Determinants of Poverty in Farming Households in Southwest Geo-Political Zones of Nigeria
Introduction
The significance of rural poverty is underscored by the fact that as much as 45% to 80% of national population reside in the rural areas and are dependent in agriculture in most developing countries Ravalion et al. 2007. Poverty can be described as the level of deprivation that encompasses shortfalls or inadequacies in basic human needs, which prevent people from achieving internationally acceptable levels of well-being Etim, et al. [1]. This situation, which has been ascribed in some quarters to production failure owing to a suppression of markets and in some other quarters to institutional and distributional failure Ognonna et al. 2007 is characterized by disease, low life expectancy and physical and mental retardation. Globally, about 1.2 billion people are in extreme poverty, living on less than a Dollar per day IFAD [2]. Majority of these people are in developing countries, 44% in South Asia, 24% each in sub- Saharan Africa and East Asia and 6.5% in Latin America and the Caribbean IFAD [2,3]. Within these regions, poverty is largely a rural phenomenon with an average of between 62 and 72% of the population living on less than a dollar a day Owuor, et al. [4]. In comparison, rural poverty also tends to be deeper than urban poverty in these regions Owuor, et al. [4].
In Nigeria rural poverty levels are relatively high. For example, a national poverty survey carried out in 2003 and 2004 indicates that the urban areas have poverty levels estimated at 43.2% while the rural areas have poverty levels that are as high as 63.8% Federal Republic of Nigeria [5,6]. The mean national poverty incidence stands at 54.7 NBS [6]. However, evidence indicates that this situation has not improved in the last 15 to 17 years in a majority of Sub-Saharan countries of Africa Owuor, et al. [4]. In Southwestern Nigeria, about 70% of the populations live in the rural sector and are dependent on agriculture as in most developing countries of the world for their livelihood Akoroba 2007.
Problem Statement
Poor people live without fundamental freedoms of action and choice that the better off take for granted Elijah [7]. They often lack adequate food and shelter, education and health, deprivations that keep then from leading the kind of life that every one values. They also face extreme vulnerability to ill health, economic dislocation, and natural disasters Owuor, et al. [4] and they are often exposed to ill treatment by institutions of the state and society and are powerless to influence key decisions affecting their lives. These are several dimensions of poverty World Bank [8]. Poverty is an unacceptable deprivation in well-being World Bank [8]. It exists when there is lack of the means to satisfy critical needs. Poverty can be regarded as the status, objective or subjective, of an individual or a population. Poverty will have an objective definition once observable and measurable indicators exist that are used to approach the material or other aspects of the lives of individuals. On the other hand, the subjective definition of poverty is when judgment (including value judgment) of individuals is taken into consideration in order to investigate their welfare Amao [9]. Reducing poverty is an important development policy issue because economic growth is obviously associated with poverty reduction. Nigeria has experienced a high incidence of poverty alleviation Etim NA, et al. [1]. The worrisome aspect of this phenomenon is the spatial differences in the incidence of poverty in Nigeria.
The United Nations Human Development Report (1998) declares that Nigerian poverty level is getting worse by the day and more than four in ten Nigerians live in conditions of extreme poverty of less than N320 per capita per month, which could hardly provide for a quarter of the nutritional requirements of healthy living. This is approximately $8.2 per month. The report ranked Nigeria 146 out of a total of 174 countries in its Human Development Index (HDI), which measures achievement in terms of life expectancy, education and real income per capita. Poverty has been identified as a rural phenomenon and its interventions will be effective only if the correct poverty causing factors are identified In recent years, because of the large prevalence of poverty, reducing it has been of great concern to many developing countries for the past few decades Babatunde, et al. [3]. This situation has created the quest for poverty reduction strategies which have been at the center stage of development programmes and policies. The progress towards the global target of halving, between 1990 and 2015, the proportion of people living in extreme poverty, has been very slow. The main problem lies in the fact that despite the high poverty rates in Nigeria little is documented on policy related determinants of rural poverty among farmers especially arable crop farming households, making it very difficult to effectively set and implement sustainable antipoverty programmes. Hence, the objective of this study was to empirically determine factors influencing arming household poverty in Oyo state.
Methodology
Study Area
The study was carried out in selected States of Southwestern Nigeria. Southwestern Nigeria comprises six states which are Lagos, Ogun, Oyo, Osun, Ondo and Ekiti. The Southwest lies between latitude 50N and 90N of the equator and longitudes 2.50 and 60N east of the Greenwich Meridan. It is bounded in the East by Delta State, the Republic of Benin in the West, Kwara and Kogi State in the North and by the Atlantic Ocean in the south. The major occupation in the States is farming in which Maize, Cassava, Rice, Yam, Oil palm, Cocoa, Timber are produced enormously. The vegetation pattern of the states is of rainforest in the south and guinea savannah in the north. Figure 1 shows the position of the study area in the map of Nigeria.
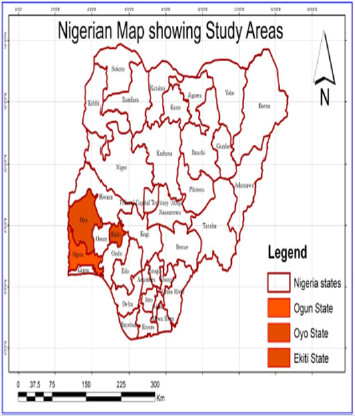
Figure 1: Map of Nigeria Showing the Study areas.
Sampling Techniques and Data Analysis
Multistage sampling procedure was used to select 600 rural farming households across the selected states (Oyo, Ekiti and Ogun) in Nigeria. First stage involved the selection of two (2) Zones from each states making 6 zones. Second stage involved random selection of two (2) blocks from each of the six (6) ADP zones respectively making 12 blocks. Stage three involved random selection of four (4) cells from each of the 12 blocks making 48 cells. While the last stage involved random selection of thirteen (13) rural households from each of the 48 cells making six hundred (600) rural farming households. Primary data were collected using structured interview guide.
Analytical Method
The statistical tools used to realized the objective of this study were tables, percentage, mean poverty ratios and multiple regression analysis.
Descriptive statistical tools such as tables, means and percentages were used to analyse the poverty line. However, the analysis used household expenditure as a proxy for income, as income was very difficult to obtain.
Z = 2/3 Y* …………………………. 1
Where,
Z = Poverty line measured in Naira. This was defined as the minimum level of consumption required and individuals or households falling below the threshold were considered poor. This was used to establish the poor and non-poor farming households. Y* = Mean of per capita household expenditure, measured in Naira and derived as the average of per capita household expenditure following Babatude, et. al. [3]
Linear multiple regression analysis was used to estimate the determinants of rural poverty following Olubanjo, et al. (2007). The implicit functional form was specified as:
P = f(X1, X2, X3, X4, X5, X6, X7,E) ……..… 2
Where
P = Poverty line
X1 = Age of the household head (Years)
X2 = Marital Status
X3 = Educational level (Years)
X4 = Household size (Numbers)
X5 = Primary Occupation
X6 = Income from Primary Occupation (₦)
E = Error term
Result and Discussion
Socio-Economic Characteristics of the Respondent
Table 1 shows the socioeconomic characteristics of the respondents in the study area. The results of the descriptive statistics reveal that 54% were male while 46% were female. Thus, this implies that male dominate farming activities than in the study area. The table also shows that 48% of the respondents were married with 27% having no formal education. Majority (44%) of the respondents have less than 5 acres of farm size with 65% choosing farming as their major occupation.
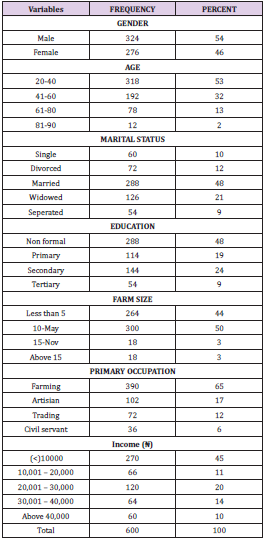
Table 1: Socioeconomic distribution of the respondents.
Note: Source: Field Survey Data, 2014
Estimated Poverty Line
The poverty lines was estimated based on per day expenditure among farming households in the study area. Results showed that the mean annual household food expenditure among the farming households was estimated as ₦11,226.11 while the poverty line was estimated as ₦427.14 per person per day. This implies that any farming household living below ₦427.14 on person per day was categorized as poor household. This implies that could not meet the daily needs of the entire farming household. Considering the mean household size of 6 persons per household, this was lower than the international poverty threshold of $1.25 per person per day for people living in sub-Saharan Africa and Asian countries as viewed by Ravallion, et al. [10]. This result tends to suggest problems of food insecurity among farming households. In other words this amount may not be able to meet the minimum daily calorie in-take of 2250 Kcal required per person per day.
Estimated Determinants of Poverty
Table 2 shows the determinant of poverty among the respondents’ household in the study area. It reveals age, marital status and household size are statistically significant at 5%, 1% and 10 respectively to their poverty level. This lends credence to some author’s finding such as Elijah, et al. [4,7] that as the age of the household head increases, poverty level decreases. Education also enhances the ability to derive, decode and evaluate useful information as well as improves the quality of labour as viewed by Onyenweaku [11-15].
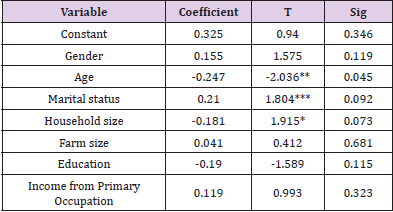
Table 2: Determinant of poverty among rural household in the study area.
Note: Field survey, 2014.
* = Significant at 10 percent ** = Significant at 5 percent *** = Significant at 1percent.
Conclusion
The poverty line of ₦427.14 obtained was a reflection of limited resources among the farming households in the study area. The results tend to suggest problems of food insecurity among poor farming households. If farming households are to improve on food security, then there is the need to provide them with adequate compensation scheme. This can be done through provision of credit facilities. This will encourage them to produce more irrespective of the cost of production and increase in income. Finally, the determinants poverty among farming households were age, marital status and household size. The result of the determinants of poverty serves as criteria for policy interventions.
For More Articles: Biomedical Journal Impact Factor: https://biomedres.us