Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
The Use of Measurement Uncertainty on Clinical Laboratories Results
Opinion
Clinical laboratories should produce the required data and analytical results in order to achieve the true interpretation and use of the results. The objective of a measurement is to detect an estimate for the true value of analytical results. The measurement uncertainty (MU) is a parameter, associated with the result of a measurement that characterizes the distribution of the values that could reasonably be attributed to the measure and [1]. Clinicians might interpret better at clinical decision levels knowing the MU of a test. The interpretation of values which are close to cut-off levels may change, when they evaluated with MU. Therefore, reporting clinical laboratories results with estimation of MU is significant to show measurements that contained within the true limits and the level of confidence. With the acceptance of the International Organization for Standardization (ISO) laboratory standard Medical Laboratories – Particular Requirements for Quality and Competence (ISO 15189), laboratories have been required to provide estimates of MU for all quantitative test results [2]. According to ISO 15189, MU should be provide available by the laboratory on request (Figure 1).
Figure 1: According to ISO 15189, MU should be provide available by the laboratory on request.
MU provides quantitative estimates of the level of confidence that a laboratory has in its analytical precision of test results and therefore represents the expected variability in a laboratory result if the test is repeated a second time [3]. MU consists measuring procedure components which are pre- and postan alytical variation and biological variation [4]. Limit values of laboratories results (within MU) are being more careful follow-up and alarming the clinician. MU is the appropriate approach for meaningfully comparing measurement results with reference values. In our opinion, the clinicians must take into account of the MU during the evaluation of clinical laboratories results. We trust that MU can help clinicians and patients to better understand the accuracy of results and evaluate clinical decision levels. At the same time, MU is useful for clinical decision but have yet to show their strength in laboratory medicine. Also, the MU is still new in the field of quantity measurement. The pros and cons of uncertainty should elucidate on their use in practical performance specifications.
Institutional Review Board Roles and Functions to Conduct Clinical Trials at a Medium-Sized Regional Hospital, Japan
Introduction
Clinical trials are a key resource for the discovery of new diagnostic, treatment and prevention methods for disease. Many of today’s most introduced prevention and treatment modalities are based on previous clinical trial results. Clinical trials are an important part of improving quality of health care [1]. Facilitators of participation in clinical trials have been linked to recommendations by reliable health care providers, a supportive family, satisfactory doctor-patient relationship that depends on culture, financial incentives, anticipation of a personal benefit to participants, convenience to participants and culturally appropriate advertisements [2]. To address such facilitators and barriers of clinical trial participation in communities, we report our institutional review board (IRB) of Matsunami General Hospital [3]. A typical central medical institution anchor of the region, Japan.
Role of IRB
IRB has the authority for jurisdiction over research involving primarily drugs, devices and biology’s that must be approved by the Ministry of Health, Labor and Welfare, Japan. The clinical research or trials are defined as: “research conducted on human subjects to determine or verify pharmacologic, absorption, metabolism, safety and efficacy of one or more research products, in addition to clinical or pharmacodynamics effects and adverse events or reactions.”
IRB Members
We do not include a member of more than one ethic committee and managers of the institution in which the trial is going to be concluded. IRB consists of following background members:
a) 3 medical experts with experience in international study designed in compliance with good clinical practice
b) 1 nurse who has over 20-year experience in clinical practice
c) 1 pharmacist who has over 20-year experience in clinical practice
d) 3 non-medical persons
e) 2 persons with learned knowledge and experience who are unaffiliated with the institution
f) 2 persons in clerical support unit
Current statue of Clinical Trial Acceptance
A total of 32 clinical trials were completed in our institution between 2004 and 2016 (Table 1). Research subjects were distributed different disciplines, approximately 30% being diabetes mellitus-related.
Table 1: Contracted clinical research 2004-2016.
Comments
Clinical trials accepted in our institution are in quality and quantity inferior as compared with those in government institutions of similar size [4]. One of major differences may result from the provoked evolution of regulations. Our institution regulations on clinical trials may be structured with the aim of attracting more community-based trials to the regional community and to meet the criteria of management policies. Aside from the institutional incentives, the lack of accreditation of IRBs raises concerns regarding the compliance of organizations, IRBs or the researchers and/or the research staff with a human study protection attempt, quality assurance and quality improvement measure accountability, adequate resources availability, and transparency by communication and interaction with the community, research participants and researchers. Encouraging IRBs to apply for accreditation would strengthen any flaws in structure of operating protocols and help our institutional circumstance to have its goal to raise its share in drug research investments. Before approving the trials, IRBs should introduce the policy to better assess the existing uncertainties in a given investigation study, employing tools, such as survey of specialists, official announcement of the protocols and systematic reviews with a focus on identifying golden standard treatment that should be contained in consideration of the proposed trial, as previously described [5]. It may be the most plausible to make an assertion that the IRB needs contributing to improvement in quality and quantity of clinical trials.
Spinal Dermal Sinus and Sacral Endothelial Cyst with Recurrent Bacterial Meningitis: A Case Report and Systematic Review of the Literature
Introduction
Congenital dermal sinus is dermoid and epithelial cyst from skin tissue or epithelial tissue residue in the cranial cavity or intraspinal canal during embryonic development. The entry of sinus is usually located in the occipital, back, waist midline skin, with hair hyperplasia, and sinus connect skin with nerve tissue which constitute the anatomical basis of infection of the nervous system. We report 1 case of recurrent bacterial meningitis caused by sacral sinus and sacral canal endothelial cysts. Meanwhile, the related literatures are systematically searched and reviewed, which provide experience for the diagnosis and treatment of bacterial meningitis caused by congenital sinus.
Case Presentation
A previously healthy 8 month-old boy was admitted because of a 9 days’ fever and a 2 times’ convulsions. Physical examination revealed a febrile, obtunded with anterior bulging fontanel. Neck stiffness was noted. Laboratory tests showed WBC10.6×109/L, neutrophile granulocyte 58.5%. C-reactive protein (CRP) 93mg/L (normal value below 8 mg/L). An urgent computed tomography (CT) of the head was performed, with normal results. Bacterial meningitis was suspected and a lumbar puncture confirmed the diagnosis. The cerebro-spinal fluid (CSF) was 8200×106/L white blood cells with neutrophile granulocyte 88%, increased total protein (190,7 mg/L) and decreased glu-cose levels 0.2mmol/L. Serum glucose level was normal (5mmol/L). The child received intravenous dexamethasone and ceftriaxone (100mg/kg. d) as empiric treatment which results of poor effects, so vancomycin (60mg/kg. d) was added. Escherichia coli with ESBL (+) was confirmed in both double blood and cerebrospinal fluid (CSF) cultures, which was sensitive to carbapenems and amino glycosides. So we replaced ceftriaxone with meropenem (120mg/kg. d) in treatment.
Five days later, the child’s condition improved, with fever resolution. Suddenly, 10 days after hospital admission, the child manifested irritability and lethargy. Moreover, a bulging fontanel was noted at the physical examination. During the hospitalization time (51days) of the child, we used cefatriaxone (4days), vancomycin (21days), meropenem (47days), compound sulfamethoxazole (60mg/kg.d) (7days, combined with meropenem), amikacin15mg/ kg.d (15days, combined with meropenem). We noticed that after the condition and examinations of child had been improved for several days, it would become worsen again. This had happened several times. Then, the patient transferred to another hospital. A needle sized skin dimpling was noticed at sacrococcygeal this time. And the child’s parents told the doctor that sacrococcygeal sinus was found after the child was born. Brain MRI revealed ventricular dilatation and hydrocephalus. Lumbar vertebra MRI revealed sacral sinus, extra medullary subdural nodules of the lumbar spine, neurogenic tumors, meningioma. The patient received sacrosacral sinus excision.
Pathology (lumbosacral skin and subcutaneous tissue) revealed cuticle cyst in subcutaneous tissue. After the surgery, the patient received postoperative continuous lateral ventricle drainage for 21days. And amikacin (10mg/kg) with dexamethasone (0.5mg) were given by lateral ventricle for 7days. The brain MRI showed that the hydrocephalus was alleviated. 21days after the surgery, the patient received lateral ventriculo ventriculoperitoneal shunt. After 3 days anti-infection with ceftazidime (120mg/kg. d), the patient was discharged. One month after discharge, the child had recurrent fever again, with 2 times’ convulsions. New symptoms appeared, including astasia, urine incontinence and constipation. Lumbar vertebra MRI showed that intraspinal tumor and syringomyelia at the lumbar 3-4 level. The patient received intraspinal occupying resection and neurolysis. Intraspinal occupying culture revealed: Escherichia coli. Pathology suggested: mature teratoma. Antibiotics were used according to drug sensitivity test. After the treatment, the child recovered well and was discharged from the hospital. The patient was followed up with no recurrence.
Systematic Review of the Literature
Using dermal sinus and bacterial meningitis as key words, we searched databases including PubMed, Embase and Chinese databases such as CNKI, VIP, and Wanfang database from the beginning of the database to November 2017. We have 22 Chinese articles and 77 English articles. Repetitive studies, non-Chinese or English literature that cannot be analysis from the cases were excluded; we got 68 cases bacterial meningitis caused by sacral sinus. Most of the patients, age from neonate [1] to adult [2], complained of fever, headache, vomiting and convulsions. Few people had back pain, lower limb pain and limping as initial symptoms. And some patients didn’t have typical symptoms while headache and vomit were transient.
Some patients were admitted in hospital without any symptoms and signs except fever. That may be related to repeated infection of low toxicity bacteria, opportunistic pathogens and early application of antibiotics. Some patients who had obscure onset and prolonged course were misdiagnosed as tuberculosis meningitis due to lack of systemic toxic symptoms and acute inflammatory reaction. In cases reported on the dermal sinus, there were 13 cases of occipital, 1 case of neck, 5 cases of chest and 18 cases in lumbosacral region. In those cases with pathogens isolated from blood or cerebrospinal fluid samples, 2 samples were proteus, 3 samples were Staphylococcus aureus, 3 samples were Escherichia coli, 2 samples were group B Streptococcus and 1 sample was Klebsiella pneumoniae. Other pathogens include Pseudomonas aeruginosa, anaerobes, Staphylococcus aureus and Escherichia coli [3]. Most of the pathogenic bacteria were derived from the normal colonization on the skin. Morgenstern believed that different bacterial meningitis caused by anatomic abnormalities (including the sinus), can provide some useful suggestion in the location of the abnormalities [4]. However, the results of the pathogen literature analysis showed that the implications were very limited.
Discussion
It was quite hard to diagnose and treat congenital dermal sinus if the patients only had clinical manifestations of bacterial meningitis, while with insidious sinus orifice and without local infection. It may be hard for the patients having dermal sinus with spinal endothelial cysts or epithelial cysts to have sinus and cysts completely removed because of tight adhesion with the spinal cord or nerve root. In this case, although the child had definite infectious pathogen and received enough dosage of effective antibiotics, meningitis was still recurring. He was treated by surgical excision of the dermal sinus in the first surgery. But the cyst in the spinal canal was not thoroughly removed. So the patient had re-infection of the same pathogen. In the second surgery, after the cyst in the spinal canal was thoroughly removed, no recurrence was found. So early diagnosis and surgical treatment is appreciated. Escherichia coli are one of the common pathogen in infant’s bacterial meningitis. It is necessary to find out the reason why the symptoms recurring after receiving appropriate antibiotics treatment. Immune deficiency, congenital anatomic abnormality, trauma and operation are all important f actors of recurrent meningitis. From the experience of this case, there was something we should pay attention to:
a. Inquire the patient history detailed;
b. Systematic physical examination, especially the midline craniospinal axis;
c. Proper imaging examination besides brain MRI.
Spinal MRI is the best imaging method for the diagnosis of intraspinal cysts, which can indicate the position of the cyst, and provide a reliable basis for clinical diagnosis and operation. In the treatment, we should actively search for the infection pathogens, select sensitive drugs according to the results of drug sensitivity experiments combined with clinical efficacy, and combined treatment should be taken into consideration when necessary. Early surgical treatment should be considered while controlling infection. In this case, the prognosis of the patient was good after thoroughly surgical removal of the sinus and spinal canal cyst which were the primary infective focus. But for children with complications of intracranial and intraspinal abscess, which caused severe neurological dysfunction, without timely surgery, the prognosis was poor. Delayed diagnosis is mainly due to the doctor’ unawareness of this type of anatomic abnormality. The importance of early diagnosis, proper examinations, surgical treatment and close follow up in patients with recurrent meningitis is stressed.
Role of Matrixmetalloproteinases in Periodontal Disease – A Review
Introduction
Periodontal disease is a common, complex, inflammatory disease characterized by the destruction of tooth supporting soft and hard tissues of the periodontium, including alveolar bone and periodontal ligament. Although the inflammation is initiated by bacteria, the tissues breakdown events that lead to the clinical signs of disease result from the host inflammatory response that develops to combat the challenge presented by the subgingival biofilm. Microbial products trigger the release of pro inflammatory cytokines and host derived enzymes, the excessive and/or dysregulated production of which results in tissue breakdown. Once the immune and inflammatory processes are initiated and the complex cytokine network is established, various inflammatory molecules play a direct role in the degradation of both non mineralized and mineralized tissues of the periodontium. One such family of inflammatory molecules is the matrix metalloproteinases which are released from different cell types present in the lesion including macrophages, leukocytes and fibroblasts or other resident cells. Human MMPs also called as Matrixins, are a group of structurally related but genetically distinct endopeptidase enzymes. They are produced at low levels or not at all in restingstate adult tissues. Control of extracellular proteolysis by MMP is critically important for survival of organisms, and this is performed by interaction with various inhibitors like endogenous inhibitors, TIMPs. This review article gives an overview of the physiological functions of MMPs and its role in the pathogenesis of periodontal diseases.
History
Study by Woessner [1] was considered as a milestone before the discovery of first MMP, Later in that year, Jerome Gross and Charles Lapiere [2] were the first to identify an MMP using a biochemical approach. In 1966, MMP-1 was purified from tadpole tail fin and back skin. MMP-2 was identified as a higher molecular mass species (72 kDa) with gelatinolytic activity; purified from human rheumatoid synovial fibroblasts by Goldberg and colleagues whereas MMP-3 was identified as a lower molecular mass species (54 kDa) from rabbit synovial fibroblasts by the Werb laboratory in 1985 and subsequently named Stromelysin [3]. In the late 1980s, Ed Harris et al. [4] first proposed the name MMP. Subsequently, the International Union of Biochemistry and Molecular Biology designated the family with the unique name MMPs and assigned each family member with an enzyme number. To be classified as an MMP family member, the enzyme should meet the following requirements:
a) proteolysis of at least one extracellular matrix(ECM) component
b) catalysis dependent on zinc at the active site
c) activation by proteinases or organomercurials
d) inhibited by EDTA,10-phenanthroline and any one of the TIMPs
e) cDNA has sequence homology to MMP-1
Initially it was thought that the proteinase be secreted in a proform but now this no longer holds as MMP-11 and MMP-28 are intracellular activated by furin and are secreted in active forms; even the membrane-bound MMPs are not necessarily secreted [5].
Classification of MMP
a. Based on the substrate specificity MMPs are classified into the following types [6].
b. Collagenases -MMP-1, MMP-8, MMP-13
c. Gelatinases- MMP-2, MMP-9
d. Stromelysins- MMP-3, MMP-10,MMP-11,MMP-12
e. Matrilysins- MMP-7, MMP-26
f. MT-MMPs (Membrane type) -MMP-14, MMP-15, MMP-16, MMP-17, MMP-24
g. Other MMPs- MMP-18,MMP-19,MMP-20, MMP-21,MMP- 23,MMP-27,MMP-28
Domain Structure Of MMP
MMPs are structurally similar but differ in substrate specificity. T he following features are seen in the structure [7]:
a. Signal peptide
b. Propeptide
c. Furin-cleavage site insert
d. Catalytic domain
e. Fibronectin-like repeats
f. Hinge region
g. Hemopexin domain
h. Membrane insertion extension
Modes of Action
Modes of action of MMPs are as follows [8]:
a. MMPs may affect cell migration by changing the cells from an adhesive to non adhesive phenotype and by degrading the ECM.
b. MMPs may alter ECM microenvironment leading to cell proliferation, apoptosis, or morphogenesis.
c. MMPs may modulate the activity of biologically active molecules such as growth factors or growth factor receptors by cleaving them or releasing them from the ECM.
d. MMPs may alter the balance of protease activity by cleaving the enzymes or their inhibitors.
Regulation of MMP Activity
The activity of MMP against extracellular matrix substrates is regulated at 4 “gates” [9]:
I. Transcriptional regulation of MMP genes
II. Precursor activation
III. Differences in substrate specificity
IV. MMP inhibitors.
Role of MMP in periodontal diseases
In periodontal diseases, MMPs play key role in the degradation of the ECM, basement membrane and protective serpins as well as in the modification of cytokine action and activation of osteoclasts. Organisms like Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans do produce collagenases for the breakdown of ECM but they do not help much in periodontal collagen degradation. One way to differentiate between mammalian and bacterial collagenases is by their different mode of collagenolysismammalian collagenase cleaves the undenatured triple helical collagen molecule at a single site resulting in characteristic 3/4 and 1/4 fragments, whereas bacterial collagenase attacks the collagen substrate at multiple sites resulting in more than 200 peptide fragments. The extracellular matrix not only consists of collagen fibrils but also their associated proteoglycans and fibronectin which must be removed first in order for the collagenase to have access to the collagen substrate. MMP-3 (stromelysin) is effective at degrading proteoglycans and fibronectin [10].
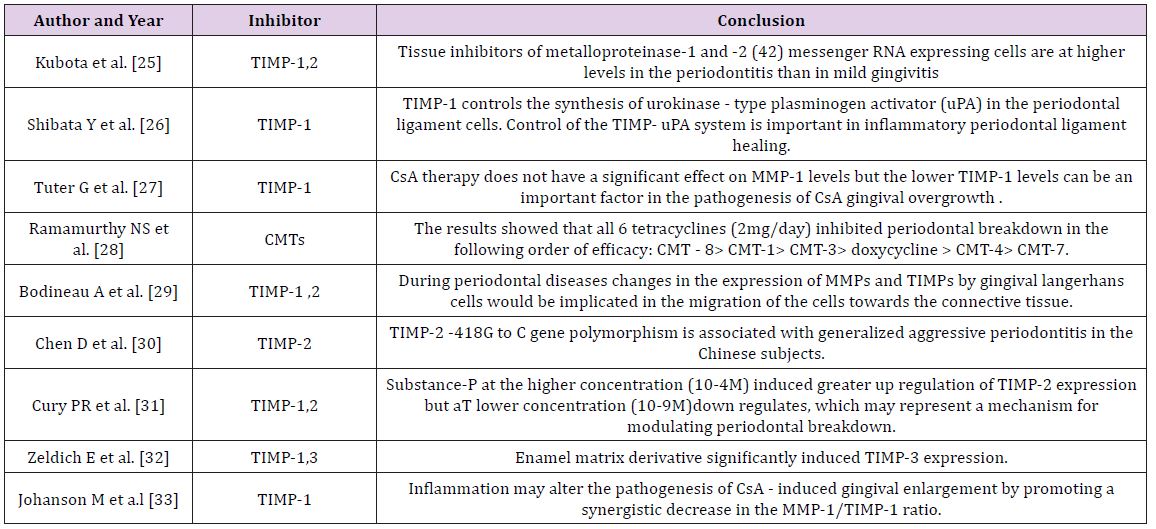
Both resident gingival and periodontal ligament fibroblasts produce collagenases that are thought to be involved in normal tissue turnover. Inflammatory cells such as neutrophils and macrophages are also responsible for production of MMPs with neutrophils being the major source of collagenase and gelatinase in inflammatory diseases such as periodontitis [11,12]. Epithelial cells can also produce elevated levels of these enzymes, which may facilitate the apical migration and lateral extension of the junctional epithelium and the subsequent loss of connective tissue attachment [13]. The evidence for the role of MMPs in periodontal destruction is strong and has been supported over many years by a number of studies; few of them are quoted in the Table 1.
Table 1: Studies related to MMPs.
Estimation of MMPs in Periodontal Disease
Matrix metalloproteinases can also process various bioactive non matrix substrates, such as cytokines, chemokines, growth factors and immune mediators, thereby mediating both anti and pro-inflammatory processes. Therefore, the levels of matrix metalloproteinases should not be interpreted solely as surrogate markers of tissue destruction but also as part of physiological or anti-inflammatory defense [21]. Based on these biochemical or immunological findings, the oral fluids have been a target for extensive research on diagnostic utilization of MMPs and their regulators as potential candidates in chair-side tests for monitoring periodontal and peri-implant diseases [21]. Samples collected to estimate the levels of different MMPs include- Saliva, GCF, and Tissue sample. Various proteomic techniques are being used to estimate the levels of these MMPs which are listed in Table 2.
Table 2: Proteomics techniques.
Role of MMP Inhibitors in Periodontal Disease
A disturbed balance between MMPs and TIMPs might contribute to the disease process in degenerative diseases. Similar patterns of MMP and TIMP expression can be found in different diseases involving matrix degradation. In some cases, the occurrence of MMPs and TIMPs in body fluids such as saliva, gingival crevicular fluid (GCF), or serum provides additional information about the progression of the disease. In healthy periodontal tissue, TIMP levels are generally higher than in inflamed periodontal tissue, in which MMP levels exceed TIMP levels. The more severe the inflammation, the higher the concentrations of active MMPs. In GCF and in gingiva from humans, MMP-1, -2, -3, and -9 are significantly increased, whereas TIMP-1 and -2 are significantly decreased. The inhibition of MMP expression or activity, or increased TIMP expression, might reduce tissue destruction in periodontitis.
Different inhibitors include [22]:
a. Alpha 2- macroglobulins
b. Tissue inhibitors of metalloproteinases
c. Inhibiting antibodies
d. Synthetic inhibitors
Endogenous or natural inhibitors such as tissue inhibitors of matrix metalloproteinases and Alpha 2-macroglobulin bind in a non-covalent fashion to members of the matrix metalloproteinase family. TIMPS probably control matrix metalloproteinase activities pericellularly, whereas Alpha 2-macroglobulin functions as a regulator in body fluids. During inflammation, however, the latter high-molecular-weight protein may escape the vasculature and also function in the extracellular matrix [10]. Multiple synthetic peptides have been formulated in an attempt to synthesize more specific chelators including phosphorus containing peptides, sulfur-based inhibitors and peptidyl hydroxamic acid derivatives.
The most widely used synthetic peptides, and the ones receiving the most attention as potential pharmaceutical agents, are the hydroxamic acid derivative. Synthetic Inhibitors of MMPs fall into three pharmacologic categories [23]:
a. Collagen peptidomimetics and non peptidomimetics, Peptidomimetic MMP Inhibitors- Batimastat, Marimastat Nonpeptidic MMP Inhibitors – BAY 12–9566, AG3340, BMS- 275291, CGS-27023A
b. Tetracycline derivatives- Doxycycline, Col-3 (metastat)
c. Bisphosphonates (Figure 1).
Figure 1: Action of various inhibitors at different levels [24].
Various studies have been done to evaluate the effect of TIMPs on periodontium. Few of them are listed in Tables 3 & 4.
Table 3: Studies Pertaining to MMPs inhibitors.
Table 4: Various MMPs and their inhibitors.
Conclusion
There is much evidence for the role of matrix metalloproteinases in the destructive processes of periodontal disease distinguishing them as a viable target for a chemotherapeutic approach. The use of a host modulatory agent such as a matrix metalloproteinase inhibitor can assist with conventional treatment for periodontitis and, when used adjunctively, can enhance and make clinical therapeutic responses more predictable in the more susceptible patient.
Neonatal jaundice is a common condition that pediatricians encounter in their practice. It is also a significant cause of neonatal morbidity world-wide and is estimated to be present in 60% of term neonates and 80% of preterm babies. Interventions to prevent progression of neonatal jaundice significantly reduce the morbidity and mortality rate of neonate [1]. Elevated serum bilirubin can damage neurons and for this reason it is measured in the neonate with obvious jaundice or signs of underlying disease [1]. Data derived from risk instruments that incorporate several factors, support the potential multifactorial etiopathogenesis of marked hyperbilirubinemia; albeit genetic contributors may go undetected and individual factors confer different degrees of risk.
Methodology
A descriptive study was conducted to assess the risk factors of neonates with hyperbilirubinemia at Sree Gokulam Medical College Hospital, Trivandrum. Using consecutive sampling technique quantitative data was collected from 110 neonates diagnosed with hyperbilirubinemia and undergone phototherapy in Neonatal units and OBG wards. Pretested and validated questionnaire and checklist was used to collect the data. Permission was obtained from institutional research committee and institutional authority. Collected data were analyzed using SPSS-18; descriptive analysis was done to know the empirical information on neonates with hyperbilirubinemia.
Results and Discussion
More than half (53.6%) of the neonates received phototherapy were males, majority of the neonates (79.10%) were classified as term according to gestational age, (81.8%) were classified as normal birth weight, (83.6%) were classified as appropriate for gestational age. More than one fourth of the neonates (31.8%) had ABO incompatibility, 9.1% had Rh incompatibility and 4.5% had both Rh incompatibility and ABO incompatibility. Nearly quarter of the neonates (21.80%) had cord bilirubin level > 2.5 mg %. 9.1% of neonates had hypoglycemia as postnatal complication. More than quarter of the neonates had caput succedenum (25.5%), (39.1%) developed yellowish discoloration (physiological jaundice) on third (49 to 72 hours) postnatal day. A large majority of the neonates (80.9%) received phototherapy for < 24 hours and nearly half of the neonates (44.5%) were in high risk zone as per nomogram designation of risk zone category for receiving phototherapy procedure. more than half of the neonates (68.2%) received direct breast feeding after birth. More than three fourth of the neonates (76%) received demand breast feeding before diagnosing hyperbilirubinemia. There was a progressive declination of bilirubin level to normal range after initiating phototherapy from day 0 to day 2.
Regarding the maternal variables of neonates with hyperbilirubinemia, it was found that nearly three fourth of the neonates mothers (66.4%) were primi. More than half (59.5%) of the multi parity mothers mentioned that their previous child had history of receiving phototherapy. Nearly one fourth of the mothers (14.5%) had GDM (gestational diabetes mellitus). Singh M has stated that gestational diabetes mellitus is a maternal risk factor for the neonate to develop jaundice [1]. More than half of the mothers (60.9%) received oxytocin derivatives during intranatal period. This finding is consistent with study findings by [2]. That the mean total and direct bilirubin levels were higher in neonates delivered using oxytocin (0.4 ± 0.1 and 17.99 ± 0.4, respectively), compared to those without oxytocin induction (0.383 ± 0.1 and 16.2 ± 0.28, respectively) (p = 0.001). More than half of the mothers (66.4%) had normal vaginal delivery. The present study finding is consistent with findings by [2], that the mean total bilirubin level was significantly higher in newborns delivered per vaginally (17.3 ± 3.5 mg/dl), compared to cases born by cesarean section (16.1 ± 3.9 mg/dl) (p = 0.02) [2].
Conclusion
The study has identified various risk factors and variables related to mother and neonates with hyperbilirubinemia. Detection of risk factors by the neonatal health team early in the mother and neonate can protect and prevent the neonate from mortality of hyperbilirubinemia.
Opportunities for the Bioeconomy of Olive Oil Byproducts
Introduction
Bioeconomy is defined as the use of biological sciences for improving adding value to the economic activity (products and services). Bioeconomy refers to the set of economic activities relating to the invention, development, production and use of biological products and processes Oborne [1]. These benefits are expected to improve health outcomes, boost the productivity of agriculture and industrial processes, and enhance environmental sustainability. It is well known that a reduction in dietary saturated fat has generally been thought to improve cardiovascular health. Dietary and policy recommendations frequently focus on reducing saturated fatty acid consumption for improving cardiometabolic health. Milk and dairy foods contain saturated fats, and their consumption often leads to a rise in plasma cholesterol level. Metaanalyses suggest a reduction in risk in the subjects with the highest dairy consumption relative to those with the lowest intake Elwood & Pickering [2].
There is a growing interest in improving fatty acids prole of milk fat by including appropriate fat sources in dairy ruminant diets. The aim is to reduce the content of medium chain saturated fatty acids (FA), which have a hypercholesterolemia effect, and increase the fatty acids considered beneficial, such as polyunsaturated FA of the n-3 series and rumenic acid (cis-9,trans-11 18:2) in milk fat Lock & Bauman [3]; Martínez Marín, Gómez-Cortés et al. [4]. The source for these polyunsaturated FA acids has been suggested to be oilseeds (sugarbeet, lineseed) and their oils. Furthermore, low quality olive oil has been also used as a source of polyunsaturated FA Castro, Cabezas et al. [5]. Intensive dairy goat, sheep and cow milk production in the Mediterranean basin is based on imported conventional ingredients to be included in concentrates. There is an opportunity for applying the principles of circular economy and bioeconomy to produce milk with lower contain saturated fat by using byproducts of olive oil chain to replace conventional ingredients with the double effect of both reducing feed cost and improving milk quality (and dairy products) relative to human health.
Use of olive oil by-products as animal feedstock
Olive cultivation is widespread in the Mediterranean regions and the olive tree spread beyond the Mediterranean (e.g. Australia, Argentina, United States of America, etc.). Feeding by-products to livestock is a practice as old as the domestication of animals. Olive byproducts have been used for Mediterranean small ruminants (goat and sheep) and also for dairy cows. Also for non-ruminant olive byproducts have been also been used. By-products derived from the olive trees and olive oil extractions are: Olive leaves (OL) that is to a mixture of leaves and small branches from both, the pruning of olive trees as well as the harvesting and cleaning of olives prior to oil extraction from olives. Olive cake (OC) consists of olive pulp, skin, stone and water although the specific characteristics of OC may differ according type of oil extraction and before and fresh or dry.
Olive stones (OS) may be a single by-product when they are well separated from pulp either before or after oil extraction. Finally, olive cake ash (OCA) that is the ashes resulting after OC is used as feedstock in biomass energy plant. Additionally, some experiences has been done using low quality oil or calcium soaps of olive oil fatty acids (CSFA). The most frequent used byproduct is the olive pomace (OP) that is one of two major by-products of the olive oil extraction industry, for every 100 kg of olives, 40 kg of OP (highly variable depending on technology). Cost reduction is a consequence of the substitution of concentrate feed with a price around 200 EUR/ton for olive byproduct with a cost of 12 EUR/t. The result of this substitution within the recommended limits achieve a 10% reduction in the cost of goat milk without affecting the yield, Molina-Alcaide, Morales-García et al. [6].
Effects of Olive Oil by-Products as Feedstock in Animal Products
Nasopoulou and Zabetakis [7] review the use of OP as an alternative dietary lipid source in compounded fish feeds resulting in the formulation of functional fish feeds and aquacultured fish according to the EU legislation (EC 1924/2006). The evidence shows an improvement of meat product with OP improve the cardioprotective properties of the final produce (fish farms) by enriching the fish lipid profile with specific cardioprotective lipid compounds of plant origin Sioriki, Smith et al. [8], Parrillo et al. [9], Nasopoulou & Zabetakis [7] also quote the use of OP as a feedstock for animal (terrestrial) feed, with some recent research in pigs Martins et al. [10] demonstrating that oleic acid supplementation have complementary effects and influence the nutritional quality of pork and DSF. Regarding ruminants, olive leaves are fibrous with a low digestibility, especially of crude protein, and they promote very poor rumen fermentation. It has also been observed that for lactating animal’s olive leaves result in an improvement in milk fat quality compared to diets based on conventional forages Molina- Alcaide & Yáñez-Ruiz [11].
The knowledge regarding the use of OC is also in line with the evidence of OL, and a significant number of authors have published the evidence. Goat milk shows a significant change in milk composition with increase, with a common result showing that contents of milk fat and milk total solids, as well as their yields, increased in the OC die with a reduction on less saturated fatty acids (FA) and more monounsaturated FA than the control, Castro et al. [5], Gomes et al. [12] and Molina-Alcaide et al. [11]. The mentioned authors agree with the conclusion that the addition of moderate amounts of oil byproducts to the diets of dairy goats has favorable effects on milk fatty acid composition from the point of view of the human consumer, without negative effects on animal performance.
Additionally, research with lactating ewes has been focused in the use of calcium soaps of fatty acids (CSFA) with different original oil (sunflower, soya and olive oil). Results with lactating ewes are also are consistent with the findings for milk goat, with Casals et al. [13], Gargouri et al. [14]; Titi & Obeidat [15]. Regarding the milk fat contain of cows according the literature review points out that a milk fat reduction is more likely when non-protected fat sources are included in diets based on corn silage but the reduction decreases with other forages Martínez Marín et al. [4], the research in milk cows is less numerous than the evidence for small ruminants (goat and sheep) with OC and other byproducts has not been frequent probably because the high productivity of milk cows and she sensitivity to changes in diet, although some positive experiences have been found with the addition of limited volumes of OL, OC and CSA.
Conclusions and Proposal For Further Research
This short note has presented the knowledge regarding use of olive oil byproducts, as low cost source for improving fatty acids contain of milk fat by including appropriate fat sources in dairy ruminant diets and therefore to reduce the content of medium chain saturated fatty acids (FA), which have a hypercholesterolemia effect, and increase the fatty acids considered beneficial, such as polyunsaturated FA. There is an opportunity to reduce the cost of dairy feed, and improve health contain of dairy products and additionally increase the value of olive oil byproducts that are currently either an environmental problem, or used as a feedstock for composting or direct field application or in the best of the cases as a fuel for biomass to energy plants. According to the principles of bioeconomy European Commission [16], the use as fertilizer or energy is the less valued alternative with animal feed or human food as prefer end destination of agricultural biomass. The use of these alternative low cost byproducts is done by some farmers without proper control and with ad-hoc formulations and methodology to be converted in a new industry that get higher value for olive byproducts, thus enhancing rural areas and simultaneously improving the quality of dairy products. Additionally, research should be done in the analysis of dairy processed products (cheese, yogurts, etc.) in order to test the quality not only from the cardiovascular point of view but also from flavor and other market qualities.
Oral Submucous Fibrosis: the Soft Tissue Marble of Asia
Introduction
Oral squamous cell carcinoma is the sixth most common malignant neoplasm worldwide. Each year it accounts for more than 300,000 cases worldwide. The 5-year survival rate for OSCC has remained at approximately 50% for the past several decades [1]. The impact of oral cancer is such that the disease and its treatment bring a heavy financial burden to both the social resources and the patient’s family with psychological stress affecting the quality of life [2]. It develops through a multistep process of genetic, epigenetic and metabolic changes resulting from exposure to carcinogens, with initially the presence of a precursor/pre-cancer such as oral leukoplakia, oral erythroplakia oral submucous fibrosis. The most frequently reported etiological agents being tobacco, alcohol, chewing of betel quid containing areca nut [3]. The global incidence of oral submucous fibrosis is estimated at 2.5 million individuals. It is one of the most predominant potentially malignant conditions in South Asia with a high rate of prevalence in India, but is now also being acknowledged in Europe and North America [4-6]. The prevalence in Indian populations is 5% for women and 2% for men, which is reflected by the fact that the habit is more common among women in some geographic areas [7].
Aetiopathogenesis
Oral submucous fibrosis (OSMF) is a chronic inflammatory disease of the oral soft tissues with progressive juxta-epithelial fibrosis resulting in increasing difficulty in chewing, swallowing, speaking and mouth opening, often associated with burning sensation inside oral cavity that is aggravated on exposure to spicy food [8]. The habit of chewing betel nut (Areca catechu) is considered to be the main etiological agent, with others factors being genetic predisposition, infections and viral agents, carcinogens, nutritional and immunologic factors [8]. The role of chilliin the pathogenesis of OSMF remains controversial and is postulated as an hypersensitivity reaction to capsaicin due to allergen induced eosinophilia [6]. The mixture of areca nut and tobacco has led to a sharp increase in the frequency of OSMF [5]. A relationship has been observed between the areca quid consumption and development of OSMF.
Areca nut (Figure 1) contains alkaloids notably arecoline and guavacoline, with a wide range of parasympatheticomimetic effects, which modulate matrix metalloproteinases, lysyl oxidases and collagenases, which affect the collagen metabolism leading to fibrosis [7]. Concomitantly, a decrease in the water-retaining proteoglycans will occur which favors an increase in type I collagen production and the flavonoids catechin and tannin in the betel nut stabilizes the collagen fibers and makes them resistant to degradation by collagenase [6]. Genetically, polymorphism of the gene coding for tumor necrosis factor α (TNF-α) leads to stimulation of fibroblasts and aberrations of other cytokines which include transforming growth factor β and interferon-γ, lead to increased production and decreased degradation of collagen. Concomitant to tobacco chewing, smoking and consumption of alcohol increases the risk of oropharyngeal malignancies. 7% to 13% lesions of OSMF can transform into oral cancer, especially squamous-cell carcinoma over a period of 10 years [6-8].
Figure 1:
Clinical Features
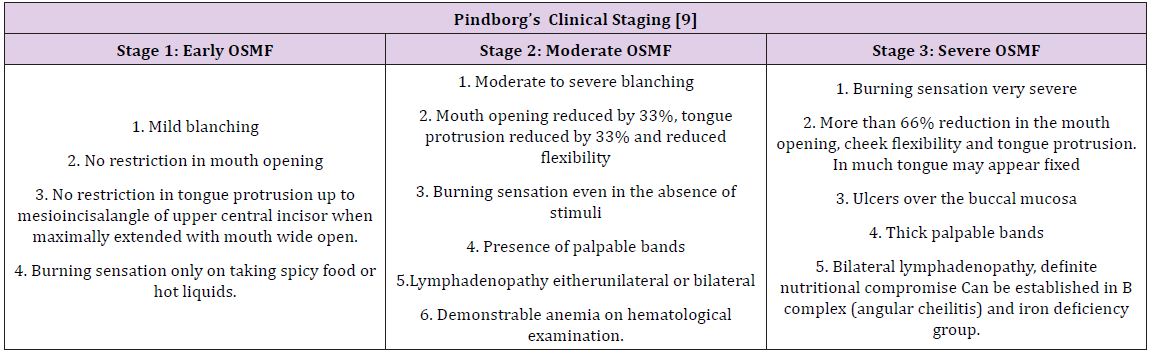
The buccal mucosa and retromolar area are the primary sites affected, followed by soft palate, palatal fauces, uvula, tongue and labial mucosa [6]. It occurs in the age group of 12–62 years with the mean age being 40 years. A definite female predilection, with the male: female ratio being 3:2 [6]. A difficulty in opening mouth accompanied with burning sensation is usually the reason for the patient’s initial visit. On examination, blanching of the oral mucosa is noted which imparts a marble-like appearance, attributed to inflammation, trailed by hypovascularity and fibrosis that may be associated with small vesicles and mucosal erosions [8]. As the disease progresses, there may be stiffness of the tongue, blanched and leathery floor of the mouth, fibrotic, depigmentation of gingiva, rubbery soft palate with decreased mobility and blanched and atrophic tonsils, and shrunken bud like uvula with impairment of activities such as eating, whistling, blowing, sucking [6]. Other symptoms are increased salivation, change of gustatory sensation, hearing loss due to stenosis of the Eustachian tubes, dryness of the mouth, nasal tonality to the voice anddysphagia to solids. Pindborg has classified OSMF into 3 stages as shown in Table 1.
Table 1: Pindborg has classified OSMF into 3 stages.
Diagnosis & Investigations
Diagnosis of the disease is mainly by clinical findings and can be confirmed by incisional biopsy. Other investigations include hematological, serological, immunological and biochemical factors which may reflect findings such as a raised ESR, slight eosinophilia, microcytosis and hyperchromic indicative of anemia. The differential diagnosis includes anemia and scleroderma which can be distinguished by other cutaneous, systemic and characteristic radiographic and laboratory findings [6].
Management
Management of OSMF includes use of hyaluronidase and corticosteroids or a combination of both. Other treatment modalities include antioxidants, Immunomodulators, Physiotherapy, Intereferon -γ, Hyper Baric Oxygen (HBO) therapy, Curcumin, Oxitard, Aloevera, Surgery [6,8,10]. Even though it is easy to diagnose but the irreversible condition reflects the failure of the present treatment modalities. The lack of knowledge and the delay in seeking treatment leads to the progression of the disease. Hence, more focus should be emphasized in detecting newer treatment modalities which is the need of the hour and the future.
Asperger syndrome is an autism spectrum disorder that is on the high functioning end of the autism spectrum it is also referred as “dash of autism”. Incidence is more in males as compared to females. It is important to note the characteristics of Asperger syndrome which can range from mild to severe [1].
a. Definition: Asperger syndrome (AS), also known as Asperger’s, is a developmental disorder characterized by significant difficulties in social interaction and nonverbal communication, along with restricted and repetitive patterns of behaviour and interests [2].
Cause
Cause of Asperger syndrome is not yet identified, although an inherited (genetic) component is believed to be involved. In special cases it may caused by pregnancy infections use of teratogens, and exposure to toxics [3].
Symptoms
Some of the symptoms that may be present are [4]:
a. Less social active;
b. Less friends;
c. Not interested in making friends;
d. Inability to express emotions;
e. No Eye contact;
f. Less facial expressions;
g. Inability to use gestures;
h. Ineffective communication;
i. Lack of relation;
j. Sensitive to external stimuli;
k. Dependent ; and
l. Repetitive actions like arm waving.
How it is Different from Classic Autism?
a. Asperger syndrome is in many ways a milder form of classic autism.
b. Whereas those with autism do not create to have relationships, children with Asperger syndrome attempts to have interaction with others, though they may have difficulty understanding conventional social rules.
c. Asperger syndrome does not usually affect language and communication skills as classic autism [5].
Diagnosis
A diagnosis is the formal identification of the condition, usually by a multi-disciplinary diagnostic team, often including a speech and language therapist, paediatrician, psychiatrist and/or psychologist [6].
Treatment
Treatments can include [7]:
a. Social skills training: In groups or one-on-one sessions, therapists teach child how to interact with others and express in appropriate ways. Social skills are learned through training.
b. Speech-language therapy: This helps in developing communication skills. This therapy provides training regarding two-way conversation and social cues like hand gestures and eye contact.
c. Cognitive behavioural therapy (CBT): It helps your child change his way of thinking, so he can better control his emotions and repetitive behaviours.
d. Parent education and training: You’ll learn many of the same techniques your child is taught so you can work on social skills with him at home. Some families also see a counsellor to help them deal with the challenges of living with someone with Asperger’s.
e. Support Group: A forum for counselling and sharing experiences among people with a similar condition or goal, such as depression or weight loss.
f. Anger management: Practicing mindfulness, coping mechanisms and trigger avoidance to minimise destructive emotional outbursts.
Conclusion
It is an autism spectrum disorder People with Asperger syndrome are of average or above average intelligence. They do not usually have the learning disabilities that many autistic people have, but they may have specific learning difficulties, Identification of the condition, usually done by a multi-disciplinary diagnostic team and treated by using therapeutic modalities.
Antimicrobial Peptides: A Wide Range of Novel Compounds and Their Role as Plant Defense Peptides
Introduction
Despite their sedentary lifestyle plants share some common aspects in their defense mechanisms against pathogens. These features are small peptides that have antimicrobial properties which is part of more ancient and widespread defense strategy in all organisms. These are a product of single gene that can be synthesized in a swift and flexible way, due to their small size they can be produced by host with minimal input of energy and biomass. Well known examples of antimicrobial peptides are cecropins that accumulate in the hemolymph of many invertebrates in response to injury or infection [1] and other example are magainins that are secreted by glands in the skin of amphibians [2].
Plant Defence Peptides
Antimicrobial peptides have long considered playing a key role in plant defense, both as a part of pre-existing, developmentally regulated defense barriers and as part of defense responses that occur upon infection. The antimicrobial peptides in animals may be linear or more complex globular structures in which antiparallel β- sheet are stabilized by disulphide bonds. But in plants only disulphide bonded peptides of second type have been identified till now [3]. The first antibacterial peptide isolated from a plant species was a purothionin from wheat flour (Triticum aestivum), which has the ability to inhibit the growth of some phytopathogens such as Pseudomonas solanacearum, Xanthomonas campestris and Cornybacterium michiganense [4]. Almost 40 years later, several additional peptides with antibacterial activity have been characterized, represented not only by thionins, now named defensins, but also by other groups of proteins such as cyclotides, glycine- rich proteins, snakins, 2S albumins and hevein-type proteins [5]. Peptides isolated from roots, seeds, flower, stem and leaves have shown activities towards pytopathogens as well as against bacteria pathogenic to humans. Over the last decade, antimicrobial peptides have become an interesting tool for the development of techniques in the control of crop loses and in the production of novel antibiotics for the treatment of various human infections [6,7].
Conclusion
Antibacterial peptides have described in a variety of plant species. They belong to a vast range of protein families. Some peptides show specificity towards gram-positive or gram – negative bacteria, but most of them are able to inhibit the activity of both. The study of their mechanism of action shows that these antibacterial peptides are involved in strong interaction with phospholipids from pathogen’s membrane. Parameters such as a molecular volume, aggregation ability and auto assembly on the membrane surface are critical for activity against bacteria. Although, the mode of action of these antibacterial peptides is well characterized, investigations on the importance of specific amino acid residues and their binding with the bacterial cell wall are still in progress.
Acknowledgement
The author is grateful to Dr. (Mrs.) Sushma Ahlawat, Assistant professor, Sam Higginbottom University of Agriculture, Technology & Sciences (SHUATS), Allahabad, India, for her kind support towards this study.
Assessment of Magnitude and Associated Factors of Adverse Birth Outcomes among Deliveries at Suhul Hospital Shire, Tigray, Ethiopia From September, 2015 to February, 2016
Introduction
Adverse birth outcomes such as prematurity, low birth weight and birth defects- represent significant problems in both developing and developed countries. Each year, about 15 million babies in the world, more than one in 10 births, are born too prematurely. More than one million of those babies die shortly after birth; countless others suffer from lifelong physical, neurological, or educational disabilities, often at great cost to families and societies [1]. Globally, an estimated 13 million babies are born before 37 completed weeks of gestation annually. Rates are generally highest in low and middle income countries and increasing in some middle and high-income countries. Complications of preterm birth are the leading direct causes of neonatal mortality and account for an estimated 27% of neonatal deaths. This comes to almost four million neonatal deaths every year [2]. From a global standpoint, the prevalence rate of preterm birth varies from 47.5 to 137 per 1000 live births. Grand multiparty, a previous history of preterm birth or abortion, younger maternal age, inadequacy of prenatal care, reported hypertension, ante partum hemorrhage, premature rupture of fetal membranes and induced labor are significant determinants of preterm birth [3,4].
Worldwide stillbirth rate has declined by 14%, from 22.1 stillbirths per 1000 births in 1995 to 18.9 stillbirths per 1000 births in 2009. But in the African region, there was only an annual decline of less than 1%. The stillbirth rate for developed countries is estimated between 4.2 and 6.8 per 1000 births, whereas for the developing world, the estimate ranges from 20 to 32 per 1000 births. Two thirds of all stillbirths occur in just two regions: South- East Asia and Africa [5,6]. In sub-Saharan Africa, an estimated 900,000 babies die as stillbirths. It is estimated that babies who die before the onset of labor, or ante partum stillbirths, account for two-thirds of all stillbirths in countries where the mortality rate is greater than 22 per 1,000 births [7]. From previous studies, preterm birth, increasing maternal age, history of stillbirth, reported hypertension, extremes of neonatal birth weight, cesarean delivery, operative vaginal delivery, and assisted breech delivery were all significantly associated with still birth [8]. According to Ethiopian Demographic and Health Survey in 2011, In Ethiopia, high rate of neonatal mortality (37 deaths per 1,000 live births)is reported and preterm birth is believe to be a major and direct cause of neonatal mortality [9]. In Ethiopia, adverse outcome of pregnancy are still major public health problems [10,11].
Adverse birth outcomes are the most important vital statistics used to assess maternal and child health program. They are indicator of the quality of antenatal care, medical services and general health services to the mother and the children [12]. Epidemiological data on the magnitude and risk factors of adverse birth outcomes are important for planning maternal and child health care services in developing countries. Most of the newborns who are admitted in neonatal wards are secondary to preterm birth and low birth weight. Most of them are also complicated with various health problems after they have been admitted with a diagnosis of either low birth weight or preterm birth. Mothers are also feeling unhappiness and become unsatisfactory after having a still birth [13]. Hence, this study aimed to determine magnitude and associated factors of adverse birth outcomes of pregnancy at a Suhul Hospital Tigray Ethiopia. The result of this study will serves as a baseline for other wide studies as well as for planning health intervention to improve the wellbeing of children and women [14-19].
Conceptual Frame Work
This frame work was developed by the principal investigator by reviewing different literatures and books (Figure 1).
Figure 1: Conceptual frame work of adverse birth outcomes and associated factors at suhul hospital from September, 2015 to February 2016.
Subjects and Methods
This was a cross sectional study conducted at Shire (Suhul) Hospital. Shire city is located in western zone of Tigray with an area of 30.0316km2 and total population of 47,284. It is 1100KM km far from the capital city of Ethiopia, Addis Ababa and 283km from Mekelle, which is a capital city of Tigray. The study was conducted between June 15 -July 15, 2016. The study population was sampled term new born babies delivered at Adwa General Hospital for the period July 1, 2014 to June 30, 2016. Individual term new born babies reviewed from mother’s chart or cards.
Source Population: were all mothers who gave birth at Suhul hospital from September, 2015 to February, 2016.
Study Population: selected cards of those mothers who gave birth at Suhul hospital from September, 2015 to February, 2016.
Study Unit: Maternal cards with adverse birth outcomes and normal birth out come.
Inclusion Criteria: All maternal cards with adverse birth outcomes and normal birth outcomes with no missing the most important information (detail records on demographic characteristics, current obstetric history, medical history and past obstetric history and delivery summary) were included.
Exclusion Criteria: maternal cards with birth outcomes of congenital anomaly.
Sampling and Sample Size Determination: The sample size was determined by using single proportion for finite population with 95% confidence interval, marginal error (d) of 4 %.
n=(z2 p(1-p))/d2
n= Sample size
z= the standard score (critical value) corresponding to 95% confidence level = 1.96.
d= the proportion of sampling error between the sample and the population = 4% (0.04).
p= prevalence
Calculation of the sample size was based on the Gondar’s prevalence which is as follows:
Equation 1:
Simple random sampling technique and card reviewing method was used. In Suhul hospital there were a total of 1590(N) deliveries from September 1, 2015 to February 30, 2016. The sample size was 425 (n). After identifying the number of cards at each month the calculated sample size was distributed to each month of study based on population proportion size and the study subjects were nominated randomly (Figure 2).
Figure 2: Sampling frame work of study participants.
Data Collection Methods: Since the file is kept at record office after discharge, data collection was done using structured checklist from clinical records of mothers’ (registration books and individual cards). Cases was identified from the records office through reviewing every record of women who gave birth at Suhul hospital from September 1, 2015 to February 30, 2016.The checklist was structured into four logical sections (socio demographic characteristics, obstetrics related factors; medical history and birth outcomes assessment). Data were collected by 3BSc midwives after giving 2 days training.
Data Quality Control: Data quality was ensured during collection, coding, entry and analysis. Pre prepared Structured checklist was used. Training was given to the data collectors and supervisors to prevent any confusion and have a common understanding about the study. Each card was checked for its consistency, provision of full information and appropriate documentation. Pretest was conducted on 21 maternal cards (with adverse birth outcome and normal birth outcome) that gave birth before September 2015. Based on the pretest modification on logical sequence, simplicity, and clarity of checklist had been done. Supervision of data collectors included observation of how the data collectors will collect data was done by supervisors. The data collectors were instructed to write cards number on the check list during the data collection so that any identified errors was traced back using the cards number. The filled checklist was checked for completeness by data collectors, supervisors and PI on a daily basis. Consequently, any problem encountered was discussed among the team and solved immediately. The collected data code was given to the completed questionnaire. The data was entered and analyzed using SPSS version 20 statistical package. Data cleaning was performed to check for frequencies, accuracy, and consistencies and missed values and variables. Any error identified was corrected.
Data Analysis: Frequencies, proportion and summary statistics were used to describe the study population in relation to relevant variables. Both Bivariate and multivariate logistic regression analysis was used to determine the association of each independent variable with the dependent variable. Variables significant in Bivariate analysis were entered into a multivariate logistic regression model to adjust the effects of cofounders on the outcome variable. Odds ratio with 95% confidence intervals was computed to identify the presence and strength of association, and statistical significance was declared if p < 0.05.
Study Variables
1. Dependent variable
• Adverse birth outcomes (Still birth, preterm birth and LBW)
2. Independent variables
3. Socio demographic characteristics
• Residence, age, marital status and ethnicity
4. Obstetric history
• Parity, gestational age, onset of labor, duration of labor, pregnancy status, mode of delivery, type of pregnancy, previous poor obstetric history, contraceptive use
Medical illness and other obstetric complications
• Anemia, UTI, Malaria, HIV/AIDS, Hypertension, Ante partum hemorrhage, HIV status, ART status, Hepatitis virus screening.
Operational Definitions
1. Adverse birth outcome: newborns delivered as preterm, low birth weight or still birth
2. Still birth: fetal loss after 28 wks of gestational age and during intra partum period.
Ethical Consideration
Ethical clearance was obtained from Mekelle University College of health science. Purpose of the study was informed for the managers, staff members and health professionals who were working at Suhul hospital.
Dissemination And Utilization Of Results
Results will be disseminated to Mekelle University, Tigray region health bureau and to Suhul hospital where the data had been collected.
Result
The Socio-Demographic Characteristics Of Women Attended Maternity Ward At Suhul Hospital, Shire, Tigray, Ethiopia: A total of 425 cards of mothers were reviewed in the study of which 283 (66.6%) were in the age group of 20-34, followed by 94 (22.2%) greater than 34 years with the mean age of 29 and standard deviation of +7. Majority of the mothers 375 (88.2) were married and more than half of mothers 234(55%) were urban residents. Regarding their ethnicity majority, 378 (88.9) of them were Tigrai followed by 41 (9.6%) were Amhara [20] (Table 1).
Table 1: Socio-demographic characteristics.
The Obstetrics Characteristics Of Women Attended Maternity Ward At Suhul Hospital, Shire, Tigray, Ethiopia: More than half of mothers 246(57.9%) were multipara and 119(28%) of mothers were Primipara. Most of the mothers, 407(95.8%) had history of ANC follow up, almost half of them 201(49.4%) had their first ANC visit during first trimester and 191(46.9%) mothers had at least four visits during current pregnancy. with regard to the status of current pregnancy 325(76.5%) of the pregnancies were wanted and planned. In this study majority of mothers 391(92%) were supplemented with Iron and Folic acid during ANC follow up. Majority of the mothers 392 (92.2%) had taken TT vaccination, of them around one third of the mothers had taken the fifth dose of TT vaccination. Regarding the type of pregnancy in this study 401(94.3%) of the pregnancy were singleton. The mean duration of labor was 13 hours with standard deviation of +4. More than three fourth of 350(82.4%) onset labor were spontaneous and majority of mothers 322(75.8%) were delivered by SVD. Two third of mothers had used contraceptives prior this pregnancy, of them 204(72.1%) had taken inject able (Table 2).
Table 2: Obstetrics characteristics.
The Medical Illness And Obstetric Complications Among Women Attended Maternity Ward at Shire Suhul Hospital Tigray Ethiopia: Fifty two (12.2%) of the mothers had medical illness, of them 16(38.2%) mothers had urinary tract infections. thirty seven (8.7%) and thirty two (7.5%) of mothers had hypertensive disorders of pregnancy and ante partum hemorrhage respectively. Twenty seven (6.4%) of mothers also had premature rupture of membrane during current pregnancy. More than three-quarter 345(81.2) of mothers were screened for HIV, of them 35(10.1%) were reactive for HIV test and 33(94.3%) of them had started HAART. All study participants were screened for hepatitis viral infection and syphilis, 28(6.6%) and 7(1.6%) of mother had positive results for hepatitis and syphilis respectively (Table 3).
Table 3: Medical illness and obstetric complications.
The ABO Among Women Attended Maternity Ward at Shire Suhul Hospital Tigray Ethiopia: The study finding showed that the prevalence of ABO among the study participant was 96(22.6%). Seven (14.3%) of low birth neonates and six (16.2%) of preterm births were still birth and 23(47%) of LBW neonates were preterm. almost half of the new born 213(50.1%) were males. The mean weight of newborns was 2.9kg with the standard deviation of + 0.6kg (Figure 3).
Figure 3: Magnitude of preterm birth, LBW and still birth.
Factors Associated With Adverse Birth Outcome Among Women Attended Maternity Ward at Shire Suhul Hospital Tigray Ethiopia: Bi-variate and multivariate logistic regressions were done to assess the predictors of ABO. Onset of labor, residence, hypertensive disorders of pregnancy, ante partum hemorrhage, PROM, previous BOH and type of pregnancy were significant at bi variate logistic labor. Mothers who had HDP were 6 times (AOR=6.368, (95%) CI: 2.880-14.080) more likely odds associated with ABO than mother without HDP. Women who had APH during respective pregnancy were 3 times (AOR=3.087, (95%) CI: 1.172-8.132) more likely odds associated with ABO than women who didn’t face APH. Mothers who had previous history of BOH were 2.3 times (AOR=2.290, (95%) CI 1.165-4.503) more likely odds associated with ABO than mothers who hadn’t bad obstetric history. Multiple pregnancies were 7 times (AOR: 7.230, 95%) CI 2.973-17.580) more likely odds associated with ABO than singleton pregnancy (Table 4).
The finding of this study showed that the magnitude of ABO among deliveries was 96(22.5%) among which the prevalence of still birth was 41(96/1000 births) and the magnitude of preterm birth and low birth weight were 37(8.7%) and 49(11.5) respectively. The prevalence is higher than the WHO estimation [20-22] and regional and worldwide estimation [5] of adverse birth outcomes this variation may be due to the difference that this study was institution based study and which was done in a zonal hospital, so that the magnitude may increase because of increasing number of referral cases from health centers and primary hospitals. The magnitude was also higher than studies done in Tanzania [23], Iran [24], China [25] and Ghana [26]. The variations between the findings may be attributable to the variations in methodological and socio-economic variations, quality of maternal health service and facilities explain differences in adverse birth outcomes in respective study areas.
The findings of this study were lower than from pervious reported studies in Jimma zone [27], Debremarkos [28,29] and Kersa east Ethiopia [30]. This variation may be due to methodological difference that the previous studies were used prospective study but in this study the methodology used was card review, hence it may limit the type and number of adverse birth outcomes. The Figure were also lower than the study findings done in north wello zone [31], this variation is attributable to the previous study was community based study. It were also a little beat lower than the study done in Gondar which showed that the prevalence of adverse birth outcome was 23% with the proportion of 14.3%, 11.2% and 7.1% preterm birth, low birth weight and still birth respectively [32]. This variation may due to methodological difference. Pregnancy induced hypertension one of the risk factors for adverse birth outcome and mother with HDP was 21.6 times more likely to associate with adverse birth outcome than mother without HDP. This finding was in line with other studies done in Iran [24]. Similar finding was also reported from the study done in India [33] which revealed that mothers with PIH were more likely to delivery adverse birth outcome as compared with those women without PIH.
This is again supported by a research done in Tanzania [34], China [25], Gondar [32], and Debremarkos [28]. This might be due to hypertension results in decreased blood flow through the spiral arterioles and decreased delivery of oxygen and nutrients to the placenta and fetus and Hypertension also might be associated with placental infarction. These researchers indicated that hypertensive disorders might play a critical role in the incidence of adverse birth outcome as supported by other studies. Evidence from earlier study showed that reduced placental blood flow leads to decreased fetal growth, with an increased risk of intrauterine growth restriction and low birth weight [29]. In this study Ante-partum hemorrhage during the current pregnancy is significantly associated with adverse birth outcomes this finding was in line with the previous studies in Iran [24], Tanzania [34] and Pakistan [35]. Similar study in Gondar also reported that Ante-partum hemorrhage is significantly associated with adverse birth outcomes, bleeding during pregnancy is one of the etiologies of anemia leading to intrauterine oxygen inadequacy [32].
Furthermore, mothers who had previous history of poor obstetric history were 2.3 times more likely to have adverse birth out comes than mothers who hadn’t bad obstetric history. This Figure was similar with previous study findings in Tanzania [23], Iran [30], China [25], Gondar [32], and north wello zone [31]. This might be due to most poor obstetrics histories are recurrent. Induced on set of labor was also significantly associated with a adverse birth out comes this may be due to different maternal and fetal indications like hypertensive disorders of pregnancy, ante partum hemorrhage, oligohydramnios, premature rupture of membrane etc, in order to prevent maternal and fetal complications. Multiple pregnancies were significantly associated with adverse birth outcomes. Similar studies in jimma zone [27] and Canada [9] also revealed Multiple pregnancies were risk factors for development of adverse birth outcome this might be due to chorionicity, in monochorionic placentation is associated with fetal mortality and morbidity in monochorionic twins the placenta is shared and inter twin vascular anastamoses, which produce various degree of twin to twin transfusion syndrome in 10% to 15% cases. Twin to twin transfusion syndrome causes discordant twin growth and, sometimes intrauterine demise of one twin. It may also result in fetal anemia or it may be related to uterine distension, increased intrauterine volume, or related complications such as cervical incompetence [9].
Conclusion
The magnitude of adverse birth outcome among the study population was higher than WHO estimation. Induced onset of labor, hypertensive disorders of pregnancy, ante partum hemorrhage, previous bad obstetric history and multiple pregnancies were the major predictors of adverse birth outcomes.
Acknowledgment
We would like to express our appreciation to Mekele University and the Department of Midwifery for their invaluable contribution towards the completion of this study. We also thank our friends and colleagues for their critical contributions.