, these perceptions can trigger anxiety, depression, coping, autonomy, self-esteem and accelerated progression of the disease [25]. In the identification of human responses in patients with chronic kidney disease, the main physiological risks related to this pathology have been highlighted. Farias et. to the. point out the overestimation of human biological responses and those related to complications by the nursing staff who provide care to patients with nephropathies in a renal center. Among 24 diagnostic labels identified, the most frequent were “risk of infection”, “excess fluid volume”, “hypothermia”, among others whose main domains were located in Safety / Protection and Activity / Rest, on the other hand, “ low situational self-esteem ”was ranked 16th in frequency [26] corresponding to the Self-perception domain in the NANDA-I [18]. The above shows what Spilogon et. to the. (2018) points out as an area of opportunity in the nursing process since it has the flexibility and openness to consider the perceptions and preferences of the user, in this case of the patient with nephropathies [27].
In the emotional category, low self-esteem was detected in the participants with CKD without transplantation, and it is that a patient with CKD has recognition and esteem needs, therefore the people in charge of their care should promote favorable behaviors in coping with the pathology and adherence to treatment, avoiding judging and repressing the failures of our human condition [28]. In contrast, the participants who had received a kidney transplant showed confidence and emotional balance, something that could be considered normal after receiving the expected transplant according to Tucker et. to the [29]. From a quantitative approach, Rocha et. to the. point out that the higher the quality of life, the better the self-esteem assessment of people with chronic kidney disease after transplantation [30]. In the economic category, while people who had not received a kidney transplant conceived the inability to enter the job market among their perception of quality of life, those who had received a kidney transplant indicated more time and autonomy to build job and academic opportunities. Reports indicate that chronic kidney disease patients face many barriers to staying or joining the workforce after starting dialysis: few opportunities, lack of financial resources to invest, fatigue and other symptoms of kidney failure, potential loss of disability benefits or medical follow-up, dialysis programming and employer biases. The social perception that CKD patients cannot work completes a vicious cycle of low job expectations [25,31].
In the family category, the perception of “being a burden” for family members influences is an important component in the perception of the quality of life of people with and without kidney transplantation. The evidence indicates that family members of patients with a history of kidney disease manifest sleep interruptions, depression, anxiety, among other disorders associated with unforeseen responsibilities related to the treatment and logistics of their relatives; they must also deal with insufficient information, medication regimen and accompany periodic hospitalizations [32]. The NANDA International classifies problems in plausible diagnostic labels of interventions focused on promoting the health of individuals, the family. and community, we can cite: Risk of fatigue of the caregiver role, Tiredness of the caregiver role, Dysfunctional family processes, Willingness to improve family processes, among others [18]. In the physical category, participants without kidney transplantation identified pain and discomfort as a condition for quality of life, a common and often severe manifestation in various populations with CKD; with prevalence’s of 40% to 60%, it constitutes a strong imperative to establish the management of chronic pain as a clinical and research priority [33]. In this regard, the labels acute and chronic pain are available in the NANDA-I [18]. Although pain and physical limitation decrease after a kidney transplant, it is important to mention that the physical and nutritional autonomy indicated by the present participants can generate an excess of confidence and the acquisition of unhealthy practices. Regulated physical training by physiotherapy specialists appears to be safe in kidney transplant recipients and is associated with better quality of life and exercise capacity [34]. With regard to diet, the Mediterranean and DASH (Dietary Approaches to Stop Hypertension) diets have been shown to be the most beneficial dietary patterns for the population after kidney transplantation by focusing on less meat and food while increasing the intake of fresh foods and plant-based options [35]. Knowledge and awareness in the kidney transplant population should be a cornerstone of therapy and an integral part of nursing responsibilities.
Therefore, nurses must educate patients about self-care behaviors and remind them of the dangerous complications of abandoning them [28]. In the participants who had not received a kidney transplant, there was an expectation of receiving a kidney transplant to improve their quality of life and, from there, improve their quality of life. In this regard, we can mention the benefits in anticipation of receiving a kidney transplant mentioned by Santos et. to the. who in a group of people with Brazilian kidney disease detected that patients who were not waiting for a transplant had a risk of poor quality of life, mainly in the emotional and physical aspects; those who were not awaiting transplantation died more frequently in the following 12 months [36]. However, betting on kidney transplantation to improve the quality of life in patients with kidney disease is not entirely recommended, in this regard we can cite the studies by Schulz et. to the. and Smith et. to the. published in 2014 and 2019, [29,37] who reported that before transplantation, patients can overestimate the gains in quality of life without finding significant improvements in it after being transplanted. Kidney transplantation is not a guarantee of improvement in quality of life in all patients with kidney disease. In the present study, those people who had received kidney transplantation did not consider an absolute improvement in their quality of life. The literature indicates that kidney transplants can provide dramatic improvements in quality of life and health status, however, the effects on the improvement are not universal and patients live in constant uncertainty as they are aware of the probability of kidney dysfunction Graft [29]. There are samples that have indicated that the expectation about the functionality or rejection of the graft generates greater fear and uncertainty than death itself [38]. The results on the perception of quality of life in people receiving renal replacement therapy support the trend of the last decade focused on the analysis of this category beyond just assessing life expectancy [39]. Among the limitations of the present, the risk of bias due to the same interpretive approach and the inability to generalize the results to the study population stands out. To compensate for the above, criteria of methodological rigor were followed and from a particular context a search for generalities was made, reinforcing the results with respect to other studies (twenty-one).
Conclusion
In transplant patients, a perception of absolute quality of life or free from discomfort is not reached and human responses are still manifested that require care and interventions to achieve the maximum level of well-being. The construction of the concept of quality of life includes physical, mental, personal and social elements that are feasible to document and in which to carry out interventions for the benefit of trafficked persons and their families, it is evident that human responses not only obey physiological needs.
B Vitamin Intake and the Risk of Colorectal Cancer Development: A Systematic Review and Meta-Analysis of Observational Studies
Introduction
Recent cancer research has increased interest in lifestyle factors like diet, physical activity, stress level or habits which are influenced by socio-economical state and socio-behavioral factors as well. They affect the human physiology and have significant impact on the development of cancer and other diseases [1-3]. According to GLOBOCAN 2020, colorectal cancer (CRC) is the third most frequent cancer type and the second most common cause of cancer death worldwide, although around 40% of the cases would be preventable [4]. Countries with better and careful cancer prevention programs have more chance to fight against CRC [5]. Dietary intake of methyl donors (such as folate, choline, betaine, methionine and vitamin B2, B6 and B12) could have important role in cancer prevention by reducing the risk of cancer and could contribute to the success of cancer therapies and to reach better quality of life (QoL) of the patients [6-8]. Dietary methyl donors are food components, which provide methyl groups for the one-carbon metabolism, which consists of two main metabolic cycles: the folate cycle and the methionine cycle [9]. Methionine has a universal methyl group and can be added to several molecules; thus, its sufficient amount supports the normal DNA methylation [10]. It is also well known that inadequate DNA methylation may lead to development of cancer [6].
The optimal function of one-carbon metabolism requires specific vitamins as well as minerals. B vitamins are catalytic co-enzymes in these processes; therefore, they can influence the availability of methyl groups [10]. Moreover, B vitamins are important in energy-yielding metabolism, oxygen transport and neuronal functions. They play essential roles in basic metabolic pathways and fundamental cellular functions consequently have an impact on cognitive and psychological processes, including mental and physical fatigue [7,11]. Besides nutritional and other lifestyle factors, genetically determined components influence the development of CRC as well. One of these is the single nucleotide polymorphism (SNP) of the methylenetetrahydrofolate reductase (MTHFR) gene. MTHFR is involved in the one-carbon metabolism, where this enzyme activates folic acid. It has a common SNP at the position of 677 (MTHFR C677T). The heterozygous mutation (CT) results in a reduced enzyme activity around 65% of the normal level, while the homozygous (TT) mutation causes only 30% enzyme activity, and both reduce the level of DNA methylation [12-14].In this meta-analysis our aim was to systematically collect publicly available data, and summarize and update the scientific knowledge about the associations between dietary B2, B6 and B12 vitamin intake and the risk of CRC in adult patients, which has already published until 15th March 2021. Moreover, we aimed to highlight the importance of the need for standardization of the way how to explain the result of a meta-analysis as well.
Materials and Methods
Study Characteristics
Our systematic review and meta-analysis based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements [15] (Table S1) focused on vitamin B2, B6 and B12 intake and the polymorphisms of MTHFR (where data were collected from cohort and case-control studies, respectively), and their effects on colorectal cancer risk in adults.
Literature Search
We carried out a systematic scientific literature search in PubMed, Ovid-Medline, Web of Science (WOS) and ProQuest electronic databases to identify observational studies presenting results on the relationship between B vitamin intake and colorectal cancer risk. Searches were accomplished in all available years until 15th March 2021. We collected publications based on combinations of the following searching terms: B vitamins, vitamin B2, vitamin B6, vitamin B12, colorectal cancer and dietary intake (i.e. PubMed: B vitamins AND colorectal cancer, vitamin B2 AND colorectal cancer, vitamin B6 AND colorectal cancer, vitamin B12 AND colorectal cancer; Ovid-Medline: vitamin B and colorectal cancer and dietary intake; Web of Science/ProQuest: vitamin B2 and colorectal cancer, vitamin B6 and colorectal cancer, vitamin B12 and colorectal cancer). We used advanced search in case of Ovid-Medline, Web of Science, and ProQuest. Electronic search, study selection and review of selected papers were undertaken by two independent authors.
Study Selection and Quality Assessment
Identified records were screened by titles and abstracts and after removal of duplicated studies, publications were reviewed based on inclusion and exclusion criteria. Inclusion criteria were: 1. Publications had to be written in English. 2. Papers had to be original articles. 3. Patients had to be adults. 4. The exposure of interest was vitamin B2, B6 and B12. 5. The outcome of interest was the diagnosis of colorectal cancer. All studies with only animal or in vitro experiments were excluded. After screening process, the remained 35 studies were assessed by eligibility criteria, which were: 1. odds ratio (OR), relative risk (RR) or hazard ratio (HR) with 95% confidence interval (CI) had to be calculated in the article; 2. the studies had to be cohort or case-control studies (these only were accepted if they discussed the association between B2, B6 and B12 vitamin intake and MTHFR polymorphism in CRC. Articles, which met all the criteria were reviewed again and these publications formed the basis of our quantitative analysis. We applied the Newcastle-Ottawa Scale (NOS) for assessing the quality of included publications in our meta-analysis [16].
Statistical Analysis
We summarized the observed treatment effect sizes including odd ratios (ORs), confidence intervals (CIs) and weights of the studies using random effects model [17-19]. Overall ORs (combined effect size, CES) and the corresponding 95% CIs and 95% prediction intervals (PIs) were calculated. The studies were tested using I2 statistic and Cochran’s Q test. In order to identify possible sources of heterogeneity, we explored studies with outlier effect sizes using funnel plot and Galbraith plot [20]. We also used the “Trim and fill” method within funnel plot to estimate true effect size and the dispersion of the combined effect size (heterogeneity) [19]. In this process both observed and adjusted combined effects size (CES) were calculated with related CI and PI, respectively [21,22]. We carried out Egger’s regression test [23] and Begg & Mazumdar’s rank correlation test to inspect possible publication bias [24]. Publication and other biases of the individual studies were evaluated according to the information found in the original articles. All statistical analysis were implemented by the tools of Meta-Essentials [25].
Results
Literature Search
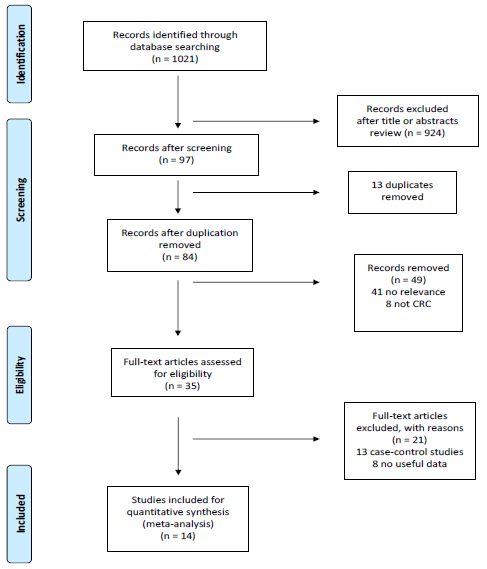
A total of 1021 articles (199 from PubMed, 178 from Ovid- Medline, 624 from WoS and 20 from ProQuest) were identified through the electronic search. After screening titles and abstracts and excluding duplicates, 84 items were reviewed according to inclusion and exclusion criteria. 35 articles went through full-text review of which 9 cohort studies focused on the effects of B vitamin intake on CRC risk and further 5 eligible items (case-control studies) discussed the connection between MTHFR polymorphism, CRC risk and B vitamin intake. Finally, 14 eligible studies were included in the quantitative analysis. The selection procedure is presented on the detailed PRISMA flow diagram (Figure 1).
Figure 1: PRISMA flow diagram of study selection for meta-analysis.
Study Characteristics
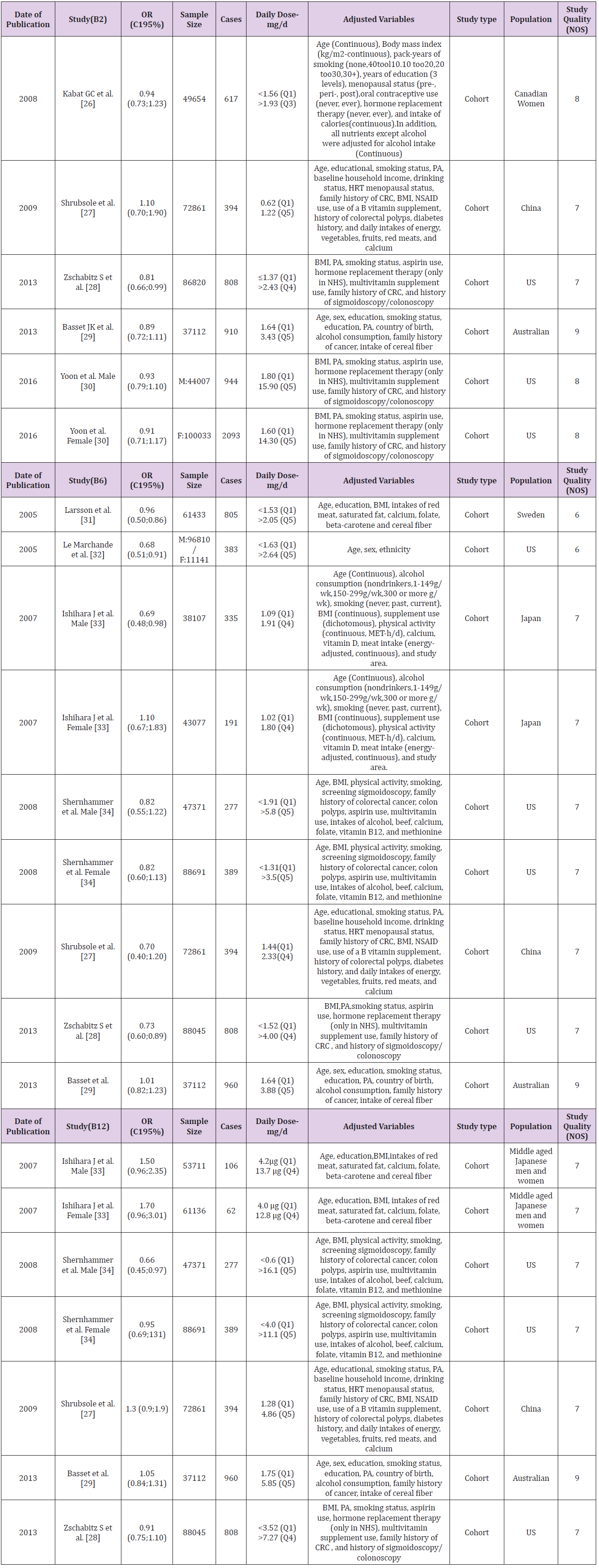
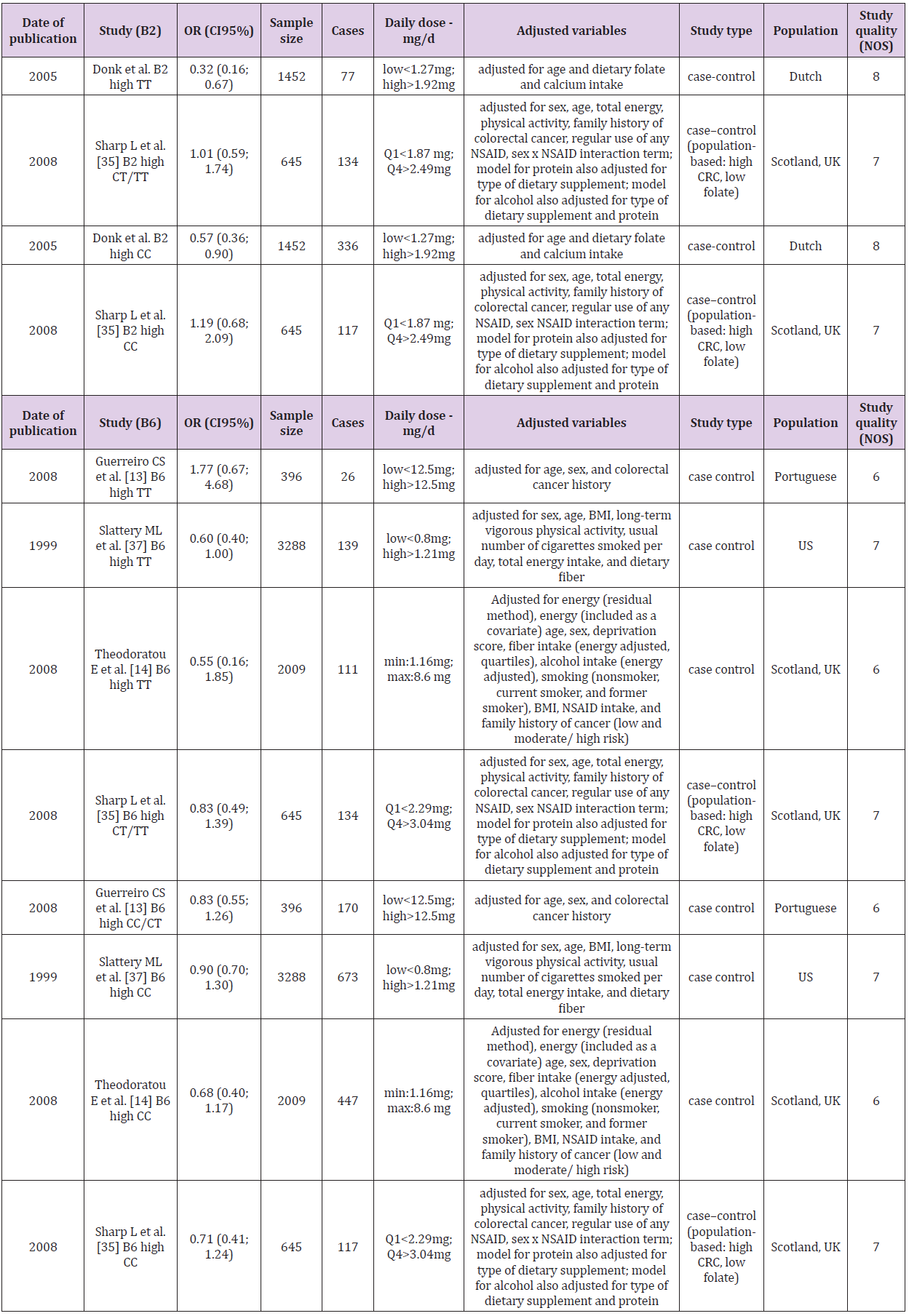
In the first analysis consisting of 9 selected articles, we calculated overall ORs for vitamin B2, B6, B12 intake and CRC risk without consideration of MTHFR polymorphism. These studies were cohort studies, 5 from America, 1 from Sweden, China, Japan and Australia. The overall sample size was 777 117 and number of cases was 8146 (Table 1). We stratified the analysis according to the type of B vitamin and individual forest plots were generated for vitamin B2, vitamin B6 and vitamin B12 with 5 [26-30], 7 [27- 29,31-34] and 4 [27-29,34] cohort studies, respectively (Figure 2). In the second analysis we evaluated the 5 eligible articles [13,14,35-37] (Figure 3A). Calculated overall OR represented the association between MTHFR C667T homozygous polymorphism and B vitamins, influencing the risk of CRC development caused by this gene variant. Regarding study design, these were case-control studies conducted mainly in Europe and the US. The 5 studies had a total of 7790 participants with 2230 cases (Table 2). The daily intake of B vitamins was categorized into low or high groups, using tertiles, quartiles or quintiles. Dose of intake varied between studies (Tables 1 & 2); therefore, we compared the highest versus lowest intake and related ORs in all cases.
Table 1: List and characteristics of publications, discussing the intake of vitamin B2, B6, B12 and the risk of colorectal cancer, included in the meta-analysis.
Table 2: List and characteristics of publications discussing the association of vitamin B2 and B6 intake, influenced by MTHFR C667T polymorphism, with the risk of colorectal cancer development included in the meta-analysis.
Association between Intake of B Vitamins and the Risk of CRC
We applied combined effect size (CES) to demonstrate the association between the highest versus lowest intakes of vitamin B2, B6, B12 and the risk of CRC.
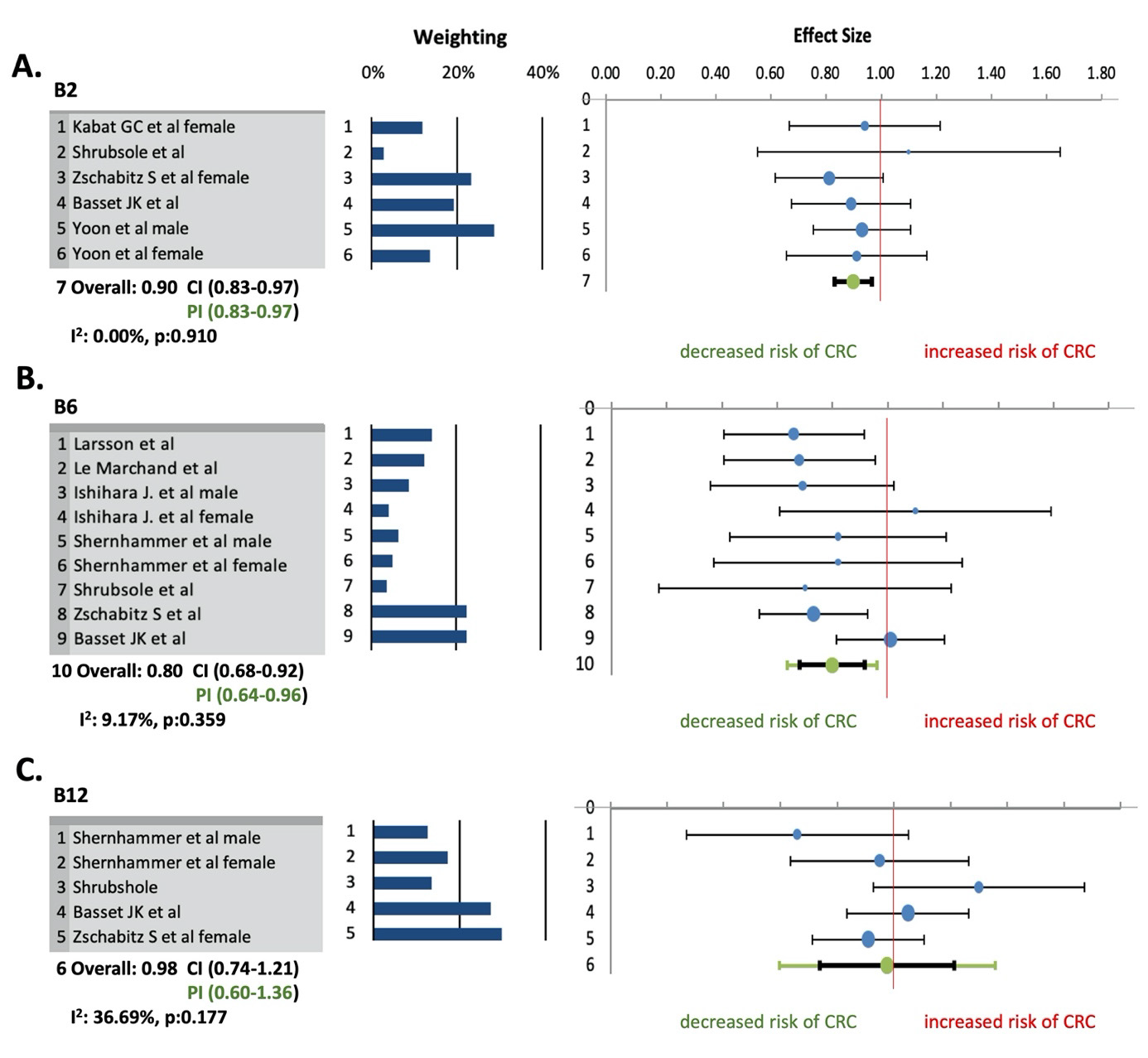
Vitamin B2: The combined effect size for the risk of CRC for highest versus lowest categories of vitamin B2 intake was 0.90 with CI95% 0.83 – 0.97, indicating higher intake of vitamin B2 had inverse association with risk of CRC. There was not difference between CI95% and PI95% values. Heterogeneity among studies was not observed (I2 = 0.00%; p = 0.910, PI95% = 0.83 – 0.97) (Figure 2A). According to the “Trim and fill” method there was also no evidence for heterogeneity in case of vitamin B2, and funnel and Galbraith plots did not show any outliers among effect sizes as well. Egger’s regression test (p = 0.202) and Begg & Mazumdar’s rank correlation test (p = 0.094) showed no possible evidence of publication bias.
Vitamin B6: The results of the meta-analysis showed a reduced risk of CRC development by higher dietary intake of vitamin B6 (CES = 0.80; CI95% 0.68 – 0.92). PI95% value (0.64 – 0.96) was similar to CI95%. A low statistical heterogeneity was detected (I2 = 9.17%; p = 0.359; PI95% 0.64 – 0.96) (Figure 2B). According to the “Trim and fill” method there was no evidence for heterogeneity in case of vitamin B6, and funnel and Galbraith plots did not show any outliers among effect sizes as well. Publication bias was not indicated according to Egger’s (p = 0.880) and Begg & Mazumdar’s (p = 0.174) tests.
Figure 2: Meta-analysis for the association of vitamin B2 (A), vitamin B6 (B), vitamin B12 (C) intake and colorectal cancer risk. Effect sizes of selected studies, discussing the association of vitamin B intake (highest versus lowest categories) and colorectal cancer, were included. The size of each dot is proportional to the weight of the study.
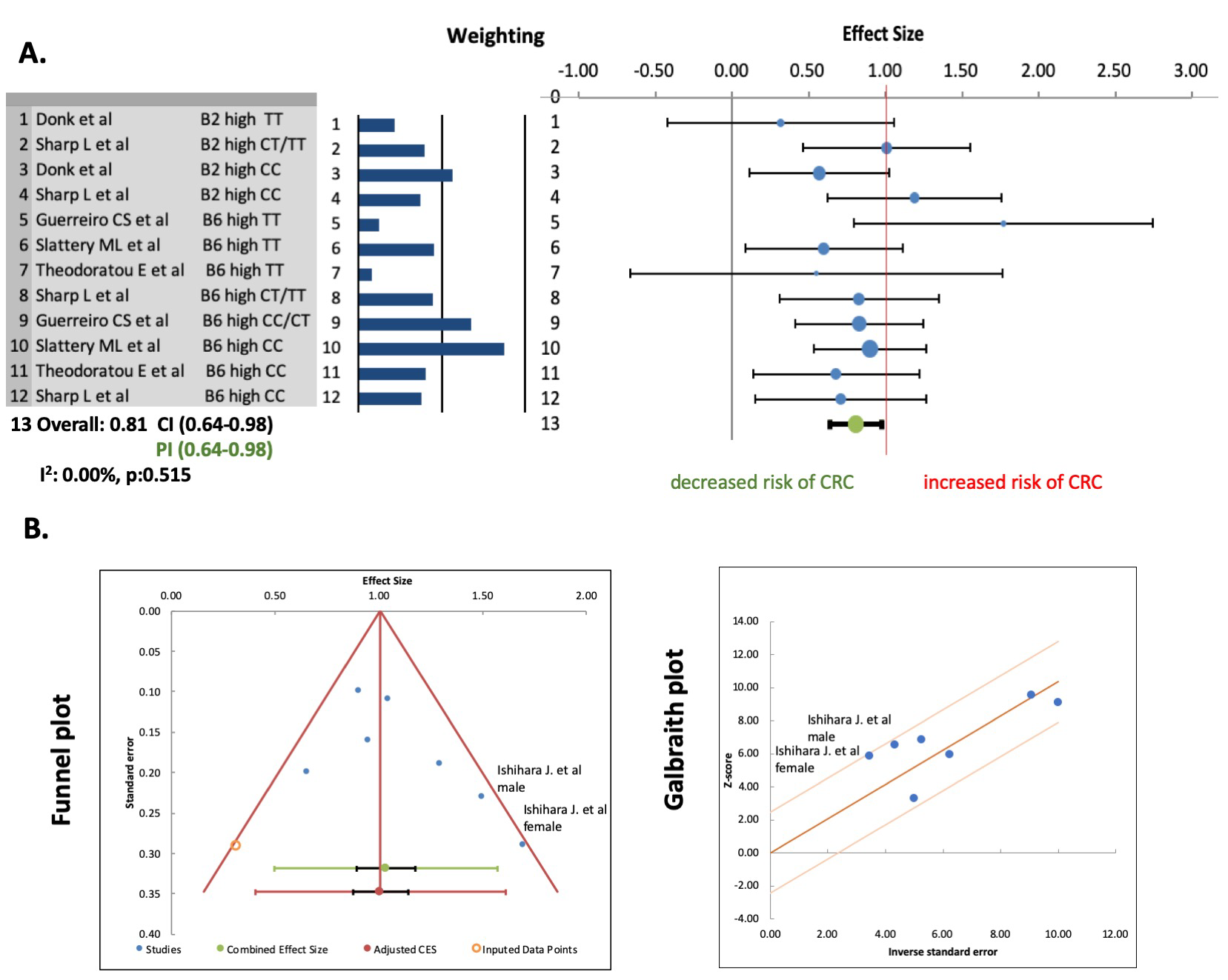
Vitamin B12: Based on combined effect size calculated from ORs of the 5 selected cohort studies, we observed that higher dietary intake of vitamin B12 could increase the risk of CRC (CES = 1.10; CI95% 0.80 – 1.39; PI95% 0.50 – 1.69) in some populations. A significant substantial heterogeneity was presented with I2 = 64.01%; p = 0.011; PI95% = 0.50 – 1.69. The “Trim and fill” method also showed significant heterogeneity (p = 0.002) as well. We visualized effect sizes of vitamin B12 intake to select outliers but neither funnel plot nor Galbraith plot (Figure 3B) suggested outliers, despite the study of Ishihara et al. was more likely to be a possible one. Excluding the results published by Ishihara et al., the meta-analysis on vitamin B12 intake changed significantly. Based on 4 studies, the recalculated CES fell below 1, changed to 0.98 (CI95% 0.74 – 1.21; PI95% 0.60 – 1.36). Heterogeneity became moderate and non-significant (I2 = 36.69%; p = 0.177) based on the regularly used calculations (Figure 2C), but not on the one proposed by Borenstein. There was no potential publication bias anymore after exclusion (p = 0.975 and p = 0.500).
Association between B Vitamin Intake and MTHFR Polymorphism
According to random effects model we found that higher dietary intake of vitamin B2 and B6 could decrease the risk of CRC in patients with MTHFR C667T polymorphism. The calculated CES was 0.81 with CI95% 0.64 – 0.98 (PI95% value was the same). Heterogeneity was not detected among the included studies (I2 = 0.00%; p = 0.515) (Figure 3A). There was also no evidence for heterogeneity by “Trim and fill” method as well. We assessed publication bias in which Egger’s regression test and Begg & Mazumdar’s rank correlation test did not show publication bias with levels of significance 0.759 and 0.340, respectively.
Figure 3: (A) Meta-analysis for the influence of MTHFR C667T polymorphism on the association of B vitamin intake and the risk of CRC. Effect sizes of selected studies, discussing colorectal cancer risk and vitamin B2 and B6 intake, were included. The size of each dot is proportional to the weight of the study. (B) Identification of outliers among studies addressing vitamin B12. Studies outside the skew boundary line of funnel or Galbraith plots are possible outliers.
Discussion
The importance of nutritional vitamin and mineral intake has increased over the last three decades parallel with the negative environmental factors affecting the human body. Lifestyle factors such as diet, physical activity, stress level and habits, which influenced by social and economic state can increase the risk of cancers. Nutrition of cancer patients requires more attention because their nutritional status is determinative not only for successful cancer treatment but to maintain their physical strength, general well-being or to reduce side effects of their therapies. Therefore, there is an expectation and necessity to measure and evaluate the effects of these vitamins, compounds and products [6,7,10,38]. Several studies suggested that dietary methyl-donors and related vitamins can contribute to cancer prevention [8,39-41]. Dietary methyl-donors, such as folate, betaine, choline,methionine and B vitamins provide methyl groups for the one-carbon metabolism of which vitamin B2, B6 and B12 can influence the availability of methyl groups [38,7,10]. B vitamins, additionally, take part in energy-yielding metabolism, oxygen transport and neuronal functions thus they affect the cognitive and psychological processes, including mental and physical fatigue [7,11].
We performed a systematic review and meta-analysis to collect recently available scientific data about the effect of dietary intake of vitamin B2 (riboflavin), B6 (pyridoxine) and B12 (cobalamin) on the risk of CRC development as well as their importance in counteracting MTHFR C677T polymorphism and consequently decrease the risk of CRC development [13,14,35-37]. Although there are well known protocols how to prepare a systematic review or meta-analysis, the interpretation of the results is varied by papers and by selected research area. Most analysis use Cochrane Q, p value and I2 statistics, applying subgroup analysis and calculate heterogeneity as well as publication bias. Heterogeneity regularly interpreted as low, moderate, substantial as follows: 30-60%, 50- 90% and 75-100%, respectively. However, we used additional measurements, the PI95% as well, to interpret our findings according to Michael Borenstein’s recently published book entitled “Common mistakes in Meta-analysis and how to avoid them” [19].
Our meta-analysis suggests a decreased risk of CRC for the highest versus the lowest intake of vitamin B2 and B6. Overall effect was determined as combined effect sizes (CES) with the related CI95% values. In general, if overall effect size is above 1, it means the risk increases, when it is placed below 1 that means the risk of CRC decreases. Our results showed that the values of CES are 0.90 for vitamin B2 and 0.80 for B6, thus these vitamins could decrease the risk of CRC. However, there are two additional, regularly used metrics in a meta-analysis, the I2 and the p value. In a regular basis these are used to evaluate the heterogeneity reflecting on how much the effect sizes varies. However, Borenstein explains that I2 is a ratio and describes us “what proportion of the variance in observed effects reflects variation in true effects, rather than sampling error”, and does not say anything about the heterogeneity. In case of heterogeneity, it is more important to answer the question: “how much the true effect size varies across the studies”, and the measurement called prediction interval (PI) are able to depict it. In our cases, the PI 95% values are 0.83 – 0.97 for vitamin B2 and 0.64 – 0.96 for vitamin B6. PI95% does not crossing 1 that means the true effect sizes are below 1, and as the interval is quite small, it means there is no heterogeneity in these studies.
With regard to the association between vitamin B12 and the risk of CRC, the analysis of the 5 included cohort studies showed that CES is 1.10 with CI95% 0.80 – 1.39 and PI95% 0.50 – 1.69. The range of PI95% crossing 1, which suggests that dietary intake of vitamin B12 could increase the risk of CRC in some populations. I2 was 64.01% (p = 0.011), which is considered as a high variance between effect sizes. As a result of the identification of outliers in ORs, we excluded the effect sizes published by Ishihara et al. Even though ORs of this study were inside the skew boundary line of funnel and Galbraith plots, our calculation suggested it is a possible outlier because the I2 reduced to 36.69% (p = 0.177) after exclusion. Although CES changed to 0.98, CI95% and PI95% still passed through 1. This suggested that we still could claim that vitamin B12 could has a negative effect on the risk of CRC in some populations because the range of PI95% suggested high heterogeneity.
Some publication has already been written that patients in the higher quartile of vitamin B12 intake had more chance to smoking and drinking alcohol, and because of this the utilization of vitamin B12 is decreased in their case [42,43]. As stated by Ishihara et al., there is possibility for positive association between vitamin B12 intake and the risk of CRC, written in their study, which remained after the adjustment of smoking habits and alcohol intake. Therefore, their result represents more likely the effect of smoking and alcohol consumption on the risk of CRC, which is a well-known positive association, rather than the dietary intake of vitamin B12 [33]. All the smoking habits, alcohol consumption and gastrointestinal disorders should be considered if we examine the effect of vitamin B12 intake on the risk of CRC as these factors make it difficult to involve patients properly into any study group based only on their known vitamin B12 intake [33,44]. This information led us to exclude vitamin B12 intake from the further analysis. After the exclusion of the study of Ishihara et al. the group of the studies became homogeneous, which is essential criterion for calculating publication bias.
Genetic polymorphisms also can influence the risk of CRC. The most well-known is the single nucleotide polymorphism of MTHFR gene at the position in C677T. This substitution is resulted in decreased enzyme activity in homozygous TT mutation with lower DNA methylation level, thereby increased risk of CRC, however it highly depends on nutritional status [12-14]. Vitamin B2 is the cofactor of MTHFR, which catalyses the formation of 5,10-methyltetrahydrofolate (5,10-THF), and through S-adenosylmethionine (SAM) influences DNA methylation. Depletion of vitamin B2 or folate causes inadequate formation of 5,10-THF and leads to increased homocysteine / S-adenosylhomocysteine (SAH) level and insufficient methylation of DNA, which increases the possibility of development of cancer [6,45,46]. Vitamin B6 is a cofactor of cystathionine-β-synthase which converts homocysteine to cysteine in the liver. Low vitamin B6 level can result in an increased homocysteine and SAM levels, which then similarly can arrest DNA methylation [6,38].
In the second part of our analysis, we investigated the association between MTHFR C667T polymorphism and intake of vitamin B2 and B6. We could confirm that appropriate intake of vitamin B2 and B6 could be possibly protective in diminishing or even eliminating the negative effect of the reduced enzyme activity in the folate cycle in case of homozygote TT patients. Additionally, vitamin B2 intake have already been reported as a protective factor for breast and cervical cancer as well, highlighting its potential protective role in cancer prevention [47-49]. There was no evidence for publication bias, indicating that the pooled results may be unbiased. We excluded the group of vitamins B12 from this analysis as well, because the effect of vitamin B12 is influenced by numerous factors as we have already described above. In contrast to the first analysis, in the second, the effect of B vitamins was handled altogether as both vitamin B2 and B6 play role in the onecarbon cycle, which is regulated by MTHFR.
The limitations of our study are similar to other meta-analysis, where several confounding factors (e.g., inadequate controls, misclassification of exposure when using FFQ, dietary intake obtained at baseline may have changed over the long follow-up period, high intake of vitamins may have been at lower risk due to other healthy habits and behaviors, adjusted variables differed in the studies) could affect the pooled result. Additionally, nutrients which was not measured in the studies could influence the risk of CRC even after an adjustment process. Details of other possible biases were described in the original papers. We used more searching engines to increase the chance for achieve the highest amount of searching terms related to our analysis as possible. We used additional metrics from Borenstein, which gives additional, valid and meaningful interpretation of the results.
In conclusion, we found that vitamin B2 and B6 may be an effective dietary component to decrease CRC risk, and they can be an important part of a dietary intervention, or a special diet during/ after cancer treatment. We found that an adequate intake of vitamin B2 and B6 – and probably B12 – could compensate the consequence of the reduced enzyme activity of MTHFR in CRC development. Therefore, it may give the opportunity to incorporate a genetic test of the MTHFR polymorphism into the screening process of CRC with recommendations for specific diet for those in need.
Citrus Limetta Extracts Inhibit Oxidative Stress in Human Skin Organ Culture
Introduction
Herbal medicines have formed the basis of traditional medical systems for centuries and occupy an interesting place in modern pharmacology. The World Health Organization (WHO) estimates that about 80% of the world’s population still depends on herbal medicines to treat various diseases because of their high availability and economic reasons [1]. Citrus, belonging to the Rutaceae family, is one of the most widely grown crops globally, especially in tropical climates and temperate regions [2]. The health benefits of citrus have been mainly associated with its high contents on antioxidant molecules such as Vitamin C and Polyphenols known for their benefic impact on human health [3]. Citrus belonged to the family Rutaceae and several commercial citrus varieties such as sweet orange, grapefruit, lime, and lemon and were considered to possess natural compounds with several health benefits [4]. The beneficial effects of citrus fruits can be attributed to their chemical constituents, including vitamins, dietary fiber, carotenoids, flavonoids, lipids, and essential oils [5,6]. Citrus limetta belongs to a type of citrus commonly known as sweet lemon, which can be cultivated in South and Southeast Asia [7]. It is small, between oval and spherical, with a greenishyellow peel, rich in polyphenols, flavonoids, flavanones, and flavones [8]. Citrus limetta Risso (Rutaceae) is known to be an antihyperglycemic plant in Mexican folklore [9]. C. limetta fruits are used for the common cold, decreasing cholesterol level, fever regulation, regulating inflammation, digestive disorders, and so forth as well as blood pressure modulator [10,11]. Flavonoids hesperidin and naringin are found to be present in the peel part of the fruit of Citrus limetta [12]. C. limetta comprised of 8–10% peel, which is perishable waste material creates a challenge in processing industries and pollution monitoring agencies [13]. Interestingly, C. limetta fruit peels possess various pharmacological activities due to flavonoids in a significant quantity [14,15]. In this context that we proposed to study in a first part the extraction of fruit peels from the Citrus limetta plant by maceration using three solvents (hexane, water and ethanol). In the second part, we studied the content of total polyphenols and flavonoids and the antioxidant effect. First, the antioxidant power was studied in a chemical system (TAA, DPPH, ABTS, and FRAP). Then, the biological system used HeLa cell lines by measuring MDA and CD levels. In addition, to study the cytotoxic effect, MTT test was realized using HeLa cells lines. Finally, the antioxidant activity of the three extracts of Citrus limetta was evaluated on skin explants.
Materials and Methods
Plant Materials and Extraction Procedure
The Citrus limetta fruits were purchased from the local market / Sfax, south of Tunisia, in March 2019. The fruits were carefully washed, cutes into small pieces, and dried in an oven at 60 °C. 100 g of plant material were treated overnight with different solvents (ethanol, hexane, and water) under gentile stirring. The different extracts were filtered through a cellulose filter, lyophilized, and frozen at -80 °C until use.
Total Phenol Determination
Total phenols were determined using the Folin- Ciocalteu reagent according to the method of Singleton and Rossi [16]. Briefly, 50 μl aliquot of the extract was mixed with 250 μl of Folin reagent and 500 μl of sodium carbonate (20%, w/v). The mixture was vortexed and diluted with water to a final volume of 5 ml. After incubation for 30 min at room temperature, the absorbance was read at 765 nm. Total phenols were expressed as gallic acid equivalents (GAE), using a freshly prepared gallic acid solution calibration curve.
Total Flavonoid Determination
Total flavonoids were measured by the colorimetric assay described by Zhishen, et al. [17]. Total flavonoids were expressed on a dry weight basis as quercetin equivalents, using a freshly prepared quercetin solution calibration curve.
Antioxidant Capacity Assays
a. Phosphomolybdenum Assay
The total antioxidant activity of the extracts was evaluated using the Prieto, et al. methodology [18]. Briefly, 100 μl of the extract was mixed with 1 ml of the phosphomolybdenum reagent (600 mM sulfuric acid, 28 mM sodium phosphate, 4 mM ammonium molybdate). After incubation at 95 °C for 90 min, the absorbance was measured at 695 nm. The total antioxidant activity was expected to be the effective concentration (EC50) compared to Vit C as a positive control.
b. 2,2-Diphenyl− 1-picrylhydrazyl (DPPH) Free Radical Scavenging Activity Assay
The radical scavenging activity of extracts against DPPH free radicals was measured using the method of Cao, et al. [19] slightly modified as follows: 20 μl of appropriately diluted samples or Vitamin C solutions was added to 190 μl of DPPH solution (100 μM). The mixture was shaken vigorously and allowed to reach a steady-state at room temperature for 30 min. Then, the absorbance was measured at 517 nm with a Beckman spectrophotometer.
c. ABTS Radical Scavenging Activity Assay
The antiradical activity was performed by the ABTS+ free radical decolorization assay as developed by Re, et al. [20]. The reaction mixtures containing 100 μl of the sample at different concentrations and 900 μl of reagent were incubated at 30 °C for 6 min. The absorbance was measured at 734 nm.
d. Ferric-Reducing Antioxidant Power (FRAP)
The principle of this method is based on the reduction of a ferric-tripyridyltriazine complex to its ferrous, colored form in the presence of antioxidants [21]. Briefly, the FRAP reagent contained 2.5 ml of a 10 mmol/L TPTZ (2,4,6- tripyridy-s-triazine, Sigma) solution in 40 mmol/L HCl plus 2.5 ml of 20 mmol/L FeCl3 and 25 ml of 0.3 mol/L acetate buffer, pH 3.6 and was prepared freshly and warmed at 37°C. Aliquots of 40 μl sample supernatant were mixed with 0.2 ml distilled water and 1.8 ml FRAP reagent. The absorbance of the reaction mixture at 593 nm was measured spectrophotometrically after incubation at 37°C for 10 min. The 1 mmol/L FeSO4 was used as the standard solution. A spectrophotometer performs the absorbance reading against a blank at 700 nm. Ascorbic acid is used as a positive control. The increase in the absorption capacity of the components indicates an increase in iron reduction.
e. MTT Cell Proliferation Assay
MTT (3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide cell proliferation assay measures the cell proliferation rate and, conversely, reduces cell proliferation viability when metabolic events lead to apoptosis or necrosis. The yellow compound MTT (Sigma) is reduced by mitochondrial succinate deshydrogenase to the blue formazan, depending on the cell viability. Cells were grown on microtiter plates (200 μl of cell suspension/well) in 96 well microplates with serial extract dilutions. After 72 h, 20 μl of MTT solution (5 mg/ml) was added to each well. The plate was incubated for 4 h at 37 °C in a CO2 incubator. After that, 180 μl of the medium was removed from each well and replaced by 180 μl of (DMSO/ methanol) (V:V). When all the crystals were dissolved, absorbance was measured at 570 nm with a microplate reader (Elx 800 microplate reader) [22].
f. Malondialdehyde (MDA) Determination
The MDA production was evaluated using thiobarbituric acidreactive species (TBARs) assay. Adherent cells were detached using trypsin/EDTA solution and centrifuged at 3000 rpm for 10 min. The pellet was resuspended in 500 μl of deionized water and lysed by five cycles of sonication during 20 s at 35% (Sonisc, vibracell). One millilitre of TBA solution (15% trichloroacetic acid, 0.8% thiobarbituric acid, 0.25 N HCl) was added. The mixture was heated at 95 °C for 15 min to form MDA-(TBA)2 adducts. Optical density (OD) was measured by a spectrophotometer (Biochrom, Libra S32) at 532 nm. Values were reported to a calibration curve of 1,1,3,3-tetraethoxypropane (1.1.3.3 TEP) [23].
g. Conjugated Dienes
After sonication, cell lysates were extracted with 3 ml (chloroform: methanol) (2:1 v/v). After centrifugation at 3000 rpm for 15 min, 2 ml of the organic phase was transferred into another tube and dried at 45 °C. The dried lipids were dissolved in 2 ml of methanol, which was determined by absorbance at 233 nm. This corresponds to the maximum absorbance of the extracted compounds [24].
Evaluation of the Antioxidant Activity of Citrus Limetta Extract on Skin Explants
a. Stress Induction
After removal, the fragments are washed three times with PBS (1×) and then incubated for 15 min at room temperature in the presence of an antibiotic and an antifungal. The fragments are then sterile cut into small pieces and cultured in a 24-well plate at the air / liquid interface, in the presence and absence of the 3 extracts at different concentrations (0.5 mg / ml; 1 mg / ml; 2 mg / ml) for 2 hours at 37 °C. After incubation, the culture medium is eliminated, and then two successive washes with PBS (500 μl) are carried out. Hydrogen peroxide is then added at a concentration of 1.5 mM in RPMI to induce oxidative stress on the skin explants. After 2 h of incubation at 37 °C, all the fragments are recovered in tubes containing formalin and stored at 4 °C until the histological sections are made.
b. Histopathological Examination
For light microscopic examination, samples were fixed in 10% neutral buffered formalin, dehydrated in an ascending ethanol series (65%, 75%, and 95%), cleared in xylene, and embedded in paraffin. Paraffin sections (5 μm) were stained with hematoxylin and eosin using a routine method. The assembly step consists of bonding the blades containing the sections.
c. Analysis data
Statistical studies are carried out using the SPSS program (19.0). The t-Student test carried out the comparison between the means. The results are represented in mean ± standard deviation (DS).
Results
Total Phenolic and Flavonoid Compounds
First, we were interested in evaluating the levels of anthocyanins, total phenolic, and flavonoïd compounds in the different Citrus limetta extracts using Follin-Ciocatleau colorimetric and AlCl3 methods, separately. The results show that the aqueous and ethanolic extract contains (166.4 ± 0.81 mg GAE / g DM; 152.29 ± 1.8 mg GAE / g DM) respectively. On the other hand, the hexane extract has a low polyphenol content (2.57 ± 0.02 EAG / g DM) (Table 1). Regarding flavonoids contents, our results indicate 75.9 ± 0.65 mg QE/g DM; 64.9 ± 1.64 mg QE/g DM for aqueous and ethanolic extract, respectively. In addition, a small number of flavonoids for hexane extract was detected (1.54 ± 0.045 EC / g DM) (Table 1).
Antioxidant Activity
a. Phosphomolybdenum Assay
The power of ammonium phosphomolybdate in the present study is expressed in mg equivalent of ascorbic acid (vitamin C) / g of dry matter. Our results indicate a total antioxidant activity for the Citrus limetta peels extracts (Table 1).
Table 1: Total antioxidant activity of Citrus limetta extracts.
b. The Scavenging Activity for DPPH Radicals
Table 2: ABTS and DPPH IC50 values for the extract of Citrus limetta (HEOA), Vit C and TROLOX.
DPPH molecules that contain a stable free radical have widely been used to evaluate the radical scavenging ability of antioxidants. Therefore, the Citrus limetta free radical scavenging activities were assayed using DPPH (Table 2). At all the tested concentrations, Citrus limetta aqueous, ethanolic, and hexane extracts showed a significant anti-radicular effect attending 84%, 83%, and 87%, respectively, compared to their synthetic antioxidant positive control (BHT).
c. The Scavenging Activity for ABTS
The antioxidant activity test results of the ABTS+ radical by ethanolic, aqueous, and hexane extracts attend 89,9%; 90,10 and 8,24%, respectively (Table 2).
d. Ferric-Reducing Antioxidant Power (FRAP)
The FRAP assay is usually used to measure the capacity of the sample to reduce the ferric complex to the ferrous form. However, our results showed that the three Citrus limetta peel extracts have a weak antioxidant activity compared to vitamin C (Figure 1).
Figure 1: Absorbance of standard Vit C and extracts of Citrus limetta peel by Ferric Reducing Antioxidant Power (FRAP) assay. Note: Various concentrations of extracts (0 to 0.25 mg/mL) and acid ascorbic were mixed with FRAP reagents. The reduction of ferric ion (Fe3+) to ferrous form (Fe2+) by extracts produces an intense blue light revealed as a change in absorption at 700 nm. Results were expressed as mean inhibition percentage (%) ± standard deviations (n = 3). Ascorbic acid at various concentrations (0 to 0.25 mg/mL) was used as standard.
e. Cytotoxicity Effect of Citrus limetta Peel Extract
To investigate the cytotoxic effect of Citrus limetta peel extracts on HeLa human cell line, cells were treated with various concentrations of extracts (Hexane, ethanolic and aqueous) ranging from 4 to 0.0625 mg/ml for 48 hours, and then submitted to the MTT test. Our results showed a cytotoxic effect of the hexane extract on the HeLa line depending on the concentrations used. The other two extracts (Ethanol and Aqueous) have less than 50% cytotoxicity for the concentrations used (Figure 2).
Figure 2: Cytotoxic effect of Citrus limetta peel extracts on HeLa cell line. Note: The inhibitory effect of different doses on cell growth was determined by MTT assay. Cells were treated with extracts at a concentration ranging from 4 to 0.0625 mg/ml. The percent of growth reduction was calculated from the extinction difference between treated cell culture and the control. Results are the means of two repetitions.
f. Effect of Citrus Limetta Peel Extracts on Lipid Peroxidation Activity
The investigation of the Citrus limetta extracts biological antioxidant activity was carried in HeLa human cell line. Cells were cultured with or without the addition of extracts for 48 hours. Oxidative stress was induced by adding 0,2 mM H2O2. Hydrogen peroxide and Citrus limetta extracts with a 0.25 mg/ml concentration were added to the HeLa human cell line simultaneously for 30 minutes.
g. Malondialdehyde (MDA)
After H2O2 treatment, a very significant increase in MDA levels in the HeLa line was observed, in comparison with the untreated cells, indicating the presence of a state of oxidative stress following the treatment of these cells by H2O2 (p <0.01). HeLa cells treated with the three extracts: ethanol, hexane, and aqueous, induce a very significant decrease in MDA levels (p <0.01 respectively) (Figure 3).
h. Conjugated Dienes (CD)
HeLa cell line treated with H2O2 induces a significant increase in CD levels compared to untreated cells (p <0.001) (Figure 3). Conversely, treating cells with Citrus limetta extracts causes a significant decrease in CD levels. This decrease is highly significant for hexane and ethanol (p <0.001) and significant for the aqueous extract (p <0.05).
Figure 3: MDA (A) and conjugated diene (B) levels in Citrus limetta peel extracts supplemented HeLa cell line. Cells were cultured in 25 cm2 flasks with 0.25 mg/ml of extracts for 48 hours. Oxidative stress was induced by the addition of cells for 30 min. TBARs and conjugated diene (CD) were compared to untreated cells (C-), cells treated with H2O2 (C+), and cells treated with extracts.
i. The Protective Effect on Skin Explants in Culture
Figure 4: Micrograph of skin sections treated with the three extracts of Citrus limetta. Note: A: control B: traited with H2O2 (1.5 mM) C: traitée with hexane extract (0.5 mg/ml) then with H2O2 (1.5 mM) D: traited with hexane ectract (1 mg/ml) then H2O2 (1.5 mM) E: traited with hexane extract (2 mg/ml) then H2O2 (1.5 mM) F: traited with aqueous extract (0.5 mg/ml) then H2O2 (1.5 mM) G: traited with aqueous extract (1 mg/ml) then H2O2 (1.5 mM) H: traited with aqueous extract (2 mg/ml) then H2O2 (1.5 mM) I: traited with ethanolic extract (0,5 mg/ml) then H2O2 (1.5 mM) J : traited with ethanolic extract (1 mg/ml) then H2O2 (1.5 mM) K : traited with ethanolic extract (2 mg/ml) then H2O2 (1.5 mM). • Detachment of the basal lamina • Pycnotic nucleus • Vacuolar degeneration
The evaluation of the antioxidant activity of the three Citrus limetta extracts was carried out on skin explants maintained in culture in the presence of different concentrations of each extract (0.5 mg/ml; 1 mg/ml; 2 mg/ml). The results obtained are compared with those found with explants cultured in the presence and absence of hydrogen peroxide (Figure 4). Our results have shown that culturing of skin explants in the complete medium does not affect the histo-architecture of the skin (Figure 4A). However, treatment with hydrogen peroxide at a concentration of 1.5 mM leads to structural disorganization of the skin, which manifests itself in the detachment of the membrane which separates the dermis and the epidermis. In addition, in the granular layer of the epidermis, the cells presented a necrotic appearance which resulted in retraction of the nuclei (pycnotic nuclei) and vacuolar degeneration (Figure 4B). The pretreatment of the skin explants at different concentrations of each Citrus limetta peel extract made it possible to minimize the oxidative damage induced by hydrogen peroxide depending on the concentration used (Figures 4C-4N). It is observed that the protective effect is most important at the level of the fragments treated with the hexane extract (Figures 4C-4E), so the total disappearance of the oxidative damage by the treatment with the high concentration of hexane extract at 2 mg/ml.
Discussion
Plants contain different phenolic compounds, including simple phenolics, phenolic acids, hydroxycinnamic acid derivatives and flavonoids [25]. The content of total polyphenols and flavonoids was determined. Our results agree with those of Mohanty, et al. [15] who showed the content of phenolic and flavonoid compounds in the aqueous and ethanolic extract of Citrus limetta [15]. Similarly, Safdar et al showed that the 4 peel extracts of Citrus reticulate L (methanols, ethanol, acetone, and ethyl acetone) presented a polyphenol content varying according to the polarity of the solvents used in the extraction [26]. Our results agree with the work of Hegazy et al. [27] who found that the polyphenol content varies between the different extracts of orange peel [27]. According to Chan et al. the choice of extraction solvent is essential because it allows the type and quantity of polyphenols to be estimated [28]. The variations in the polyphenol content depend on the polarities of the solvents used and their concentration level. Citrus limetta extracts analyzed in this work showed potent radical scavenging activity. We have demonstrated that GEo has an interesting antioxidant activity which is highlighted by the TAC, DPPH, ABTS+, FRAP. Our results agree with the literature that showed that citrus possesses an anti-free radical activity DPPH, according to Padilla, et al. [29]. The Citrus limetta aqueous extract can trap the DPPH radical with a percentage inhibition of 42.5%. Other Citrus reticulate L methanolic extract studies have shown a high antioxidant potential (72.83 ± 1.22%) [26]. Other work studied three extracts of the peel orange (Citrus aurantium) that showed significant antioxidant power with low IC50 values (acetone 781.9 μg / ml; ethanol 1,137.9 μg / ml; methanol 1,402.9 μg / ml) [30]. The same extract showed comparable antioxidant activity to TROLOX using the ABTS radical. Our results agree with Oboh et al., who showed the presence of an antioxidant effect of the peel of Citrus sinensis, Citrus paradisii, and Citrus maxima extracts against the radicals ABTS [31]. The Citrus limetta extracts had a weak FRAP value, which was in disaccord with the results obtained by Farha et al. that confirmed that the Citrus limetta methanolic extract has moderate antioxidant (iron-reducing capacity) activity [32]. The variation in antioxidant activity depending on the tests can be explained by the fact that this antioxidant activity depends not only on the concentration but also on the structure and antioxidants nature [33]. Our results showed a cytotoxic effect-dependent concentration of Citrus limetta extracts with Hexane on HeLa cell lines. Other studies on the aqueous extract of Citrus unshiu (a species of the same family as the Citrus limetta) showed the presence of a cytotoxic power of the latter on the line MDA-MB-231 with a concentration of 1,5 mg/ml. This cytotoxic effect is attributed to the disruption of the mitochondrial transport system [34]. On the other hand, Diab et al. showed that the ethanolic peel extracts of Citrus sinensis L reduced the HL-60 cell line viability [35]. According to the results, to investigate the antioxidant activity of our extract on the cells model, we choose a concentration that induces less than 20% of toxicity. The concentration used is 0.25 mg/ml in all the experiences. HeLa cells are treated simultaneously with H2O2 and extracts. Our results induce a very significant decrease in MDA levels, which agrees with the work, which showed that the methanolic extract of Citrus limetta peel exhibits antioxidant activity demonstrated by a reduction of MDA levels [36]. To the best of our knowledge, our study is the first to determine the antioxidant potentials of Citrus limetta peel on the skin by analyzing histopathological findings.
Conclusion
Citrus limetta is a promising source of natural antioxidants, as indicated by its high contents of polyphenols, flavonoids and by its considerable DPPH and ABTS free radical scavenging activities and FRAP value. In addition, the histological study of skin fragments has shown dose-dependent protection of our extracts against lesions.
Rare Primary Pulmonary Sarcomatoid Carcinoma with Isolated Pancreas Metastasis: Case Report and Literature Review
Introduction
Sarcomatoid change is an uncommon phenomenon (accounts for approximately 0.4%) in non-small cell lung cancer (NSCLC) which is characterized by poorly differentiated neoplasm containing sarcoma or sarcomatoid components [1-3], its pathological diagnosis include five subtypes (pleomorphic carcinoma, spindle cell carcinoma, carcinosarcoma, giant cell carcinoma and pulmonary blastom) and require high-quality sampling of the tumor [4]. Since pulmonary sarcomatoid carcinoma (PSC) is generally a form of highly aggressive malignancy in NSCLC, it is no wonder that it has an extremely poor prognosis [1]. Previous studies have shown that patients with PSC respond poorly to platinum based standard regimens and develop easily to chemotherapeutic resistance [2,5], and thus it is absolutely essential to explore and work out a more effective therapeutic strategy. Here, we reported a 59-year-old patient who was admitted for attacks of acute pancreatitis and was diagnosed with PSC with isolated pancreas metastasis, an even rarer malignance. Then, we reviewed the literature available and hope to seek out safer and more effective treatment strategies which can improve the prognosis of PSC patients.
Case Description
A 59-year-old male, an active smoker with a 40-year history of tobacco smoking (an average of 40 cigarettes per day), presented to a hospital in Xuzhou on November 26, 2020, he complained of persistent epigastric pain for half a day after heavy drinking. The patient denied any previous history of respiratory or digestive disease and malignancies. The results of hematological examination showed a mild leukocytosis and hyperamylasemia (130U/L; reference range: 30-110U/L), therefore, the patient was initially thought to had acute pancreatitis. However, According to the images of chest and abdomen computed tomography (CT), a lesion (46mm × 31mm) in the right lower lung lobe was detected; a cystic lesion was existed in the body of pancreas, and cystadenocarcinoma remained to be ruled out. In order to further clarify the patient’s condition and diagnosis, the patient then underwent positron emission tomography (PET)/CT. As shown in Figure 1, the two nodules which located in the inferior lobe of right lung and the body of pancreas had significantly increased fluorodeoxyglucose metabolism and were considered to be malignant lesions. Then, the patient underwent the CT-guided percutaneous pulmonary nodules puncture biopsy, and the pathological diagnosis was poorly differentiated lung adenocarcinoma.
Figure 1: Partial PET/CT scanned images of the patient’s chest and abdomen. The nidus in the inferior lobe of right lung (A) and the body of pancreas (B) had significantly increased fluorodeoxyglucose metabolism and were considered to be malignant lesions.
In order to receive further comprehensive treatments, the patient was subsequently admitted to the Affiliated Hospital of Xuzhou Medical University. The result of magnetic resonance cholangiopancreatography showed a 1.1cm × 1.5 cm lesion in the pancreatic body (Figure 2). Considering that the lesions on the lung and pancreas were isolated and the patient was in good general condition with acceptable examination results of blood routine, liver and kidney function, serum electrolytes and coagulation function, the patient underwent the state-of-the-art Da Vinci robotic assisted laparoscopic resection of pancreatic lesions, thoracoscopic lobectomy and intrathoracic lymph node dissection on December 15, 2020 after excluding the surgical contraindications and thorough communication with the patient and his families, and the patient recovered well after surgery. The postoperative pathological results demonstrated that the two lesions in the inferior lobe of right lung and the body of pancreas were malignant with extensive necrosis, and the tumor sizes were 1.5cm × 1.5cm × 0.5 cm (pulmonary lesion) and 1.3cm × 1.1cm × 1cm (pancreatic lesion), respectively, no definite vascular and nerve invasion, no cancer cell involvement at the bronchial cut-off, vascular cut-off and the cross-section of pancreas, no tumor metastasis was detected in the group 7 and 11 lymph nodes.
Figure 2: Representative images of magnetic resonance cholangiopancreatography of the patient. The examination revealed a 1.1cm × 1.5cm lesion in the pancreatic body.
Figure 3: A. Immunohistochemical staining results of CK7, CK8, CKpan, TTF1, Vimentin in lung tumor tissue and B. CKpan, NapsinA, TTF-1 in pancreatic metastasis tissue.
The immunohistochemistry (IHC) results of lung tumor (Figure 3A) were Ki67 (+, about 50%), TTF-1 (partial +), CD56 (-), Syn (-), CgA (-), P40 (-), CK5/6 (-), CK7 (focal +), NapsinA (partial +), CKpan (+), CK8/18 (+), Vimentin (+), S100 (±), HMB45 (-), Melan-A (focal +), LCA (CD45)(-), ALK (-), CD30 (-), DPC4 (+), Bcl-10 (-), PAS (several endochylema +), which corresponded to poorly differentiated carcinoma with a tendency to sarcomatoid carcinoma. The pancreatic tumor was consider metastatic poorly differentiated carcinoma with TTF-1 (partial +), NapsinA (+), CKpan (+) and Bcl-10 (-) (Figure 3B). Overall, the patient was definitively diagnosed with the right PSC with isolated pancreatic metastasis. According to the 2020 National Comprehensive Cancer Network guideline, the patient received the first cycle of chemotherapy with Gemcitabine (2g, day1 and 7) combined with Carboplatin (800mg, day 1) on January 20, 2021. However, the patient’s platelet level significantly decreased and the lowest number was 30*109/L on the 13th day after chemotherapy, hence, the chemotherapy regimen was adjusted to Abraxane (400mg, day1) combined with Nedaplatin (40mg, days 2 to 3), and the patient regularly received four cycles without severe adverse reactions.
Shortly thereafter, the patient developed tumor recurrence and metastasis which were indicated by the CT examination on June 22, 2021, a new mass with uneven enhancement appeared in the upper lobe of right lung, suggesting tumor metastasis; multiple nodular high-density shadows appeared in the liver and stomach space which were considered as lymph node metastasis. Due to the high expression level of PD-L1 (+, tumor proportion score was about 70%) in the patient’s tumor tissue, the patient’s therapeutic regimen was then adjusted to Camrelizumab (200mg) combined with Anlotinib (12mg per day, days 1to 14, 21 days per cycle). However, the patient presented with abdominal pain with hematochezia on the 15th day after the immunotherapy combined with targeted therapy. After comprehensive examinations, the patient was considered to have an acute episode of immunological enteritis, and the new nidus in the right adrenal area was considered metastatic. The patient subsequently received comprehensive treatments of antiinflammatory, analgesic, fluid replacement and electrolyte balance, the symptoms were gradually controlled and relieved. Considering the recent significant weight loss (Figure 4A) and poor appetite of the patient, it was not suitable for chemotherapy. Therefore, the patient is now receiving maintenance therapy with Anlotinib. The patient’s therapeutic process has been summarized as shown in Figure 4B, and we now estimate that the patient’s subsequent survival time is relatively short.
Figure 4: A. Weight change curve of the patient during treatment and B. The summary of his therapeutic process.
Discussion
Pancreatic metastasis of lung cancer is rare, its frequency was mainly related to the histological types and small cell lung carcinoma has the highest incidence which was followed by lung adenocarcinoma [6], while the morbidity of PSC with pancreatic metastasis was extremely low. In this study, we reported a patient who suffered from PSC with isolated pancreas metastasis, after simultaneous resection of the pulmonary and pancreatic masses by state-of-the-art Da Vinci robotic surgery, the patient underwent multiple cycles of chemotherapy, immunotherapy and antiangiogenesis therapy, and he has survived for more than 11 months.
Due to the highly malignant and aggressive characteristics of this tumor, the vast majority of patients with PSC are tended to presented at advanced stage at the time of diagnosis, thus losing the opportunity of surgical resection, therefore, effective systemic treatments are of great importance. It is widely known that the determination of effective therapeutic strategies should be based on well-defined molecular mechanisms of tumorigenesis and cancer progression, whereas little was known about PSC’s molecular pathogenesis now because of its rarity and heterogeneous morphology [2].
In order to describe the mutational profile of sarcomatoid carcinoma, Fallet V, et al. used high-throughput genotyping technology to test 114 surgical biopsies from 81 patients with sarcomatoid carcinoma for 214 mutations affecting 26 oncogenes and tumor suppressor genes, they found that the most frequent mutations were KRAS, EGFR, TP53, STK11, NOTCH1, NRAS and PI3KCA, and the EGFR mutations were almost always rare mutations (89%) [7], and this result had been confirmed by Terra SB, et al. [8]. The above finding suggested that testing for targetable mutations should be considered for patients with PSC, because a subpopulation may benefit from some molecular targeted antitumor drugs which have been approved for clinical use. Another promising new therapeutic strategy of PSC is the use of immune checkpoint inhibitors, because several studies had illustrated that PD-L1 was overexpressed in PSC [9-11]. Moreover, Pecuchet N, et al. demonstrated that, compared with the PSCs with APOBEC enzyme and homologous recombination deficiency, the PSC patients with tobacco-associated signatures had a higher rate of PD-L1 overexpression and a poorer overall survival [12]. The growing body of studies regarding the molecular mechanisms of PSC support that the malignant tumor is not only morphologically diverse, but also quite genetically diverse. Hence, the discovery and description of genetic events might provide novel treatment choices for PSCs, and potentially improve the patients’ prognosis and bring PSC into the era of targeted therapy and immunotherapy.
Conclusion
In this study, we described an extremely rare case of PSC with isolated pancreas metastasis which was presented as acute pancreatitis initially. For PSC patients with isolated metastasis, if the patient’s physical condition permit, surgical resection of the lesions could be considered and thus obtain high-quality tissue specimens for gene detection, which would provide a stronger basis for the selection of subsequent systemic therapy strategies including gene targeting treatment and immunotherapy.
The Obstacles and Overcoming the Challenges that Transgender Women who have HIV Encounter in Jamaica
Opinion
Knowledge about people who oppose the binary system of gender identity is an under-researched area. There is enormous social pressure to conform to religious expectations about masculinity and femininity. It is extremely difficult to manage and negotiate a gendered self-concept that is oppositional to your sex. This paper explores the importance of confronting the denial of health rights to transgender women in Jamaica. Although transgender women are disproportionately affected by the HIV pandemic there is ignorance about their negative experiences of HIV testing. A social-ecological theoretical approach examines the overrepresentation of transgender women among individuals suffering from HIV in Jamaica. This intersectional method analyses HIV testing, healthcare, personal beliefs, cultural norms and relationships. A community-based qualitative research project with people who are living with HIV (PLHIV), women who have sex with women (WSW), men who have sex with men (MSM), bisexual and transgender organizations in Kingston was conducted. 1 focus group with 8 transgender women and in-depth semi-structured interviews with 20 transgender women between the ages of 18 and 30 years old was studied. The focus group and interviews were recorded, transcribed and analysed with a thematic approach.
The transgender women come from diverse ideological and socio-economic backgrounds. They share the conditions of HIV related stigma, discrimination and mistreatment from healthcare workers that reflect Jamaican values and makes them often conceal their gender identities. Among the interviewees 75 % had received an HIV test. Of these 25% were HIV positive (Logie, et al. [1]). In Jamaica there are extremely high levels of homophobia, lesbophobia, biphobia and transphobia that are frequently fatal. Cross-dressing is a matter of life or death. This is demonstrated by the heinous killing of Dwayne Jones. In 2013 the 16 year old Jones attended a party dressed in women’s clothes. When a woman at the party who knew Dwayne informed men that Jones was cross-dressing s/he was murdered by an angry mob [2-5]. It was transphobic overkill as the gender-non-conforming youth was perceived as provoking attack by deceiving the men who s/he danced with. Dwayne was beaten, chopped, stabbed, shot and run over with a car. There was outraged international media coverage of the killing that demonstrated the lack of LGBT rights in Jamaica. There was little local concern or media attention of the hate crime. As usual in these executions the perpetrators were not caught. The terrible nature of Dwayne’s murder makes one question the psychological disturbance of the killers. What types of people would respond in such a savage and tragic manner to cross-dressing? What does the lack of Jamaican social condemnation suggest about the population?
The transformation of policies, practices and provisions are vital to reduce prejudice, harassment and violence. Radical interventions are necessary to oppose transphobia and improve access to HIV prevention services. There is little information about the HIV prevention requirements of transgender people. The problems of gaining access to HIV testing is due to mistreatment by medical staff who are vehemently opposed to caring for Lesbians, Gays, Bisexuals and Transgender (LGBT) people and (PLHIV). These stereotypical and non-confidential issues contribute to huge mistrust and fear. Many healthcare workers urgently require correct information about HIV transmission that negates their transphobia. Transgender women are encouraged to get HIV testing when they have social support and the benefits of knowledge [6-9]. The political will to decriminalize The Buggery Law has the potential to greatly reduce bigotry, brutality and trauma but it can also create a backlash. It is crucial that transgender women deal with their unique concerns such as survival challenges and HIV risks that are connected to discrimination in education, employment and social services. This is essential to foster equity, improve sexual health and protect the rights of transgender women.
The Relationship between Quality of Life, Bone Pain, Skin Pruritus and Depression among Patients with Secondary Hyperparathyroidism: A Cross-Sectional Study
Introduction
SHPT is a common complication of CKD that is characterized by derangements in the homeostasis of calcium, phosphorus and vitamin D [1]. SHPT causes high-turnover bone disease, leading to a decrease in bone mass [2]. Loss of bone mass is mainly manifested by increased cortical bone, with a reduction of bone resorption and mineralized bone on the surface of the cortex due to mineralization defects, with severe bone pain and fracture in severe cases [3]. Pruritus is an unpleasant feeling associated with the urge to scratch; it is a subjective symptom that is caused by many factors and has multiple dimensions [4]. The causes of skin pruritus in patients with SHPT may be related to the increase in parathyroid hormone (PTH), hyperphosphatemia and the accumulation of some medium and large molecular toxins, such as β2-mg, in vivo [5]. Parathyroidectomy (PTX) is the main treatment at present and might also reduce calcium-phosphorus product concentrations, PTH and inflammatory factors, thus controlling vascular calcification and relieving bone pain and skin pruritus [6].
Studies have shown that low QOL and severe physical discomfort can affect patients’ mental health, especially depressive symptoms [7]. In this study, we hypothesize that there is a mediating effect between bone pain, skin pruritus and depression. QOL is a health concept that comprehensively evaluates the qualitative and quantitative factors such as physical function, psychological, social, economic and emotional factors in a patient’s life and is used to evaluate the quality of life in a comprehensive way, which should be based on living standards, but its meaning is more complex and extensive [8]. Kim, et al. research [9] showed that QOL had a strong correlation with pain and depression or anxiety. McIntyre et al. research [10] showed that QOL had a mediating effect between symptoms and depression, which indicated that QOL can indirectly affect depression as a mediating variable. JungHye et al. research [11] proposed a QOL protection model, and the model considered QOL as a protective factor that can regulate the negative impact of risk factors on development outcomes. There are many influencing factors of SDS. At present, the current research mainly focuses on the direct effects of pain and QOL on the occurrence of SDS, but the joint effect of pain and QOL on SDS is not explained. In view of this, this study hypothesize that bone pain/skin pruritus can not only directly affect SDS of SHPT patients, but also indirectly affect SDS by changing the intermediary link of QOL.In this study, it is assumed that QOL plays a regulatory role in the mediation model of bone pain, skin pruritus and depression. In summary, this study hypothesizes that there is a relationship between QOL, bone pain, skin pruritus and depression and that QOL has a mediating effect between bone pain, skin pruritus and depression.
Methods with Statistical Considerations
Participants and Data Collection
A cross-sectional study was conducted in a third-class hospital in Liaoning Province, China, from January 2017 to December 2020. The patients with SHPT were aware of the content of the survey before their participation, and on the day before the questionnaires were distributed, with the agreement of the Northern Theater General Hospital ethics committee, we issued informed consent forms to each patient. In this study, the inclusion criteria was all patients needed PTX and signed informed consent and the exclusion criteria was severe cardiac insufficiency and cognitive dysfunction. A total of 325 questionnaires were distributed, and those that were missing more than 20% of values or had low writing quality were excluded from this survey. In total, 320 questionnaires were considered valid (98.46% effective response rate).
Measures
Measurement of QOL: We measured QOL by using the brief table of the quality-of-life measurement scale (WHOQOL-BREF). The WHOQOL-BREF, a self-reported scale, has 24 items, and each item has a 5-point Likert-type scale ranging from 1 to 5. The total score of the scale ranges from 16 to 80, and higher scores indicate better QOL. There are four dimensions in this instrument: the physiological dimension, the psychological dimension, the social relation dimension and the environmental dimension [12]. In this study, the Cronbach’s α coefficient of internal consistency for the overall scale was 0.857.
Measurement of Bone Pain and Skin Pruritus: We used the Visual Analog Scale (VAS) to measure bone pain. This scale draws a long horizontal line on the paper; one end of the horizontal line is 0, indicating no pain, the other end is 10, indicating severe pain, and the middle region indicates different degrees of bone pain [13]. This method was also used to measure the degree of skin pruritus.
Measurement of Depression: The Self-rating Depression Scale (SDS) is composed of 20 items and 4 dimensions: psychoemotional symptoms, somatic disorders, neuromotor disorders and psychological disorders. The SDS asks about the degree of depression in patients using a 4-point Likert Scale that ranges from never (1 point) to always (4 points), and the total score ranges from 20 to 80 [14]. In this study, the Cronbach’s α coefficient of internal consistency for the overall scale was 0.842.
Statistical Analysis: SPSS 21.0 and AMOS 23.0 were used for the statistical analyses. First, single sample K-S test was used to test whether the measurement data conformed to normal distribution. If it was, it was expressed as `x±s, otherwise it was expressed as median or interquartile range. We conducted descriptive analyses of the sociodemographic variables and Pearson correlation analysis of the other variables. Multiple linear regression analysis was used to test the mediating effect, and the bootstrap method in the AMOS structural equation model was used to further verify the mediating effect. The process of parameter estimations could exclude measurement error [15]. According to related research and theories, a hypothetical relationship model was created and is shown in Figures 1 & 2. Two SEM models were presented, as follows: QOL is an intermediary variable between bone pain, skin pruritus and depression. The structural path hypothesis is that bone pain and skin pruritus have direct and indirect effects through depression. Furthermore, it shows the results for goodness-offit indexes obtained with SEM for the total sample and individual samples.
Figure 1: The earth’s society: anthropoid setups.
Figure 2: Mediating effect of QOL on skin pruritus and SDS.
Results
Demographic Characteristics of the Participants
There were 320 patients with SHPT in this study: 172 (53.8%) were males, and 148 (46.2%) were females. 95(92.19%) had different degrees of forgetfulness,302(94.38%) had varying degrees of fatigue. The age of the patients ranged from 20 to 70 years. The years of renal failure ranged from 2 to 30, and the average was 10.71±4.64 years. The years of SHPT ranged from 1 to 9, and the average was 3.07±2.13 years.
Descriptive Statistics
In this study, the measurement data showed a normal distribution, so it was expressed as `x±s. The QOL score ranged from 25 to 68, with an average of 41.76±8.15. The scores for bone pain and skin pruritus ranged from 1 to 10, with averages of 5.08±2.65 and 3.58±3.19, respectively. The years of bone pain ranged from 0 to 10, and the average was 2.30±1.95. The years of skin pruritus ranged from 0 to 8, and the average was 2.13±2.05. The SDS score ranged from 20 to 65, and the average was 46.04±8.98. The preoperative PTH ranged from 588 to 2934 pg/ml, and the average was 1729.15±376.20 pg/ml. The serum calcium ranged from 1.95 to 2.93 mmol/L, and the average was 2.43±0.19 mmol/L. The serum phosphorus ranged from 1.30 to 3.59 mmol/L, and the average was 2.38±0.52 mmol/L. The comparative results of each scale for SHPT patients with different demographic characteristics are shown in Table 1.
Table 1: Descriptive statistics (N=320).
Preliminary Correlation Analyses
First, the correlation analysis of renal replacement therapy (RRT) type, renal failure time, dialysis vintage, duration of SHPT and QOL, bone pain, skin pruritus, SDS showed that renal failure time was significantly (P<0.01) negatively correlated with QOL (r=-0.232) and positively correlated with skin pruritus (r=0.142) and SDS (r=0.149), other variables were not relevant. The Pearson correlation analysis of QOL, bone pain, skin pruritus and SDS is presented in Table 2. The results showed that QOL was significantly (P<0.01) and negatively correlated with bone pain (r=-0.509), skin pruritus (r=-0.517) and SDS (r=-0.465). Bone pain was significantly (P<0.01) and positively correlated with skin pruritus (r=0.568) and SDS (r=0.450). Skin pruritus was significantly (P<0.01) and positively correlated with SDS (r=0.426).
Table 2: Correlations between the main variables (N=320).
Testing for the Mediation Effect
The variable was normalized first, and three regression equations were established according to the purpose of this study. Equation 1: depression as the dependent variable and bone pain or skin pruritus as the independent variable; Equation 2: QOL as the dependent variable, with SDS and bone pain or skin pruritus as the independent variable; and Equation 3: SDS as the dependent variable, with QOL and bone pain or skin pruritus as the independent variable. The results showed that bone pain and skin pruritus could significantly predict depression (β=0.485/0.375, p≤0.001) and that bone pain and skin pruritus could significantly predict QOL (β=-0.407/-0.337, P≤0.001). When bone pain or skin pruritus and QOL predicted SDS at the same time, the predictions were significant (β=0.310/0.223, p≤0.001; β=-0.429/-0.450, p≤0.001). This indicated that the direct or indirect effects of bone pain or skin pruritus on SDS were significant; that is, QOL plays an intermediary role between bone pain or skin pruritus and SDS. The results are shown in Tables 3 & 4.
Table 3: The moderating effects of QOL (Part 1).
Table 4: The moderating effects of QOL (Part 2).
Verification of the Mediating Effect
On the basis of multivariate regression analysis, the bootstrap method was used to further test the intermediary effect of QOL. To test the intermediary effect, we needed to establish a structural equation model, and we used AMOS 23.0 to test it. The specific path analysis diagram is shown in Figures 1 & 2. The structural equation model fit results showed that CMIN/DF=2.437/1.202 (<3); AGFI=0.928/0.965, GFI=0.960/0.980, TLI=0.961/0.994, IFI=0.973/0.996, and CFI=0.973/0.996 (>0.9); and SRMR=0.042/0.026 and RMSEA=0.067/0.025 (<0.08), indicating that the model fit well. The results showed that the confidence intervals for both the direct and indirect effects of bone pain and skin pruritus on SDS did not reach 0. The mediating effect model of QOL was established, and the mediating effect was 0.212/0.275, accounting for 48.62%/45.08% of the total effect. See Tables 5 & 6 for details.
Table 5: Results for total, indirect and direct effects of bone pain on SDS with QOL as a mediator.
Table 6: Results for total, indirect and direct effects of skin pruritus on SDS with QOL as a mediator.
Discussion
The Depression Status of SHPT Patients
Previous studies have shown that Cinacalet can inhibit PTH in a short time [16], but most patients cannot afford it because of its high price. Meanwhile, previous studies in our department have shown that patients taking Cinacalcet for more than 5 years cannot continue to suppress PTH, but PTX can better suppress PTH, improve symptoms and quality of life. With the transformation of medical models into biological/psychological/social models, the phenomenon of bodily disease accompanied by anxiety and depression has attracted wide attention in the field of medical psychology. The main symptoms of patients with SHPT are depression, memory loss, insomnia, nightmares, etc [17]. However, there are few investigations on QOL and depression psychology at home and abroad. In this study, patients had a high level of depression, with an incidence of 77.81%. The average SDS score was 46.04±8.98, which was higher than the norm [18]. This result indicated that the mental health level of patients with SHPT was low, which suggested that more attention should be paid to patients with SHPT in China. The generation of depressive symptoms includes many factors, such as pain, pruritus, occupation, education, income, and insurance [19], but in the early stage of depression, relieving discomfort over time and giving timely social or emotional support can largely avoid the occurrence of depression [20]. The SDS score of male patients in this study was higher than that of female patients; however, this is different from Liu’s findings [21], which may be related to the fact that men are under more economic pressure and most patients are unable to work due to hemodialysis. There were significant differences in SDS scores among patients with different occupations, education, incomes, and insurance, which may be because the patients with high education and a good job generally enjoy higher medical insurance reimbursement and take Cinacalet, lanthanum carbonate and other drugs to alleviate SHPT [22].
The Status of SHPT Patients’ QOL, Bone Pain, and Skin Pruritus
The vast majority of SHPT patients have skin pruritus, bone pain, electrolyte disorder, coupled with long-term dialysis leading to the destruction of various systems of body, which complicates the screening, such as sleep disturbances, fatigue, loss of energy and poor appetite. However, no related surveys on QOL, bone pain, or skin pruritus in patients with SHPT have been reviewed at home or abroad. In this study, the average QOL score was 41.76±8.15, which was lower than the norm [23], and the average score for bone pain was 5.08±2.65, which was higher than the norm [24]. This was consistent with Galvez-Sanchez’s [7] and Rehman’s [25] findings. In this study, skin pruritus had a greater impact on the patient’s body than bone pain. PTX can improve the symptoms of bone pain caused by bone deficiency and hypocalcemia.
The Mediating Effect of QOL
The results of Pearson correlation analysis showed that QOL, bone pain, skin pruritus and depression were significantly correlated with each other, and that bone pain and skin pruritus positively predicted the level of depression. This was consistent with the results obtained by Brophy et al. [26]. and laid the foundation for the subsequent analysis of mediating effects. Notably, regression analysis revealed that there was a partial mediating effect between bone pain, skin pruritus and depression, which provided a basis for the verification of mediating effects. At the same time, some studies also showed that patients with low QOL have a significantly higher risk of depression, and QOL is an important predictor of depression in SHPT patients, which is basically consistent with the results of this study. The bootstrap method was used to further verify the mediation effect. The results showed that a mediating effect of QOL between bone pain, skin pruritus and depression was established, and the mediating effect was 48.62%/45.08%. BI also confirmed that QOL played a role in mediating depression [27]. In clinical work, we should encourage SHPT patients to improve symptoms causing discomfort through PTX in a timely manner, which can greatly reduce depression and improve QOL.
Medical staff should guide family members to actively participate in all aspects of patients’ life and treatment, timely grasp the psychological function of patients, and strengthen the care for patients. Encouraging patients to participate in more social activities can buffer the negative effects of various pressures on body and mind, improve sleep quality, reduce depression and other psychological disorders. Therefore, we set up we chat group for SHPT patients to answer the medical problems after discharge online, such as adjusting blood calcium, regular follow-up within the group. The department should carry out the corresponding mental health survey regularly and give timely intervention to the patients with severe pain, pruritus, sleep disorder and depression tendency, and take positive and effective measures to improve mental health level in time. In summary, QOL, bone pain, skin pruritus and depression are closely related in patients with SHPT and there may be a full mediating effect of QOL between bone pain or skin pruritus and depression. It is suggested that alleviating bone pain and skin pruritus in SHPT patients can alleviate the state of depression through the mediating effect of QOL.