Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
The Effect of Local Anesthesia (Lidocaine 2%) with Epinephrine (1:100,000) On Blood Pressure Level of Hypertensive Patients Reported To a Tertiary Care Hospital, Peshawar, Pakistan
Abstract
Objective: The objective of the study was to evaluate the effect of local anesthesia (Lidocaine) with epinephrine (1:100000) on blood pressure level and medicine used by hypertensive patients having Prehypertension, stage I and stage II hypertension.
Methodology: This randomized controlled trial study was carried out in the department of Oral and Maxillofacial Surgery, Sardar Begum Dental College, Peshawar, Pakistan from February 2016 to August 2016. A total of 88 male and female hypertensive patients were selected and were divide into two groups through lottery method: Group A: Having 28 patients who receive 3 cartridges of Lidocaine 2% with epinephrine (1:100,000).Group B: Having 22 patients who receive 3 cartridges of lidocaine 2% without epinephrine (1:100,000). The blood pressure was measured prior to injection, 5minutes after injection, during extraction and after extraction of the tooth. Aspiration was carried out prior to injecting the local anesthesia. Statistical analysis was performed using SPSS 22. P ≤ 0.05 was considered as significant.
Discussion: No significant increase in SBP and decrease in DBP were seen 5 minutes after injection, during extraction and after extraction of the tooth. The most commonly medicine taken by patients were β-blockers n=42 (47.72%). Pearson correlation revealed that increasing the duration of tooth extraction will decrease SBP (-.204) and DBP (-.106). ANOVA showed that the increase or decrease in SBP and DBP was statistically not significant (P=.698) between intergroup. Chi-square statistics exhibit that hypertension is highly associated with 40-49 years age group (X2=21.286, P=0.000). Regression analysis showed no significant relationship between β-blockers and local anesthesia with epinephrine 1:100,000.
Conclusion: Three cartridges of local anesthesia with epinephrine 1:100,000 have no significant effect on SBP and DBP in pre-hypertensive, stage-I and stage-II patients
Hypertension is the systolic blood pressure (SBP) of ≥ 140mmHg or diastolic blood pressure (DBP) of ≥90mm Hg [1]. More than 90% of causes of hypertension are not clear but there are certain regulatory systems of blood pressure as well as environmental factors which contribute in regulation of blood pressure [2]. Blood pressure is also regulated by cardiac output and heart rate [3]. Over expression of the genes which controlled these regulatory systems may contribute in high blood pressure [4]. Due to high prevalence of hypertension globally, it is one of the most frequent disease seen in the patients who are visiting the dental hospitals and clinics [5,6]. In Pakistan approximately 33% of adult population suffers from hypertension and is the most common amongst cardiovascular diseases [7].
One utmost apprehension of dental treatment for hypertensive patients is the unexpected and marked increase in blood pressure that could lead to life-threatening complications therefore thesepatients contribute a major risk group in the dental treatment [5,8]. Local anesthetics combined with vasoconstrictors are used in most of the dental procedures [9]. Vasoconstrictors in the local anesthesia are added to enhance duration of local anesthesia, to halt systemic toxicity and to assist in hemostasis [10]. The most frequently used local anesthesia in many countries is Lidocaine and it was the first local anesthetic to be marketed in 1948 [5,11]. Epinephrine is the leading vasoconstrictor used in dental practices today [6,9]. Epinephrine acts on both α and β receptors but dominate on β. Acting on α1 epinephrine causing vasoconstriction in the peripheral blood vessels [12] while increase in the heart rate and blood pressure is due to the effect of epinephrine on β1 receptors [13].
There is controversy exists among different studies. Some believe that local anesthesia with epinephrine increases blood pressure as well as heart and should be contraindicated in hypertensive patients [5,11,14,15]. While some studies showed that the use of local anesthesia with epinephrine has no substantial effect on blood pressure and heart rate when one-three dental catridges are used as the amount of epinephrine is very low [16- 18]. Daubländer et al. [19] and Meechan et al. [20] demonstrate that it is obligatory for dental professionals to be cautious in proper use of local anesthesia with vasoconstrictor and care is needed when selecting and administrating these anesthetics to avoid systemic complications. The objective of the study is to evaluate the effect of local anesthesia (Lidocaine) with epinephrine (1:100000) on blood pressure level and medicine used by hypertensive patients having Prehypertension, stage I and stage II hypertension.
Methodology
This randomized controlled trial study was carried out in the department of Oral and Maxillofacial Surgery, Sardar Begum Dental College, Peshawar, Pakistan from February 2016 to August 2016. The ethical approval for this study was taken from the hospital’s ethical committee. A cardiologist was on call during the procedure and emergency equipments were arranged. Relaxed atmosphere was provided for the tooth extraction in these patients. All patients were informed about the aim of the study and a well-documented proforma about demography, hypertensive medications and informed consent was taken prior to the procedure. The procedure was performed under the supervision of the head of the department.
A total of 88 male and female hypertensive patients were selected through non-probability purposive sampling using Kelsey formula for clinical trials with a level of significance α=0.05, power=0.80, prevalence ratio 5.4 and odds ratio 7.The patients were divided into two groups through lottery method:
a) Group A: Having 44 patients who receive 3 cartridges of lidocaine 2% with epinephrine (1:100,000).
b) Group B: Having 44 patients who receive 3 cartridges of lidocaine 2% without epinephrine (1:100,000).
The criterion for the stages of hypertension was set as that of American Heart Association [21]. The age selected was 20-70 years, SBP ≤179 and DBP≤ 110 and those diagnosed ≥ 6months. All those hypertensive patients with other systemic diseases like diabetes mellitus, hepatitis, HIV, immunocompromised, patients undergoing radio or chemotherapy and those who are allergic were excluded from the study. All those were also excluded who were agreed prior to procedure but unwilling to complete it. The blood pressure was measured with a conventional calibrated sphygmomanometer keeping the cuff on the patient’s left arm and in supine position, four times during the whole procedure: Prior to injection, 5minutes after injection, during extraction and after extraction of the tooth. Aspiration was carried out prior to injecting the local anesthesia.
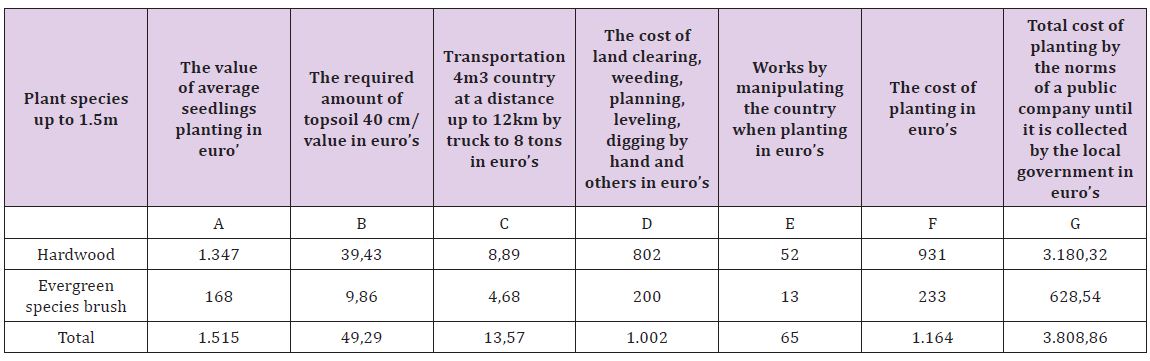
Statistical analysis was performed using SPSS 22. One way ANOVA was used for descriptive statistics and intergroup comparisons. Linear regression analysis was used to show the relationship of medicines with hypertension. Chi-square statistics were used for association of age and hypertension. Pearson correlation was applied for relation of hypertension after tooth extraction with time of extraction. P ≤ 0.05 was considered as significant (Table 1).
Table 1: Stages of Hypertension.
Results
The mean age presented was 39.4 ± 15.8 years. The female to male ratio was 3.88:1. The results of medicines taken byhypertensive patients and age groups involved are shown in Table 2 and Figure 1 respectively. The mean SBP and DBP prior and after tooth extraction is shown in Table 3. The effect of duration of procedure with SBP and DBP prior to local anesthesia with and without epinephrine (1:100,000) injection and after tooth extraction is shown in the Figure 2 and Figure 3 respectively which exhibit that SBP decreases when operator increases the time of tooth extraction while there is no such variation exists in DBP with time. When Pearson correlation was applied it also revealed that the duration of tooth extraction has negative correlation on SBP (-.204) and DBP (-.106). ANOVA when applied for intergroup comparison disclosed that the increase or decrease in SBP and DBP were statistically not significant (P=.698). Chi-square statistics exhibit that hypertension was highly associated with 40-49 years aged group (X2=21.286, P=0.000).
Figure 1: Percentages of hypertensive patients according to the age groups.
Figure 2: SBP and DBP prior to local anesthesia with epinephrine injection and after tooth extraction with time taken to complete the procedure.
Figure 3: SBP and DBP prior to local anesthesia without epinephrine injection and after tooth extraction with time taken to complete the procedure.
Table 2: Different medicines used by hypertensive patients.
Table 3: Mean Systolic blood pressure (SBP) and Diastolic blood pressure (DBP) before and after tooth extraction with P value (≤0.05).
The mean SBP was 147.50±17.29. At a constant level of SBP(140.00) there will be 5.882 increase occurred in after 5 minutes of LA with epinephrine and were statistically significant (P=.04). When the relation of β-blockers and epinephrine was evaluate the increase was same but statistically not significant (P=.737).The mean DBP after 5 minutes of local anesthesia with epinephrine was 89.29±12.07. There was no increase or decrease seen. While in patients using β-blockers, DBP increased by 3.84 and is statistically insignificant (P=.772).
The mean SPB was 143.57±17.15. There will be 5.717 increase occur in SPB with medications and was statistically significant (P=.026). The mean DBP was 90.71±10.86. Medications will not affect DBP (P=.984) during tooth extraction. The mean SBP after tooth extraction was 143.57±17.15. The relationship of medication with hypertension showed that there will be 6.583 increase and is highly significant (P=.009). When β-blockers were related the increase will be 10.58 but statistically not significant (P=.536). The mean DBP was 88.64±12.32. The increase in DBP is statistically not significant for medications (P=.073) as well as for β-blockers (P=.218). Regression analysis also showed that those who are taking medications early morning results in decrease of SBP (-2.22) and DBP (-1.64) but the decrease is not significant (P=.749) and (P=.742) respectively.
Discussion
This study not only focuses on the effect of LA with epinephrine on the blood pressure level of hypertensive patients but also interpret the relationship of medication used by hypertensive patients and especially β-blockers with SBP and DBP. Furthermore, the study described the correlation of duration of tooth extraction with SBP and DBP. The study revealed that the most frequently medicines used by hypertensive patients were β-blockers n=42(47.72%) and the most dominant gender involved was female. The female to male ratio was 3.88:1 showing high prevalence in females. Silvestre et al. [22]. showed that angiotensin II receptor antagonist were the most frequently used medicine by hypertensive patients and prevailed a ratio of 1.9:1 between female and male patients.
The present study noted that there was a decrease occur in DBP of pre-hypertensive, stage-I and stage-II hypertensive patients by 1.90mm Hg while SBP increases in all these patients by 2.54mm Hg. But the increase in SBP and decrease in DBP were statistically insignificant. Chaudhry et al. [23] demonstrate that the mean DBP after extraction decreases after tooth extraction which harmonize with results of the current study while there was significant increase seen in the mean SBP of stage-II hypertensive patients (21mmHg) after extraction which contradict this study. The decrease seen in the mean DBP of the present study matches the results of the study done by Abu-Mustafa et al. [24], Silvestre et al. [22] proclaim no significant changes in SBP and DBP while determining at three time points in those patients who received local anesthesia with vasoconstrictors which support this study. Ogunlewe et al. [25] conducted a study on two groups, one received Lidocaine 2% with epinephrine 1:80,000 while other group received plain Lidocaine 2%. After administration of anesthesia no significant difference was observed between these groups however, a significant difference was seen during tooth extraction in both groups which contradict present study.
The current study revealed that no adverse effect was reported in those patients who were using β-blockers. The changes in the mean SBP and DBP after 5 minutes of anesthesia with epinephrine, during and after extraction were insignificant in these patients however Hersh et al. [26] observed a significant interaction between β-blockers and epinephrine when Lidocaine with epinephrine 1:100,000 was used. This study also found that increasing the tooth extraction time will results in decreasing SBP and DBP. The limitation of this study is its small sample size. Apart from its small sample size the study demonstrate a thorough evaluation of the effect of local anesthesia with vasoconstrictor on the blood pressure level. The effect of duration of tooth extraction, use of 03 cartridges and patients using β-blockers in the sample size are idiosyncratic to this study. However, the results cannot be anticipated for the true estimation within the general population. The future study may be to concentrate the effect of local anesthesia with vasoconstrictor in patients using β-blockers with large sample size.
Conclusion
The findings of present study concluded that use of three cartridges of local anesthesia with epinephrine 1:100,000 have no significant effect on SBP and DBP in pre-hypertensive, stage-I and stage-II patients provided to prevent accidental intravascular injection.
Acknowledgment
We are thankful to Dr.Alam Khan for his assistance who were on call Cardiologist, working in CCU, Khyber Teaching Hospital, Peshawar, Pakistan.
Microspheres for Cosmetic and Medical Injections Must be Free of Phagocytosable Microparticles under 20 Microns
Abstract
A more serious complication after the injection of all dermal fillers is the late occurrence of foreign body granulomas. The reason must be the retention of a foreign material in the memory of the macrophages, which likely had phagocytosed it years before a granuloma manifests itself as reddish-blue, dense nodules. This sudden granulomatous immune reaction is probably triggered by a sudden systemic bacterial infection which can be recalled by one-third of all granuloma patients. A vigorous removal of small PMMA particles < 20 μm in the only FDAapproved permanent injectable wrinkle filler ArteFill® and deep dermal injections, have decreased the granuloma rate from 0.5%, experienced with earlier-generation products of Artecoll® in Europe, to 0.01% (4 in 42,000 patients) in China when injected in the deep dermis.
a) Injectables: When collagen injections for wrinkle correction and lip augmentation became fashionable in the early 1980ies, dermatologists and plastic surgeons quickly realized that they did not last for 2 years beneath facial wrinkles, as promised by the manufacturer, but their positive effects rather vanished within 3 months. In order to prolong the effectiveness of collagen-based dermal fillers, a mixture with highly tissuecompatible and non-biodegradable PMMA-microspheres was suggested and tested in pre-clinical studies at the University of Frankfurt/Main Germany in 1985 [1]. Subsequently, after positive results in a limited number of volunteer patients, European clinical trials were initiated [2] and a new permanent injectable wrinkle filler Artecoll® has been marketed in Europe since 1994 (Figure 1)[3], in Brazil since 2009 [4], and in China since 2002 [5]. In the US, next-generation product ArteFill® received FDA-approval in 2006 as the first and only permanent dermal filler (now Bellafill®) [6].
Figure 1: Artecoll after 10 years: each 40μ-microsphere is still encapsulated by a macrophage. Fibroblasts have produced broad collagen bands, which give the permanent implant a soft rubberlike consistency Ten Year Artecoll GL-NL.
b) Granulomas: Since granulomas have occurred after all dermal filler injections, including collagen and hyaluronic acid, the authors have investigated possible causes for granuloma formation. Foreign body granulomas can occur suddenly in approximately 1:2,000 injected patients months or even years after the injection [7]. They appear suddenly in all injected sites, grow rather rapidly to the size of peas or even beans, and, if untreated, usually remain for a few years untilthey disappear spontaneously [8]. Histologically, granulomas after PMMA-fillers show further than normal separated PMMA microspheres due to an over production of collagen, hyalinization, macrophages engulfing microspheres, and a high number of giant cells. The latter originate from a fusion of up to 40 “frustrated macrophages” that cannot destroy or remove the microspheres (Figure 2). The treatments of choice are repeated intralesional corticosteroid injections (triamcinolone, Kenalog®) in rather high doses [7].
Figure 2: Typical PMMA-granuloma in which the microspheres are pushed apart by massive hyaline secretion. The increase of macrophages and especially foreign body giant cells (dark spots) is obvious PMMAgranuloma with giant cells.
c) Macrophages: All injectable microspheres made from either PMMA (Artecoll®/Bellafill®), calcium-hydroxyapatite (Radiesse®), polylactic acid (Sculptra®), polycaprolactone (Ellanse´®), etc. have an average diameter of 40μm, just small enough to pass through a tiny 26g needle (with an inner diameter of 260μm), yet large enough to escape phagocytosis by macrophages, the cells which clean the inner vertebrate tissues from all foreign materials (Figure 3) [7]. Macrophages have a diameter of 10-20μm and migrate through all connective tissues of the body, phagocytosing cell debris of dead cells, bacteria, and foreign particles, up to a size below their own. The migration of macrophages is facilitated by swelling (postinjection edema), which widens the “openings” between the fibers of the connective tissue from 5μm up to about 20μm. Since the life circle of macrophages is only 2 days before they are indigested by their younger peers, their “memory” on former immune stimulants like bacteria and the surface structure and chemistry of foreign bodies appears to be transferred as well, from one generation of macrophages to the next one (Figure 4) [7].
Figure 3: In a normal PMMA-implant, macrophages (dark blue) expand in order to embrace the 40μm-microspheres. They are stuck in the implant and cannot move away to transport their memory to the immune system Macrophages surround microspheres.
Material and Method
Small Particles
The process of PMMA-microsphere production starts with the injection of hot PMMA-syrup into floating cold water: as faster thewater runs or is stirred, as smaller the microspheres develop from the injected droplets. In a round drum, the small microspheres originate in the periphery, the larger around the center. Unfortunately, after all different production methods are very small microspheres or irregular PMMA-particles contained or attached to the smooth and identical bigger microspheres (Figures 5 & 6). These small particles must be removed by sieving and washing, since they may be the reason for the memory of the macrophages (Figure 4).
Figure 4: The theory of granuloma induction Granuloma theory: a) Macrophages phagocytose b) small particles, c) macrophages forward and keep the memory of particles over years; d) a systemic infection stimulates macrophages; e) macrophages attack bacteria and PMMA-particles at the same time. They cannot destroy particles, fuse to giant cells, and form granulomas.
Figure 5: Small PMMA-particles are only visible under the microscope beneath a water droplet Small particles beneath a droplet of water.
Figure 6: Small particles are attached to 40μm-microspheres Small particles attached to 40μm PMMA.p>
PMMA size specifications
Dermal fillers containing particles with irregular surface (Macroplastique® and Dermalive®) have been prohibited or removed from the market because of a very high rate of foreign body granulomas. Histologically, a huge number of macrophages and especially giant cells-a fusion of “frustrated macrophages”- were attached to the sharp peaks and ridges of these particles made from hard silicone or ground acrylic lenses but were unable to engulf or destroy them. Consequently, many patients had suffered from granulomas after subdermal injections of these two products. This fact led to discussions with the FDA in the early 2000’s when the manufacturer of Arte Fill agreed to implement the suggestion by the FDA to reduce all PMMA microparticles of less than 20microns to below 1% by the number (not volume) in order to minimize the potential of granuloma formation [9].
FDA’s rational, based on the author’s own research on microparticle phagocytosis, transport and dislocation [10] is as follows: larger than 20μm PMMA particles or microspheres cannot be phagocytosed by one smaller macrophage but are encapsulated by at least 3 macrophages and kept in place (Figure 3). They cannot move from the injection site but are stuck in the implant for the rest of the patient´s life. If small particles are phagocytosed, the macrophages can move away along with these particles to lymph nodes, liver, or lung, and deposit their foreign non-destructible content there [10]. Interestingly, if a high number of small microspheres are injected in one bulk, the microspheres will not be phagocytosed but remain as a bulk (Figure7), surrounded by a wall of macrophages, which each had engulfed 50 to 100 small microspheres, and were unable to move away from the injection site, as well. This is the body´s way of render harmless huge numbers of small particles [10].
Figure 7: A bulk of PMMA-microspheres of 4 μm in diameter is not phagocytoses but surrounded by PMMAfilled macrophages and connective tissue, which keeps the bulk in place. Capillaries are invading, however, changing the bulk into a “living tissue” [9] PMMA 46mox400.
Proof of Theory
Our theory is supported by the fact that the rate of granuloma formation has significantly decreased since FDA’s approval of ArteFill® in 2006 (Figure 8), i.e. after the injection of PMMAmicrospheres that meet FDA’s quality standard (Figure 9) [3, 11]. In Brazil, where other PMMA-injectables with a high content of small particles are still marketed and injected in high volumes today, the rate of granulomas has remained relatively high (Figures 10 & 11) [12, 13].
Figure 8: The granuloma rate dropped worldwide after sieving and consequent washing of the 40μm-microspheres . After deep dermal or epiperiosteal injection the rate is 0.01% in China [5] Gran rate.
Figure 9: The analysis in a Coulter-Multisizer 3 reveals 3.84% small particles in a sieved but the not washed PMMA fraction Lerche Analysis 2012 – Copy (2).
Figure 10: A Brazilian PMMA-product of 2012 shows all kinds of PMMA-impurities and small particles [12] Metacrill_700x_9 1.
Figure 11: Brazilian normal PMMA-histology at 3 years shows still a strong foreign body reaction with many giant cells Brazil PMMA 3 years arm.
Conclusion
Product “Safety” must come before effectiveness, especially in personal aesthetics products, such as injectable wrinkle fillers or tissue volumizers. During the past 35 years, many aesthetic injectables have been discontinued because of unacceptable side effects and complications, which sometimes occurred even several years after the injection. A rigorous and meticulous search for the cause of granuloma formation leads the author to the discovery of bacterial infections as the leading trigger [7]. At the same time, while performing microscopy and scanning electron microscopy (SEM) examinations of our PMMA-spheres (Figure 12), we discovered impurities of smaller PMMA-particles between ranging from 1μm to 20μm (Figure 7). Macrophages can transport these particles from the injected PMMA-implant to the immune system, where the memory regarding former small particles and their chemical nature are stored, until a systemic infection may trigger a stronger attack against PMMA and cause granuloma formation [7]. To significantly reduce the risk of, or even prevent granuloma formation after PMMA microsphere injections, the spheres have to be absolutely round and smooth and must not contain any particles of less than 20 microns. The same quality standard must apply to future injectable bulking agents for the treatment of gastroesophageal reflux (GERD), stress urinary incontinence (SUI), and degenerative disc disease (IDD), containing larger PMMA spheres of 125 microns (Figure 13) [13,14].
Figure 12: Apparently “clean” PMMA-microspheres between 36μm and 46μm: the content of small particles cannot be seen in this SEM picture because the focus is higher than the ground PMMA microspheres.
Figure 13: For the therapy of urinary incontinence and gastric reflux, the larger venous plexus in the urethral and esophageal sphincter request larger microspheres of 125μm – compared to 40μm-microspheres used for subdermal injections v.
Disclosure
All authors have been involved in the development of safe, injectable PMMA microspheres and currently have no financial interest.
Mitochondrial Hormone Receptors – an Emerging Field of Signaling in the Cell’s Powerhouse
Abstract
Hormone receptors that are classically located in either cytosol or nucleus or in the plasma membrane are also found in mitochondria. Notably, they belong to different categories, such as proteins mainly known as hormone-dependent transcription factors, receptor tyrosine kinases, multimeric ligand-gated ion channels, and G protein-coupled receptors. Some of them represent mitochondrial variants, whereas others seem to be almost or fully identical with the extra mitochondrial forms. In some cases, mitochondrial receptors are associated with the outer membrane, whereas others are integrated in the inner membrane and act by signaling towards the matrix. In functional terms, some steroid receptors display genomic actions at the mitochondrial chromosome, whereas membrane-bound receptors transmit metabolic effects in the matrix or at the electron transport chain and modulate mitochondrial structure and length or apoptosis.
Abbreviations: GPCRs : G Protein Coupled Receptors; GUCY2s : Guanylyl Cyclases; RTKs: Receptor Tyrosine kinases; GR: Glucocorticoid Receptor; GRE: GR Response Element; MnSOD: Mitochondrial Superoxide Dismutase; ETC: Electron Transport Chain; PR: Progesterone Receptor; EGFR: Epidermal Growth Factor Receptor; PKA : Protein kinase A
Introduction
The classic view of hormone receptors comprises categories of
(i) Membrane-bound proteins, such as G protein-coupled receptors (GPCRs), receptor guanylyl cyclases (GUCY2s) and receptor tyrosine kinases (RTKs), and
(ii) Intracellular, typically genomically acting receptors that exert their effects as transcription factors in the nucleus. In the latter category, the ligands are small, sufficiently lipophilic molecules able to cross the plasma membrane. Some of their receptors associate with their ligands in the cytoplasm, others directly in nucleus, but sometimes, variants of these receptors may be membrane-associated and transmit nongenomic actions, as found, e.g., in some steroid receptors. In recent years, evidence has accumulated that receptors for hormones and other endocrine factors also exist in mitochondria, as will be outlined in this article. Depending on the respective molecules, the knowledge on transfer of the receptors or receptor variants to the mitochondria as well as on the intramitochondrial signaling mechanisms is different. Nevertheless, the details already known to date are fundamentally expanding our understanding of mitochondrial regulation by hormones, and this emerging field provides exciting insights into the participation of mitochondria in the control of cellular functioning.
Steroid, Tyrosine hormone, and Vitamin D3 Receptors in Mitochondria
In addition to the well-understood genomic actions in the nucleus and several non genomic extra mitochondrial effects, the localization of steroid receptors in mitochondria has been repeatedly described. The presence of a glucocorticoid receptor (GR) in mitochondria had been demonstrated as early as in 1993 [1]. In another pioneering study, which was, however, poorly considered for several years, a GR response element (GRE) was shown to be present in a D-loop of the mitochondrial chromosome [2]. Meanwhile, several investigations have demonstrated GR translocation to mitochondria [1-5], a process that depends on glucocorticoid availability [1-5] and on a mechanism reminiscent of the transfer into the nucleus, also involving heat shock proteins and an immunophilin [4].
Mitochondrial GR localization in conjunction with the existence of a GRE in the mitochondrial chromosome strongly indicates a regulation of mitochondrial gene transcription by glucocorticoids. In addition, the mitochondrial GR seems to be involved in apoptosisinduction in thymocytes, which may not be surprising with regard to the presence of the proapoptotic machinery in this organelle [5]. Mitochondrial localization has been multiply shown for the estrogen receptor-β (ERβ) [6,7], the ER variant anyway known for its nongenomic signaling. In addition to modulation of bioenergetics [6], effects on mitochondrial gene expression were assumed [7]. Moreover, translocation of the usually genomically acting ERα was reported [8]. A more specific and, to a certain degree unexpected, nongenomic action has been recently described for this other estrogen receptor.
In breast cancer cells, ERα was shown to physically interact with the mitochondrial superoxide dismutase (MnSOD) [8]. As MnSOD is activated by the mitochondrially localized sirtuin SIRT3 by deacetylation at K68, an interference with the acetylation status of K68 was studied. These experiments revealed a correlation of ERα/MnSOD association with acetylation of this regulatory lysine [8]. Another recent finding of high actuality concerns the role of long noncoding RNAs (lcRNAs) in mitochondrial ER actions [9], results that may find parallels in the regulation of other mitochondrial steroid receptors. The nuclear-encoded lcRNA SRA (steroid receptor RNA activator) is also found in mitochondria. A relationship to ERs exists insofar as estrogens induce the nuclear SRA repressor protein SHARP (SMRT/HDAC1-associated repressor protein).
Another inhibitory action on SRA is caused by the protein SLIRP (SRA stem-loop interacting RNA-binding protein), a player that is present in mitochondria and also modulates mitochondrially encoded RNAs (mtRNAs) and has effects on the electron transport chain (ETC) [9]. These findings indicate that mitochondrially located ERs may be stabilized by SRA, but seem to be inhibited by estrogen-dependent up regulation of SHARP in the nucleus and by actions of SLIRP in the mitochondria. These results and their interpretation strongly underline the importance of the nuclearmitochondrial interplay as well as the previously unexpected complexity of the coordinated relationship between nuclear and mitochondrial genomes.
A mitochondrial progesterone receptor (PR) has been demonstrated and discussed in terms of nongenomic effects [10- 13]. These actions concern respiratory activity, such as increased mitochondrial membrane potential and oxygen consumption [10-12], a role that would be in line with metabolism-enhancing properties of property of progesterone, as known from the postovulatory increase in temperature. The mitochondrial PR variant has been shown to be truncated, in which N-terminal domains as well as the DNA-binding domain are absent [10]. Therefore, this PR variant can only act nongenomically. Genomic effects in mitochondria via PR would only be possible, if additional variants can be detected. Two variants of the receptor for another intracellularly acting hormone, triiodothyronine (T3), were discovered in mitochondria [14-16]. Both are truncated forms of the receptor TRα1 of different lengths, p43 and p28. The p43 protein was shown to stimulate mitochondrial gene expression and to influence cell differentiation and apoptosis [16], whereas the role of p28 remains to be identified. The vitamin D3 receptor (VDR) was also detected in mitochondria [17-21]. VDR translocation was reported to take place via the permeability transition pore [18]. VDR signaling seems to mainly result in the suppression of respiratory activity [19-21]. Additional effects on lipid metabolism have been discussed.
EGFR, a Receptor Tyrosine Kinase, in Mitochondria
EGFR (epidermal growth factor receptor) is an example for a receptor tyrosine kinase that has been shown to be translocated to mitochondria [22]. This finding differs from the previously discussed cases insofar as the ligand is not a low-molecular weight molecule such as steroids, T3 and the vitamin D3 hormone, but represents a peptide of 53 amino acids. However, as proteins like the receptors are translocated, there should be no fundamental problem to also translocate the ligand. Mitochondrial EGFR has been studied in detail in non-small-cell lung cancer cells. It was shown to be internalized by endocytosis and, thereafter, attached to mitochondria [22]. The translocation was stimulated by EGF.
EGFR signaling caused several effects concerning the ETC, in particular, increased ATP formation, but also induced changes in mitochondrial structure and distribution, with consequences to enhanced cell motility. By interfering with the mitochondrial fusion factor Mfn1, it shifted the fusion/fission balance towards fission [22]. Notably, the inhibition of mitochondrial fusion leads to facilitated redistribution of the smaller mitochondria within cells, which would be impossible with the longer organelles that can, in the extreme, fuse to large networks. An important advantage of redistribution is avoidance of peripheral mitochondrial depletion.
Mitochondrial Localization of Tetrameric and Pentameric Membrane-bound Receptors
Translocation of membrane-bound receptors composed of several subunits, frequently heteromers, to mitochondria appears, at first glance, to be rather unlikely. Nevertheless, this has been shown or concluded to be possible. With regard to an endocytosis mechanism that initiates translocation, this is, however, not at all implausible. A report concerning a mitochondrial NMDA receptor, which represents a tetrameric ionotropic glutamate receptor, indicated several actions concerning enhanced production of reactive oxygen species, however, along with reduced cytochrome c release [23], effects that would require in-depth analysis and confirmation.
In liver and brain, several nicotinic acetylcholine receptors were reported to be mitochondrially localized [24-26]. In these tissues, the heteropentameric subtypes α7β2, α4β2 and, to a minor extent, α3β2 were detected, whereas in the lung, the α3β4 receptor subtype prevailed [24]. The nicotinic receptors were reported to be associated with the outer mitochondrial membrane and to be involved in the regulation of apoptosis, partially in a protective way. The 5-HT3 receptor represents another pentameric, ionotropic receptor type that was found in cardiac mitochondria [27]. However, the receptor was not analyzed with regard to the various 5-HT3 subtypes, which differ in their composition of subunits. The receptor was reported to increase the respiration control ratio and to inhibit the opening of the permeability transition pore.
GPCRs in Mitochondria
Similar to other membrane-bound receptors, GPCRs have to be integrated into membranes. In the case of GPCRs, insertion of seven transmembrane domains is required. Nevertheless, even these larger integral membrane proteins can be translocated to mitochondria. One example concerns the serotonin receptor 5-HT4 [27], which differs from the afore-mentioned ionotropic 5-HT3. In functional terms, the mitochondrial 5-HT4 receptor was reported to decrease the respiration control ratio, contrary to 5-HT3, whereas the opening of the permeability transition pore was, again, found to be inhibited [27]. Particular insights were obtained by studies on the type-1 cannabinoid receptor CB1, which is also translocated to mitochondria [28-31].
Apart from its neurobiological relevance, the particular significance of one of these studies [31] concerns the signaling mechanism of the mitochondrially located CB1. It was shown to modulate the activity of the soluble adenylyl cyclase (sAC) in the matrix via the α-subunit of a Gi protein. This allows conclusions on the orientation of the receptor. It has to be located in the inner membrane, with the C-terminus that has to interact with Gi towards the matrix side and the ligand binding pocket towards the intermembrane space. The functional consequences of this signaling mechanism are reduction of cAMP levels in the matrix and lower protein kinase A (PKA) activity. Insofar this antagonizes the activation of sAC by bicarbonate, which serves to adapt the respiratory electron flux to the activity of the citric acid cycle.
Enhanced matrix PKA activity leads to phosphorylation of ETC subunits, especially in Complex 1, and presumably, also in other sites. The up regulation of phosphorylation of Complex 1 subunits as initiated by bicarbonate enhances electron feeding to the ETC, whereas the down regulation via CB1 decreases the entrance of electrons into the ETC. These findings on the effects mitochondrial CB1 were also important for interpreting the mitochondrial action of the melatonin receptor MT1. This receptor subtype was shown to be located in mitochondria, contrary to MT2 [32]. Under basal, non compromised conditions, melatonin regulates respiration and Complex 1 activity in a similar way as cannabinoids via CB1. Therefore, it was concluded that MT1 has to be correspondingly oriented in the inner mitochondrial membrane and acts via Gi, sAC inhibition, decrease of cAMP concentration and PKA activity [33].
Conclusion
The localization of hormone receptors in mitochondria considerably expands our insights into the actions of their ligands. It is a remarkable fact that entirely different types of receptors, which are, from a conventional point of view, either present in the cytosol and/or nucleus or in the plasma membrane, can be found in mitochondria. Moreover, the membrane-bound receptors belong to different categories, such as RTKs, multimeric ligandgated ion channels or GPCRs. This multiplicity sheds light on the complexity of cellular processes which connect nuclear, cytosolic and mitochondrial functions in a concerted way. This emerging field will certainly gain increasing future importance and unravel numerous poorly understood connections in cell biology and biomedicine as well.
Total Knee Arthroplasty using Computer Assisted Surgery in Paget ’s disease of Knee-A case report
Abstract
The purpose of this case report is to highlight the advantages of computer assisted navigation surgery (CAS) to improve the accuracy in performing Total Knee Arthroplasty (TKA) in a patient affected by Paget’s disease of the femur and secondary osteoarthrosis of knee. Paget’s disease can be associated with technical difficulties while performing knee arthroplasty because of intra and/or extra-articular deformity in either sagittal or coronal planes or both and there are published reports of sub-optimal varus or valgus placement of components by the manual technique. A 55-year-old male with monostotic Paget’s involvement of the femur with lateral femoral bowing and end stage arthrosis in the knee was managed with a primary cemented cruciate-retaining TKA using Aesculap Orthopilot 5.0 navigation system. His pre-op VAS score of 8/10 and Oxford Knee Score of 20 improved to 2/10 and 42 respectively at 1 year follow up. Knee involvement with Paget’s in Indian population is extremely rare and we are not aware of any previous case reports of using CAS in performing TKA in Paget’s. CAS can obviate the need for corrective osteotomy when performing TKA in patients with extra-articular deformity.
Paget’s disease is a disorder of bone characterized by increased bone turnover, enlargement and thickening of the bone which is unusually brittle, more prone for deformity or fractures in weight bearing joints and arthritis of joints with affected adjacent bones [1]. As the proximal femur and pelvis are more commonly affected, hip arthritis and challenges with total hip arthroplasty [2,3] are well described than the knee arthritis and total knee arthroplasty [4]. We report a case of monostotic Paget’s involvement of distal femur and associated knee arthritis that underwent a total knee arthroplasty by computer assisted surgery. Paget’s involvement especially isolated involvement of distal femur and knee in Indian population is rare as compared to the Western population [5]. We are not aware of any previous reports of using computer assisted surgery in Paget’s involvement of the knee. The purpose of this report is to highlight the role of computer assisted surgery in achieving optimal component alignment in cases of intra or extra articular deformity which is seen with Paget’s disease.
Case Details
A 56-year-old male presented to us with severe disabling pain in his right knee affecting his day to day activities and which failed to respond to conservative measures. His plain radiographs showed mixed sclerotic and lytic lesions involving the entire shaft of the femur and a diagnosis of Paget’s was made on the typical radiological signs [6] on plain radiographs (Figures 1 & 2) and MRI (Figure 3). There was an anterolateral bowing of the femur about 100 and knee arthrosis changes with intra-articular varus deformity. There was no involvement of the tibia (Figure 2). His pre-operative pain score was 8 on visual analogue scale (VAS) and Oxford Knee Score [7] (OKS) was 20. The patient underwent a primary cemented cruciate retaining TKA by computer assisted navigation system (B Braun Columbus, Aesculap Orthopilot 5.0 navigation). The patient was placed supine, under spinal anaesthetic and tourniquet control a midline incision with sub vastus arthrotomy was performed. Using femur and tibia infra-red trackers, registration of the thefollowing bony landmarks was made-posterior most part of medial and lateral femoral condyles, lowest point of medial tibial plateau, highest point of lateral tibial plateau, knee centre, anterior femoral cortex, most prominent points of medial and lateral malleoli and hip, knee and ankle centres were marked.
Figure 1: Plain radiograph showing the mixed sclerotic and lytic lesion typical of Paget’s involving distal femur with arthritic changes in the knee. Note: There is no tibial side involvement with Paget’s.
Figure 2: Long leg radiographs showing the characteristic lateral femoral bowing and involvement of the entire femur with Paget’s. Notice the normal pelvis and contralateral femur.
Figure 3: The typical features of Paget’s on T2 and T1 weighted MRI images showing a dominant signal intensity similar to that of fat corresponding to early mixed active phase.
The pre-operative deformities recorded on navigation system were 30 varus and 120 flexion deformity (Figure 4). After appropriate soft tissue releases and bone cuts, cemented cruciate retaining implants with size 6 femur, size 3 tibia and size -10 polyethylene insert was implanted. The final alignment postoperatively was 10 valgus and 70 flexion (Figure 5). The femoral component was intentionally anteriorized and inserted in flexion to avoid any notching of anterior femoral cortex (Figure 6). There was no need for a corrective osteotomy of the femur for the extraarticular deformity. The total blood loss was 180ml and operative time was 62minutes. Intra-operatively the knee was infiltrated with a cocktail mixture of 0.2% Ropivacaine-30ml, Ketorolac-60ml, Morphine 4mg, 0.5ml of 1:1000 Adrenaline and normal saline 30ml. An epidural catheter was inserted in the knee and left in place for 48 hours to facilitate regular infiltration with 0.2% Ropivacaine. Apart from these measures, the patient was given an adductor canal block in the immediate post-operative period. Adductor canal block is a pure sensory block which does not affect the quadriceps functionand the patient was made to walk on day 0 with walker support along with commencement of immediate knee mobilization. The patient was also administered 1gm Tranexamic acid IV just before the surgery. There were no drains inserted. The antibiotic prophylaxis was with 1gm Cefuroxime intravenous pre-operatively and two further doses post-operatively. Thromboprophylaxis was with 2.5 gm Apixaban twice a day for two weeks along with TED stockings. The patient had an uneventful recovery and was discharged on day 3 and followed up on days 14, 6weeks, 3months, 6months and 1year. The patient returned to normal activities at 3months and at latest follow-up of 1 year the OKS was 38 and VAS score for pain was 2 (Figure 7).
Figure 5: computer navigation images showing the final component alignment./p>
Figure 6: Immediate post-operative radiograph showing correction of deformity and restoration of mechanical alignment. Notice the femoral component in slight flexion to avoid anterior femoral notching.
Figure 7: 1 year follow-up clinical photograph showing excellent functional.
Discussion
Paget’s disease of the bone is associated with a hypervascular and hyperdynamic state and the bone is unusually hard and brittle. The differential diagnosis of Paget’s is osteopetrosis, fluorosis, sclerotic secondaries. Arthroplasty surgery in a joint adjacent to a Pagetic bone poses special challenges with the amount of blood loss, increased operative time, bone hardness requiring special blades and drills to make the bone cuts and most importantly restoration of the correct mechanical alignment in view of any extra articular deformities [8,9]. These technical difficulties are well described with regards to hip arthroplasty but less literature with regards to the knee. All the reported cases in the knee are with conventional technique which reported satisfactory results but none with computer assisted surgery. Exposure of the knee can also be difficult in Paget’s knee because of soft tissue contracture and hyperplastic patella [10] which we did not face in our case. When using an intramedullary guide by the conventional technique there is a possibility of femoral and tibial component size mismatch [4]. With the computer assisted surgery this problem can be overcome. In patients of Paget’s with knee involvement the deformities are usually complex and multiplanar.
There could be a combination of intra and extra articular deformities and the extra-articular deformities may be in either sagittal or coronal planes along with torsional deformity. In the TKA done by conventional technique, there are reports of the knees being left outside the acceptable range of 50-100 valgus because of the difficulty in achieving a correction of the multiplanar deformities [4,11,12]. In the sagittal plane, because of the anterolateral bowing there is a potential risk of placing the femoral component in excessive flexion or extension by the conventional technique, in addition to the difficulty in using an intramedullary jig because of the bone hardness and risk of femoral perforation. With the help of computer assisted surgery [13], the hip, knee and ankle centres are accurately marked and potential anterior or posterior femoral notching can be avoided without affecting the flexion-extension gaps. We could also balance the knee with using a cruciate retaining prosthesis. There are previous reports of combined femoral corrective osteotomy and intramedullary nailing with simultaneous knee arthroplasty [14,15] for coronal planedeformity more than 100 and sagittal plane deformity more than 200. We could achieve satisfactory restoration of the alignment and balancing without the need for corrective osteotomy with the aid of computer assisted surgery.
In cases of hip arthroplasty, both cemented [16] and uncemented [17] designs have been used with good long term success. There are limited studies with regards to knee replacements; However, these have not shown any early component loosening [4,18]. Our limitations are short follow-up of only 1year and this being only a single case report because of the rarity of the problem in Indian population and that too monostotic involvement of the femur with knee arthritis. Computer assisted surgery is not universally available and has a steep learning curve. There are no long term studies to show the superiority of computer assisted surgery over conventional technique in terms of functional outcome. However, the senior author (KKE) was well experienced in computer assisted surgery.
Conclusion
Paget’s involvement around the knee can be associated with both intra and extra-articular deformities and Total Knee Arthroplasty in these patients can be technically challenging when performed by conventional technique. Computer assisted surgery can help map the multi-planar deformity and achieve optimal overall final component alignment and ligament balancing.
Prognosis Comparison Molecular Subtype Breast Cancer between Young and Adult Women at General Hospital Dr. M Djamil Padang
Abstract
Breast cancer is a heterogenic disease with various biologic profiles and clinical prognosis. A research in Netherland by Esther, et al 2013, showed that molecular subtypes of breast cancer have different distribution and prognostic between young and adult, but there is no local and national data.A Comparative research with cross sectional design was Held in January-April 2015 with 96 samples of breast cancer women with age < 40 years old and > 40 years old, recorded in medical records and breast cancer registrated from 2012-2014. Young women Breast cancer at General Hospital Dr. M. Djamil Padang for 3 years (2012-2014) are 27.1% and the adult are 72.9%. In bivariate analysis, there are no relationship between characteristics of tumor with recurrent and death event while in the adult women breast cancer, tumor size and metastases have relation with recurrent and death event that are statistically significant. There are different characteristics and description of molecular subtype breast cancer between young and adult women, young ages are tend to have big tumor, lymph node positive, lympovascular invasion, high grade tumor, proliferation index Ki67 high and negative hormone receptor. There are different tendency of prognosis women breast cancer between young and adult based on molecular subtype but statistically, the relationship is not significant.
Keywords: Age; Breast Cancer Molecular Subtype; Prognosis
Introduction
Breast cancer is a heterogenic disease with various biological profile and clinical prognosis [1]. Most patients with breast cancer are old women, but we still lack of specific guideline about evidence based therapy for this age group. Population of Young woman with breast cancer, otherwise, has based the decision about breast cancer therapy on prognostic, predictive factors, and tumor characteristic [2]. The European Society of Breast Cancer Specialist defined young women as women aged less than 40 years [3]. There is favorable correlation between ages with biological characteristic of the tumor. Compared with young age, old aged patient with breast cancer had more diploid, low s-phase fraction, normal p53, negative or low epidermal growth factor receptor and c-erB2 [4]. Breast cancer in women aged under 40 years old tend to has larger size (tumor median is 2 cm in young age and 1.5 cm in old age), more advanced stadium when diagnosed (more likely with positive lymph gland) and more aggressive (less likely to have good differentiation), low expression of estrogen/progesterone receptor (ER/PR), high expression of human epidermal growth factor receptor2 (HER2), and Ki67 marker proliferation [5-10]. Tumor with positive hormone receptor has better outcome, where luminal A tumor has slower progressivity compared with luminal B tumor. While tumor with negative hormone receptor have aggressive natural pathogenesis and poor outcome [2].
Although it has been given the optimal treatmentt, but some clinical trials showed that breast cancer patient with young age had worse outcome compared with old aged breast cancer patient [10]. The distribution and prognostic effect of certain molecular subtype from old aged breast cancer patient compared to young aged breast cancer patient is remains unclear. A study conducted by Esther et al. [10] in Netherland showed that breast cancer molecular subtype has distribution and prognostic effect difference between old aged breast cancer patient compared to young aged breast cancer patient. While the data about comparison about distribution and breast cancer molecular subtype prognostic between young and old aged breast cancer patient, either local or nationwide, was not found by author. This is why author wanted to investigate thedifference of breast cancer molecular subtype prognostic between young and old aged breast cancer patient at Dr. M DjamilGeneral Hospital, Padang.
Material and Method
Population and Sample: The population in this study was all of the breast cancer patient who registered at the medical record and breast cancer registration on Divison of Oncology Surgical Department Dr. M Djamil Hospital Padang.The sample in this study was breast cancer patient who diagnosed andtreatment according to protocol and registered atthe medical record and breast cancer registration on Divison of Oncology Surgical Department Dr. M Djamil Hospital Padang in 2012-2014 by using the simple random sampling technique.
Female breast cancer patients young age (≤ 40 years) and older (> 40 years) who had done histopathology and immunohisto chemistry examination. Exclusion criteria:
I. Breast cancer patients with cancer of the other organs were not metastasis of breast cancer
II. Breast cancer patients who died within a period of three years by another cause
III. Breast cancer patients with medical records could not be traced.
Research Pathways:
Figure 1 in this study, the data collected was secondary data from medical record archives and breast cancer registration in Division of Oncology Surgical Department Dr. M Djamil General Hospital Padang.
Figure 1:
Data Processing
The data in this study were been through several process including:
a) Data Editing: Conducted in the data storage to make sure that the data in medical record and breast cancer registration met the criteria so the mistake can be avoided
b) Data Coding: the data was given number and code to make the analysis easier
c) Data Entry: the data was inputted into the computer
d) Data Cleaning: to recheck if there was any mistake in data and also to correct and examine the data to make sure the data was valid
Results
Research result was found after all of data from medical records and breast cancer registrations in Oncology Surgery Division of Surgery Department of Centre General Hospital Dr. M. Djamil Padang years 2012 – 2014. Home visiting was done for patients who live in West Sumatera Province. Patients that live out of West Sumatera be interviewed by phone or interviewed when they were following up to Oncoligy Surgery Polyclinic. The number of samples in this research was 96 breast cancer patients who have inclusion criteria. From 96 breast cancer patients, all of them had histopathological diagnosis, immunohistochemistry status, but only 32 patients had lympovascular invasion status and 59 patients had their histopathology grading. Data was processed computerize. Data analyses was done descriptively and using Chi – square test for finding correlation between 2 variables with confidence index was 95%.
Univariate Analysis
Breast cancer characteristics:
Table 1 from 15 death patients, 12 dead caused by breast cancer and 3 because of other causes.
Table 1: Distribution Frequency of Breast Cancer Characteristics.
Bivariate Analysis
Table 2 statistically, this difference is not significant (p>0,05), there is no correlation between histopathology type of breast cancer with recurrence rate both age or either overall criteria (Table 3).
Table 2: The Correlation of Histopathology with Result of Recurrence Treatment Based on Patient’s Age.
Table 3: The Correlation of Histo-pathology with Death Rate Based on Patient’s Age.
Statistically, this difference is not significant (p > 0, 05), there is no correlation between histopathology type of breast cancer with death rate both age or either overall criteria. The percentage of death is more in patient with invasive lobular carcinoma type.
Based on Tumor Grade
Table 4 statistically, this difference is not significant (p >0, 05), there is no correlation between tumor grade with recurrent both age or either overall criteria. The young age has more recurrence rate than adult patient, especially in grade III tumor (Table 5). Statistically, this difference is not significant (p >0, 05), there is no correlation between tumor grade with death rate based on age or either other all criteria. Based on tumor grade, young breast cancer patient’s survival rate is less bad (Table6).
Table 4: The Correlation of Tumour’s Stage with Result of Recurrence Treatment Based on Patient’s Age.
Table 5: The Correlation of Tumour’s Stage with Death Rate Based on Patient’s Age.
Table 6: The Correlation of Lymphovascular Invasion with Result of Recurrence Treatment Based on Patient’s Age.
Statistically, this difference is not significant (p >0, 05), there is no correlation between lympovascular invasion with recurrence rate both age or either overall criteria. Statistic test could not be done in young age because of no recurrent data in patient without lympovascular invasion. Recurrent percentage is more in breast cancer patients with lympovascular invasion (Table7). Statistically, this difference is not significant (p > 0, 05), there is no correlation between lymphovascular invasion with death rate in breast cancer patient. Statistic test could not be done in young and adult because of there is no enough data. Generally, more of breast cancer patients died with lympovascular invasion (Table 8).
Table 7: The Correlation of Lymphovascular Invasion with Death Rate Based on Patient’s Age.
Table 8: The Correlation of Tumor Size with Result of Recurrence Treatment Based on Patient’s Age.
Statistically, this difference is not significant (p >0, 05), there is no correlation between tumor size with recurrence rate, although based on age or other all finding. Young breast cancer patients have bigger size and more recurrence rate compared with adult patients (Table9). Statistically, this difference is significant (p <0, 05), there is correlation between tumor size with death rate, but not significant on younger age. Young breast cancer patients have higher death rate than adult patients, and the young has bigger tumor size (Table10).
Table 9: The Correlation of Tumor Size with Death Rate Based on Patient’s Age
Table 10: The Correlation of Glands Lymph Involvement with Result of Recurrence Treatment Based on Patient’s Age.
Statistically, this difference is not significant (p >0, 05), there is no correlation between glands lymph status with recurrence rate based on both age or either overall criteria. Young breast cancer patients with positive glands lymph involvement have higher recurrence rate than adult patients (Table11). Statistically, this difference is not significant (p >0, 05), there is no correlation between glands lymph status with death rate on breast cancer patient, both age or all other. Young breast cancer patients with positive lymph glands have higher death incidents than adult patients.
Table 11: The Correlation of Glands Lymph Involvement with Death Rate Based on Patient’s Age.
Based on Metastasis
Table 12 statistically, this difference is significant (p <0, 05), there is correlation between metastasis with death on adult patients and overall, but not significant on young patients. Young breast cancer patients without metastasis are more death than adult patients.
Table 12: The Correlation of Metastasis with Death Rate Based on Patient’s Age.
Based on molecular subtype
Table 13 statistically, this difference is not significant (p >0, 05), there is no correlation between breast cancer’s molecular subtype with recurrence based on age either overall. Young breast cancer patients with any molecular subtypes are more recurrence than adult patients (Table 14). Statistically, this difference is not significant (p >0, 05), there is no correlation between breast cancer’s molecular subtype with death based on age either overall criteria. The death breast cancer patients are more on young age, especially triple negative subtype.
Table 13: The Correlation of Molecular Subtype with Result of Recurrence Treatment Based on Patient’s Age.
Table 14: The Correlation of Molecular Subtype with Death Rate Based on Patient’s Age.
Discussions
From medical records data and breast cancer registry, there were 96 breast cancer patient who underwent treatment in dr. M. Djamil General Hospital from 2012 until 2015. The difficulty in this study was the lack of evaluation of tumor’s grading and lymphvascular invansion’s status by anatomy pathology department, there were only 59 patients of 96 patients who had tumor grading and only 32 patients who had lymphovascular invansion’s status. There were 27 cases of recurrent breast cancer and 15 patients died, but only 12 patients who died of breast cancer.There were many factors affect the prognostic of breast cancer and age was the most important factor for recurency risk whithout depend on the other factors (indenpendent risk factor) [11-14]. There was relationship between age and biological characteristic of tumor [4]. Patologic subtype is one of prognostic factors breast cancer. The most histopathologic type of breast cancer was invasive ductal carcinoma [15]. There was a differency between invasive ductal carcinoma and invasive lobular carcinoma. Invasive lobular carcinoma was more occured with old age, biggest tumor size, positive of receptor hormone, negative of HER2 and p53, and rarely invade the vascular if compared with invasive ductal carcinoma, but it often multifocal, multicentric and bilateral, associated with increased risk of contralateral breast cancer, low grade histology, often metastasize to unusual locations like gastrointestinal tract and died. Particulary, invasive lobular carcinoma show characteristics that lead to good prognostic compared to invasive ductal carcinoma [16,17].
In this study, invasive ductal carcinoma was the most type occured which is 76 patients (79,2%). From 20 invasive lobular carcinoma’s patients, most of them occured at old age (> 40 years old) which were 15 patients. However, percentage of reccurent events and death was greater in young cancer patients. (38,5% and 16,7%) with same type histopatology which was invasive lobular carcinoma (40% and 20%). If it associated with other tumor characterisics, invasive lobular carsinoma in young age had tumor with T4 stadium and positive lymph node. Most of them had ER (-), PR (-), and HER2 (-). One of patients had lung metastasis. In this study showed that characteristic tumor was more influenced by young age than other histopathologic tumor although invasive lobular carcinoma had better prognostic, it will be a bad prognostic if it occured in young age. Grade of histology tumor assessed by differentiation degree of tumor tissues.50 Tumor with high grade had abnormal shape and tend to aggressive, reccurency, and metastasize. Breast cancer patients with high grade tumor include in the high risk group and indicated to had adjuvant chemotherapy. There was reverse relationship between tumor differentiation grade with pathomorphological response (PMR) grade in breast cancer patients who had neoadjuvant chemotherapy, where well differentiated tumor had bad respon.
In this study, recurrence and death was higher than tumor with grade II and III. Based on age, young patient had worse prognostic than old patient because most of them had grade III tumor. In old patient, the recurrence and death more frequent in grade II tumor. In general, these tumor had big size (T2), had positive lymph node when diagnosed, vary response of hormone receptor but most of them had high index of Ki6714%. This was concordant with characteristic of high grade tumor, which was the higher tumor’s grading means more aggresive and fast proliferations that noted by high index of Ki67, bigger size, and invasion to other tissue like lymph node but there was no far metastasis when diagnosed. Most of these patients had adjuvant therapy, but there were recurrence, both locoregional or far, and died in 3 years after diagnosed. This was caused by reccurency process occured when treatment and other criteria like young age and positive lymph node caused patients in high risk group. Invasion of lymphvascular was an important step in complex process for metastasis and an important criteria to decide the next treatment [18]. Invasion of lymphvascular was an indenpendent bad prognostic factor on invansive breast cancer patients [19].
Young Ju Song et al. reported percentage of OS and DFS 5 years lowest in patients with lymphvascular invasion compared whose not. In this study, patients with lymphvascular invasion had bad prognostic with higher percentage of recurrence and death (33,3% and 20%). The result of statistic test showed there was no relationship between lymphvascular invasion with residif and death (p+ 0,209 and p= 0, 092). There was no data about recurrence in young patients without lymphvascular invasion, it was difficult to compare prognosis between these both group age with lymphvascular invasion. This was caused by the lack of data, there only 32 patients of 96 patients that had lymphvascular invasion status. Lymphovascular invasion is a step in complex process of tumor metastasis and also important for the next treatment. Lymphovascular invasion is a poor prognostic factor which is independent in patient with invasive breast cancer. Young Ju Song, et al has the percentage of OS and DFS 5 years lower in patient with lympovascular invasion compared with the patient without lympovascular invasion. In this research, patient with lympovascular invasion have a poor prognostic with percentage of recurrence and mortality (33,3% and 20%). Statistical test result shows there is no connection between lympovascular invasion with recurrence or mortality (p = 0,209 dan p = 0,092). There is no data or evidence about recurrence condition in younger patient and mortality in older patient with or without lympovascular invasion, so it is hard to compare the prognosis from age category. This is due to only 32 out of 96 patients that have lympovascular invasion.
All of the patients with lympovascular invasion with recurrence condition or death have histopathological type of ductal invasive carcinoma, this is in accordance with the literature that said this type of histopathological more often invade the lympovascular tissue compared to invasive lobular carcinoma. Young patient have worse prognosis. Every young patient with recurrence condition, died after treatment, but in the other hand there is no mortality in old patient with recurrence condition. Characteristic of tumor in young patient has poor prognosis due to a large tumor size, presence of positive lymph node, high grade tumor, negative hormone receptor and also high proliferation index of Ki67. There is accumulation from several poor prognostic factors in young age patient with breast cancer. The difference is, old patient with breast cancer have better prognosis due to presence of positive estrogen and progesterone also low grade of Ki67. Tumor size is one of prognostic factor in breast cancer [13]. Tumor size is correlated to the presence and amount of axillary lymph nodes involved, and also an independent prognostic factor, with increase recurrence that is concomitant with tumor enlargement [20]. Lethality of breast cancer increase with tumor size and presence of regional lymph node [21].
In this study, the incidence of recurrence and mortality increase with tumor size (38,5% and 27%). Young patient with breast cancer tend to have bigger size of tumor and higher recurrent incident compared to old patient with breast cancer. Percentage of tumor with T4 in young age patient who experience recurrent (44, 4%) while in old patient (33,3%). Most of tumor with T4 has positive lymph nodes in both ages. Young patient with breast cancer has more mortality with percentage (16, 7%) compared to old patient (11,6%), however tumor with T4 has more mortality in old patient (28,6%). This is likely due to most of patients already having distant metastasis when diagnosed. This correlation was statistically significant in tumor size with mortality incident in old patient (p = 0, 03) or mortality incident in old patient with metastasis (p = 0,01). This can be explained that most mortality of death patient with T4 tumor has metastasis. Hormone receptors, expression of HER2 and Ki67 are the prognostic factor of breast cancer. Tumor with positive hormone receptor have better outcome compare to tumor with negative hormone receptor. Ki67 describes the proliferation of tumor cell and provide information and independent prediction of the response to chemotherapy and prognosis for breast cancer patient who received neo adjuvant chemotherapy [22,23]. Breast cancers in young woman (< 40 years old) tend to have low estrogen or progesterone expression and high expression of HER2 also proliferation marker of Ki67. The result of this study in accordance with literature that young woman with breast cancer (< 40 years old) has worse prognosis than older age (>40 years old) with higher recurrent percentage and mortality (38, 5% vs 24,3% dan 16,7% vs 11,6%).This poor prognosis at young age also in accordance with molecular subtypes that is triple negative (ER/ PR -, HER2 -). Recurrent occurrence at old patient (>40 years old) is more common in over expression of HER2 subtype and higher percentage of mortality in luminal B subtype.
However statistically, correlations between molecular subtypes with the prognosis of breast cancer based on age were not significant. Recurrent incident and mortality in younger patient is higher than older patient in every molecular subtype, this is probably because accumulation of poor prognosis factors based on age group which is large tumor size, positive lymph nodes, presence of lympovascular invasion, high grade tumor, high index of Ki67 proliferation. That means young age is associated with poor prognosis of breast cancer. Like other cancer, breast cancer is considered as part of the accumulation of multiple genetic changes resulting in excessive expression of oncogenes and loss of tumor suppressor. DNA methylation changes will ultimately lead to instability in genetic characteristics of cancer through various ways [24-26]. Data of methylation has been associated with clinico pathologic parameter to clarify the role of methylation in breast cancer carcinogenesis. Report from Widschwendter, et al showed a significant difference in hormone receptor status among the group with DNA methylation [27-30]. Through Southern analysis of BRCA1 promoter region, methylation was found in 11% sporadic breast cancer cases and inversely related to the expression of estrogen and progesterone receptors [24]. Song ping et al assessing the relative frequency of methylation in the two groups based on age between African-American and European-American. They found that young age (< 50 years old) breast cancer patient ethnic African-American and negative ER had significantly higher index of methylation in CDH13 locus compared to breast cancer patients ethnic European-American with the same characteristic [31-40].
Preoperative Uterine Artery Embolization for Huge Prolapsed Pedunculated Submucosal Fibroid
Opinion
Uterine fibroids (myomas) are very common affecting more than 60% of women over the age of 45 years [1,2]. Although many fibroids are asymptomatic, some may cause exhausting symptoms including heavy menstrual bleeding and pelvic pain. Submucosal fibroids, in particular pedunculated fibroids prolapsed into the vagina, are associated with heavy uterine bleeding and subsequent heavy anemia. The management of prolapsed pedunculated fibroid is determined by the origin and thickness of the pedicle, size, and its location. Uterine artery embolization (UAE) is increasingly being applied as a minimally invasive treatment alternative to surgery for the reduction of uterine fibroid symptoms [3]. UAEinduced depletion of blood flow through the whole myometrium and endometrium may be a useful adjunct to surgery for massive fibroids to reduce intraoperative blood loss [4].
Case 1
A 50 year old woman, G3P3, had a 1-year history of intermittent vaginal bleeding and progressive anemia. Physical examination revealed an ellipse of semi-solid; smooth surfaced mass occupying the vaginal cavity and hemoglobin level was remarkably decreasing (1.2 g/dl). Transfusion therapy was started immediately and intravenous iron prescribed to optimize her hemodynamic state. MRI detected a vaginal heterogenous mass 10x15x11cm, with regular edges and a vascular pedicle (Figure 1a). The mass seemed to dilate cervix up to the uterine fundus. Consideration of the inability to reach the pedicle through the vagina and the heavy vascularization of the fibroid led to the surgical approach through abdominal. The patient was put off UAE to reduce the blood supply, within 24 hours, with a surgical excision of 70% of the fibroid vaginally and subsequent simple abdominal hysterectomy and bilateral salpingo-oophorectomy.
Figure 1a: Large pedunculated submucosal fibroid prolapsed into the vagina in 50-year-old women. Sagittal T2-weighted MR images show a solid mass occupying vaginal cavity (arrow head) and atrophic normalappearing uterus was visible (arrow). Pathologically, the tumor was diagnosed as a leiomyoma.
Case 2
A 53-year-old woman, G2P2 (2 cesarean sections), was referred to us complaining of significant vaginal discharge for 2 years. Pelvic examination detected an over man’s fist sized, well-circumscribed mass in the vagina. Laboratory examinations revealed hemoglobin of 4.5 g/dl. MRI detected a margin-free vaginal mass 8x9x13 cm, with a highly vascular pedicle (Figure 1b). The patient was submitted to transfusion therapy, UAE proceeding later with subsequent total abdominal hysterectomy with salpingo-oophorectomy within 48 hours.
Figure 1b: Large pedunculated submucosal fibroid prolapsed into the vagina in 53-year-old women. Sagittal T2-weighted MR images show a solid mass occupying vaginal cavity (arrow head) and atrophic normalappearing uterus was visible (arrow). Pathologically, the tumor was diagnosed as a leiomyoma.
A 53-year-old woman, G2P2 (2 cesarean sections), was referred to us complaining of significant vaginal discharge for 2 years. Pelvic examination detected an over man’s fist sized, well-circumscribed mass in the vagina. Laboratory examinations revealed hemoglobin of 4.5 g/dl. MRI detected a margin-free vaginal mass 8x9x13 cm, with a highly vascular pedicle (Figure 1b). The patient was submitted to transfusion therapy, UAE proceeding later with subsequent total abdominal hysterectomy with salpingo-oophorectomy within 48 hours.
For pedunculated fibroids prolapsed into the vagina, the most frequently chosen approach includes vaginal twisting or ligation and excision, morcellation of large fibroids has been used, with or without hysteroscopically assistance techniques [3]. Like our cases, due to the risk of excessive blood loss because of its size, the great feeding vascularization and the thick pedicle of the fibroid, the vaginal approach was limited, preoperative adjunct UAE before the surgical approach may be attractive to minimize blood loss. The subsequent vaginal morcellation and abdominal hysterectomy can be performed in a blood supply-depleted field. Although of smaller dimension, and therefore our case needed special management. Although there is only two case of similar prolapsed fibroid in the literature [5,6], UAE may be very attractive before extracting large fibroids prolapsed into the vagina as a safe and minimally invasive technique.
What Should Oral Health Clinicians Tell Their Patients About Oral HPV? A Brief Review
Introduction
In the United States, it is estimated that there are at least 20 million new cases of sexually transmitted infections (STIs) each year, with a prevalence of 110 million people infected, and costing the country 16 billion dollars. The Centers for Disease Control and Prevention (CDC) estimates just over 14 million new cases of HPV infection each year in the US, where half consist of young people between the ages of 15-24 [1]. Approximately 90% of HPV infections will clear within a few years without any symptoms. However, for the infections that do persist, serious health risks may be the outcome.
HPV Natural History
We actually are still in the infancy stages regarding the natural history of HPV. However, the information we do have on cervical cancer guides the model for oral cavity cancer (OCC) and oropharyngeal cancer (OPC). HPVs are categorized into low-risk (wart-causing) and high-risk (cancer-causing) types. Globally, HPVs type 16 and 18 cause approximately 70% of cervical cancers [2]. The other two most common HPV types are 6 and 11, which predominantly cause genital warts. The tissues within the oropharynx are comparable to the tissues of the cervix, thus it is not surprising that we see a similar paradigm occurring between the two regions regarding HPV infection. For example, HPV can be found in precancerous lesions of the oral cavity, which is the same case in cervical cancer [3].
HPV Risk Factors
Internationally, over time, there have been changes in sexual behaviors with the age of sexual interaction beginning much younger; along with the increasing number of sexual partners one has [4-6]. As well, sexual practices have changed with oral sex being performed more by men and women within the 30-49 year age range compared with older adults [5,6]. As such, it is not surprising that HPV infection of the oral cavity is strongly associated with sexual behavior, but what is still perplexing is that it is twice as predominant in males as in females [7]. A multicenter study observed that the frequency of HPV detection in oral cancer biopsy specimens was higher among individuals who reported having more than one sexual partner or having oral sexual contact [8]. Furthermore, an increased risk of oral cancer has been reported both in women with cervical cancer and in spouses of women with cervical cancer [8,9]. These results may collectively suggest a common mode of HPV transmission between the oral and genital area, reinforcing the possibility of sexual transmission of the virus in the oral cavity. Potential reservoirs for the virus are proposed to be the tonsillar crypts [10,11] as well as periodontal pockets [12]. Also, an association between long-standing periodontitis and the risk of tongue cancers has been demonstrated [13]. A recent pilot study observed the oral health status of 223 patients and HPV infection [14]. Their results demonstrated a trend between oral HPV 16 infection and poor clinical oral health status. Thus, it is imperative that oral health practitioners continue to educate their patients on the connections between oral health status and acquiring other diseases.
HPV Prevention
Abstinence of any sexual behavior, including kissing, would be the most obvious form of prevention, but that is not likely to occur. The Advisory Committee on Immunization Practices (ACIP) recommends the initiation of routine HPV vaccines beginning at the age of 11 or 12 currently there are three different types of HPV vaccines on the market. Gardasil has two kinds available: thequadrivalent vaccine, which protects against types 6, 11, 16, and 18; and the nonavalent vaccine, which protects against the same types as the quadrivalent vaccine plus five more types (31, 33, 45, 52, and 58). Cervarix has a bivalent vaccine for HPV types 16 and 18. The quadrivalent vaccine was introduced in 2006 and approved for males in 2009. When we look at data extracted between 2003- 2006 and 2009-2012 we see evidence of vaccine efficacy in HPV prevention within women (Figure 1) [15]. For all age groups except for females 25-29, there was a decrease in the prevalence of HPV between the two time periods.
Figure 1: Human Papillomavirus – Cervicovaginal Prevalence of Types 6, 11, 16 and 18 Among Women Aged 14-34 Years by Age Group and Time Period, National Health and Nutrition Examination Survey, 2003-2006 and 2009-2012.
Herrero [16] provided evidence that HPV vaccines used to prevent cervical cancer can be effective in preventing infection of oral HPVs. In a randomized clinical trial in Costa Rica, 7,466 women between the ages of 18-25 years were given the bivalent vaccine for hepatitis A as a control. During the last visit of the blinded 4-year study, 5,840 subjects gave oral specimens in order to evaluate vaccine efficacy (VE) against oral infections. The results demonstrated a VE of 93.3%. The authors theorized that if protection was seen in females the same should occur in males, and that this could be a primary preventative measure for HPV-related oral cancers.
HPV Detection
Regarding oral HPV detection, there currently are only two companies that provide oral HPV testing. Oral DNA Labs provides their service to only patients that visit their oral health practitioner. SelfCollect.com also provides oral HPV testing that is available to the public without having to visit the dental office. Keiko DNA Labs, a Seattle-based start-up, hopes to provide a more accurate diagnostic test using Real-Time PCR. All sampling methods from each company are non-invasive. HPV-associated OCC/OPC According to the Oral Cancer Foundation, there will be approximately 48,000 new cases of OCC/OPC annually, with a rate increase of >50% mortality rate each year globally [17,18]. Even with some improvements in scientific efforts and screening, the mortality rate of OCC remains high and the 5-year disease-free survival rate remains quite poor [19].
While HPV-associated OCCs are present, it is the HPV-associated OPCs that are more of a concern as studies have demonstrated HPV association from 30to>90% in OPC cases. Variation between studies results from a variety of factors such as sampling technique (ie. swab, brush, and oral rinse), method of detection (ie. PCR, real-time PCR), and differences in type of molecules being detected (ie. DNA, RNA, p16). The difficult aspect of HPV-associated cancer diagnosing is that transformation of HPV-infected cells to malignant lesion can take many years with little to no symptoms. Treatment of HPVassociated cancers usually consists of excision of tissues infected with malignancy along with chemotherapy or radiation therapy depending on the case.
Closing Remarks
Oral health practitioners have a plethora of items to discuss with their patients regarding basic oral hygiene care. However, HPV is definitely becoming a topic of conversation while visiting the dental office. Thus, when it comes to educating about oral HPV, take away items from this review are:
a) HPV is the #1 STI in the US
b) 90% of HPV infections clear within a few years
c) HPV vaccination is highly recommended for all pre-teens, and may be effective for HPV prevention in adults as well
d) Alcohol consumption, tobacco and marijuana usage, poor oral health, and sexual behaviors can increase risk of HPV infection
Identical Ovarian and Deep Pelvic Endometriosis with Colorectal Involvement in Monozygotic Twins: A Case Report and Review of the
Abstract
Endometriosis is a common benign gynecologic disease characterised by the presence of ectopic endometrial tissue outside the uterus. We present a brief review on the genetic factors underlying endometriosis, followed by a case report on concordant anatomical distribution of deep infiltrating endometriosis (DIE) in a pair of monozygotic (MZ) twins. To our knowledge, this is one of the first reported cases of DIE in MZ twins. The remarkable concordance and resemblance of deep disease involving the same anatomical sites, ovaries, pelvic floor and rectosigmoid colon in our MZ twins reiterates the role and impact of genetic factors in the pathogenesis of endometriosis.
Keywords: Deep Infiltrating Endometriosis; Sigmoid Resection; Monozygotic Twins; Genetics
Abbreviations MZ: Mono Zygotic; DZ: Di Zygotic; DIE : Deep Infiltrating Endometriosis; IVP: Intravenous Pyelogram; TVS: Transvaginal Ultrasound; RES: Rectal Endoscopic Sonography; SMM: Smooth Muscle Metaplasia
Introduction
Endometriosis is a polygenic multi factorial disease. Incidence of deep infiltrating endometriosis (DIE) involving the GI tract is estimated at 8-12% [1,2] and commonly involves the rectosigmoid colon. Endometriosis is one of the most common benign gynecologic diseases. It causes pelvic pain and sub fertility, and is characterised by the presence of ectopic endometrial tissue outside the uterus [3]. Endometriosis is under-diagnosed and associated with a mean latency of 6.7 years from onset of symptoms to definitive diagnosis [4]. Most estimates of prevalence are made on the basis of surgical cases or small samples, and are highly selective, ranging between 5% and 10% in women of reproductive age, and up to 50% among infertile women [5-7]. Endometriosis has an important socio-economic impact, because it greatly lowers quality of life for a significant portion of the population, and is responsible for substantial health expenditure, diagnosis, treatment, and loss of economic performance. The cost of endometriosis to the US health care system was $69.4 billion in 2009 [8]. Despite 150 years of hypothesis-driven research, the cause of endometriosis remains uncertain. Therapeutic options are therefore limited, often lacking unanimous consensus. However, there is mounting evidence that endometriosis is a complex multifactorial disease, with both genetic and environmental components contributing to disease susceptibility [7]. In 1980, Simpson et al. published the first formal genetic study of endometriosis [9]. Studying 123 probands with histologically proven endometriosis, they found that 5.9% of female siblings over the age of 18 years had endometriosis; the mothers were affected in 8.1% of cases.
However, only 1% of the patients’ husband’s first-degree relatives (controls) had the disease. Women with an affected sibling or parent were more likely to have a severe form of endometriosis [10]. Severe endometriosis was present in 61% of probands who had an affected first-degree relative, whereas it was only present in 23% of the affected probands with no affected first-degree relatives. One recent meta-analysis combining results from a genome-wide association study and replication studies showed that of the nine loci found to be associated with endometriosis in at least one of the studies, six remained statistically significant genome-wide, and two showed borderline statistically significantgenome-wide association with moderate/severe disease [11]. In an Australian twin-based study, a twofold increase in endometriosis risk in monozygotic (MZ) compared with dizygotic (DZ) twin pairs was reported [7], which suggests that the genetic component contributing to phenotypic variability in endometriosis is about 52%. These data imply that endometriosis is a complex genetic trait, and indicate that a number of genes interact with each other to form disease susceptibility, with the phenotype emerging in the presence of environmental risk factors which in themselves account for 53% of disease liability. Environmental chemicals, as well as food, have been discussed as possible contributing factors [12-14]. However, there is no existing evidence as to the nature of this environmental contribution. Only one study to date has used quantitative analysis to examine the contribution of genetic and environmental factors to endometriosis, using a small twin sample [7]. A larger twin sample is expected to provide further clarification on the role of genetic and environmental factors [12-14]. In this report, we present a case of deep infiltrating endometriosis (DIE) in a pair of monozygotic (MZ) twins.
Material and Method
A pair of monozygotic twins was referred to our office within the same year, mainly due to severe chronic pelvic pain and infertility, with the following pertinent clinical information.
a) Twin A : A 31-year-old nulliparous woman was admitted to Farmanieh Hospital (Tehran, Iran) complaining of heavy menstrual blood loss, progressive chronic severe pelvic pain and dyspareunia for the past six years, painful defecation with passage of narrow, occasionally blood-tinged stool, and history of failed hormonal medical treatment on and off during the past six years. The patient had been infertile for the past two years. She had a history of hypothyroidism, thalassemia minor, cervical spinal cord tumour surgery, rhinoplasty and eye surgery. Transvaginal ultrasound detected a 25 x 22mm cyst in the right ovary and two heterogeneous hypoechoic foci (32 x 21mm and 29 x 18mm respectively) in the left ovary; these observations were compatible with endometrioma. Colonoscopy results were negative. Hemoglobin level was 11.4g/dL, serum CA 125 level was 60.67U/mL, serum CA 19-9 level was 6.4 U/mL, and AMH level was 5.7ng/mL. Intravenous pyelogram (IVP) results were negative.Magnetic Resonance Imaging (MRI) revealed two T1 foci in both ovaries (25 x 15mm and 20 x 10mm high respectively), which was suggestive of a hemorrhagic cyst or, more probably, a dermoid cyst. No other pathology was noted, including for the intestinal tract.
b) Twin B: A 31-year-old nulliparous woman was admitted to Farmanieh Hospital (Tehran, Iran) complaining of menorrhagia, progressive severe pelvic pain with rectal radiation for six years, painful defecation with occasional blood-tinged stool, severe dyspareunia for the past two years and failed hormonal medical treatment for the past six years. She had a history of hypothyroidism, thalassemia minor, mitral valve prolapse rhinoplasty and eye surgery. Two transvaginal pelvic ultrasounds revealed a small anterior wall myoma; there were no other findings. Hemoglobin level was 10.8g/dL, serum CA 125 level was 21U/mL, serum CA 19-9 level was 9.4 U/mL, and AMG level was 7.4ng/mL. IVP results were within normal limits. MRI of the pelvis detected three small myomas (10-15mm) at the anterior uterine wall and a 20 mm follicle in the left ovary. There were no other findings, including for the bowel. Colonoscopy results were within normal limits. A double-contrast barium enema detected segmental luminal narrowing with upward displacement of the sigmoid area, with mucosal thinning. These findings suggested extrinsic pressure, mostly due to endometriosis, which seemed to have involved the posterior wall of the sigmoid colon.
Results
Twin A
A laparoscopic segmental sigmoid resection was performed, with staple re-anastomosis, resection of pelvic floor DIE, and resection of a bilateral endometrioma. The procedure took 152 minutes. The patient was discharged after four days shown in below Figure 1.
Figure 1: Laparoscopic images for Twin A. (A) Anterior uterine myoma, (B) Attached left adnexa to stenotic RS colon, (C) Left adnexal colonic adhesion, (D) Left ovarian endometrioma, (E) Right ovarian endometrioma, (F) Segmental resection of RS colon, (G) Resected bowel with deep endometriosis, (H) DIE pelvic floor,and (I) DIE at peritoneal site of invagination.
Twin B
Twin B’s initial procedure was performed in the same month as Twin A’s procedure. Laparoscopic adhesiolysis was performed, with resection of pelvic floor DIE, resection of ovarian endometrioma, and shaving of rectal deep endometriosis. Bowel resection was deferred because of inadequate bowel preparation, and laparoscopic sigmoid resection with staple anastomosis was performed 8 weeks after the initial procedure (Figure 2).
Figure 2: Laparoscopic images for Twin B. (A) Myoma at anterior uterine wall, (B) Left ovarian endometrioma severely attached to sigmoid colon, (C) Ovarian attachment to sigmoid colon, (D) Left ovarian endometriosis, (E) Right ovarian endometriosis, (F) Shaving DIE off rectal surface, (G) Defect at rectal surface, (H) DIE pelvic floor with rectal involvement, (I) DIE peritoneal site on invagination, right side, (J) Segmental resection of RS colon, (K) Resected bowel with undivided DIE nodule and (L) Resected bowel with divided DIE nodule.
Discussions
Anatomical involvement of the relevant pelvic organ in this pair of identical twins was nearly identical. The twins had grown up in the same environment all their lives, both worked as secretaries at the same institution, and both were experiencingnot only the symptoms of DIE, but also signs and symptoms of intestinal involvement. The ultrasound and MRI for both patients was reported negative, which clearly indicates the importance of experienced radiologists for the detection of deep endometriosis [15], and reiterates the importance of bimanual exam by clinicians, particularly at the time of menstruation, to achieve an accurate diagnosis,. In fact, available data clearly indicates that the accuracy of good physical examination (PE) is not much different from that of transvaginal ultrasound (TVS), rectal endoscopic sonography (RES) and MRI, all within the 80% range [16]. Twin A was managed by laparoscopic segmental sigmoid resection and staple reanastomosis, along with global resection of DIE from the pelvic floor and endometriomas. We were intending to do the same for Twin B, but in OR the lack of adequate bowel preparation was noted; thus bowel resection was postponed and was performed 8 weeks later under adequate bowel preparation.
However, after resection of endometriomas and pelvic floor deep lesions, larger DIE at the posterior cervix with extension to the rectum was managed by laparoscopic shaving, and the defect was closed in two layers. No intraoperative or postoperative complications were encountered in either twin. In many instances, the culprit for DIE is endometrioma, which starts from its peritoneal site of invagination (Figure 3). By extension medially, it involves the parametrium, rectum, recto-vaginal space, and, by deeper extension, the ureter and hypogastric nerve may also be involved. Thus, timely and proper surgical management of endometrioma and excision of its dependent peritoneal site could serve not only to manage patients’ pain, but also to conceivably prevent a significant percentage of DIE. In one study focusing exclusively on patients with rectosigmoid lesions, 48% and 84% had ovarian endometriosis and retrocervical lesions, respectively [17] (Figure 3).
Figure 3: Endometrioma and the peritoneal site of invagination.
Both superficial peritoneal and ovarian endometriomas may be found in association with DIE in variable percentages, thus contributing to the intensity of painful stimuli, as well as to infertility [18]. Thisraises the question of whether DIE is an independent form of the disease, or whether it represents its most severe clinical representation [19]. Nisolle and Donnez have argued that peritoneal endometriosis, ovarian endometriosis and adenomyotic nodules of the rectovaginal septum are three different entities [20]. In a retrospective observational study by Kamergorodsky [21]. Involving 176 patients and 271 biopsies, the histologic differentiation in superficial endometriosis, DIE and ovarian endometriomas was evaluated. Results showed a predominance of the undifferentiated glandular pattern (33.5%) and mixed glandular pattern (46.9%) in deeply infiltrating endometriosis lesions, whereas the welldifferentiated glandular pattern (41.8%) was most frequently seen in superficial endometriosis lesions, and in ovarian endometriomas a predominance of both the undifferentiated (40.5%) and mixed patterns (37.8%) was observed. There was no significant histologic difference between infiltrative endometriosis of the uteroscacral ligaments, recto-vaginal endometriosis, or bowel endometriosis. There was a predominance of the well-differentiated pattern in more superficial lesions and the undifferentiated pattern in deeper lesions, suggesting a similar mechanism to explain the invasive potential of endometriosis.
Recently, Sapkota [22] analysed genetic risk scores derived from two large European genome-wide association (GWA) datasets from a previous multi-ethnic GWA meta-analysis of endometriosis. They found that genetic factors contributing to minimal disease might differ from those contributing to more severe endometriosis, and that more severe endometriosis cases exhibit greater genetic loading than minimal or mild disease. The genetic burden generally increased from less severe (minimal) to more severe disease, consistent with disease progression. Considering the fact that endometriotic lesions undergo repeated cyclic bleeding (injury) and repair like other organs leading to fibrosis [23], it has been suggested that endometriotic lesions are fundamentally wounds with repeated tissue injury resulting in smooth muscle metaplasia(SMM) and ultimately fibrosis, which somehow do not heal like an ordinary wound [24]. This points to the complex microenvironment and cross-reaction of endometrioc lesions with other cells, i.e. platelets and macrophages, their gradual but progressive evolution to SMM and fibrosis and, on occasion, to malignancy and the new traits/phenotypes they may acquire while losing old ones. This dynamic feature of endometriotic lesions may explain the reason for some conflicting results in this area of research, including the fact that development of biomarkers for the diagnosis or prognosis of endometriosis has posed a challenge, at least until now.
Endometriosis appears to be a progressive disease, as evidenced by longitudinal laparoscopies in female baboons [25]. There are at least eight studies reported (with a total of 162 patients) on repeat laparoscopy in women assigned to placebo treatment. The results indicate nearly equal distribution among women whose disease stage deteriorated (31%), was unchanged (32%), or improved (38%). In fact, all but one study noted that 23% of placebo patients had complete regression of the disease over intervals of 4 to 39 months, meaning that in over two thirds of women the disease will either persist or progress [26-33]. The clinical presentation of the disease followed a similar trend and evolution in both of our cases. Each twin had undergone a long history of slowly progressive pelvic pain from the point of intensity, developing bowel symptoms and dyschesia as time passed, with dyspareunia and change in stool diameter to the point of bowel stenosis and impending obstruction. All of this is consistent with the progressive nature of the disease reported in the existing literature.
Deep infiltrating endometriosis, contrary to being an estrogendependent disease, usually does not respond well to hormonal suppressive therapy. Adequate surgical excision of the lesions provides the best long-term results and symptomatic relief [31- 34] but surgical treatment of colorectal endometriosis has been quite controversial, and there is no consensus on whether the treatment should be conservative (shaving or discoid resection) or radical (segmental bowel resection and anastomosis) [35]. Lately, there has been a great deal of effort to advocate shaving as the treatment of choice, mainly because of higher early and late complications in segmental colorectal resection [36]. The efficacy of segmental colorectal resection is very debatable; data in this regard is controversial and, to a great deal, dependent upon the surgeon’s experience [37,38]. Findings from histopathologic analysis of specimens from segmental bowel resection indicates that in 50% of cases there is a satellite lesion independent of the primary deep nodule.The deepest layer of the bowel wall containing endometrioticfoci at the primary lesion is in the submucosal layer in 70% of cases and the internal circular muscle layer in 30%. Furthermore, persistent lesions are present in 50% of patients treated with discoid or shaving resection [39]. The latest systematic review of different surgical approaches to bowel and rectovaginal endometriosis showed that the complication rate is variable for conservative and radical treatment. Recurrence rate for shaving was reported at 22.2%, for discoid resection 5.17%, and in segmental resection 2.19%; these rates were significantly different [37]. Positive bowel resection margins as well as age <31 years and body mass index ≥23kg/m2 appear to be important independent predictors of disease recurrence [40].
Our patients were managed according to the extent of their pathology, intensity of pelvic pain, and future fertility, thus minimising the chance of recurrence. Most importantly, patients’ wishes and decisions regarding the type of clinical management to be pursued were incorporated, following proper counselling and explanation. It is crucial to keep in mind that there is currently no scientifically proven best treatment technique for bowel endometriosis, and comparison of different currently practised techniques is not possible. According to our current knowledge regarding the nature of disease pathology and its progression, recurrence should be as much a source of concern as complications for any given surgical technique. Resection of DIE should be global, not local, and limited to the bowel. Operations should be performed by an experienced surgeon and a well-organised team, in a multidisciplinary fashion. In summary, we present a case of advanced DIE in monozygotic twins; one of the first such cases to our knowledge. Our findings reiterate the importance of genetic factors in the aetiology of endometriosis. These cases also reinforce the importance of the following considerations for surgeons considering conservative treatment for colorectal endometriosis:
a) The extent of lesions cannot be assessed macroscopically with certainty.
b) Assessment of the depth of infiltration of endometriosis foci in the bowel requires an expert radiologist.
c) In the majority of rectal endometriosis nodules, the fibrosis which is the landmark for shaving does not surround, but follows behind the glandular epithelium and stroma.
d) More than 2cm of bowel tissue must be removed from the main lesion to obtain clear margins in two thirds of patients.
e) Low rectal lesions (<5–8cm from the anal verge) are associated with a higher risk of complications.
f) A great majority of patients have been through previous surgeries and have a good chance of recovering and becoming pain-free.
Concentration Dependent Structural, Morphological and Optoelectronic Properties of Sprayed Cadmium Based Transparent Conducting Oxide
Abstract
The effect of precursor concentration on the physico-chemical properties of cadmium oxide (CdO] thin films deposited using simple and effective chemical spray pyrolysis technique (SPTJ is studied for the first time. The X-ray diffraction study shows polycrystalline, face centered cubic structure of CdO films. Field emission scanning electron micrographs and cross-sectional images of CdO thin films shows that morphology of films changes from rough to smooth and thickness of the films increases from 794 nm to 1523 nm, as cadmium content increased in spraying solution. X-ray photoelectron spectroscopy confirms presence of 4d, 4s, 3d5/2, 3d3/2, 3p3/2, 3p1/2 fine structural states of cadmium and 1s fine structure state of oxygen. The optical study shows that the direct band gap energy values decreases from 2.58 to 2.42 eV with increase in precursor concentration which is attributed to B-M effect. The Hall Effect measurement indicates that all the films exhibit n-type semiconducting behavior, the electrical resistivity decreases from 34.5 x 10-4 to 2.7 x 10-4 Ωcm for 0.025M to 0.1 M solution concentration and further increase to 12.5 x 10-4 Ωcm for 0.125 M concentration. The CdO thin film deposited with 0.1 M precursor concentration exhibits the best optoelectronics properties amongst the all other CdO films. It shows transmittance of 74 %, high figure of merit of 25.3 x 10-3 (Ω)-1, carrier concentration of 5.87 x 1020 /cm3 and mobility of 40 cm2/Vs. Photoluminescence spectra of CdO thin film gives two significant photoemission peaks at 434 and 539.80 nm (green) when they are excited at 400 nm wavelengths
The first report of a transparent conducting oxide (TCOJ was published in 1907, when Badeker reported that thin films of Cd metal deposited in a glow discharge chamber could be oxidized to become transparent while remaining electrically conducting. Since then, the commercial value of these thin films has been recognized, and the list of potential TCO materials has expanded to include, for example, Al-doped ZnO, CdSnO2, SnO2, F-doped In2O3, and many others. TCOs are an essential part of technologies that require both large-area electrical contact and optical access in the visible portion of the light spectrum. High transparency, combined with useful electrical conductivity (>103 Scm-1), is achieved by selecting a wide-band gap oxide. Most of the useful oxide-based materials are n-type semiconductors that ideally have a wide band gap (>2.5 eV], the ability to be doped to degeneracy, and a conduction-band shape (dictating electron effective mass] that ensures that the plasma- absorption edge lies in the infrared range [1].
August 2000 issue of MRS Bulletin is well timed to provide an overview of TCO, included articles cover the industrial perspective, new n-type materials [2] by Tadatsugu Minami, new p-type materials [3] by Hiroshi Kawazoe, Hiroshi Yanagi, Kazushige Ueda, and Hideo Hosono, novel deposition methods, applications and processing of transparent conducting oxides [4] by Brian G. Lewis and David C. Paine, and approaches to developing both an improved basic understanding of the materials themselves as well as models capable of predicting performance limits. There is a renewed interest in research on TCOs, mainly due to its numerous different properties and applications.
Cadmium Oxide (CdOJ is one of the promising TCO having high absorption in the order of 103 cm-1, high transmittance > 75 % , band gap of ~2.3 eV and high conductivity in the order of 104 S/m, made it applicable in photodiodes [5], phototransistors [6], photovoltaic cell [7], transparent electrodes [8], liquid crystal displays [9], UV detectors and UV-emitting diodes [10]. The properties of a TCO layer depend not only on its chemical composition, but also on the method used for its preparation. These preparative methods include physical methods (sputtering, evaporation, pulsed laser deposition) and chemical methods (chemical vapor deposition, sol-gel, and chemical bath deposition, electro-plating). There are number of physical and chemical techniques of thin film deposition. Amongst these various deposition techniques, the spray pyrolysis technique (SPT) is one of the chemical techniques which have many advantages compared to other chemical or physical technique such as low cost, easy to handle, easy doping, vacuum does not required at any stage, comparably more adherent films are formed in single step deposition and various properties of films can be tuned by varying the preparative parameters of the SPT, like substrate temperature, quantity of spraying solution, concentration of precursor solution, nozzle to substrate distance, spray rate etc. [11].
In our previous work [12], it is found that CdO films deposited at 350oC substrate temperature and quantity of 40 ml precursor solution with thickness of 1371 nm shows the best results like low resistivity of 3.7 x 10-4 Ωcm, high carrier concentration of 7.3 x 10 20 cm’3, mobility of 23.11 cm2/Vs and figure of merit of 18.23 Ω-1. There are very few reports on effect of concentration on various properties of TCO materials. Baneto et al. [13] reported the effect of precursor concentration on structural, morphological and opto- electric properties of ZnO thin films prepared by spray pyrolysis where it is revealed that morphology significantly depends on the precursor concentration, which is governed by nucleation and/or growth process. It is also verified that the optoelectrical properties of the films can be tuned by depositing films with proper precursor concentration. Effect of concentration of SnCl4 on different phsico- chemical, optical, electrical sprayed fluorine doped tin oxide thin films have been studied by Moholkar et al. [14].
Effect of ageing of the precursor solution on the structural, morphological, optical and electrical properties of ternary Cd ZnO thin films was studied by Balu et al. [15] where they have found that the Cd ZnO film prepared from 3 days aged precursor solution exhibit better surface morphology and the optical band gap decreased with increase in aging period of the starting solution which is attributed to quantum confinement effect. In one more report, Helen et al. [16] studied the influence of precursor concentration on the properties of spray deposited CdO thin films. It is found that the transmittance gets enhanced with increase in precursor concentration whereas the optical energy band gap value decreases from 2.50 eV to 2.37eV. Electrical studies revealed that the CdO thin film prepared using 0.15 M solution possesses lowest resistivity in the order of 10-4 Ωcm. So far there are no reports on the properties of sprayed CdO thin films in which effect of precursor concentration is studied. In the present investigation, CdO thin films have been deposited on glass substrate with different concentration of cadmium precursor solution by SPT and their structural, morphological, compositional, optical and electrical properties have been studied.
Experimental Details
CdO thin films were deposited by SPT as described in our previous report, using aqueous solution of cadmium acetate [(Cd (CH3COO)2] as a precursor with slight modifications [17]. The solution of 0.025 M to 0.125 M concentration Cd(CH3COO)2 [LobaChemie Pvt. Ltd. Mumbai, India] was prepared in double distilled water (DDW), and sprayed onto the preheated ultrasonically cleaned glass substrates at 350oC temperature and further allowed to cool at room temperature. The other parameters like quantity, substrate temperature, spray rate, nozzle to substrate distance were kept constant throughout this experiment. All the obtained films were appeared as faint yellowish in color, transparent, well adherent to the substrates and pinhole free. Such obtained films were further characterized by using various characterizing tools. The structural properties were studied by X-ray powder diffractometer [Bruker AXS, D2-Phaser, USA] using Cu Kα (λ. = 1.5406 Å) operated at 30 KV, 20 mA. The micro structural study was carried out using field emission scanning electron microscopy (FE-SEM) [Hitachi S – 4800, Japan]. The thickness of the thin films was obtained from the cross sectional FE-SEM images. Energy dispersive X-ray analysis (EDAX) connected with FE-SEM was carried for confirming elemental presence in deposited film. The fine structural states of cadmium and oxygen were obtained from XPS study [Kratos Analytical, ESCA 3400, UK] [18]. The transmission and optical absorption spectra were studied at room temperature within 400 – 800 nm wavelength range using UV-vis spectrophotometer [Shimadzu UV- 1800, Japan]. The room temperature electrical measurements were carried out with Hall Effect set up in van-der Pauw configuration [SES Instruments, Roorkee, India]. The photoluminescence spectra were recorded using spectrofluorometer [Fluromax – 4, Japan].
Results And Discussion
Go to
X-Ray Diffraction (Xrd) Study
The XRD patterns of0.025 M, 0.05 M, 0.075 M, 0.1 M and 0.125 M CdO thin films deposited at 350oC substrate temperature is shown in (Figure 1). All CdO thin films prepared with different precursor concentrations shows good match with pure CdO film when compared with JCPDS card number 01-075-0592 [18]. Three major peaks corresponding to (111), (200) and (220) planes obtained in XRD pattern, represents the polycrystalline face centered cubic structure of the CdO thin films. Along with these peaks, two minor peaks corresponding to (311) and (222) planes are also observed. The crystallite size is estimated using the Scherrer’s formula [19].
Figure 1: XRD patterns of 0.025 M – 0.125 M CdO films deposited at 350 oC substrate Temperature.
The average crystallite size obtained for 0.025 M, 0.05 M, 0.075 M, 0.1 M and 0.125 M CdO thin films from XRD data are 18.72 nm, 33.60 nm, 25.17 nm, 35.75 nm and 26.50 nm respectively. This variation in crystallite size can be correlated to the increased cadmium content in film with increase in concentration as well as to the increased thickness [20]. Though the concentration increases the location of the diffraction peaks does not change significantly but the XRD intensity strongly varies with the concentrations of cadmium precursor solution. The initial increase in the XRD peaks for CdO thin film can be explained by the creation of new nucleation centers due to the Cd atoms.
The subsequent decrease in the XRD peak intensities for higher concentration can be described by two factors; firstly, by the saturation of the newer nucleation centers and secondly, due to the change of the energy absorption at the time of collision, and of the physical and chemical interaction between ad-atoms and the film. The decrease in crystallite size to 23.61 nm for 0.125 M CdO film is due to the saturation of cadmium in the film for higher concentration [21]. The crystallites in a polycrystalline material normally have a crystallographic orientation different from that of its neighbors. The preferred orientation of the films is described by texture coefficient (TC), which is evaluated from equation [22],
The calculated TC values are depicted in Table 1, from the measured TC values, it is clear that all films have preferential orientation along (111) and (200) planes as the TC values calculated for these planes are greater than one. It is observed that the peak intensity along (111) and (200) plane of the film enhances when concentration of solution is increased from 0.025 M – 0.1M and the peak intensity decreased for 0.125 M CdO film it may be due to saturation of cadmium at this high concentration in film.
Table 1: The values of 20, (hkl), TC, a, e, D and 8 for sprayed CdO thin films with different cadmium acetate concentration deposited at 350 0C.
The lattice constants obtained corresponding to different planes is ~4.68 Å and standard lattice constant of CdO is 4.69 Å, it means that the compressive strain is present in the deposited films. The strain in the CdO film is determined using the equation [23].
The average strain in the film is obtained by taking slope of a graph of (βcosθ)/λ Vs sinθ/λ. (Figure 2) shows such a graph of 0.1 M CdO thin film. It is seen in that all the points do not lie on a linear fitted straight line which represents that strain is present in the CdO film and it is 1.95 x 10-2 in 0.1 M CdO thin film. The average strain evaluated for all other CdO films are depicted in Table 1, it varies nonlinearly between 1.66 x 10-2 – 2.56 x 10-2. The initial increase in the strain with increase in precursor concentration may be due to change in crystallite size which influences the grain boundaries (Figure 3).
Figure 2: Williamson- Hall (W-H) plot of 0.1 M CdO film, for strain broadening.
Figure 3: Typical NRF plot to determine lattice constant of 0.1 M CdO film deposited at 350 oC using spraying solution quantity of 40 ml.
The dislocation density (δ), defined as the length of dislocation lines per unit volume, which varies with crystallite size ‘D’, has been estimated using the equation [24].
The lesser values of ‘δ’ obtained 0.782 x 1015 lines /m2 for the 0.1 M CdO thin films indicate and confirms the degree of crystallization is higher for it the dislocation density of other CdO films depicted in (Table 1). The values Braggs angle (2θ), Miller indices (hkl), texture coefficient (TC), lattice constant (a), strain (εs), crystallite size (D) and dislocation density (δ) of all the deposited CdO thin films are presented in (Table 1)
Surface Morphology Study
Figure 4: (a-e) Surface and cross-sectional FE-SEM images of CdO thin films deposited for 0.025M – 0.125 M precursor concentrations at 350 oC substrate temperatures.
Figure 4 shows the surface and cross-sectional FE-SEM images of CdO thin films prepared using 0.025 M to 0.125 M concentration of spraying solution 40 ml deposited at 350 oC substrate temperature. It is observed that all the films are, dense and strongly adherent to the substrates. The film deposited at 350 oC and precursor concentration of 0.025 M shows random arrangement of irregular shaped grain like structure which may be due to insufficient concentration of precursor solution concentration. The grains are well connected with very few voids. The thickness of 0.025 M CdO film is 794 nm. The micrograph of 0.05 M CdO film shows improvement in grain size and growth of film, it may be with increase in precursor solution concentration more nucleation centers are available for film growth, dumbbell like structure is seen, the thickness of the film observed is 997 nm. It has proper and well managed arrangement of larger grains having relatively less voids. The film deposited with 0.075 M has thickness of 1005 nm and it is observed that the grains are get agglomerated to form somewhat like spherical clusters and few voids are also seen in this film. With the further increase in concentration the void free continuous smooth film surface is obtained for 0.1 M CdO film, and thickness increased to 1371 nm.
Finally the film deposited at 0.125 M shows very compact surface morphology, the film nature is very compact and densely packed , no voids are seen all the surface of the film it may be due to the cadmium content in solution increases and saturated over the surface. The thickness of the 0.125 M CdO film is 1523 nm. This type of nature can be further ascribed to better crystallinity, low disordering into film structure [25]. The film thickness is found to be increased with increase in concentration of spraying solution from 0.025 M to 0.125 M which may be due to increased growth rate due to availability of more nucleation sites, also as with increase in concentration of precursor solution cadmium content increases which promotes the coalesce process.
Figure 5 shows the EDAX spectra of typical 0.1 M CdO thin film deposited at 350 oC substrate temperatures. From EDAX spectra, the presence of Cd and O elements in deposited CdO film is confirmed and their atomic percentages are found to be 58.23 at.% and 41.77 at.% respectively, indicating that the CdO thin films are sub-stoichiometry which leads to the semiconducting behavior and increase in carrier concentration of the CdO films. The typical EDAX spectrum shows CdO film is oxygen deficient which is one of the reason for improved electrical conductivity of the films.
Figure 5: EDAX of typical 0.1 M CdO thin film deposited at 350 oC substrate temperature using spraying solution quantity of 40 ml.
X-Ray Photoelectron Spectroscopy (Xps) Study
The XPS measurements is carried out for identifying the elements and their stoichiometry in the film, survey scan spectra of CdO film and narrow scan spectra of Cd and O are recorded separately for quantitative analysis and to identify the oxidation states of the Cd and O. Survey and detailed scan XPS spectra for Cd 3d, O 1s of 0.1 M CdO thin film deposited at 350oC substrate temperature shown in (Figure 6) It shows various peaks belonging to Cd, O, C and Auger electron transitions. Along with it various satellite peaks corresponding to other elements are also observed.
Figure 6: X-ray photoelectron spectroscopy (XPS) (a) survey scans of 0.1 M CdO thin film (b) Narrow scan XPS spectrum of 3d core level of cadmium in 0.1 M CdO thin film (c) Narrow scan XPS spectrum of oxygen in 0.1 M CdO thin Film.
Photoelectron peaks observed at 10.4, 108.3, 404.5, 411.3, 618.1 and 651.6 eV correspond to 4d, 4s, 3d5/2, 3d3/2, 3p3/2, 3p1/2 fine structure states of Cd, respectively, whereas peaks at 772 and 976.5 belongs to the Auger electron peaks of Cd and O, respectively Along with this, peak at binding energy 285.15 eV is 1s core level of carbon [26]. The presence of carbon is due to contamination which resulted from the film handling and exposing to air before the XPS measurement. Peak at 531.5 eV is attributed to the oxygen 1s fine structure state. Except s state p, d, f states splits into the doublet which is due to the presence of electrons with different spin-orbit coupling that have different binding energies indicating different fine structure states. Narrow scan XPS spectrum of the 3d core level of Cd is shown in (Figure 6). Electron orbit splitting of core level into doublet is due to spin orbit coupling of electrons. Observed spectrum is deconvoluted into two doublets lying at different energy levels. Two doublets belong to the two different chemical states of the Cd viz. Cd+1 and Cd+2. Intense doublet lying at 406.5 and 413.3 eV corresponds to the 3d5/2 and 3d3/2 core levels of Cd due to the Cd+2 chemical state. Photoelectron peaks lying at binding energy 405.0 and 411.7 eV corresponding 3d5/2 and 3d3/2 core levels of Cd due to the Cd+1 chemical state.
Area under the curve determines concentration of the corresponding chemical state of the element. Thus it could be concluded that the concentration of the Cd+1 valence state is less as compared with the Cd+2 states. Doublet separation of the peaks for both the doubles match well with the reported values. The area under the curve is measured, and the ratio of the 3d5/2 and 3d3/2 is calculated to be 0.65 which is agreeing well with the theoretical value 0.66 for the ratio of 3d doublet. Ratio of Cd+1 and O+2 chemical states present in the film observed is 0.38. Presence of Cd in Cd+1 state confirms oxygen deficiency which is responsible for the better electrical conductivity of CdO thin films which is also seen in resistivity measurements.
Peak full width at half maximum (FWHM) provides important information about the lifetime of the photoemission process and also about the chemical state of the elements. It is the energy broadening AE called lifetime broadening which is different for different spin orbit coupling. Narrow scan XPS spectrum of oxygen is shown in (Figure 6c) which is deconvoluted into a quadruplet with energy values 532.5, 531.5, 528.28 and 533.4 eV. Most intense peak lying at 531.5 eV binding energy level is due to the oxygen bonded to Cd and that at other binding energy level is due to the presence of adsorbed water on the film surface due to exposing films to environment
Optical Properties
The optical characterization of 0.025 M to 0.125 M CdO thin films is done using UV-Visible spectroscopy at room temperature in the wavelength range of 200 nm to 800 nm. The absorbance spectra recorded is shown in Figure 7(a) and typical transmittance of 0.1 M CdO thin film is shown in Figure 7(b). The maximum transmittance of 74 % and relatively higher absorbance of 1.8 cm-1 at 550 nm is observed for 0.1 M CdO thin film. The direct optical band gap energy values are calculated for 0.025 M – 0.125 M CdO thin films by extrapolating linear portion of the graph of (αhν)2 νs. (hv) on hv axis at α =0 as shown in (Figure 8). The values of direct band gap decreases from 2.58 eV to 2.42 eV for CdO films deposited at 0.025 M to 0.125 M concentrations, and are depicted in (Table 2).
Figure 7: Absorbance of 0.025 M – 0.125 M CdO films and Transmittance of typical 0.1 M CdO film deposited at 350 oC using spraying solution quantity of 40 ml.
Figure 8: The plots of (αhν)2 Vs hν of 0.025 M – 0.125 M CdO thin films deposited at substrate temperature of 350 oC using spraying solution quantity of 40 ml.
Table 2: The values of sheet resistance (Rs), thickness (t), transmittance (T), figure of merit (ϕ), resistivity (ρ), carrier concentration (n), mobility (μ), Fermi energy (EF), IR reflectivity ( IR) and effective length (l) of 0.025 – 0.125 M CdO films.
The 0.025 M CdO film has maximum band gap energy value of 2.58 eV, amongst all other CdO films and further Eg decreases with increase in precursor concentration to 2.42 eV for 0.125 M CdO thin film which can be attributed to higher carrier concentration due to which absorption of the light by the carriers increases, leading to the higher absorption coefficient (a) in the 0.125 M CdO film as well as the decrease in Eg is attributed to the incorporation of some impurity energy levels in the forbidden energy gap of the CdO caused by the incomplete thermal decomposition of Cd (OH)2 precipitation collected on the surface of the substrate for the films coated with higher solution concentration.
The obtained results are similar to the results reported by Prathap et al. [27] who have reported that the Eg decreases as the molarity of In2O3: Mo films increases prepared using SPT Theoretically, the increase in carrier concentration in degenerate semiconductors causes two opposite effects, namely the band gap widening (BGW) and band gap narrowing (BGN). The BGW was explained by Moss-Burstein (B-M) effect, which stated that all characteristic energies including the optical absorption edge of a degenerate n-type semiconductor is shifted towards higher energy by amount proportional to the increase in electron density in the conduction band through the following relation
The theoretical calculated value of
However, in the present work the Eg is inversely proportional to ‘n’. Therefore, the BGN plays the major role in explanation of the present results due to the high density of carriers (n > 1019 cm-3). The BGN is consisting of two parts. The first part of the bandgap shrinkage arises due to the electron-impurity interaction leading to band tailing and described for degenerate semiconductor with parabolic band approximation by the following relation [28,29]
Where ‘ћ’ is the Planck’s constant and is the ratio for of reduced effective mass to free-electron mass, which is equal to 0.274 for pure CdO. Therefore, the value of the coefficient is sbgn = 4.49X10-15eVcm2 . It is seen in Figure 9(a) the s1bon in present case obtained is 3.07 x 10-15 eVcm2 which is close to the theoretical value.
Figure 9: Plot of Eg – Ego Vs n2/3 and optoelectronic function for CdO film.
The second part of BGN results from the Columbic interaction (C-int) between carriers and is given by [29]
where εo is the permittivity of free space, e is the electronic charge, and εr is the dielectric constant . Thus
Therefore, the total BGN is equal to
The bandgap shift can be determined mainly by the BGN effects, as
Where Cf is a fitting parameter The plot of
The difference might come from the non-parabolic band effects [29] The IR reflectivity is one of the main requirements for a high quality solar window material. The efficiency of flat collector reduces considerably because of the escape of the thermal energy in the form of IR radiation the TCO having high reflectivity can be used to overcome this difficulty the IR reflectivity is calculated using relation [14].
The value of 1/εo co= 376 Ω the free space impedance the reflectivity of the film oscillates over 94 – 96 % and this is along with good transmittance suggest that films are used in window layer in solar cell, in different optoelectronic devices like in flat panel displays, collectors photo thermal conversion and work electrode in electrode position processes. The IR reflectivity obtained by using above relation for 0.025 M – 0.125 M CdO thin films are 65.95 %, 94.79 %, 95.98 %, 97.97 % and 91.82 % .The highest reflectivity of 97.97 % obtained for 0.1 M CdO thin film, make it suitable candidate for applications in heat reflecting mirrors.
Fermi energy and mean free path
The degeneracy of the films confirmed by evaluation of Fermi energy using formula [14]
Where m* is the value of effective mass = 0.21 me in case of CdO. The degeneracy can be confirmed by comparing values of EF with kT if Ef >> kT , it means films are degenerate. Secondly by plotting graph of EF Vs n, if the graph is linear the semiconductor is degenerate. Figure 10 shows the plot of Fermi energy (EF) Vs carrier concentration (n) for CdO film which is straight line it means the CdO has degenerate semiconducting nature.
Figure 10: Typical plot of EF Vs n to determine degeneracy of CdO film material for all the CdO films prepared with different concentration.
The free path in TCO film may interact with different scattering centers like thermal vibration of the lattice, ionized and neutral impurities and the grain boundary regions. For degenerate semiconductor the ionized impurity and grain boundary scattering are important than the scattering by neutral impurity. If there is mismatch between the mean free path and the crystallite size it means that the grain boundary scattering is not dominant mechanism, in that case the other scattering mechanism like lattice scattering, impurity scattering mechanisms are more dominant which affect the electrical conductivity. The mean free path is calculated by using following formula [14].
Where symbols have usual meaning. The calculated values of T are depicted in (Table 2). In case of CdO film deposited with various concentrations of 0.025 M to 0.125 M at 350 oC substrate temperature, the calculated values of mean free length for 0.05 M, 0.075 M and 0.125 M CdO film are nearly matches with the crystallite size given in (Table 1), therefore, it is concluded that the grain boundary scattering is dominant phenomenon for obtained mobility values whereas in 0.025 M and 0.1 M CdO films the lattice scattering, impurity scattering are dominant phenomenon.
Another important scattering mechanism responsible for electrical properties is ionized impurity scattering which can be checked by calculating and comparing the mobility values experimentally obtained with the mobilities of ionized impurity [14].
It is observed that there is much difference in the experimentally obtained mobility values of CdO film and calculated mobility values using above relation, therefore, it is concluded that the ionized impurity scattering is not dominant phenomenon in present case. The values of experimental and calculated mobilities are depicted in (Table 2).
Electrical properties
The variation of electrical resistivity (ρ), carrier concentration (n) and mobility (μ) of 0.025 M to 0.125 M CdO thin films measured at room temperature by four point probe Hall method in standard van der Pauw configuration is presented in (Table 2). The resistivity decreases from 34.5 x 10-4 to 1.25 x 10-4 Ωcm with increase in precursor concentration for 0.025 M to 0.125 M CdO film. The decrement in the electrical resistivity of the CdO thin films with the increase in concentration of precursor concentration is due to increment in crystallinity, enhancement in carrier concentration and mobility of charge carriers. It is well known that the nature of defects and grain boundaries of different thin films are strongly dependent on the crystal quality.
The defects and grain boundary acts as free electron trap centers, which reduces the charge carrier concentration and become scattering centers, leading to a decrease in electrical mobility. These reported values of resistivity are very small compared to the results obtained for CdO thin films obtained by various physical and chemical methods [28-30]. (Figure 11) shows the variation of carrier concentration and mobility for 0.025 M to 0.125 M CdO thin films deposited at 350oC substrate temperature.
Figure 11: The variation of carrier concentration and mobility of CdO films deposited at 350 oC for 0.025 M – 0.125 M precursor concentrations.
From the point of view of application of transparent conducting oxide in optoelectronic devices, figure of merit (Ф) is one of the important parameter, which is calculated from well known Haackes formula [31]. The figure of merit (Ф) for 0.1 M CdO is the highest compared to the reported value of Ф for CdO thin films prepared by various chemical and physical thin film deposition technique, in this study it is 25.3 x 10-3 (Ω)-1. It is observed that figure of merit increases with increase in concentration up to 0.1 M CdO thin film and then decreases due to increase in sheet resistance and increase in crystallite size as shown in (Figure 12). The sheet resistance (Rs), thickness (t), transmittance (T), figure of merit (Ф), resistivity (ρ), carrier concentration (n), mobility (μ), Fermi energy (EF), IR reflectivity (R), and free path length (l) are presented in (Table 2).
Figure 12: The variation of figure of merit ® and R s of 0.025M – 0.125M CdO thin films deposited at 350 oC substrate temperature.
Photoluminescence study
(Figure 13) shows the room temperature PL spectra of CdO thin films deposited with different precursor concentration. Two emission peaks at 434 nm and 539.80 nm (green) are observed significantly for 0.075 M and 0.1 M CdO thin films when films are excited at 400 nm wavelength which is due to the combination of electron and hole from the conduction and valance band whereas for 0.025 M and 0.05 M CdO film the peaks are observed at 429.34 and 535.44 nm wavelength of which intensity is less due their high band gap energy. The peak at 539.8 nm arises due to the oxygen vacancies in CdO thin films; because photo generated holes in valence band recombine with an electron in conduction band [32].
Figure 13: PL spectra of CdO films of 0.025 M-0.125 M precursor concentrations deposited at 350 oC substrate temperature.
Conclusion
CdO thin films have been deposited on glass substrate with different concentration of cadmium precursor solution by SPT. It is noteworthy that the concentration of precursor solution plays an important role in changing the properties of CdO thin films. The XRD study reveal that all the CdO films are polycrystalline face centered cubic in nature, textured along (111) and (200) planes, minimum value of strain 1.95 x 10-3 and dislocation density 0.785 x 1015 lines /m2 confirms high degree of crystallization present for 0. 1.M CdO film. Surface morphology of films changed from rough to smooth and thickness of the films increases from 794 nm to 1523 nm, as cadmium content increased with concentration of spraying solution. Presence of Cd in Cd+1 state confirms oxygen deficiency which is responsible for the better electrical conductivity of CdO thin films. The optical direct band gap decreases from 2.58 eV to 2.42 eV with increase in precursor concentration is due to BGN related to M-B shift. The highest reflectivity of 97.97 % obtained for 0.1 M CdO thin film, make it suitable candidate for applications in heat reflecting mirrors. All the CdO films show n-type semiconducting behavior with electrical resistivity lies in the range of 34.5 x 10-4 to 2.7 x 10-4 Ωcm. The film deposited of 0.1 M concentration exhibits the highest figure of merit 25.3 x 10-3 (Ω)-1, carrier concentration of 5.87 x 1020 /cm3 and mobility of 40 cm/Vs. Two photoemission wavelengths are observed at 434 and 539.80 nm when excited at 400nm wavelength. These improved electrical parameters of films make them useful in optoelectronic applications.
Ecological and Economic Importance of Mulching Within the Urban Areas of Large Cities of the Republic of Serbia
Abstract
This paper indicates the advantages of using mulching in conditions of real exploitation in difficult terrain within the city area in the Republic of Serbia. The work was written to include impacts on specific ecosystems within cities, which are generally very heavy: burdened by passing a large number of vehicles, pedestrians, a large number of different stepping, and the influence of salting in the winter provision of transport and the impact of drought in the summer. The authors point out that the mulching observation was done basically with the economic aspect. In addition, it can be noted that there are numerous benefits of mulching which are underutilized in the real exploitation so far. On the narrow spaces, which are generally long, a few hundred meters to several kilometers, that are actually dividing strip, green islands has been raised over the past decade. In these conditions the application of machinery is difficult, and the entire processing is handmade. One of the models of problem solving is the application of mulching that fully meets the ecological and economic principles of management of public lands. The implementation of such an approach would mean reducing allocations taxpayers, and the results do not harm the ecological principles, but on the contrary, it would have positive impact on the areas of green spaces within cities.
Keywords: Mulch; The Economic and ecological impact; Urban surfaces
Introduction
Local governments and cities of the Republic of Serbia must develop the ecological-economic approach especially as imminent actual convergence of the Republic of Serbia with the EU countries. In the context of real convergence with the EU, the Ministry of Agriculture and Environmental Protection of the Republic of Serbia in recent years has made a large number of laws and decrees ordering the application of the greening of large urban areas while preserving the already planted green areas of cities. In order to perform these tasks with great appreciation spending funds taxpayers, cities must implement positive solutions to addressing the issues of ecology and economy. In this paper the authors have tried to find some answers, with the main purpose to broad population enjoys the benefits of the application of mulching. Mulching land, especially in the cities has advantages over passive observation of deterioration of green areas of cities or maintaining those with considerable financial allocations.
Material and Method
To make this work the authors used the documents public company founded by the city of Novi Sad. It has been operating in the market of Novi Sad and wider since 24.11.1962. Last bringing into line organization is done on the basis of the Decision of the City of Novi Sad, which was published in the Official Journal of the City of Novi Sad number 29/2005 and 53/2008 [1,2]. The survey was conducted in a representative and prestigious company with decade’s reputation and with more than 400 full-time employees. This company is the second largest in the Republic of Serbia for landscaping, maintenance of green areas and other activities related to agriculture and ecology. Specificity maintenance of green areas in cities, especially in narrow areas is exceptional. There must be met by numerous factors such as: the visual experience for residents and visitors to the city, it is extremely difficult to do all agronomic operations because of the narrow space, difficult work processing operations of green spaces, because it must be provided leeway traffic, and there are great citizens’ trampling green spaces.
Multidisciplinary approach for proper functioning of specific green spaces in cities, and green islands that are raised in large cities boulevards essentially begins with recognition of specific space [1,3]. In such difficult raise conditions the green areas that need to have multiple effects on users must be taken of the methods that will be applied. Authors gave the results of research which included the period 2012-2014 by applying the classical methodsof planting, mulching, and application of green areas, especially those which were planted perennial shrubs and short ornamental trees. In the classical model of raising seedlings on green islands we see many impacts of degradation, such as stepping on the soil, the irreversible removal of fertile surface layer during washing streets, the accumulation of snow on the green island with a large amount of salt, etc. For these reasons, it must be accessible to a different approach to try to somehow reduce part or most of the negative impact on the green island boulevards and other urban spaces. In this paper, the authors tried to answer some questions related to the degradation of these urban areas, i.e. erosion and reduction primarily surface layer of green area [4], using mulching on such spaces.
The point of all of these activities should be protecting of the surface layer of newly built green islands cities, and to better respond the ecological, visual experience of city dwellers, on the other hand these activities reduce costs taxpayers local communities and cities. Ecological approach is one of the primary in achieving humane life in big cities, and in order to approach full capacity it must include the science of marketing [5,6], which will long-term accompany any activity and with striking acceptable image at wide population [7-10]. In addition respecting the marketing [11] which will primarily explain to the citizens the significance of introducing new environmentally acceptable models for the community, and observation of socio-economic conditions [12] in which citizens live big cities is necessary. The application of the new mulching model in difficult environmental conditions for plants, as well as by demanding conditions for raising and maintenance of plant species in the cities, builds on previous research that includes a minimum investment of taxpayers with satisfactory effects [13,14].
Results
Authors of this paper showed the survey based on a standard approach with raising green islands in the urban areas and boulevards in the big cities of the Republic of Serbia, and at the same time showing the possible results of the introduction of models that includes mulching space between the planted plants. (Tables 1,2) the authors present their research classical model and the planting and maintenance of urban areas with the use of mulching.
Table 1: The conventional method of planting and maintenance after the first year of vegetation numerical values for green islands in the cities or partial lane roads shrubs to 2000m in length, width 0.5m, respectively 1000 m2 in the big cities of the Republic of Serbia.
Table 2: The method of planting with the use of mulching and maintenance after the first year of vegetation is shown in green islands in the cities, or dispensing lane roads shrubs at 2000m in length, width 0.5m, respectively 1000 m2 in the big cities of the Republic of Serbia.
Explanation of Tables:
A = The value of average seedlings with the proposed structure of 80:20 (240 pieces sawmills: 40 pieces of evergreen species) planting in favor of sawmills in euro’s
B = the required amount of topsoil 40 cm/value in euro’s
C = Transportation 4m3 country at a distance up to 12 km by truck to 8 tons in euro’s
D = the cost of land clearing, weeding, planning, leveling, digging by hand and others in euro’s
E = Works by manipulating the country when planting in euro’s
F = the cost of planting in euro’s
G = Total cost of planting by the norms of a public company until it is collected by the local government in euro’s
Source: Author’s calculation Table 2.
Results authors which were obtained are given in the table view 3rd (Table 3).
Table 3: Economic comparison of the classic ways of planting and maintenance of green islands towns and models that apply mulch to maintain the city’s specific surface area of 1000m2 in the big cities of the Republic of Serbia.
Explanation of Tables:
A= The value of average seedlings with the proposed structure of 80:20 (240 pieces sawmills: 40 pieces of evergreen species) planting in favor of sawmills in euro’s.
B= The required amount of topsoil 40 cm/value in euro’s.
C= Transportation 4m3 country at a distance up to 12 km by truck to 8 tons in euro’s.
D= The cost of land clearing, weeding, planning, leveling, digging by hand and others in euro’s.
E= Works by manipulating the country when planting in euro’s.
F= The cost of planting in euro’s.
G= Total cost of planting by the norms of a public company until it is collected by the local government in euro’s.
In this paper recalculating the average value of planting and maintenance of greenery with the use of mulching in the Republic of Serbia, as, were performed at the mean rate of the National Bank of the Republic of Serbia as of 05/12/201, compared to EUR 1 = 123.17 dinars.
Discussions
There is a constant need for innovation of existing models of raising green areas, with the main purpose to improve the heterogeneous conditions of people’s lives in cities.
a. Using the mulching model to a better and environmentally sound manner with small investment, we achieve better results in growing the desired plant species after planting (up to 50%).
b. Citizens much less trampling and destroying perennial vegetation planted on green urban islands which raises the visual experience of inhabitants, less investments in restoration of plantation while reducing expenditures land of the upper layer and up to 100% compared to the classic model of planting and maintenance of the mentioned area.
c. Applying mulching model the plants are better able to withstand the accumulation of snow mixed with a large amount of salt, reducing the need for replacement of topsoil every few years.
d. Both models represents the cost for local government and cities in Serbia, except that the mulching model is about 55% cheaper for taxpayers cities, while achieve better ecological and psychological effects on citizens.
e. According to the classical model of greening green urban islands on boulevards and other narrow places per m² costs taxpayers about 3 €, while using the mulching per m² costs about 2 €, which represents a decrease of about 52%.
f. In the cities there is a need for continuous landscaping all narrower and more difficult terrain, which requires additional expenses related to greening and maintenance, the needs are continuously growing and increasing, therefore there is a need for the use of new models which give better results. One such model authors presented through the use of mulching models in areas of cities.
Conclusions
This paper was created at the beginning of 2015, after years of research and real use of mulching models during the planting and maintenance of plant species in difficult terrain in cities in the Republic of Serbia. The authors provided realistic representations of the advantages of this model, based on the real exploitation mulching models compared to the classic model of raising greenery in cities. Just some of the advantages of using this model are shown. Raising the greenery inside the cities is the cost for local government, but also the obligation to the citizens. In this context it is important to find the optimum balance between the desires for ecological approach greening difficult urban terrain, but also the economy of costs, and the authors tried to show the real benefits of mulching compared to standard greening, primarily on the boulevards of cities. The application of the mulching is ecological and economically justified, and from the standpoint of saving by using mulching, we save about 50% of funds per m². The application of the mulching is possible on different grounds, as well as in different countries, and the whole model is based on ecological principles that have a positive impact on soil and ecosystems suffer major environmental impacts.
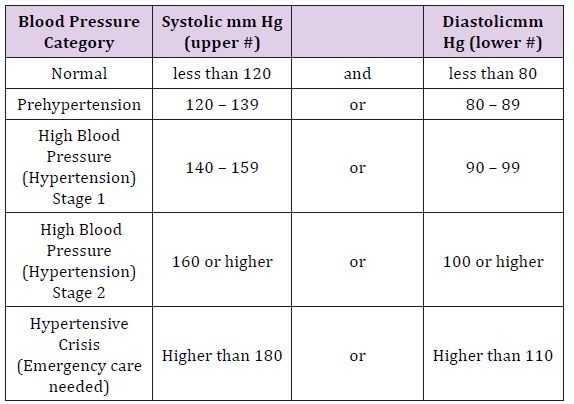
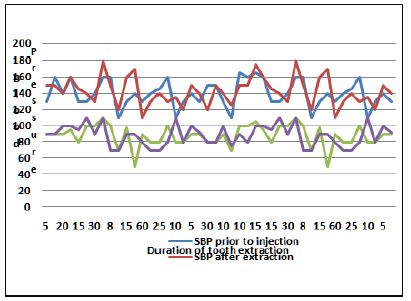
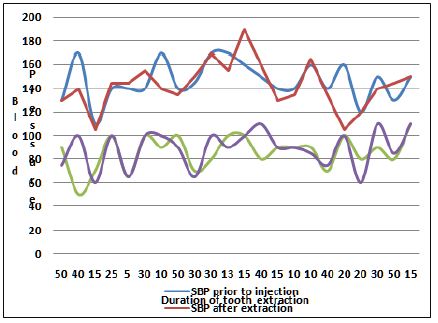
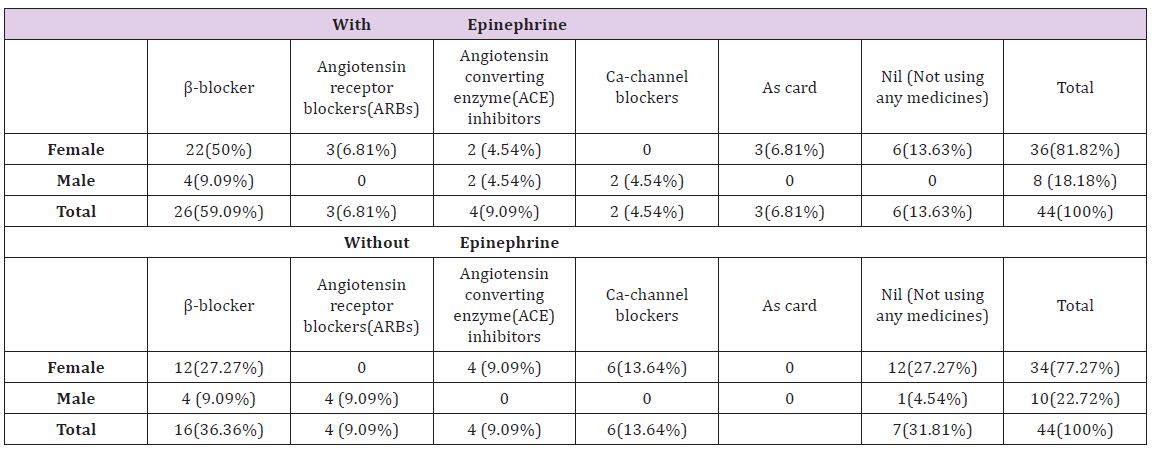
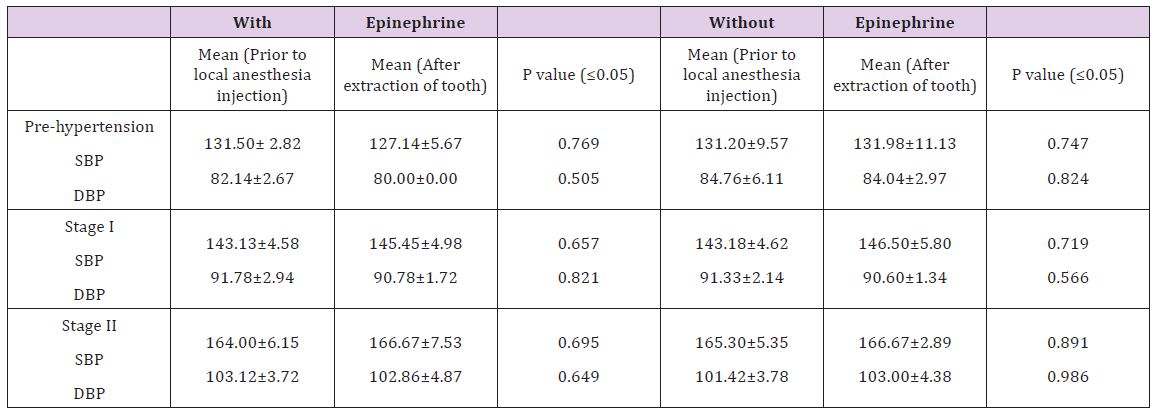















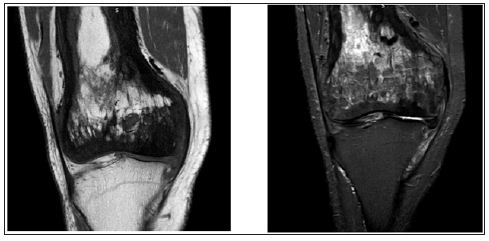

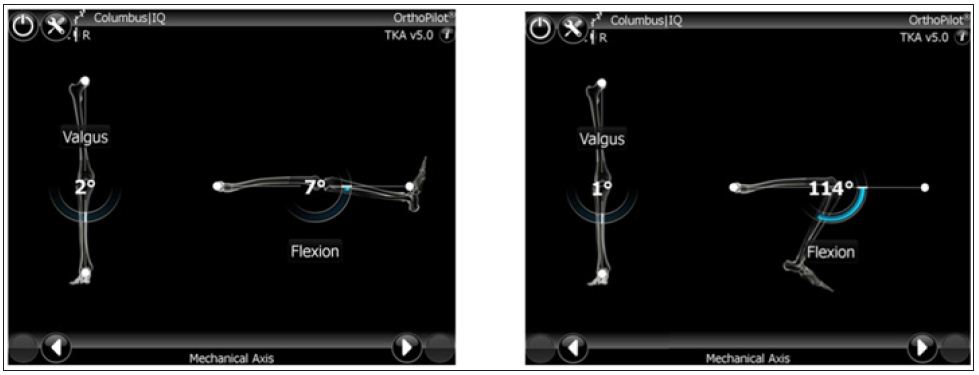


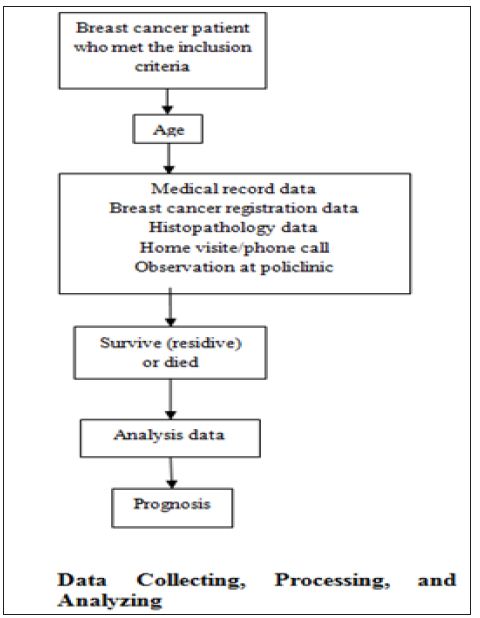
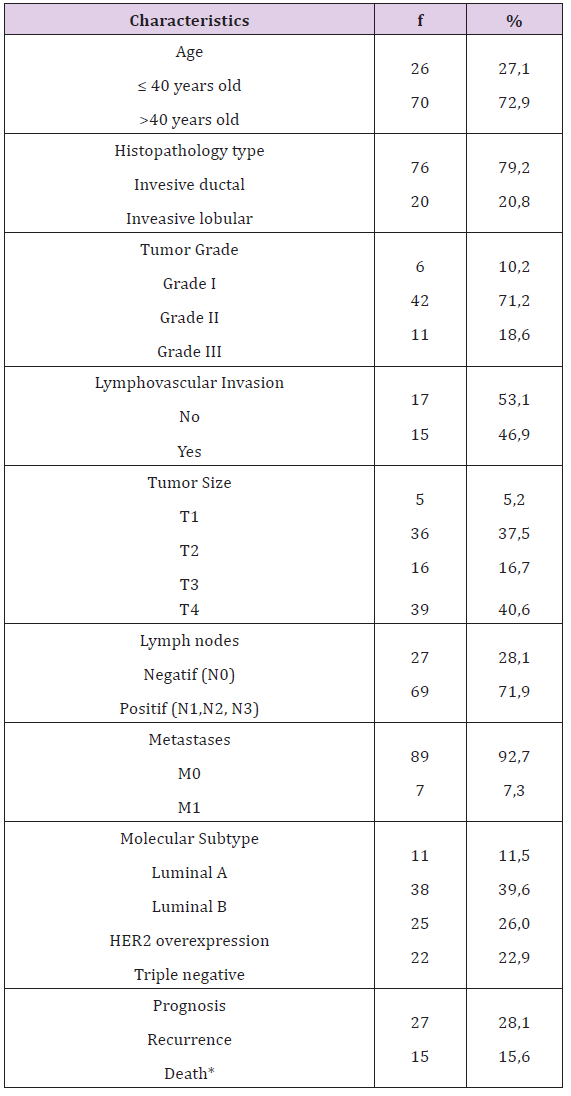
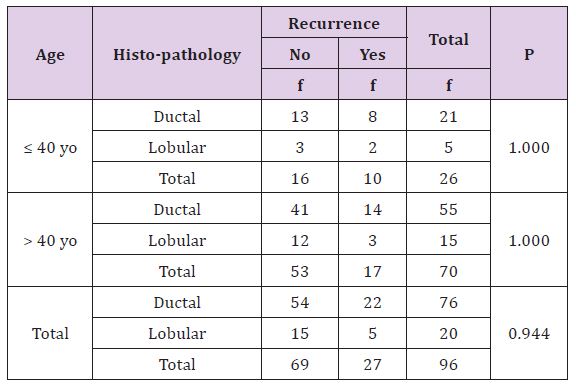
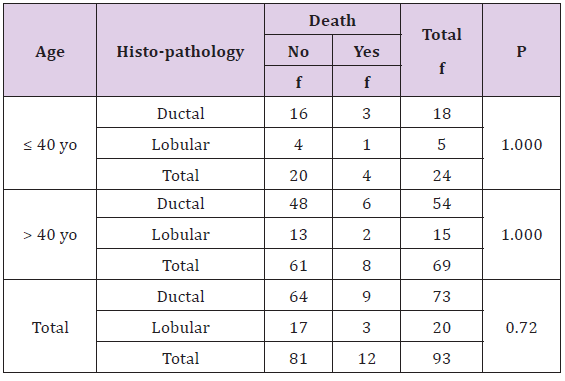
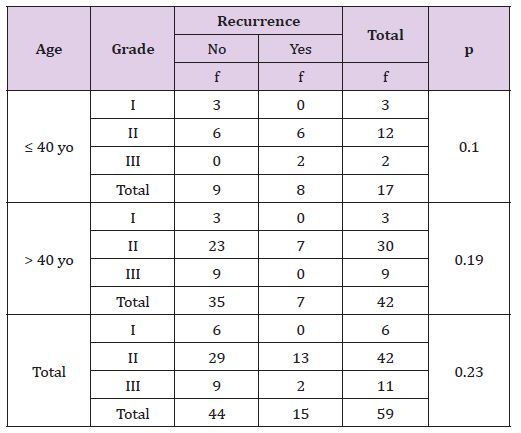

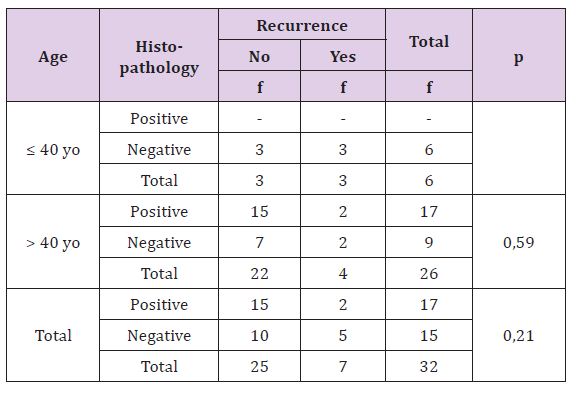
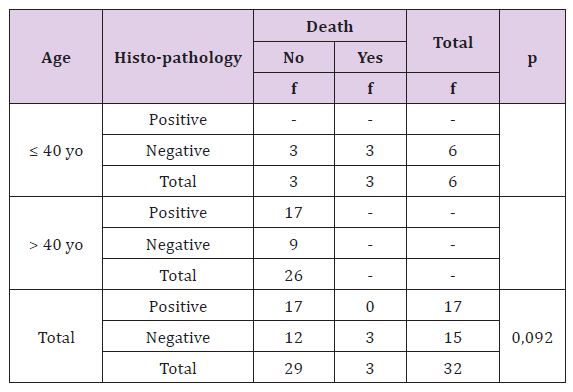
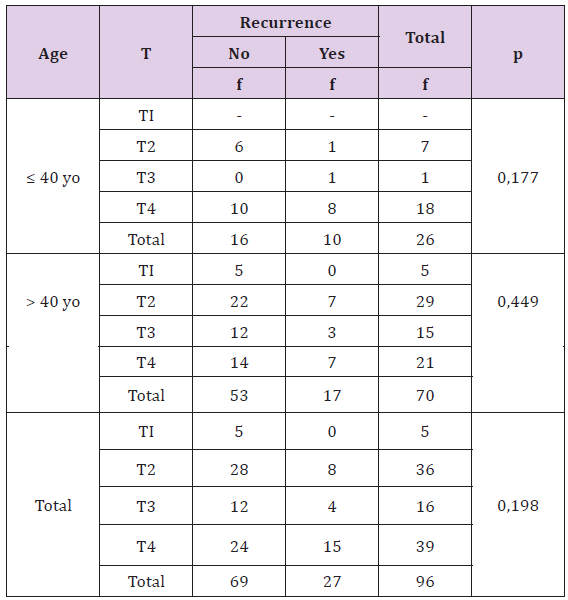
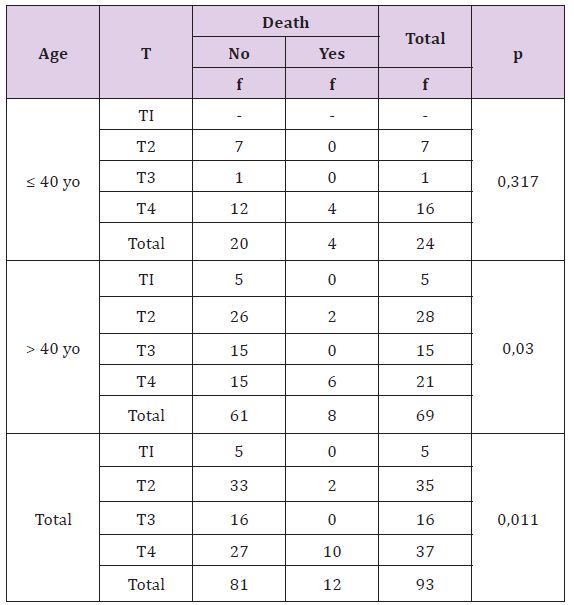
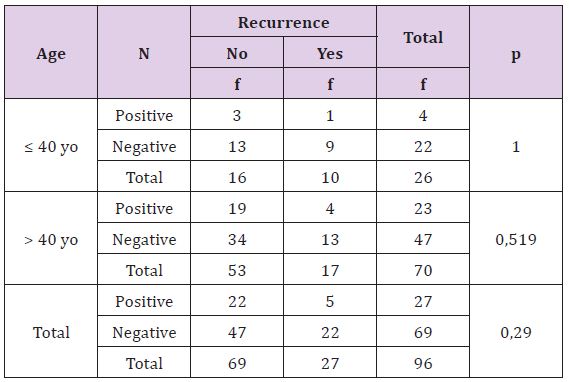
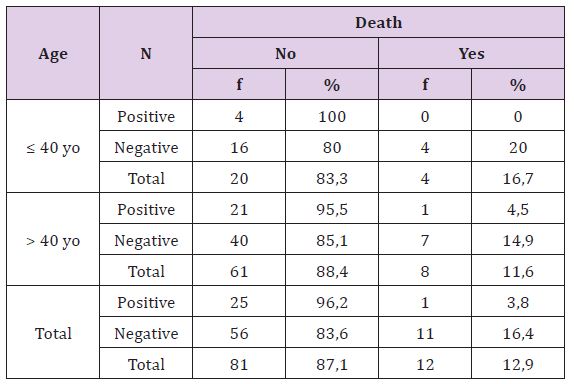
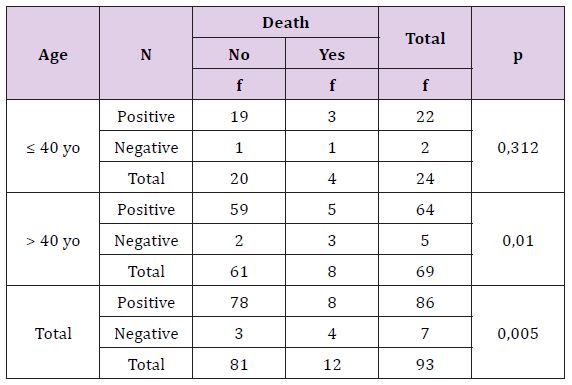
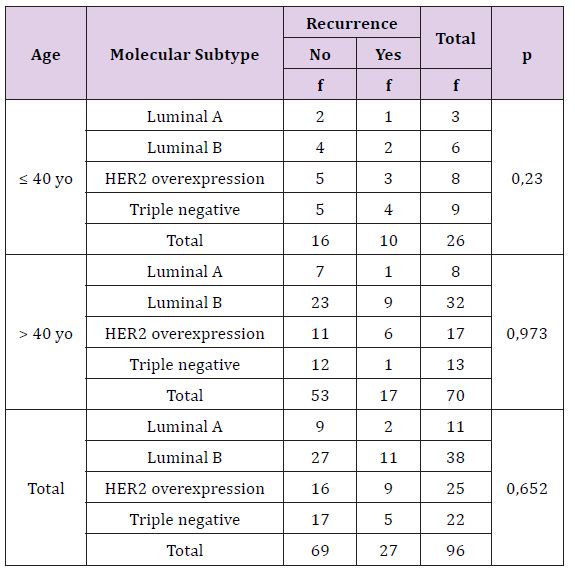
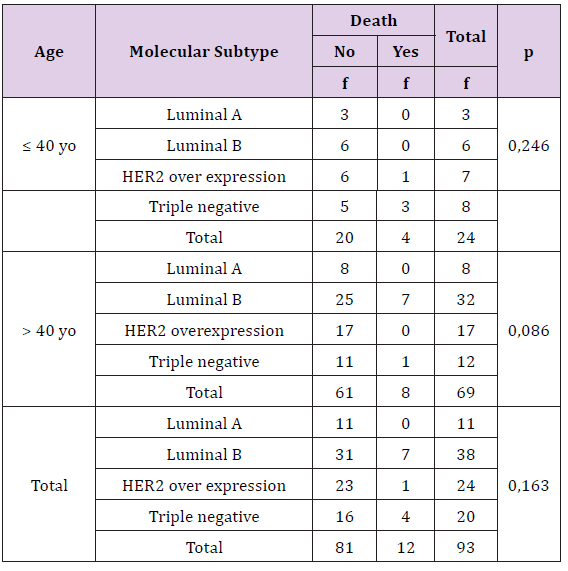





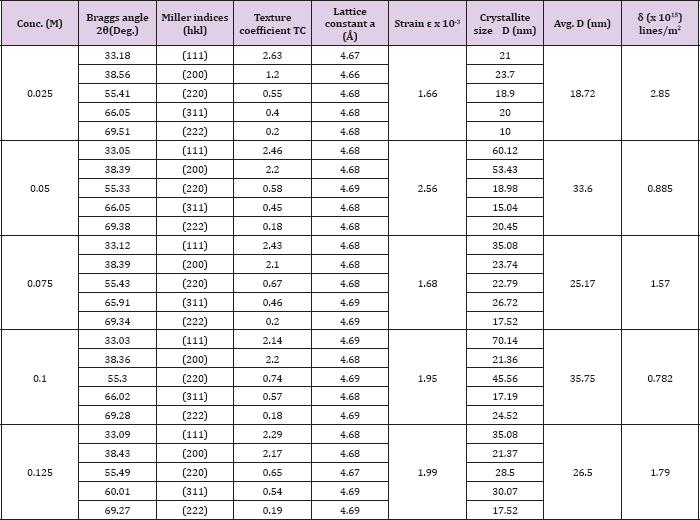
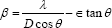



 is the ratio for of reduced effective mass to free-electron mass, which is equal to 0.274 for pure CdO. Therefore, the value of the coefficient is sbgn = 4.49X10-15eVcm2 . It is seen in Figure 9(a) the s1bon in present case obtained is 3.07 x 10-15 eVcm2 which is close to the theoretical value.
is the ratio for of reduced effective mass to free-electron mass, which is equal to 0.274 for pure CdO. Therefore, the value of the coefficient is sbgn = 4.49X10-15eVcm2 . It is seen in Figure 9(a) the s1bon in present case obtained is 3.07 x 10-15 eVcm2 which is close to the theoretical value.