Acute Effects of Aerobic Physical Activities on Attention and Concentration in School-aged Children
Abstract
Purpose: It is unknown whether or not a PA intervention can produce positive effects on students’ attention and concentration late in the school day (i.e., afternoon). Thus, the purpose of this study was to examine the acute effect of 30-min PE lessons on students’ attention and concentration late in the school day.
Methods: A total of 115 fourth- and fifth-grade students participated in this study with the mean age of 9.41 years old for fourth grade students (n=58) and 10.41 years old for fifth-grade students (n=57). One fourth-grade class and one fifth-grade class were randomly assigned to the intervention group, while the other one fourth-grade class and the other fifth-grade class were randomly assigned to the comparison group. The intervention took place after all classes attended a 30-min regular late afternoon academic lesson. The intervention students took the d2 Test of Attention before and after attending a 30-min aerobic PA-focused PE lesson, while the comparison students took the d2 Test of Attention before and after attending a 30-min lecture-typed PE lesson. The d2 Test is standardized paper and pencil letter-cancellation test that measures neuropsychology performance of the students in the areas of sustained and selective attention as well as concentration.
Results: 2 (pre-test vs. post-test) x 2 (Experimental Group vs. Comparison Group) ANOVA revealed a significant effect of time, but no significant effect of group for processing speed (TN), accuracy (E%), and concentration (CP). Further, the repeated measures ANOVA indicated that there was no significant interaction between time × group in TN and E%, but there was a significant level of the time x group intervention in CP, close to p< .05.
Conclusion: It was concluded that after participating in both the 30-min aerobic PA-focused PE lesson and the 30-min interactive lecturetyped PE lesson late in the school day, the students had greater improvement in attention and concentration, compared to after attending the 30-min regular academic lesson.
Keywords : Focused attention; Sustained attention; Concentration; Aerobic physical activity
Introduction
A growing body of studies has shown positive effects of physical activity (PA) on attention and concentration in school-aged children [1-9]. Attention is defined as the ability to resist distractions and concentration is referred to the ability to stay focused [5,10,11]. Attention and concentration are key to cognitive processes such as encoding, recalling, information processing, and problem solving. Therefore, attention and concentration play essential roles in successful academic performance [11-17]. However; children are sitting in the classroom for prolonged periods of academic instructions from morning to afternoon during a school day. Especially, the prolonged sedentary lifestyle reduces students’ attention to academic instructions and concentration on task engagement [11,15,18]. To address this critical issue, investigating the acute effects of PA on increasing attention and concentration in school-aged children has been of great interest in school settings. Empirical studies have examined the acute effects of a single bout of different types, durations, and intensities of PA on attention and concentration performance in school-aged children [1-10]. In a systematic review of 12 studies in acute effects of a single bout of PA on children’s attention in the laboratory and the school settings, four out of seven studies showed that aerobic PA was positively associated with attention and concentration [11]. Supporting that, a study by Tine and Butler [8] examined the acute effects of a 12- min single bout of aerobic exercises on attention and concentration in 164 students aged 10-13. The results indicated that both lowerincome and higher-income students in the intervention group showed significant higher performance in selective attention than the control group who were sitting while watching 12-min film clip [8].
Also, the other study investigated the acute effects of a 50-min aerobic exercise PE lesson with moderate-to-vigorous intensity and a 50-min coordinated ball skills PE lesson with the same intensity on 3-5 grade students’ attention and concentration performance in d2 test, compared to a 50-min regular academic lesson [1]. The results indicated that the students who took aerobic exercise PE lesson and an academic lesson showed a significant higher attention performance from pre-test to post-test than the students who took the coordinated ball skills PE lesson, which had less improvement.1 However, it was unknown when the varying types of the exertions took place across a school time [1].
Further, a study examined the acute effects of 15-min “no break”, passive break, moderate intensity PA break, and vigorous PA break on 123 fifth-grade students’ attention performance [5]. The results revealed that a passive break, moderate intensity aerobic PA, and vigorous intensity aerobic PA yielded a significant better selective attention performance than “no break”. Of the four conditions, participating in moderate intensity aerobic PA resulted in the most pronounced acute effect on attention performance. In addition, a study compared the acute effect of 10-min coordinated exercises with 10-min a regular PE lesson on adolescent students’ attention and concentration in a school setting.2 The results showed that both coordinated exercises group and regular PE group with the same moderate intensity monitored by heart rates significantly increased their attention and concentration from pre-test to posttest. However, coordinated exercises group showed a significantly higher degree of performance in d2 test compared to the regular PE group [2].
Furthermore, a study examined the immediate and 40-min delayed effects of a 20-min cognitively engaging aerobic type of physical games on 2nd-grade students’ updating, inhibition, and shifting performance [3]. The results revealed that the students in the experimental group showed a significant immediate improvement in inhibition performance compared to the control group who listened to age-appropriate story. However, no significant acute effects of the intervention on updating and shifting performance were found. The results showed no significant intervention effect on inhibition after 40 min of cognitively engaging physical activity [3]. In contrast, Schmidt et al. [6] examined 90 fifth-grade students’ attention and concentration in revised d2 test before, immediately after, and 90 min after students’ participating in 45-min coordinated, aerobic PA (experimental condition) compared to the control students who were taking a regular 45- min academic lesson. They found that the experimental students did not show significant improvement in d2 test immediately after the intervention. In contrast, after 90 min of the intervention, the experimental group showed greater improvement in attentional performance [6].
To date, a handful of studies showed empirical evidence that the single bout of aerobic PA with moderate intensity and varying durations of 10-min, 12-min, 15-min, 20-min, and 50-min yielded beneficial acute effects on attention and concentration in schoolaged children [1-11]. A meta-analysis review indicates that the students aged 11-13 showed the largest effect of the positive association between PA and cognition.19 However, most of the studies did not report when the varying durations, intensities, and types of a single bout of PA intervention took place across the school time. Due to a lack of studies examining the timing of the intervention effect on attention and concentration, it is unknown whether or not the PA intervention can produce positive effects on students’ attention and concentration late in the school day (i.e., afternoon). Given the fact that students start their school day from early morning to afternoon, students are engaging in several instructional academic lessons for roughly 6-7 hours of the school time. It was evidenced that students’ attention and concentration were lower late in the school day compared to early in the school day [18].
School teachers often claim that the last two class periods of the school day were the most challenging for them to gain students’ attention to their instructions and to motivate them stay focused on the task engagement and performance [18]. To solve this imperative issue, there is a critical need to develop feasibly implemented intervention strategies that increase students’ attention and concentration late in the school day. Physical education is a school-required curriculum for all students to take and provides all students with quality and variety of PA experiences. Therefore, physical education is used as a feasible and effective intervention strategy for generating a positive acute effect on attention and concentration in school-aged children [1-3,6].
The purpose of this study was to examine the acute effect of 30- min PE lessons on students’ attention and concentration late in the school day. This study will test two research hypotheses:
a) students will show a higher level of attention and concentration performance immediately after the 30-min PE lessons late in the school day than immediately after the 30- min regular academic lesson (before the PE lessons);
b) students in the 30-min aerobic PA-focused PE lesson will show higher positive changes in attention and concentration performance than students in the 30-min lecture-typed PE lesson from pre- to post-test late in the school day.
The significance of this study lies in using a regular school PE lesson as the intervention strategy for improving students’ attention and concentration, especially in the afternoon, the late school day. Positive findings will support the effectiveness of the PE intervention in improving students’ attention and concentration, leading to successful academic performance. The cost-effective, feasible, and scalable intervention wills benefit students in developing academic-enhanced attentional behaviors.
Methods
Study designTwo fourth-grade and two fifth-grade classes at one elementary school were recruited for this study. One fourth-grade class and one fifth-grade class were randomly assigned to the intervention group, while the other one fourth-grade class and the other one fifthgrade class were randomly assigned to the comparison group. The intervention took place after all classes attended a 30-min regular late afternoon academic lesson. The intervention students took the d2 Test of Attention before and after attending a 30-min aerobic PA-focused PE lesson, while the comparison students took the d2 Test of Attention before and after attending a 30-min lecture-typed PE lesson.
ParticipantsAll students enrolled in the two fourth-grade classes and the two fifth-grade classes were invited to participate in this study. A total of 115 fourth- and fifth-grade students participated in this study with the mean age of 9.41 years old for fourth grade students (n=58) and 10.41 years old for fifth-grade students (n=57). An approval for conducting this study was obtained from the University Institutional Review Board (IRB)-Health Sciences and Behavioral Sciences (HSBS) (HUM00122551). The signed consent forms were obtained from the parent/guardian of 115 students. Also, written assent forms were gathered from the students prior to pre- and post-testing. At the end of the study, 22 children who were absent in either session and/or did not complete the d2 Test either at pre-test or at post-test was deleted from data analysis. A final data analysis consisted of 93 students who completed the pre- and post-tests and participated in their respective intervention group (n=39) and comparison group (n=54) (Flow chart 1).Flow chart 1: Timelines for the D2-test after the academic lessons (before the PE lessons) and after the PE lessons.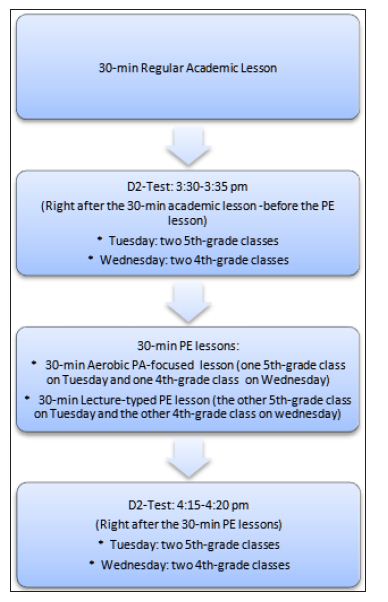
Data CollectionPre-test: Figure 1 shows the timelines for the students in the fourth- and fifth-grade classes to take pre-test (after the 30- min regular academic lessons), 30-min aerobic PA or 30-min PAbenefits lecture, and post-test. One week before the pre-test, each teacher who was trained in the protocols of the test explained the directions for taking the test to the students. The students were then asked to practice the two lines of the test according to the standardized directions for taking the test in order to ensure all students understand the testing procedures. On each of the test days in the afternoon during a school day, the participating students took the d2 Test of Attention in their respective classroom. After completing the pre-test, the students turned in their testing sheets to their PE teachers.Figure 1: Changes in TN for the two groups.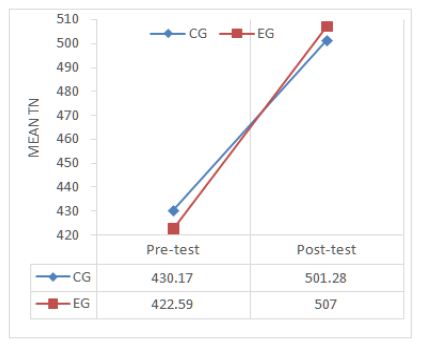 Intervention: Right after the pre-test, the intervention students started the 30-minute aerobic PA-focused PE lesson. The lesson consisted of 5-min warm-ups (jogging around the track, followed by stretching exercises), 16-min relay race running and running through obstacle courses on a regular track and field court (i.e., 400-meter lanes), and 4-min cool down stretching exercises, in addition to 5-min class organization and instructions. In contrast, the comparison students participated in the 30-min lecture on benefits of PA and appropriate methods of PA in a regular PE lesson. During the lecture, the PE teacher showed the pictures in relation to the benefits of varying exercises, asked students to conduct mock interviews with their peers about their PA participation and methods they used, and summarized the benefits of PA and appropriate methods of engaging in PA.Post-test: After finishing the lecture-typed PE lesson, the control students performed on the d2 Test while following the same testing procedures as the pre-test in their classroom. For the intervention students, right after the aerobic PA-focused PE lesson, they returned to their classroom and took the d2 Test of Attention while following the same testing procedures as the pre-test as well. The PE teachers collected the testing sheets from their students.
Intervention: Right after the pre-test, the intervention students started the 30-minute aerobic PA-focused PE lesson. The lesson consisted of 5-min warm-ups (jogging around the track, followed by stretching exercises), 16-min relay race running and running through obstacle courses on a regular track and field court (i.e., 400-meter lanes), and 4-min cool down stretching exercises, in addition to 5-min class organization and instructions. In contrast, the comparison students participated in the 30-min lecture on benefits of PA and appropriate methods of PA in a regular PE lesson. During the lecture, the PE teacher showed the pictures in relation to the benefits of varying exercises, asked students to conduct mock interviews with their peers about their PA participation and methods they used, and summarized the benefits of PA and appropriate methods of engaging in PA.Post-test: After finishing the lecture-typed PE lesson, the control students performed on the d2 Test while following the same testing procedures as the pre-test in their classroom. For the intervention students, right after the aerobic PA-focused PE lesson, they returned to their classroom and took the d2 Test of Attention while following the same testing procedures as the pre-test as well. The PE teachers collected the testing sheets from their students.
Outcome Measure- d2 Test of AttentionThe d2 Test is standardized paper and pencil letter-cancellation test that measures neuropsychology performance of the students in the areas of sustained and selective attention as well as concentration [20]. It consists of 14 lines of 47 randomly mixed letters “d” or “p” with 1-4 dashes arranged individually or in pairs above or below the character. The students are instructed to scan the characters and mark only the letter “d” with 2 dashes either above or below, or one dash on top and one on the bottom within 20 s per line for a total of 4 min and 40 s to complete the test. Distractors come in two forms, more or less dashes above or below the “d”, and the letter “p”… .d d d.. .Three parameters of the d2 Test for sustained and selective attention and concentration were used for data analysis in this study. They area. TN: the total number of items processed within the d2 test. TN is a quantitative measure of the processing speed;b. E%: the sum of omission and commission errors divided by the total number of items processed. E% is a measure of accuracy and thoroughness; andc. CP: the total number of correct responses minus commission errors. CP is an objective measure of attention span and concentration ability.Values of both TN and E% are subject to learning effects, while CP is viewed as independent from manipulative [20,21]. The d2 Test had high test-retest reliability coefficients for all parameters, ranging from .95 to .98 [21]. The d2 Test has been proven to be an internally valid measure of scanning accuracy, speed, discriminant validity and fluctuation across trials.21The test-retest reliability of the d2 Test has been shown to be very high (.95-.98) for all parameters [20,21]. Test values for criterion, construct, and predictive validity have been stable over the course of 23 months after the initial testing [20,21].
Descriptive statistics of TN, E%, and CP at pre- and posttest were computed for each group. Percentage improvement in TN, E%, and CP (percentage improvement= (Mt2-Mt1)/Mt1 x 100)) from pre- to post-test for the experimental group and the comparison group were computed. In addition, independent t-tests were performed to compare the pre-test in the three dependent variables between the two groups. Also, descriptive statistics of the percentage improvement in the three dependent variables were conducted for each group. A 2 x 2 mixed factor analysis of variance with repeated measures was used to examine differences between pre- and post-test (within subjects) and differences between the experimental group and the comparison group (between subjects). ANOVAs with repeated measures were conducted separately for the TN, E%, and CP. When the assumption of sphere city was violated, the Greenhouse-Geyser correction was reported. Post hoc contrast (Bonferroni adjustment) was used to test effects between the two groups. The η2 was calculated as the effect size of ANOVAs. We did not include the gender into the analysis because previous validation studies showed no gender differences in each parameter of the d2 Test. Statistically significant level for all analyses was set at p < 0.05. All data were analyzed using SPSS version 24.
Descriptive Statistics
Table 1 presents the descriptive statistics of pre-and post-test in d2 Test of Attention between the experimental group (EG) and the comparison group (CG) as well as the percentage improvement in the three dependent variables from pre- to post-test between the two groups. At pre-test, the CG’s mean scores in TN (processing speed) and CP (focused attention) were slightly higher than the EG’s mean scores. The higher numbers of TN and CP indicate the better performance in attention and concentration. The CG’s mean score in E% (accuracy and thoroughness) was similar to the EG’s mean score. The lower scores in E% represent the better accuracy. Further, independent sample t-tests revealed no significant mean differences between the two groups in TN, E%, and CP (t=.360, df=78.40, p=.720; t=.389, df=90.94, p= .682; t=.919, df=80.44, p =.895) at p>.05.
Table 1: Means and standard deviations for three parameters of d2 Test at pre- and post-tests and for improvements between the experimental and the control group.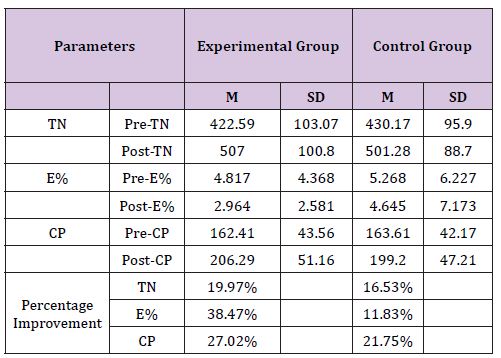
At post-test, the EG’s mean scores in TN and CP were higher than the CG’s mean scores. Also the mean score in E% of the EG was much lower than that of the CG. Regarding the percentage improvement in the three dependent variables from pre- to posttest for each group, both groups showed increased mean scores in TN and CP and decreased mean score in E%. The results indicated the two groups’ performance in TN, E%, and CP was improved from the pre- to the post-test. However, the EG’s percentage improvement in E%, CP, and TN were greatly higher, moderately higher, and higher than the CG’s percentage improvement in the three dependent variables.
ANOVA with Repeated Measures
Table 2 illustrates the results of 2 (pre-test vs. post-test) x 2 (CG vs. EG) ANOVA repeated measures. The results showed a significant effect of time, but no significant effect of group for the three dependent variables (TN, E%, and CP). The results indicated that all participants in both groups significantly improved their d2 test performance and decreased the number of errors from the pre-test to post-test with a relatively large effect sizes (Table 2), and (Figure 1-3). Further, as presented in (Table 2), the repeated measure ANOVA revealed no significant interaction between time × group in TN and E %. However, (Figure 2) shows a relatively large degree of changes from pre- to post-test for the EG compared to the CG. Also, (Figure 2) displays relatively large different mean scores in E% between the two groups at the post test. Echoing the results, (Table 2) shows EG had a larger percentage improvement in E% compared to the CG. In addition, the significant level of the time x group intervention in CP was close to p<.05. The results indicated that the EG showed a higher change in performance of CP (focused attention) from pre-to post-test which compared to the CG (Figure 3). Furthermore, at the post-test, independent t-tests indicated that there was no significant performance improvement in TN, E%, and CP between the two groups (t=.015, df=75.181, p>.05; t=-.003, df=53.545, p>.05; t=.480, df=87.731, p>.05).
Figure 2: Changes in E% for the two groups.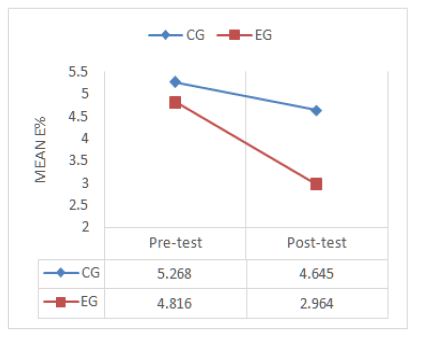
Figure 3: Changes in E% for the two groups.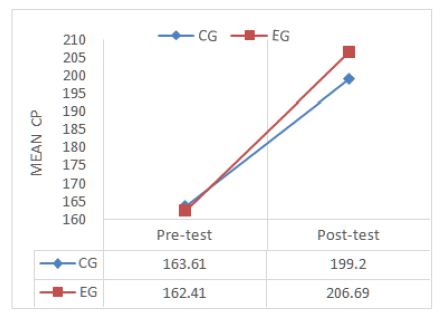
Discussion
This study investigated whether the afternoon PE lessons could improve attention and concentration in school-aged children. Participants took d2 Test before (after taking the 30-min regular academic lesson) and after participating in either 30-min aerobic PA-focused PE lesson (experimental group) or 30-min lecture on benefits and methods of PE lesson (comparison group) late in the school day. Confirming the first hypothesis, the students scored significantly higher in TN, E%, and CP immediately after the 30-min PE lessons (30-min aerobic PA-focused PE lesson and in 30-min lecture-typed PE lesson), compared to the pre-test (immediately after the 30-min regular academic lessons). Our results supported previous consistent findings showing that acute bouts of aerobic PA (e.g.,10-min, 12-min, 15-min, 20-min, and 50-min) immediately enhanced attention and concentration performance in school-aged children [1,2,5,7,8].
Furthermore, the results partially supported the second hypothesis that students in the 30-min aerobic PA-focused PE lesson will show higher positive changes in attention and concentration performance than students in the 30-min lecture-typed PE lesson from pre- to post-test. In this study, the students in the 30-min aerobic PA-focused PE lesson showed a higher degree of better processing speed, accuracy, and concentration performance and a higher level of percentage improvement in the three parameters compared to the comparison group, although did not reach a significant level of p<.05. Partially supporting the present result, Gallotta et al. [1] found that students in the two groups: the 50- min aerobic PA-focused PE lesson and 50-min academic lessons about humanistic subject matter showed a higher level of attention before and after the classes compared to the students in the 50-min coordinated exercises-focused PE lesson.
Previous studies have explored potential physiological mechanisms for generating beneficial acute effects of aerobic PA on attention and concentration in school-aged children (20-30). Studies found that acute bouts of aerobic PA increased cerebral oxygenated blood flow, alpha activity of the precuneus [23,24]. Also, acute bouts of aerobic PA activated connections of the neuro networks between cerebellum and frontal cortex and elevated levels of Brain-Derived Neurotrophin Factor (BDNF) in the blood [5,25,26]. These increased levels play important roles in improving brain functions such as attention span, concentration, and working memories, and visual-spatial abilities [24-29]. However, the previous studies have not examined whether the enhanced acute effects of the aerobic PA on students’ attention and concentration are implied to late in the school day.
The unique finding of this study showed that the fourth- and fifth- grade students demonstrated faster working speed, better accuracy, and higher concentration scores immediately after participating in 30-min aerobic PA-focused PE lesson late in the school day, compared to immediately after taking the regular academic lesson in the afternoon. According to the lesson content described in the methods section, the students were engaged in vigorous intensity level of aerobic PA in the 30-min aerobic PAfocused PE lesson. Our finding was contrary to previous studies reporting a positive effect of moderate intensity level of acute PA on attention in school-aged children [2,5,19].
The inconsistent finding might be related to the intervention conditions which occurred at different timings of the school day. In the previous studies, students taking the d2 Test before and after acute bouts of PA with varying intensity levels and durations took place in the morning of the school day. Previous findings showed that a short bout of moderate intensity level of PA produced positive beneficial effects of attention and concentration for school-aged students in the morning of the school day [2,5,19]. However, our unique finding suggests that participating in 30-min aerobic PAfocused PE lesson has pronounced, facilitating effects on attention and concentration in school-aged children in the afternoon, especially late in the school day.
Another unique finding of this study indicated that the students showed significantly higher performance in attention and concentration immediately after the 30-min lecture-typed PE lesson compared to immediately after the 30-min regular academic lesson. This finding might be related to the lesson content and instructional methods. As described above, during the 30-min lecture-typed PE lesson, the students focused on learning a variety of PA methods and the benefits of PA participation. In order to make the lesson content meaningful and authentic to students, the PE teachers encouraged students to take active responsibility for their learning process through engaging them in conducting peer interviews, sharing their findings of the interviews about benefits of PA and methods for PA from students’ perspectives and experiences, and highlighting the shared findings related to the lesson focus.
These inquiry-based, students-engaged active learning strategies might spark students’ interests in, enhance their motivation for, and increase their enjoyment of learning the lesson content. Motivation and positive mental state play roles in boosting the level of arousal, which facilitates cognitive responses such as attention and concentration performance [30,31]. Similarly, Janssen et al [5]. Found that the students showed a significant higher attentional performance after participating in the 15-min story-telling lecture, compared to the students after attending the regular academic tasks (mathematical problems). Also, in line with the present finding, previous studies evidenced that the interactiveand active-engagement instructional methods are more effective than traditional lectures for gaining students’ attention to the learning process, focusing on the task engagement, and staying focused on the instructional process [32-35]. This study suggests that the lecture-typed lesson in which the students are engaged in active, responsible, and cooperative learning processes is critical to facilitating students’ attentional performance even late in the school day.
In general, the strength of this study is to use the schoolscheduled PE lessons as the treatment conditions to examine their acute impacts on students’ attention and concentration late in the school day compared to the regular school-scheduled academic lesson. Further, the study suggests that in order for students to pay attention to instructions and maintain task-engagement, school administrators may intentionally schedule a regular PE lesson in the afternoon whenever possible, or may alternate a morning PE lesson with an afternoon PE lesson per semester for students. Also, PE teachers may incorporate more aerobic-typed PA that is developmentally appropriate for their students’ fitness and skill levels into their afternoon PE lessons. In addition, school administrators may use professional development activities to provide their teachers with opportunities for learning and implementing innovative instructional strategies such as active and interactive learning, cooperative learning, collaborative learning, and problem-based learning. Teachers may deliberately and appropriately incorporate these instructional strategies into learning and teaching processes to ensure students to be active learners instead of passive learners. The suggestions resulted from this study are potentially feasible for schools to implement in school settings.
It is worth to note that this study has three limitations. First, this study did not use passive rest as the control group. The main reason is that this study took place in a school setting. If we asked students to simply rest for an entire academic lesson merely for the sake of this study, this would interrupt the school’s regular academic schedules, so that the school administrators and teachers as well as parents would be hesitant to allow their students to participate in this study. Second, this study did not objectively measure students’ intensity level of aerobic PA during the 30-min aerobic PA-focused PE lesson, although shuttle running and running through the obstacle courses continuously are good example of vigorous intensity aerobic-typed PA. Due to different levels of students’ aerobic fitness which is an important moderator impacting PA and cognitive functions [25,36,37],future studies may objectively measure students’ intensity levels in different experimental conditions using accelerometer to examine acute effects of aerobictyped PA with varying intensity levels on students’ attentional performance late in the school day.
Third, this study did not examine any delayed effects of the 30- min aerobic PA-focused PE lesson and the 30-min lecture-typed PE lesson on students’ attention and concentration in the afternoon of the school day. Chang et al. [38] found significant acute PA effects on attentional performance 11 to 20-minute after the PA intervention. Further, Schmidt et al. [6] reported students’ showing pronounced improvement in attention and concentration 90-min after the 45- min coordinated motor skills PE lesson in the morning of the school day. As the acute PA produces positive delayed effects on attentional performance, future studies may examine varying delayed effects of the 30-min aerobic PA-focused PE lesson on students’ attentional performance in the afternoon of the school day. The positive findings would further evidence that implementing afternoon aerobic PA-focused PE lessons is instrumental to keeping students stay-focused in the next regular academic lesson.
It was concluded that after participating in both the 30-min aerobic PA-focused PE lesson and the 30-min interactive lecturetyped PE lesson late in the school day, the students had a large size of improvement in attention and concentration, compared to after attending the 30-min regular academic lesson. However, there was no significant different degrees of improvement in the processing speed, accuracy, and concentration between the students in the aerobic PA-focused PE group and the students in the interactive lecture-typed PE group from before to after the PE lessons, although the experimental students showed a higher percentage of improvement in the three parameters compared to the comparison students. This study suggests that a regular school-scheduled PE lesson that focuses on aerobic-typed PA is instrumental to improving students’ attention and concentration, especially in the late school day.
For More Articles: Biomedical Journal Impact Factor : https://biomedres.us