Compromised Health and Constrained Human Life in COVID-19 Pandemic, and Concurrent Healthcare Transformation
The SARS-CoV-2 Infection and COVID-19 Pandemic
The current ongoing pandemic of COVID-19 caused by SARSCoV- 2, is associated with high morbidity and mortality in several countries across the globe. A prompt and effective detection of the disease is crucial to identify those infected, to monitor the infection from epidemiological perspective, and to take measures for its containment. On the other hand, the early diagnosis and efficient treatment of COVID-19 including newer therapeutic modalities such as monoclonal antibodies against SARS-CoV-2, may contribute to the individual clinical improvement and limit the morbidity and mortality in the society at large. The likely course of COVID-19 pandemic not certain, and the pandemic being considered a major health hazard, may continue in the foreseeable future or may with low or moderate level of transmission become endemic. The COVID-19 vaccines bear hope to bring COVID-19 pandemic under control, paving a way for its endemicity [1]. In this respect, the WHO in a recent communique indicated that COVID-19 in various countries including India may be entering some kind of stage of endemicity with low or moderate level of transmission [2].
The effects and fallouts of COVID-19 pandemic are striking as it has impacted the social, economic, political, and healthcare aspects of human life. The pandemic is being considered a major health hazard that may continue to afflict human life in the foreseeable future. The transformation of life, thus, at the individual level as well as at the community and collective levels, seems inevitable. Another aspect of the COVID-19 pandemic is the unprecedented levels of misinformation, rumours, and conspiracy theories related to COVID-19 relayed and reproduced by lay and social media, dubbed ‘infodemic’ by the WHO, which are counterproductive to the fight against the pandemic in the short and long term. There are concerns about low to middle income countries (LMICs) related to the COVID-19 preparedness, knowledge sharing, intellectual property rights, and environmental health together with the serious constraints regarding readiness of health care systems to respond to the pandemic. In fact, the spread of COVID-19 presents an extraordinary ethical dilemma for resource constrained nations with poorly developed health and research systems.
In the current crisis, sharing of scientific knowledge and technology has an important role to play. In addition, emergency preparedness is a shared responsibility of all countries with a moral obligation to support each other [3]. The ongoing pandemic has led to a situation in which the scale of emergency is similar to WWII, requiring decisiveness and commitment. In LMICs, the greatest challenge is to design strategy for early response to COVID-19 outbreaks. South Asia holds a quarter of the world’s population with currently COVID-19 affected countries including Afghanistan, Pakistan, India, Nepal, Bangladesh, and Sri Lanka which may have severe constraints in management of the pandemic. In fact, the current low number of reported cases from these areas is likely to be due to less testing with limited resources in these countries. The resource allocation should be rational, transparent, and based on scientific evidence as the current COVID-19 crisis presents challenges that are beyond and above the earlier outbreaks. Efforts for developing and supplying medical devices, diagnostic tools, vaccines, therapeutics, and other medical technologies for COVID-19 pandemic should be tackled judiciously.
Restricted Human Life and Compromised Health
The SARS-CoV-2 Infection control measures are recommended to prevent exposure as well as reduce transmission of the infection include the personal preventive measures at individual level such as mask-wearing, diligent hand washing, particularly after touching surfaces in public, respiratory hygiene (covering the cough or sneeze), avoiding touching the face (in particular eyes, nose, and mouth), cleaning and disinfecting objects and surfaces, and ensure adequate ventilation of indoor spaces. Apart from the mask-wearing decreasing exposure to the infection, has also been hypothesized to reduce the viral load when exposed, and hence to reduce the risk of severe illness [4]. There are other public health measures apart from personal preventive measures for infection transmission reduction focused for source control and containment of infection and include social/physical distancing, stay-at-home orders, school, venue, and nonessential business closure, bans on public gatherings, and travel restrictions with exit and/or entry screening.
The preventive measures are supplemented with aggressive case identification and isolation and contact tracing and quarantine. In the containment areas, the residents are encouraged to stay alert for symptoms and practice appropriate measures to reduce further transmission. The widespread testing and quarantine strategies are imposed to quickly identify secondary infections in an exposed individual and reduce the risk of exposure to others. There are strategies involving self-quarantine at home, with maintenance of at least six feet (two meters) distance from others at all times. There are variations about preventive and quarantine measures for vaccinated and unvaccinated individuals, and those with a recent history of SARS-CoV-2 infection. All these measures restrict human interactions and social and economic activities. The COVID-19 pandemic has thus imposed multiple restrictions on human life, with added risks to unprecedented morbidity and mortality, compromising the global human health, in general [5].
The COVID-19 pandemic has profoundly changed the human life, caused tremendous human suffering, and challenged the basic foundations of socioeconomic well-being, beyond the immediate impacts on health. The short and long-term impacts are likely to be severe for the disadvantaged groups such as older people, children, and women in LMICs. The COVID-19 outbreak poses significant challenges for the elderly, who have high risks for serious complications which can significantly deteriorate their functioning, health status, and social connections. The closure of schools and home confinement during health pandemics has enduring effects on child and adolescent psychological well-being. In today’s increasingly urban world, the cities may be better equipped than the rural areas to respond to the COVID-19 crisis as the latter vastly lack health care facilities. The COVID-19 will, thus, have a negative impact on various dimensions of human life and the potential for deeper effects with GDP and average household income falling by over 10%, unemployment rising by 5 percentage points and life expectancy dropping by half a year.
The Evolving Healthcare Options and Innovations
The COVID-19 pandemic has been a reality check for various provisions of healthcare available in different countries, including the preventive and therapeutic, outdoor consult as well as indoor and intensive care. Whereas in China, the totalitarian regime was able to deal with the pandemic with an iron hand, fully bifurcate COVID-19 healthcare from that for non-COVID-19, and ably carry out preventive measures and vaccination program, in other countries situation has been different. The public health surveillance programs and available infrastructures were shown as not consistently optimal. Additionally, the existing healthcare facilities were unable to cope with the sudden surge and manage intense pressure on their workload especially in the settings of acute care. Even with contingency plans well laid out, healthcare systems were incapable to cope with the abrupt surge in demand and needed to be transformed. The COVID-19 pandemic, thus, has acted as a transformation catalyst, accelerating the implementation and adoption of changes in healthcare. The emerging prototypes of healthcare delivery appear to put more emphasis on preventive measures, remote care, and utilization of innovative digital technologies.
The Hospital-at-Home (HaH) concept was already making inroads in the conventional hospital-based healthcare approach for a large number of diseases, with the hospice service being a surrogate example. In fact, it is being dubbed as the next frontier in the healthcare delivery and our experience with the pandemic has fast accelerated the HaH programs. The emerging HaH programs have advantage of lower costs and readmission rate, while maintaining quality and safety levels, and better patient experience. Build on the HaH concepts, the conditions can be identified and progressively dispensed with home-based primary and secondary care (Figure 1).
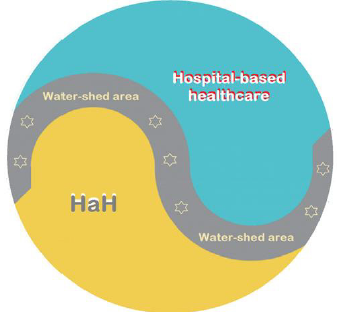
Figure 1: The conventional hospital-based healthcare, the HaH and the water-shed area for intermediate health conditions.
Similar to the scenario in various sectors, the health services and healthcare too have had profound impact owing to COVID-19 pandemic. The COVID-19 pandemic has brought home the realization that a significant proportion of healthcare activities can be tendered remotely equally effectively through technologically empowered approach. As related to the healthcare, there are certain salient aspects likely to emerge in the post-COVID-19 era.
1. There is shifting of large number of patients to remote care. The telehealth services have already been used in emergencies and during crises in the past. With possibility of quality transfer of data, audio and video communications during the COVID-19 pandemic, their utilization has widely accelerated. The pandemic has become a catalyst for swift implementation of online consult and therapy, replacing the clinician/patient face-to-face outdoor consultations.
2. In the hospital setting, the remote care is now being widely used for screening prior to the visit and triage assessment, for the indoor and ICU monitoring and supervising of patients in hospital by off-site experts. This trend is likely to persist to large extent in the post-COVID-19 period, as it provides higher convenience both for clinicians as well as patients.
3. In the mental healthcare, too, the remote consultation is proving helpful. It is likely that once mental healthcare institutions have developed the capabilities of serving their patients through digital technologies, a blended approach in future would emerge, where e-mental-health solutions cover an increasingly greater part of routine services.
4. The remote care system in form of HaH is likely to serve further as an adjunct for the gradual adoption of newer and advanced technologies, such as, the use of drones as delivery vehicles for critical supplies, robotics, the widespread 3D-printing of healthcare-related items, and smartphone-enabled monitoring of patients’ adherence to treatments.
The Healthcare Transformation – Evolution of HaH
As related to the public health, with the availability of the mobile-enabled technologies, there is an improved operation of surveillance systems and data analysis. The mobile-enabled technologies can be deployed en-masse to monitor quarantined individuals and trace exposed individuals with temporal and geographical correlates. The new tools are likely to move further into the public health domain and support the interconnected and hypercomplex global situations in real-time. On the other hand, the healthcare, in general, is needed to be people centred and integrated. The patient centred services include diagnosis and treatment and other supportive aspects of healthcare, whereas integrated healthcare involves adequate provision and efficient delivery of safe and quality health services. The people-oriented approach, on the other hand, implies planning the healthcare services by assessing the needs and expectations of community and applying them in a methodological and efficient way. The integration of modern technologies including telemedicine in healthcare services will improve the quality of healthcare.
The COVID-19 pandemic has led to realization about the limitations of existing healthcare systems and their capacity to respond to healthcare emergencies including infectious disease epidemics. It has underlined the inadequate health literacy among general population to grasp the healthcare recommendations and their outcomes [6]. It has also served as a reminder for proactive planning and preparedness. In addition, it has highlighted the necessity for technologically oriented solutions for healthcare provision and the need for significant healthcare transformation. On the other hand, it has opened the pathways to evolution and expansion of the concept of HaH incorporating communication technology-based approach as a major step to deliver healthcare at home or closer to home with all necessary steps to safeguard the safety and privacy of the participants.
In fact, the healthcare at home (HaH) can be modelled on lines of the hospice care as a multidisciplinary team approach, generally home-based and sometimes providing services through freestanding facilities, in nursing homes, or within hospitals for handling potentially treatable conditions such as pneumonia, heart failure, and alike, with brief hospital stays if necessary (Figure 2).
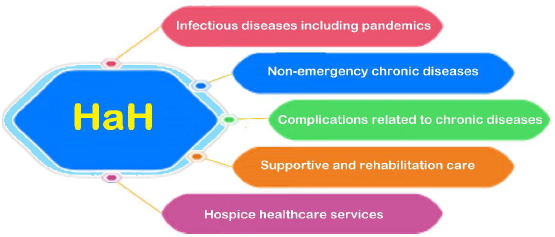
Figure 2: The development of home-based healthcare and potential spectrum of HaH.
The HaH describes a delivery paradigm where the entirety of the hospital-based inpatient care modality is substituted with intensive at-home treatment approach enabled by digital technologies, multidisciplinary teams, and ancillary services [7]. The potential spectrum of HaH can incorporate the hospice care. But as compared to the latter, apart from providing healthcare services for the terminally ill and elderly in form of hospice care, the HaH can be also useful for all those patients who need intense medical care and treatment but can be managed with help of technological monitoring and remote supervision by healthcare professionals at their homes with possible access to a nearby medical facility or hospital. HaH can make possible for people to receive a variety of medical services in their homes and can satisfactorily deal with various health conditions, as it incorporates therapeutic and nursing care, and medical assistance. In fact, the HaH is being envisaged as an alternate attractive model for accommodating increased demand for inpatient health care and as we prepare for the post-COVID-19 pandemic era, there are evolving salient features of HaH potentially promising to maximize the benefits of transformed health care [8].
The Management and Delivery of Healthcare at Home
During the COVID-19 pandemic, there has been a decline in emergency department visits and hospital admission rates in various countries [9]. It seems that in addition to a shift to virtual healthcare, COVID-19 also influenced emergency department visits and hospital admissions unrelated to COVID-19 itself. The studies from both Spain and Italy have shown a reduction in admissions and procedures related to conditions like myocardial infarction and acute coronary syndrome [10,11]. A recent study from Thailand demonstrated that during a national lockdown for COVID-19, there was a significant reduction in daily emergency department visits [12]. Similarly, a study from Melbourne, Australia documented that during times of COVID-19 restrictions there was a significant reduction in ED visits [13]. According to a survey by Canadian Home Care Association, there has been a decline of around 72% in emergency department visits, in turn resulting in the reduction of hospital admission rates [14]. These reductions in outpatient service and admissions underline the need to develop an alternative modality of healthcare for patients still requiring inpatient management for their acute and chronic medical conditions.
The integration of modern technologies like electronic health record (EHR) and telemedicine in healthcare services will save time and resources and provide better healthcare to the users. There are five major technologies which are likely to reform home-based healthcare, and include use of various biosensors, GPS, remote monitoring tools, electronic data and analysis, and telehealth. The e-Prescriptions generated are easy to be transmitted and compatible with the EHR.
In general, the HaH comprises of the following benefits:
1. With the primary focus of HaH, people get medical support at home rather than spending time in a medical facility. Further, it allows people to stay comfortably at their residential facility rather than at hospitals, having lower cost and various psychological advantages.
2. Activities of daily living are not altered and supported in-home in usual ways while maintaining a good quality of life for them in the known and perceptive atmosphere.
3. With the home care provided to patients with chronic health issues such as diabetes and respiratory disease, clinical trials have shown fewer complications and better health outcomes. The personalized and skilled care improves the overall response to the treatment.
4. With the real-time monitoring with technological equipment, the patients are seen and followed in real-time. Along with the AI and automation, the HaH aims to streamline the processes such as scheduling appointment, data collection, maintaining EHR, e-prescriptions, and scheduling and providing other health-related services as and when needed to improve the overall patient care at home.
The Covid-19 pandemic has amplified interest in HaH in the United States, European countries, and elsewhere as an alternative care model for both COVID-19 and non-COVID-19 patients, who can be remotely managed aided by current regulatory flexibilities (15). In fact, the HaH is being envisaged as an attractive model for accommodating unprecedented demand for inpatient capacity created by Covid-19. As we prepare for the health care for the postpandemic era, there are salient issues to be solved to maximize the benefits of HaH –
1. The HaH models must encompass the provision of healthcare of analogous intensity to hospital inpatient standards, and have a specified geographic catchment area, with properly defined correlates.
2. As the HaH is supposed to create the acute hospital care at home and to enable health systems to provide intensive care at home for patients with various acute and chronic conditions, this may lead to a remarkable expansion of HaH.
3. There is a unique opportunity to extend and expand HaH in current times, which can become a new vehicle for integrating non-medical services into healthcare as the patients may require further support due to complexity of their illness.
4. With the advances in digital technologies and their increased utilization by patients and healthcare providers, there is taking place transformation of the home environment into a preferred healthcare delivery site.
5. As the health awareness and rising cost of healthcare services may lead to increase in demand of HaH, managing and delivering HaH with technological backup should be affordable and providing quality service.
6. Further, a regulatory and policy implementation roadmap is required for provision of HaH, which should be accompanied by monitoring tools, such as, public reporting, patient registries, and maintenance of reliable database.
Conclusion – The Healthcare Solutions for the Future
With the COVID-19 pandemic having impact on almost every aspect of human life, the lessons have been learned relating to provision of healthcare. The telemedicine and virtual online consultations have been helpful in dealing with sudden surge and demand for healthcare both outdoor consult as well as emergency visits, and indoor and ICU care. During the COVID-19 and now in post- COVID-19 phase the alterations in provision of healthcare and its transformation have been enormous. The conventional healthcare encompassing outdoor consult and hospital-based care is being increasingly replaced by tele- and video- consultations, remote technologically assisted indoor care, and HaH. While the hospitalbased care cannot be fully dispensed with, a large proportion of it being increasingly assigned to HaH. The technologically assisted remote healthcare, outdoor as well as indoor, with its availability and acceptability, and associated challenges and benefits, is the new reality of current times.
For More Articles: Biomedical Journal Impact Factor: https://biomedres.us