Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Author: biomedicalopenaccessjournals
The only motto of Biomedical Journal of Scientific & Technical Research (BJSTR) Publishers is accelerating the scientific and technical research papers, considering the importance of technology and the human health in the advanced levels and several emergency medical and clinical issues associated with it, the key attention is given towards biomedical research. Thus, asserting the requirement of a common evoked and enriched information sharing platform for the craving readers.
BJSTR is such a unique platform to accumulate and publicize scientific knowledge on science and related discipline. This multidisciplinary open access publisher is rendering a global podium for the professors, academicians, researchers and students of the relevant disciplines to share their scientific excellence in the form of an original research article, review article, case reports, short communication, e-books, video articles, etc.
Family Counseling with a Child with Learning Disabilities or Disability
Introduction
Nowadays it is generally accepted the belief that counseling intervention in families with children either with disabilities or with learning difficulties or generally with special needs is necessary. It is therefore necessary to understand how essential the science of counseling psychology is and how long a counselor can stand by parents who have children with special needs, in order for them to provide the appropriate help to their child and finally to harmonize daily life. of their family.
Children with Special Needs
The term “special needs” refers to children with disabilities who are classified into categories according to the problems they face. These are a) Hearing problems b) Vision problems c) Special learning difficulties d) Autism e) Mental retardation f) Motor problems g) Behavioral disorders h) Speech disorders i) Personality disorders j) Chronic diseases [1]. Children with disabilities need in addition to special pedagogical treatment and psychological support, which can be achieved through the counseling process, so as to meet their personal, educational, social and professional needs [2]. There is no doubt that the role of counselor or psychologist is absolutely necessary so that children and adolescents feel supported and safe in the above areas. At the same time, however, prevention must be extended to the family system. In other words, it is necessary for the parents of children who face some problems to seek the appropriate counseling and psychological help, so that they can realize and at the same time understand early on the needs of their children, but also to support and unwind themselves psychologically.
Having a Child with Special Needs
Having a child without a doubt is one of the most important experiences of our lives. But it ends up being the most painful, when what we had dreamed of suddenly collapses because the child, we brought into the world does not live up to our dreams. As a result, completely unprepared parents view the event as a disaster, resulting in psychological shock, which determines their later life [3]. The treatment of this event by the parents is divided into two phases: a) The divisive phase according to which most parents are in a state of shock and subconsciously often have abominable thoughts such as for example thinking that they would prefer their child or even to die themselves. The most common reaction in the end is for parents to try to give birth to another child, to make their regrets more bearable and to restore their self-confidence and morale. b) The recovery phase of the relationship during which there is a variety of reactions. Most of the time the parents are too attached to the child and consciously conflict with his disability. In this second phase, it is necessary to be properly informed and supported by expert counselors, so that parents can more easily accept their child’s problem, feel relieved and therefore be able to function more effectively [4].
Defining Counseling
The term Counseling presupposes working with individuals but also with couples, during which the counselor manages to discover as well as to explore the methods that will bring him a more creative and satisfying life [5]. This type of counseling helps parents actually discover the extent of their child’s disability and assess their developmental prospects. It also enables them to be more decisive but also to implement their decisions more effectively. Also, during the sessions, the parents learn the ways that will help them to mobilize and offer their child more help. Still, through counseling they gain more courage and thus develop over time defense mechanisms of survival. The path of early counseling, that is, according to [6] offers long-term benefits to the whole family.
The Role of the Consultant
In order for a Counselor to implement a correct counseling intervention and to give accurately and without evasions a correct information, it is certain that he must possess the necessary theoretical and practical training so that he has the ability to guide correctly as well as to support them psychologically. parents of children with special needs. The counselor must possess the correct knowledge on the disorders he is called to deal with and of course on the counseling and psychology. The main roles of the Consultant are three. Primarily, they have a therapeutic role as their job is to help people cope with this difficult phase of their lives. Their second role is a preventive role as it prevents the anticipated difficulties that the family may face in the future. The third role of the counselor is educational and evolutionary because it enables people to plan how to get the most out of their experiences which will enable them to discover and accomplish everything, they are capable of achieving. He must also accept himself to be intelligent, to be dignified and above all to be possessed by humanity and compassion.
The Role of the Parent
Nowadays parents can play an active role during their children’s rehabilitation therapy. It is easily understood that parents have the ability to observe their children’s daily behaviors that do not manifest themselves during the examination or visit to a health professional. They can also be involved during their participation in psychological support and early intervention programs and most of the time manage to have amazing therapeutic results [7]. Parents who seek and receive special help are able to act therapeutically as far as their children’s behavior is concerned and by using the programs and treatment strategies, manage to successfully deal with the difficulties that their child faces during treatment and rehabilitation. Also, parents who are trained in counseling, are able to perceive inadequate behaviors, such as speech difficulties, difficulties in self-care and behavioral issues. Thanks to the knowledge they have acquired, they are able to judge which methods are appropriate and choose them, so that they can intervene and help immediately and prevent such behaviors, such as outbursts of laughter or anger and other outbursts. In addition, they know when it is necessary to support their child and how to reach the desired behavior slowly [8].
The Advisory Process
Throughout the counseling process, it is important for parents to be informed as clearly and accurately as possible about the report, the diagnosis, the prognosis and the ways to deal with the problem [8]. There are many counseling theories with similarities and differences between them and with their own counseling procedures. The following steps are followed in the counseling process in which the Counselor and the Counselor participate. 1) Stage 1: The Counseling process begins with the first contact of the counselor and the Counselor, who by creating a good psychological climate, set the desired goals. 2) 2nd Stage: In this stage, the relationship between the Consultant and the Consultant is built, which is the most important element that will lead to the success of the counseling process. Here the Consultant has the dominant role, since he is the one who with his correct behavior should facilitate the smooth outcome of the process. This will be achieved more easily, since it positively affects the Counselor, who, by adopting his personal way of thinking, now helps and believes in himself. The purpose of this second stage is to create the right climate of trust that will help parents express how they feel, express doubts and discuss the goals they have set for their child. 3) Stage 3: This stage leads through the development of a positive relationship between the Consultant and the Consultants in setting and delimiting the goals. 4) Stage 4: After setting the goals, the Consultant, taking into account the personalities of himself and the Consultant, applies his scientific knowledge in order to choose the appropriate consulting method. 5) 5th Stage: This stage is the end of the whole counseling process. This process is therefore considered successful when the initial goals have been achieved.
Conclusion
With the right guidance and support of families of children with special needs, it is possible in our time, as we saw above, for these families to find their own tactics for solving the problems they face as well as to use various techniques in their personal daily lives. You put more emphasis on these elements of the family that are considered more positive as well as on gaining in terms of selfconfidence [2]. In other words, counseling for families with children with special needs, whether it is some kind of disability or a special learning disability, can offer a better quality of life, peace of mind and clarity in order to help the child properly and effectively.
Abdominal Wall Metastasis without Primary Lesion or Definitive Diagnosis until Repeat Histology of Specimens from Laparoscopic Cholecystectomy: A Case Report
Background
Tumors located in the abdominal wall are often related to occupational and iatrogenic factors, and increased cases of abdominal wall metastases are reported along with increased removal of resected tumors by laparoscopy. Since the first laparoscopic cholecystectomy (LC) was performed in 1987, [1] LC has become the gold standard operation for benign disease of the gallbladder. With the explosive increase in LC rates, the incidence of incidental gallbladder carcinoma (IGBC), which has a more favorable prognosis than cancers presenting with symptoms, is found in 0.18-2.1% of patients during or after LC, diagnosed during or after cholecystectomy by pathology has increased [2-5]. Port-site metastasis (PSM) is a complication caused by the removal of IGBC using laparoscopic techniques, with an incidence of 14%–29% [6]. Several authors have reported cases of port-site adenocarcinoma metastasis of IGBC of unknown origin following LC. We present herein a case of PSM that was difficult to diagnose due to an incorrect histopathological examination and was discovered 3 years after LC was performed. The patient remained alive for 2 years without any treatment after the first sign of a recurrent tumor was found by the patient.
Case Presentation
A 57-year-old woman was admitted to our hospital because of aggravating pain in the right upper quadrant and a progressively enlarging mass with tenderness, measuring 20 cm × 4 cm, palpated at the right rectus abdominis region. The patient had undergone only one surgery, five years prior: she underwent LC using the threeport technique owing to symptomatic cholelithiasis diagnosed as chronic cholecystitis after a postoperative histological examination at an outside hospital. The patient first noticed the hard mass, measuring approximately 3 cm×3 cm, with intermittent pain in the right upper abdomen 2 years prior. Then, she underwent abdominal ultrasonography, which indicated only agenesis of the gallbladder. A wait-and-see policy was adopted, and the patient was discharged from the hospital and has not received any special treatment over these 2 years.
What Tests are Indicated to Narrow Down the Differential Diagnosis?
To determine the cause of abdominal pain and the mass at the uncommon location, relevant auxiliary examinations were performed. Abdominal contrast-enhanced computed tomography (CT) showed a thickened right rectus with uneven density whose enhancement was not obvious, indicating that the mass could be a benign lesion. Abdominal contrast-enhanced magnetic resonance imaging (MRI) also showed the mass as more likely a fibroma durum. Then, an ultrasound-guided needle biopsy of the mass was performed to further clarify the nature of the mass, and metastatic adenocarcinoma tissues were found. The mass was diagnosed as a metastatic adenocarcinoma.
What is the Origin of Adenocarcinoma?
As the carbohydrate antigen (CA) 19.9 level was 367.0 U/ml, above the normal range, the adenocarcinoma cell was believed to originate from the gastrointestinal tract, but no tumor foci were found on gastroscopy, colonoscopy, or whole-abdominal and pelvis enhanced CT. A positron emission tomography–computed tomography (PET-CT) scan was performed and primary lesion was not found, neither. According to abdominal MRI, the mass passed through the longitudinal section of the rectus abdominis and presented as a spindle shape near the subxiphoid laparoscopic scar. As tumors located in the skin are often related to occupational and iatrogenic factors, PMS could not be excluded. A repeat histopathologic examination of the gallbladder was performed at our hospital and revealed adenocarcinoma in the specimen. Therefore, the diagnosis was gallbladder adenocarcinoma with PMS.
What is the Most Suitable Treatment for the Patient?
On the basis of the PET-CT data and given the extensive metastases in the abdomen, a second operation to achieve radical resection was impossible, and the patient was initiated on the GP regimen (gemcitabine, cisplatin), the standard chemotherapy regimen for patients with advanced biliary tract cancer [7].
Discussion and Conclusion
Laparoscopic surgery has been widely accepted to treat benign diseases due to its desirable advantages, such as low blood loss, quick recovery, minimal pain, a short hospitalization time and few complications. Nowadays, a histological examination, which is often performed after surgery, is the gold standard for the diagnosis of benign or malignant tumors. Under these circumstances, the frequency of incidental gallbladder cancer is 0.25%-0.89%, as demonstrated by routine histopathological investigation after LC for benign disease [8-12]. In addition, 50%-70% of patients are diagnosed incidentally with gallbladder cancer based on cholecystectomy specimens for presumed benign indications [13]. The prognosis of IGBC (median OS 32.4 months) is better than that of non-IGBC (median OS 17.2 months), [13] and according to the current guidelines, reoperation, including complete portal lymphadenectomy and bile duct resection, is required for patients with T1b, T2 or T3 disease [14]. Since the first case of PSM was reported as an unusual complication of LC in 1991, [15] many centers have reported similar cases, and the incidence of PSM in IGBC is 10.3% [16]. Most of the metastases are found at the extraction site, [16] showing that few wound protection measures (avoiding bile spillage and using retrieval bags) may cause direct contamination and increase the risk of PSM due to the lack of awareness of possible metastases. Other factors related to laparoscopic techniques, including pneumoperitoneum and carbon dioxide, have been described as risk factors [17-19]. PSM, a manifestation of aggressive disease progression, is generally found 1 to 6 months and as late as 4 years after performing LC [6]. Port-site excision (PSE) has been considered a routine treatment, along with radical reoperation, but it has been demonstrated to have no benefits in improving survival, and recurrence at the wound site may be associated with aggressive tumor biology [20,21]. PSE has shown to benefit patients with PSM without other metastases [22,23]. Chemotherapy is now a common therapy [24]. While it is necessary to investigate a larger group of patients diagnosed with IGBC after LC is performed. PSM is thought to be associated with an advanced T stage and poor histopathological features [3]. The median survival duration is typically 10.3 months [16], while the patient described herein remained alive for 2 years without any treatment after the first sign of a recurrent tumor was found by the patient herself. Whether PSM indicates the aggressive nature of the tumor is still not clear. In addition, a longer follow-up study on patients with PSM is needed.
Activated Protein C (APC) Promotes A Healing Phenotype in Cultured Murine Tenocytes Via Protease- Activated Receptor (PAR)-2, but not PAR-1
Background
Tendon is the connective tissue that transmits the force from muscle to bone to facilitate joint movement. Healthy tendon is comprised of fibroblast-like tenocytes between parallel collagen fibres. Injury to a tendon triggers an ordered triphasic healing response: (i) Inflammation, (ii) Repair and (iii) Remodeling [1]. Hindrance to these sequential stages can halt the healing cascade, leading to tendinopathy.
‘Tendinopathy’ is a non-specific term used to describe pathology in, and/or pain arising from a tendon. Indications of tendinopathy include collagen disorganization, increased cellularity and a poor tendency to heal [2,3]. Tendon injuries cause considerable morbidity in the general adult population [4]. The ideal treatment for tendinopathy is yet to be elucidated and should be focused on elucidating the key functional pathways implicated in the disease [5]. Activated protein C (APC) is an endogenous serine protease of physiological importance due to its potent anti-coagulant, anti-inflammatory and cytoprotective properties [6]. Protein C is mostly produced by the liver and is secreted to the blood where it is activated to APC when bound to the thrombin-thrombomodulin complex. Endothelial protein C receptor (EPCR) can enhance this activation. Once activated, APC exerts either its anti-coagulant activity, or while still bound to EPCR it can cleave protease activated receptors (PARs) to elicit cytoprotective effects via numerous signaling pathways, including inhibition of the nuclear factor (NF)- κB, and activation of the mitogen-activated protein (MAP) kinase and glycogen synthase kinase (GSK)-β3 pathways [7]. PAR-1 and PAR-2 have been found to be vital to cell functions in various body systems including musculoskeletal system [8,9], the nervous system [10], cardiovascular system [11], respiratory system [12,13], as well as the integumentary system [14-24].
In a previous study, APC has been shown to stimulate a healing phenotype in sheep tenocytes via the EPCR [25]. APC increased tenocyte proliferation, matrix metalloproteinase (MMP)-2 activity and collagen type I deposition in a dose and time dependent manner [25]. Additionally, the MAP kinase pathway was proposed to be involved; APC dose-dependently stimulated phosphorylated (P)- extracellular signal-regulated kinase (ERK)-2 and inhibited P-p38 [25]. Whilst APC has been shown to exert some of these effects on tenocytes via EPCR, whether and how PARs are involved remains to be elucidated. Understanding the molecular mechanisms of APC is crucial in maximizing its therapeutic potential in tendinopathy.
Methods
Aim
The aim of this study was to determine whether APC stimulates murine tenocyte healing and if so, to assess the involvement of the receptors and underlying mechanisms in vitro.
Cell Isolation, Culture and Treatment
Three weeks old female wild type (WT), PAR-1 knock out (KO) or PAR-2 KO mice (all are with a C57 background) were bred and obtained from Kearns Facility, Kolling Institute, University of Sydney. 6 mice were used for each gene knockout with a total of 18 mice used. Mice were euthanized by a trained, individually; separate from animal room, in a visible chamber, with 100% carbon dioxide with a fill rate of 70% of the chamber volume per minute. Mice were observed for cessation of respiration within 2 minutes and carbon dioxide flow continued for another 1 minute thereafter. After euthanized, mouse-tail skin was physical peeled back; tendon stripped off and cut into an amorphous mass of small pieces. Tenocytes were extracted from the tail tendon using a 0.2 % Type 1 collagenase digestion medium and then cultured in Dulbecco’s modified Eagle’s medium (DMEM) containing 10 % foetal bovine serum (FBS), 100 U/mL penicillin and 100 μg/mL streptomycin. The unused mouse tissues were cremated and discarded. Confirmation of complete deletion of PAR-1 and PAR-2 at the gene level was further achieved by reverse transcription (RT)-PCR. After confluency, cells were trypsinized, reseeded into individual 24-well culture plates, and grew. When approximately 90 % confluency was reached, cells were switched to serum free DMEM overnight, then changed to fresh serum free DMEN and treated with recombinant human APC (Eli Lilly, Indianapolis, Indiana USA).
After treatment, culture supernatants were collected for zymography and cells were lysed by NET lysis buffer (100 mM NaCl, 1 mM EDTA, 20 mM Tris, 0.5 % Triton X100) supplemented with protease and phosphatase inhibitors (Roche, Sydney NSW Australia) for western blot. Cells from passages 1 to 4 were used in experiments. Royal North Shore Hospital Animal Ethics Committee approved usage of mouse tissues. All experiments were performed three times.
Gelatin Zymography
MMP-2 and MMP-9 protein secretion and activation in the cell culture supernatants were detected by gelatin zymography under non-reducing conditions, as described previously [26]. In brief, the proteins were separated by electrophoresis under non reducing conditions with gelatin retained in the gel. After electrophoresis, the gel was renatured with Triton® X-100, and subsequently developed in an appropriate activation buffer. During this development, the concentrated, renatured MMPs in the gel digested the substrate. After incubation, the gel was stained with Coomassie® Blue, and the MMPs were detected as clear bands against a blue background of undegraded substrate. The clear bands in the gel were then quantified by densitometry.
Western Blotting
The expression and activation of ERK1/2, AKT and GSK-β3 by tenocytes were investigated by Western blotting as described previous [25] β-actin was included to assess equal loading.
MTT Assay
Tenocyte proliferation was assessed by the 3- (4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay. Cells were counted and seeded in a 96-well plate with 200 μl of 10 % FBS in DMEM. After overnight attachment, the medium was replaced with fresh 2 % FCS DMEM and APC treatments were applied. Cells were incubated at 37 °C for a total of 72 hrs. Three hrs prior to termination of the experiment, 10 μl of 2 mg/mL MTT solution was added to each well. After 3 hrs incubation, the medium was removed and replaced with 100 μl of dimethyl sulfoxide. The colour change resulting from the solubilisation of formazan crystals was quantified using a microplate spectrophotometer (BioRad) operating at 570 nm. A baseline reading was also taken at 630 nm to minimize background interference.
Scratch Wound Assay
Tenocyte migration was examined via a scratch assay. Cells were counted and seeded into 24-well plates and grown to 70% confluency. One vertical line was scratched down the center of each well using the point of a sterile 1 mL pipette tip, creating a cellfree “wound” area approximately 2 mm in width. To standardize the position of the wound when photographing, small indents were made in the well using a sterile 31G needle. Cells were washed twice with 1 mL of media to flush away any suspended cells. Cells were then starved in 2 % FBS DMEM and photos immediately taken. To distinguish the contribution of proliferation to the migration of tenocytes into the “wound” area, cells were pre-treated with mitomycin C (10 μg/mL, Sigma, Aldrich) 2 hrs before “wounding” to inhibit proliferation. Cells were then treated with 1 μg/mL APC and photos were taken again after 24 hr. Cell migration was determined by calculating the fold change of cells that migrated into wound areas in 24 hours by:
mRNA Isolation and Quantitative Real Time PCR
mRNA was isolated using RNAzol RT Isolation Reagent (Molecular Research Center, Cincinnati, OH USA). Primers for EPCR, PAR-1 and PAR-2 were designed and checked for specificity using the National Center for Biotechnology Information BLAST search tool [27]. The murine primer sequences for EPCR (NM_011171.2: 183bp) were 5ʹ′-ATCTGACCCAGTTCGAAAGC-3ʹ′ (forward) and 5ʹ′- GGCCGGAAACTTACAAAAGC-3ʹ′ (reverse); PAR-1 (NM_010169.3; 199bp) were 5ʹ′- ACTTCACTTGCGTGGTCATT -3ʹ′ (forward) and 5ʹ′- GAAACGATCAACGGCACAAG-3ʹ′ (reverse); PAR-2 (NM_007974.4; 164 bp) were 5ʹ′-CCTTACTGCATCTGCCTACG-3ʹ′ (forward) and 5ʹ′- AATGCACTACGAGCAGAAGG -3ʹ′ (reverse). RT Quantitative PCR was performed to determine the amounts of EPCR, PAR-1 and PAR- 2 gene expression in tenocytes from WT, PAR-1 KO and PAR-2 KO mice (The Rotor-Gene 6000 Real-Time PCR machine, Corbett Life Science, Mortlake Australia). Data were analysed using the relative quantification method, and results expressed as fold change (ΔRn) relative to wild type (WT) untreated samples. β-Actin housekeeping gene expression was used to normalize mRNA levels of PAR-1, PAR- 2 and EPCR.
Statistical Analysis
All data was expressed as mean ± standard deviation (SD). Results were analysed using one-way analysis of variance (ANOVA), in combination with and followed by Tukey post-hoc test. GraphPad Prism software was used for statistical computations. A p-value < 0.05 was considered statistically significant.
Results
Gene Expression of EPCR, PAR-1 or PAR-2 in WT, PAR-1 and PAR-2 KO Cells
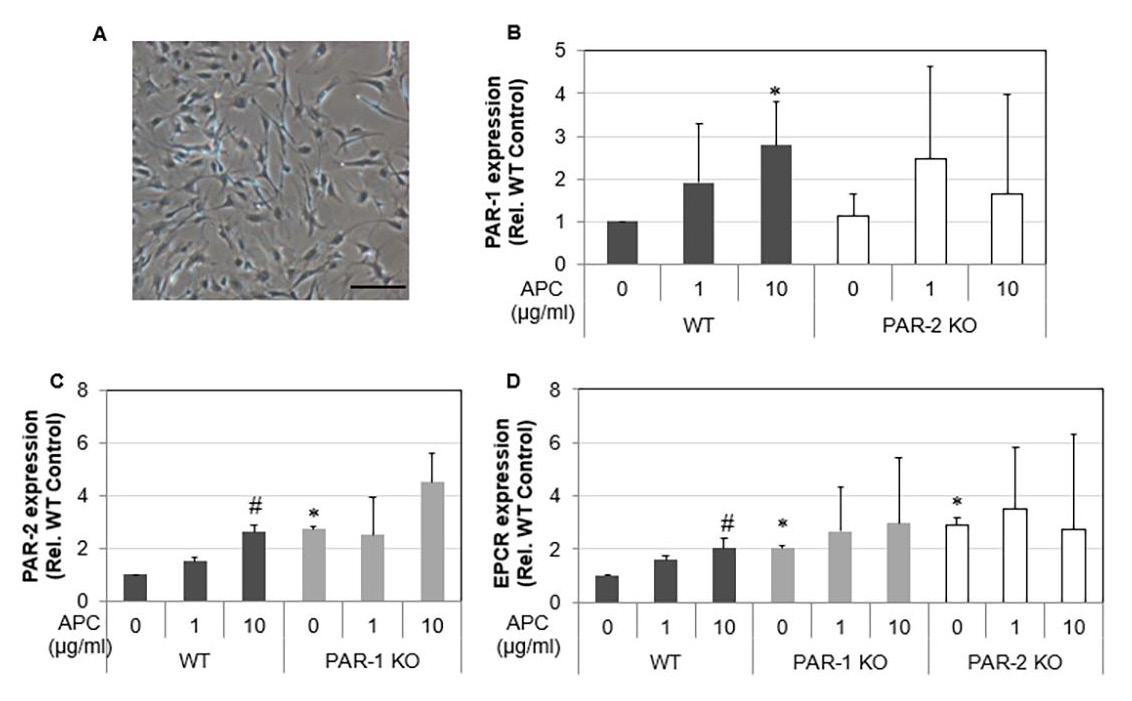
A homogenous cell population was obtained and morphologically identified as fibroblast-like cells. Spindle-shaped contours were observed using inverted phase-contrast microscopy (Figure 1A). Tenocytes from 3 w/o mice demonstrated that, as expected, PAR-1 KO cells had no expression of PAR-1 and PAR-2 KO cells had no expression of PAR-2 (data not shown). Interestingly, expression of PAR-1 by PAR-2 KO cells did not change whereas PAR-2 expression was increased 2.7 folds by PAR-1 KO cells. EPCR expression was stimulated in both PAR-1 KO and PAR-2 KO cells (Figures 1B-1D). In WT cells, EPCR, PAR-1 and PAR-2 expression showed a dose-dependent response to APC treatment. There were 1.6 and 2-fold increases (p<0.05) in EPCR expression in response to APC at 1 and 10 μg/mL, respectively (Figure 1D); a 2.7-fold increase in PAR-1 expression and a 2.7-fold increase (p<0.05) in PAR-2 expression at 10 μg/mL APC by WT tenocytes (Fig. 1B&C). However, the expression of PAR-2 and EPCR by PAR-1 KO tenocytes or the expression of PAR-1 and EPCR by PAR-2 KO tenocytes did not display a statistically significant response to APC treatment (Figures 1B-1D). This data indicates that APC can regulate its receptor expression, while knockout PAR-1 or PAR-2 abolishes this effect of APC.
Figure 1: The gene expression of EPCR, PAR-1 and PAR-2 in WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: Tenocytes at passage 1 from 3 w/o WT, PAR-1 KO and PAR-2 KO mice were treated with APC (1, 10 μg/ml) for 24 hrs. A) Micrograph of tenocytes growing from collagenase digestion tendon at passage 1. Scale bar: 100 μm. B) Gene expression of PAR-1 in WT and PAR-2 KO tenocytes. C) Gene Expression of PAR-2 in WT and PAR-1 KO tenocytes. D) Gene expression of EPCR in WT, PAR-1 KO and PAR-2 KO tenocytes. Quantitative RT-PCR of EPCR, PAR-1 and PAR-2 expression in tenocytes normalized to β-actin. Bars show mean ± SD (n=3). *p< 0.05 vs WT Control and #p< 0.05 vs their own controls, one-way ANOVA calculated using Tukey post-hoc analysis.
Proliferation and Migration of Tenocytes
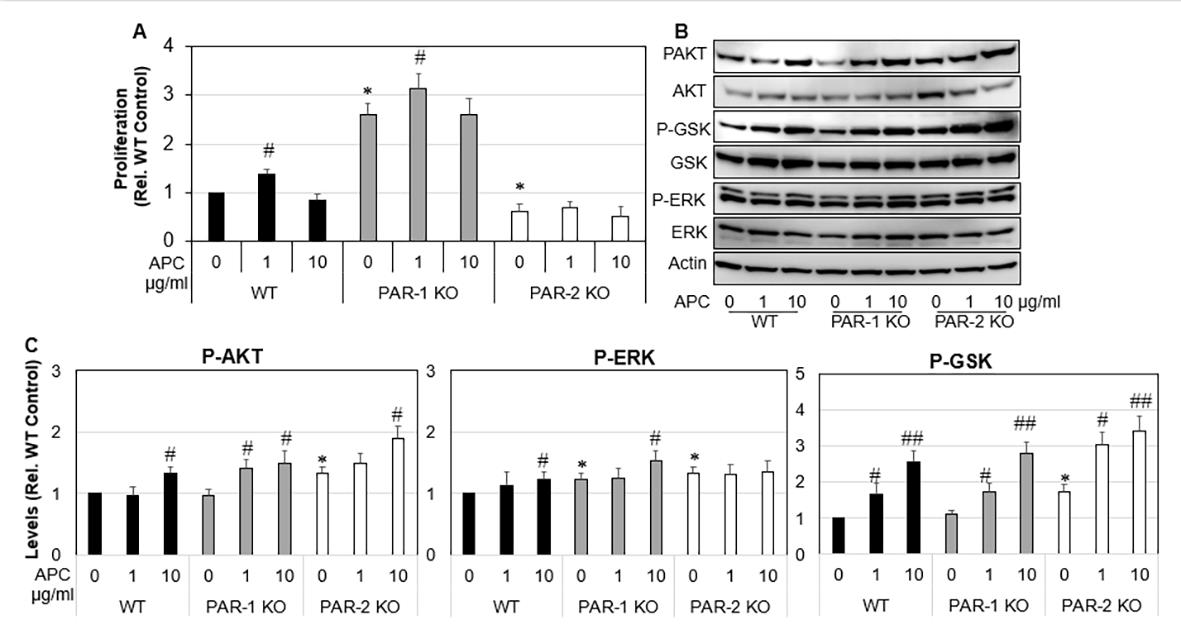
Figure 2: Proliferation and MAP Kinase expression of WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: WT, PAR-1 KO and PAR-2 KO tenocytes were treated with APC (1, 10 μg/ml) for either 24 hrs or 72 hrs. A) Tenocyte proliferation assessed 72 hrs after APC treatment by MTT assay. B) Expression and activation of ERK, AKT and GSK-β3 24hrs after APC treatment detected by Western blot. C) Data are semi-quantitation by Image J and depicted in the graph as fold change relative to control. Results shown are mean ± SD (n=3) *p< 0.05 vs WT Control and #p< 0.05 vs their own controls (no treatment), one-way ANOVA calculated using Tukey post-hoc analysis. ##P<0.01.
Cell proliferation and migration are vital for tendon healing. Under basal conditions, proliferation of PAR-1 KO tenocytes was increased by 3.3-fold compared WT tenocytes (Figure 2A), p<0.0001). In contrast, PAR-2 KO tenocytes showed a 0.6-fold decrease in proliferation when compared to WT control. APC promoted proliferation of WT tenocytes by ~1.3-fold (p<0.05), PAR- 1 KO tenocyte by 1.2-fold (p<0.05) (Figure 2A) at 1 μg/ml when compared to their own controls (Figure 2A). APC had no significant effect on the proliferation of PAR-2 KO tenocytes (Figure 2A). These results suggest that APC dose-dependently promotes tenocyte proliferation, similar to other cells showed previously [28], and this stimulating effect is likely via PAR-2. To investigate the underlying mechanisms, western blot was performed to examine the activation of ERK, AKT and GSK-β3, three intracellular molecules that associated with cell proliferation/survival [7,29-32]. Compared to WT, activated forms of ERK, AKT and GSK-β3 were significantly higher in PAR-2 KO cells (Figures 2B & 2C). APC stimulated the activation of AKT and GSK-β3 in all primary cells, and the activation of ERK in WT and PAR-1 KO cells (Figures 2B & 2C).
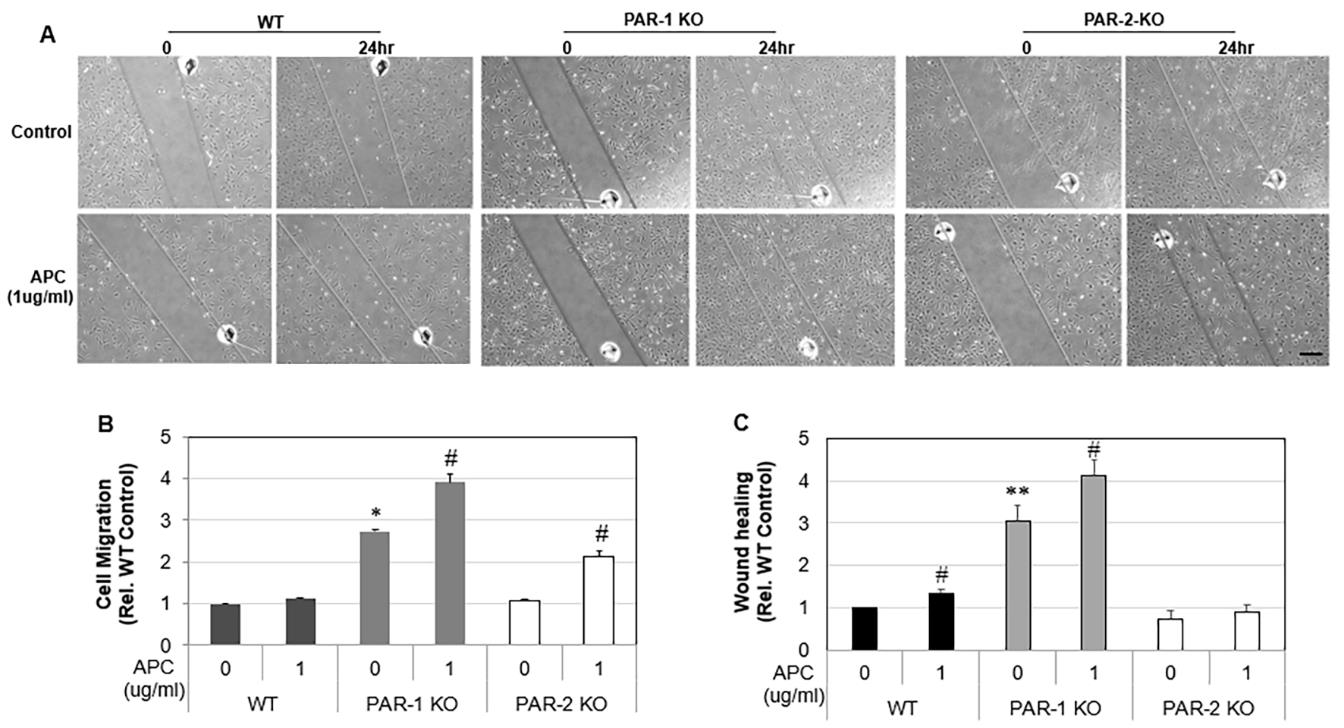
Similar to proliferation, unstimulated PAR-1 KO tenocytes showed a 2.7-fold (p<0.0001) increase in cell migration compared to WT cells, whereas PAR-2 KO tenocytes did not differ from WT control. APC (1 μg /mL) had no effect on WT tenocyte migration (Figures 3A & 3B), but stimulated PAR-1 KO tenocyte migration by 1.4-fold (p<0.0001) and PAR-2 KO tenocytes migration by 2.1- fold (p< 0.001), when compared to their own controls (Figures 3A & 3B). Wound healing is a combined effect of cell migration and proliferation. As expected, wounds created in PAR-1 KO cell monolayers healed 3-fold faster than WT cells (Figure 3C), whereas wounds on PAR-2 KO cell monolayers healed at a similar rate to that by WT control. APC at 1 μg/ml promoted ~1.3-fold increase in wound healing by PAR-1 KO and WT by not PAR-2 KO cells (Figure 3C).
Figure 3: Migration and wound healing of WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: WT, PAR-1 KO and PAR-2 KO Tenocytes were treated with APC for 24 hrs. A) Representative images of migration assay. B) Tenocyte migration assessed 24 hrs after APC treatment (1 μg/ml) by a scratch assay. C) Tenocyte wound healing assessed 24 hrs after APC treatment (1 μg/ml) by a scratch assay. Results are expressed as mean ± SD (n=2). Scale bar: 250 μm. *p< 0.05 vs WT Control and #p< 0.05 vs their own controls, one-way ANOVA calculated using Tukey post-hoc analysis. **p<0.01.
MMP-2 and MMP-9 Expression by Tenocytes
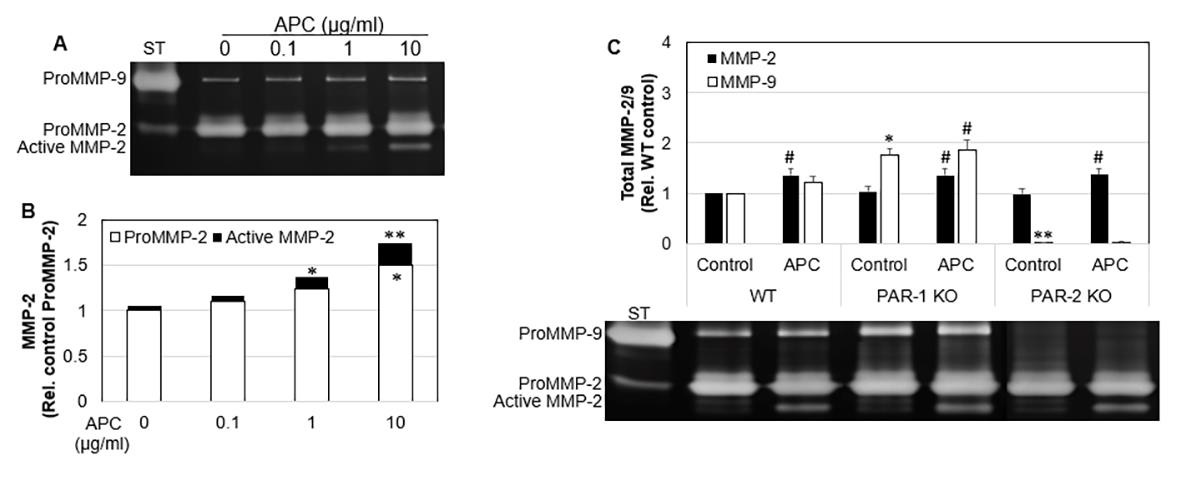
MMP-2 and MMP-9 aid the remodeling phase of healing by contributing to the turnover of collagen and extracellular matrix, and cell migration in many cell types [8,33-35]. Gelatin zymographical data showed that WT tenocytes displayed a dose response increase in MMP-2 expression and activation from 0.1 to 10 μg/mL of APC (Figure 4A). There was a 1.5-fold increase (p<0.05) in MMP-2 expression and 1.7-fold increase (p<0.01) in total MMP-2 at 10 μg/mL APC compared to the control (Figure 4A). APC increased MMP-2 in WT, PAR-1 KO and PAR-2 KO. APC had no effect on WT MMP-9, however, increased MMP-9 expression in PAR- 1 KO cells. PAR-2 KO cells showed decreased MMP-9 expression. These findings show APC increases MMP-2 by PAR-1 and PAR-2, however decreases MMP-9 via PAR-1 and increases MMP-9 via PAR- 2 in murine tenocytes.
Figure 4: The expression and activation of MMP-2 in WT, PAR-1 KO and PAR-2 KO tenocytes in response to APC. Note: WT, PAR-1 KO and PAR-2 KO Tenocytes were treated with APC for 24 hrs. A) MMP-2 expression/activation in WT cell culture supernatants, detected by zonography. Data are semi-quantitation by Image J and depicted in the graph as fold change relative to control. B) Total MMP-2 and MMP-9 in cell culture supernatants, comparing treatment with APC, detected by zymography. Data are semi-quantitation by Image J and depicted in the graph as fold change relative to control. Results shown are mean ± SD (n=3) *p< 0.05 vs WT Control and #p< 0.05 vs their own controls, one-way ANOVA calculated using Tukey post-hoc analysis. **or ##p<0.01.
Discussion
APC is an endogenous serine protease of physiological importance. It has potent anti-coagulant, anti-inflammatory, antiapoptotic and cytoprotective properties. The therapeutic potential of APC has been demonstrated in wide variety of pathologies including sepsis, wound healing, ischemic stroke, lung disorders, kidney injury, diabetic nephropathy, inflammatory bowel disease, systemic lupus erythematosus, amyotrophic lateral sclerosis and cancer metastasis [36-41]. The therapeutic effects of APC on tendon healing have been far less studied. In the only previous study of tenocytes, APC increased tenocyte proliferation, MMP-2 activity, type I collagen deposition and stimulated a healing phenotype in sheep tenocytes [25]. The actions of APC are largely via binding to EPCR, which subsequently activates PAR-1 [42]. However, APC promoted murine skin wound healing via PAR-2, but not via PAR- 1 [43]. Whether and how APC via these receptors mediates the tenocyte healing phenotype has not previously been investigated. In the current study, we demonstrated that deletion of PAR-1 increased tenocyte proliferation, migration and wound healing, whereas deletion of PAR-2 decreased tenocyte proliferation and has no effect on cell migration or wound healing when compared to WT cells; PAR-1 KO and PAR-2 KO cells exhibit increased EPCR expression; APC enhances tenocyte proliferation, migration and wound healing in WT or PAR-1 KO cells, and had limited effect in PAR-2 KO cells. These data indicate that APC promotes tenocyte proliferation and migration by PAR-2, not PAR-1.
Tenocyte proliferation and migration are vital stages of tendon repair [1]. In this study, PAR-1 and PAR-2 displayed differential functions on these two events in mouse tenocytes. This is consistent with a previous study which showed that PAR-2 knockout mice healed significantly slower than wild-type mice and this delayed healing was not altered by adding APC, indicating that APC acts through PAR-2 to heal murine wounds [43]. Similarly, PAR-2 but not PAR-1 modulates synovial macrophage maturation in posttraumatic osteoarthritic mice and thus may play a critical role in the initiation of patient Osteoarthritis [8], and PAR-2 KO mouse synovial fibroblasts exhibited slower rates of proliferation and invasion of than normal cells [9]. These differential functions of PAR-1 and PAR- 2 have also been found in other types of cells or diseases. PAR-1 activation promotes proliferation of human keratinocytes [14] and dermal fibroblasts [15]. It has been shown blocking PAR-1 inhibits APC-induced proliferation in human keratinocytes and thus PAR- 1 appears to promote anti-apoptotic and neuroprotective effects [16,17]. In contrast, PAR-2 affects keratinocyte differentiation, maintains the epidermal barrier, regulates inflammation [18-22] and pain perception [23], and has a tumor-protective role in the skin [24]. In relation to the nervous system, PAR-1 has been shown to mediate mechanisms underlying astrogliosis, vital after brain injury [10].
In regards to the respiratory system, PAR-1 contributes to protective effects of APC on vascular barrier integrity [12] whereas PAR-2 increases ciliary beating which is vital against inhaled pathogens [13]. Additionally, for the cardiovascular system, PAR-1 KO mice have shown an absence of APC’s protective effects against myocardial ischemia/reperfusion injury via inhibition of apoptosis and inflammation [11]. It was found that APC stimulated murine ectopic bone volume and enhances angiogenesis in a model of Bone Morphogenetic Protein 2 induced bone formation. Mechanistically, APC enhances cell proliferation and activates a number of canonical kinase pathways in a PAR1-dependent manner [44]. In comparison, APC induced PAR-1 signaling was shown to regulate the retention and recruitment of EPCR expressing mice bone marrow hematopoietic stem cells [45]. APC was shown to suppress RANKL-induced human osteoclast differentiation mediated through EPCR, PAR-1, S1P receptor, and ApoER2 [46]. While the noted studies above describe different effects of PAR-1 and PAR-2, it must be highlighted that the outcome of PAR activation by the same protease or synthetic agonist can also vary between tissues and cell types [47]. Therefore, the therapeutic role of APC via PARs extends and differs thorough a number of different studies and cell types.
The remodeling stage of tendon healing is predominantly achieved by tissue-degrading enzymes, MMPs [33,48,49]. MMP-9 degrades the ECM days after injury, while MMP-2 participates in both the ECM degradation and remodeling throughout the healing process [34,50,51]. MMP-2 has been associated with increased angiogenesis in in vitro and in vivo studies, however the role of MMP-9 is less distinct [35]. As a result, APC increasing MMP-2/- 9 activity/expression in PAR-1 KO tenocytes may prove vital in stimulating extracellular matrix degradation, angiogenesis and ultimately tendon healing. Other studies [52] have suggested the APC pathway is a potential target for prevention of MMP-2/-9/-13 activation and cartilage extracellular matrix degradation in patients with OA.
The MAPK pathway is essential in regulating key cellular activities including mitogenesis, motility, and survival in many cell types [7]. Although associated with cancer development, distinct MAP kinases including ERK, AKT and GSK-β3 are essential for proliferation and the normal tissue repair process [30-32]. In previous studies, APC has been shown to cleave PARs to elicit cytoprotective effects via numerous signaling pathways, including the MAPK Pathways [29]. In this study, APC stimulated the activation of AKT and GSK in all 3 cell lines, and the activation of ERK in WT and PAR-1 KO cells. This may help explain why PAR- 1 KO mice showed greater cell proliferation. Another study Xue, et al. [25] found that APC dose-dependently stimulated/inhibited ERK/p38 signaling in sheep tenocytes at 24 hours, respectively. It is feasible that MAP kinase signaling in response to APC is different in different species and at different time frames post treatment, being 1hr in our study.
Since tendinopathy can be both hyper- or hypo-cellular [53], fine-tuning the balance between APC’s interaction between PAR-1 and PAR-2 could help regulate tenocyte equilibrium. These finding could be vital as a large body of evidence suggests the promise of regenerative medicine will be achieved by focusing on augmenting the natural healing response, where little is known about the synergistic and antagonistic interactions of growth factors and perhaps their receptors to produce the best effects [54,55].
Conclusion
We demonstrated that depletion of PAR-1 increased tenocyte proliferation, migration and wound healing, whereas depletion of PAR-2 only decreased cell proliferation and had no impact on cell migration or wound healing when compared to WT cells. Depletion of PAR-1 or PAR-2 increased EPCR expression, but has no effect on either PAR-2 or PAR-1 expression. APC enhanced tenocyte proliferation only in WT or PAR-1 KO cells, not in PAR-2 KO cells; promoted migration and wound healing in PAR-1 KO cells; and increased migration only in PAR-2 KO cells. These findings suggest that APC promotes tenocyte proliferation, migration and wound healing largely by PAR-2, and not PAR-1. APC increases MMP-2 by PAR-1 and PAR-2, however, decreased MMP-9 via PAR- 1 and increases MMP-9 via PAR-2 in murine tenocytes. Overall, APC promotes a healing phenotype in cultured murine tenocytes largely via PAR-2, no PAR-1. By shedding light on APC’s therapeutic mechanistic action through PARs, this work has laid the initial platform in maximizing APC’s potential in improving tenocyte healing and treating tendinopathy.
Asymptomatic Submucosal Lipoma of the Anal Canal: A Report of an Incidental Colonoscopic Finding in an Elderly Patient with Colonic Diverticuli
Background
Lipomas are benign adipose tissue tumors commoner between the ages 40 -60 years and have a preponderance in the male gender [1]. They may be solitary or multiple, superficial or deep in location and are usually asymptomatic. Cosmetic concerns (in larger lipomas), pain or discomfort are the common indications for removal of superficial lipomas and these commonly occur in the trunk, head and neck regions. Deep-seated lipomas are relatively uncommon; they occur in the thorax, retroperitoneum or abdominal cavity [2]. Intra-abdominal lipomas usually affect the omentum, mesentery, the submucosa and subserosa of the gastrointestinal tract (GIT) [3]. Lipomas are the second most common non-epithelial benign GIT tumours after leiomyomas [4]. The most commonly affected region of the GIT is the colon, with the highest incidence at the cecum, ascending colon, transverse colon, and the left colon (in decreasing order as one approaches the rectum) [4]. Occurrence of a lipoma in the anal canal is extremely rare with only one case reported so far by Porta et al in 1979! [5]. In diverticulosis of the colon, there is a transmural outpouching of the colonic mucosa through an area of weakness. This mural weakness-the primary pathology in diverticulosis-is of multifactorial aetiology and the predisposing factors include weakened points of vascular entry into the colonic wall, reduced dietary fiber, hereditary factor, reduced physical activity and obesity [6]. In ventral abdominal wall hernias, stretching of abdominal musculature (because of an increase in its content as seen in obesity) and separation of muscle fibers with weakening of aponeurosis are known to weaken the integrity of the fascia leading to herniation [7]. Whilst the role of mural adipose tissue in the development of GIT diverticula is yet to be established, Yekeler et al have however reported a case of two coexisting rarities- an oesophageal lipoma that resulted in an oesophageal diverticulum due to extramucosal impact of the lipoma [8]. We present an interesting incidental finding of a submucosal anal lipoma in an elderly man who had a concomitant presence of colonic diverticula with an increased submucosal adipose tissue in the vicinity of the diverticuli. This case is reported in line with the SCARE criteria for case reports [9].
Case Presentation
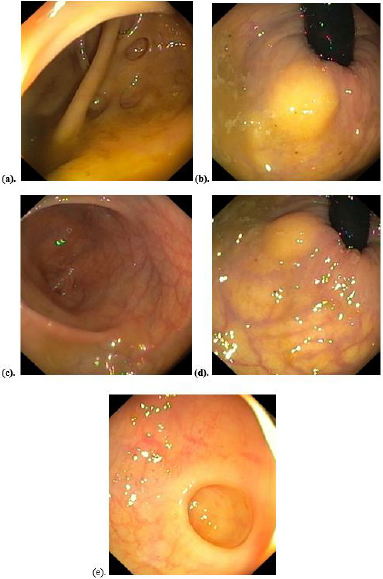
A 70-year-old male retiree was referred for colonoscopy on account of recurrent passage of bloody stool of three months duration, last episode being two weeks earlier. He had no history of anal pain, discomfort, or anal protrusion. There was no change in bowel habit, reduction in stool caliber, melaena, abdominal pain or tenesmus. There was no history of anorexia, haematemesis, early satiety and he does not have a history of peptic ulcer disease. He had no fever, weight loss or any comorbid illness. He had no history of anal trauma or previous anal surgery. No personal or family history of similar illness or malignancy in the past. He was not on any anticoagulation. On examination, he was pale, otherwise other aspects of his general and systemic examinations were normal with a body mass index of 23.1 kg/m2. A pre-procedural rectal examination did not reveal any abnormality. Colonoscopy revealed multiple diverticuli in the caecum, ascending colon and descending colon (Figure 1a) with a 5mm x 3mm sessile polyp in the descending colon. There was a yellowish, oval, submucosal sessile mass (about 10mm x 8mm in widest diameters) with a lobulated surface, about 3cm from the anal verge (Figure 1b). The mass exhibited positive pillow or cushion sign. The mucosa of the transverse colon, sigmoid colon (Figure 1c) and rectum was normal. However, there was an increased yellowish hue to the large bowel submucosa around the anal canal (Figure 1d) and the sites of diverticula (Figure 1e). No stigmata of recent bleeding were seen. The descending colonic polyp was removed with cold biopsy forceps (Figure 2a). The anal submucosal mass was biopsied revealing the characteristic naked fat sign (Figure 2b). The anal submucosal mass was reported to be benign at histology while the descending colonic polyp was reported as an adenomatous polyp with low grade dysplasia. He has been on conservative care for the colonic diverticulum and has remained asymptomatic both for the diverticulum and the anal submucosal lipoma 3 months post colonoscopy.
Figure 1: Colonoscopic findings: a) Caecal diverticuli b) Yellowish submucosal mass of the anal canal c) Sigmoid colon mucosa d) Increased submucosal adipose tissue around anal mass e) Increased submucosal adipose tissue around a sigmoid colon diverticulum.
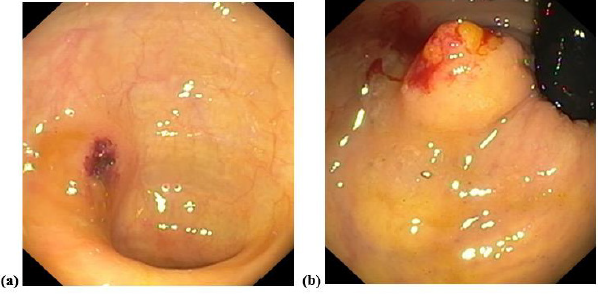
Figure 2:
a) Site of descending colonic polypectomy
b) Anal mass showing spilling out of adipose tissue following biopsy (naked fat sign).
Discussion
Lipomas are common benign tumour of mature adipose tissue that usually occur in superficial locations – most common location being subcutaneous. The relatively uncommon deep-seated lipomas either present atypically or as incidental findings [10]. In the GIT, they are usually subserosal or submucosal in location, the colon being the most affected region. Involvement of the rest of the large bowel decreases anal-ward. We presented an extremely rare report of a submucosal lipoma of the anal canal with a curious finding of concomitant existence of divertculi at areas of increased submucosal adipose tissue. We discuss this case in terms of rarity and then, its peculiarities. The rarity of this case lies in the fact that it is a deep-seated lipoma occurring in the anal canal. The most distal GIT lipomas reported in the literature are those of the rectum and these presented as polypoid submucosal masses protruding through the anal canal or casuing rectal bleeding [11,12]. Beyond the rectoanal canal, the perianal region, lipomas are also rare with a report of a perianal lipoma occurring years after surgery for a perianal abdscess [13]. The aetiology of the perianal lipoma was likely traumatic, similar to the report by Uscilowska et al on para-anal lipoma resulting from perineal trauma [14]. Beyond trauma, the other risk factors for lipoma formation include genetic predisposition, obesity, hyperlipidaemia and diabetes mellitus [15]. There risk factor for lipoma in our patient was not apparent. This was not a surprise since such deep-seated lipomas are incidentalomas like in our patient. Colonic lipomas are usually asymptomatic except when they are larger than 2cm, torsed, or pendulated. The small size, submucosal location and sessile nature of the lipoma in our patient may explain the asymptomatic nature. The sigmoid colon is said to be the commonest site of colonic diverticulosis, although a study on our patient population by Akere et al revealed right colonic preponderance [16,17] The endoscopic appearance of most colonic diverticuli is that of an outpouching of the mucosa with an otherwise pink-looking mucosa/submucosa due to the rich vasculature of these layers. In diverticulitis, the mucosa of the diverticulum is reddened with or without a surrounding fibrinous slough [18]. The peculiarity of our report is the increased submucoal adiposis in the vicinity of colonic diverticuli, with a predominantly yellowish (than pink) hue to the mucosal color (Figure 1e). These diverticuli involved the caecum, ascending and descending colon with none in the sigmoid colon, the mucosa of which appeared normal (Figure 1c). It therefore stimulates curiosity as to a possible link between increased large bowel mural adiposi and a possible predisposition to subsequent diverticulum formation in the areas where these adipose tissues are located. The plausibility of this link may not be far-fetched if the underlying pathology of colonic diverticulum- mural weakness-is considered. It is therefore more compelling to associate increased submucosal adiposis in our patient with his colonic diverticuli considering the established effect of same adipose tissues on tougher tissues like aponeurosis in abdominal wall hernias. Whilst colonic diverticulosis is commoner in older patients like our patient, Brouland et al reported a large colonic diverticulum in a young male arising due to colonic mural weakness by multiple colonic lipomatosis [19]. The risk factors for colonic diverticulosis include comorbidities (like hypertension and diabetes mellitus), increased luminal pressure (from colonic dysmotility, reduced dietary fiber), genetic risk factors (like Ehlers-Danlos syndrome, Coffin-Lowry and renal polycystic disease), obesity/reduced physical activity, smoking and increasing age [20]. Age alone may not explain the diverticuli seen in our report and none of the other known risk factors was apparent. Although the endoscopic features of the submucosal anal mass we reported were in keeping with a lipoma, histological report did not show the presence of adipocytes. This is a common limitation of endoscopic biopsies where only the mucosal layer is usually biopsied except multiple biopsies are taken at the same spot to include deeper layers. A limitation of this report is our inability to do endoscopic ultrasound which would have confirmed the location of the lipoma. Facility for endoscopic ultrasound is not available in Nigeria as at the time of this report to the best of our understanding.
Conclusion
Lipomas of the anal canal are rare. Although an incidental endoscopic finding in this report, coexistence of large bowel lipomas with increased submucosal adiposis in the vicinity of colonic diverticuli may suggest an aetiological role of such lipomas in colonic diverticulosis.
Comparing In-Lab Full Polysomnography for Diagnosing Sleep Apnea in Children to Home Sleep Apnea Tests (HSAT) with an Attending, Online Video Technician
Introduction
Obstructive Sleep Apnea (OSA) in children is a recognized childhood health disorder with an estimated prevalence ranging from 1% to 5% [1,2]. The clinical manifestations usually include snoring, disrupted sleep, restlessness, sweating and salivation during sleep, and excessive daytime sleepiness or hyperactivity and irritation [3,4]. OSA in children is characterized by irregular, partial, or complete obstruction of the upper airways during sleep, with the disruption of normal ventilation and sleep patterns caused usually by hypertrophy of the adenoids and tonsils. Risk factors include obesity, neuromuscular disease, Down syndrome, and micrognathia [3,5]. Continuous quality sleep is essential for growth, development, good health, and well-being. Left untreated, OSA can lead to adverse health, developmental, and behavioral outcomes [5-7]. Considering the high prevalence of OSA and its deleterious consequences, access to early and accurate diagnosis is critical. Overnight, in-laboratory, technician-attended Polysomnography (PSG) is considered the gold standard for diagnosing OSA in children [2,8]. PSG provides objective measures of sleep quality, sleep architecture, respiratory parameters, and an index of the breathing disturbance during sleep. However, the in-lab PSG test has some distinct limitations and disadvantages, especially for diagnosing OSA in children. In particular, in-lab PSG does not simulate the child’s sleep in his or her familiar home environment. Moreover, placement of multiple sensors and electrodes by an unfamiliar technician in a strange room and bed can be stressful to young children and many times impairs not only their cooperation but also the quality of sleep that the PSG test purports to measure [9]. In addition – hospital-based diagnostic testing limits access to families living far from centrally-located medical diagnostic services. Beyond these difficulties, the coronavirus (COVID-19) pandemic has reduced access to in-lab PSG more generally, as healthcare providers paused many non-urgent health care services in order to decrease the risk of infection, especially in hospital environments. This led to near-complete closure of sleep laboratories and clinics during lockdowns around the world. As a result, concerns about lab-based sleep studies now include not only questions of their efficacy, but also of their safety. As a result, the Home Sleep Apnea Test (HSAT) for children is increasingly considered as an alternative to in-lab PSG. In contrast to adults, where home sleep tests for diagnosis of OSA is the common practice, the clinical use of HSAT in children is not well established. In particular, there are few studies comparing the effectiveness of HSAT to PSG for diagnosing OSA in children. This shortcoming is significant, as the use of HAST has the potential to improve the validity of the sleep study, while reducing possible exposure to infectious diseases during overnight hospital stays. In addition, making HSAT more widely available can increase access to needed sleep studies for children. The 2017 American Academy of Sleep Medicine (AASM) Position Paper summarized four published articles focusing on the technical feasibility of HSAT for evaluating OSA in children. The paper concluded that the validity of the home test depends on the training of the person who places the sensors and is reduced when the sensors were placed by untrained caregivers instead of trained professionals [8]. To assess the validity of data obtained from HSAT, this study tested the impact of providing home caregivers with prior training as well as the support, in real time, of an attending online video technician on the night of the sleep study. The technician guided them set up the system, place the sensors, and then monitored the child throughout the night using a web camera. Comparing the data obtained from these assisted home sleep studies to those obtained in standard PSG studies, we hypothesized that HAST with attending on-line technician can provide valid and reliable way for diagnosis sleep apnea in children.
Methods
Participants
100 children, 54 boys and 46 girls, ages 3-11 (average age 5.2, SD 1.2) assigned randomly either to in-lab full polysomnography or to a Home Sleep Apnea Test (HAST). All children were referred to a sleep study in order to rule out sleep apnea.
Polysomnography
For in-lab full polysomnography we used a standard inlab Somnoscreen-PSG type sleeping test device (Somnomedics, Germany). Sleep channels included: Electroencephalography (EEG), Electro-Oculography (EOG), leg and chin Electromyography (EMG), nasal flow, chest and diaphragm breathing, snoring, Electrocardiography (EKG), heart rate, blood oxygen saturation, body position, and video.
HAST
For the Home Sleep Apnea Test (HAST) we used a Somnotouch home sleep testing system (Somnomedics, Germany). Sleep channels included: nasal flow, chest and diaphragm breathing, snoring, heart rate, blood oxygen saturation, activity, body position, and online video recording using a Xiaomi 360 web-camera and portable Wi-Fi card.
Procedure
In-lab PSG: The sleep testing room was a standard test room at the Sleep Medicine Research Center at Assuta Medical Center. The child and his or her parents were invited to the sleep center at 8:00 PM. A skilled and trained technician interviewed the parents about the medical history of the child and then connected the child to the full PSG system in the sleep lab. The technician monitored the child’s sleep throughout the night from the control center in the sleep lab. The next morning, the parents completed a standard satisfaction questionnaire. Sleep data were analyzed by a skilled and trained sleep technician in accordance with the AASM guidelines (AASM, 2007). We calculated continuity and architecture sleep parameters in addition to breathing and oximetry parameters, including the number of apnea and hypopnea, Apnea Hypopnea Index (AHI), baseline and minimum saturation, the number of desaturations, the percentage of sleep time with O2 levels below 90% saturation, and the percentage of time spent snoring. HAST: The parents came without the child to the sleep center at Assuta Medical Center on the evening of the sleep study to meet a professional sleep technician for 20 to 30 minutes. During the meeting, the technician reviewed the child’s medical history and then taught the parents how to set up the system for conducting the home sleep study. After practicing what they learned, the parents returned home with the home sleep test system, including a digital video camera. Using real-time video, the technician guided the parents at home while they set up the system and placed the sensors on their child. After the parents completed the setup, the technician monitored the child’s sleep throughout the night using the digital web camera. If there were any technical issues, such as a problem with the attachment of a sensor, the technician telephoned the parents and guided them as they made necessary corrections. After the child woke up the next morning, the parents removed the sleep system and returned it to the sleep center for analysis. The parents were asked to complete a satisfaction questionnaire similar to that filled out by parents after PSG. Sleep studies were included in data analysis if at least 70% of the information collected during the study was valid. For the HSAT studies, a professional scoring technician calculated the Total Sleep Time (TST), Time In Bed (TIB), Sleep Efficiency (SE), number of apnea and hypopnea, Apnea Hypopnea Index (AHI), baseline and minimum saturation, the number of desaturations, the percentage of time below 90% saturation, and the percentage of time spent snoring.
Results
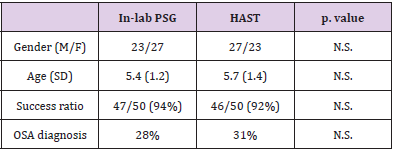
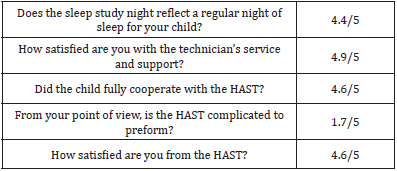
T-tests found no significant differences in the demographic profiles of the children in the PSG and HSAT groups (gender and age), in the success ratio, or in the OSA diagnosis between the sleep studies conducted with in-lab PSG and HAST (Table 1). Table 2 presents the Apnea Hypopnea Index (AHI), Oximetry Disorder Index (ODI), Baseline blood saturation (Baseline O2), minimum blood saturation (minimum O2), percentage time of blood saturation below 90% (TIB90%), Time In Bed in minutes (TIB), and Total Sleep Time (TST). Again, t-test comparisons found no significant differences between the in-lab PSG and HAST in any of these parameters with the exception of one: Time In Bed (TIB) and Total Sleep Time (TST) was significantly longer in the HAST group than in the PSG group. Survey results indicated that parents were very satisfied with HAST. In general, the parents gave high scores for the HAST. They reported that the night reflected a regular night of the child, the setup was friendly and easy, and the technician was available and pleasant (Table 3).
Table 1: Demographic, success ratio, and the percent diagnosed with OSA: in-lab PSG vs. HAST.
Table 2: Breathing disorder index (AHI), oximetry parameters (ODI), time in bed (TIB) and total sleep time duration (TST).
Table 3: Parent HAST Satisfaction Rankings.
Discussion
This study found no significant differences between data obtained from in-lab full PSG and HAST in all breathing and oximetry parameters for diagnosis of Sleep Breathing Disorder (SBD) in children. It is important to note that the majority of children are referred to sleep laboratories in order to rule out sleep-related breathing disorders [10], making it important that evaluations focus on child breathing and oximetry channels and video (picture and sound). These results support those from previous studies that found no differences between HAST and in-lab PSG for evaluating OSA in children. For example, Goodwin et.al report no differences in PSG performed within two months after HAST in the respiratory parameters [11]. Jacob et al. performed both a HAST and PSG within one week for diagnosis of OSA in children and revealed good correlation between the two types of studies [12]. Finally, Alonso-Alvarez and colleagues compared simultaneous HAST to PSG and found no significant differences in total number of apneas or hypopneas between the HAST and the PSG, or in-laboratory respiratory polygraphy studies [13]. However, these studies did not address the concern that data validity can be affected by the training of those who set up the home sleep system. This study addressed this shortcoming by providing the attendance, supervision, and support of a real time online video technician, yielding reliable data in a setting more favorable to the accurate diagnosis of OSA in children. The gold standard for the diagnosis of Obstructive Sleep Apnea (OSA) in children is in-laboratory Polysomnography (PSG) [2,8]. One major reason for the preferability of in-lab sleep study is the demand for a skilled technician during the setup phase and to control the sleep study. In our HAST we used an online technician that was an all-night attendant, using a web video camera, in order to monitor the sleep study. We find that the parent’s guidance before the sleep study and the technician’s online video supervision during the set-up of the system on the child, and online monitoring during the night, can replace the physical attendance of technician. Additional support for the value of HAST comes from the fact that there were no significant differences in the failure rate of sleep studies between in-lab full PSG and HAST with an online technician, indicating that there was no observed advantage for the physical attendance of the technician over the online attendance. Finally, significantly longer sleep times of the children in HAST with online support indicates that sleep is better in a child’s natural environment, improving the quantity and the validity of data obtained from the home sleep study. This addresses one of the major challenges for in-lab sleep studies for children. Although home sleep apnea testing is widely used in adults to diagnose OSA [14], its use in children has been much more limited, reflecting concerns about its validity for accurately measuring the duration of sleep time. A major challenge with HAST in children is the difficulty in determining the sleep time without using EEG, EOG, and EMG channels. Actigraphy is suggested as a reasonable technique for measuring sleep due to its high accuracy (85-90%) and sensitivity – the ability to correctly identify sleep (90-97%). Marino et al. concluded that actigraphy is a useful and valid means for estimating total sleep time with some limitation in specificity (the ability to correctly identify alertness) [15]. Yet, specificity has been higher in studies of nocturnal sleep-in children (54-77%) [16]. In our data, the Time In Bed (TIB) and the Total Sleep Time (TST) were significantly longer in HAST compared to in-lab PSG. In our HAST we calculated Time In Bed (TIB) and Total Sleep Time (TST) using two more channels besides activity: position and video. We believe that the combination of these three channels is more sensitive and specific than activity only. It needs to be evaluated in more studies. A major question with in-lab full polysomnography is, “Does the sleep study in the sleep lab reflect the regular sleep of the child?” From our extensive experience in the Assuta Medical Center sleep lab, some children will experience major problems sleeping in an unfamiliar environment and not in their own bed. Moreover, even when they succeed in falling asleep in the sleep lab, their sleep does not simulate that experienced at home. The parents’ responses to the study questionnaire supports our hypothesis that home sleep studies improve the validity of sleep data collected to diagnose OSA in children. From the parent’s answers we observed a high rate of similarity between the HAST night and a regular night for the child. Moreover, parents report high cooperation from the child for the sleep study at home and high satisfaction from the HAST in general. Although the coronavirus pandemic (COVID-19) advanced the use and legitimacy of telemedicine in many areas in medicine, its advantages in diagnosing OSA in children are significant. With the real-time online attendance of a sleep technician, this study showed that home sleep studies can provide data of equal quality to in-lab PSG while improving the quality and duration of a child’s sleep, reducing in-hospital exposure to infectious disease, and improving access to diagnostic services for families living far from centrallylocated medical services. Taken together, these advantages of HAST, when supervised by a real-time online technician, suggest that it should be the first choice for diagnosing OSA in children.
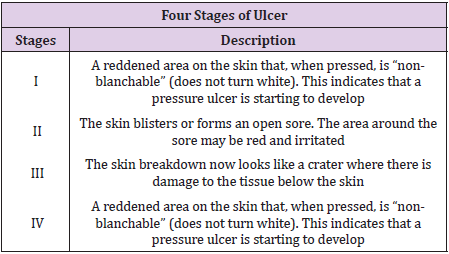
Pressure ulcers (PU) occur mainly in bedridden patients and are difficult to manage and treat once they develop. Patients who are unable to change their position because of spinal cord injury, cerebrovascular accident or general weakness are at a high risk of developing PU. These patients are typically elderly, have a long hospital stay and often have multiple comorbidities. The perioperative period is the time period of a patient’s surgical procedure. It commonly includes ward admission, anesthesia, surgery, and recovery. Perioperative may refer to the three phases of surgery: preoperative, perioperative, and postoperative, though it is a term most often used for the first and third of these only – a term which is often specifically utilized to imply ‘around’ the time of the surgery. Pressure ulcers can induce serious problems during patient care processes. A pressure ulcer is an area of localized damage to the skin and underlying tissue caused by pressure, shear, friction, and/or a combination of these. Recent studies have suggested that the overall incidence of pressure ulcers in the hospital range from 1%-11%, whereas the range varies between 4.7% and 66% among surgical patients. Different kinds of prevalent pressure ulcers have been reported in different countries, ranging from 10.1%-23.1%.
This indicates that surgical patients are usually at a high risk of developing pressure ulcers. The incidence of pressure ulcer leads to greater misuse of nursing resources and high medical costs. Pressure ulcers are not only adverse events in a hospital stay, that have to be treated and justified, but represent also a quantifiable risk in terms of morbidity and mortality. Adjusted for hospital, diagnosis related group (DRG), sex, race and age group, a case-control study revealed 3.98 extra days in hospitals and 7.23% attributable mortality, if a pressure ulcer occurs (Zhan & Miller 2003). From 1990-2001, pressure ulcer was mentioned as one cause among others for 3.79 deaths per 100,000 population in the USA (Redelings et al. 2005) as against the single underlying cause in 18.7%. The authors identified a high concurrence with sepsis (39.7% of all deaths with indication of a pressure ulcer). The risk factors associated with pressure ulcers amount to more than 100 and include medical diagnoses, patients’ demographic characteristics, anthropometrics, physiological status, nutritional status, and hospital environment, among others. The occurrence of pressure sores is a main obstacle to the long term rehabilitation of spinal-cord injured patient [1-3] (Table 1).
Table 1:
To achieve the best functional result with the most efficient use of resources, a comprehensive treatment plan is needed, that include preoperative workup, physical therapy, nutritional considerations, wound care, treatment of spasticity and reflex spasm, pre and postoperative bowel management, pulmonary consideration, anesthetic consideration, antimicrobial regimen. Surgical patients are prone to developing HAPU. In the United States, patients with HAPU had a longer length of stay, higher total hospitalization costs, and greater odds of readmissions compared with patients with no HAPU. Preventing HAPU involves accurate and ongoing risk assessments so that preventive measures can be implemented as early as possible and carried out throughout the period of immobility. The prevalence of HAPU among surgical patients is about 8.5% or higher depending on the type and the duration of the surgery. Patients with proximal femur fractures or patients after major lower limb amputation, the incidence of pressure ulcers was high (10.4% and 8.8%, respectively). Patients undergoing bowel surgery and peripheral vascular reconstructions are also prone to developing pressure ulcers. Several plausible mechanisms might be accounting for increasing risk of infections in relation to prior pressure sore exposures [4-6]. To start with, pressure sores were perceived to induce impairment of skin protection function by destroying integrity of erythematous skin and prompting reproduction and growth of pathogenic bacteria.
Pressure ulcers might introduce possible resources and entrances of pathogens to human body, which was possible to result in local infections in human body. Secondly, chronic pressure ulcers were supposed to persist chronic inflammation, which might lead to stimulation of cytokines and inflammation factors. An expansive literature suggest that long-term and excessive consumption of cytokines and inflammation factors might be accounting for immune suppression, and in turns led to a weaken ability to prevent invasions and attacks of pathogens. Thirdly, immobilization, as a primary risk factor for the occurrence and development of pressure sores, was considered to be associated with pneumonia. Immobilization might have destructive effects on removing function of bronchial secretions, which was conductive to reproduction of pathogen and help to result in pneumonia. Studies demonstrates an increased risk of several specific infections (surgical incision infection, pneumonia, urinary tract infection) within 14-day after spinal cord operation in patient with pressure sores preoperatively. Among the four stages of pressure ulcer, stage IV has the highest risk of postoperative infections. Intensive care units (ICUs) have the highest PU incidence rates in health care settings, which have been reported as high as 50% .The high rates in the ICUs can be attributed to the high acuity of patients, the nature of their critical illness and the highly invasive nature of the interventions and therapies that critically ill patients receive. Identifying patients at risk for PU development is essential for the effective implementation of PU prevention programs and usage of resources [7-10].
Method
Cochrane Library, MEDLINE/ PubMed, Scopus, CINAHL were used. The search was limited to the English language. In a final search, the reference lists of the included articles were also handsearched to identify further relevant articles.
Eligibility Criteria
Studies met the inclusion criteria if they assessed the effects of preventive measures on surgical patient. If the full text of an article could not be obtained, we included its abstract only when it had sufficient data.
Study Selection
Two independent reviewers screened and selected articles based on the title, subsequently on abstract and finally on full text. Disagreements were resolved via discussion with a third reviewer.
Data Extraction
The following information was extracted from the studies that met the eligibility criteria:
a. first the author’s name and year of publication;
b. participant characteristics (country of origin, sample size and mean age);
c. study characteristics (methods of participant allocation, allocation concealment, blinding, drop-out rates and reasons for drop-outs);
d. nature of aromatherapy intervention (type, dose, duration, route of administration for experimental and control interventions);
e. outcomes (instrument used to assess anxiety and outcome data).
Quality Assessment
The risk of bias of the included studies was assessed independently by two reviewers using the Cochrane Collaboration’s ‘Risk of bias’ tool. The criteria consisted of selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), and reporting bias (selective outcome reporting). Each item was classified as ‘low risk of bias’, ‘high risk of bias’, or ‘unclear risk of bias’. Disagreements were resolved by discussion between two reviewers.
Description
Pressure ulcer development was strongly correlated with indication for admission. In specific patient categories, such as patients with proximal femur fractures or patients after major lower limb amputation, the incidence of pressure ulcers was high (10.4% and 8.8%, respectively). Patients undergoing bowel surgery and peripheral vascular reconstructions are also prone to developing pressure ulcers [11-15].
Preoperative Work-Up
Patient Candidacy: Prior to becoming a candidate for reconstructive surgery, the patient must be prepared physically and mentally endure 6-10 weeks of hospitalization. Patient exhibits selfmotivation since a successful result is obtainable only with patient cooperation. The team approach for spinal cord injured patient. The physical medicine and rehabilitation physician is the primary care doctor for the spinal cord injured patient and intimately involved with perioperative care. Before a procedure the patient must be in optimum physical health, be free of spasms and contractures, be in adequate nutritional status, be able to tolerate the prone position (if needed) and have adequate pulmonary function.
Physical Therapy for SCI Patients: The role of physical therapist have great importance in the care of SCI patient, that prevent contractures. The exercise and proper positioning in bed combat the deforming forces caused by paralysis and spasticity. Custome cut out cushions are useful in proper positioning. The occupational therapy department aids our patient with positioning which causing iatrogenic skin problems. A pressure pad evaluation aids the selection of a cushion with the best pressure distribution properties for the patient with a tendency towards decubitus ulcers.
Preoperative Positioning: Surgical candidates must tolerate prone position for a minimum of 4 weeks postoperatively and must exhibit operatively the ability to maintain the position adequately. Position individualized according to the location of pressure sores. Prone position is mostly applied since the pressure ulcer seen in ischial, sacral, and trochanteric area mainly. The prone position is assumed for 4 week postoperatively with side-side movement and range of motion beginning 6-7 week post operatively.
Nutritional Consideration: Before surgery nutritional status must have priority. The serum albumin level should be greater than 35g/100ml, the lymphocytic count should be greater than 220g%. Delayed cutaneous hypersensitivity is also indicator of decreased visceral protein. Inability to respond to placement of purified protein derivative, mumps, or candida antigens correlate and with higher rates of sepsis and high mortality rates in acute surgical patient.
Wound Care
Preoperative Wound Care: The care of the open ulcer consists of debridement of obviously devitalized tissue. Debridement is done surgically just to the point of bleeding with additional debridement accomplished by frequent dressing changes using mesh gauze sponges/kerlix to debride the wound, decrease the bacterial count. The use of povidone – iodine offer no therapeutic benefit over the use of saline in wound treatment.
Roengenograms: Chest and pelvic roentgenograms are routinely done preoperatively. If there is a large wound with a tracking sinus, a simple sinogram is performed using radio opaque dye injected through a foley catheter to evaluate the extent of the ulcer and help in the preoperatively planning for reconstruction.
Treatment of Spasticity and Reflex Spasms: Excessive reflex activity below the level of the upper motor neuron lesion often exists after a spinal cord injury. The obliteration of supraspinal inhibitory pathways is the reason postulated for this phenomenon. In the immediate postoperative period the spasms can cause bleeding and hematoma that may result in flap necrosis.
Medical Treatment: The drug of choice at the institute for rehabilitation and research is baclofen, which is believed to act centrally and poly synaptically within the spinal cord and brain stem. This begun at a dosage of 5-10mg 4 times a day, not to exceed 100mg daily. Side effects are minimal in patient with SCI, however with a dosage greater than described memory lose and confusion may occur. Diazepam may be used alone or with baclofen. It acts centrally within the brain stem and cerebral cortex to affect spasticity with initial dosage 5mg a day until a total use of 40mg a day is reached. Dantrolene can also be used for the treatment of spasms, it acts on excitation-contraction coupling mechanism of muscle fiber itself. It has a bed effect on liver so that serum glutamic pyruvic transaminase must be monitored monthly. Initial dosage is 25mg twice a day, increased to 25mg 4 times a day then by 25mg increment every third to fifth day to a maximum 200mg daily.
Surgical Management of Spasms
Nerve Blocks: Usefulness of peripheral nerve block is primarily confined to patients who have incomplete lesions and who are not candidates for subarachnoid blocks, since we want to preserve as much sensation and useful motor functions initial attempt with lidocaine, have to repeat as needed.
Epidural Stimulator: Most useful in patients with incomplete lesions but costly.
Subarachnoid Blocks (Phenol Rhizotomy): Useful for patients with complete lesions. Specific for lower extremities and don not affect the trunk and upper extremities.
Urological Management
Initially indwelling catheter is utilized following by intermittent catheterization with or without a condom catheter. Patients who are not voiding or who have high residuals are given methenamine as well as ammonium chloride (1 mg of each every 6 hrs).
Proper Diet and Bowel Management: We have found that even the most complex pressure sores can be successfully managed without a diverting colostomy.The preoperative regimen begun 3 days prior to surgery with a clear liquid diet. The bowel is cleansed with enemas and mild laxatives.
Postoperative Diet and Bowel Management: The clear liquid diet is continued for 5 days postoperatively.1 tab (2.5mg) twice a day is given for 5 days to constipate patient. If contamination does occur the area is thoroughly cleansed and dried immediately. The patient resume their prior bowel program on the 6th day postoperatively.
Antimicrobial Regime for the Decubitus Ulcer: Clinical and experimental studies indicate that anti-microbial agents prevent infection when effective concentrations are prevent infection when effective concentration are present in tissues during or shortly after the surgical procedure. Maximum bacterial shedding occurs during this time. A single parenteral dose of antimicrobial agent is given just prior to surgery, providing adequate tissue levels throughout the procedure. Antibiotics are selected on the basis of preoperative cultures and sometimes modified when the result of intraoperative cultures are known. The duration of administration of antimicrobial agents is individualized, based on the extent inflammation, suppuration, sinus tracts, and bone involvement.
Septic Patient with Decubitus Ulcer: The sin qua none of the treatment of sepsis associated with decubitus ulcer is surgical debridement. The antibiotic regimen is also need for aerobic and anaerobic bacteria.
Pulmonary Consideration: Vital capacity is measured preoperatively in the prone and supine position. After the patient position is changed, he or she is observed for clinical signs of respiratory embarrassment, Arterial blood gas may be obtained 20 minutes after the patient’s position changed.
Sitting Regimen: A pressure pad evaluation must be performed postoperatively to determine new sitting surface requirement. Sitting is begun in the sixth or seventh postoperative week, beginning with 30 minutes of sitting twice during the first day. Lanolin massage of surgical site keeps the area soft and moist. However, pressure ulcer rates can only be used as an indicator of quality of care if certain crucial aspects of data collection and interpretation are taken into account. The VP pad is better than the HDF pad in relieving pressure. However, the measured average pressures for both types of pads were all higher than the threshold value of the capillary closing pressure (32mmHg; Schultz, 2005). Neither of them could reduce the pressure below the capillary closing pressure, which may have contributed to the occurrence of pressure ulcers in both groups. Both the average and peak pressures, measured after applying the VP pads, were significantly lower compared to measurements of the HDF pad; however, there was no significant difference between the two types of pad regarding the prevention of pressure ulcers.
Obese individuals had significantly lower values of surface pressure and shear force than slender individuals at the coccygeal bone site. At the sacral bone site and the thigh site, the values of surface pressure in the obese group were significantly higher than those of the slender group. The reason why obese subjects had higher values was not obvious, but the magnitude of pressure at the sites was low, and so the effect of bony prominences would not be apparent by weight distribution in the obese types. In clinical practice, subjects should be positioned at the bending conformity point or shifted 10cm from that point toward the head of the bed whenever bed operations are performed in order to avoid generating harmful shear forces and surface pressures. There are multiple possible reasons behind the correlation between PCA use and increased pressure ulcer incidence. Frist, the use of a PCA pump can relieve the sense of pain, a decreased sensation and blocked motor nerve owing to a PCA pump might accelerate the development of pressure ulcers. Meanwhile movement actually can be considered self protection for bedridden patients, however PCA can reduce the patient’s sense of pain so that they will reduce their movement, which can reduce the patient’s ability to self protect. Similarly the use of PCA may make patients over emphasize the disease severity so that they may fear moving.
Second because a PCA pump can relieve painful sensations, patients may be less willing to move in order to stay comfortable. Third in order to avoid the events of catheter prolapse and compression, postoperative patients are fearful of moving. Bed- or wheelchair-bound patients tend to suffer from multiple pressure sores and often undergo several operations over the years for reconstruction of the tissue’s integrity. This makes every pressure sore recurrence over previously reconstructed and therefore scarred tissue more complex to treat. Fillet flaps from nonfunctioning body parts not only impose little or no donorsite morbidity but can also prolong pressure sore recurrence by offering robust tissue for padding. In paraplegic patients with massive or bilateral pressure sores, where all other reconstructive measures have been exhausted, fillet flaps offer a last resort option for pressure sore management.
Conclusion
Conscientious effort is needed to prevent the development of HAPU through the early identification of risk and early implementation of preventive measure. So in my opinion when we compare all the points in discussion most applied and applicable method to achieve the best functional result with the most efficient use of resources, a comprehensive treatment plan is needed, that include preoperative workup, physical therapy, nutritional considerations, wound care, treatment of spasticity and reflex spasm, pre and postoperative bowel management, pulmonary consideration, anesthetic consideration, antimicrobial regimen. The majority of MDRPUs were related to poor positioning or fixation of respiratory equipment. Occurrence of these ulcers could be prevented with implementation of preventive strategies such as regular assessment of the area underneath and around medical devices and regular repositioning or securement of devices (45). Using protective dressings to secure and stabilize devices also could reduce the risk for MDRPU development.
A Rare Case of Ventricular Rupture and Aortic Endocarditis Due to SARS-COV-2 Treated By 2 Step Cardiac Surgery
Introduction
Although SARS-CoV-2 infection primarily targets the respiratory system [1,2], cardiac complication is the most common comorbidity. Several studies from China reported acute cardiac injury in 7.2% to 27.8% among hospitalized patients [3-5]. Some of the cardiovascular complications of COVI- 19 include STelevation myocardial infarction [6], myocarditis [7], cardiogenic shock, arrhythmias, pericardial effusions, cardiac tamponade [8] and infective endocarditis [9]. We report the case of a patient who developed COVID-19 endocarditis and myocarditis with the development of tenacious mediastinal-epicardial adhesions responsible for injury to the right ventricle treated with pericardial patch in two steps.
Case Presentation
Informed consent was obtained by the patient. Consent from the institutional review board was waived, being a clinical case. A 46-year-old male was referred to our hospital with progressive shortening of breath of recent onset. Transthoracic echocardiography revealed bicuspid aortic valve with moderate insufficiency and ascending aortic aneurysm with a maximum diameter of 55mm. No coronary artery disease was found at the angiogram. The patient underwent replacement of the ascending aortic with aortic valve repair (subcommisural annuloplasty). The postoperative course was uneventful and the patient was discharged home. Transthoracic echocardiography showed ejection fraction of 55% and mild aortic valvular insufficiency. After a day the patient performed COVID-19 molecular swab test resulted positive with mild symptoms: fever (37.5°C), mild dyspnea, changes in taste. Two months later the patient was readmitted because of progressive dyspnea (NYHA class III). Transthoracic echocardiogram showed severe aortic valve insufficiency. Transesophageal echocardiogram confirmed severe aortic valve insufficiency with prolapse of the non-coronary cusp and vegetation on both cusps.
Figure 1: Right Ventricular reconstruction without cross clamp, in cardiopulmonary bypass.
Figure 2: Results of right ventricular repair at the time of delay surgical treatment of aortic valve replacement after 10 days.
The patient was referred for redo surgery of aortic valve replacement with mechanical prosthesis. At reoperation, the approach was through median sternotomy after cardiopulmonary bypass instituted by cannulation of the right femoral artery and vein. The surgery was complicated in the first phase by laceration of the right ventricle due to very tenacious mediastinal-epicardial adhesions from pericarditis caused by COVID-19. The patient underwent repair of the right ventricle with bovine pericardium patch (Figures 1 & 2). After discussion in heart team (cardiac surgeon, cardiologist and cardioanesthesiologist) it was decided to postpone the aortic valve replacement. The patient was transferred to intensive care. Ten days later the patient underwent aortic valve replacement with mechanical prosthesis (Sorin Bicarbon 25mm). The postoperative course was uneventful and the patient was discharged home in NYHA class I. Transthoracic echocardiography showed ejection fraction of 45%. After one year the patient was in NYHA class I with aortic prosthesis in place without periprosthetic leaks and vegetations.
Conclusion
This is a rare case reported in the literature of endocarditis and myocarditis caused by COVID-19 characterized by very tenacious mediastinal-epicardial adhesions. More attention is needed during the reopening of patients with previous COVID-19 because, despite the start of CEC and the empting of the right cardiac section, the risk of injury of the right ventricle is very high. When it happens, we suggest to proceed in two steps. In the first step is useful only to repair the right ventricle and in the second step, after 10 days, to proceed with aortic valve replacement/repair. This is important to avoid clamping the aorta which can cause ischemia of the repaired tissue, long CEC times with additional risk for the patient. In conclusion the message to take home is not to underestimate the tenacious adhesions from CVID-19 related myocarditis and, in case of laceration of the right ventricle, proceed in two steps to allow the stabilization of the patient in intensive care.
This is a rare case reported in the literature of endocarditis and myocarditis caused by COVID-19 characterized by very tenacious mediastinal-epicardial adhesions. More attention is needed during the reopening of patients with previous COVID-19 because, despite the start of CEC and the empting of the right cardiac section, the risk of injury of the right ventricle is very high. When it happens, we suggest to proceed in two steps. In the first step is useful only to repair the right ventricle and in the second step, after 10 days, to proceed with aortic valve replacement/repair. This is important to avoid clamping the aorta which can cause ischemia of the repaired tissue, long CEC times with additional risk for the patient. In conclusion the message to take home is not to underestimate the tenacious adhesions from CVID-19 related myocarditis and, in case of laceration of the right ventricle, proceed in two steps to allow the stabilization of the patient in intensive care.
Genetic Testing and Counselling for Cancer: Evolution, Future and Psychological Impact
Background
The field of cancer screening and testing has come a long way; its evolution from basic biochemical tests screening for particular analytes [1] to the use of gene-based testing and screening models is a definitive example of the evolution of our understanding of cancer syndromes and their underlying genetic basis. Identification of people with cancer predisposition syndromes and germ line pathogenic variants [2] has become easier with the advent and utilization of genome-wide gene sequencing panels [3,4] chromosomal arrays, and whole exome/genome sequencing and, somatic tumor testing (especially for childhood cancers), emphasizing the increasing necessity for both cancer predisposition testing and genetic counselling programs specializing in the testing, management and care of cancer [5]. Genetic counsellors are uniquely qualified to address cancer risk, interpretation of genetic results, and the inevitable complications of the subsequent ethical [6], legal and psychosocial issues that are encountered by individuals dealing with this malady [7,8]. Obtaining informed consent [5,6] from both minors and adults, ascertaining the timing for a genetics referral, providing periodic counselling and the associated aid overtime (especially in the smooth transition of younger patients to adult/ geriatric care) [8,9] and the dearth of childhood cancer predisposition syndromes are some of the unique challenges that plague us today [10]. Incidental findings due to the prevalence of genetic testing are associated with their own set of psychological implications [11]. In countries like India, where there is enormous disparity between socio-economic classes, a genetic counsellor will encounter additional problems including the lack of awareness and education amongst the under-privileged classes, genderand religion-associated disparity in terms of cancer treatment, management and the reality of the influence of political agendas over government health policies.
Entry to Genetic Counselling
Referral to a genetic counselling clinic for cancer evaluation can occur due to the prevalence of cancer syndromes within the family (family history) [12], ethnicity [13,14], phenotypic expressions, high-risk tumour types, non-oncological findings, like the lippigmentation and greater the characteristic macules associated with Peutz-Jeghers syndrome and neurofibromatosis type1 (and bi-allelic mismatch repair) respectively and incidental findings (variances in predisposition genes on chromosomal microarrays and secondary findings detected by exome sequencing) [9]. Family history alone, however, is not a reliable factor when accounting for the necessity of a referral as cancer predisposition has been reported in many cases of absence of said history [10], This can be due to the formation de novo variants, parental germ line mosaicism [15], increasing incidence of smaller nuclear families, low penetrance and recessive inheritance masking an inherited syndrome. Hence, a combination of the aforementioned factors should be taken into account when making a genetics’ referral. Moreover, the future holds the possibility population based genetic testing for cancer predisposition syndromes. Oncologists are confronted with the possibilities of identifying whether reported variants are indicative of somatic changes or inherent germ line susceptibility [16] and thus subsequent referral to a genetics’ clinic for their particular expertise becomes necessary.
Timing of Genetic Counselling Initiation
The optimal timing of the first genetic counselling session is at the time of tumor diagnosis or after the initiation of treatment in cases of poor prognosis, to ensure that the possibility of prophylactic surgery is considered. The genetic counsellor is qualified to advise the patient on many issues associated with the patient prognosis, associated treatment plans and psychological developments [17,18]. In the case of poor prognosis, DNA banking should be administered, and genetic testing organized in a timely manner in order to assess and counsel their relatives to minimize the economic and psychological burden of post-mortem testing.
Pre-Test Genetic Counselling
Informed consent should be obtained from the patient before they undergo any genetic testing procedure. This involves complete discussion of all aspects related to the test and consequent implications, including information regarding tests most suitable to the patient (based on the various factors that have prompted the referral), the surveillance protocol that may follow (especially in cases of transition from childhood to adulthood), psychosocial [11], ethical and privacy concerns, which all vary in accordance with the laws of different countries, and plans for disclosing results to at-risk relatives [6,19]. Adults are required to provide verbal and written assent towards the procedure; minors should be guided through these discussions in an age-appropriate manner and adolescents should provide verbal and written consent in conjunction with their parents or primary guardians [9]. This allows older children to become involved with and more accustomed to their unique situation and have any fears or misconceptions addressed. The basic tenet of genetic counselling is to give patients the tools required for them to make informed autonomous decisions [20] regarding the testing and management options available to them based on factual (stratified) risk information [21-25]. Despite concerns of exacerbating patients’ anxiety, genetic testing in the absence of prior genetic counselling is linked with negative outcomes including the violation of ethical standards, ordering of unnecessary, perhaps costly, genetic tests, misinterpretation of these results and adverse effects on the patients’ psyche.
Genetic Testing
The invention of Next Generation Sequencing (NGS) technology is the biggest advancement in genetic testing seen in recent years wherein analysis is performed at a multiple gene level, or even whole transcriptomic, genomic and exomic levels, at a relatively lower cost, especially when the increased sensitivity and efficiency of obtaining results are taken into account [16]. A test should be ordered after consultation with a genetic counsellor and the choice of laboratory should be based on the type of test, its level of analysis, methodology and their variant interpretation techniques, expenses involved, time factors and their policies on privacy and ethics. The variants are reported in accordance with the five-tier classification proposed by The American College of Medical Genetics and Genomics (ACMG), namely, pathogenic, likely pathogenic, variant of uncertain significance, likely benign and benign [9,26]. Despite the succinctness of this model, further interpretation by an expert is important especially when deciding the significance/ level of pathogenicity of variants (Table 1).
Table 1: Genetic tests for cancer gene mutation.
Note: {WES – Whole Exome Sequencing; WGS – Whole Genome Sequencing, NGS – Next Generation Sequencing, SNP – Single Nucleotide Polymorphism}
The sensitivity of these tests for identification of pathogenicity varies from greater than 95% to less than 50% and thus, a genetic counsellor must provide counsel on risk perception and management options based on empirical data and in conjunction with the oncologist. Identification of variants without certain significance tailors the advised management options to include surveillance protocols and the possibility of family variant tracking. Relatives can be tested for these only when consent is provided by the patient [6]. The inheritance patterns associated with the identified pathogenic variant determine the relatives who are atrisk. For example, if a syndrome follows an autosomal dominant pattern of inheritance, there is a 50% risk of inheriting a pathogenic variant, and its associated risks, to first-degree relatives of the proband [16,27].
Post- Test Genetic Counselling
For those individuals with a positive diagnosis, post-test counselling involves specific treatment/ management options and the necessity of periodic evaluation. In cases of childhood diagnosis of a hereditary cancer syndrome, reproductive and psychological implications especially, change over increasing age. Hence, lifelong risk management, and understanding of the options for reproductive (post- and pre-natal) counselling [28], testing post-birth, adoption, and/or utilizing donors is disseminated with increasing age of the patient in an appropriate manner suited to the child’s developmental stage8,9. Surveillance options [29] and information regarding the advent of new testing options can only be provided for at-risk individuals/ families if periodic follow-up with the genetic counsellor is maintained.
Psychological and Sociological Implications
Negative effects on the psyche of a patient with a positive diagnosis are primarily concerned with surveillance protocols and the reality of a life-long economic burden8. Invasive medical procedures [30], procedures requiring sedation or general anesthesia, false positive results, incidental findings are implicated by various studies in causing psychological distress to the patient and their families. There arises a general frustration with lack of positive results when it comes to therapies advised, inconclusive outcomes of tests and the delivery of false-positive results (increased in whole-body MRIs) [31], impaired quality of life, reduced satisfaction with care, and worse overall survival. Patients undergoing surveillance may experience anxiety with regards to scanning, referred to as “scanxiety”, and children especially may feel adversely towards repeated blood draws and the claustrophobic confinement experienced during MRI scans [9]. Young adults face an ever-increasing economic burden as they are as of yet not financially secure enough, and may not even possess insurance cover [20], to support life- long management programs. On the contrary, proactive surveillance and psychological support, from say, cancer survivor groups, may empower the patient and are viable avenues to lead a more well-adjusted life. The patient relies on the care team in such scenarios due to generation of trust and confidence in their counsel [32,33]. Cancer genetic counselling in India. In India, there are about a million cases of cancer diagnosed yearly. When the population of the subcontinent is taken into account, these rates of incidence and mortality, match those seen in high-income countries [34]. These elucidate the lack of early-detection strategies and positive results of treatments within the medical landscape of the country [35]. Studies show that breast, lung, oral, cervical, gastric and colorectal cancers [36] have the highest incidence rates in India. It is evident that most causative agents implicated in cancer in the Indian population are avoidable (tobacco and alcohol consumption, lack of education with respect to female hygiene) [34,37]. There is a general lack of education and support for the low-income, socially underprivileged families owing to the fallacies of an increasingly capitalist state of government [38-40]. Even governmental policies regarding general health are found to be inadequate in the face of growing mortality due to cancer. It is the second-leading cause of death amongst the Indian population. A patriarchal society has also generated the spread of female reproductive cancers as the importance of feminine hygiene is not acknowledged by many; additionally, a greater economic burden to finance health care is placed on women [41]. In conjunction with the lack of resources and such a mind-set, most evidently seen in under-privileged communities, the incidence of cervical cancers has witnessed an increase over the past 5-10 years. In India, the age of onset of the female reproductive cancers is around a decade earlier than that of developed nations (45-50 years in the former, compared to >60 years of the latter) [42]. Moreover, oncofertility can be improved by developing management, treatment strategies that comprise of professionals from multiple specialties, say a counselling team that includes a reproductive endocrinologist [43] apart from an oncologist, psychologist and the geneticist. Hence, advancement of cancer-associated clinical programs with respect to diagnosis, screening, management/ treatment particular to the Indian race [44] are a necessity in the mission to better the state of women’s health in India [42,45].
Conclusion
Cancer testing and management is an ever-growing field primarily due to our increasing understanding of unknown syndromes and their underlying genetics, and the expansion of available information of known cancer syndromes. In accordance with these basic developments, there should be a correlating evolution in the various genetic testing and counselling practices available for the same. These take the form of improved access to aforementioned resources and formulations of government policies that tackle health care from this perspective [45]. One such advancement can be the necessitation of population-based genetic screening [46,47] and testing for common pathogenic variants of the most abundantly found cancer syndromes, e.g. BRCA 1 and 2 testing for breast cancer [4,42,48]. This type of policy can hold many implications in reducing the burden of cancer in many developing economies, like India. In the same vein, there have been discussions on the use of e-health interventions [49] like psychoeducational interventions delivered via web-based environments with auxiliary methods of communication, which includes support with professionals and peers, offer improved awareness and access to the required support for informed, autonomous decisionmaking. Personalized medicine is an avenue of modern medicine gaining quick popularity as it is tailored to an individual and their needs. Corroborating advancements in cancer genetic testing and counselling to personalized care will initiate the incidence of more positive outcomes as it pertains to lifelong care and management practices [5,11,18,50,51].
Extractive Values and Antioxidant Properties of Leaves, Seeds, Pods and Coats Moringa Plant
Introduction
Antioxidants are molecules that fight free radicals in human body [1]. Antioxidants cause protective effect by neutralizing free radicals which are toxic byproducts of natural cell metabolism. Research is increasingly showing that antioxidant rich foods and herbs have health benefits. Medicinal herbs are the richest sources of antioxidants compounds [2]. Antioxidants are biomolecules which tackle and destroy free radicals and scavenge diseases [3]. Sagar, et al. and Shao, et al. reported that green plants are chief sources of natural antioxidants, and they are capable of tackling free radicals [3-5]. Moringa oleifera belongs to the single genus family Moringaceae and it is most studied of the thirteen species of Moringa trees [6,7]. It is a deciduous tree that grows up to 12 m tall with an umbrella-shaped crown and grows extremely fast which can reach up to 4 m in its first year. Its leaves are alternate bi or tri-pinnate, 20-70 cm long. Leaflets are usually oval, rounded at the tip, and 1-2cm long and they are dark green in colour with almost whitish in the lower surface [8,9]. Fahey, 2005 reported that the leaves of Moringa oleifera are the most nutritious part of the plant, being a significant source of vitamin B6, vitamin C, pro-vitamin A as beta- carotene, flavonoids, 46 antioxidants, magnesium and protein among other nutrients. The plant is called “Zogale” in Hausa, “ Ewe Igbale” in Yoruba, “Ikwe Oyibo” in Ibo and “Egelengedi” in Idoma while its English name is Bean oil tree or drumstick tree or miracle tree or “Mother’s Best Friend” [6,10,11]. Though a lot of research works have been done on moringa plant [10,12-16]. but there is little, or no work done on the effect of solvents in extracting phytochemicals from the seeds, coats, pods and leaves of the plant. Therefore, the focus of this research work is to evaluate the potency of solvents in extracting bioactive ingredients from seeds, coats, pods and leaves of moringa plant as well as to investigate and compare the antioxidant properties of the first two highest yield solvent-extracts with that of the raw sample with a view of establishing which of the moringa plant parts (seeds, leaves, pods and coats) is richest in phytochemical constituents and antioxidant properties.
Materials and Methods
Source of Materials
The seeds, coats, pods and leaves of Moringa oleifera were collected from a compound of a building at Ajagbale Street, Oka, Ondo City, Ondo State, Nigeria. All chemicals used were of the analytical grade with the highest purity available (<99.5%) and procured from Sigma Aldrich, USA.
Preparation and Extraction of Seeds, Coats, Pods and Leaves of Moringa Plant
The different parts of moringa plant were cut into smaller pieces for easy air-drying. The dried samples were ground separately using electric blending machine (Solitarire Mixer Grinder VTCL Heavy Duty 750 Watts) and each part was sieved with 40 mm mesh size. The powdered samples were divided into portions, packed in air tight containers labelled appropriately prior to extraction. Each sample was extracted separately with each solvent (acetone, chloroform, ethyl acetate, ethanol, methanol and water) at ratio 1:10 for 72 h during which it was intermittently shaken on a shaking orbit machine The resulting mixture was filtered through a 0.45 μm nylon membrane filter. The extracts were desolventised to dryness under reduced pressure at 40 oC by a rotary evaporator (BUCHI Rotavapor, Model R-124, Germany). Weight of extract obtained was used to calculate the percentage yield of extract in each solvent and the dry extracts were stored in a refrigerator (4 0C) prior to analysis [17-19].
Determination of Antioxidant Property
Total Flavonoid
0.1g of extract was weighed into a sample bottle; 10 mL of 80% methanol was added and allowed to soak for 2 hours. 0.4 mL of the solution was measured into a 10 mL volumetric flask, 1.2 mL of 10% sodium hydroxide, 1.2 mL of 0.2 M concentrated sulphuric acid and 3 mL of 3 M sodium nitrate were added. 4.2 mL of distilled water was used to make it up. The absorbance was read using 6850 UV spectrophotometer at wavelength 325 nm [20].
Ferric Reducing Antioxidant Power (FRAP)
0.1g of extract was weighed into a sample bottle; 10 mL of 80% ethanol was added. 2.5 mL sodium phosphate buffer (0.2 M Na2PO3, pH 6.6) and 2.5 mL of 1% potassium ferricyanide were added and incubated at 50˚C for 20 minutes. 2.5 mL of TCA (trichloroacetic acid) was added to stop the reaction. 2.5 mL of the aliquot was taken and diluted with 2.5 mL distilled water and 0.5 mL of 0.1 % ferric chloride was added and allowed to stand for 30 minutes in the dark for color development. The absorbance was read using 6850 UV/Visible spectrophotometer at wavelength 700 nm [21].
DF: Dilution factor. If not diluted, then DF = 1
Total Phenol
0.1g of extract was weighed into a sample bottle; 10 mL of distilled water was added to dissolve. 1 mL of the solution was pipetted into a test tube and 0.5 mL of 2 N Folin-Ciocalteu reagent and 1.5 mL of 20 % sodium carbonate solution was added. The solution was allowed to stand for 2 hours and the absorbance was read using a 6850 UV/Visible spectrophotometer at wavelength 765 nm. Garlic acid solution was used as standard viz 0.5 mg, 1 mg, 2 mg, 4 mg, 6 mg, 8 mg and 10 mg [22].
DF: Dilution factor. If not diluted, then DF = 1
DPPH (2, 2-Diphenyl-1-Picrylhydrazyl) Scavenging
0.1g of extract was weighed into a sample bottle and 10 mL of ethanol was added, stirred for 15 minutes and allowed to stand for 2 hours. 1.5 mL of the extract was pipetted into a test tube and 1.5 mL of DPPH solution was added. The 6850 UV/Visible spectrophotometer was zeroed with ethanol as the blank solution. The absorbance/ optical density of the control (DPPH solution) was read. The absorbance of the test sample was read at 517 nm. [23].
DF: Dilution factor. If not diluted, then DF = 1
Iron (Fe2+) Chelation Assay
0.1g of extract was weighed into a sample bottle, 150 μL of 500 μM FeSO4 was added. 168 μL of 0.1M Tris-HCl (pH 7.4) and 218 μL of saline solution was added. 100 μL of the solution was taken and incubated for 5 minutes, before addition of 13 μL of 0.25% 1, 10-phenanthroline. The absorbance was read using 6850 UV/ Visible spectrophotometer at wavelength 510 nm [24].
Statistical Analysis
Statistical significance tests were performed using SPSS (v. 20, IBM SPSS Statistics, US) at p < 0.05 by means of one-way analysis of variance (ANOVA) followed by LSD post hoc multiple comparison and the experimental results were expressed as mean ± standard mean deviation of three replicates.
Results and Discussion
Extractive Values of Solvent Extracts of Leaves, Seeds Pods and Coats of Moringa Plant
The extractive values (% yield) of leaves, seeds, pods and coat moringa plant using acetone, chloroform, ethanol, ethyl acetate, methanol and water are contained in Table 1. The result showed that the percentage yield of moringa leaf extract was 11.095±0.805 in ethyl acetate, 9.291±2.234 in ethanol, 8.497±0.713 in water, 8.108±2.219 in methanol, 7.039±2.084 in acetone and 3.055 ± 1.735 in chloroform. The percentage yield of moringa pod extract was 2.146±0.003 in methanol, 1.347±0.001 in ethanol, 1.047±0.000 in ethyl acetate, 0.898±0.002 in chloroform, 0.850±0.000 in acetone and 0.199±0.002 in water. The percentage yield of moringa coat extract was 8.709±0.414 in acetone, 3.333±0.108 in ethanol, 3.160±2.731 in methanol, 3.062±0.534 in ethyl acetate, 2.149±1.799 in water and 1.451±0.502 in chloroform. The percentage yield of moringa seed extract was 30.151±1.221 in acetone, 29.997±1.558 in ethyl acetate, 27.725±2.714 in ethanol, 26.190±3.452 in methanol, 23.942±2.955 in chloroform and 21.417±10.455 in water. In each of the solvent used, there was a significant difference at p<0.05 in the extractive values of the seeds, leaves, pods and coats of moringa plant. In all the solvents used for extraction, it was observed that the extractive value (%) was highest in moringa seed and least in moringa pod. All the solvents used had the first two highest extractive values in moringa seeds and leaves except acetone that had its first two highest extractive values in moringa seeds and coats. According to Alachaher, et al. 2018 [21], there are quite number of factors in which extraction of bioactive compounds depends. The selection of solvent system largely depends on the specific nature of the bioactive compounds being targeted. Also, different solvent systems are available to extract the bioactive compounds from natural products. Extraction efficiency is affected by the chemical nature of phytochemicals, the extraction method used, sample particle size, the solvent used, as well as the presence of interfering substances. Under the same extraction time and temperature, solvent and composition of sample are known as the most important parameters [21].
Table 1: Extractive value of solvent extracts of moringa plant.
Note: * = Result values are expressed as mean value of triplicate determinations ± standard mean deviation
Different letter in the same row showed significant difference (p<0.05).
Antioxidant Properties of Solvent Extracts of Leaves, Seeds, Pods and Coats of Moringa Plant
Antioxidant properties were carried out on the plant raw sample and the first two solvent extracts with the highest extractive values. The antioxidant properties of raw sample, ethanol and ethyl acetate extracts of leaves; acetone and ethyl acetate extracts of seeds; methanol and ethanol extracts of pods as well as acetone and ethanol extracts of coats of moringa plant were examined and these are presented in Table 2 to Table 5. The antioxidant properties of raw sample, ethanol and ethyl acetate extracts of moringa leaves is depicted in Table 2. The concentration (mg/100g) of total flavonoid in moringa leaves ranged between 0.122±0.001 – 0.332±0.001 with ethanol extract had the highest concentration of 0.332±0.001 mg/100g, followed by ethyl acetate extract with concentration of 0.268±0.002 mg/100g while the powdered raw sample has the least concentration of 0.122±0.001 mg/100g. The total phenol concentration (mg/100g) in moringa leaves ranged between 0.181±0.002 – 0.349±0.003 with ethanol extract having the highest concentration of 0.349±0.003 mg/100g, followed by ethyl acetate extract with concentration of 0.251±0.001 mg/100g while the powdered raw sample had the least concentration of 0.181±0.002 mg/100g.
Table 2: Antioxidant properties of moringa leaves.
Note: * = Values are expressed as mean value of triplicate determinations ± standard mean deviation; GAE =Garlic Acid Equivalent Different letter in the same row showed significant difference (p<0.05).
Table 3: Antioxidant properties of moringa seeds.
Note: * = Values are expressed as mean value of triplicate determinations ± standard mean deviation; GAE =Garlic Acid Equivalent
Different letter in the same row showed significant difference (p<0.05).
Table 4: Antioxidant properties of moringa pods.
Note: * = Values are expressed as mean value of triplicate determinations ± standard mean deviation;GAE =Garlic Acid Equivalent
Different letter in the same row showed significant difference (p<0.05).
Table 5: Antioxidant properties of moringa pods.
Note: * = Values are expressed as mean value of triplicate determinations ± standard mean deviation; GAE =Garlic Acid Equivalent
Different letter in the same row showed significant difference (p<0.05)
The percentage DPPH (2,2-diphenyl-1-picrylhydrazyl) scavenging activity of powdered raw sample showed the highest value of 89.25±0.21% followed by ethanol extract of 63.10±0.30% while ethyl acetate extract had the lowest value of 57.45±0.16%. The ethyl acetate extract of moringa leaves exhibited the highest reducing power of concentration of 0.87±0.02 GAE followed by ethanol extract which had concentration of 0.47±0.00 GAE while the powdered sample had the least concentration of 0.32±0.01GAE. There were significant differences at p < 0.05 in the total flavonoid, total phenol, DPPH, iron chelation assay and ferric reducing antioxidant power of raw sample, ethanol extract and ethyl acetate extract of moringa leaves. The antioxidant properties of raw sample, acetone and ethyl acetate extracts of moringa seeds is displayed in Table 3. The total flavonoid concentration (mg/100g) of moringa seeds ranged from 0.363±0.002 – 0.392±0.000 in which the powdered sample had the highest concentration of 0.39±0.000 mg/100g, followed by ethyl acetate extract with concentration of 0.379±0.001 mg/100g while the acetone extract has the least concentration of 0.363±0.002 mg/100g.
There was no significant difference (p < 0.05) in the total flavonoid content of raw sample, acetone extract and ethyl acetate extract of moringa seeds. In moringa seeds, the total phenol concentration (mg/100g) was between 0.059±0.001 – 0.349±0.00. The ethanol extract had the highest concentration while the powdered raw sample had the lowest concentration of total phenol. The ethyl acetate extract of moringa seeds had total phenol concentration of 0.251±0.001 mg/100g. There was significant difference (p < 0.05) in the total phenol concentration of raw sample, acetone extract and ethyl acetate extract of moringa seeds. The DPPH (2,2-diphenyl-1-picrylhydrazyl) radical scavenging activity of powdered raw sample of moringa seeds had the highest activity of 79.81±0.11% followed by ethyl acetate extract with DPPH activity of 77.43±0.16% while acetone extract showed the lowest activity of 71.86±0.30%. There was significant difference (p < 0.05) in the DPPH (2, 2-diphenyl-1-picrylhydrazyl) radical scavenging activity of raw sample, acetone extract and ethyl acetate extract of moringa seeds. The iron chelation activity (%) ranged between 22.36±0.11 – 39.72±0.09 with the lowest and highest concentration in raw sample and acetone extract respectively while the ethyl acetate had iron chelation activity of 38.12a±0.07%. There was no significant difference (p < 0.05) in iron chelating activity of acetone extract and ethyl acetate extract of moringa seeds. The ethyl acetate extract of moringa seeds exhibited the highest ferric reducing antioxidant power of concentration of 0.55±0.00 GAE followed by acetone extract which had concentration of 0.54±0.01 GAE while the powdered sample had the least concentration of 0.29 ±0.01 GAE. There was no significant difference (p < 0.05) in ferric reducing antioxidant power (FRAP) of acetone extract and ethyl acetate extract of moringa seeds. The antioxidant properties of raw sample, methanol and ethanol extracts of moringa pods is shown in Table 4. The concentration (mg/100g) of total flavonoid of moringa pods ranged between 0.038±0.000 – 0.082±0.002 with methanol extract having the highest concentration and the powdered sample having the least concentration while the total flavonoid concentration of ethanol extract of moringa pod was 0.059±0.001 mg/100g. There was significant difference (p < 0.05) in total flavonoid concentration of raw sample, methanol extract and ethanol extract of moringa pods. The total phenol concentration (mg/100g) of moringa pods was between 0.031±0.000 – 0.131±0.001.
The highest and lowest total phenol concentration were found in ethanol extract and raw sample of moringa pods respectively while methanol extract had total phenol concentration of 0.059±0.000 mg/100g. There was significant difference (p < 0.05) in total phenol concentration of raw sample, methanol extract and ethanol extract of moringa pods. For DPPH (2,2-diphenyl-1-picrylhydrazyl) scavenging activity of moringa pods, it was observed that methanol extract showed the highest value of 96.82±0.20% followed by powdered raw sample which had 83.75±0.11% while ethanol extract showed the lowest value of 81.95±0.10%. There was no significant difference (p < 0.05) in DPPH scavenging activity of raw sample and ethanol extract of moringa pods. The iron chelating activity (%) of moringa pods ranged from 28.14±0.01 – 36.73±0.03 with the lowest and highest concentration in methanol extract and raw sample accordingly and that of ethanol extract was 32.14±0.02%. There was significant difference (p < 0.05) in iron chelating activity of raw sample, methanol extract and ethanol extract of moringa pods. The ferric reducing antioxidant power (FRAP) of methanol extract of moringa pods exhibited the highest reducing power of 0.53±0.03 GAE, followed by ethanol extract of 0.42±0.01 GAE while the powdered raw sample had least concentration of 0.25±0.00 GAE. There was significant difference (p < 0.05) in ferric reducing antioxidant power of raw sample, methanol extract and ethanol extract of moringa pods. The antioxidant properties of raw sample, acetone extract and ethanol extract of moringa coat is presented in Table 5. The total flavonoid concentration (mg/100g) of moringa coats ranged from 0.049±0.000 – 0.317±0.002 with acetone extract had the highest concentration and the powdered raw sample had the least concentration while ethanol extract had total flavonoid of 0.258±0.001 mg/100g. The concentration (mg/100g) of total phenol of moringa coat was between 0.031±0.000 – 0.118±0.002. The acetone extract and ethanol extract had the lowest and highest concentration while the raw sample of moringa coat had total phenol concentration of 0.063±0.001mg/100g.
The DPPH of ethanol extract moringa coat showed highest activity of 95.20±0.12 % followed by powdered sample which had activity of 85.07±0.09% while acetone extract showed the lowest activity of 72.13±0.10%. The iron chelating activity (%) of moringa coats was between 11.18±0.00 – 44.91±0.04. Ethanol extract had the highest iron chelating activity while acetone extract had the lowest and that of raw sample was 30.34±0.02 %. The ferric reducing antioxidant power of acetone extract of moringa coats exhibited the highest reducing power of 0.85±0.05 GAE followed by ethanol extract of 0.64±0.03 GAE while the powdered raw sample has the least concentration of 0.32±0.01 GAE. There were significant differences (p < 0.05) in all the antioxidant properties considered for raw sample, acetone extract and ethanol extract of moringa coats [25-28].
Conclusion
The moringa seeds are richest in bioactive ingredients and this is followed by moringa leaves while the least bioactive ingredients are found in moringa pods. The solvent extraction efficiency of bioactive ingredients in moringa plant decreases in the order of acetone, ethyl acetate, ethanol, methanol, water and the least is chloroform. The utilization of acetone, ethyl acetate, ethanol and methanol in extracting bioactive ingredients of high antioxidant activities from the seeds and leaves of moringa plant is economical and effective. Further scientific investigation can be conducted using acetone, ethyl acetate, ethanol and methanol extracts of seeds and leaves of moringa plant as antioxidants or preservative in edible oils and their antioxidative potentials can be compared with synthetic antioxidants such as butylated hydroxyl anisole (BHA), butylated hydroxyl toluene (BHT) etc. in edible oils.
Epidemiological and Cytological Aspects of Cervical Dystrophies in Senegal Using Cervico-Uterine Smears
Introduction
The cervico-uterine smear or cervical smear is a collection of cells from the cervix in order to detect at an early stage any cellular abnormality that may suggest the presence of precancerous or cancerous lesions of the cervix as well as lesions of dystrophy [1]. Dystrophy is an abnormality of cell growth, which is distinct from the metaplastic phenomenon and dysplasia. It consists of mild and limited morphological abnormalities, thought to be of inflammatory or hormonal origin. These abnormalities must be considered according to the context in which they are observed (ectopy metaplasia, atrophy, treatment, irrigative states, and infections) [2].
Methods
It was a retrospective study from August 1, 2014 to June 1, 2016 carried out at the Aristide LE DANTEC hospital in the laboratory of clinical cytology and reproductive biology. The technique used to detect dystrophy lesions was the cervico-vaginal smear
Patients
The study involved 2391 cases of significant cervico-uterine smears in women from various health facilities in the country and sometimes in the sub region. Women in their menstrual period and women in advanced pregnancy were excluded.
Cervico-uterine Sampling
The cervico uterine sampling made in the laboratory of clinical cytology and reproductive biology at Aristide LE DANTEC hospital of Dakar was carried out according to the following procedure: registration of the patient on arrival, the patient was registered in a register with an identifying number, second name, first name, age, and origin and billing number. After this step, a receipt with the registration number was given to the patient to be presented on the day the results are to be retrieved; and interrogation was carried out based on the survey form.
Papanicolaou Coloration
The slides are then dried and stained using the Papanicolaou method.
Interpretation
Satisfactory smears are smears with an abundant epithelial cell population (covering 20% of the slide) of intact morphology, corresponding to squamous (ectocervix), glandular (end cervix) or metaplastic cells without inflammatory reaction or excessive bleeding. These are smears that cannot be reliably analyzed for the following reasons: paucicellar swabs; dense inflammatory or hemorrhagic lesions masking the epithelial elements.
Ethical Consideration
The study protocol was approved by the Ethics Committee of the faculty of medicine, pharmacy and odontology in Cheikh Anta Diop University, Dakar, Senegal. A written informed consent was taken from all participants.
Statistical Analysis
The data was stored and analyzed on the Excel software.
Results
Age
The mean age of the patients was 47.72 years with a standard deviation of 11.37 years. The most represented age (mode) was 40 years (Figure 1).
Figure 1.
Reason of Sending
Routine check-ups with no apparent clinical manifestations represented 43.16% of patients. The other requests were due to various clinical manifestations: metrorrhagia, primary or secondary amenorrhea, pelvic pain, and dysmenorrhea.
Types of Dystrophies
Multiple dystrophic lesions (60.85%) were found of infectious (mild, moderate and intense) and hormonal type. Infectious dystrophies accounted for 54.37%. The infections encountered were bacterial, parasitic (chlamydial), fungal or viral (herpetic) (Table 1).
Table 1.
Discussion
Epidemiological Data
Systematic analysis of the results of our study provided us with important information on the epidemiological data of cervicouterine smears in Senegal. Indeed, after 22 months of collection, the mean age of the patients in our series was 47.72 years with extremes between 15 and 88 years. In Ethiopia, Mesele and his team found the same average age in 2010 (47.7 years), after 6 months of study [3]. This age generally corresponds to the period of genital activity in most women. Epidemiological studies have shown a strong correlation between sexual age and certain HPV infections [4] and patients were sometimes referred by various public (more than 65%) and private health facilities. This can be explained by the rather accessible cost of this examination in our center (less than 10 euros) compared to private structures that perform this same examination. Our countries have very little universal health coverage, unlike several countries in the North where adherence to screening is higher but limited in some areas by disparities [5]. Our patients lived mostly on the outskirts of Dakar, 53.47%. The departments of Pikine and Guédiawaye are home to more than 50% of Dakar’s population [6]. We therefore believe that increasing the number of public screening facilities in the Dakar suburbs would surely increase adherence to systematic screening. Asymptomatic subjects referred for routine screening represented 43,.17%. These results are in contrast to those obtained by Diallo and his team, who showed 20 years ago that in the absence of functional urogenital signs, women rarely consulted Senegalese health facilities for early detection of cervical lesions [7]. In France, the high health authority recommends systematic screening for precancerous and cancerous cervical lesions by cervico-uterine smears every three years in women aged 25 to 65 [8]. We note that education, information and communication about cervico uterine diseases are fundamental in their prevention.
The Dystrophic Smears
Dystrophic smears with an inflammatory background were founded in 60.73% of patients, 54.37% of which were infectious. Infections are of several types (viral, bacterial, parasitic and mycotic), sometimes intertwined. Cervicitis and cervico-vaginitis are very frequent in developing countries and are characterized by desquamation and ulceration of the surface epithelium with infiltration of neutrophils [9]. A study conducted in the same department found a rate of dystrophy almost similar: 61.33%. The frequency of infections in our countries is explained by several factors including polygamy, poverty and ignorance.
Conclusion
Cervical dystrophy lesions are benign lesions that could, by their persistence, lead to low-grade epithelial lesions.