Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
A Bone Marrow Aspirate Concentrate procedure (BMAC) is an innovative regenerative method implemented in medical practice since the early nineteenth century as a simple medical relief that grew steadily through good experiences and training. Consequently, these undifferentiated stem cells create diverse kinds of differentiated cells. [1]. The BMAC procedure is an uncomplicated technique that runs on various diseases not cured by traditional remedies or pathologies that need principal medicine. Therefore, in the BMAC method, the operator inserted the BMAC in the hurt tissue to form subsequent physiological chains in the involved tissue. Consequently, the BMAC exhibited the capability to assist the diseased tissue microstructure for tissue reconstruction over time. [2]. The earlier BMAC testers attempted victorious trials of the BMAC method in animals and later in humans with excellent outcomes. Furthermore, the experimenters illuminated the growing pertinence of the BMAC in many disorders and unmanaged conditions [3]. BMAC method included catching a small amount of the participant bone marrow from the (anterior or posterior part of the pelvis) by local an aesthesia as an outpatient procedure. The operator transfers this part of bone marrow to a specialized laboratory in an aseptic way. Hence, the laboratory operator collects the stem cells by an activation device like “Adi-Stem, AdiLight-2 Photo device” and guards these stem cells to reinsert them into the same patient blood or the diseased tissue for the cure [4]. Consequently, the doctor proffered the sufferer a painkiller and advised of bed rest for a week. After that, the specialist will follow the patients with education and rehabilitation after the BMAC shot, but if the patient did not benefit from the first shot of BMAC, the physician gave a second injection after three weeks [5]. BMAC accommodates immature stem cells plus growth factors, which gave more influence than the “autologous platelet-rich plasma”. Hence, this plasma holds the growth factors only. Afterward, this essential contrast offers the BMAC effectiveness in tissue regeneration plus emblematic symptom amelioration [6]. In 2020, the Food and Drug Administration (FDA) in the USA approved “blood-forming stem cells” or “hematopoietic progenitor cells” from umbilical cord blood, but in 2021 the USA approved other types of stem cells. Nevertheless, some principal academic hospitals in the USA and developed nations with excellent results. Further, Native Stem Cell Hospitals practiced BMAC treatment following 2014. Moreover, in 2020 the Food and Drug Administration acquired specific guidelines [7].
1. Usher syndrome 2. Ear Cartilage loss 3. Cochlear disease
I. Brain
1. Autism 2. Stroke 3. Traumatic Brain
Complications of BMAC
A. Most of those complexities are minor and settle spontaneously. 1. Pain in situ 2. Simple discomfort 3. Hematoma 4. Numbness 5. Need repeated applications
Limitations of BMAC Procedure
1. Not Licensed in Some Countries 2. Expensive 3. Not In Health Insurance List 4. Repeated Injections 5. Need Special Laboratory Tools
Results
BMAC procedure is harmless, comfortable, safe, plus high satisfaction technique. Furthermore, BMAC had lower patient mortality plus morbidity.
Conclusion
BMAC is a good choice in curing or alleviating man’s difficultto- treat diseases.
Biostatistical Analysis on Anti-breast Cancer Drug Screening
Introduction
Breast cancer is one of the most common malignant tumors in women, and a malignant tumor occurring in ductal epithelium of the breast. Estrogen is involved in the growth and differentiation of mammary epithelial cells in hormone dependent tumors. It plays an important role in the occurrence and development of breast cancer [1]. Estrogen mainly acts through the estrogen receptor expressed in the nucleus, that is, by binding with estrogen receptor (ER) to form a complex [2]. Research shows that ERα is expressed in normal breast epithelial cells less than 10% but expressed in breast cancer cells around 50%-80%. ERα has become an important target of endocrine therapy for breast cancer [3]. Currently, antihormone therapy is commonly used in breast cancer patients with ERα expression, which controls estrogen levels through regulating estrogen receptor activity. ERα mediates the E2 up regulation of PI3K/Akt signaling pathway and promotes cell proliferation [4]. Compounds that can antagonize ERα activity may be candidates for treatment of breast cancer. For example, tamoxifen and renoxifene are the ERα antagonists for clinical treatment of breast cancer [5]. In order to screen potential active compounds, a potential compound model is usually established to collect compounds and bioactive data by targeting the specific estrogen receptor subtype targets associated with breast cancer. The quantitative structureactivity relationship (QSAR) model of compounds was constructed with the biological activity descriptor as the independent variable and the biological activity of compounds as the dependent variable. The model was used to predict the new compound molecules with good biological activity or guide the structural optimization of existing active compounds. A compound that wants to become a candidate drug, besides having good biological activity (here refers to anti breast cancer activity), also needs to have good pharmacokinetics and safety in human body. It is called ADMET property, including absorption, distribution, metabolism, excretion and toxicity. When determining the biological activity of a compound, it is also necessary to consider its ADMET properties as a comprehensive consideration. In this paper, the coupling degree between bioactivity descriptor and ER activity is verified by BP neural network. After determining that the screened bioactivity descriptors can indeed affect ERα activity to a great extent, the ADMET property of bioactivity descriptors is further verified.
Overview of BP Neural Network
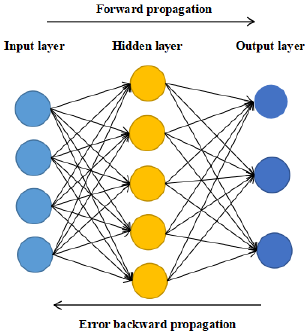
Figure 1: Basic structure diagram of BP neural network.
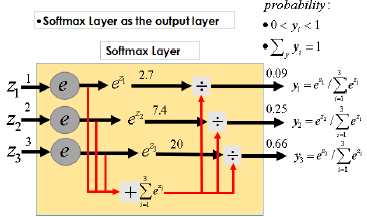
Artificial neural network is widely used in pattern recognition, function approximation and so on. BP neural network is a multilayer feedforward network simulating human brain. It has good adaptability and training ability, belongs to nonlinear dynamic system, and including two processes: forward propagation of information and back propagation of error. BP neural network consists of three parts: input layer, hidden layer and output layer. The input layer receives the input information, and then transmits the information to the hidden layer. The hidden layer analyzes and processes the data. Finally outputs acceptable information through the output layer. This information is continuously corrected through the reverse propagation of error, which can make full use of the coupling between data. BP neural network shows excellent accuracy in many fields. Therefore, this paper selects neural network as the main prediction method. Whether it is regression network or prediction network, the setting of the hidden layer and the number of hidden nodes of the network is very important. Too few hidden layers and hidden nodes will lead to less data information that the neural network can process, resulting in low prediction accuracy, and too many hidden layers will lead to overfitting of the model. There is no general calculation formula for the setting of the optimal number of hidden nodes. It is more based on the empirical formula or changing the number of hidden nodes to continuously train the model to find the number of hidden nodes with the smallest error [6-8]. Basic structure diagram of BP neural network is shown in Figure 1. The activation function of BP neural network usually uses softmax function to give corresponding weight to each node and transfer information between nodes in the network. In addition, there is an offset weight in the propagation of each layer of network, which is an additional constant of SoftMax function. In the model training, the gradient optimization algorithm (Adam algorithm) is used to optimize the model to obtain the best results [9].
Its operating principle is shown in Figure 2.
Figure 2: Principle of Softmax function.
Adam Algorithm: Initialize 1st, 2nd moment vector and timestep:
do while:
Computing the gradient:
Update biased first moment estimate:
Update biased second moment estimate:
Compute bias-corrected first moment estimate:
Compute bias-corrected second moment estimate:
Update parameters:
Where α is the step length, β ;β ε [0,1] is the momen estimation of exponential decay rate, and f(θ) is the random objective function of parameter θ. Adam algorithm will be used to optimize the parameters of BP neural network in order to accelerate convergence and improve accuracy. The model is: • Step 1: Initialize the network weight and bias, give each network connection weight a small random number, and each neuron with a bias will also be initialized to a random number. • Step 2: Forward propagation. Input a training sample, and then calculate the output of each neuron. The calculation method of each neuron is the same, which is obtained by the linear combination of its inputs. • Step 3: The gradient descent method is used to calculate the error and carry out back propagation. The weight gradient of each layer is equal to the input of the connection of the previous layer multiplied by the weight of the layer and the reverse output of the connection of the next layer. • Step 4: The weight gradient in the third step is used to adjust the network weight and neural network bias. • Step 5: Back propagation, Adam algorithm is used to accelerate the weight adjustment, initialize the moment vector and exponential weighted infinite norm to 0, update the parameters through vector operation, and iterate in t time from step size to 1. Sort errors and return. • Step 6: At the end of judgment, for each sample, judge if the error is less than the threshold set by us or has reached the number of iterations. We’ll finish training, otherwise, return step 2.
Data Description and Preprocessing
In this paper, the bioactivity description data set is used to verify the ERα activity and ADMET properties respectively. The description dataset contains 729 biological activity descriptors of 1974 compounds. Because the data dimension is too large and contains a large number of repetitions and useless variables, this paper selects 15 most representative biological activity descriptors from the 729 biological activity descriptors of 1974 compounds. Firstly, low variance filtering is used to delete the biological activity descriptors with low information, then considering the correlation and independence between variables, Lasso regression is used to select these variables, and finally considering the coupling degree between variables and ERα activity. The final 15 most representative biological activity descriptors are obtained. The specific steps are as follows: • Step 1: Because the variance of variable can reflect the degree of dispersion, the variable with small variance contains little information, which cannot provide key and useful information for the construction of the model. Therefore, for 729 biological activity descriptors of 1974 compounds, the variance of 729 variables is calculated and arranged from large to small. • Step 2: After cleaning the biological activity descriptors with low information or no information, use the remaining molecular descriptors to further process the repeated information of the data, so as to make the data relatively independent. In this paper, Lasso feature selection method is used to propose a variable from two variables with strong correlation to eliminate duplicate information. The essence of lasso feature selection method is to seek the sparse expression of the model and compress the coefficients of some features to 0, so as to achieve the purpose of feature selection. The parameter estimation of lasso feature selection method is as follows:
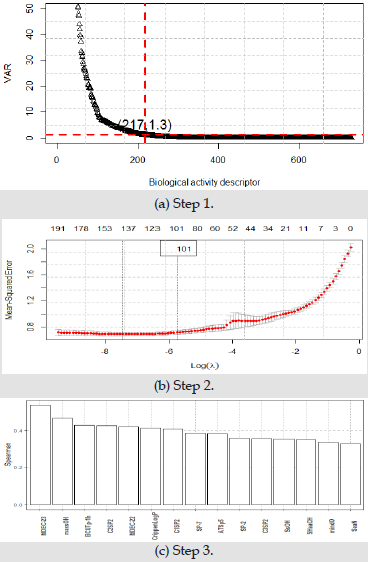
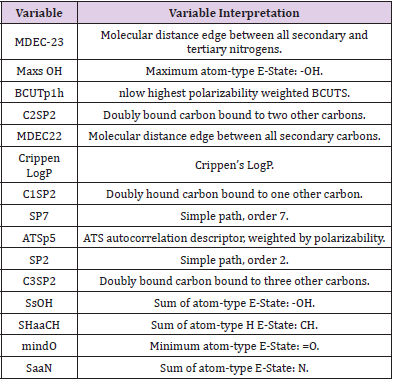
λ is a nonnegative regular parameter, which represents the complexity of the model. The greater its value, the greater the penalty of the linear model, λ Determined by cross validation. • Step 3: Spearman rank correlation coefficient is a nonparametric index to measure the dependence of two variables, which can reflect the coupling degree between variables. This paper uses Spearman rank correlation coefficient to obtain the final 15 representative biological activity descriptors. Three screening processes by Figure 3 shows, in step 1, 217 biological activity descriptors with variance greater than 1.3 were left. In step 2, 101 bioactivity descriptors were retained by lasso feature selection. In step 3, 101 biological activity descriptors are sorted according to Spearman rank correlation coefficient, leaving the most representative 15 biological activity descriptors. The final screening results are shown in Table 1. ADMET properties are composed of five aspects: absorption, distribution, metabolism, excretion and toxicity. The corresponding values are provided in the form of two classifications, ‘1’ represents good or yes, and ‘0’ represents poor or no. Comparison table of ADMET properties are shown in Table 2.
Figure 3: Principle of Softmax function.
Table 1: Comparison table of biological activity descriptor.
Table 2: Comparison table of ADMET properties.
Model Training and Prediction
In order to avoid over fitting and improve the generalization ability of the model [10], we cut the remaining 15 bioactivity descriptors into 80% of the training set and 20% of the test set. Considering the coupling and the nonlinear relationship between the data, the neural network is used for training and prediction, the training set is used to set the model parameters, and the test set is used to calculate the default accuracy and verify the rationality of the model. When training the model, we should also consider the convergence speed of the model. Neural network is a complex structure with large amount of calculation. When there are too many input variables in the input layer and the amount of data is too large, gradient optimization algorithm is usually used to accelerate the convergence speed of neural network. Adam algorithm is used for model optimization in this paper. The results are as follows:
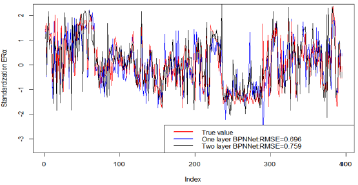
Figure 4: The predict of Adam-BPNNet.
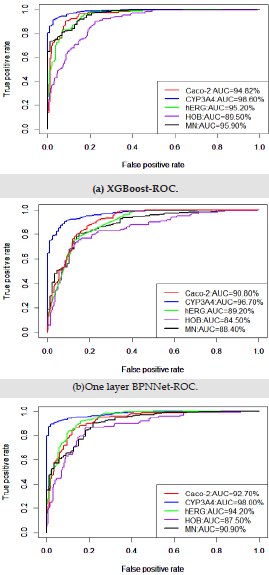
As can be seen from Figure 4, The red line is the logarithm of ERα, the blue line is the regression prediction result of neural network with one hidden layer, and the black line is the regression prediction result of neural network with two hidden layers. Among them, when the hidden layer is 1, the mean square error of prediction is 0.696, and when the hidden layer is 2, the mean square error of prediction is 0.759.Obviously, when the hidden layer is 1, the regression prediction result is more accurate, and the good prediction accuracy shows that the ERα activity can be controlled by controlling the 15 biological activity descriptors selected in this paper, so that we can inhibit the ERα activity. In order to ensure that the selected bioactivity descriptors have good medical properties, the ADMET properties of these 15 bioactivity descriptors were verified. The commonly used machine learning methods are used for multiple prediction to eliminate contingency. ROC curve shown in Figure 5. It can be seen from Table 3 that the three models show very high prediction accuracy, among which xgboost performs best. The three models show that CYP3A4 is highly coupled with 15 biological activity descriptors, HOB is the lowest coupled with one biological activity descriptor, but the prediction accuracy also reaches 0.895. This shows that the 15 biological activity descriptors selected in this paper can not only reflect ERα activity to a great extent, It can also reflect good ADMET properties.
Figure 5: ROC curve of each classification method.
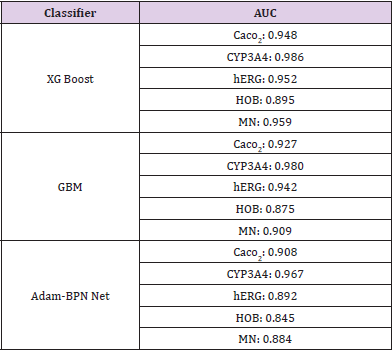
Table 3: Comparison table of AUC values of different classification models.
Conclusion
The results show that the 15 biological activity descriptors selected in this paper can predict ERα activity with a low mean square error of 0.676, which indicates that there is a high coupling between them. In addition, they can also reflect the properties of ADMET at an average level of 0.948, so they have good medical value. The development of anti-breast cancer drugs is a complex and long process. In this process, it is necessary to test the effects of drugs containing various biological components on target cells. If all the combined drugs are tested, it will be a long process. In order to improve the development cycle and cost of anti-breast cancer drugs, we can consider using these bioactive descriptors to synthesize breast cancer resistant compounds. Because the experimental data are limited, the influence of these 15 bioactive descriptors on the activity of other target cells is not considered. Therefore, the bioactive descriptors selected in this paper have limitations in the effect of breast cancer. Furthermore, lasso feature selection method is used to screen bioactivity descriptors, which may omit some important bioactivity descriptors. When the synthetic breast cancer drugs are synthesized, the best value or range of bioactive descriptors can further reduce the development cost and development cycle of anti-breast cancer drugs. Therefore, in this paper, we can further study the best values of various bioactive descriptors. At the same time, we also hope that the variable screening method and validation method can be applied to more biopharmaceutical processes.
Viet Nam’s Mandatory Motorcycle Helmet Law 2007 and its Impact on Road Traffic Injuries Mortality in a Mountainous Province: A Population-Based Mortality Registration, 2005-2018
Introduction
Road traffic injuries (RTIs) are a public health burden globally. The number of deaths due to road accidents worldwide is exceptionally high, with an estimated 1.35 million deaths and 20 – 50 million injuries each year (World Health Organization (WHO). 2020b). Road traffic is among the leading causes of mortalities due to injuries for all age groups, especially among children and youth and young adults aged 5 to 29 (World Health Organization (WHO). 2018). Globally, road injuries were responsible for more than 55 million years of life lost, 7 million years lived with disability, and 64 million disability-adjusted life years in total, with corresponding age-standardized rates of 745, 126, and 871 per 100,000 population, respectively James SL, et al. [1]. The two most common road traffic injuries are head and spinal cord injuries, which are the leading cause of death and trauma for motorcycle users (World Health Organization (WHO). 2018). Such injuries may result in an enormous economic burden and use extensive portions of a countries health expenditure (World Health Organization (WHO). 2013b, 2018). The risk of encountering RTIs among middle and low-income countries (LMICs) is three times higher than in higherincome countries (World Health Organization (WHO). 2020b). Motorcycles are the most widely used transport in Viet Nam, accounting for more than 90% of total personal transport registrations (World Health Organization (WHO). 2013a). The average rate of annual road traffic injury mortality was reported approximately 18 per 100,000 population before 2007 (Health Environment Management Agency, Ministry of Health. 2011). In response to the rising burden due to RTIs, the Viet Nam government enacted a comprehensive helmet use legislation for motorcyclists in June 2007 (Government of the Socialist Republic of Viet Nam (GOV). 2007). This legislation included obligatory helmet-wearing rules to all two-wheeled and three-wheeled vehicles on all roads, with heavy fines for non-users, and increased enforcement Passmore, JW et al. [2]. The helmet use rate in Viet Nam immediately escalated from 40% in 2007 to over 95% in the following year and has remained steadily above 90% since then (World Health Organization (WHO). 2020a). The introduction of mandatory helmet-wearing legislation in Viet Nam was anticipated to have averted 2,200 deaths and 29,000 head injuries in the year 2008 Olson Z, et al. [3]. The helmetwearing law is useful, especially among less wealthy families. Many countries have presented similar successful results of putting helmet-wearing laws into practice, resulting in head injuries dropping by 33% in Taiwan and 41% in Thailand after implementing such laws Chiu, WT, et al. [4,5]. Similar studies have examined the effectiveness of helmet law enactment on traffic mortality in Viet Nam. At the national level, traffic deaths related to motorcyclists, and total traffic deaths, in the year following the introduction of the helmet law in Viet Nam dropped by 36% and 18%, respectively Passmore, JW et al. [2,6]. The study by Phung et al. across all provinces in Viet Nam revealed that many areas experienced a significant decrease in potential years of life lost (PYLL) of more than 80% due to RTIs, and the summary post law PYLL stopped increasing six months of implementation helmet laws Phung D, et al. [7]. Another study in an outlying district of a large city in Viet Nam found that motorcycle-related injuries and deaths during the post-law period decreased significantly, by 47% and 31%, respectively Ha NT, et al. [8]. Although the efficacy of helmet laws was demonstrated in reducing road injuries and deaths at the national level, evidence in remote areas is still needed. This study aimed to evaluate the impact of mandatory helmet legislation on the potential change of mortality in Lang Son province, a large mountainous region in northern Viet Nam. This province has an area of 8.310,09 km2 with five national highways (Lang Son Provincial Statistics Office. 2019). Before 2007, the government implemented legislation and enforced motorcycle helmet use, but the helmet use rate stayed low as of 2005 Dinh VH, et al. [9].
Method
Data Sources and Data Items
To obtain the traffic-related fatalities, all deaths in Lang Son Province between January 2005 and December 2018 (missing data 2009-2010) were listed based on an official form referred to as the A6. Form A6 is collected according to decision No. 2554/2002/ QD-BYT of the Ministry of Health to register all causes of deaths in the community. Thereby, the registration process was reviewed monthly for each fatal case by the commune health stations (a total of 200 communes). The completeness, sensitivity, and specificity of the A6 system were reported as 93.9%, 75.4%, and 98.4%, respectively Stevenson M, et al. 2012. Based on form A6, all accidentrelated deaths were identified. To evaluate the completeness and the accuracy of the list, all accidents related deaths were compared with the register at the Center of Disease Control of Lang Son Province. To improve the accuracy in identifying the cause of death, each case was reviewed by trained researchers to confirm any underlying causes of death. All cases with unclear causes were listed and then feedback to the corresponding commune health centers to clarify and confirm the cause of death. If a decision was not obtained, trained researchers would call the deceased’s relatives to identify the underlying cause of death. All underlying causes of death were coded following ICD-10. Then, traffic-related fatalities were extracted based on ICD-10 codes (V01-V89). Additionally, the deceased’s information of age, gender, date of death, and the average population of their commune in the corresponding year was collected based on designed data collection forms. Guidelines on how to determine the underlying cause of death and methods to collect data were sent to each commune health station, annually, for data collection.
Data Analysis
First, the crude death rate per 100,000 person-years was estimated. To estimate the age-standardized mortality rate per 100,000 person-years, we applied the accurate statistical data from the World Health Organization standard population for 2000- 2025. Mortality rates were described by year, sex, and age group to observe the trends and differences. Next, Poisson regression was used to estimate the mortality risk ratios (MRR) and 95% confidence interval (95%CI). The cut point of 0.05 of the p-value was considered statistically significant. The data were calculated using Stata version 13.0 (Stata Corp, College Station, Texas). Additional references can be found in the bibliography in the Appendix.
Results
Mortality Caused by Road Traffic Injuries Total Both Sexes
A total of 1841 deaths were identified by the A6 system, which consisted of 1542 and 299 deaths of men and women, respectively. Lang Son province experienced a crude mortality rate of 20.3 per 100.000 person-years from 2005-2018. All mortality indexes in men were higher than that in women. In terms of age, death cases were most prevalent among those aged under 70 years in both sexes. Overall, the estimated proportion of death cases under 70 years of age was as high as 94%, with 96% in men and 84% in women (Table 1). The overall proportion of deaths in both genders due to road traffic injuries was 3.74% (1,841 cases of road traffic injuries vs. 49,253 total cases). Mortality rates from 2005 to 2018 averaged around an approximate value of 20, with the highest in 2011 and the lowest in 2008.
Combining all death cases from 2005 to 2018, the overall agestandardized mortality rate, according to WHO-ASR, was 20.1 per 100.000 person-years. The number of death cases grew gradually from 2005 (148) to 2007 (164), followed by a sharp decrease in the 2007-2008 period (114). It could be explained by the fact that in 2007, the Vietnamese government passed legislation to force helmet wearing for all users of motorcycles, which was the most widely used personal transport in Viet Nam. However, mortality due to injuries in traffic accidences rose drastically between 2011 and 2013 and varied greatly from 2013 onwards. From 2005 to 2018, the adjusted MRR per year increment demonstrated a slight decline (0.991, 95% CI 0.980, 1.001). This declining trend was, however, non-significant (p = 0.093). The proportion of deaths under 70-year-old was notably high and was consistently above 90% in all years (Table 2).
Mortality Due to Road Traffic Injuries in Men
The estimated proportion of deaths due to road traffic injuries was 4.93% (1,542 cases of road traffic injuries vs. 31,262 total cases) in men. The crude mortality rate varied greatly from a low of 25.2 to as high as 46.4 deaths per 100.000 person-years in 2008 and 2011, respectively. When combining all cases from 2005 to 2018, the age-standardized mortality rate per 100.000 personyears by the WHO-ASR was 33.9. Like the overall trend, male deaths increased from 2005 to 2007 and experienced a sharp decline during the 2007-2008 period, followed by an elevated number of deaths from 2008 onwards. This fluctuation was attributed to the introduction of the helmet-wearing laws in 2007. The per-year increment MRR showed a non-significant declining trend (MRR (95% CI): 0.992 (0.980, 1.003), p=0.158). The proportion of deaths among men under the age of 70 was exceptionally high and was above 95% in almost all the years given (Table 3).
Mortality Due to Road Traffic Injuries in Women
The estimated proportion of deaths due to road traffic injuries was 1.66% (299 cases of road traffic injuries vs. 17,990 total cases) in women. Great variability was noticed within the crude mortality rate and MRR value across different years. However, this change in women was regarded as non-significant (Per-year increment MRR (95% CI): 0.987 (0.961, 1.014), p=0.335), which was similar to the mortality rate in men. After standardizing by age, according to WHO-ASR, the overall mortality rate was 6.7 per 100,000 personyears. Compared with men, the proportion of deaths in women under 70 was lower in general and fluctuated between 74.1 in 2013 and up to 94.1 in 2018 (Table 4).
Age-Specific Mortality Rate
Figure 1 illustrates the trend in the age-strata mortality rate by sex between 2005 and 2018 with the exclusion of 2009-2010 data due to missing reports. Overall, the mortality rate was highest among the 20-29 age group (34.7 deaths per 100.000 personyears), followed by the 70-79 age group (29.3 deaths per 100.000 person-years) and 80+ age group (26.5 deaths per 100.000 personyears). Men accounted for most of the death cases due to injuries by traffic incidences. The death rate in men was highest among the 20-29 age group (59.9 deaths per 100.000 person-years) and remained steadily high (above 30%) from 30-39 age group and older, whereas in females, the rate reached a peak at 70-79 age group (21.9 deaths per 100.000 person-years).
Discussion
This is the first study to assess the impact of helmet legislation on mortality related to RTC in Lang Son, a mountainous province in Viet Nam. Data were derived from the national health report system in this province under the A6 form. The present study indicated a slightly decreasing trend in road traffic mortality, but it was not statistically significant, after implementing the mandatory motorcycle helmet law. Although most deaths were aged under 70 years old, differences in ages were observed between the sexes. This study found that helmet law in 2007 reduced road traffic mortality from 2007 to 2008, which was statistically significant. However, between 2011 and 2018 there was only a slight decline, and it is seen as non-significant statistically. The efficacy of the mandatory helmet laws was far from expectation in the mountainous area of Lang Son, specifically. The introduction of helmet wearing laws has been proven to enhance road safety, according to studies in countries neighboring Viet Nam Chiu WT, et al. [4,5], and largescale studies both at the national Passmore JW, et al. [2,6,7], and provincial level Ha NT, et al. [8]. However, after 2007, the RTIsrelated death number in Lang Son province showed a slight yet non-significant declining trend among male and female road users. One study by Ha et al. showed that more severe traffic injuries, including head injuries, were documented during the post-law period Ha NT, et al. [8], which raises questions about the quality of helmets used in the examined region. Using cheap helmets with poor quality and incorrect helmet wearing is common in Viet Nam Passmore JW, et al. [2,10]. Self-awareness of helmet use was also likely to be affected by social norms, safety beliefs, education, and awareness of traffic rules, which are distinctive for each geographical region Phung D, et al. [7], Urie Y, et al. 2016. A review study in Greece proved that the major reasons for noncompliance with the wearing of seat belts and helmets were education and culture Chliaoutakis JE, et al. [11]. Another study in Iran indicated that awareness of traffic legislation and enhancement of safety training towards motorcyclists was the key to helmet use Haqverdi MQ, et al. [12]. Additionally, rural areas might have more RTIs and RTIs-related deaths than modernized areas because of many environmental and cultural factors Chliaoutakis JE, et al. [11,13]. The majority of drivers in mountainous areas are unlicensed and underage Jiang B, et al. [13], which was also regarded as a result of a lack of compliance and policing of the laws. Distance from qualified medical emergency centers was another problem in remote areas, resulting in more deaths as traffic injuries were not treated properly and promptly Jiang B, et al. [13]. The present study also shows that fatalities due to road traffic injuries in men were higher than in women, as reported by previous author’s studies Chiu WT, et al. [4,14,15]. Many studies indicated that alcohol use increases risk among drivers Borges G, et al. [16,17]. In particular, alcohol use was a factor because of the drinking culture in Viet Nam Lincoln M [18]. A study in rural areas of the North of Viet Nam reported that the prevalence of alcohol consumption was 66% among men and 5% among women, respectively Kim BG, et al. [19]. This study has revealed that mortality in men was highest among the 20-29 age group as they are likely to have traffic-related habits, such as risky driving behavior and alcohol consumption Papadakaki M, et al. [20]. Nonetheless, the death rates from 30 to 80+ years of age remained consistently high, irrespective of age group. In contrast, RTIs among females were most prevalent towards the later age group of 70-79. The elderly female population is considered as vulnerable road users. They rarely participated in traffic as direct vehicle users due to the inability to operate a vehicle safely, requiring both physical and mental capability for immediate decisions whilst driving Kim SC, et al. [19]. This study has several limitations. First, the quality of data was unable to be validated due to the nature of secondary data, in particular, such as deaths without reporting by deceased’s relatives. However, the A6 system was proven to be highly reliable for road injury studies Stevenson M et al. 2015; Stevenson M et al. 2012. Secondly, the impact of other factors that may influence mortality rates, such as the availability and readiness, and the quality of the health care system, were not considered, which may distort the findings. However, the present study also suggested a hypothesis regarding the impact of mandatory motorcycle helmet laws on the trend of traffic-related mortality in a mountainous area in Viet Nam. Thirdly, missing data from 2009 to 2010 might not reflect the true effectiveness of helmet-wearing laws implemented in 2007.
Conclusion
The RTIs related annual mortality in Lang Son province decreased slightly but was statistically non-significant, indicating that helmet law implementation in 2007 had little impact on the overall death rates in this area. Therefore, further in-depth studies need to be considered to comprehensively assess the impact of helmet law on death-reducing outcomes in mountainous areas, including feasibility, acceptability, and sustainability.
Mortality Due to Suicide in Viet Nam: Time Trend and Related Socio-Economic Status in A Province and Nationwide from 2005 to 2014
Introduction
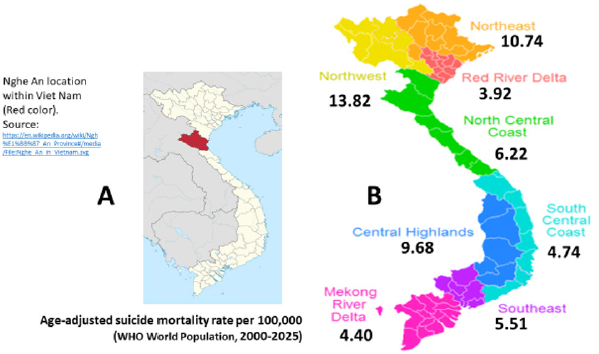
Suicide was defined as a self-imposed death where people kill their selves deliberately and voluntarily (Pilgrim, 2014). Suicide has been acknowledged as a significant social and public health problem with approximately 800,000 people dying due to suicide every year. Suicide accounted for 1.4% of all deaths worldwide, making it the eighteenth leading cause of death in 2016. WHO reported that 79% of suicides occurred in low- and middle-income countries in 2016 WHO [1]. Social inequality has been recognized as a significant risk factor for suicidal behaviors in both developed and developing countries. A previous study indicated that arealevel socioeconomic disadvantage increased the risk of attempting suicide among adolescents in the US Yildiz, et al. [2]. A systematic review from 14 different European countries found that there was a significant association between socioeconomic disadvantage and suicidal behavior from 2005 to 2015 Cairns, et al. [3]. Another review revealed a constituent trend at the individual level indicating that poverty is linked with suicidal ideations and behaviors among people living in low- and middle-income countries Iemmi, et al. [4]. Vietnam is among developing countries located in South East Asia having drastic changes in socio-economic conditions in the past decade. The Vietnam average population has reached 94,666 thousand persons in 2018. The gross domestic product of Vietnam has increased from 1,064 USD per capita in 2011 to 2,389 USD per capita in 2017 General Statistics Office of Vietnam [5]. The crude death rate of Vietnam was 6.8 per 1000 people in 2015 Ministry of Health [6]. However, the mortality due to suicide and related factors are unknown in Vietnam. As suicide is preventable, understanding the changes, consequences and the impact of socioeconomic status is vital to provide evidence-based recommendations. This study aims to examine the changes in mortality due to suicide from 2005 to 2014 in a province and the link between socioeconomic status and mortality due to suicide at the provincial level and national level (Figure 1).
Figure 1:
(A) Nghe An location within Viet Nam and (B) Age-adjusted suicide mortality rate per 100,000 by social-economics status.
Methods
Study Design
This is a descriptive study of the registered death case series due to suicide (ICD-10: X60-X84) in the Nghe an province during 2005-2014 (1,695 cases) and nationwide in 2005 (3,808 cases).
Study Setting
We annually collected data of population by sex and causes of death to suicide for the present study through the A6 mortality registration system. In this study, we selected the Nghe an province to collect data at the provincial level because the database was available for ten year-period from 2005 to 2014. The Nghe an province is located in the North Central Coast with an average population of 3,080,000 people in 2015, ranked as the fourth most populous province in the country General Statistics Office of Vietnam [5]. The number of deaths collected in the Nghe an province covered the period of ten years from 2005-2014. Data at the national level were collected across all 64 provinces/cities in 2005. This year, Viet Nam had 10,769 commune health stations (CHS) of 671 districts within all 64 provinces/cities. There was 67.8% of all 10,769-commune health stations employed physicians. Therefore, this existing advantage official grass-root health system network provided a favorable environment to report the cause of death in general as well as suicide in particular for the present study. The average population number of each commune in Viet Nam was about 7,617 residents. According to the estimated crude death rate of 500 per 100,000 per year, the estimated number of deaths per month at one commune was three cases. Therefore, the head of the commune health station can registry into the A6 book actively as the requirement by the ministry of health Le, et al. [7].
Data Collection
In Vietnam, the national mortality registration system, officially named A6 mortality registration, established by the Ministry of Health in 1992, recorded all deaths from commune-level by each CHS. We annually collected data through A6 mortality registration from 2005-2014 for the Nghe An province and the whole year of 2005 for all 64 provinces and cities. The designated data collection form was yearly sent to 10,769 CHSs of 671 districts within all 64 provinces/cities in 2005. The heads of CHSs were data collectors who recorded all dead cases including death due to suicide including five variables of name, age, sex, date of death, and cause of death. These variables were presented in the data collection form named “Mortality registration”. A guideline of mortality registration and the causes of death including the underlying cause, immediate cause, and a contributing cause of death recommended by WHO was prepared WHO [8]. The printed data collection form with a guideline, each CHS receiving at least one set, was sent to the directors of 64 provinces/cities Health Department with a request letter of data collection. In 2005, we had received 10,184 completed forms of “Mortality registration” (94.6% of all 10,769 CHSs nationwide). Data was inputted into an Excel file for 671 districts within all 64 provinces/cities in 2005. The cause of all deaths was code ICD-10 and suicide (ICD-10: X60-X84) for the present study.
Data Quality Validation
For data validation, after obtaining the mortality database, all causes of death were determined by using the WHO Verbal Autopsy questionnaire that was referred to as “the goal standard” WHO [8]. In Nghe An province, data quality was validated for completeness and accuracy of mortality registration in a District for 1,581 deaths occurring in 2014. For all causes including suicide cases, the estimated completeness was excellent reaching as high as 97% Thuong NV, et al. [9]. The estimated Kappa was excellent for the group of injury including suicide, reaching as high as 81%; the reference group was Verbal Autopsy’s database (unpublished data).
Data Analysis and Statistical Methods
All obtained data about deaths as well as demographic information was computed using Excel software. We checked for a health event and the cause of death and code following ICD-10. The Excel data were exported to STATA 10.0 for analysis. Mortality rates ratios and 95% confidence interval (MRR, 95%CI) were estimated by performing logistic regression analysis, adjusting for sex, age groups (0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, and 80+), the proportion of unknown underlying cause of death (ICD- 10: R01-R99) and all-cause mortality rates. For the time trend during the period 2005-2014, we divided it into five sub periods of two years (2005-2006: reference group, 2007-2008, 2009- 2010, 2011-2012, and 2013-2014). For socioeconomic status, we divided 64 provinces/cities into nine regions from the highest to lowest social-economic developments. Region 1 (reference group) includes the two most populous cities (Hanoi and Hochiminh City). Regions from 2-9 include Red River Delta, Mekong River Delta, South Central Coast, Southeast, North Central Coast, Central Highlands, Northeast, and Northwest.
Ethical Approval
The research protocol was approved by the Ethics Committee of Hanoi Medical University on 25 November 2008.
Results
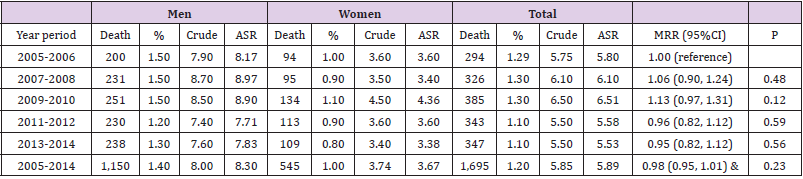
(Table 1) presents data for the Nghe an province. During the ten years of 2005-2014, the system recorded 1,150 dead cases among males, 545 cases among females, and a total of 1,695 deaths due to suicide. After age-adjusted, the suicidal mortality rate per 100,000 for males ranged from 7.40 (in the years of 2011-2012) to 8.70 (in the years of 2007-2008); for females ranged from 3.38 (in the years of 2013-2014) to 4.36 (in the years of 2009-2010). When compared to the period 2005-2006, the risk of death from suicide during 2013-2014 was not significantly changed, MRR, 95%CI: 0.95 (0.82, 1.12), p=0.56. Per increments time-period MRR (95%CI): 0.98 (0.95, 1.01), p for trend=0.23. (Table 2) shows the number of deaths due to suicide for the whole country in 2005 in total and by sex. The system recorded 3,808 dead cases of which 65.0% accounted for males. The suicidal mortality rate per 100,000 among males (7.89) was two times higher than females (3.53), giving a men-to-women ratio of 2.24 (Table 3) presents the number of deaths due to suicide, mortality rate ratios, and 95% confidence interval by nine socioeconomic regions throughout the country in 2005. Nine regions were ordered from the highest to the lowest socio-economic conditions. It is significant that the lower level of socio-economic conditions, the higher the mortality rate ratios. This trend was similar for males and females.
Table 1: Number, crude and age-standardized rate per 100,000 by sex and time during 2005-2014 in the Nghe An province.
Note: ASR: Reference to the WHO World Standard (2000-2025) & per increments time-period MRR (95%CI): 0.98 (0.95, 1.01), p for trend=0.23.
Table 2: Number, crude and age-standardized rate per 100,000 by sex in all 64 provinces/cities in 2005.
Note: ASR: Reference to the WHO World Standard (2000-2025)
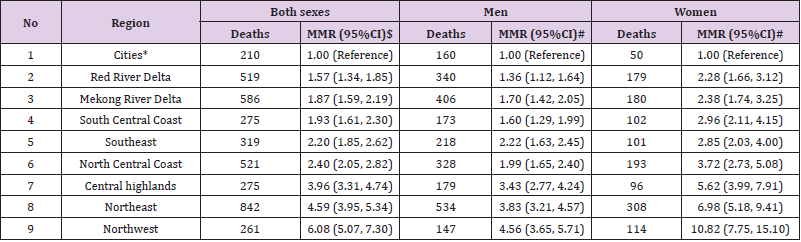
Table 3: Risk of suicide by social-economic status in 2005.
Note: *Hanoi and Ho Chi Minh cities (The reference group) MMR (95%CI): Mortality rates ratio and 95% confidence interval $ adjusted for age and sex; # adjusted for age
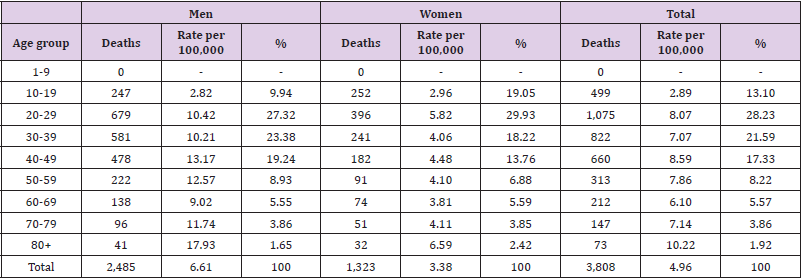
The lowest MMR was found in the Red River Delta (excluding Hanoi) (MMR=1.57; 95%CI=1.34-1.85 in total after being adjusted for age and sex; MMR=1.36; 95%CI=1.12-1.64 for males; MMR=2.28; 95%CI=1.66-3.12 for females; age-adjusted for males and females). The highest MMR was observed in the Northwest (MMR=6.08; 95%CI=5.07-7.30 in total after being adjusted for age and sex; MMR=4.56; 95%CI=3.65-5.71 for males; MMR=10.82; 95%CI=7.75- 15.10 for females; age-adjusted for males and females). Compared to the region with the highest level of socio-economic condition, the individual living in the lowest region had an increased risk of 6.08 times higher to die by suicide. A similar risk was 4.56 times higher for males and 10.82 for females. (Table 4) presents the number of deaths due to suicide and the mortality rate per 100,000 people by age group. The highest mortality rate was found in the age group of 80 and over (10.22 in total, 17.93 for males, and 6.59 for females). The lowest mortality rate was found in the age group of 10-19 (2.89 in total, 2.82 for males, and 2.96 for females). No dead cases due to suicide were recorded for the age group of 1-9. We did not find a particular change in the suicide mortality rate by age group. The men-to-women ratio remains different at all age groups, except a group of 10-19. Among working-aged from 20 to 59, there were 2,870 deaths due to suicide or 75% of 3,808 suicide cases occurred at the working ages.
Table 4: Percent distribution and age-specific suicide mortality per 100,000 by sex and age groups, deaths reported from 64 provinces/ cities in 2005.
Discussion
The main findings have shown a whole country’s suicide status in 2005 and the fatal health event has not been changed during ten year-period from 2005 to 2014 in the Nghe An province, pointing out of suicide being a neglected serious mental health problem. Social determinants of low socioeconomic status or poverty were significantly increased the risk of suicide at disadvantage areas. The other important findings were suicide occurred among senior citizens and about three-fourth of total cases of premature death at working ages. To the best of our knowledge, this is the first study in Vietnam examining the mortality rate due to suicide and the association between suicide and socio-economic status nationwide. The sources of data are reliable because they were collected from the national registration system. The mortality rates are adjusted by age and sex as appropriate. The most important findings from our study are that socio-economic status was negatively associated with suicide mortality rate ratios. Compared to the region with the highest level of socio-economic condition, the individual living in the lowest region had a significantly increased risk of suicide. This finding is in line with previous studies that reported that socioeconomic disadvantage increased the risk of suicide at both the individual level and area-level in many countries Cairns, et al. [2-4]. The suicide dead cases for the whole of Vietnam was 3,803 with an overall mortality rate (ASR) per 100,000 was 5.53, men 7.89 and women 3.53, giving men-to-women ratio 2.24. This mortality rate in Vietnam is much lower than the suicide death rate reported in India (22.0 cases per 100,000) Patel, et al. [10]. The suicide death rate was higher among males that were consistent with findings from other studies Patel, et al. [10,2,4]. We found a significant number of 2,870 deaths due to suicide (75%) occurred during the working ages. This finding raises a concern about adult mental health care in Vietnam and further studies on the causes and risk factors at different occupations. Research worldwide supposed that low socioeconomic conditions, especially unemployment are strongly related to suicidal mortality, and poor psychosocial working conditions associated with suicide Guseva Canu, et al. [11- 13]. Suicidal behaviors include the complex process of thoughts, planning, and attempts. Social support plays an important role in preventing suicide from the beginning of suicidal ideation. Help-seeking behaviors are reported to be correlated with the effectiveness of preventing suicide among working ages Ko, et al. [14]. In Vietnam, researches focus on suicide in the young population more than in the elderly. The highest suicide mortality accounted for the age group from 80 years old in our study suggested that health care for the elderly in Vietnam needs to be studied further. Sociodemographic including social isolation, becoming a widow/ widower, bereavement, health conditions, and mental health problems such as dementia are recognized as risk factors of suicidal behavior in older adults in many countries Conejero, et al. [15]. Along with economic development, Vietnam is facing with challenges of an aging population and social disparities that may increase the prevalence of suicidal behaviors in older people. One of the leading causes of suicide is depression and mental illnesses. One possible explanation for the high suicide mortality at low socioeconomic regions may be that mental health problems have been neglected in these regions with the lack of mental health care and mental health education. Although Vietnam has a good healthcare system from the grassroots level as commune health stations, mental health services are not available and accessible for local people in disadvantaged regions. Individuals with mental illnesses or individuals with suicidal behavior can place a significant financial and social burden on communities. Therefore, understanding mental health problems among different age groups or different socioeconomic conditions is necessary to propose comprehensive preventive programs. Despite these findings, it is important to note some limitations associated with the study. There were potential under-reported deaths due to suicide because people want to hide this sensitive health event and most of the suicide cases were not admitted into hospitals. The other limitation was that there was no available full information on causes of suicide that occurred among the working ages and senior citizens. Our research project is continuing and these limitations will be fixed in the next updated study.
Conclusion
The findings suggest that there was a big gap in mental health care between social-economic status and input support from domestic and international aids to avoid preventable suicide in disadvantaged regions in Viet Nam is highly needed.
Ivermectin for Early Treatment and Prophylaxis of COVID-19 When Exposed to Patients: Author’s Perspective
The world is currently facing a great challenge of the current COVID-19 pandemic that has swept the world’s population and affected all aspects of life including health and economic affairs. This forced many countries to take measures, including preventing popular gatherings and aspects of life in clubs, universities and schools, and closing their borders, in addition to taking physical distancing measures and wearing face masks to prevent the spread of infection [1]. In this regard, we tried to investigate the effect of ivermectin as a prophylaxis in close contacts of confirmed cases of COVID-19. This depended on some previous reports about potentiality of the medication against viruses and our noticing of its effect in treating or reducing infections among patients particularly those in the early stages of the disease. Furthermore, it is previously approved by WHO and US FDA as a safe drug having no serious reported side effects. Moreover, it has been used previously on large scales for mass prophylaxis against some parasitic diseases such as filariasis in epidemic areas. Then, we have registered the first clinical trial allover the world in this regard by date of May 2020 after taking the institute approval and; thereafter, a consent was provided from the participants whom in close contact of cases after discussing the trial and clarifying that it’s the first investigation all over the world [2,3]. Then, more than 65 clinical trials and studies have been done. Nearly, all of them proved positive results of ivermectin use not only for prophylaxis but also in treatment of COVID-19 disease [4]. Moreover, another meta-analysis study proved efficacy of ivermectin for combating the current pandemic [5,6]. Ivermectin is a safe, non-expensive and available drug. It has been previously approved by US FDA as a well-tolerable safe drug used previously for treatment and even mass prophylaxis of several parasitic drugs. It has been investigated in the current pandemic and proved a high effectiveness for chemoprophylaxis against SARS-CoV-2. Use of ivermectin can provide temporary protection that is not longterm immunity as occurs with a vaccine. Therefore, its use may be repeated. Ivermectin could be one of the hopes for ending the current dilemma of SARS-CoV-2 pandemic if used properly under medical supervision [7,8]. It can be used for mass prophylaxis of the whole population at the same time especially for poor and middle-income countries that do not have the facilities to deliver good effective vaccines. Otherwise, it can be used as an emergency in case of exposure or contact with the patient and even used at the onset of infection. However, it may not be useful in treating severe cases because the virus can cause many organs to fail [9,10]. We recommend further studies to confirm the effectiveness of ivermectin in preventing COVID-19 rather than dismiss it on the basis of insufficient evidence. Studying is very easy, does not take much time and does not cause economic or health burden. This also does not require special equipment or abilities except for volunteers to join through the investigation.
Docking Study of Modified Acetohaxamide and Modified Metformin with IRAK Protein
Introduction
In the recent years much of the scientific efforts have been shifted towards computer and its applications to assist explorations in the area of biology sciences and developed a new discipline as bioinformatics [1-3]. One of the important aspect of this area of research the designing of drugs based on the in-silico methods, which ultimately are validated through wet laboratory techniques [4]. Objective of the present study was to evaluate the docking study of modified acetohexamide and modified metformin with IRAK protein, which is involved in diabetes mellitus.
Materials and Methods
Protein sequence which is responsible for diabetes mellitus retrieved from NCBI. This IRAK protein has been used in the sequence. Briefly, acetohexamide and its modified structure; moreover metformin and its modified structure were docked with IRAK protein. The protein data bank was used to retrieve the structure of the protein. Both the protein and ligands were present in sdf files and were converted into pdb in the discovery studio, then these files were convert into pdbqt files in the auto dock software. And finally all the structures were docked with IRAK protein by using vina tool. Detailed dodifications of the parent compounds/ drugs are given here.
Modified Acetohaxamide
Acetohaxamide was modified as: a) We change H45 to S45 b) Then attached O34 to N1
Modified Metformin
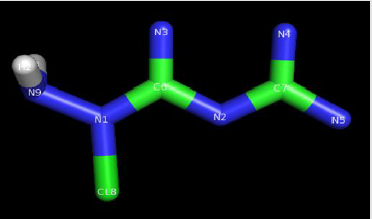
Metformin was modified as: a) Changed H9 into N9. b) Then H8 was changed into Cl8. Structure of modified acetohaxamide and modified metformin are given in Figures 1 & 2.
Figure 1: Modified acetohexamide.
Figure 2: Modified metformin.
Results and Discussion
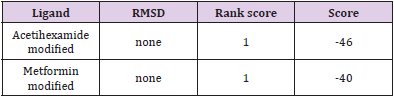
Docking results of our study are given in Table 1. There were 9 pockets in total. Modified acetohaxamide in pocket 5 gave lower bonding energy while modified metformin gave lower bonding energy in many pockets.
Table 1: Docking results of our study.
ADMIT Properties
ADMIT Properties of the candidates are given in Table 2.
Table 2: ADMIT Properties of the candidates.
Drug Scoring by DSX-Online
Drug scoring of the modified drugs are given in Table 3 which were obtained by DSX-online. When we discuss the results of our study, we have come to know that modified metformin was a very good option to develop in real structure and go through wet laboratory validation. It showed very worthy outcome as it showed lower (-4.9) bonding energy as compared to the original compound.
Table 3: Drug scoring of the modified drugs.
Conclusion
Molecular docking study provides an opportunity to identify good drugs that may further be used for validation in actual.
Effect of Phosphorous Fertilizer on the Functioning and Functioning Component of “Brassica Napusl (B.N.) in Rain Fed Agriculture, in Different Groups Phosphorous Soil Fertility
Introduction
“Brassicsa napusl” is oil producing plant which plays important role in the human nutrition with its oil production, and it also has an important role in the food for animals and birds [1]. This plant contains more than 40% oil in its seeds and about 40% protein in its meal and that is why this plant is considered very important [2-4]. High amount of oil contamination in canola and also suitable corrected acidic fat mixture cause its dominance in the world market. Since, more than 90% of the country’s eating oil is imported from abroad, therefore it is important to value this plant [4]. Sandhu, et al. [5] reported in their research shortage of phosphor caused stop in the growth and formation of reproductive organs and grows very slowly and therefore the plant is short in branches and the number of saddles, weight in every 1000seeds. MaJumdar and Sandhu[5]reported that the phosphor fertilizer in the number of seeds in saddle, weight of 1000 seeds has been increased a little but their results did not have any effect in the increase of the functioning. Holmes, et al. [6-7] showed in their research that phosphorous seeds very rarely have high effects on the rape seed’s function and the height of this effect depend on the amount of phosphor in the soil. In Indian soil it has been reported that the phosphorous fertilizers have positive reaction on the functioning and functioning component but its 3effect is little [5,8- 10]. Sajed, et al. [1] in an analysis on the Zucchini with thin layer seeds reported that using of phosphorous fertilizer caused increase in the number of lateral shoots, functioning, number of fruit and the amount of seeds production.
Materials and Methods
The test has taken place in Behbahan in southeast of Khozistan state with the longitude 12`, 15° east and latitude of 36`, 30° north and the height of 320 meters from the sea level. Behbahan is an area with semi deserted climate which located in hot steppe climate. Average of rainfall and 10 years temperature is equal to 313.5 milli meters and 25 degrees centigrade respectively. To understand the effect of phosphorus fertilizer on the functioning and sub functioning of component of canola in the rain fed agriculture in different groups of soil phosphorous fertilizing, 16 tests have been conducted in 4 areas. In each area 4 tests in 4 groups of phosphors usable in soil (less than 3ppm, between 3-6ppm, between 6-10ppm and more than 10ppm) have been repeated in 4 treatments of phosphorous fertilizer in the form of complete random block (0, 25, 50, 75 k.g. p2 o5 in hectare) from the triple super phosphate. It means that in each group of soil fertilizing by the amount of phosphate used in the soil for test in the form of complete random block plan in 4 treatments of phosphoric fertilizer in 4 repetitions. The space between these 4 areas are about 35 to 50 kilo meters and the space from the fields to each area was between 3 to 5 kilometers therefore each test consists of 16 terraces. Each terrace with the length of 5 meters with 8 implant lines with 30 centimeters space between them and the space between the bushes on each row was 5 centimeters, the space of terraces in relation to each other in each side was 1.5 meter and the repetitions space also was 1.5 meter. The date of implanting was fixed on the date of the first rainfall in the autumn in the area. Hayolla 401 was used in the test. Method of cultivation was serial and the amount of used seeds was 8 kilograms in hectare. In all the treatments 60kg/ha pure nitrogen (1/2 base +1/2 at the time of shooting (stemming) from the urea source and 50 kilograms of K2 O in each hectare from the potassium sulfate were used as the base. Gain for removal after ripening of saddlebags from an area equal to (1.5*4 meters or 6 meters) from each terrace was done and seed’s functioning has been determined at the moisture of 10%in hectare. The numbers of bushes in unit, number of seeds in saddlebag, number of saddlebag in bush in unit and the weight of one thousand seeds were measured. In this research MSTAT software was used for statistical analysis. Comparisons of averages have been conducted according to LSD test. Variance analyses of 2 agricultural years have been conducted according to composite variance analysis.
Results and Discussion
Functioning and Functioning Components
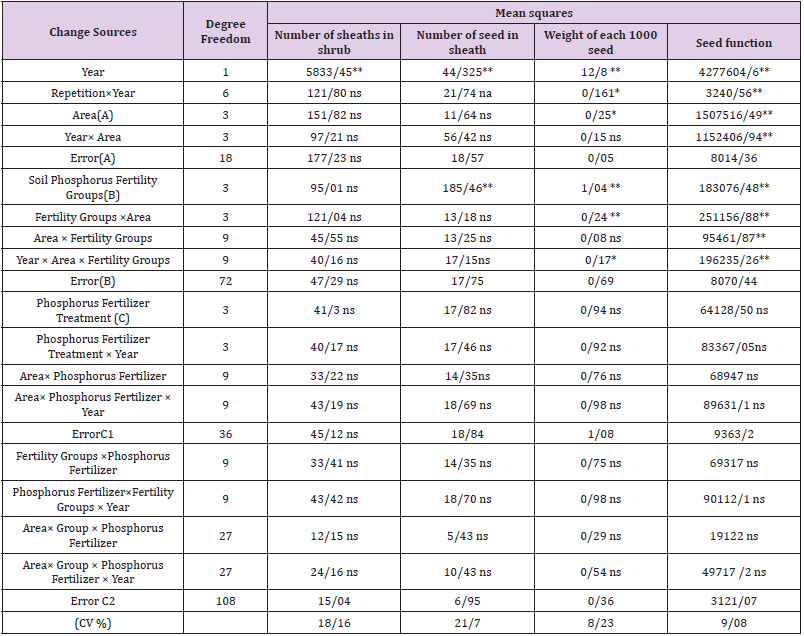
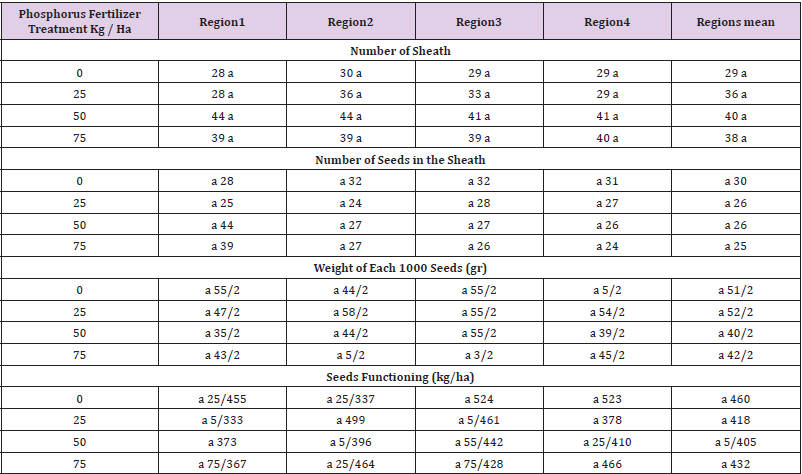
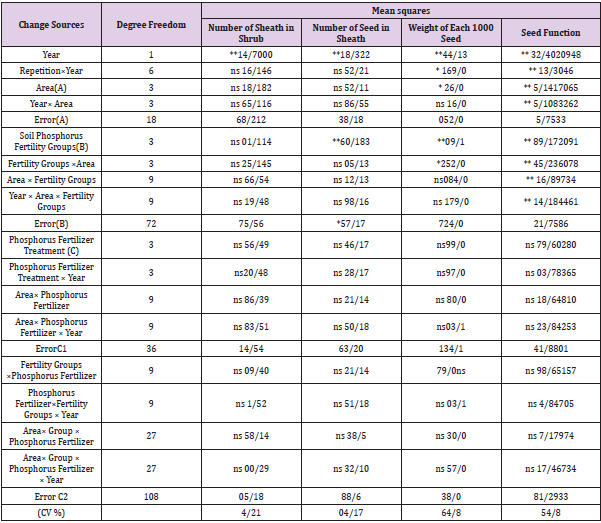
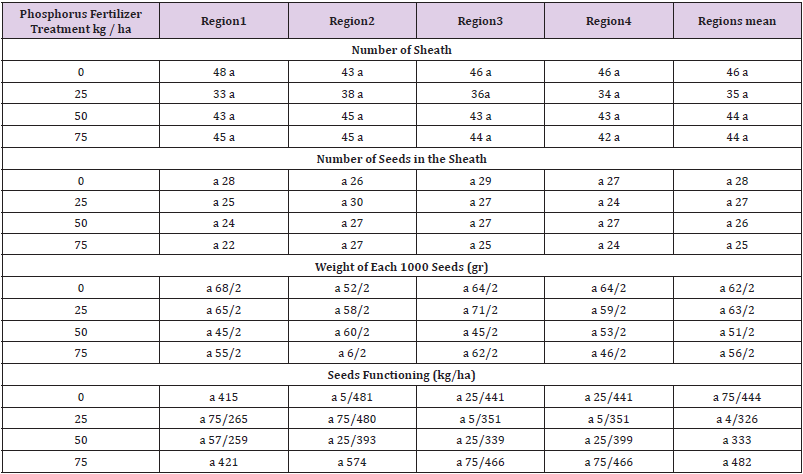
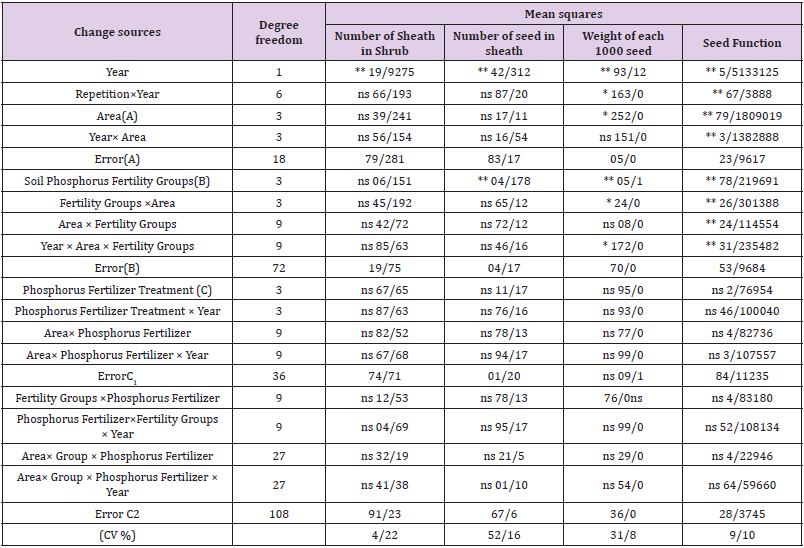
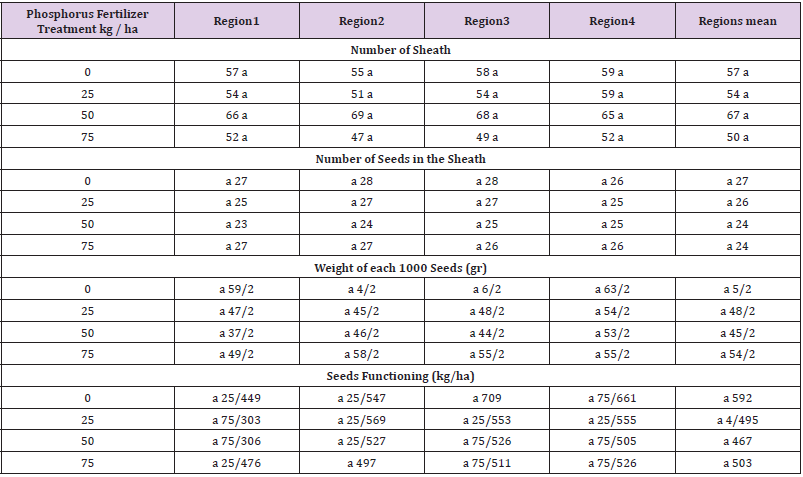
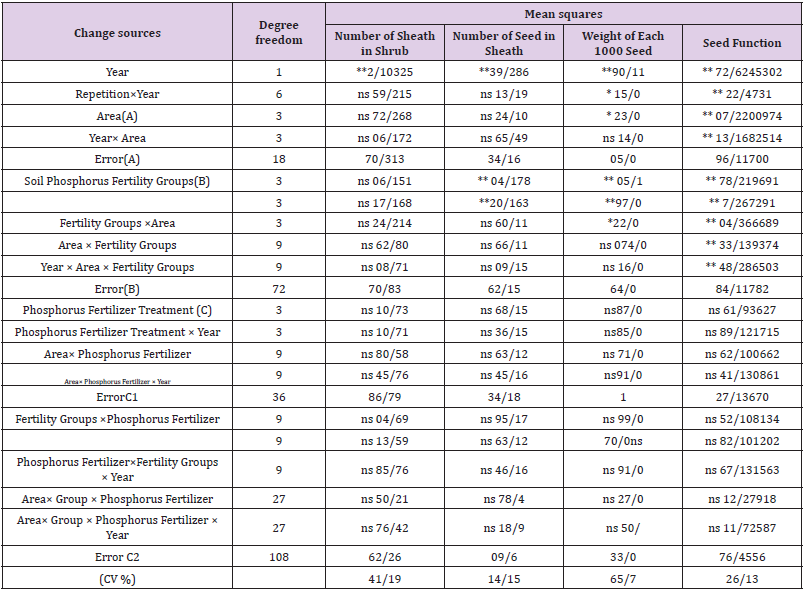
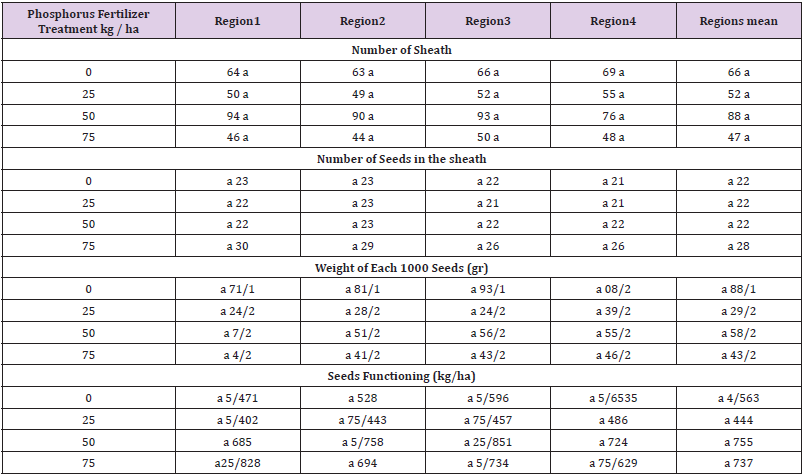
Results of composite variance analysis of 2 agricultural year on the functioning and functioning components showed less than 3 percent ppm in the fertilizing group of phosphorous soil which shows that the effect of phosphorous fertilizer’s treatment on the seed, saddle, number of seeds in the saddle and weight of 1000 seeds isn’t meaningful but the mutual effect (area *fertilizing group) on the seed functioning is meaningful (Table 1). Results obtained from (Table 2) for comparison of fertilizer treatment with witness treatment according to “LSD” test show that there isn’t a meaningful difference through the seed functioning, number of saddle, number of seeds in saddle and thousand seeds weight between witness treatment with the fertilizing and all are located in one group. In 3-6 ppm soil phosphor of fertilizing group, effects of phosphorous fertilizer treatment on the seed functioning, number of saddles, number of seeds in a saddle and weight of 1000 seeds could be found which was not meaningful. The mutual effect (phosphorous fertilizer * fertilizing group) of this group on the seed functioning is meaningful but, on its components, it isn’t meaningful and mutual effect (areas * fertilizing group) on the seed functioning is meaningful (Table 3). According to LSD test there isn’t a meaningful difference between phosphorous fertilizer treatments with phosphorous fertilizer with witness treatment (Table 4).
Table 1: Compound variance analysis functioning and functioning component rape in fertility group soil absorption phosphorus < 3ppm.
Table 2: The mean comparison two-year, number of sheath bags, number of seeds in the sheath, weight of each 1000 seeds, seeds functioning, in phosphorus deferment treatments, in regions with fertility (<3ppm) for applied test (L.S.D).
Note: The effect treatment no significant for properties no mention amount (L.S.D).
Table 3: Compound variance analysis functioning and functioning component rape in fertility group soil absorption phosphorus between 3-6ppm.
Table 4: The mean comparison two-year, number of saddle bags, number of seeds in the saddlebags, weight of each 1000 seeds, seeds functioning, in phosphorus deferment treatments, in regions with fertility (3-6ppm) for applied test (L.S.D).
The composite variance analysis in phosphorous fertilizer treatment absorbable in the soil during two years showed ppm of between 6 to 10. The effect of phosphorous fertilizer treatment and the mutual effect in this group (phosphor fertilizer * fertilizing group) on the functioning and its components was not meaningful. But mutual effect (areas * fertilizing group) on the seed functioning was meaningful. On one hand according to LSD test there wasn’t a meaningful difference between fertilizing treatments with witness treatment in the group. (Tables 5 & 6). In phosphorous soil of fertilizing group of more than 10 ppm results of composite variance analysis for two agricultural years were shown. Phosphorous fertilizing treatment and their mutual effect (phosphor fertilizer * fertilizing group) on the seed’s functioning was meaningful. (Table 7). Results of table 8 show that there isn’t a difference between phosphorous fertilizing treatment with a witness treatment according to LSD test. Considering the results of the test, it can be said that phosphorous fertilizer very rarely have much effects on the seed functioning of Brassica napuls. on the other hand, some of the soil specifications such as organic materials, moisture and the amount of phosphor absorbable in the soil are effective. In the soil with higher amount of organic materials and more suitable moisture the functioning is difference in relation to witness treatment even though it isn’t meaningful.
Table 5: The mean comparison two-year, number of saddle bags, number of seeds in the saddlebags, weight of each 1000 seeds, seeds functioning, in phosphorus deferment treatments, in regions with fertility (3-6ppm) for applied test (L.S.D).
Table 6: The mean comparison two-year, number of saddle bags, number of seeds in the saddlebags, weight of each 1000 seeds, seeds functioning, in phosphorus deferment treatments, in regions with fertility 6-10ppm for applied test (L.S.D).
Note: The effect treatment no significant for properties no mention amount (L.S.D).
Table 7: Compound variance analysis functioning and functioning component rape in fertility group soil absorption phosphorus over >10 ppm.
Table 8: The mean comparison two-year, number of sheath bags, number of seeds in the sheath, weight of each 1000 seeds, seeds functioning, in phosphorus deferment treatments, in regions with fertility (over 10ppm) for applied test (L.S.D).
The amount of phosphor absorbable in soil in group of (3-6) and (6-10) ppm in relation to phosphor group absorbable (less or very high) has suitable effect on the seed functioning. In some of the soil phosphor fertilizing group (medium or high), the amount of fertilizing phosphor, number of saddles and weight of 100 seeds increases a little but their 3effect on the seed functioning is not enough in research on the Brassica napuls plant it has been reported that phosphorous fertilizer does not increase the seed functioning but the height of the plant, number of intial subshrubs and number of saddles will increase a little and also the phosphorous fertilizer has no effect on the number of seeds and weight in 1000 seeds. Mojumdar and Sandhu [5] reported that phosphorous fertilizer increases the number of seeds and weight of 1000seeds a little. But their results have no effects on the increment of seed function. Holmes and AInseley [7-8] mentioned that the phosphorous fertilizer very rarely causes effects on the B.N seed functioning and its effect depends on the amount of phosphor in the soil. In India regarding the effect of phosphorous fertilizer on the function and its components no positive reaction was noticed. The reason for it is due to the soil condition. Singh, et al [9-14] regarding Indian soil reported that the phosphorous fertilizers have positive effect on the functioning and its components, but it is a little. On research on the medical plant of paper seed pumpkin reported that more phosphorous fertilizer showed the number of seeds in the bush, weight of dried seed in bush and maximum weight of dried seed in each square meter. Also, the use of phosphorous fertilizer causes increase in the number of lateral shoots, functioning and the number of fruit and amount of medical pumpkin seed’s production [1,15].
Conclusion
Different treatment of phosphorous fertilizer in all groups of soil phosphorous fertilizing have no meaningful effect on the functioning and functioning component of B.N. (number of saddles, number of seeds in the saddle and weight of 1000 seeds.
The Mosquitoes (Diptera: Culicidae) and their Medical and Veterinary Importance in an Arid Zone of Central Iran
Introduction
More than 17% of infectious diseases are vector-borne diseases that cause 700,000 deaths annually [1]. About 60% of emerging and re-emerging infectious diseases are zoonoses. In the last three decades, more than 30 new human pathogens have been identified, 75% of which are of animal origin [2]. In the Eastern Mediterranean Region of WHO, zoonoses are a public health threat [3]. Mosquitoes are considered the most important arthropods in medicine and health due to the transmission of pathogens causing some important infectious diseases such as malaria, filariasis, and arboviral diseases [4-6] and are present worldwide except Antarctica [7]. Mosquitoes belong to the order Diptera, suborder Nematocera, and family Culicidae [8]. Culicidae has two subfamilies Anophelinae and Culicinae and 70 species in Iran. Mansonia uniformis was the newest genus and species that was added to the mosquito fauna in Iran [9]. Mosquito larvae are found in a variety of environments, including natural and man-made habitats, with temporary or permanent water sources, stagnant or running water, contaminated or clean water, with or without vegetation. Mosquito larvae are also found in small places where water collects, such as pots, used tires, and animal footprints [4,5]. According to the latest study conducted of mosquito fauna in Kashan, there are 3 genera and 13 species in this county including Anopheles. claviger, An. maculipennis s.l., An. superpictus s.l., An. turkhudi, Culex deserticola, Cx. hortensis, Cx. mimeticus, Cx. perexiguus, Cx. pipiens, Cx. theileri, Culiseta annulata, Cs. longiareolata, Cs. subochrea [10], also Cx. torrentium larva has been found at an ovitrap in Kashan County [11], and species of Anopheles multicolor, Culex modestus, Aedes caspius, and Ae. pulcritarsis have been reported from previous studies in this county [12,13]. Susceptibility to mosquito-borne diseases has increased due to globalization and led to the spread of emerging and re-emerging pathogens in new and old habitats. Economic and social factors, global trade, transport and tourism have caused the spread of vectors and diseases transmitted by them [7,14]. In livestock, mosquito bites may cause stress and pain, resulting in reduced livestock fitness. In addition, mosquitoes can also transmit pathogen between livestock reservoirs (episodic) and, humans (zoonotic diseases) [7]. Mosquitoes can transmit pathogens in Iran, including causes of arboviral diseases (avian pox, bovine ephemeral fever, dengue fever, Rift Valley fever, West Nile fever), bacterial diseases (Anthrax, Tularemia), helminthic diseases or helminthiases (mosquito-borne filariasis), protozoans (Avian malaria, Human malaria) [6]. Due to global climate change, more animal and human populations will be exposed to these pathogens [7]. Due to the importance of mosquitoes in human and animal health, the present study was performed to evaluate diseases transmitted by mosquitoes and the status of these diseases in Kashan County
Mosquito- Borne Diseases in Kashan County
To find diseases transmitted by mosquitoes, we searched the terms “mosquito-borne pathogens”, “mosquito-borne diseases”, “mosquito-borne infections”, “mosquito-borne viruses”. Data were extracted from all articles. An intensive search of scientific literature was reviewed using the search term in the following databases: “PubMed”, “Web of Knowledge”, “Scopus”, “Google Scholar”, “SID”, etc. Mosquito-borne disease names including ‘malaria, avian malaria, West Nile (WN) fever, Dengue (DEN) fever, Sindbis (SIN) fever, lymphatic filariasis, tularemia, tularaemia, anthrax’, lumpy skin, and mosquito-borne pathogens such as Plasmodium, Dirofilaria, Flavivirus, Alphavirus, Phlebovirus, Orthobunyavirus were reviewed. Also, cases of mosquito-borne diseases identified in Kashan, were inquired from Kashan University of Medical Sciences and Kashan Veterinary Organization.
Protozoal Diseases
Human Malaria
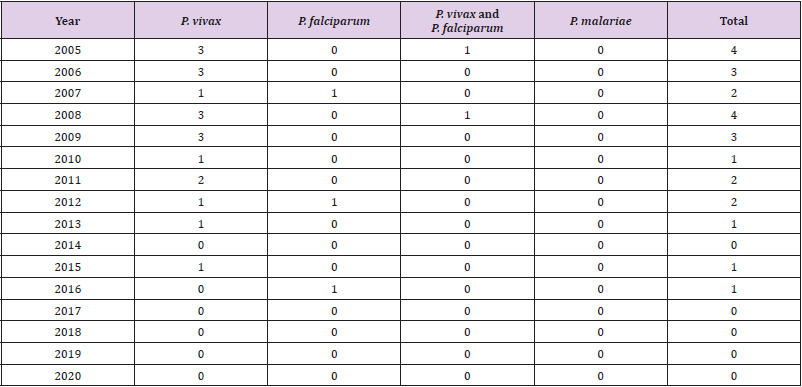
Malaria is a health threat. This disease is caused by a parasite that is transmitted to humans through the bite of infected Anopheles mosquitoes and can be prevented and treated. In 2019, almost half of the world’s population was at risk for malaria. Most deaths occur in sub-Saharan Africa. However, Southeast Asia, Eastern Mediterranean, Western Pacific, and Americas also have the case of diseases and deaths. In 2019, cases and the number of deaths due to malaria were 229 million and 409,000, respectively. Plasmodium falciparum and Plasmodium vivax are the most important parasite species of human malaria [15,16], which are biologically transmitted by some anopheline mosquitoes [17]. Many effective efforts have been done for malaria control in the past that caused decreased morbidity and mortality in Iran [18,19]. At the present, malaria has been eliminated in most parts of Iran [20]. A malaria pre-elimination program started in Iran in 2009, restricted the local transmission of this disease [21]. The results of a study showed that the imported cases (from the eastern neighboring countries) have increased from 2009 onward, compared to indigenous cases [20]. WHO (2020) reported the Islamic Republic of Iran had no indigenous malaria cases in 2018 and 2019[15]. Kashan County is located in the central plateau region of Iran, where have a lower risk of malaria infection compared to southern/ southeastern parts. Seven Anopheles species (An. maculipennis Meigen s.l., An. sacharovi Favre, An. culicifacies Giles s.l., An. dthali Patton, An. fluviatilis James s.l., An. stephensi Liston, An. superpictus Grassi s.l.) are malaria vectors in Iran [22]. Anopheles superpictus s.l. species is the most abundant and distributed among Anopheles in Kashan County [10,12,13], and is one of the seven species of malaria vectors in Iran [22,23], also An. maculipennis s.l. [10,12], An. claviger [10,12,13], An. multicolor [12,13], and An. turkhudi [10] have been reported from Kashan County. An. maculipennis s.l. is the main vector in the Caspian coast in northern Iran [24]. In Kashan County, from 1986 to 1997, a total of 498 malaria patients have been reported, of which 95% were Afghan immigrants and 5% were Iranian travelers or immigrants from other parts of the country [13]. There are malaria cases from 2005 to 2020 and parasite species in Table 1, all malaria cases in these years were reported from Afghan immigrants.
Table 1: Human malaria cases and parasite species from 2005 to 2020 in Kashan County.
Avian Malaria (Bird Malaria)
Culicidae mosquitoes belonging to different genera (Culex, Coquillettidia, Aedes, Mansonia, Culisetta, Anopheles, Psorophora) transmit many species of avian Plasmodium [25-29]. Bird malaria has been reported in some provinces of Iran including Fars Province [30,31], and Mazandaran Province [32,33]. Kalani et al. for the first time, reported two hematozoa, including Aegyptianella and Plasmodium in Isfahan Province [34]. But no information is available about the vectors of this disease in birds in these provinces. Culex pipiens is the main vector in some countries including Austria [35], Japan [28], Portugal [36], Spain [37], and Turkey [38]. In Austria Cx. torrentium is also main vector [35]. Culex theileri in Portugal and Spain are known as a vector [36,37]. Aedes caspius s.l., Cx. modestus and Cx. perexiguus are vectors in Spain [37]. No avian malaria has been reported from birds in Kashan County, but there are species of Aedes caspius s.l, Cx. pipiens, Cx. torrentium, Cx. theileri, Cx. modestus and Cx. perexiguus in different districts of the county [10-12].
Mosquito-Borne Viruses (Arboviral Diseases)
Bovine Ephemeral Fever
Bovine ephemeral fever is an arthropod-borne disease of cattle and water buffaloes. The disease agent is from the genus Ephemerovirus within the Rhabdoviridae family. Biting midges (Diptera: Ceratopogonidae) and mosquitoes Aedes, Anopheles and Culex are known as the main vectors [39-42]. There is no information about the vectors of the virus in Iran [6]. In Iran, bovine ephemeral fever virus has been found in cattle and water buffalo in provinces Razavi Khorasan [43], Khuzistan [44], Fars, Tehran, West Azerbaijan [45], and Qazvin [46]. The virus has not been reported in Kashan County.
West Nile Fever
West Nile Virus (WNV) distributed in Africa, Europe, the Middle East, North America, and West Asia, is a member of the family Flaviviridae, Flavivirus genus, and belongs to the Japanese encephalitis complex. Human is most often infected by infected mosquito bites. Genus Culex is the principal vector of WNV, in particular Cx. pipiens. Birds are the reservoir hosts of WNV, In Europe, Africa, Middle East, and Asia [1,47]. In nature WNV is held in a mosquito-bird-mosquito transmission cycle and Culex spp. are the main vectors [48]. In a study, Cx. pipiens infection with WNV was reported in Guilan Province, north of Iran [49]. Also, it has been reported that Aedes caspius to be infected with the virus in the northwest of Iran [50]. West Nile virus has been identified by ELISA in horses in at least 26 of the 31 Iranian provinces and is the most important and most widespread mosquito-borne arbovirus in Iran [51-53]. Culex perexiguus, and Cx. modestus have also been reported as the principal vectors of WNV in Asia and Europe [54]. These mosquitoes have been reported from Kashan County [10,12], but no information is available about them, and birds infected with WNV in this County.
Lumpy Skin Disease (LSD)
Lumpy skin disease is a vector-borne pox disease of domestic cattle and Asian water buffalo and is characterized by the appearance of skin nodules [55]. Lumpy skin disease virus (LSDV) is a member of the genus Capripoxvirus and the family Poxviridae and is one of the most warning diseases in cattle from the perspective of OIE (Organization for World Health Animal Diseases), so it is mandatory that disease-free countries report it to OIE within 24 hours of confirmation of the disease [56]. The original vector is probably different in geographical areas, including the common stable fly (Stomoxys calcitrans), mosquitoes such as Aedes aegypti, and some species of African mites Rhipicephalus and Amblyomma spp. [55]. Lumpy skin disease (LSD) outbreaks in Kenya were caused incidence of Aedes natronius and Culex mirificus mosquitoes [57]. Culex spp. mosquitoes that feed multiple times on different hosts can increase the probability of transmission [58]. Lumpy skin disease was first seen in Zambia in 1929, then spread to all parts of the Sub-Saharan Africa as well as Madagascar. This disease was first observed in 2014 in western Iran. The outbreak of the disease in Iran followed the spread of the disease in neighboring western countries, including Turkey and Iraq. This disease has been reported from 31 provinces of the country with different prevalence percentages and epidemiological data of the disease indicate that the disease has spread epidemically among cattle and calves of different breeds. High risk provinces were including the provinces of West Azerbaijan, Kurdistan, Ilam, Khuzestan, and Kermanshah. Epidemiological data of the disease in the country show that the prevalence is less than 1% (0.55%) [59]. This disease has not been observed in Kashan so far, but due to the presence of the disease in livestock of neighboring provinces, there is a risk of disease for Kashan.
Mosquito-Borne Filariases
Dirofilariasis
Dirofilaria is a long, slender parasitic worm that infects a variety of mammals. The infection is transmitted by mosquito bites. There are many species of Dirofilaria, but infection in humans is usually caused by three species: D. immitis, D. repens, and D. tenuis. Dogs and wild dogs such as foxes and wolves are the main natural hosts of these three species. Dirofilaria immitis is also known as “heart worm” [60]. Dirofilaria repens and D. immitis infection has been found in humans and dogs in 16 provinces of Iran including Guilan [61], Garmsar [62], East Azarbijan Province [63], Gilan, Mazandaran, Golestan, East, and West Azerbaijan, Ardebil, Markazi, Isfahan, Khorassan, Khuzestan and Hormozgan [64,65], Ahvaz City [66,67], Kerman [68], and Meshkin-Shahr [69]. Vector of D. immitis in Ardebil Province is Cx. theileri [61,70]. There is no information about this disease in Kashan County.
Setariasis (Setariosis)
Setaria (Nematoda: Spirurida: Onchocercidae: Setariinae) infects ruminants. Species of Setaria digitata, S. equina, S. labiatopapillosa, S. marshali, S. cervi have been reported in horses, cattle, sheep, goats, donkeys, wild sheep, and water buffalo in 10 provinces [71-82]. This nematod is transmitted by mosquito species of the genera Aedes, Anopheles, Armigeres Theobald, Culex and Mansonia [83]. Setaria equine has been found from Anopheles maculipennis females in Ardebil Province [70]. There is no information about this disease in Kashan County.
Checklist of Mosquitoes (Diptera: Culicidae) of Kashan County
A checklist of mosquitoes of Kashan County is presented as follow: Family Culicidae Meigen, 1818 Subfamily Anophelinae Grassi, 1900 Genus Anopheles Meigen, 1818 Subgenus Anopheles Meigen, 1818 1. An. (Ano.) claviger (Meigen, 1804) 2. An. (Ano.) maculipennis s. l. Meigen, 1818 Subgenus Cellia Theobald, 1902 1. An. (Cel.) superpictus s. l. Grassi, 1899 2. An. (Cel.) multicolor Combouliu, 1902 3. An. (Cel.) turkhudi Liston, 1901 Subfamily Culicinae Meigen, 1818 Tribe Aedini Neveu-Lemaire, 1902 Genus Aedes Meigen, 1818 Subgenus Ochlerotatus Lynch Arribálzaga, 1891 1. Ae. (Och.) caspius (Pallas, 1771) s.l. [Oc. caspius (Pallas) s.l.] 2. Ae. (Och.) pulcritarsis (Rondani, 1872) [Oc. pulcritarsis (Rondani)] Tribe Culicini Meigen, 1818 Genus Culex Linneaus, 1758 Subgenus Barraudius Edwards, 1921 1. Cx. (Bar.) modestus Ficalbi, 1889 Subgenus Culex Linneaus, 1758 1. Cx. (Cux.) pipiens Linnaeus, 1758 (see Note 26) 2. Cx. (Cux.) torrentium Martini, 1925 3. Cx. (Cux.) perexiguus Theobald, 1903 4. Cx. (Cux.) theileri Theobald, 1903 5. Cx. (Cux.) mimeticus Noè, 1899 Subgenus Maillotia Theoald, 1907 1. Cx. (Mai.) deserticola Kirkpatrick, 1924 2. Cx. (Mai.) hortensis Ficalbi, 1889 Tribe Culisetini Belkin, 1962 Genus Culiseta Felt, 1904 Subgenus Allotheobaldia Broelemann, 1919 1. Cs. (All.) longiareolata (Macquart, 1838) Subgenus Culiseta Felt, 1904 1. Cs. (Cus.) annulata (Schrank, 1776) 2. Cs. (Cus.) subochrea (Edwards, 1921)
Conclusion
Information about the role of mosquitoes in the transmission of pathogens in Kashan County is limited. Due to the construction of bird garden in Qamsar, and entry of birds from 17 different countries into this area, and importance of mosquito-borne diseases in the country, vector-borne disease surveillance, is necessary for the best integrated vector management. The life cycle of mosquitoes requires two types of environments: aquatic habitats (eggs, larvae, and pupae) and terrestrial ecosystems (adults) [17]. Control strategies of mosquitoes may be to controlling adults or larvae at the breeding sites. Methods of insecticide-treated bed nets (ITN) and indoors residual spraying (IRS) are used to control adult mosquitoes [84]. But these methods are not effective in controlling exophilic and exophagic mosquitoes [85]. Environmental management is one of the most effective and sustainable methods for controlling of vectors of diseases. The concept of environmental management for mosquito control is a range of methods including long-lasting physical transformation of larval habitats, temporary changes of larval habitats, which makes the environmental conditions unsuitable for vector breeding, and reduce human/vector/ pathogen contact [86]. Application of these methods depending on the type of larval habitat can reduce mosquito populations and reduce the risk of disease transmission.
Effects of Drug Addiction and Abuse on Academic Performance of Students Within the Age of 14-30 Years
Introduction
Drugs are substances that influence the physical and mental state of persons essentially and destructively any substance that can prompt compulsion, abuse and reliance is a medication [1]. The level of enslavement for drugs increments with every day of utilization. On the off chance that drugs are not accessible, the patient shows discriminating withdrawal manifestations when prompt restorative consideration is expected to forestall physical and mental decay, even demise (Psychology) [2]. World Health Organization (WHO 2002 and 2003) characterizes tranquilize as a compound substance planned for indicative, restorative or palliative utilization or for altering physiological elements of man and creature, [south_Asia_Regional_Profile_Sept_2005/08_ bangladesh.pdf]. Opium has been used for medical purposes since 3500 years ago. Morphine was discovered in 1806 and codeine in 1832. Cocaine was extracted from leaves of coca plant in 1860. Injecting morphine and heroin was expanded at the beginning of 20th century [3-5]. Addiction to drugs is one of the saddest tragedies of modern man which threatens his life. Despite this, unfortunately tendency toward these deadly substances, especially opiate substances, is daily increasing, especially among adolescents [6]. Drug consumption in Iran has started thousands of years ago. Over the last century, expanded consumption of heroin and other narcotics, especially ecstasy and cocaine during past decades has complicated the condition of drug abuse in our country [3,7-10]. Studies conducted by United Nations show that more than 180,000,000 people in the world are addicted to drugs [11-14]. On the other hand, quitting addiction is complicated and difficult and is not successful most of the times [15]. Hashish is the most prevalent drug being used in America and many other countries. In North America, south and center of America most problems occur due to consumption of cocaine [16]. Most used drugs in Europe are cannabis, heroin, amphetamine and hallucinatory, besides to ecstasy. In most Asian countries most problematic drugs are cannabis and opiate substances [17,18]. According to a United Nations Office on Drugs and Crime (UNODC) Report (2005), about 200 million people, or 5 percent of the world’s population age between 15 and 65 have used drugs at least once in the last 12 months. Likewise, according to the World Drug (2005) reported that, the use of illicit drugs in all Nations has increased in recent years. For most of Europe and Asia, opiates accounted for 62 percent of all drug treatment sought in 2003. A survey in the Czech Republic showed that 37% of new drug users were teenagers between 15 and 19 years old. In Egypt, drug use – in particular heroin use – is becoming a serious problem and nearly 6 percent of secondary and tertiary school students admit to having experimented with drugs [15]. The history of human race has also been the history of drug abuse [19]. History tells us that the Chinese used Opium as a cure of dysentery before the 18th century. European countries such as Britain and Holland were known to exchange opium growth in their colonies for tea and silk with China [20].
State of Drug Abuse and Drug Addiction Global Perspective
Drug abuse is a global problem that poses a great danger to the lives of individuals, society and political stability and security in many countries [United Nations 1995]. According to the United Nations (2005), the use of illicit drugs has increased throughout the world and the major world trend is the increasing availability of many kinds of drugs among ever widening spectrum of consumers [21-23]. A study carried out by the London School of Economics in 1980, on students learning behavior revealed a relationship between drug abuse addiction and poor academic results [Otieno et al. 1994]. The continent, over recent years has experienced an upsurge in the production, distribution and consumption of drugs with the youth and young adults being most affected [24-26]. In Ethiopia, it is reported that 82 per cent of the street children in Addis Ababa use some kind of a drug [27-29]. According to the United Nations (UN) statistics (2013), 37,000 people in Africa die annually from diseases associated with drug abuse.
State of Drug Abuse and Drug Addiction: Bangladesh Perspective
Adolescents, especially those who are socially weak, may choose drug abuse as a means to integrate themselves into a peer group, and thereby increase self-esteem and decrease anxiety [30]. They feel failure and frustrated. Parental factors exert significant influence on the overall development of the child. It is not only impairing public health, but also corrupting institutions, retarding socio-economic development, and threatening political stability and, in some cases, impacting state security [31-33]. Due to drug addiction, criminal activities are increasing with alarming rate in all over the country. Especially in urban areas like Dhaka, Chittagong, Rajshahi, Khulna, Barisal and Sylhet. According to Family Health International (FHI) about 50 lac people of Bangladesh are drug addicted [34].
Materials and Methods
The present study designed as descriptive, qualitative and cross-sectional type, conducted in various Rehabilitation centers located in Dhaka city. The study population was consist of students in Rehabilitation center aged 14 to 30 years old. Random sampling technique (Probability sampling) was applied for determining sample size and data collection. Data was collected by a self-administered questionnaire, which was pre-tested. The investigation was conducted upon 143 students in various rehab center located in the Dhaka city located in the Dhaka city. The questionnaire and findings are based on the objectives and variables. Data was processed and analyzed using Microsoft Excel and SPSS version 21.00.
Ethical Considerations
Approval letter for conducting research was taken from American International University- Bangladesh (AIUB) during MPH courses
Results and Findings
In the present study, 34.97 percent of the participants were 14-18 year olds, 38.46 percent of the participants were 19-23 year olds, 18.18 percent were 24-27 year olds and 8.39 percent were 28-30 year olds (Figure 1), 79.72 percent of the participants were males, and 20.28 percent of the participants were females. Showed that 15.38 percent of the participants were below SSC, 29.37 percent passed SSC, 34.97 percent passed HSC, 16.08 percent passed bachelors and 4.20 percent passed masters (Figure 2). In the present study, 62.94 percent participants were lived in urban area whereas, 37.06 percent were lived in rural area, 62.94 percent participants were lived in nuclear family and 37.06 percent were lived in join family. The analysis indicates that 37.76% of the respondents’ abused drugs for the first time at the age of 14-18 years old, 33.57% of the respondents abused drugs for the first time at the age of 19-23 years old, 20.28% were abused drugs for the first time at the age of 24-27 years old and 8.39% were abused drugs for the first time at the age of 28-30 years old.
Figure 1: Distribution of the participants by their age.
Figure 2: Distribution of the educational qualification of the participants.
Figure 3: Distribution of age of the participants when did they abuse drugs for the first time.
The present investigation indicates that 37.76% of the respondents abused drugs for the first time at the age of 14-18 years old, 33.57% of the respondents abused drugs for the first time at the age of 19-23 years old, 20.28% were abused drugs for the first time at the age of 24-27 years old and 8.39% were abused drugs for the first time at the age of 28-30 years old (Figure 3). (Figure 4) indicates that 16.78% of the respondents have been addict for 0-2 years, 18.89% of the respondents have been addict for 2-3 years, 38.46% of the respondents have been addict for 3-4 years and 25.87% of the respondents have been addict for more than 4 years. The analysis indicates that 44.76% of the respondents were influenced to take drugs by friends, 28.67% were by classmates, 15.38% were by relatives, 6.29% were by himself and 4.90% were influenced by others (Figure 5). According to the results, the respondents indicated that Yaba was major abused drugs in the age between 14-30 years. 31.47% of the respondent were abused Yaba, 21.68% were abused Phensedyl, 20.98% were abused Cannabis (ganja), 14.69% were abused heroin, 7.69% were abused Sleeping pills (seduxen) and 3.49% were abused other drugs (Figure 6).
Figure 4: Distribution of the length of time of participant’s taking drugs.
Figure 5: Distribution of participants those who are influenced to take drugs by.
Figure 6: Distribution of major abused drugs which causes addiction by the participants.
The analysis showed that 70.63% of the respondents abused more than one drug at the same time and 29.37% of the respondent abused only one drug at the same time. Figure 7 indicated that Yaba was major abused drugs in the age between 14-30 years. 31.47% of the respondent were abused Yaba, 21.68% were abused Phensedyl, 20.98% were abused Cannabis (ganja), 14.69% were abused heroin, 7.69% were abused Sleeping pills (seduxen) and 3.49% were abused other drugs. The findings summerized in (Figure 8) shows that, 27.27% of the respondent abuse drugs due to peer pressure, 21.68% of the respondents due to frustration, 16.78 % due to mental stress relief,10.49% due to curiosity, 12.59% due to build-up self-esteem& ability to increase performance.6.99% due to sense of euphoria, and 4.20% due to easy access or availability of drugs. The analysis showed that, 56.64% of the respondents had more than one reason of drug addiction and 43.36% of the respondent had only one reason of drug addiction.
Figure 7: Distribution of participants how did they procure money for drugs.
Figure 8: Distribution of the Major causes of drug abuse and drug addiction of the participants.
The analysis showed that 28.67 % of the respondent were procure money for drugs from illegal works, 13.29% were procure money from own earning, 46.15% were procure money from family and 11.89% were procure money from friends. The results on the effects of drug abuse experienced by the respondents indicate that headache, memory loss, gastritis, insomnia, bad tempered and instability were serious effects of drug abuse that the respondents experienced as expressed by the percentage of 5.59, 4.90, 13.29, 32.87, 20.28 and 23.07 respectively. In addition, the study also found out that red eyes, nervousness and fatigue also have been observed due to drug abuse and drug addiction. (Figure 9) shows that 74.83% of the respondent had more than one physiological consequences and 25.17% of the respondent had only one physiological consequences. Figure 9 showed that, 29.37% of the respondent were encouraged to get into the rehab center by friends, 11.19% were encouraged by teachers, 44.75% were encouraged by their families and 14.69% were encouraged by their relatives. It was evident that, 27.28 % of the respondent were engaged with any criminal activities but majority 72.72% of the respondent did not engaged with any kind of criminal activities. The analysis showed that, 70.63% of the respondents abused more than one drug at the same time and 29.37% of the respondent abused only one drug at the same tim.
Figure 9:
A. Distribution of physiological consequences due to drug addiction by the participants. B. Distribution of participants those who are influenced to take drugs by.
It was found that, 28.67 % of the respondent were procure money for drugs from illegal works, 13.29% were procure money from own earning, 46.15% were procure money from family and 11.89% were procure money from friends (Figure 7). The present results reveals on the effects of drug abuse experienced by the respondents indicate that headache, memory loss, gastritis, insomnia, bad tempered and instability were serious effects of drug abuse that the respondents experienced as expressed by the percentage of 5.59,4.90,13.29,32.87,20.28 and 23.07 respectively. In addition, the study also found out that red eyes, nervousness and fatigue also have been observed due to drug abuse and drug addiction. The result of the present study showed that 74.83% of the respondent had more than one physiological consequences and 25.17% of the respondent had only one physiological consequences. (Figure 10) showed that, 29.37% of the respondent were encouraged to get into the rehab center by friends, 11.19% were encouraged by teachers, 44.75% were encouraged by their families and 14.69% were encouraged by their relatives. The third objective sought to find from respondents the likely effects of drug addiction on academic performance. The results on the effects of drug addiction on academic performance among respondents was severe grade decades, drop out ,low concentration span, discontinuation of academic career, lack of interest in extra curriculum activities and strained relationship with other students.25.87% of the respondent had grade decades, 7.69% had drop out, 41.26% had low concentration span,9.09% had discontinuation of academic career,4.90% had lack of interest in extra curriculum activities and 11.19% of the respondent had strained relationship with other students (Figure 11). The analysis indicates that 28.67 % of the respondent received treatment from rehabilitation centers for 1 year, 19.58% of the respondent received treatment for 2 years, 7.69% of the respondent received treatment for more than 2 years and 44.06% of the respondent received treatment for 6 months (Figure 12).
Figure 10: Distribution of participants those who encouraged to get into the rehab center by.
Figure 11: Distribution of effects of drug addiction on academic performance of participants.
Figure 12: Distribution of the participants’ period of time to receive treatment from Rehab center.
Discussion
According to Family Health International about 50 lac people of Bangladesh are drug addicted. The World Health Organization [WHO, 2003] estimates that, about 50 cror people in the world are affected by the abuse of drugs. Many of the adolescent users begin their experiment with drugs though smoking cannabis (marijuana) cigarettes, use of heroin. Typically, they begin by sniffing it (snorting) and finally injecting it intravenously (shooting the mainline) [35,36]. Findings on how the subjects developed their habits indicated that 50% first took drugs through drug user friends and under pressure, 20% out of frustration and 15% out of curiosity. The study reports that the highest incidence of addiction occurred between 23-26 years old [37]. Due to drug addiction, criminal activities are increasing at an alarming rate all over the country, especially in urban areas like Dhaka, Chittagong, Rajshahi, Khulna, Barisal and Sylhet. The present study tries to explore the effects of drug addiction and drug abuse on academic performance of young students [38,39]. The purpose of this study was to determine the effects of drug abuse and drug addiction on Academic performance of students within age 14-30 years. The study includes the addict’s students who received treatment from drug treatment and rehabilitation centers. The majority of the drug users were male even though the involvement of female was also evident. In the present study 79.72% of the respondents were males and 20.28% of the respondents were females. The present, YABA is the most frequently abused drugs by the respondents. The study also shows that70.63% of the respondents were abused more than one drug at the same time. The study also found that, 56.64% of the respondents had more than one reason of drug addiction and 43.36% of the respondents had only one reason of drug addiction. About 27.27% of the respondents were engaged with any criminal acts [40]. The present study found that insomnia, headache, memory loss, gastritis, bad-tempered and instability were serious physiological effects of drug abuse and drug addiction of the respondents. The current study shows that drug abuse and drug addiction have adversely affected the academic performance of the respondents. Declining grades, drop out, low concentration span, discontinuation of academic career, strained relationship with other students and lack of interest in extra-curriculum activities are the adverse effects of drug addiction which directly related with academic career of the respondents. This is in agreement with United Nations (2005) view that cognitive and behavioral problems experienced by alcohol and drug-using youth may interfere with their academic performance and also present obstacles to learning. Again drugs abused effect the brain; this result in major decline in the functions carried out by the brain. According to Abot (2005) drugs affect the student’s concentration span, which is further drastically reduced setting in boredom sets in much faster than for non-drug and substance abusing students. The students who abuses drugs is likely to lose interest in schoolwork including extra curriculum activities. The study shows that the respondents were encouraged to get into the Rehab center by Friends, by teachers, by family members and by their relatives [41]. In the present study, 28.67% of the respondents stayed in the rehab center for 1 year to more than 2 years and majority of the respondents were stayed in the rehab center for 6 months. More than half of the respondents (83.22 %) were regret for their actions and (88.21 %) of the respondents want to go back to a healthy life.
Conclusion
Most of the respondents that involved in drug use and abuse fall between the age brackets of 14-23 years. Yaba is the most frequently abused drugs by the respondents. Phensedyl, Cannabis ganja, heroin and sleeping pills (Seduxen) are also abused in significant proportion. They are addicted to drugs because of the influence of peer groups, frustration, mental stress relief, curiosity. The study found out that insomnia, headache, memory loss, gastritis, bad-tempered and instability were serious physiological effects of drug abuse and drug addiction of the respondents. Drug abuse and addiction have adversely affected the academic performance of the respondents. More so, the effects of drug abuse and addiction have resulted into respondent declining grades, drop out, law concentration span, discontinuation of academic career, strained relationship with other students and lack of interest in extracurriculum activities. Government should prevent the cultivation/ sales of deadly herbs that encourage drug abuse. Government should strictly enforce its existing laws against drug abuse through its regulatory agencies [42]. Parents and guardians should endeavor to monitor their children, so that they do not engage in drug abuse. Counseling education should be introduced in campuses to revive those who have already been engaging in the act [43-57].
Creation of Innovated Macrocyclic Sulfazan-Formazan Compounds and Linear Sulfazan-Formazan for the first Time Globally with their Assay as Antifungal
Introduction
Sulfazan compounds were invented for the first time globally by researcher Prof. Dr. Nagham Aljamali in 2019 was named as sulfazan compounds [1-3]. The researcher also developed and devised the basics of their preparation methods, the conditions of each method, their interactions, the reaction medium, and their naming. Then she developed them into cyclic sulfazan and cyclic formazan compounds [4-7] that were also prepared for the first time in April 2021 in this current study and also developed and established methods for their preparation and reaction conditions, and the current research included the preparation of innovative types of cyclic sulfazan compounds, linear sulfazan, cyclic formazan and linear formazan.
Sulfazan Compounds
Are organic sulfur compounds that were prepared in researches [1-3] as first time by Dr. Nagham Aljamali in 2019 from several reactions that include the reaction of the coupling of basic mercapto and thiol compounds with azo compounds using one of the conditions (pyridine, piperidine, triethylamine,…) [7-9] and its chemical structure is (Ar-N=N-S-R).
Formazan Compounds
Are a class of organic compounds of importance in organic chemistry because it contains two highly effective groups (-N=N=C-N-) or (-N=N-C-N-NH-) in several fields of chemistry [8-14], especially in coordination chemistry [15,16], as a ligand because they contain free electrons and donor atoms to coordinate with ions to form complexes [17-19] and types of them as anticancer [20-22].
Cyclic Formazan and Cyclic Sulfazan
These compounds invented by the researcher Dr. Nagham Aljamali in April 2021 for the first time [4,5]. Initial foundations and methods for preparing these compounds were established, and to determine the conditions [4-8] of their interaction and the auxiliary factors used to prepare them. They were considered among the organic compounds of importance in organic chemistry because they contain two highly effective groups in several fields of chemistry, especially in coordination chemistry, as a ligands because they contain doublets. Free electrons and donor atoms to coordinate with ions to form complexes [23-28]. Formazan also enter many anti-bacterial [29-33] and anti-fungal compounds [34- 37] and types of cancer [38,39], especially breast and laryngeal cancers, as anti-bacterial and anti-fungal, and other studies [40,41].
Instruments and Experimental Part
All melting points were uncorrected and dignified on an electrothermal apparatus (Switzerland) in an open capillary tube. FT.IR spectra were detailed on Fourier transform infrared spectrometer (FT-IR) in( FT-IR- 3600) infrared spectrometer via employing KBr Pellet technique., 1H.NMR spectra were recorded in DMSO-d6 as solvent using (TMS) as internal standard and chemical shifts are expressed as (δppm)., also Mass– Spectra for some of them other studies like evaluation against types of fungi).
Procedures
Preparation of Compounds{1, 2}
Cysteine (0.01 mole) was dissolved in (30ml) absolute ethanol with semicarbazide(0.01 mole) with refluxing for (10hrs) in presence of phosphoric acid as closing agent, according to procedures [6-9], the product filtered ,dried ,recrystallized to yield Oxadiazole amine Derivative-Compound [1], which reacted (0.01 mole) in (50 ml) absolute ethanol with p-iodobenzaldehyde (0.02 mole) with refluxing for (3hrs) in presence of (3 drops of glacial acetic acid), according to procedure [6- 9], the product filtered ,dried ,recrystallized to yield Aldamine -Compound [2] (Figure 1).
Figure 1: Synthesis of Compounds{1,2}.
Creation of Inventive Macrocyclic Sulfazan-Formazan Compound{3}
Aldamine compound [2]was (0.01 mole) dissolved in basic solution from (Piprydine) then reacted with (0.02 mole) of diazo salt of o- phenyl diamine via many steps in basic solution to formation invented Macrocyclic Sulfazan-Formazan after (48hrs), the product filtered ,dried ,washed by distilled water, recrystallized to yield Invented Macrocyclic Sulfazan- Formazan [3] by following literatures [1-5].
Creation of Inventive Macrocyclic Sulfazan-Formazan Compound{4}
Macrocyclic Sulfazan-Formazan Compound{3} refluxed (0.01 mole) for (4hrs) in (40ml) absolute ethanol in presence of cupper acetate (0.92gm) in closing step of amine group in ortho- position from azo- group to formation Triazole derivative according to procedures [6,7] , the product filtered ,dried ,recrystallized to yield Invented Macrocyclic Sulfazan-formazan of Triazole derivative [4], according to procedures [6-10] (Figure 2).
Figure 2: Creation of Invented Macrocyclic Sulfazan- Formazan Compounds {3,4}.
Creation of Inventive Linear Sulfazan- Formazan Compound{5}
Aldamine Compound [2] about (0.01 mole) was reacted basic solution (Pyridine) via many steps in coupling reaction with (0.03 mole) of p-bromophenyl diazonium salt in basic medium, after (10hrs), the product filtered ,dried ,washed by distilled water, recrystallized to yield Invented Sulfazan- Formazan [5], according to procedures [1-5].
Creation of Inventive Linear Sulfazan- Formazan Compound{6}
Aldamine Compound [2] about (0.01 mole) was reacted basic solution (Pipyridine) via many steps in coupling reaction with (0.03 mole) of p-methoxyphenyl diazonium salt in basic medium, after (10hrs), the product filtered ,dried ,washed by distilled water, recrystallized to yield Invented Sulfazan- Formazan [6], according to procedures [1-5] (Figure 3).
Figure 3: Creation of Invented Sulfazan- Formazan Compounds {5,6}.
Results and Discussion
In recently study, various of Invented Macrocyclic Sulfazan- Formazan Compounds and linear Sulfazan- Formazan have been created in same procedure that followed and invented [1-5] by Dr. Nagham in year 2019 that got a patent to invention of Macrocyclic Sulfazan-Formazan compounds, then several studies were carried out to improve these innovative compounds by the using of spectral identification like : 1H.NMR spectra, FT.IR- Spectra, Mass- Spectra., other studies represented by (Melting points, evaluation against types of fungi)., all the results are revealed in Tables and figures.
Spectral Analysis
FT.IR- Spectral Evidence of Invented Macrocyclic Sulfazan- Formazan Compounds and Linear Sulfazan-Formazan Compounds : The first characterization of innovative compounds by shifting of frequencies of Aldamine group (CH=N) in starting compounds (Imine compounds) that were about at (1612) Cm-1 in starting compounds (imine compounds) were shifted to (1627) Cm-1 for (-C=N-) due to formation of Macrocyclic Formazan and band at (1310) Cm-1 due to (-S-N=N-) to Sulfazan group in Macrocyclic Sulfazan compound , also appearance of three bands due to partitions of azo group of Sulfazan and Formazan in Macrocycle (-N=N-) are (1423 ,1455, 1490) Cm-1 for (-N=N-S-)-Sulfazan and (-N=N-C-)-Formazan in compound {3}., While in compound [4] appeared band at (3298) Cm-1 due to (NH) in Triazole ring as a result of ring closure that resulted from closing of amine group in ortho- position with Azo group to formation Triazole ring, besides to appearance of bands at (1629) Cm-1 for (-C=N-) due to formation of Macrocyclic Formazan and band at (1304) Cm-1 due to (-S-N=N-) to Sulfazan group in Macrocyclic Sulfazan compound , also appearance of three bands due to partitions of azo group of Sulfazan and Formazan in Macrocycle (-N=N-) are (1432 ,1456, 1498) Cm-1 for (-N=N-S-)-Sulfazan and (-N=N-C-)-Formazan., and other compound like this., all frequencies explained according to reference [35].
1H.NMR- Spectral Evidence of Invented Macrocyclic Sulfazan-Formazan Compounds and Linear Sulfazan- Formazan Compounds
The second characterization of innovative compounds by disappearance of peak for imine group (CH=N) in starting compound (Aldamine compound) that were at δ (8.27) in Compound {2} (starting compound) due to formation of (N=C-N=N) for (Formazan and Sulfazan groups) in created compounds, also in compound [4] appeared peak at δ (5.35) due to (NH) in Triazole ring as a result of ring closure that resulted from closing of amine group in ortho- position with Azo group to formation Triazole ring, all peaks explained according to reference [35].
Mass– Spectral Evidence of Invented Macrocyclic Sulfazan-Formazan Compounds and Linear Sulfazan- Formazan Compounds
The third characterization of inventive compounds by partition of innovative cyclic compounds via appearance of fragments in spectra in Figures 4-6.
Figure 4: Mass–Spectrum of Invented Macrocyclic Sulfazan- Formazan Compound{3}.
Figure 5: Mass–Spectrum of Invented Macrocyclic Sulfazan- Formazan of Triazole Compound {4}.
Figure 6: Mass–Spectrum of Invented Linear Sulfazan- Formazan Compound{5}.
Other Characterization
All Invented Macrocyclic Sulfazan- Formazan and Linear Sulfazan-Formazan were studied to collect all The chemical and physical properties, in Table 1.
Antifungal Assay [17,18] of Invented Sulfazan-Formazan Derivatives
The assessment of Invented Macrocyclic Sulfazan-Formazan derivatives and Invented Linear Sulfazan-Formazan derivatives tested against kinds of fungi epitomized through (Aspergillus) with (Candida Albicans) for all the invented compounds at three concentrations were occupied range of three analyses that occupied for each concentration (20, 30, 50μgm) rendering to the method [17,18], Table 2. The results improved that the Invented Macrocyclic Sulfazan-Formazan compounds and Invented Linear Sulfazan- Formazan compounds have good results as inhibitor of fungi growth and the invented macrocyclic Sulfazan- Formazan compound [5] has more activity than other invented macrocyclic Sulfazan-formazan compound due to structure of compound [5] involved sufazan group (-N=N-S-) with formazan group (-N=CN= N-) more than other compounds besides to (Br) atoms , while compound [6] has less inhibition activity due to its structure ( -OCH3) methoxy group.
Table 1: Other characterization of Invented Macrocyclic Formazan Compounds.
Table 2: Antifungal Assay of Invented Sulfazan-Formazan Compounds in Concentration (30μ.gm).
All Invented Macrocyclic Sulfazan-Formazan derivatives and Invented Linear Sulfazan-Formazan compounds gave good evidences for their structures via various spectral techniques, also some of them studied against types of fungi that gave good data and good activity in inhibition of growth of Fungi.