Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Author: biomedicalopenaccessjournals
The only motto of Biomedical Journal of Scientific & Technical Research (BJSTR) Publishers is accelerating the scientific and technical research papers, considering the importance of technology and the human health in the advanced levels and several emergency medical and clinical issues associated with it, the key attention is given towards biomedical research. Thus, asserting the requirement of a common evoked and enriched information sharing platform for the craving readers.
BJSTR is such a unique platform to accumulate and publicize scientific knowledge on science and related discipline. This multidisciplinary open access publisher is rendering a global podium for the professors, academicians, researchers and students of the relevant disciplines to share their scientific excellence in the form of an original research article, review article, case reports, short communication, e-books, video articles, etc.
Cannabis Abuse and Suicide in Non-Affective Psychosis: A Recent Literature Mini-Review
Introduction
Schizophrenia is a severe chronic psychiatric disorder characterized by delusions, hallucinations, disorganized thought and/or behavior and negative symptoms [1]. Compared to the general population, schizophrenic patients have and increased risk of suicide [2-4]. According to the WHO, suicide is the most common cause of death among patients affected by a psychotic disorder [5]. There is a close relationship between schizophrenia and suicide [6]. Bleuler defined suicidal impulse as “the most severe of schizophrenic symptoms” [5]. It has been reported that schizophrenia reduces overall life span by approximately 10 years. Suicide is the largest single contributor to this reduced life expectancy. Suicide is the most common cause of death among people with schizophrenia [5]. There is also a strong correlation between schizophrenia and substance abuse disorder (SUD), including cannabis. In fact, cannabis is the most common substance of abuse in the world, being easily available at low cost [7]. Substance use and psychosis appear to be linked by reciprocal interactions, in terms of the development, evolution, and severity of the disorders [8-10]. According to some studies, patients with schizophrenia have an increased risk of developing a substance use disorder [11]. On the other hand, substance use can represent a trigger for a psychotic episode, or a precipitating factor for an already florid psychosis [12-15].
According to the current evidence in the literature regarding cannabis use disorder (CUD) and synthetic cannabinoids (SCs), not only they seem to be a possible risk factor for the development of a psychotic disorder, but also are likely to be involved in the progression of the disease as well as determining the severity of symptoms [16-21]. Evidence also seems to suggest that the abuse of cannabis or synthetic cannabinoids may increase violent behaviors both directed towards others and themselves [22-24]. For this reason, we decided to conduct a literature search with the aim of better clarifying the existence of a possible relationship between suicide and cannabis use or abuse, as well as explaining and evaluating nature and characteristics of this correlation.
Methods
Data source
We searched the PubMed database from 2010 to November 2021 using the following search string: “(“Suicide”[Mesh] OR suicide[tiab] OR “suicide attempt*”[tiab] AND “suicidal behaviour*”[tiab] OR suicidality[tiab] OR “suicidal ideation*”[tiab] OR “self injurious behaviour*”[tiab] OR “self-injurious behaviour*”[tiab] OR “suicide idea” [tiab] OR “self harm*”[tiab] OR “suicidal thought*”[tiab] OR “suicidal thinking*”[tiab] OR “self injur*”[tiab] OR suicidality[tiab]) AND (“Schizophrenia Spectrum and Other Psychotic Disorders”[Mesh] OR schizophrenia[tiab] OR “nonaffective psychos*”[tiab] OR “non-affective psychosis” [tiab] OR “non affective psychosis”[tiab]) AND (Cannabis[tiab] OR “Cannabis use disorder*”[tiab] OR Marijuana OR cannabinoid*[tiab] OR endocannabinoid*[tiab] OR CUD[tiab] OR “Cannabis”[Mesh] OR “Marijuana Abuse”[Mesh] OR “Endocannabinoids”[Mesh] OR “Cannabinoids”[Mesh] OR “Synthetic cannabinoid*”[tiab])”.
Eligibility Criteria
For our mini review we focused on studies regarding patients diagnosed with schizophrenia or schizophrenic spectrum disorders or diagnosed with non-affective psychotic disorder induced by the use of SCs, who used cannabinoids and attempted suicide or had suicidal ideation. We included all studies that reported the effects of cannabis on suicide risk, including ideation or attempts. We excluded those regarding self-harm that did not have suicide as a goal. We included only reports written in English. Specifically, we included all articles that reported on the effects of cannabis in general, THC, CBD, and synthetic cannabinoids. We applied the following exclusion criteria: articles in which self-injurious acts were mentioned but without suicidal intent; articles in which patients were not diagnosed with schizophrenia or schizophrenic spectrum disorders or diagnosed with non-affective psychotic disorder induced after using SCs; articles that did not include specifically cannabinoids use but included drug abuse as a general category. Titles and abstracts were screened for inclusion by three researchers (A.C., E.C. and A.P.). A fourth investigator (V. R.) was assigned for those cases in which there was no agreement about whether the manuscript met the criteria for inclusion.
Results
The research yielded a total of 49 articles which have been screened according to the inclusion criteria. Among these, 8 studies published between 2010 and 2021 were selected. Study designs distributed as follows: reviews (2), cohort studies (1), meta-analysis (1), cross-sectional analysis (2), systematic review (1); longitudinal studies (2); case reports (1). An Australian cross-sectional analysis (“Is cannabis a risk factor for suicide attempts in men and women with psychotic illness?”), performed on a sample of 1790 people diagnosed with schizophrenia or schizophrenia spectrum disorder, shows a positive correlation between cannabis use in adult males and suicide attempts. This study indicates a different gender susceptibility in response to cannabinoids regarding suicide risk, thus laying the foundations for further investigation to understand whether regular cannabis use has an influence on specific biological mechanisms that could explain the differences observed between men and women. However, the article concludes that there may be confounding factors and (depression, loneliness, homelessness and hallucinations) that need to be considered [25]. The Danish court study “Associations between substance use disorders and suicide or suicide attempts in people with mental illness”, performed on 35 patients, reports that cannabis is associated with an increased risk of suicide attempt in people with schizophrenia (HR: 1.11, 95% CI: 1.03-1.19).
As previously suggested, the associations between SUD and suicide attempts can be explained either by causal associations or by shared genetic and environmental vulnerabilities that predispose to both outcomes [26]. The longitudinal study “Suicidal behavior in first-episode nonaffective psychosis: Specific risk periods and stage-related factors” considers cannabis use, along with depressive symptoms, as the predominant risk factor for suicidal behavior over time. In particular, the article emphasizes the risk of cannabis use during first-episode psychosis (FEP), being this a phase characterized by a particular vulnerability to cannabis abuse, which appears to be an important risk for suicide attempts. Therefore, it would be important to assess the intervention on substance use during FEP as a valuable strategy to achieve the goal of reducing if not preventing suicidal risk [27]. The longitudinal study “Persistent cannabis use among young adults with early psychosis receiving coordinated specialty care in the United States” confirms the correlation between chronic cannabis use and increased suicidal ideation and risk. This article also underlines the importance of an intervention on the use of cannabis in the field of suicide risk prevention and quality of life [28]. In the Mendelian randomized study “Studying individual risk factors for self-harm in the UK Biobank: A polygenic scoring and Mendelian randomization study” polygenic scores (PSs) were generated to index 24 possible individual risk factors for self-harm, including suicide risk.
The results identify PSs, which appear to be predictors of selfinjurious acts. Concerning lifetime cannabis use, the study shows that it actually is a predictor of risk for suicidal self-injurious acts [29]. The only selected study involving synthetic cannabinoids follows the same trend as the studies before mentioned. The crosssectional analysis “Clinical characteristics of synthetic cannabinoidinduced psychosis in relation to schizophrenia: a single-center cross-sectional analysis of concurrently hospitalized patients” [22] specifically studying the effects of synthetic cannabinoids, states that a psychosis induced by this specific kind of drug exhibits a very high rate of suicidal ideation and acts. The two articles dealing exclusively with the CBD molecule show conflicting results. In the first study “The effects of cannabidiol (CBD) on cognition and the other symptoms in outpatients with chronic schizophrenia: a randomized placebo-controlled trial” [30], conducted by administering 600 mg/day of CBD for six weeks to schizophrenic patients stabilized with antipsychotics, no increase in suicidal risk was observed compared to the placebo-treated control group. Thus, this article found no association between CBD and increased suicidal risk. On the other hand, the study “A Review of Human Studies Assessing Cannabidiol’s (CBD) Therapeutic Actions and Potential”14, aiming to test the efficacy and safety of CBD, proves that the impact of this substance requires further investigation. In particular, the authors emphasize the need to understand in a more detailed way the effects of CBD on suicidal ideation, which seems to be a rare but dangerous adverse event when used in combination with anticonvulsant drugs.
Conclusion
From our review only few data have emerged regarding the correlation between cannabis use and suicide risk in patients with schizophrenia or other schizophrenia spectrum diseases, therefore we can’t draw definitive conclusions. Nonetheless these studies seem to point toward a positive correlation of cannabis use with increased suicide risk. It is not clear whether a single active component or rather a set of active metabolites is the explaining cause of the increased suicide risk, and unfortunately the data and the limited knowledge of the substance consumed by the patients included in the selected studies do not allow us to have a better understanding of the underlying phenomena. We think that greater clarification on these issues could be critical in reducing suicidal risk in patients with schizophrenia or schizophrenia spectrum disorders.
Juggling Between the Cost and Value of New Therapies: Does Science Still Serve Patient Needs
Decades of hope for a cure vanished into thin air when cost outweighed the value of the first gene therapy for thalassaemia, obliging the manufacturing company to withdraw it from Europe. This may create a precedent for other curative therapies that are currently in the pipeline after many years of research, raising questions over their future acceptance by payers and the fulfilment of their purpose: to cure as many patients as possible.
Frequent transfusions, chronic pain, absence from school and work, discrimination, mental health issues are just a few of the daily challenges that patients with thalassaemia face. Standard care with lifelong regular blood transfusions, iron chelation therapy and multidisciplinary care has achieved an increase in life expectancy [1,2]. However, a curative therapy would further allow patients to lead a new life with equal opportunities and challenges, as every other person not suffering from a severe chronic disease. The Thalassaemia International Federation (TIF), representing the united voice of people with thalassaemia and their families globally, has been striving for more than three decades to empower research on a curative approach for thalassaemia.
Haematopoietic stem cell transplantation (HSCT) offers the possibility of cure, but bears specific limitations, i.e. HLA-identical sibling matching and young age [3]. Gene therapy may overpass these challenges, covering more patients and a larger age span. Research on genome-based therapies persisted for decades and this journey has been difficult and immensely challenging until a few years ago [4,5]. The small US-based biotech company bluebird bio that undertook the improvement of a vector produced by Leboulch in 1994, finally succeeded in what predecessors failed [6], partly because it paid attention to the patients’ perspective and their everyday journey with this debilitating disease. Stakeholders always knew that an innovative and complex therapy for thalassaemia would be expensive but always supported its development. Governments and academia provided grants, the industry invested in product’s improvement, healthcare professionals and patients monitored the pipeline and hoped for access. But when the European Medicines Agency granted the gene therapy product of bluebird bio, called ZyntegloTM, a conditional market authorisation in May 2019, everyone focused on numbers and cost-effectiveness studies [7] However, no health economist would ever capture accurately the real cost of thalassaemia in terms of pain, uncertainty and fear.
The withdrawal of an authorised gene therapy from Europe will most probably slow down or even halt the access of people with thalassaemia to curative approaches, rendering the future of thalassaemia treatment gloomy at the very least. And if the developed countries of Europe cannot afford an innovative therapy, what will happen to low- and middle-income countries, where the 80% of the global thalassaemia population lives? Depriving patients from a chance to be cured is at the minimum unethical and constitutes a violation of human and patients’ rights endorsed for decades now by relevant European Union and international bodies. It is also a discriminatory behaviour against people with thalassaemia, given that patients in other disease areas do receive innovative therapies bearing a hefty price tag. It is of utmost important for all stakeholders engaged in the development of medicines, and especially the industry and academia, to seek early and transparent dialogue during the long course of drug development to identify timely safety and cost hurdles.
The developers of medicines, after having invested considerable funds in developing and commercialising a product, should not be left exposed to failure but be given the necessary space, time and motivation to mitigate problems in market access. Additionally, a central, special fund on innovative therapies should be created and managed by the European Commission to compliment national funds of Member States for novel therapies. Governments need to develop synergies and discuss pricing early on, considering the lessons of the past and the challenges to come. As countries do not have unlimited financial resources, governments may opt for joint procurements in the context of regional alliances, such as the Valletta Declaration or the BeneluxA initiative, that increase their negotiating power for the purchase of expensive therapies. Finally, treating physicians and patients should become actively and meaningfully involved in the development process from the very early stages to provide concrete information on medical and other priorities, the potential number of patients that could benefit from innovative therapies, and short and long-term plans for the access of eligible patients to such therapies. Everyone has a role to play and we all share the same responsibility for the sad decision of bluebird bio to withdraw its services (even temporarily) from Europe. Life cannot be measured using mathematical models. Science needs to be available, accessible and most importantly, at the service of patient needs.
In Vitro and in Vivo Antimicrobial Effects of Aloe Vera Fermented Hericium Erinaceum KU-1 for Food Borne Pathogens and Helicobacter Pylori
Introduction
Aloe vera is most commonly known representative of aloe which belongs to the Liliaceae family and has been used as a remedy in many cultures. It is short-stemmed perennial and has leaves with sharp thorns. Aloe contains ingredients such as aloe ulcin, alomicin, aloetin, and aloesin, so it is widely known to have effects for anti-ulcer, anticancer, antiviral, antibacterial, and antifungal [1]. Hericium erinaceus is an edible mushroom and is used for gastrointestinal diseases by regulating gut microbiota and immune system [2]. It has the rich diterpenoid compounds, steroids, and polysaccharides and is known to have the antimicrobial activities against Helicobacter pylori, a human gastrointestinal pathogen [3,4]. As such, the mixture of the mycelium of Aloe vera and Hericium erinaceus was expected to have a strong antimicrobial effect, but it has not been studied yet. Therefore, we aimed to study the antimicrobial effects of Aloe vera fermented Hericium erinaceum KU-1 for food borne pathogens and Helicobacter pyloriin vitro and in vivo.
Food borne pathogens, such as E. coli, Salmonella and Listeria, are major causes of gastrointestinal disease worldwide. Enterohemorrhagic E. coli O157:H7 causes hemorrhagic colitis, which is occasionally complicated by hemolytic uremic syndrome [5-7]. It is estimated that E. coli O157:H7 infection causes over 73,500 cases of illness each year in the United States [8]. Salmonella spp. are facultative intracellular organisms that grow primarily inside the macrophages of the liver and spleen. S. enterica serovar Typhimurium is the most commonly isolated Salmonella serotype, accounting for 23% of laboratory confirmed Salmonella cases among the more than 1.4 million infections each year in the United States [9]. This infection is characterized by clinical symptoms such as fever, abdominal pain, and diarrhea in both animals and humans. Listeria monocytogenes is a gram-positive intracellular bacterium that is normally nonpathogenic in healthy individuals. However, in pregnant women, newborn infants, the debilitated elderly or immunocompromised people, it may cause severe clinical disease including meningoencephalitis, septicemia, or abortion [10-15].
It is estimated that L. monocytogenes infection causes about 2,000 to 2,500 cases of illness and as many as 500 deaths per year in the United States [16]. Helicobacter pylori is characterized by its typical corkscrew-like appearance and is at least twice as long as H. heilmannii [17], with a low infection rate of 0.08-1.0 % in humans [18,19]. Its infection has been described mostly in relation to chronic gastritis [20,21], gastric ulcers [22] adenocarcinoma [23] and MALT lymphoma [24] in men. Antimicrobial chemotherapeutic agents have been widely used to control these gastrointestinal infections. However, widespread use of antibiotics is now being discouraged due to problems including the emergence of drug-resistant strains and chronic toxicity [25]. In addition, antibiotics are often responsible for acute diarrhea due to the loss of normal intestinal microbes and the protection they provide against pathogenic organisms [26]. As alternatives, Hericium erinaceum (HE) such as KU-1 and their mycelium have been administered.
It is well known as lion’s mane or monkey head mushroom have health-promoting attributes including antimicrobial properties [27-29], immunomodulation [30-33], anti-tumor characteristics [34-36], and hypocholesterolemic effects [37,38]. These findings have caught the attention of nutrition, food, and microbiology scientists and have heightened interests to produce functional foods. We isolated HE KU-1 and their mycelium from Pterocarpus indicus, and Cyclobalanopsis spp. This HE KU-1 was fermented in an appropriate Aloe vera broth, condensed by vacuum evaporation, and mixed with equal doses of each pathogenic strain. In this study, the antimicrobial effects of this HE KU-1 fermented condensate mixture (ALOHEM) were evaluated using in vitro and in vivo models of food borne pathogens and Helicobacter pylori.
Materials and Methods
Microorganisms
coli O157H:7 ATCC 43894 (American Type Culture Collection, Rockville, MD, USA), Salmonellaenteritidis CCARM 11066 (Culture Collection of Antibiotic Resistance Microbes, Seoul, Korea), Staphylococcus aureus (KFRI 240, Korea Food Research Institute, Wanju-gun, Jeollabuk-do, Korea), and Listeria monocytogenes ATCC 19115 and ATCC 51774, were used as pathogenic strains.
Mycelial Culture
Figure 1: Manufacturing process of ALOHEM.
The preparation process of ALOHEM is as shown in Figure 1. HE KU-1 mycelium was maintained on solid Ko medium [39] which is composed of glucose 18.02 g, arginine 2.613 g, ammonium acetate 2.613 g, CaCl2 0.33 g, KH2PO4 8.5 g, MgSO4·7H2O 2.0 g, FeSO4·7H2O 0.02 g, ZnSO4·7H2O 0.02 g, MnSO4·7H2O 0.02 g, agar 18.0 g and distilled water 1 L at pH 4.5~5.0. A single colony of each HE KU-1 mycelium was inoculated into 10 mL of the Ko broth in a 15 mL conical tube and cultured in a shaking incubator (NB 205, N-Biotec, INC., Bucheon, Kyoungki-Do, Korea) at 200 rpm and 28℃ for 2~3 days [39] HE KU-1 mycelia were fermented in Aloe vera broth on a jar-fermenter (CelliGen 115, Eppendorf, INC., NY, USA) at 150 rpm, 28℃ for 3~4 weeks. 99% of Aloe vera extract (Aloe vera gel W®, KimJeongMoon Aloe Ltd., Jeju-Do, Korea) was tested.
Preparation of Aloe vera Fermented Hericium erinaceum KU-1 Condensate Mixture (ALOHEM)
Following fermentation period of 3-4 weeks at 25~28°C, the HE KU-1 mycelia were isolated from a single colony and tested for their inhibitory effects on various food-borne pathogens. The HE KU-1 mycelia were removed by centrifugation at 2,700 ´ g for 30 min and the fermented media was concentrated 20 fold into a solid content by vacuum evaporation. Each concentrated medium was mixed with an equal weight of Aloe vera extract and lyophilized. The final ALOHEMs were prepared by mixing each condensate of equal weight and stored at 4℃ until use.
Animals
Five-week-old specific pathogen-free (SPF) female BALB/c mice (Seoul National University Laboratory Animal Center, Seoul, Korea) for S.enteritidis infection and ICR mice (Daehan-Biolink, Chungbuk, Korea) were used for H. pylori infections. They were housed in polycarbonate cages in isolators and fed a commercial pellet diet with water ad libitum. Food and water were removed from the cages 5 hours prior to inoculation of the bacteria and/or ALOHEM. All animal experimentation was performed in accordance with the laboratory animal guidelines of Korea University (Seoul, Korea).
In vitro Assessment of Antimicrobial Effects of the ALOHEM
Each pathogenic strain was grown to an optical density (OD) of 0.8-1.0 at 600 nm. Briefly, 200 mL of each bacterium was added to conical tubes containing 10 mL of appropriate concentrations (0, 1.25, 2.5, 5, 10 %) of the AFHCM in TS broth and incubated with shaking at 200 rpm and 37℃. And 1 mL of each culture was taken at 0, 1, 2, 3, 4, 6, and 8 h post incubation and centrifuged at 5,000 rpm for 10 min. The supernatants were discarded and the bacterial cells were floated in 1 mL of fresh TS broth. Finally, the OD was measured at 600 nm. This process was repeated once. To determine whether the antimicrobial effects of the ALOHEM are due to pH, tubes containing various concentrations of the ALOHEM were adjusted to pH 7.2 by the addition of NaOH. Subsequently, 200 mL of cultured S.enteritidis was added to each tube and incubated at 37℃. OD was measured at 0, 2, 4, 6, and 8 h post incubation using the same method as the sample preparation described above. This process was not performed against the other pathogens.
In vivo Assessment of Antimicrobial Effects of the ALOHEM
For S.enteritidis infection models, 1 mL containing 5 ´ 107 CFU of S.enteritidis was added to each tube containing 9 mL of the ALOHEM at various concentrations (2.5, 5, and 10%) or of the TS broth (positive control), vortex-mixed, and used as inocula. The mice were immediately administered with 0.5 mL of each inoculum (2.5 ´ 106 CFU of S.enteritidis per mouse) via the intragastric route while the negative control mice were administered with the same volume of TS broth. Subsequently, the mice of each treated group were administered with 0.5 mL of ALOHEM of their respective concentration once a day for 4 days and the mice of positive and negative groups received 0.5 mL of TS broth. Bacteria from fecal samples were counted by plating on XLD (Difco) agar at 12 h, 1, 2, 3, and 4 days post-inoculation (pi) days and mortality was checked at 21 days pi.
pylori originating from pig’s stomach had been kept in the gastric passage of mice [40]. Three H. heilmannii-infected mice were necropsied by cervical dislocation and the stomachs were collected. They were carefully opened and the gastric content was removed by washing with sterile phosphate buffered saline (PBS). The stomachs were then added to a conical tube containing 10 mL of sterile PBS, electrically homogenized (Ultra-turrax T25, Ika, Staufen, Germany), and the resulting mixture was used as an infective inoculum. Then 1 mL of the infective inoculum was added to each tube containing 9 mL of 2.5, 5, and 10% ALOHEM or TS broth (positive control), respectively, and vortex-mixed. The mice were immediately administered 0.5 mL of each inoculum intragastrically while the negative control mice were administered the same volume of TS broth. Subsequently, the mice of each group were administered 0.5 mL of each concentration of the ALOHEM once a day for 2 months pi, at which time all mice were euthanized by cervical dislocation and necropsied. Their stomachs were collected, opened, and the gastric contents were removed as described above. The gastric samples were then fixed in 10% buffered formalin for 24 h, processed, and embedded in paraffin wax as standard protocol. Sections measuring 2 micrometers each were prepared and stained with hematoxylin and eosin (H&E) and modified Steiner’s silver stain (Sigma, St. Louis, MI, USA) for histopathological examination and for the detection of H. heilmannii, respectively.
Results
Antimicrobial Effects in vitro of Various Concentration of ALOHEM
The ability of the ALOHEM to inhibit the in vitro growth of food-borne pathogens was evaluated and the results are shown in Figure 2. Just before the pathogens were added to each tube, the pH levels of the solutions were measured at 4.03 (10% ALOHEM), 4.32 (5% ALOHEM), 4.96 (2.5% ALOHEM), 6.02 (1.25% ALOHEM), and 7.24 (0% ALOHEM). The growth of all strains except E. coli O157:H7 was completely inhibited by the presence of the ALOHEM at concentrations above 2.5%. All strains except L.monocytogenes ATCC 51774 began to grow in the broth containing the concentration of 2.5% ALOHEM 2 to 4 h post incubation, although the growth rate was lower than that of the control broth (0% ALOHEM) (Figure 2A-2E). However, when the pH of the broth was adjusted to 7.2, the presence of the ALOHEM at any concentration did not inhibit the growth of S.enteritidis at all (Figure 2F).
Figure 2: In vitro growth of E. coli O157:H7 (A), S. aureus (B), L. monocytogenes ATCC 19115 (C), L. monocytogenes ATCC 51774 (D), S. enteritidis (E) was inhibited by the presence of ALOHEM. Data show the mean value of two experiments performed. At the initial time of experiment, the pH of each broth containing 0% (-■-), 1.25 % (-▲-), 2.5 % (-ⅹ-), 5 % (-◆-), and 10 % (-●-) ALOHEM was 7.24, 6.02, 4.96, 4.32, and 4.03, respectively. Another experiment was performed to clarify the effects of pH on the antimicrobial ability of the ALOHEM (F). Each broth containing the different concentrations of the ALOHEM was adjusted to pH 7.2 with NaOH. Because the ALOHEM brings about a brown hue, optical density depended on the concentration of the ALOHEM at the start of the experiment (0 h).
Bacteria Count Evaluation by ALOHEM
Antimicrobial effect of the ALOHEM against S.enteritidis and H. heilmannii infection was assessed in BALB/c and ICR mice, respectively. Table 1 shows the viable bacterial count from the fecal samples. The number of isolated bacteria was dose-dependently less in the mice inoculated with an admixture of the ALOHEM and the bacteria than in the mice that received only the bacteria (positive control). However, bacteria were steadily isolated in the mice that received 2.5% and 5% ALOHEM over the first 4 days. Bacteria were isolated from only one mice of the group administered with 10% ALOHEM 4 days following injection. The limitation of the bacterial count was 4.00 log10 CFU/g feces.
Table 1: Bacterial counts from fecal samples.
aValues in parentheses represent the number of mice from which bacteria were isolated. All groups originally consisted of five mice.
Assessment of Mortality by ALOHEM
Mortality was assessed for 28 days pi. Daily administration of the ALOHEM or TS broth in each group was terminated when the first mortality occurred in the positive control group on day 5 pi. All mice of the positive control group died within 7 days of injection (Figure 3). Although all mice in the 2.5 and 5% ALOHEM treated group eventually died, mortality occurred between 9- and 11-days pi, later than that of the positive control group. Within the 10 % ALOHEM treated group, one mouse died on day 14 pi and another on day 18 pi, while the rest survived until 21 days pi (Figure 3).
Figure 3: Mortality of the mice dosed with S. enteritidis throughout the experimental periods; the positive control group (-□-), 2.5 % (-△-), 5 % (-ⅹ-), and 10 % (-○-) ALOHEM treated groups.
The Histopathological and Microbiological Findings
Table 2 summarizes the histopathological and microbiological findings. The results show that the use of ALOHEM did not suppress the bacterial colonization and histological lesions in the stomach at all.
Table 2: Histopathological and microbiological findings of the mice stomachsa.
aexpressed as number of detected mice/ number of tested mice. bconsisted of infiltration of mononuclear cells in lamina propria and submucosa. cassessed by Steiner’s silver stain.
Histological Lesions
Figure 4: Marked colonization (arrows) of H. heilmannii in the lumen of the gastric glands of (A) a positive control mouse and (B) a mouse inoculated with an admixture of 10% ALOHEM and H. heilmannii. (C) Infiltration of mononuclear cells and (D) presence of lymphoid follicle in the submucosa of the gastric body of mice inoculated with the admixture of 10% ALOHEM and H. heilmannii. A, B, C; Bar = 250 mm, D; Bar = 62.5 mm.
Regardless of the concentration of the ALOHEM treatment, marked colonization of H. heilmannii was observed in the lumen of the gastric glands, gastric pits, mucosal surfaces, and intercellular spaces of all infected mice (Figure 4A&4B). Histological lesions such as the formation of lymphoid follicles, cystic changes, and mild inflammation in the mucosa or submucosa were randomly observed (Figure 4C&4D). No bacteria and histological lesions were observed in the negative control group.
Discussion
Many studies have recently shown that Hericium erinaceum have antimicrobial effects. The potential mechanisms by which mushrooms might exert their antimicrobial activity includes the production of hericenone, other metabolites such as hydrogen peroxide and short chain fatty acids, and specific antimicrobial compounds such as antibiotics [41,29,38]. In the present study, we have shown that the ALOHEM effectively inhibits the in vitro growth of enteropathogens such as E. coli O157 H:7, S.enteritidis, S. aureus, and L.monocytogenes. In vivo experimentation also revealed that the presence of 10% ALOHEM increased the survival rate of mice infected with S.enteritidis. In addition, the survival time of the 2.5 and 5% ALOHEM groups was extended beyond that of the positive control group, even though all mice died within 11 days pi.
This might be because the presence of 2.5 and 5% ALOHEM did not completely inhibit the growth of S.enteritidis and the bacterial growth rapidly progressed after the ALOHEM administration was terminated (4 days pi). Also, the presence of the ALOHEM did not inhibit the colonization of H. heilmannii in the stomach. These divergent results made it difficult to identify the antimicrobial mechanism of the ALOHEM. We first considered the low pH due to the hericenone as the factor, because the pH of each broth was in inverse proportion to the concentration of the ALOHEM. Based on this consideration, the pH of each broth was adjusted to 7.2 by the addition of NaOH and 200 µL of an overnight culture of S.enteritidis was subsequently added to each broth. As a result, bacterial growth was not inhibited in any of the broths. This finding indicates that the antimicrobial effects of the ALOHEM might be due to low pH, which is also the reason that the presence of the ALOHEM did not inhibit the colonization of H. heilmannii in the stomach. H. heilmannii is able to colonize the stomach by increasing the gastric pH through its urease production.
Therefore, it is likely that H. heilmannii mixed with 10% ALOHEM could survive at a low pH level by producing urease and colonizing the stomach. Previous findings [41] have shown that some hericenone produce by Hericium erinaceum spp, although able to inhibit a variety of pathogenic bacteria, do not inhibit the growth of both Salmonella sp. and Vibrio cholerae, when the effect of acids was excluded. Our preliminary study also shows that long periods of ALOHEM administration did not affect clinical signs, or the gross and histopathological lesions of the mice (data not shown), indicating that its ingestion might not pose health risks to humans and in fact be effective in preventing infections due to food borne pathogens.
Conclusion
This study was investigated the antimicrobial effect of an Aloe vera fermented Hericium erinaceum (HE) KU-1 condensate mixture (ALOHEM) using in vitro and in vivo models of food borne pathogens and Helicobacter pylori. The presence of the ALOHEM effectively inhibited in vitro growth of food borne pathogens such as E. coli O157:H7, S. aureus, L.monocytogenes, and S.enteritidis. However, when the pH of the broth was adjusted to 7.2, the ALOHEM did not inhibit the growth of S.enteritidis at all. The in vivo antimicrobial effects of the ALOHEM against S.enteritidis and H. pylori were also assessed. In S.enteritidis-infected mice, the ALOHEM decreased the viable bacteria found in the feces and the mortality rate. However, it did not affect the gastric colonization of bacteria and histopathological lesions in mice infected with H. pylori, which is able to colonize the stomach by increasing the gastric pH through its urease production. These findings showed that the ALOHEM might have antimicrobial ability by decreasing pH.
Invent a Removable Orthosis with the Ability to Prevent Foot Drop and Venous Thrombosis and Maintain Muscle Contraction
Introduction
From the perspective of the World Health Organization (WHO), health is the science and technology of disease prevention, providing medical services for immediate diagnosis, treatment and development to address problems. Safety is one of the most important aspects of health care systems [1]. Increasing the quality of work, consequently, increases the accuracy and improvement of the treatment process, the speed of the treatment process and also patient satisfaction [2]. Intensive care includes taking care of patients with life-threatening diseases, under the supervision of the most skilled personal, with advanced equipment and facilities, which includes all sensitive care related to the patient’s life [3,4]. A significant part of the treatment system’s effort is focused on being able to provide the best services to its patients in the shortest time and at the lowest cost. Intensive care units (ICUs) have an important place due to the high human and economic costs that they can incur for the health care system [5,6].
Patients with problems such as diabetic ketoacidosis, hypertensive emergency, non-accidental self-poisoning, heart failure, ischemic heart disease and cerebrovascular disease and respiratory conditions can be mentioned [7-9]. Numerous studies have been performed to identify the increasing mortality factors of patients admitted to the ICU. Infectious shock, age, smoking and nosocomial infections are among the factors that increase mortality in ICU wards [10,11]. A comprehensive study of UK hospitals showed that the mortality rate of patients admitted to ICU wards is about 20.6% [12] and that of Singapore public hospitals is 9.4% [13]. Complications of hospitalization in the Intensive Care Unit include foot drop, deep vein thrombosis[14], muscle atrophy [15] and so on. Venous thromboembolism (VTE), including deep vein thrombosis(DVT) and pulmonary thromboendarterectomy (PTE), is a public health problem that results in 250000 hospitalizations per year in the United States [16,17]. On the other hand, one hundred to fifty thousand people are hospitalized every year due to a benign and treatable disease, but die due to pulmonary embolism, while with prevention, the death of these patients can be prevented [18].
Risk factors for this disease are immobility, cancers, myocardial infarction, respiratory failure, surgery, trauma, obesity, use of female hormones and inherited coagulation disorders [19]. Another complication of hospitalization is “foot drop”. Foot drop or foot prolapse is a condition in which a person is unable to perform the dorsiflexion joint function properly due to weakness or paralysis of the anterior tibialis muscle or other muscles originating in the peroneal nerve. Foot drop can be unilateral or bilateral. Symptoms such as pain, weakness, and numbness are sometimes seen with this complication [20]. Diagnosis of this complication is easily possible by physical examination, but the use of imaging techniques and electromyography can also help to examine this complication more closely [21]. Today, there are various treatments to control foot drop, which considering the cause of this complication, the appropriate treatment method is adopted. Among the available treatments for prevention and correction of foot drop, physiotherapy, electrical stimulation and teaching the most common treatments using ankle foot orthosis [22].
Other complications of hospitalization in the intensive care unit include muscle atrophy [15], bed sores, etc. At present, according to the subject and results of research, one of the ways to prevent and reduce complications in hospital wards is to produce and use a mobile orthosis with the ability to prevent foot prolapse and venous thrombosis and maintain muscle contraction. In the following, we will talk about its structure. This idea has been registered in the Patent Organization of Iran under invention number 103769.
Methods
This project started with a new researcher idea Then by searching in the scientific content of articles and book, the title and proposal the project was compiled with opinion of the supervisor. Then model of the device was designed in collaboration with graphic & mechanical engineers Fianccy. The main tool was invented by the researcher. By mechanic engineer and solid work the design of this tool with professional software with academic-theorical proposal researchers (Mahmoudi and Mohammadbeik) about making a tool for the purpose of preventing foot drop, deformity of toes, muscles atrophy, improvement of blood return from distal to proximal organs and keep the function of vainvalves, assessment of vital signs and keep the power of foot solid muscles and prevention from muscels atrophy. This idea is designed by softwares and then the file of this designing was transferred to laboratory by researcher and work mechanic engineer in order to hardware designing and maquette. The structure of orthosis was discussed in terms of all angle’s morphology, measurement of figure based on standards and again after changing s figures and ,measurement was redesigned by software expert.
Figure 1: According to Figure 1
1. Orthotic body
2. Mechanical lock
3. Electric leads.
This mobile orthosis with the ability to prevent foot drop and keep the function of vain valve and assessing the vital signs is composed of (mechanical lock: 3×2cm, body: 40 cm length , pulse sensor: 0.5× 0.5 cm, pulse oximeter sensor: 0.5× 1 cm, inflatable inner layer R: 12cm, outer layer R: 15cm, electrical message transmitter leads: R: 1cm, insole: 25cm, removale hinge R: 2cm, connector between inner laye and air pump R:2cm. Orthosis is made up of upper and lower sections which after right locating(positioning) of foot in it, two sections will be connected to each other by mechanical lock (according to Figure 1, number 2). for motion of foot in its rang of motion (ROM), first removable hinge(according to Figure 7, number 11) is connected to monitor screen which is seprated from orthosis by a wire. all normative motion for foot’s motion(foot’s dorsal flexion, foot’s sole flexion,invertion , overtion) will be done by a program which is designed on screen and by choosing each motion, message will be transferred to removable hing(according to Figure 2, number 11) by a wire and by moving the orthosis, the foot moves in the desired direction and according to instruction given to program , the foot remains at desired posture for specified period of time (5s) and returns to its initial posture again.
Figure 2: According to Figure 2
1. 7- outer layer of orthosis
2. 8- inner layer of orthosis
3. 11- Removable hinges.
Figure 3: According to Figure 3
1. Air pump
2. LCD
3. Power on
4. Power off
5. Junction with interface.
Figure 4: According to Figure 4
1. 4- Connector
2. 5- Orthotics insole
3. 6-Upper part of orthosis.
Figure 5: According to Figure 5
1. Tens devices
2. LCD
3. Power on
4. Power off
5. Wire connection position.
Four foot motion (foot’s dorsal flexion, foot’s sole flexion, invertion and overtion) is done through a program which is programmed on the screen memory via removable hing, the duration of doing this motion, number of times, the amount of foot’s rest until next move. For preventing deep vein thrombosis (DVT) and maintaining the one way valve function, first the portable small air pump (according to Figure 3, number 1) which is available in the market is connected to the connector between air pump (according to Figure 4,number 4) and inflatable inner layer (according to Figure 2, number 8 ) by an air tube through transfering air from pump to inflatable inner layer the action of inflating and emptying takes place. Of course the number of times, intensity of wind pressure is defined by screen (according to Figure 4, number 6) available on pump’s body(according to Figure 3, number 1) and applied on foot, which this action causes standard pressure(17 mmhg) on one way valve and it causes continuity and helping blood circulation and prevents from the reduction of one way valve function.
Figure 6: According to Figure 6
1. 9- pulse Oximeter sensor
2. 10- Pulse Sensor.
Also electrical leads (according to Figure 1, number 3) are connected to the desired position (according to Figure 5, number5) by a wire and after connecting to tennes machine (impulse maker machine) by making impulses causes electrical stimulation of muscles and prevents muscles failure and atrophy that voltage intensity, duration of muscle stimulation, number of stimulation are controlled and done by screen (according to Figure 5, number 2) and planning is done. According to location of the sensor in the upper part of orthosis(according to Figure 6 , number 10) number of dorsal pedis pulse is measured and shown on the screen. Also by placing pulse oximeter sensor on the upper part of orthosis (according to Figure 6, number9), the amount of oxygen saturation is shown on the screen. By making movable orthosis and due to structure and muscle electrical stimulation prevents reduction of muscle contraction, atrophy and foot drop and causes maintaining valve function and the amount of oxygen saturation is studied through dorsal pedis pulse sensor and pulse oximeter sensor and can prevent the accurance of many diseases and the death caused by them.
Discussion
This research has been done in the field of medicine and medical engineering. Due to the extent of the foot drop and Deep vein thrombosis when providing medical care to the drug, the use of preventive equipment is felt to prevent this problem. Due to the innovative design of this design, Used to prevent ankle foot drop, deformity of the toes, muscle atrophy, improve blood flow from the lower to the upper and improve blood flow from the lower to the upper and monitor vital signs monitor vital signs and maintain the strength of the leg muscles. The advantages of this plan include moving the foot in four directions (flexion of the back of the foot and flexion of the sole of the foot and inversion and oversight), the ability to plan the number and time of movements, check vital signs in the lower limb, prevent reduction of contraction Muscles, preventing blood stasis and thrombosis in the lower extremities, preventing atrophy and muscles mass. Also, according to the research of Esfandiari et al (2017), a study entitled Literature Review of the Effect of Ankle-Foot Orthosis on Gait Parameters After Stroke [23] and Alnajar et al (2020), with Title Advances in neuroprosthetic management of foot drop [24] and prenton et al (2018), with Title FUNCTIONAL ELECTRICAL STIMULATION AND ANKLE FOOT ORTHOSES PROVIDE EQUIVALENT THERAPEUTIC EFFECTS ON FOOT DROP [25], and this research, the use of preventive equipment to prevent Ankle foot drop, toe deformity, muscle atrophy, improving blood flow from the lower to the upper and maintaining pigeonhole valve function and monitoring vital signs and maintaining leg muscle strength is suggested.
On Possible Regulation of Cancer Cells Growth Dynamics Using Electromagnetic Effects on the Body
Introduction
This work is a logical continuation of a series of previous works devoted to the analysis of the influence of external constant and variable electromagnetic (abbreviated as EM) fields on biological objects (see articles [1,2]). This report will focus on the study of the influence of variable EM fields on the cellular structure of the body. In this case, the system of the Lotka-Volterra equations [3,4] will be taken as the basis for calculations and estimates, which we will modify accordingly in relation to our problem, relying to a large extent also on the work [5]. It is not difficult to formally introduce any type of interaction into the system under study. The main issue is always the physical and mathematical justification of the appropriate type of interaction and understanding how to apply it to a particular task. It is this justification that we will now deal with in order to achieve this goal. It is worth noting beforehand that issues related to the mathematical description of cancer diseases have been dealt with for a relatively long time, and there are a number of results in this area, described in some detail, for example, in [6- 7]. The approach proposed below is based on considerations other than those mentioned above and gives a theoretical prediction for the treatment of such diseases.
The Energy of Cell Interaction with the EM Field
In order to find the interaction we are interested in, we will need to take into account the following two very important points. Namely, firstly, this interaction should be invariant with respect to the time sign inversion, and, secondly, it should take into account the concentration of “predators” and “preys”. In our case the role of predators will belong to cancer cells, the concentration of which we will designate with a letter n , and the role of the preys – to healthy cells; their concentration we will designate with a letterm . Note that we adhere to the same designations as in [5]. It is quite clear (see monograph [8]) that the interaction of any bodies with the EM fields can be different from zero only if the internal structure of the object under consideration allows to take into account its polarization p and magnetization m . However, if almost any object, including a cell, is under long-term exposure to constant EM fields, it will be certainly polarized. This means that, despite its extremely complex structure, there will be a slight deformation of the cell, which allows us to consider the polarization p . This means that we may take into account the possible interaction of cellular substance with a variable electric field E′(t ) , but only after the 0 E polarization of the cell is induced by the applied constant electric field. Such an interaction, attributed to a unit of volume, as it is known [8], formally has the form of a negative scalar product −p⋅E′ , where
Where αñ − is the cell polarization coefficient As for the magnetic field, if there are magnetic atoms in the cell structure in the form of, for example, iron, manganese or other magnetic particles, as well as moving charges, the energy of interaction with an external variable magnetic field will necessarily manifest itself H′(t ) in the same way as with an electric field, but already having the form of −m⋅H′(t ) where
This vector represents the magnetic moment of the cellular substance, χñ − is the magnetic susceptibility of the cell, and H0 − is the constant magnetic field applied to the body.
The account of interaction with the field will be given further phenomenological (see formulas (18), (19)) in the form of dependencies of coefficients b(t ) and c (t ) (see equations (5)).
Basic Equations and their Analysis
If we denote some average energy of the corresponding group of cells as 1,2 ε , then taking into account (3) and based on the results of [5], we can write the following expression for the functional we are interested in
Where functions Φ1,2 (n,m) are given in [5], and their explicit form is not important for us now.
Using the general method of deriving equations proposed in [9], we arrive as a result at the following system of two nonlinear equations that adequately describes our case:
Where a − will be considered a constant parameter, and we will need functions b(t ) and c (t ) further below.
As we can see, if we assume that b(t ) = 0 in the upper equation, we get the generalized Lotka-Volterra equation [3], [4], in which coefficient c (t ) is a function of time. And if we believe that c (t ) = 0 , then we get the generalized Verhulst equation (see [5]), in which coefficient b(t ) is a function of time [10].
Equations (5) also automatically take into account the condition of preserving the total amount of cellular substance in the body, that is,
Where μ1,2 − the masses of one healthy and one cancer cell are, respectively, M − is the total mass of the cellular substance, and V − is the volume occupied by it.
Based on the ratio (6), it is easy to find the time dependencies n(t ) and m(t ) that we are interested in. Indeed, expressing one of them by equation (6), for example m(t ) , we have
Where
After substituting (7) into the upper equation of the system (5), we arrive to the following solution
Where 2 C − is the integration constant, and the function
Constant 2 C is found from the initial condition n(0) = n0 . As a result
Substituting solution (9) into (7) now, we come to the following time dependence of the temporal behaviour of healthy cells:
As we can see from obtained solutions (9) and (12), the healthy and diseased cells behave quite adequately. Specifically, if the function is A(t ) = b(t ) −Gc (t ) > 0 , then the disease wins, because
In this case, the function A(t )must be such that condition (13) is fulfilled. As we can see from (9) and (12), in this case
And
At some point of “switching” function A(t ) = b(t ) −Gc (t ) changes sign, that is, it becomes negative ( A(t ) = b(t ) −Gc (t ) < 0 ) and we get the opposite picture. In this case, the disease recedes, and we come to equality
And healthy cells are restored, that is:
Now, as for the functions b(t ) andc (t ) . Due to the fact that the connection with the EM field has the form of a dipole interaction, then, based on purely physical considerations and the correct dimension of the equations, the form of these coefficients can only be as follows:
Where 1,2 a − the linear dimensions of diseased and healthy cells are, respectively, c S − is the contact area along the border line between them, and the dot above the letter means differentiation according to time.
Thus, function (10) of out interest, taking into account (1), (18) and (19), should be the following
Where β − is the angle between the direction of the external constant field and vectorE ′(t ) .
As we can see from (20), when changing the direction of the polarity of the fields, function A(t ) must change the sign to the opposite. By doing this, we achieve the opposite effect, that is, following the theory proposed above, there will have to be the destruction of diseased cells and the growth of healthy ones.
In this case, we may express function E′(t ) , for example, in the form of a linear time dependence, that is
Where γ − is a certain growth coefficient.
The Main Idea of the Work
The general physical considerations outlined above concerning possible methods of combating malignant tumours (and not only them, but many other similar diseases), allow, in our opinion, to select such variable fields and their amplitudes, which, in the process of reversal magnetization of their directions, will certainly lead to a positive therapeutic result.
Conclusion
Concluding this message, it is worth paying attention to two important points. The influence of variable EM fields on the reproduction of malignant tumours has been studied; It is shown that the proposed model quite adequately describes both the growth and disappearance of cancer cells, that is, the recovery of the body.
Invent a Removable Orthosis with the Ability to Prevent Foot Drop and Venous Thrombosis and Maintain Muscle Contraction
Introduction
From the perspective of the World Health Organization (WHO), health is the science and technology of disease prevention, providing medical services for immediate diagnosis, treatment and development to address problems. Safety is one of the most important aspects of health care systems [1]. Increasing the quality of work, consequently, increases the accuracy and improvement of the treatment process, the speed of the treatment process and also patient satisfaction [2]. Intensive care includes taking care of patients with life-threatening diseases, under the supervision of the most skilled personal, with advanced equipment and facilities, which includes all sensitive care related to the patient’s life [3,4]. A significant part of the treatment system’s effort is focused on being able to provide the best services to its patients in the shortest time and at the lowest cost. Intensive care units (ICUs) have an important place due to the high human and economic costs that they can incur for the health care system [5,6].
Patients with problems such as diabetic ketoacidosis, hypertensive emergency, non-accidental self-poisoning, heart failure, ischemic heart disease and cerebrovascular disease and respiratory conditions can be mentioned [7-9]. Numerous studies have been performed to identify the increasing mortality factors of patients admitted to the ICU. Infectious shock, age, smoking and nosocomial infections are among the factors that increase mortality in ICU wards [10,11]. A comprehensive study of UK hospitals showed that the mortality rate of patients admitted to ICU wards is about 20.6% [12] and that of Singapore public hospitals is 9.4% [13]. Complications of hospitalization in the Intensive Care Unit include foot drop, deep vein thrombosis[14], muscle atrophy [15] and so on. Venous thromboembolism (VTE), including deep vein thrombosis(DVT) and pulmonary thromboendarterectomy (PTE), is a public health problem that results in 250000 hospitalizations per year in the United States [16,17]. On the other hand, one hundred to fifty thousand people are hospitalized every year due to a benign and treatable disease, but die due to pulmonary embolism, while with prevention, the death of these patients can be prevented [18].
Risk factors for this disease are immobility, cancers, myocardial infarction, respiratory failure, surgery, trauma, obesity, use of female hormones and inherited coagulation disorders [19]. Another complication of hospitalization is “foot drop”. Foot drop or foot prolapse is a condition in which a person is unable to perform the dorsiflexion joint function properly due to weakness or paralysis of the anterior tibialis muscle or other muscles originating in the peroneal nerve. Foot drop can be unilateral or bilateral. Symptoms such as pain, weakness, and numbness are sometimes seen with this complication [20]. Diagnosis of this complication is easily possible by physical examination, but the use of imaging techniques and electromyography can also help to examine this complication more closely [21]. Today, there are various treatments to control foot drop, which considering the cause of this complication, the appropriate treatment method is adopted. Among the available treatments for prevention and correction of foot drop, physiotherapy, electrical stimulation and teaching the most common treatments using ankle foot orthosis [22].
Other complications of hospitalization in the intensive care unit include muscle atrophy [15], bed sores, etc. At present, according to the subject and results of research, one of the ways to prevent and reduce complications in hospital wards is to produce and use a mobile orthosis with the ability to prevent foot prolapse and venous thrombosis and maintain muscle contraction. In the following, we will talk about its structure. This idea has been registered in the Patent Organization of Iran under invention number 103769.
Methods
This project started with a new researcher idea Then by searching in the scientific content of articles and book, the title and proposal the project was compiled with opinion of the supervisor. Then model of the device was designed in collaboration with graphic & mechanical engineers Fianccy. The main tool was invented by the researcher. By mechanic engineer and solid work the design of this tool with professional software with academic-theorical proposal researchers (Mahmoudi and Mohammadbeik) about making a tool for the purpose of preventing foot drop, deformity of toes, muscles atrophy, improvement of blood return from distal to proximal organs and keep the function of vainvalves, assessment of vital signs and keep the power of foot solid muscles and prevention from muscels atrophy. This idea is designed by softwares and then the file of this designing was transferred to laboratory by researcher and work mechanic engineer in order to hardware designing and maquette. The structure of orthosis was discussed in terms of all angle’s morphology, measurement of figure based on standards and again after changing s figures and ,measurement was redesigned by software expert.
Figure 1: According to Figure 1
1. Orthotic body
2. Mechanical lock
3. Electric leads.
This mobile orthosis with the ability to prevent foot drop and keep the function of vain valve and assessing the vital signs is composed of (mechanical lock: 3×2cm, body: 40 cm length , pulse sensor: 0.5× 0.5 cm, pulse oximeter sensor: 0.5× 1 cm, inflatable inner layer R: 12cm, outer layer R: 15cm, electrical message transmitter leads: R: 1cm, insole: 25cm, removale hinge R: 2cm, connector between inner laye and air pump R:2cm. Orthosis is made up of upper and lower sections which after right locating(positioning) of foot in it, two sections will be connected to each other by mechanical lock (according to Figure 1, number 2). for motion of foot in its rang of motion (ROM), first removable hinge(according to Figure 7, number 11) is connected to monitor screen which is seprated from orthosis by a wire. all normative motion for foot’s motion(foot’s dorsal flexion, foot’s sole flexion,invertion , overtion) will be done by a program which is designed on screen and by choosing each motion, message will be transferred to removable hing(according to Figure 2, number 11) by a wire and by moving the orthosis, the foot moves in the desired direction and according to instruction given to program , the foot remains at desired posture for specified period of time (5s) and returns to its initial posture again.
Figure 2: According to Figure 2
1. 7- outer layer of orthosis
2. 8- inner layer of orthosis
3. 11- Removable hinges.
Figure 3: According to Figure 3
1. Air pump
2. LCD
3. Power on
4. Power off
5. Junction with interface.
Figure 4: According to Figure 4
1. 4- Connector
2. 5- Orthotics insole
3. 6-Upper part of orthosis.
Figure 5: According to Figure 5
1. Tens devices
2. LCD
3. Power on
4. Power off
5. Wire connection position.
Four foot motion (foot’s dorsal flexion, foot’s sole flexion, invertion and overtion) is done through a program which is programmed on the screen memory via removable hing, the duration of doing this motion, number of times, the amount of foot’s rest until next move. For preventing deep vein thrombosis (DVT) and maintaining the one way valve function, first the portable small air pump (according to Figure 3, number 1) which is available in the market is connected to the connector between air pump (according to Figure 4,number 4) and inflatable inner layer (according to Figure 2, number 8 ) by an air tube through transfering air from pump to inflatable inner layer the action of inflating and emptying takes place. Of course the number of times, intensity of wind pressure is defined by screen (according to Figure 4, number 6) available on pump’s body(according to Figure 3, number 1) and applied on foot, which this action causes standard pressure(17 mmhg) on one way valve and it causes continuity and helping blood circulation and prevents from the reduction of one way valve function.
Figure 6: According to Figure 6
1. 9- pulse Oximeter sensor
2. 10- Pulse Sensor.
Also electrical leads (according to Figure 1, number 3) are connected to the desired position (according to Figure 5, number5) by a wire and after connecting to tennes machine (impulse maker machine) by making impulses causes electrical stimulation of muscles and prevents muscles failure and atrophy that voltage intensity, duration of muscle stimulation, number of stimulation are controlled and done by screen (according to Figure 5, number 2) and planning is done. According to location of the sensor in the upper part of orthosis(according to Figure 6 , number 10) number of dorsal pedis pulse is measured and shown on the screen. Also by placing pulse oximeter sensor on the upper part of orthosis (according to Figure 6, number9), the amount of oxygen saturation is shown on the screen. By making movable orthosis and due to structure and muscle electrical stimulation prevents reduction of muscle contraction, atrophy and foot drop and causes maintaining valve function and the amount of oxygen saturation is studied through dorsal pedis pulse sensor and pulse oximeter sensor and can prevent the accurance of many diseases and the death caused by them.
Discussion
This research has been done in the field of medicine and medical engineering. Due to the extent of the foot drop and Deep vein thrombosis when providing medical care to the drug, the use of preventive equipment is felt to prevent this problem. Due to the innovative design of this design, Used to prevent ankle foot drop, deformity of the toes, muscle atrophy, improve blood flow from the lower to the upper and improve blood flow from the lower to the upper and monitor vital signs monitor vital signs and maintain the strength of the leg muscles. The advantages of this plan include moving the foot in four directions (flexion of the back of the foot and flexion of the sole of the foot and inversion and oversight), the ability to plan the number and time of movements, check vital signs in the lower limb, prevent reduction of contraction Muscles, preventing blood stasis and thrombosis in the lower extremities, preventing atrophy and muscles mass. Also, according to the research of Esfandiari et al (2017), a study entitled Literature Review of the Effect of Ankle-Foot Orthosis on Gait Parameters After Stroke [23] and Alnajar et al (2020), with Title Advances in neuroprosthetic management of foot drop [24] and prenton et al (2018), with Title FUNCTIONAL ELECTRICAL STIMULATION AND ANKLE FOOT ORTHOSES PROVIDE EQUIVALENT THERAPEUTIC EFFECTS ON FOOT DROP [25], and this research, the use of preventive equipment to prevent Ankle foot drop, toe deformity, muscle atrophy, improving blood flow from the lower to the upper and maintaining pigeonhole valve function and monitoring vital signs and maintaining leg muscle strength is suggested.
Results
Results of this study and other surveys can be one of the most effective ways to prevent prevent ankle foot drop, deformity of the toes, muscle atrophy, improve blood flow from the lower to the upper and monitor vital signs and maintain the strength of the foot muscles. Also using orothesis can decrease it significantly. Besides, modifying the preventive policies such as producing instruments like Removable orthosis is recommended. We are ready to work with all institutions and individuals in the fields of economics, education, research and health and startups for this idea. If you wish, please contact us via masoudmahmoudi515@ymail.com email.
Screening of Cervical Cancer in the Dakar Region by Cervico-Vaginal Smear: Epidemiological and Cytological Aspect
Introduction
The cervical smear (CSF) or pap smear is a collection of cells from the cervix for the early detection of any cellular abnormality that may suggest precancerous or cancerous lesions of the uterus [1]. Cervical cancer is one of the most common cancers in the world, particularly in women. Indeed, it is the 3rd most common cancer in women worldwide and one of the most common in our regions [2]. More than 80% of uterine carcinomas are found in developing countries [3]. Cancerous and pre-cancerous lesions of the cervix are therefore a real public health problem in many African countries like Senegal [4]. Cervical cancer is preceded by a long latency phase characterised microscopically by a broad spectrum of events ranging from cellular atypia to various degrees of dysplasia or cervical intraepithelial neoplasia (CIN) before progression to invasive cancer.
Method
This is a retrospective study of 2391 cases of significant cervical smears performed in the period from 01 August 2014 to 01 June 2016. This work was carried out at the Laboratory of Cytology, Cytogenetics and Reproductive Biology of the University Hospital of Dantec in Dakar. First, patients were registered in a register with an identification number, surname, first name, age, origin and telephone number. The interview is carried out before the sample is taken and focuses on marital status as well as gynecological and obstetric complaints and history. The sample is taken from a woman in a gynecological position by inserting a suitable speculum which exposes the cervix then use a cytobrush to take the actual smear by scraping the ectocervix and then the endocervix. Finally, two slides marked exo and endo respectively and the patient’s ID number are spread out. The slides were then fixed with a fixative, dried and stained using the Papanicolaou method. After the staining step, the slides were mounted and then read under the microscope. We wrote the reports in the computer. We used the computer and the register for data processing and were able to collect cases of smears that could be interpreted. All women with inflammatory and atrophic smears of menopausal origin were excluded from the study. The data were stored and analysed in Excel.
Result
We collected 2391 files. The mean age of the patients was 47.72 years with a standard deviation of 11.37 years. The most represented age (mode) was 40 years. Referrals from level 1 and 2 hospitals were 65%. The rest were referred by private doctors’ surgeries, by the pension institute and by some clinics. Patients referred for routine check-up without apparent clinical manifestation were 43.16%. The other requests were due to various clinical manifestations: metrorrhagia, primary or secondary amenorrhea, pelvic pain, dysmenorrhea’s majority of patients (51%) were married in a monogamous union. single women accounted for 14% of the total. The remaining 35% were in polygamous households. Patients with intraepithelial lesions were 7.27% and of these highgrade lesions (HSIL) represented 2.63%.
Discussion
The systematic analysis of the results of our study has provided us with important information on the epidemiological data of cervico-vaginal smears in Senegal. Indeed, after 22 months of data collection, the average age of the patients in our series was 47.72 years with extremes between 15 and 88 years. In Ethiopia, Mesele and his team found the same average age in 2010 (47.7 years), after 6 months of study [5]. This age generally corresponds to the period of genital activity in most women. Epidemiological studies have shown a strong correlation between sexual age and certain infections, particularly HPV [6]. Patients were sometimes referred by various public (more than 65%) and private health structures. This can be explained by the relatively affordable cost of this examination in our center (less than 10 euros) compared to private facilities that perform the same examination. Our countries have very little universal health coverage, in contrast to several countries in the North, where the uptake of screening is greater but limited in some areas by disparities [7]. Patients living in the outskirts of Dakar were 53.47%.
The departments of Pikine and Guédiawaye account for more than 50% of the population of Dakar [8]. We therefore believe that increasing the number of public screening facilities in the suburbs of Dakar would probably increase adherence to routine screening. These results are in contrast to those obtained by Diallo and his team who showed 20 years ago that in the absence of functional urogenital signs, women rarely consulted health facilities in Senegal for early detection of cervical lesions [4]. In France, the Haute Autorité de Santé recommends systematic screening for precancerous and cancerous cervical lesions by cervico-vaginal smear every 3 years in women aged between 25 and 65 years [9]. We thus note that education, information and communication about cervical-uterine diseases are fundamental to their prevention. Of the patients screened who were in a monogamous union, 51% were in polygamous households compared to 35%. Polygamy is a major feature of matrimonial systems in sub-Saharan Africa. It is underpinned by cultural and religious perceptions [10].
Studies have shown a major preponderance of HPV infections in non-monogamous spouses, even in developed countries [5,6]. Our study also looked at the parity of women. Indeed, 8.67% of them had more than 5 children. High parity appears to be a very important risk factor for the occurrence of cervical cancer. Studies in Ethiopia, Costa Rica and Thailand found a higher incidence of cervical cancer in women who had more than five children. Weakening of the cervical mucosa, which reduces the spontaneous elimination of HPV, could explain this link. Other studies in Denmark and Manchester found no association between parity and cervical cancer incidence [5,11,12]. Patients with dyskaryotic cyto-morphological abnormalities of the cervical intraepithelial neoplastic type were 7.27% with 4.64% low-grade intraepithelial lesions (LSIL) and 2.63% high-grade intraepithelial lesions (HSIL). In 20 years, we have seen a very significant reduction in the rates of dysplastic lesions, which were estimated to be 20.54%, of which 17.56% were low Bethesda smears and 3.36% were high-grade smears [4]. Studies have shown that 12% of LSIL can develop into invasive cancer, compared with 1% of HSIL [13]. However, only histology after colposcopy of the lesions could confirm its cytological abnormalities.
Conclusion
Thanks to the work undertaken by Papanicolaou since 1928, gynecological cytology has proved to be of prime importance in the fight against and treatment of dysplastic lesions, and in raising the awareness of health workers, government officials and the education of women in Senegal.
Investigation of the Effect of Indoor Airflow on Separation of Coronavirus from Ambient Contaminated Surfaces
The Coronavirus disease 2019 (COVID-19) is a devastating challenge for many countries worldwide. A new class of Coronavirus, known as SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2) has been found to be responsible for the occurrence of this disease. According to the World Health Organization (WHO), the disease is rapidly spreading around the world, and, to date, the virus has affected more than 200 countries, causing severe health, economic, and social disruption to the entire human population [1]. There are two modes of transmission: the first is through respiratory droplets, while the second is through contact routes [2-4]. Respiratory droplet transmission is due to coughing or sneezing by an infected person to a healthy person. This type of transmission can be avoided by keeping a safe distance between people, and by not coughing or sneezing in open air [5] Another form of transmission is through contact route, in which the infected person somehow transmits the virus onto a surface and infects healthy persons through various mechanisms, such as the airborne contaminations considered in this investigation. This type of transmission depends upon surface stability, which is the duration of time a material can hold the virus. The Coronavirus can sustain itself up to 72 hours on surfaces like plastic and steel [6,1]. One of the principal uncertainties is related to how COVID-19 is transmitted, especially the factors which may accelerate or delay its spread. These factors include the mode and speed of transition, and interaction of Coronavirus with surfaces such as landing, attachment, survival and detachment. This is particularly important in indoor spaces, where density of people, availability of open surfaces, and circulating airstream can possibly increase the risk of infection. In this regard, World Health Organization (WHO) believes it is urgent to investigate the transmissibility of Coronaviruses from contaminated surfaces [7]. Very recent case studies in localized outbreaks of COVID-19, such as the Diamond Princess Cruise ship in Japan, some restaurants in China [8], and some Call Centers in South Korea [9], have shown that contaminated surfaces in indoor spaces are potential sources for spreading the Coronavirus. In the United States, Centers for Disease Control and Prevention (CDC) believes that because respiratory droplets can land and survive on some surfaces, it is possible that surfaces could be a real issue in transmission of COVID-19 (CDC, 2020). In fact, due to the lack of information, the mechanism by which a contaminated surface spreads the Corona virus is not clearly understood. It is crucially important to study whether the main cause of the Coronavirus spread is separation from surfaces by indoor airstream or touching of the contaminated surfaces.
The potential of viral spreading via contaminated surfaces depends particularly on the ability of the virus to maintain infectivity whilst it is in the environment. This is affected by a combination of biological, physical, and chemical factors. Rapid spread of viral infections through contaminated surfaces is common, particularly in crowded indoor establishments, such as schools, day-care facilities, nursing homes, business offices, hospitals, and transport systems [10]. Interactions that take place between viruses and surfaces are determined by their characteristics, which involve electrostatic, hydrophobic, and/or ionic strength of the virus [11,12]. Therefore, it is necessary to systematically investigate how ambient airflow influences the contaminated surfaces. Viruses are believed to be the most disinfection-resistant microbial pathogens [13]. Therefore, a better understanding of how they relocate and attach to surfaces is very important. In this regard, one of the significant factors that governs the spread of a virus is how it interacts with surrounding surfaces and the strength of the virussurface bond. This is especially important in indoor spaces such as hospitals, classrooms, offices, etc. When a virus lands on a surface, a variety of bonds can play role(s) in virus-surface interactions, such as electrostatic bonds, hydrophobic bonds, Van der Waals bonds, hydrogen bonds, charge-transfer bonds, and biospecific bonds [14]. In this list, electrostatic interaction has been recognized as the dominant factor for virus-virus or virus-surface interactions [15-19]. Viruses are colloid-sized particles composed of capsid proteins encapsulating infectious genetic material (nucleic acids). The surface charge on viruses is caused by ionization of the typical amino acid groups.
Surface functional groups on these amino acids are dominated by carboxyl and amine groups, which yield viruses with amphoteric surfaces and pH values ranging from 3 to 7. Therefore, viruses may be positively or negatively charged [20]. Many studies have been performed to measure the force needed to detach a virus from a surface. Several techniques have been developed for measuring forces between biological structures, including mechanical springs made from glass fibers [21], vesicle-based force transducers [22], optical tweezers [23], and surface–force apparatus [24]. These methods have sufficient sensitivity (0.01–1 nN ) to detect the intermolecular forces between protein bindings but lack spatial resolution. Atomic force microscopy (AFM) has been extensively used to measure the adhesive force of the protein-based structure of a virus to the surface. The major advantage of AFM over these other techniques is its spatial resolution and lateral resolution, which is of paramount importance at micron and nanoscales [25]. The average adhesion force of proteins (including Coronaviruses) to different surfaces has been reported from 44 up to 250 pN [26], 140 to 180 pN (ROHDE, 2020), and 257±25 pN [27]. The adhesion force between a surface and a protein-based structure can change due to a variation of many parameters such as the type of protein, pH, the morphology, and the materials of the surface. In this study, the average adhesion force of a virus to a surface (Fa) is considered between 40 and 140 pN . Moreover, Coronavirus virions are assumed spherical, with diameters of approximately 125 nm, as depicted in recent studies by cryo-electron tomography and cryo-electron microscopy [28-30].
SARS-CoV-2 viruses could be spread in the surrounding air due to the regular human activities such as exhaling, sneezing, coughing, talking etc. The virus can be considered airborne until the time that it deposits onto a surface. There have been several studies that investigated the motion and spread of the suspended viruses in air before their deposition on surfaces [31-34]. Deposition of the airborne particles on surfaces depend on different factors including the size, shape, and weight of the particles, and the velocity and direction of airflow (flow pattern) [35,36]. Numerous experimental and theoretical investigations have been conducted to study the conditions of particles’ deposition on solid surfaces [36-41]. Once the particles settled on a surface, the resuspension of the particles depend on the application of external force to detach the particle from the surface. Studies show that about 70% of the aerosol particles and droplets settle on the surfaces and walls. There have been several studies, which linked the transmission rate of SARS-CoV-2 viruses to the direct contact of the humans with contaminated surfaces [42-44]. However, if the indoor airflow could cause the resuspension of the SARS-CoV-2 viruses, then it increases the chance to be inhaled by the occupants in the vicinity of the surfaces.
This study focuses on the effect of airflow (the speed of air current flowing through indoor spaces) on transmissibility of the Coronavirus. Its aim is to investigate whether or not the Coronavirus can be dispersed from a contaminated surface into the air and transferred onto a new surface. The findings of this study can help us to have a better risk assessment of being in closed spaces, where Coronavirus contaminated surfaces exist. In this regard, regular surfaces in a typical building are simply modeled in two major categories, including flat plates and circular cylinders. Furthermore, the effect of surface roughness has been considered in the models. Three main categories of materials were considered in this study including glass, steel, and wood, with mean roughness values of 1,46, and 183 μm respectively [45]. Based on the ASHRAE standards [46], the velocity of air in a room depends on the various factors such as the floor area, height of the ceiling, cooling or heating purposes, number of occupants, and types of the buildings. However, regardless of the mentioned factors, generally, the goal is to keep the indoors air velocity below 0.25 ms-1 for cooling and less than 0.15 ms-1 for heating. Moreover, the duct design standards of ASHRAE, holds the limitation of 12.6 ms-1 of the maximum airflow through the ducts with different shapes [47]. A study by Gong et al. suggests that the acceptable air velocity range for local air movement, is between 0.3 and 0.9 ms-1 [48]. In this study, five different velocities including 0.1, 0.5, 1, 5, and 10 ms-1 were considered in order to cover the overall range of indoor airflows from regular applications to the very unlikely extreme cases. The indoor air flows have random directions, and the stagnant areas are also common; therefore, the exposure of the surfaces to the airflow varies with that regard. In this study, it was assumed a fan controlled the direction of the airflow with respect to the surface. In this regard, three conditions were considered: airflow parallel to a flat surface, perpendicular airflow toward a flat surface, and airflow over a circular cylinder.
Methodology
Airflow towards a Flat Plate
A condition can be considered, in which air flows toward a flat surface (e.g. fan blowing toward a screen, see Figure 1). If the direction of the airflow is perpendicular to the flat surface (Figure 1), the resulted momentum force on the surface is calculated from the following [49]:
Figure 1: Schematic of the momentum impact of the fluid flow perpendicular to the plate.
Where, FV (N) is the normal momentum impact on the area attacked by the fluid flow. The negative sign in Eq. 1 means that FV is in opposite direction to the incoming fluid jet. UA (ms-1) is the velocity of the air flow in x direction. ρ = 1.204 kgm-3, is the air density at T = 20°C, LA (m) is the thickness of the jet, and b (m) is the width of the plate in Z direction. Considering Eq. 1, FV is calculated based on the area of attack, LA×b. By assuming that LA =b = 1cm (the approximate area of the tip of a fingerprint), the calculated momentum impact with respect to the array of the applied velocities, U = {0.1, 0.5, 1, 5, 10} ms-1, was calculated. By modeling a Coronavirus as a sphere with diameter of D = 125 nm (Fehr and Perlman, 2015), the surface area of a virus is Therefore, viruses can be fitted in an area of the tip of a fingerprint (A=10-4 m2). By assuming that, the whole area covered by n number of viruses, the momentum impact on each virus was calculated by:
A viscous region with thickness of LB=LC forms along the flow in y direction in Figure 1.The analysis of the flow in those regions are similar to the boundary layer of a laminar flow parallel to the horizontal flat plate. If the airflow hits an inclined flat plate with the angle of β, the resultant momentum force is less or equal to the perpendicular air flow jet (β=0).
Airflow Parallel to the Flat Plate
Figure 2 shows the schematic of the flow over a flat plate. By assuming a one-dimensional flow (U>>V) over the plate, at room temperature as T = 20°C, and atmospheric pressure, the 2-D Naiver- Stokes equations for laminar, incompressible, steady state flow (Eq. 3) was solved with finite difference method.
Figure 2: A schematic of the parallel laminar airflow passes over a horizontal flat plate in macroscopic and microscopic scales (a model for a desk).
The nodal network considered as square with Δx=Δy=1μm. The boundary conditions were as in the following:
The assumption of non-slippery wall boundary condition was made based on the calculation of Knudsen number, Kn = λ/L, where λ is the mean free path of the gas (in current case, air at atmosphere pressure, λair = 68 nm) and L is the length-scale of the flow (in current case L=1cm). Based on theory [45], if Kn is significantly smaller than one (in current case, Kn =68×10-7), the wall can be considered nonslippery. The wall shear stress can be calculated with the Blasius exact solution for laminar boundary layer as the following:
The production of the surface area of a virus and the wall shear stress resulted from the airflow provides a good estimation of the amount of force applied to a single virus attached on a flat plate. Two assumptions were applied in this calculation (Eq. 5); first, the wall shear was calculated without considering the existence of a virus. Moreover, it was assumed the shear wall was applied 62.5 nm above of the flat surface at the equator of the sphere (see Figure 3).
Figure 3: Force acted on the virus attached on a flat surface.
The Effect of the Surface Roughness on the Force Applied on a Single Coronavirus
The mean roughness value is specifying and comparing the height difference between the peaks on an otherwise smooth surface or troughs of the same amplitude. The nanometer-scale viruses with unknown numbers can randomly occupy the entire peaks and valleys of a surface. On the other hand, the shape, height, and the number of micrometer-scale bumps and troughs are random on a rough surface (Figure 4). In order to investigate the effect of the roughness on vulnerability or resistance of an attached virus against the airflow, two models are considered. The models were considered based on Dejaguin method [50], which has been widely practiced for particle resuspension studies [51,52].
a) Model 1: Ziskind showed that particles tend to occupy stable positions. Therefore, if the roughness of the surface is greater than the particle sizes, the particles mainly occupy the vacant areas between the peaks. Those picks which surrounded the particles were actually protect the particles from the applied external flow rates and decrease the resuspension rate of the particles significantly. We assumed that the viruses were accumulated in a sharp corner or valley and attached there (Figure 5). Based on the Falkner-Skan solution of the inviscid flow passing corners [45,53], the maximum velocity that a fluid can reach into a valley is umax=0.9999 uin. The velocity in the valley depends on θ as shown in Figure 5; however, regardless of the shape of the valley, it cannot reach a value higher than umax. This means the viruses will be protected against the airflow inside the valley and will be less vulnerable to the airflow in comparison to the situation in which the virus are attached on the plane plate. Deeper in the valley, the re-circulating eddies form making the velocities even smaller in comparison with the velocity on the flat plate ().
b) Model 2: In this model, it is assumed that an isolated virus attached to a single peak next to a perfect plane plate under the influence of the air flow. The peaks and valleys of a rough surface work like obstacles and decrease the velocity of the flow passing through them. It can be concluded the most vulnerable condition for a virus against the attacking flow occurs when it is sitting at the top of a peak. (See Figure 6). The solutions of 2-D Naiver-Stokes equations with finite difference method, provide the value of the velocity vectors at each node with any desirable height. Moreover, by assuming the height of a peak (H) is equal to the mean roughness (Ra) value of a material, the amount of the drag force, which is applied on an isolated virus at the peak can be calculated by Stokes’ sphere-drag equation:
Figure 4: The random number of valleys and peaks with different heights and depths form a rough surface,
a) smooth surface of a glass sample
b) rough surface of a steel sample.
Figure 5: The schematic of the viruses attached in a shallow crevice.
Figure 6: The schematic of an assumption that a single virus attached at the peak of a rough surface just next to a perfect plane plate in order to guarantee the extreme possible vulnerability of a virus against an undisturbed airflow.
where U is the applied velocity, μ=1.825×10-5 Pa.s is the dynamic viscosity of air at T=20°,P=1 atm, and r=62.5 nm is the radius of a Coronavirus. The Stokes’ equation is valid if ; however, for the airflow over a Coronavirus the Knudsen number is . In this situation, a slip correction factor is needed to be considered to adjust the Stokes’ drag force [53,54]. By calculating the Cunningham slip correction factor (Cs) [54,55], the corrected drag force is equal to is as the following:
Where A1=1.257, A_2=0.4, and A3=0.55 are empirically determined constants [56,57] Cs is 2.53 and therefore, the calculated drag forces are needed to be divided by 2.53 to count for non-slippery condition; however, in order to increase the margin of safety and work with the higher values of applied forces on a modeled virus and roughness, the Cunningham correction is not considered in the current study.
Flow Over a Cylinder
Door handles are among the most touched surfaces in a room and their contamination with Coronaviruses are very likely. A typical door handle can be modeled as a circular cylinder with the diameter of 2.5 cm. It was assumed that the freestream wind velocity in x direction, U∞, is much greater than two other velocity components, V and W. The Reynolds number of the different air flows pass the cylinder with applied velocities of U∞ = {0.1, 0.5, 1, 5, 10} ms-1, at T = 20°C (ν = 1.516×10-5 m2s-1), are far less than the critical Reynolds number, ReD,C = 250,000, which guaranties the laminar flow regime around the cylinder. The Hiemenz’s polynomial velocity distribution [46] was considered for calculating the boundary layer with finite difference method.
Where, x^*=x⁄r is the dimensionless arc length and r is the radius of the cylinder. By considering x as the tangential and y as the vertical directions on the surface of the cylinder, a domain was defined like shown in Figure 5. The domain was considered for 2-D finite different solution of Naiver-Stokes equations on the cylinder. Based on Hiemenz model, the separation point takes place at ∅_ sep≈80.5°; therefore, the domain in x direction was considered as while and Δy=1 μm. Higher freestream velocities result in smaller thickness of boundary layers; therefore, the domain of 0 ≤ y ≤ 25 mm was considered for U∞=0.1,0.5 ms- 1,while 0 ≤ y ≤ 2.5 mm was taken for U∞=1,5 and 10 ms-1. The two-dimensional, steady, laminar, incompressible boundary layer equations at constant temperature and pressure are the same as Eq. 3-a and 3-b. The boundary conditions of the system were as the following:
Momentum Impact of the Airflow Perpendicular to a Plane and Rough Plate
The adhesion force (Fa) between a Coronavirus and a solid surface is estimated as 40 140 a N ≤ F ≤ p . The applied forces on a Coronavirus with respect to the jet velocities are shown in Table 1. Considering the values of the applied forces due to the perpendicular airflow jets, even for the extreme case of , is far less than . Therefore, it is very unlikely that such vertical airflowjets cause any movement or removal of a Coronavirus from a plane plate. Since the direction of the jet flow is perpendicular to the surface, the two roughness models in this study do not play a significant role. If model 1 is considered, the airflow should impact a virus in a sharp corner which is less vulnerable to the applied force at the plane plate. On the other hand, if model 2 is considered, the condition of a virus located just a few micrometers closer to the airflow jet makes no difference in compression with the condition of the attached virus on a plane plate.
Table 1: Momentum impact of the vertical airflow jet on the 1 cm2 of a plane plate and a sphere-modeled Corona virus with D=125 nm.
The Force Applied to an Isolated Virus Resulted from the Parallel Airflow to a Plane and Rough Plate
Considering the exact solution of Blasius for a laminar flow over a flat plate (Eq. 4), the wall shear stress leads to infinity at x=0. This means if a virus is attached to the edge of the plate x=0, it will be removed from the surface regardless of the free stream velocity of air. If a Coronavirus is attached at x=1 nm on a plane plate, then the wall shear for the highest velocity of airflow, U=10 ms-1, is W τ =1.56 kPa which leads into FD2=76.4 pN . This value indicates that the movement of a Coronavirus at x=1 nm is still possible with such an applied velocity. However, 3 nm further, at x=4 nm, the movement of virus becomes very unlikely since FD2 (x=4 nm) =38.2 pN for U=10 ms-1. It is also very important to consider the fact that experiencing velocities like U=5 or 10 ms-1, is extremely unlikely in a building and such velocities exist only inside the big air canals. Even for the extreme case of U=10 ms-1, only at the first 3 nm from the plates’ edge, an isolated virus is vulnerable to movement or removal from the surface. Figure 7 shows the magnitude of the force, D2 W s F =τ × A , applied on an isolated virus due to the wall shear at the first 100 nm of a plate from its edge for 2 free stream velocities of U=5 and 10 ms-1. The max value of FD2 for different applied freestream velocities at x=1 nm are shown in Table 2.
Figure 7: Magnitude of the forces applied on an isolated virus due to the shear stress on a plane plate in the first 100 nm from the edge of the plate.
Table 2: Force applied on an isolated virus located at x=1 nm from the edge of the plane plate due to shear stress.
Considering Figure 6, since the peak-height of the smoothest material, glass, with Ra=1 μm, stands outside of the boundary layer at x=0, the applied free stream velocity will hit the isolated virus at tip of the bump (see Figure 8a). The Stokes drag forces (Eq. 6), which applied on a virus due to the different applied free stream velocities are shown in Table 3. The force values in Table 3 show that even for the unreal extreme model 2 case (considering an isolated virus at the peak of a rough surface), at unlikely position of the edge of a plate (x=0), it is impossible for regular air velocities in a building to overcome the adhesion force (Fa) between a single Coronavirus and a solid surface. However, the results show that for extreme applied velocities with consideration of all extreme assumptions, it is possible for the airflow to move the virus from the edge of a flat surface. In this study, the highest peak of a rough surface is wood with Hwood=183 μm. The thickness of a boundary layer depends on the applied free stream velocity. Higher velocities result in boundaries with steeper edges and smaller thicknesses, δ. Therefore, in order to keep the peak of the rough surfaces inside the boundary layer, the peaks should be considered further far away from x=0 with respect to the applied free stream velocities. For U=10 ms-1, the first point at which the wood-peak will be located inside the boundary layer is at x=346 μm.
This is the furthest point among all applied velocities. Inside the boundary layer, the velocity of each node can result in a drag force applied on a single Coronavirus at the peak of a rough surface (see Figure 8b). The x-component velocities (u) versus x are depicted in Figure 9 at y=183 μm through the entire domain, 0 ≤ x ≤10 mm, for U=1 and 10 ms-1. The trends of the graphs for the other applied velocities are the same, but the (u) values are different. It is clear in Figure 10b that during the first 346 μm, the peak of a rough wooden surface stands outside the boundary layer u=U=10 ms-1. The average applied drag forces due to the x-component velocities at y=1,46 and 183 μm for all cases in the domain of 0 ≤ x ≤10 mm are summarized in Table 4. The possibility of the movement of an isolated virus from the peak of a modeled rough surface is relatively high for the free stream velocities of U=5 and 10ms-1 in 1 cm distance from the edge of the plate. However, it is very unlikely the other applied velocities cause the removal of the virus from the peak in that domain. The applied drag forces with respect to the free stream velocities in Model 2 of the roughness at x=10 mm, are summarized in Table 5. It is obvious that the movement of the virus is only possible for U=10ms-1 on the wooden-surface at x=10 mm. This means that within 1 cm distance from the edge of the plate, the displacement of an isolated virus is possible for freestream velocities equal or higher than U=10 ms-1, which exceeds the common indoors air velocities.
Figure 8: The condition of the peak of a rough surface with respect to the boundary layer.
a) at x =0, the green peak, all the peaks stand outside of the boundary layer.
b) The peaks (e.g. the orange one) of all three materials are inside the boundary layer at x ≥ 346 μm for all the applied free stream velocities.
Figure 9: Schematic of the laminar airflow passes the circular cylinder and the defined domain in order to study its boundary layer.
Figure 10: The velocity components in x direction at y=186 μm above the flat surface, representing the peak of a wooden rough surface, for two applied velocities
a) U=1 ms-1, and
b) U=10 ms-1
Table 3: The magnitude of force applied on an isolated virus attached at the peak of a rough surface at the edge of the plate (x=0 nm) outside the boundary layer.
Table 4: The average applied drag force due to the x-component velocities at y=1, 46 and 183 μm for all applied free stream velocities in the domain of 0≤x≤10 mm.
Table 5: The applied drag force due to the x-component velocities at y=1,46 and 183 μm for all applied free stream velocities at x=10 mm.
The Force Applied to an Isolated Virus Resulted from Airflow Over Plane and Rough Circular Cylinder
he Hiemenz velocity distribution model (Eq. 8) indicates that the maximum free stream velocity, U(x*), takes place at ∅=71.2° regardless of the applied U∞; however, the maximum wall shear stress forms between ∅=50°-60° for different applied U∞. Figure 11 shows how the boundary-layer profile forms along the curve from the stagnation point for every Δ∅=20° until it reaches its separation point at ∅sep=81°. The favorable gradient increases the wall shear stress up to ∅=60°. Figure 12 shows the shear wall profile of the U∞=1 ms-1 over the cylinder model. The trends of the shear wall profiles around the cylinder are as the same as Figure 12 for all five applied U∞, but the maximum values and their point of occurrences are different (Table 6). Even for the highest applied velocity U∞=10 ms-1, the drag force on an isolated Coronavirus is less than the adhesion force. Considering Figure 6, it would be necessary to figure out about the velocity profiles at y= 1,46 and 183 μm, which represent the peak of the glass, steel and wood surfaces inside the boundary layer around the cylinder (model 2). Having the velocity profile at each height, the max velocity will be considered in order to calculate the highest possible applied drag force on an isolated virus at the peak of a rough surface (FD3). Figure 13 Error! Reference source not found. shows the velocity profile of U∞=1 ms-1 at three desirable heights. The maximum velocity takes place around Φ=50°. The trends of the graphs for the other applied incident velocities (U∞) are the same with U∞=1 ms-1; however, the resulted velocities at each peak inside the boundary layer varies with respect to the applied incident velocities.
Figure 11: Velocity profile of the laminar flow pass a cylinder with free stream velocity of U∞=1 ms-1 based on Hiemenz model at four different arc ranges Δ∅ = 20°,40°,60°,80°.
Figure 12: Wall Shear profile on a cylinder exposed to the laminar external air flow with U∞=1 ms-1.
Figure 13: Velocity profiles in x direction at y= 1, 46, and 183 μm, representing the applied velocity at the peak of the three rough surfaces: glass, steel, wood consequently.
Table 6: The locations where the maximum wall shear stress takes place on the surface of a cylinder exposed to the laminar airflows with the various U∞ and its representative force with respect to the surface area of an isolated corona virus modelled as a sphere (AS).
Table 7 shows D3,max F values, it also indicates that only in the case of U∞=10ms-1, the maximum velocity at y=186 μm (wood model) within the boundary layer will result in a drag force of D3,max F =55.75 pN . Such a drag force may cause the removal of an isolated Coronavirus from the peak. Considering the extreme rareness of such an incident velocity in a room, it can be concluded that it is very unlikely that the regular airflows over the cylindrical shape objects (e.g. door handle) can cause the movement or removal of Coronaviruses from a surface.3.4 Verification of the obtained results. The mean roughness value of the surface in addition to the size of the particles specify the adhesion force between the particle and the surface and also determine the effect of external flow on the particles. However, it has shown in several research papers that when the size of particles are reduced from micro- to nano-scale, the topography of surfaces and the dimension of the particles play more important role in determination of required drag force for resuspension rather than the types and materials of the particles [58].
Table 7: Maximum possible drag forces, which resulted from the velocity profiles around the circular cylinder, applied at an isolated virus at the peak of three rough surfaces: glass, steel and wood.
Ziskind, Ibrahim et al, Jiang et al, Mukai et al., and Soltani and Ahmadi showed that for given flow and surface conditions the size of the particle plays the most important role in detachment [59-62]. Kim, and Corn and Stein showed that by decreasing the size of the particles the required drag force for resuspension of them increases significantly [63,64]. Therefore, due to the very small size of the SARS-CoV-2 viruses, it is justifiable to consider the experimental studies which conducted on the particles with the same sizes as the virus. Hubbe showed in his experimental studies that the required shear stress for detachment of TiO2 particles with diameter of 144 nm is about 200 Pa [65]. Considering the diameter of a Coronavirus, dp =125 nm, it can be concluded the applied shear must be greater than 200 Pa in order to detach the Coronavirus from the plane surface. Based on the analytical calculation provided in our study, the wall shear stresses resulted from the applied free stream velocities of U = 10 and 5 ms-1 can only reach over 200 Pa at the first 20 nm of the edge of the flat plate.
Such a conclusion can be made by only comparing the wall shear values and the obtained experimental results from other studies. In our studies, we concluded that the only first 4 nanometers from the edge of the flat plane can be regarded as a potential region for resuspension when U=10 ms-1 was applied [66]. showed in their experimental studies that the glass particles with the diameter of between 1-10 μm on hardwood and vinyl flooring were not detached by the applied freestream velocities less than 18 ms-1 [66]. Corn and Stein observed that the velocity up to 117 ms-1 was required for resuspension of glass particles with the diameter of 10.6 μm on smooth glass surfaces and Jiang et al. found that velocities greater than 50 ms-1 were necessary to resuspend 11 μm poly (methyl methacrylate) (PMMA) particles [67,68] gathered a wide range of experimental studies indicating that an average velocity of 25 ms-1 is required for resuspension of micro-scale particles from different surfaces [69]. Such experimental results support the provided conclusion in our study since for nano-scale size of a Coronavirus even greater applied velocities are required than the ranges suggested based on experiments in previous studies for micro-scale particles.
In addition to the technical fluid mechanics studies, the new experimental studies in real situations are in strong agreement with the conclusions of our model. For example, [70]. investigated the risk assessment of viral transmission of SARS-CoV-2 viruses from the contaminated surfaces due to the indoor airflows [70]. In their comprehensive study of Shanghai Public Health Clinical Center with 115 rooms, they concluded that the indoor airflow could not resuspend the SARS-CoV-2 viruses from various contaminated surfaces. They collected samples from floors, walls, washbasins, furniture, medical and personal protective equipment surfaces, as well as air samples, from airborne infectious isolation rooms. They also collected air samples from 15 rooms and areas close to the surfaces. They found no SARS-CoV-2 virus in the air close to the surfaces which all exposed to air supply from the air conditioning system in the rooms. Moreover, they collected surface samples from air exhaust and HEPEA filters and failed to detect any virus. Similarly, air samples collected in the corridor or the changing rooms of the semi-contaminated area did not show any presence of the virus. They finally concluded the risk of airborne transmission of SARS-CoV-2 in airborne infectious isolation rooms was low (1.62%) due to the directional airflows.
Many other studies have been conducted since the beginning of the pandemic, which do not directly verify the obtained results of our model; however, they show almost no evidence of the resuspension and spread of SARS-CoV-2 viruses due to the indoor airflows. For example, in a research study regarding the virus transmission in plane cabins, [71] concluded that in the regularly ventilated cabin, those who seated near the windows were subject to less infectious particles. [72] In their review and interpretation of [73]. investigation showed that despite the existence of the contaminated surfaces like windows, seats, laptops etc., the nearby passengers did not get infected by the viruses, while the direct air supply from the ceiling air inlets continuously reached those surfaces [74]. Some other studies like modeling study of the COVID-19 outbreak on the Diamond Princess cruise ship by Huang, et al. [75], or the epidemiological and modelling study of the COVID-19 transmission in train passengers by Hu et al. show no evidence of resuspension of the SARS-CoV-2 viruses due to the indoor airflows [76-80].
Conclusion
In this study, the effect of the indoor air circulation on the separation of a Coronavirus from surfaces was investigated. For this purpose, different configurations of the surface models with respect to the directions of airflows were considered. Regarding to the results, the following conclusions were made. In the case, where airflow applied perpendicularly on a flat plate, even for the highest applied velocity (10 ms-1), the separation of a Coronavirus is unlikely. The indoor parallel airflows to the flat surfaces have low potential to remove attached viruses in most of the conditions. In the case of the plane plates, at the edge of the plate, the applied shear is infinity due to the Blasius equation. At locations more than 4 nm away from the edge, even for the highest applied velocity (U=10 ms-1), the drag force applied on an isolated Coronavirus is less than the minimum adhesion force. In the case of the rough plates, at the edge of the plates, all of the modeled peaks are protruding out of the boundary layer. Therefore, the drag force was calculated on an isolated Coronavirus considering the freestream velocity. For three cases, where the free stream velocities were 0.1, 0.5 and 1 ms-1, the separation of a Coronavirus was unlikely. For two other cases, U=5 and 10 ms-1, the drag forces were 107.5 and 215 pN , respectively. Therefore, the viruses were vulnerable to removal. In the regions, a few micrometers away from the edge of the plate, where the peak of a rough model stood in the boundary layer, the applied drag forces were negligible for all the rough models except for U=5 and 10 ms-1. In the case of U= 10 ms-1 applied on the wooden-surface; the possibility of the virus movement was high since the minimum drag force in the domain of 1 cm from the edge was more than 100 pN .
For plane surface of a cylinder, the calculated drag forces were less than 1 pN for all applied velocities; therefore, the separation of an isolated Coronavirus was extremely unlikely. In the case of the airflow over the rough circular cylinders, most of the calculated drag forces were less than 40 pN, except for U= 10ms-1) applied on the wooden-rough model at ϕ=50°, which was 55.75 pN . Therefore, the separation of a Coronavirus from a rough cylindrical surface is very unlikely. Overall, it is very unlikely that typical indoor airflows could remove Coronavirus from different surfaces. The separation of viruses may take place at very high air velocities (e.g. 5 and 10 ms-1), at locations such as edges of flat plates or at specific angles with respect to the horizontal plane (ϕ=50°) on cylindrical surfaces.
Auxiliary Device for Full-Arch Digital Scans in Edentulous Jaws
Introduction
Digital impression is not a procedure in itself but represents the first step in a “new” way of conceiving the prosthetic procedure: the digital work-flow. Intra-oral scanning (IOS), Computer Aided Design (CAD) and Computer Aided Milling (CAM) make it possible to avoid the conventional procedures with a significant reduction in production times. Digital technologies are radically revolutionising the prosthetic approach in both clinical and laboratory aspects [1-6]. To date, in implant-supported dental prostheses, scientific literature has validated the use of IOSs for capturing optical impressions for the design and manufacture of short-span restorations such as single crowns (SCs) [7-10] and partial prostheses (PPs) [11-13]. However, in case of long-span restorations, in particular full arches (FAs), IOSs do not yet seem to be sufficiently accurate, as reported by several studies [14,15] and reviews of the literature [16,17]. Although some studies claim that optical systems provide sufficient accuracy in complete-arch impressions, scientific evidence on the intraoral scanning of complete-arches with teeth is lacking and outdated [17]. Elastomeric impressions of complete arches are significantly more accurate than those of optical arches [18] and the precision of intraoral scanners decreases as the distance between each scan body increases [19-21]. As the free scanning area increases, the intrinsic imprecision of the procedure increases, with progressive distortion of the impression and, consequently, a reduction in accuracy.
Edentulous arches, in particular the lower arch, represents still today a challenge for the optical impression: it is confirmed by the evaluation of full arch scans obtained with different scanning systems compared to data obtained with traditional impression. Taking impressions using elastomeric materials to capture dental implants position is still the most widely used technique and remains the gold standard. However, the elastomeric method requires procedural shortcomings and, in addition, the technique is uncomfortable either for the patient or for the clinician [6-8]. Nevertheless, a consensus regarding the implementation of IOS in complete-arch edentulous patients rehabilitated with multiple dental implants has not yet, been established [15].
Obtaining reliable digital scans of arches where there are large homogeneous areas- between implants in edentulous arches- can be challenging, even impossible [20]. Difficulties are due to the absence of anatomic irregularities in the scanned area. In addition, Scan Bodies’ geometry can drive IOS to “interpretation errors”: scanners can recognize different Scan Bodies interpreting them as the same one [21]. Andriessen et al [21] reported that most digital scans of edentulous arches were unusable. The distance between implants also influences the accuracy of the digital scan so that longer the distance with a uniform surface is, more challenging the scanning process become [20,22]. These problems reflect IOS difficulties in matching multiple images captured during the scanning process [23]. Intraoral scanner’ software builds 3D images ‘by best-fit alignment’ of photographic frames collected by camera. The acquisition of larger areas is more challenging and software algorithm processes become more complex [23]. However, despite area’s extention, in edentulous patient, lack of differences in curvature radius leads additional difficulties. Geometric and colour differences (according to the technology used) detected by the scanner will simplify the matching process. The lack of these features in edentulous oral cavity means that digital scanning of edentulous arches is a very difficult tasks in these patients (Table 1).
Table 1: Medium distances group A and B.
To solve the problem related to intraoral scan of edentulous arches, several authors suggest several methods with the aim of create artificial anatomical references to compensate the distance between Scan Abutments; in this way, the intraoral acquisition is easier and more accurate. Some authors used auxiliary removable devices interconnecting the scanbodies (with guides, polymer bases obtained through the use of a 3D printer) [24-26]. Methods proposed in literature partially solved the problem but usually require very sophisticated procedures that often are not recommended to the traditional physical impression. To date, therefore, despite advanced technologies, in critical clinical conditions intraoral scanning can lead to non-faithful and inaccurate models.
The aim of the study is to show a new concept to improve accuracy of intraoral acquisition in all those critical cases in which the distance between consecutive Scan Abutments affects the trueness of intraoral scans. The procedure outlined in the study has the peculiar property of not requiring complex and laborious steps. The auxiliary device is made of technopolymer material (Polyether ether ketone-PEEK) and it consists in an hexagonal body connected to a settable screw. (Figure 1) The device is designed to be screwed onto a previously drilled Scan Abutment and it does not rest directly on soft tissue so oral mucosa is not covered during the intraoral scan. The chance to successfully acquire oral mucosa with devices assembled on scan bodies avoids the need to acquire two separate impressions, with and without the auxiliary deviceresulting in discomfort for the patient and in extended clinical time.
Figure 1: Design of the device.
Materials and Methods
Stereophotogrammetry technology (PIC Camera; PIC DENTAL), thanks to extraoral scanner, allows to gauge the inaccuracy associated with intraoral scanning of an edentulous arches. Gold standard STL file is acquired by indirect method by taking a physical impression, developing the cast, placing PIC Abutments on the laboratory analogues and scanning it with an extraoral scanner. Then, the gold standard is compared to STL file obtained by the direct intraoral scanning of the same arch. The ethics committee examined the research project and gave its approval to the study (ethics committee “Università Federico II” protocol no. 128/21). Patients provided written informed consent to the treatments and to the publication of the study. Written informed consent was obtained from patients for the publication of any potentially identifiable images or data included in this article.
For each of the 11 subject involved in the study three different impressions were carried out. The physical impression was performed according to “open tray splinted” impression technique using polyether material (3M Impregum Penta Soft) mixed thanks to dedicated equipment (Pentamix type). Analog transfers were pooled with self-curing resin and interdental floss. Each impression thus obtained was made into plaster cast using class 4 gypsum mixed by a vacuum- pressure casting machine. Specific targets (PIC Abutments) were placed on each transfert; then, the model was scanned using an extraoral scanner (X5 Dentsply Sirona). EOS provides an STL file where abutments are truthfully setted and we can use it as control (gold standard). Intraoral scanner (Omnicam Dentsply Sirona) is used to record two different digital impressions: the first impression is normally acquired with the only scan abutments seated (Group A) while the second impression involves the experimental device assembled as part of the “scan structure” (Group B). All digital impressions were performed by the same practitioner and all of them have been obtained according to manufacturer’s scanning protocol, starting from the distal area on one side reaching the opposite side through the occlusal area. Using a specific software (Geomagic Control X 2020) we proceed to the alignment and subsequent one-to- one comparison of the STL files obtained from IOS with the STL file obtained from EOS (Gold standard). (Figures 2 & 3) The primary measurement refers to the mean distance (average of the points dismatching between the two STL files) obtained through Geomagic 3D software. P values under 0.05 are expected to be statistically significant. Data provided by the software, expressing mean and standard deviation values either the lowest or highest distances, were summarized using standard descriptive statistic.
The null hypothesis imposes no statistically significant difference between the mean distances Group B- Gold standard and Group A-Gold standard. The comparison between the two different approaches (IOS with and without auxiliary device) is carried out by Student’s t-tests for paired samples. In the current study, the alternative hypothesis does not state direction of deviation therefore “two-tailed” test is adopted. The two-tailed test is a nondirectional hypothesis test, described as a test in which the critical region falls on both sides of the normal distribution. Thus, an alternative hypothesis is accepted in place of the null hypothesis if the calculated value falls in one of the two tails of the probability distribution (Figure 4).
Figure 2: Scan Abutment plus device in peek on the model.
Figure 3: Device in peek in the oral cavity.
Figure 4: Comparison between stl control and stl with Commercial Scan Abutment.
Results
The two-tailed t-test for paired samples is used to test the null hypothesis that the average distances of the points made using the Scan Abutments according to the standard protocol (group A) are not significantly higher than those obtained using Scan Abutments with the experimental device (Group B). Assuming a difference of 0.1 mm between the two approaches (Group A and Group B) as clinically relevant and a standard deviation of the differences equal to 0.09 (value obtained through the evaluation of preliminary data), a sample size of 11 scans for each protocol will be enough to highlight any difference with a power of 0.9 and a two-tailed significance level of 0.05. Statistical analysis performed by using Spss software showed statistically significant differences (P <.05). Based on the results, the null hypothesis was rejected: group B values, significantly closer to zero, reflect a higher degree in their overlap with the control file. The “color maps” are used to qualitatively compare and evaluate the results: closer is the number to zero, smaller the difference between the two files is. The colors from blue to red indicate in a qualitative way the dimension of the mismatching between the file (A or B) and the gold standard control (Figures 5 & 6).
Figure 5: Alignment between stl control and stl with Commercial Scan Abutment plus device.
Figure 6: Comparison between stl control and stl commercial Scan Abutment plus device.
Discussion
Evidence suggests that intraoral scanning accuracy varies greatly with interimplant distance, intraoral scanner type, scan body type and operator experience. Several clinical factors can contribute to the global deviations in complete-arch intraoral scanning: the present study shows how the absence of anatomical references in edentulous arches has a negative influence on the accuracy of digital dental scans and how artifical anatomical references can be used to obtain easier and more accurate digital impressions. Limitations of the present study include the small sample size and the use of a single type of intraoral scanner. Comparison of the scans obtained with other intraoral scanners available on the market, still with the help of the device, will be reason for further research.
Conclusion
Based on the results, the null hypothesis was rejected. Full-arch digital implant impression, taken using intraoral scanners, was found to be less accurate than the same impressions recorded by the support of the experimental removable device. The present study shows how the absence of anatomical references in edentulous arches has a negative influence on the accuracy of digital dental scans and how artifical anatomical references intraoral make the acquisition in critical cases easier and more accurate.
Numerous biological effects of pyramid structure (PS) have been reported in recent years. For example, Indian scholars found that the seed germination rate and radicle length of plants under the PS were significantly higher than those of the control group [1-3], and other reported effects included accelerated would healing of mice, improved preservation time of food [4-7], and reduction in the occurrence of tumor in mice accompanied by the improvement in liver enzyme activity along with some other biochemical and physiological indicators, which could explain the retardation of the tumor cell growth [8].Despite the accumulating amount of evidence of biological effects reported, there is very little research investigating the underlying biological mechanisms for the observed phenomena. The PS has been proposed to generate a torsion field [9], which has been extensively studied for its biosocial effects. As a portal to receive, process and integrate information in cells, mitochondria play a critical role when cells were exposed to stimuli including external Qi from a Qigong master [10], Chinese texts with different meaning [11], and torsion field [12]. Our group has previously found that the exposure of cultured mammalian cells to the above stimuli can induce changes in numerous parameters related to the mitochondrial functions, such as the production of ATP, ROS, MMP and mtDNAcn, as well as the cellular oxidant capacity reflected by the reduced GSH.In this study, we used 293T cells to examine any potential responses in the mitochondria for cells grown under PS, with the goal of examining potential underlying biochemical mechanisms of the effects generated by a pyramid. We examined parameters including the growth and vitality of the cells, mitochondrial functions including the production ATP, ROS, MMP, the cellular oxidant capacity reflected by the reduced GSH, as well as cell senescence related parameter such as the telomere length.
Materials and Methods
Cell Culture
The 293T cells was obtained from National Infrastructure of Cell Line Resource (Beijing, China, http://www.cellresource.cn) as visceral cells which grow rapidly. The culture conditions and inoculation process of these cells can refer to our previous articles [12].
Pyramid Structure Model
Figure 1: The copper pyramid model.
The pyramid model used in the study is made of copper (some studies believe that the effect of copper is more obvious than other materials [3]) according to the true proportion and angle of ancient Egyptian pyramids. The copper pyramid model with a square of length 280 mm and height 280 mm (Figure 1).
Experimental Design
Two groups of 293T cells culture were used, including a treatment group (cultured in the pyramid model and named as ‘PS’), and a control group, named CK (away from the pyramid model). 293T cells were seeded at a density of 5~6×105 cells/plate into a 10cm plate, and after a 3h attachment period, plates of the ‘PS’ group were placed in the pyramid model for 24h treatment. The plates for the ‘CK’ group were placed under normal growth conditions in another room about 50 meters away. The cells were collected and subjected to different assays at 4h and 24h respectively during incubation. All experiments were performed in triplicate (Figure 2).
Figure 2: PS: pyramid structure treatment group; CK: control group.
Biochemical Analysis
In the experiment, the detection methods of various biochemical indexes of 293T cells, such as ATP, ROS, MMP, protein, cell viability, SOD and GSH, were unified in our research group [12].
Gene Expression Analysis
Because of using the same research vector (293T cells), the parameters of gene expression analysis such as transcriptome sequencing and mitochondrial DNA quantification can refer to the previous work [12].
Statistical Analysis
Values of different measurements were normalized to a respective mean control value from untreated samples and expressed as percent control. All data are expressed as mean ± standard deviation (SD). They were analyzed by analysis of variance (ANOVA) and Least Significant Difference (LSD) using GraphPad InStat software, where P <0.05 was considered statistically significant.
Results
Effects of Pyramid Structure on Cell Growth
Compared to the control cells, PS did not affect the cell growth and cell viability at 4 hours post treatment and 24 hours (Figure 3), indicating that PS treatment for short period did not affect cell growth evidently (Figure 3).
Figure 3: Effects of PS on 293T cells growth. (a) Cell Amount; (b) Cell Viability.
Effects of Pyramid Structure on Mitochondrion
However, the mitochondria were significantly affected by PS as shown in Figure 4. The ATP level of cells in the PS group was upregulated by 20% and 35% at 4h and 24h respectively (Figure 4a) compared to that of the control group. The cellular ROS level was significantly decreased by pyramid at 4h but was not affected at 24h (Figure 4b). MMP level was both upregulated significantly at 4h and 24h (Figure 4c). The activity of GSH, an antioxidant protein, was increased by pyramid at 4h and 24h (Figure 4d), showing a potential role of antioxidant of PS.
Figure 4: Effects of PS on mitochondrion. (a) ATP level; (b) ROS level; (c) MMP level; (d) GSH level. *, P<0.05. *Significantly different from the control group.
Effects of Pyramid Structure on mtDNAcn and Telomere Length
Cellular mtDNAcn and telomere length were detected using the qRT-PCR technology and no obvious changes was observed at 4h and 24h in the cells of pyramid group according to the results (Figure 5). All in all, PS modulated the function of mitochondrion in cells and may protect the cells from oxidative damage by upregulating the level of anti-oxidative protein and downregulating ROS level.
Figure 5: Effects of PS on mtDNAcn and telomere length. (a) mtDNAcn; (b) Telomere length.
Discussion
In this study, we found that the activity of mitochondria in 293T cells became more active under the influence of PS, and the levels of MMP and ATP were significantly up regulated. At the same time, the overall antioxidant capacity of cells was improved. The PS significantly increased the content of GSH and reduced the level of ROS. No significant changes in cell growth and telomere length were observed in the study, indicating that the PS has a mild effect on cells, which avoids the negative effects caused by strong stimulation. Studies have found that the liver enzyme activity of mice in PS shaped feeding cages is significantly increased [8]. The plasma cortisol content of adult female rats exposed to long-term PS changed significantly, and the antioxidant defense ability of erythrocytes was improved [13,14]. In addition, some researchers found that the PS can accelerate the healing of mouse wounds [4,6], which indicates that the cellular activity of mouse wounds is stimulated, which is very similar to our results. As the “power plant” of cells, mitochondria provide energy for cells, and as a bridge for energy transformation inside and outside cells, they can respond to external stimuli in time. The influence of PS is considered as a torsion field [9], which collects the surrounding fine energy through the spatial layout of the structure itself, and then through the induction of mitochondria in the cell, so as to improve the activity and antioxidant capacity of the cell.
Previous studies mainly focused on the effect of PS on biological system, but there were few studies on the effect at the cell level. In this study, we used biochemical and molecular biological methods to determine that the PS has an obvious promoting effect on cell antioxidant and mitochondrial activity, which is helpful to further study the mechanism of PS effect. The healing effect of this special spatial structure also provides a new way for noninvasive treatment.
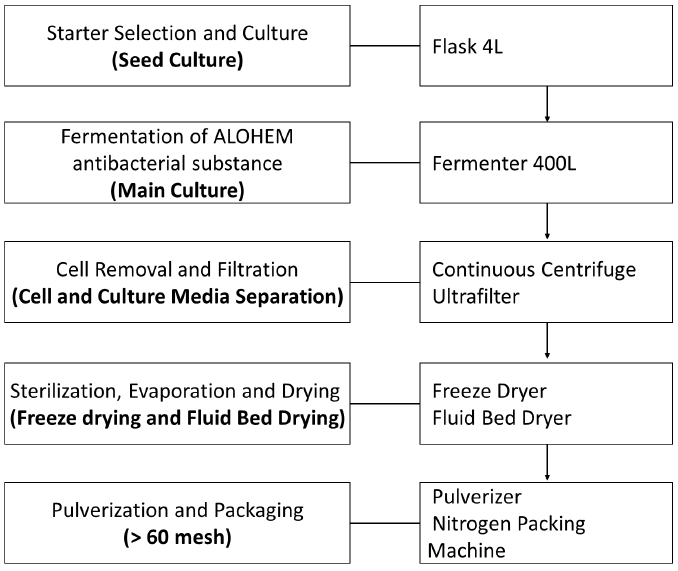
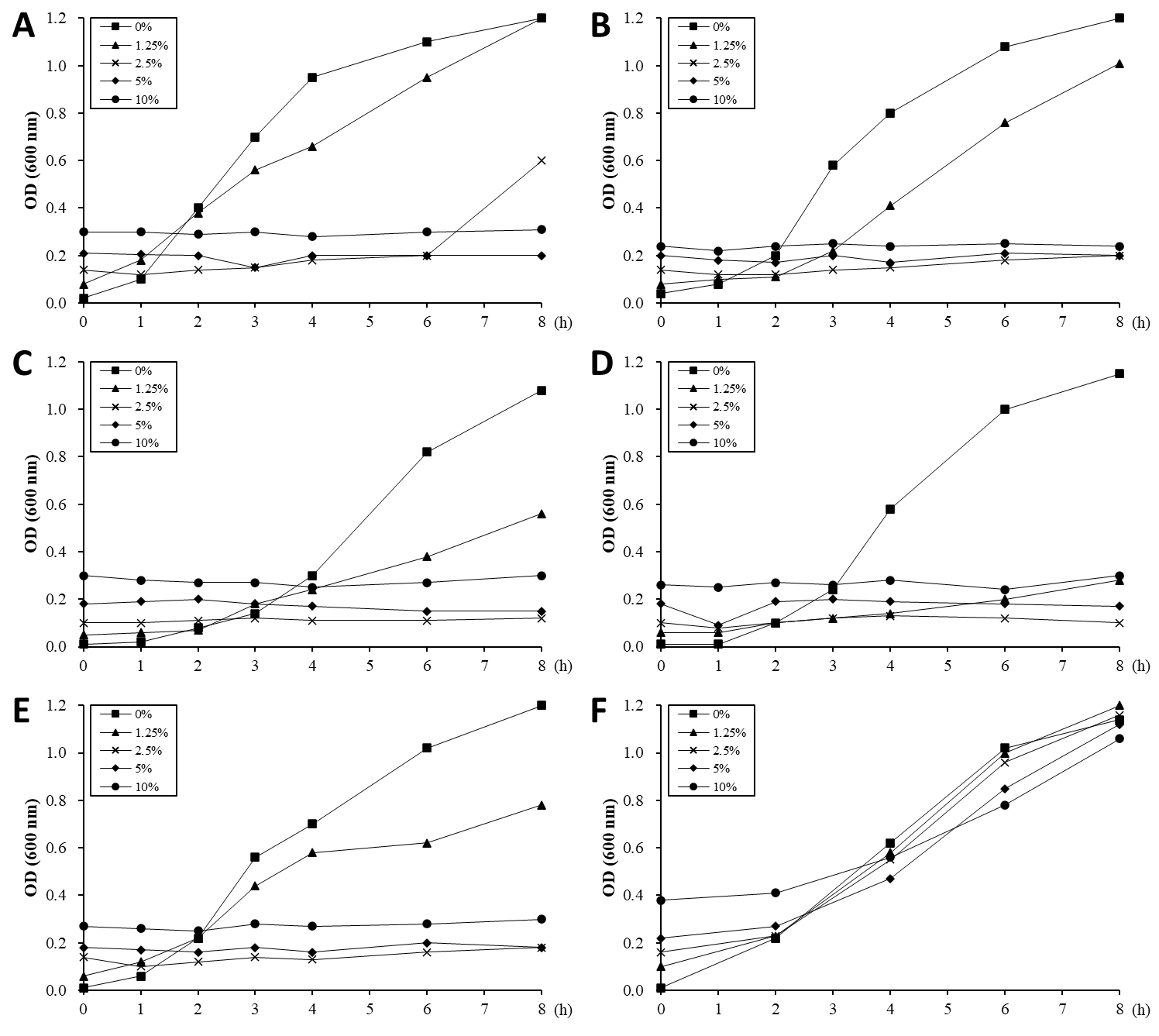

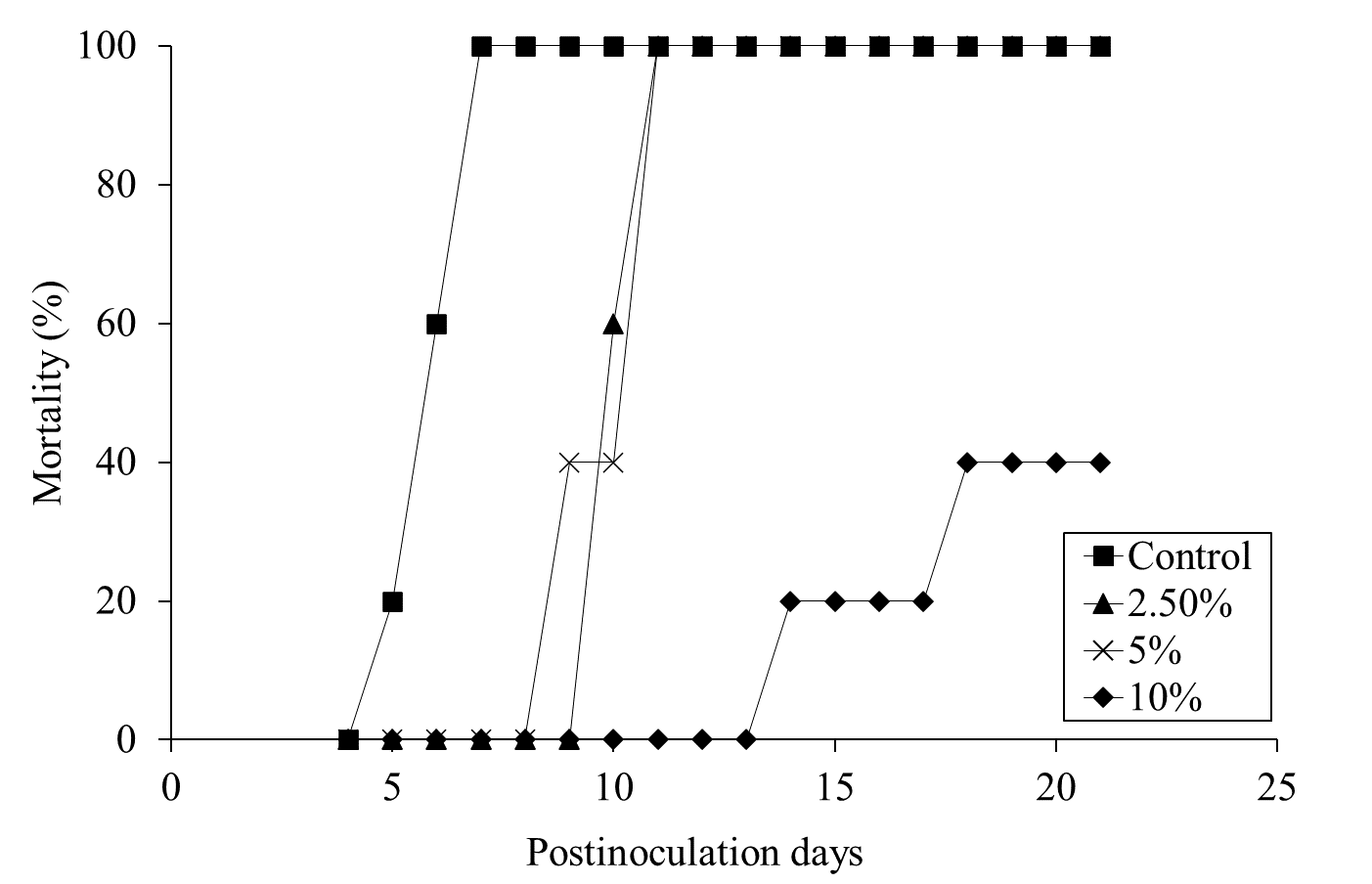
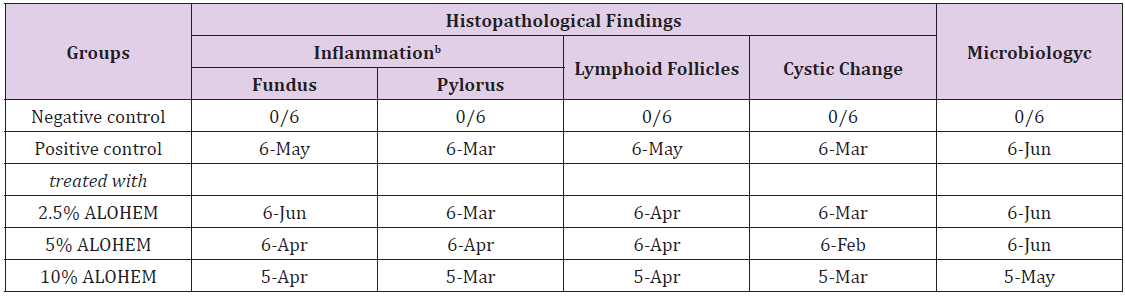
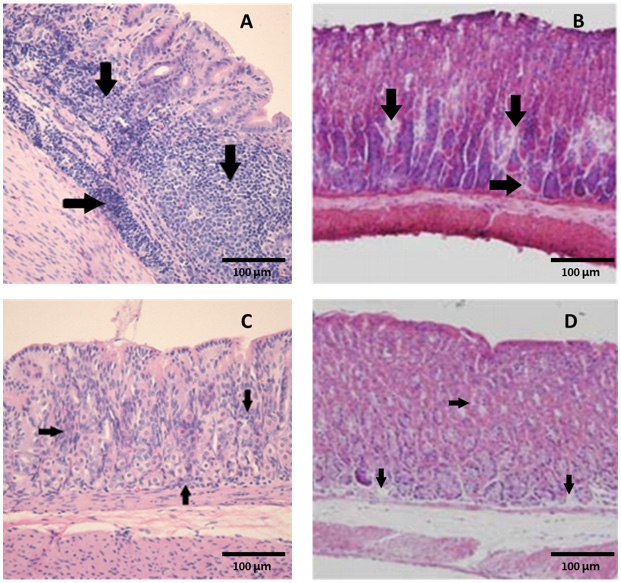
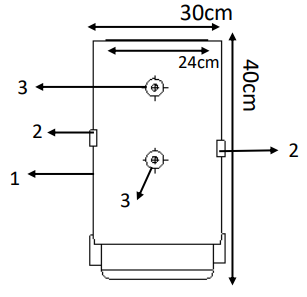
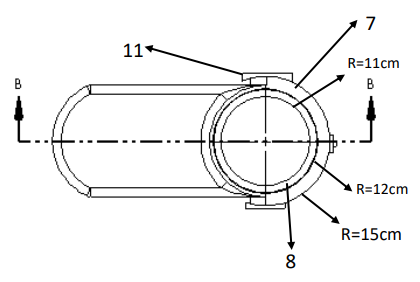
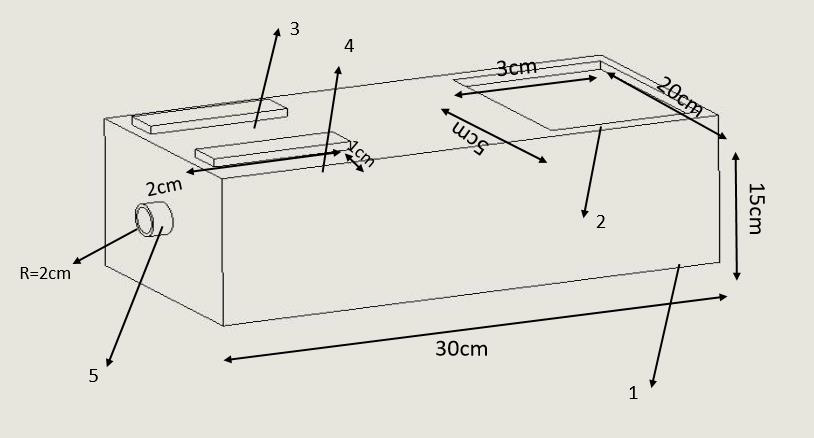
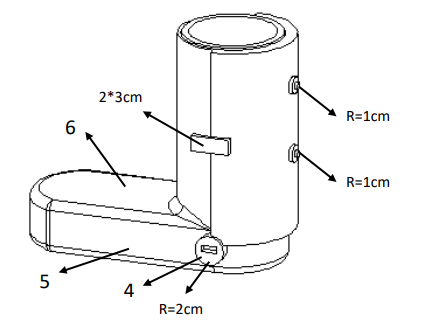
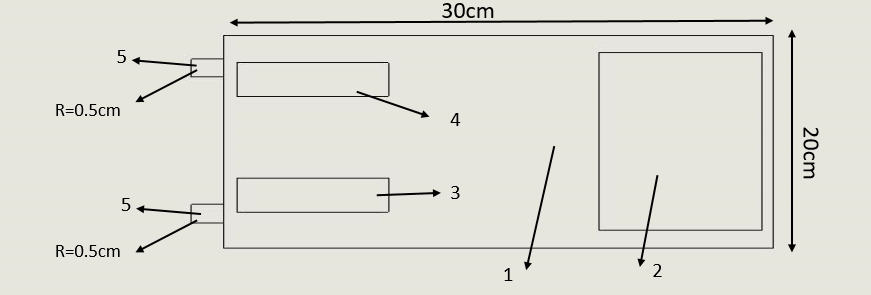
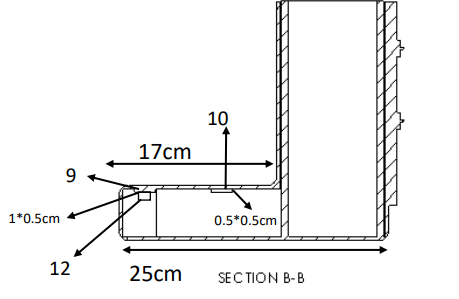





















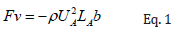
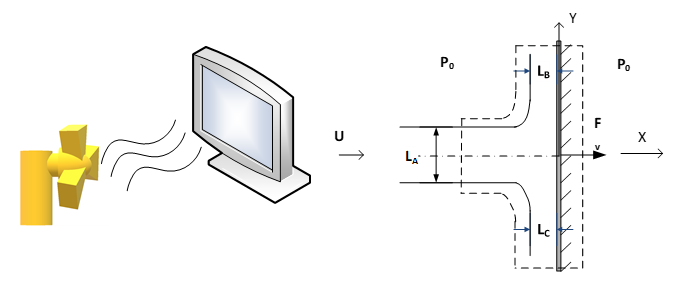
 Therefore,
Therefore,  viruses can be fitted in an area of the tip of a fingerprint (A=10-4 m2). By assuming that, the whole area covered by n number of viruses, the momentum impact on each virus was calculated by:
viruses can be fitted in an area of the tip of a fingerprint (A=10-4 m2). By assuming that, the whole area covered by n number of viruses, the momentum impact on each virus was calculated by:
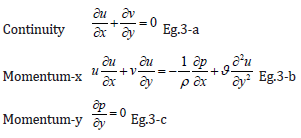
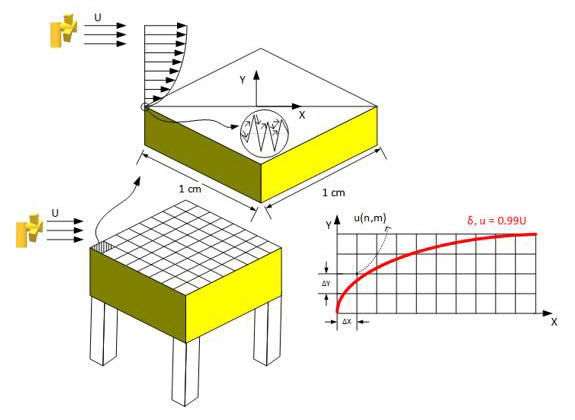
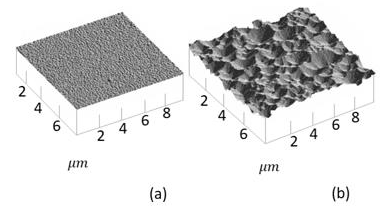
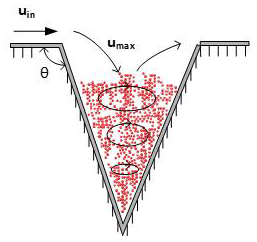
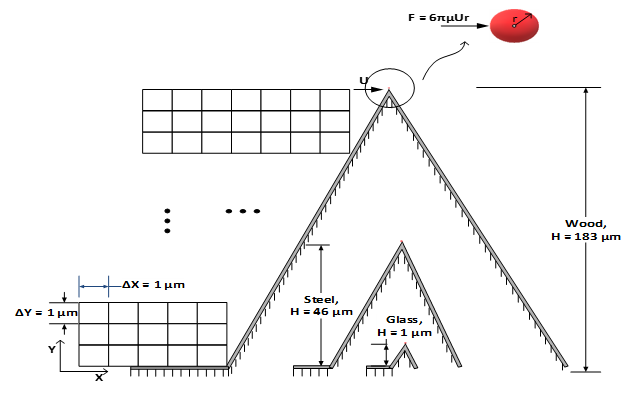
 is as the following:
is as the following: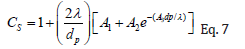
 of the different air flows pass the cylinder with applied velocities of U∞ = {0.1, 0.5, 1, 5, 10} ms-1, at T = 20°C (ν = 1.516×10-5 m2s-1), are far less than the critical Reynolds number, ReD,C = 250,000, which guaranties the laminar flow regime around the cylinder. The Hiemenz’s polynomial velocity distribution [46] was considered for calculating the boundary layer with finite difference method.
of the different air flows pass the cylinder with applied velocities of U∞ = {0.1, 0.5, 1, 5, 10} ms-1, at T = 20°C (ν = 1.516×10-5 m2s-1), are far less than the critical Reynolds number, ReD,C = 250,000, which guaranties the laminar flow regime around the cylinder. The Hiemenz’s polynomial velocity distribution [46] was considered for calculating the boundary layer with finite difference method.
 while
while  and Δy=1 μm. Higher freestream velocities result in smaller thickness of boundary layers; therefore, the domain of 0 ≤ y ≤ 25 mm was considered for U∞=0.1,0.5 ms- 1,while 0 ≤ y ≤ 2.5 mm was taken for U∞=1,5 and 10 ms-1. The two-dimensional, steady, laminar, incompressible boundary layer equations at constant temperature and pressure are the same as Eq. 3-a and 3-b. The boundary conditions of the system were as the following:
and Δy=1 μm. Higher freestream velocities result in smaller thickness of boundary layers; therefore, the domain of 0 ≤ y ≤ 25 mm was considered for U∞=0.1,0.5 ms- 1,while 0 ≤ y ≤ 2.5 mm was taken for U∞=1,5 and 10 ms-1. The two-dimensional, steady, laminar, incompressible boundary layer equations at constant temperature and pressure are the same as Eq. 3-a and 3-b. The boundary conditions of the system were as the following: