Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Health Informatics: A Vital Strategy to Tackle Pandemic Diseases
Mini Review
Medical records for a patient’s medical information were written on paper with the details of their medical history and care, but they were not in widespread use until 1900-1920 [1]. Physicians have to go through all paper charts to search for relevant information for the patients. They may end up not finding any information linked to the disease because these records on paper have restrictions on retrieving information and being limited with information. The writings of medical records have evolved to be maintained in a computer system to make it convenient for physicians [2]. Data is a valuable asset in the calibration, validation, and evaluation of any condition, and it plays a critical role in comprehending the disease. As of now, we are aware of the critical significance of health informatics, particularly in the maintenance of medical records. Medical records and health-related data play an important part in many disease outbreaks, the secondary disease approaching after these diseases, one of them the whole world faced recently is COVID-19. According to statistics, the rising number of people diagnosed with COVID-19 as a tragedy can provide a wealth of information for measuring and studying these types of ailments in the future, allowing for early detection and treatment. The term “health informatics” refers to the use of information technology and modern computer software to maintain medical records that contain not only episodic medical interactions but also health and lifestyle data with information on the effectiveness of drugs and therapeutic strategies in the form of Electronic Health Records (EHR), has become popular in recent years [1]. When we talk about Health Informatics (HI), the discussion is about the multidisciplinary field encompassing a wide range of disciplines that one conceptualizes, constructs, develops, implements, and evaluates. The assessment is based on related methods, tools, and concepts for clinical care and research support [3]. Due to the virulence and transmissibility of the causative virus, SARS-CoV-2, the pandemic coronavirus outbreak of 2019 has piqued the interest of many researchers and medics throughout the world [2]. This pandemic has had an impact on the global economy and healthcare system. Even in an era when information technology reigns supreme, exact information about the number of cases, the severity of disease, mortality rate, and clinical predictions lags [4]. Applying digital technologies such as big data analytics, next-generation communications networks, and artificial intelligence could solve this fundamental difficulty connected to pandemic management and containment. Collaborative data infrastructures, databases, and digital technologies are some of the existing health informatics solutions that have the potential to speed up COVID-19 epidemiology, pathophysiology, and healthcare system dynamics discoveries. There are issues with data sharing and governance and the near-term directions for improving and supporting clinical research in the COVID-19 pandemic [5]. Public health authorities must be able to access the data shared globally to monitor the COVID-19 outbreak. The ‘Worldometer,’ which offers a real-time update of the actual number of individuals suffering from the covid-19 disease worldwide, daily new cases of the disease [6], disease distribution by nations, and disease severity, are just a few of the initiatives taken by the organizations [7]. Artificial Intelligence (AI) and Deep Learning techniques can help to improve COVID-19 detection and diagnosis. These algorithms can be used as a primary screening tool for suspected infections, and those who are at a higher risk of disease can be tested for confirmation or quarantined. Although most patients with coronavirus infection exhibit minor symptoms, clinicians are using the same amount of isolation, treatment, and monitoring techniques on all of them [7]. By automating various processes such as determining the role of treatment and care by analyzing clinical data with the use of pattern recognition approaches, and digitalization of patient’s reports in terms of medical records for future reference, AI and machine learning-based systems can be used to reduce the burden of work for health care professionals and medical staff [8]. Furthermore, this massive data can be utilized to train multiple machine learning algorithms to classify patients as patients with mild, moderate, or severe disease, particularly those at high risk of mortality, based on the severity of the infection, to treat the patient most effectively accordingly [7]. The patient data can be utilized as a training dataset for predicting other patients’ mortality risks using a prognostic prediction algorithm based on machine learning approaches [8].
Gynaecological Management in Siddha System of Medicine
Obstetrics and Gynaecology in Siddha Medicine
In India, the prevalence of gynecological disorders are alarming in situation at present. Due to the social stigma, the women do not disclose their gynecological disorders even to their closest neighbors. They disclose their problems to the local herbal healers or practitioners only. Noticeable rise in the gynecological disorders in India during the last few decades has drawn interest of all medical sciences to search for an effective alternative in the treatment of female reproductive tract disorders with minimal untoward effects. Women of contemporary era seek guiding principle towards sustaining her wellbeing. The practitioners are performing an excellent task in this regard. It is the responsibility of consultants to adhere to this commitment and principles, explore the knowledge and provide healing to her ailments. The health status of a girl /women is the backbone of the family and society. The health issues during childhood, adolescent period, pregnancy and postmenopausal stages are preventable and can be managed well with Siddha system of Medicine. The branch dealing with the health of the female reproductive organs (Gynaecology) [1] in Siddha system is called as “Magalir Maruthuvam” and the branch dealing with healthy maintenance of pregnancy, labour and puerperium (Obstetrics) in Siddha system called is called as “Sool Maruthuvam”. Pre and post-natal care in Siddha system for attaining a healthy offspring is essential for future generation. Also, the higher statistics of caesarean section in this advanced technical days, make the people to get the inputs of traditional system for their safe parturition. Hence Sool, Magalir Maruthuvam is the branch of Medicine dealing with the diseases of female reproductive organs in female children, adolescent girls, post-menopausal women, female infertility, pregnancy, antenatal, natal & post-natal care and their management and treatment through Siddha system of Medicine [2]. Siddha aims at preservation and maintenance of health and hence there is a tremendous scope of Siddha practitioners in Gynaecology to face the challenge of making Siddha as primary and only care for many benign disorders.
Common Gynecological Diseases
The common gynaecological disorders are infertility, amenorrhea, menorrhea, Poly Cystic Ovarian Syndrome (PCOS), Pelvic Inflammatory Disease (PID), Leucorrhoea etc., These are termed as mentioned below: a) Sinaipaineerkatti (PCOS) b) Soothagavali (Dysmenorrhea) c) Perumpadu (menorrhagia) d) Vellainoi (leucorrhoea) e) Maladu (infertility) [2] etc., The treatment for female gynaecological diseases with present day modern allopathic drugs that may be prescribed for a long period of time, have significant side effects such as nausea, vomiting and other digestive problems; liver and kidney disorders, involvement of heart related problems [3]. Various Siddha formulations and available herbal-polyherbal- herbo mineral practices for gynaecological disorders, which are depicted in the Siddha literatures possessing potential therapeutic values, with scientific validations are being practiced by Physicians across the state of Tamilnadu, India. The therapeutics in Siddha enunciates the treatment to the core of the ailments [4].
Infertility in Females
Infertility is a common clinical problem and is defined as inability of a couple to conceive naturally after one year of regular unprotected sexual intercourse. In Siddha System of Medicine, Female Infertility is generally called as Karpa Rogam (i.e diseases which prevents pregnancy) or Pen Maladu. The patients were treated according to everyone’s complaints and conditions. Siddha system of medicine provides a complete and trusted line of treatment for female infertility.
Antenatal Care
Makapperu kaalam (Pregnancy period) is a crucial period in the life of a woman during which she has to adopt the healthy behaviours for the development of the embryo in healthy environment. Some major food regimens are mentioned in Siddha literatures for women that have to be followed throughout the gestational period for combating the possible occurrence of common ailments for the women during the entire gestational period. Another food regimen is dealt for the wellness of both the mother and the growing foetus to have normal labour process. This has to be adhered during every month of pregnancy for a healthier antenatal period (under the guidance of an expert) and for a normal delivery [5].
Postnatal Care
Most of the deaths of either mother or newborn after delivery are preventable if utmost care of both is available. The mother who had experienced the stress and strain during labour requires time to recover completely. In addition to this, she has to take care of her baby too as the newborn baby is completely dependent on her. Accordingly, Siddha system of Medicine has scientifically designed the post-natal care of both mother and the baby with diet and customs that are aimed to have normal puerperium for mothers and the normal health status of the newborn. Many complications may occur leading to delayed developmental milestones and sometimes death also. The regimen described in the literatures are planned in order to bring the woman to her pre pregnancy state and to make adaptation of the baby to the external environment. The Siddha post-natal regimen is formulated based on the food and nutrition, the physical and the mental activities of mother and child. This includes daily food pattern for the feeding mother with the ingredients of galactagogue and uterine tonics. The feeding of colostrum’s to the baby is stressed to boost the immunity of the newborn [6].
Care of Women in Postmenopausal Period
Menopause is the permanent cessation of menstruation resulting in the loss of ovarian follicle development [7]. Irregular periods, hot flushes, night sweats, vaginal dryness and itching, and mood swings– all these are typical symptoms of menopause. Siddha system of Medicine view menopause as a natural transition of life process in a female. Health problems arising during this period indicate imbalances in the humoral factors of the body and diet of the women plays a vital role in balancing hormones during premenopause and menopause periods [8]. Siddha system emphasizes to take a varied diet which contains fruits, vegetables, whole grains that are rich sources of phyto estrogen. Lifestyle management is recommended during the time of menopause [9]. The treatise of Siddhar Theraiyar on “Prevention of diseases” which insists every individual to follow certain codes and regulations in daily and seasonal regimens is the actual method of combating menopausal disorders in a women. Siddha system of Medicine is the traditional system which takes care of a women even from the day one of the conception of the zygote which is going to be the futuristic women.
Leightner, Inoue, and Lafaye de Micheaux [1] are the first researchers to apply a variable slope estimation procedure to the spread of an infectious disease – Covid-19 [2]. They applied this technique to data from Brazil, Europe, South Africa, the United Kingdom, and the USA for early 2020 to the end of March 2021. They used weekly data on the number of “new” Covid-19 cases to estimate the change in “new” Covid-19 cases next week due to one more “new” Covid-19 case this week. I follow what they did in some ways and deviate in others. Specifically, I continue to use a one week lag because the Center for Disease Control [3] says that the medium incubation period for Covid-19 is four to five days and the data available for North America is weekly. However, I deviate from what Leightner, et al. [1] did by using the number of cases of Covid-19 in time periods t and t + 1 instead of the number of “new” Covid-19 cases. I made this change because all current cases of Covid-19 can spread the disease, not just “new” cases. Leightner, et al. [1] data ended in March of 2021, but the data for this paper extends through October 9, 2021.This extension of the data is important because the Delta variant of Covid-19 hit North America after March of 2021, and the Delta variant is much more infectious. Finally, I find estimates for the spread rate of Covid-19 in Mexico and Canada – two countries not examined by Leightner, et al. [1]. I use the same variable slope estimation technique employed by Leightner, et al. [1] which is Reiterative Truncated Projected Least Squares (RTPLS).
Materials and Methods
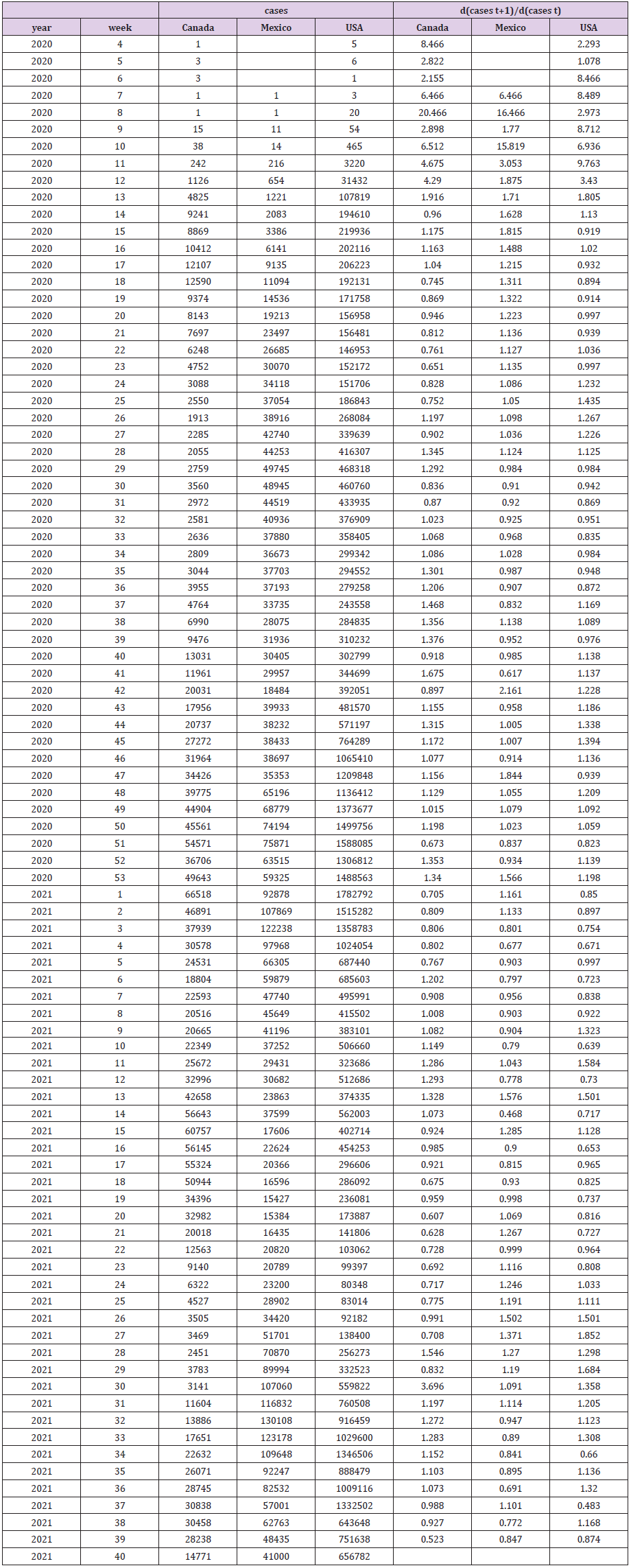
The data was downloaded from the webpage of the European Centre for Disease Prevention and Control (2021) [4]. I began the data series for each country at the point when that country’s number of Covid-19 cases remained above one for the rest of the data set. This resulted in Canada’s and the USA’s data starting in the fourth week of 2020 and Mexico’s data starting in the seventh week of 2020. The data is presented on the left side of Table 1 and depicted in Figure 1. Leightner, et al. [1] use simulation tests to compare and contrast three different variable slope estimation methods – variable slope ordinary least squares (VSOLS), variable slope generalized least squares (VSGLS), and reiterative truncated projected least squats (RTPLS). Although VSGLS is theoretically the best linear unbiased estimate (BLUE), Leightner, et al. [1] used RTPLS because simulations show that RTPLS produces noticeably less error than VSGLS when all the variation in the dependent variable is due to omitted variables and RTPLS captures non-linear relationships better than VSGLS and the spread of a disease is nonlinear [5]. Simulations show that VSOLS was always far inferior to both VSGLS and RTPLS.
Figure 1: Number of Cases of Covid-19.
All three variable slope estimation methods are built upon the following ideas: (1) Omitted variables destroy the reliability of estimated coefficients and statistics when they affect the estimated slope (if an omitted variable does not affect the slope in the sample or population, then it merely adds more random noise to the estimation, and does not bias the estimates), (2) If omitted variables affect the estimated slope and they are ignored, then the estimation procedure produces a constant slope, when in truth the slope varies due to the omitted variables (thus the resulting estimates are hopelessly biased), and (3) Omitted variables will affect the relative vertical position of observations [6].
All three variable slope estimation procedures use the relative vertical position of observations to capture the influence of omitted variables; all three produce a separate slope estimate for every observation where differences in these slope estimates are due to omitted variables. Variable slope estimation produces estimates that show all the ways that the dependent and independent variables are related (i.e. total derivatives); in contrast to more traditional estimation techniques which produce estimates holding all other included variables constant (thus, partial derivatives). Leightner, et al. [1] explain all three variable slope estimation procedures, test all three using simulations, and then uses RTPLS to estimate the spread rate of Covid-19 as described above. Leightner, et al. [7] and Leightner [8] explain RTPLS and present the mathematical equations used in it. Both Leightner, et al. [1] and Leightner, et al. [7] are open access articles. Published applications of RTPLS include estimates of the inflation/unemployment tradeoff, pollution abatement, effectiveness of monetary, fiscal, exchange rate, and trade policies, and the effects of China accumulating US dollars on the value of the US dollar and on the US trade deficit.
Results
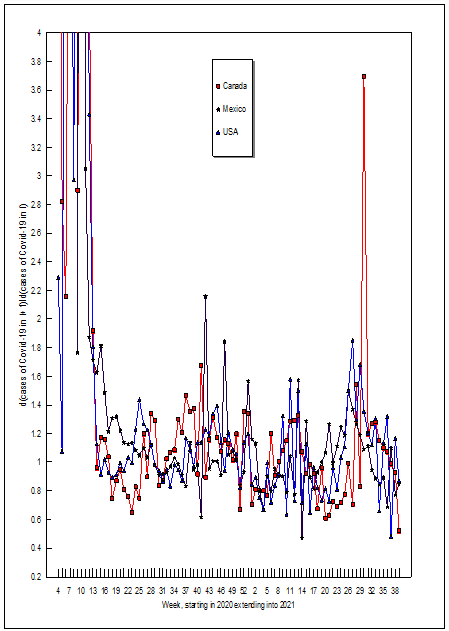
Figure 1 plots the data over time. The two upward spikes in the number of Covid-19 cases in the USA correspond to new variants of the virus. Variant B.1.1.7 hit the world in September 2020 (≈week 38) and the Delta variant hit North America in June of 2021 (≈week 25) (Center of Disease Control and Prevention, 2021) [9]. Figure 1 shows that Mexico and Canada also experienced these new variant spikes (although Canada’s Delta spike occurred with a 6 week lag). The noticeable declines in Covid-19 cases in early 2021 in all three countries corresponds to when vaccines were first available. The estimates for d(cases of Covid-19 in t+1)/d(cases of Covid-19 in t) are given in the right half of Table 1 and depicted over time in Figure 2. The d(cases of Covid-19 in t+1)/d(cases of Covid-19 in t) estimates are highest and most unstable when Covid-19 first emerged in each country. The d(cases of Covid-19 in t+1)/d(cases of Covid-19 in t) value for Canada in the fourth week of 2020 means that an additional case in that week would be correlated with 8.466 additional cases the next week. A close examination of Figure 2 reveals some common trends for all of North America: (1) from 2020 week 13 through the end of 2020 d(cases of Covid-19 in t+1)/ d(cases of Covid-19 in t) estimates were on an upward trend, (2) d(cases of Covid-19 in t+1)/d(cases of Covid-19 in t) fell in early 2021 as vaccinations become available, (3) d(cases of Covid-19 in t+1)/d(cases of Covid-19 in t) again rose between weeks 4 and 13 of 2021, then fell between weeks 14 and 22, rose again between weeks 21 and 30, and then fell after week 30 of 2021.
Table 1: The Data and Empirical Estimates.
Discussion
It should be noted that the estimates of d(cases of Covid-19 in t+1)/d(cases of Covid-19 in t) given in Table 1 and depicted in Figure 2 are for both increases and decreases in the number of cases in time t. However, every time the estimate of d(cases of Covid-19 in t+1)/d(cases of Covid-19 in t) was less than one, Covid-19 cases declined the next time period. This means that if Canada, Mexico, and/or the USA could reduce the number of cases in time t by one [perhaps by stricter social distancing laws, mandating vaccines, or rapid testing and quarantining [10], then the number of cases in time t+1 would decline by less than one. However, if something (like a new Covid-19 mutation or more humid, cooler weather) would increase the number of Covid-19 cases in time t, then the number of cases in time t+1 would increase by more than one. Thus it is harder to kill this virus than it is for it to spread. Governments and people need to do all that they can to beat this virus, because it is easier to spread than it is to defeat.
Figure 2: d(Cases of Covid-19 in t+1)/d(Cases of Covid-19 in t).
Declarations of Interests
None. • This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Relationship Between Vitamin D Levels and Covid-19 Severity Due to Circulating SARS-COV-2 Variants in Argentina: A Presentation of Clinical Cases
Introduction
During the current pandemic of atypical pneumonia caused by the SARS-CoV-2 coronavirus, it has been observed that vitamin D (VD) deficiency would represent a significant risk factor in the severity and prognosis of COVID-19 with a higher prevalence of hypertension and cardiovascular diseases. As of August 2021, Argentina was the second Latin American country with the highest number of confirmed cases and the fifth with the highest number of deaths from COVID-19, according to official statistics [1], despite having been subjected to one of the longest quarantines of the world, which justifies and strengthens the selection of this country to carry out research works such as the one presented here. Previous studies consider that the weighted average prevalence of VD deficiency in the Argentine adult population is around 43.3% [2]. In this context, the present study aimed to investigate the possible relationship between the evolution of the disease concerning serum VD levels in a series of clinical cases of patients with COVID-19. They were admitted to the critical care area of Hospital Luis Carlos Lagomaggiore, Mendoza, Argentina.
Presentation of the Series of Clinical Cases
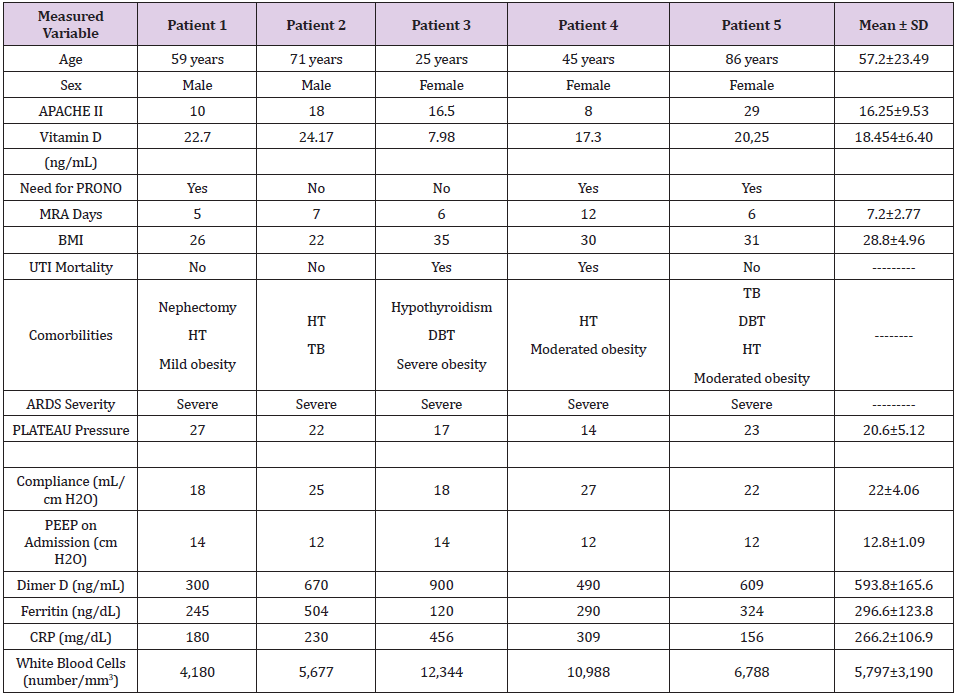
We present a series of 5 patients, 2 men and 3 women in an age range of 25 to 86 years, with a positive diagnosis by polymerase chain reaction (PCR) to detect SARS-CoV-2. They all required admission to the critical care unit due to acute respiratory failure and received the standard care recommended to manage this pathology (invasive hemodynamic monitoring, mechanical ventilation, and other procedures). Table 1 shows the clinical cases and the most outstanding variables analyzed. Biochemical/ inflammatory parameters were requested (vitamin D, D-Dimer, ferritin, ultrasensitive C-reactive protein, blood count, among others). Likewise, ventilatory mechanics measurements were performed at the time of linkage to mechanical ventilation (MRA). As observed in the series of cases presented, the serum VD levels in all the patients analyzed are below what is established as normal or sufficient levels of VD (> 30 ng/mL), reaching not only levels of insufficiency (<30 ng/mL), but even VD deficiency (<20 ng/mL). Regarding mortality, of the total sample (100%), 2 (40%) patients died. The deceased patients were identified as 3 and 4, and they also had the lowest values in the VD dosage (7.98 ng/mL and 17.3 ng/mL, respectively).
Table 1: Variables were analyzed in the 5 patients belonging to the series of clinical cases studied. Abbreviations: acute respiratory distress syndrome (ARDS), HT (hypertension), BMI (body mass index), TB (smoking), DBT (diabetes), ICU (intensive care unit), PEEP (end-expiratory pressure), MRA (mechanical ventilation), CRP (C-reactive protein), and Mean ± SD (mean ± standard deviation of the 5 patients) for the quantitative variables.
Discussion
The 5 patients studied showed a significant increase in inflammatory parameters, accounting for the severity of the COVID-19 developed, starring the characteristic cytokine storm. Consistent with our results, some previous studies have suggested the existence of an inverse relationship between serum VD levels and the degree of severity due to COVID-19 [3-8]. However, none of them has specifically evaluated this relationship in patients affected by the variants of SARS-CoV-2 Gamma (Manaus) and Lambda (Andina), with a majority presence in Argentina at the date of this study [9].Therefore, the importance of this research is fundamentally in that its results would contribute significantly to establish an inverse relationship between serum levels of VD and severity of COVID-19 in patients infected by the variants mentioned above, representing an essential contribution to the genomic surveillance process [10], not only in Argentina, if not in all those countries in the world that are mainly affected by the presence of the Lambda and Gamma variants. This contribution would significantly improve the prevention and treatment of COVID-19, mainly when any of these variants develops the infection. Likewise, additional studies should be performed in populations with another viral circulation profile to evaluate this relationship (VD levels vs COVID-19 severity) versus other SARS-CoV-2 variants.
Authors’ Contribution
All authors contributed in the same way in the conception and design of the review, with a substantial contribution on the data, analysis and interpretation of the contents, writing and critical review of the article for its intellectual content.
Declaration of Conflict of Interest
The authors declare no potential conflicts of interest concerning the research, authorship and/or publication of this article.
Financial Support
The authors declare that they have not received financial support for the research, authorship and/or publication of this article.
Immunogenicity and Safety of Sinopharm COVID-19 vaccine in young mice
Introduction
The severe acute respiratory syndrome caused by coronavirus 2 (SARS-CoV-2), also called COVID-19, has quickly spread over the whole world and raised severe public health distresses. The scientific society is intensely requested investigating treatments that would potentially be effective in fighting COVID-19 [1,2]. During July 2021 WHO revealed that the COVID-19 pandemic caused more than four million deaths worldwide. Vaccination has been established to limit the further spread of SARS-CoV-2 virus. Children are also vulnerable to SARS-CoV-2 infection, although they display milder clinical symptoms of the disease [3]. This susceptibility raises the possibility of transmission between family members and risk to elderly members who are more prone to the disease [4]. There are four categories of vaccines in use: whole virus, protein subunits, viral vectors and nucleic acid (RNA and DNA). There are additional vaccine candidates currently in the pipeline for COVID-19. All vaccines are trying to attain immunity to the virus, and some may be capable to stop transmission. By finding a proper molecule on the virus they are initiating an immune response to the antigen. In the case of COVID-19 the antigen is usually a characteristic spike protein found on the surface of the virus which assist attacks of human cells [5-7]. In case of using the entire virus (such as Sinovac and Sinopharm) it produces an immune response with the help of antigen presenting cells (APCs) such as dendritic cells (DCs) [8]. In particular, DCs have essential functions in capturing molecules, fragmenting them into smaller peptides and presenting the antigenic peptides on their major histocompatibility complex (MHC) I and II to prime T cells for the start of cellular and humoral immunity against the virus [9]. The study aims to evaluate the immune response of Sinopharm COVID-19 vaccine and its safety in young mice aged two weeks.
Materials and methods
Experimental Animals
Young Swiss Albino male mice (10 ± 2 g) with 14 days old were used for experiments. In order to reduce the contact caused by environmental alterations and handling during behavioral studies, mice were acclimatized to the Laboratory Animal Holding Center and laboratory surroundings for three days and at least one hour before experimentation, respectively. Mice were kept under standard conditions with food (low protein diet) and water available ad libitum. The animals were housed six per cage in a light-controlled room (12 h light/dark cycle, light on 07:00 h) at 27°C and 65% relative humidity. All experiments were carried out between 09:30 and 15:00 h. Each test group consisted of 12 mice, and each mouse was used only once. All animal experiments were conducted according to guidelines set by the Institutional Animal Ethics Committee of the National Medical Research Centre (NMRC35/2009).
Clinical and Necropsy Observations
This study represents one constituent of the safety evaluation program for using Sinopharm COVID-19 vaccine for very young mice to assess efficacy and toxicity. The aim was to evaluate these parameters following the administration of the proposed human vaccine dose. The mice were divided into three groups of 12. Group one received a single dose of 0.5 ml Sinopharm COVID-19 vaccine, Group two received two doses of 0.5 ml Sinopharm COVID-19 vaccine and the second dose was given after 21 days, and group three(control) received two doses of 0.5 ml of 0.9 % NaCl. Mice were examined every day for 40 days. Any signs of ill health were recorded daily. Blood samples for IgM and IgG were taken from animals on day 14 and day 30 after first vaccine application. At necropsy a full macroscopic examination was performed on each animal. Organs macroscopically examined were the spleen, lungs, liver, kidney, heart, brain, testes, and ovaries.
Statistical Analysis
The difference among various treated groups and the control groups were analyzed using one-way-ANOVA followed by using unpaired Student’s t-test. The results were expressed as the mean ± SEM of the number of experiments, with p< 0.05 indicating a significant difference between groups. All p values reported are for a one-tailed test. The significance level was chosen at α = 0.05.
Results and Discussion
Mice have been the most generally used animals in scientific research [10,11]. This could be attributed to the fact that the mouse genome is 99% identical to the human genome, and mice have similar patterns with respect to human organs and systemic physiology. The Sinopharm Beijing Covid-19 vaccine is produced by Beijing Institute of Biological Products (BIBP), subsidiary of China National Biotec Group (CNBG), they use inactive or weakened virus (19nCoV-CDC-Tan-HB02) strain as antigen which based on a form of the virus that has been inactivated or weakened so that it does not cause disease, but is still able to produce an immune response. It has been reported that the effectiveness of the vaccine is approximately 87.5% for the prevention of hospitalizations of Covid-19 patients, 65.9% for prevention of Covid-19, 90.3% for the prevention of intensive care unit admissions, and 86.3% for the prevention of Covid-19-related deaths [12]. Furthermore, children younger than 12 years old are at their crucial phase of growth and development; concern must be taken to assess the long-term effect of COVID-19 vaccine on their growth and development. In addition, children who are going to be vaccinated should have enough immunity and safety against COVID-19 vaccine [13]. It has been reported that Pfizer and Moderna messenger RNA (mRNA) vaccines studied in children older than 12 years and were found safe and effective. In addition, Pfizer and Moderna vaccines were also tested in children under 12, with the aim of involving babies from just six months old. Although teenagers only seldom get badly sick with Covid-19, they are able to spread the infection. Hence, vaccination will be able to assist stopping the pandemic [14]. Sinopharm’s institute in Wuhan approved for emergency utilization on children aged between three and seventeen by the China National Biotec Group in August 2021. China began to permit people aged between three and seventeen to obtain a dose of COVID-19 vaccines in early June 2021, making it the first country to declare the endorsement of vaccines for such a young age group [15]. None of the mice used in the study showed any sign of abnormality or ill health throughout the 42 days postimmunization observation for the three groups after the first dose of immunization. At necropsies no macroscopic treatment related changes were observed. Antibody binding the SARS-CoV-2 spike protein was induced by vaccination, and as expected, the temporal induction of anti-spike IgM was faster than that of IgG. The mice injected with Sinopharm COVID-19 vaccine, or 0.9% sodium chloride solutions were generally in good condition, no obvious clinical unusual symptoms were observed, and no death occurred during the observation period. The mice body weights in control and vaccine groups increased but the increase was more with the vaccinated group by around 1.5 times compared with the initial weights. There were significant differences in body weights and food intakes noted between the vaccine and negative control groups throughout the study period. Furthermore, no abnormal changes were found in the gross autopsy results of all mice investigated.
Conclusion
Our study shows that the Sinopharm COVID-19 vaccine given to 14 days old mice produces an immune response with no side effects ascertain its safety and protection efficacy against COVID-19. We highly recommend post-marketing surveillance of the vaccine safety when given for children for a longer period than that in adults.
Contributions from the Autonomous University of Zacatecas in the Epidemiology, Diagnosis and Treatment of Trichinellosis, 1986-2021
Introduction
In Mexico, the first reports of Trichinellosis were by Dr. Olvera in 1896 [1], later by Dr. Perrin in 1939, and Dr. Mazzotti carried out the first epidemiological studies in 1943 [2]. The latest reports from the national health secretary are those obtained from 1990- 1994, 2000-2002, 2014, 2015 and 2016, with a total of 1122 cases, the states with the highest number of cases from 1990-2016 were: Hidalgo 216, Chihuahua 113, Veracruz 81, Jalisco 76 and Oaxaca 55, Zacatecas no cases have been reported since 1994, and from 1990- 1994 40 cases were reported [3]. Zacatecas is a state of the Mexican Republic located in the north of the country, it has an area of 75,275.3 Km2, a population density of 21.5 inhabitants / Km2 that represents 3.8 of the national territory and with a population of 1,622,138 inhabitants. distributed in 58 municipalities being the most populated Guadalupe, Zacatecas and Fresnillo, which represents 1.3% of the national population. There are 95 men for every 100 women. 59.4% have basic education, 77.5% have piped water, 96.3% have drainage, 99.3% electricity, 79.7% have some medical safety regime. The economically active population is dedicated to agriculture, livestock, mining, services and industry [4]. The Autonomous University of Zacatecas (UAZ) is considered the civilizer of the north, it was founded in 1832, and its autonomy was in 1968, which currently has an approximate population of 40 thousand students and 6 thousand teachers and administrative personnel UAZ 2020. Trichinellosis was detected for the first time in Zacatecas in 1975, and 4 outbreaks were reported in 1978, the most significant being that of Laguna de Carretero (Municipality of Villanueva), with a fatality of 33%, from 1979-1988 17 outbreaks were reported. The most important being Valparaíso (with one death), and Pozo de Gamboa where a 20-year-old pregnant woman lost the product. Trichinellosis was found to be more frequent in urban than rural areas, the age group from 15-44 years being more affected (49% of cases) and referring to sex 1: 1.8 male / female. Zacatecas currently has 58 municipalities and Zacatecas, Villanueva, Valparaíso, Panucho, Jerez, Jalpa and Guadalupe were affected at that time, and the transmission route was due to the consumption of poorly sewn chorizo, the diagnosis was by direct plate compression techniques, that received the name of trichinoscopy, and by the indirect technique of micro immuno-diffusion-double [5]. The objective of the present work is to make a report of the work carried out in this parasitosis during the period of 1986-2021 in the Autonomous University of Zacatecas.
Materials and Methods
a) Implementation of experimental models, murine (Balc / C mouse, Long Evans rat), domestic dog, rabbit, York pig [6-13]. b) Characterization of the life cycle of Trichinella spiralis [11,14,15]. c) Establishment of direct techniques (plate compression, artificial digestion, and hematoxylin / eosin) and indirect (double microimmunodiffusion, Dot-ELISA, IFI, Western Blot, intradermal reaction) for the diagnosis of Trichinella spiralis [16-23]. d) Evaluation of albendazole in a murine and pig experimental model, its evaluation with 3, 5, 7, 10, 14 days of treatment. In the initial phase of the infection, in the intestinal and muscular phase [11,23,25,26]. e) Evaluation of albendazole in pregnant rats, with the same treatment days [27]. f) Evaluation of the total antigen of Trichinella spiralis in murine and pig models, and of the 45 KDa band in murine models. In the intestinal, muscular phase and after 30, 60, 90 and 120 days of immunogen application. The purpose was to evaluate the modifications of the T. spiralis nurse cell in Long Evans rats immunized with total soluble antigen of T. spiralis and sacrificed at different times. We worked with 25 male rats of 2 and a half months of age, immunizing 20. Subsequently, the 25 rats were challenged with infected T. spiralis meat, sacrificing 5 rats every month, plus a control rat per 4 months, when sacrificing them, direct plate compression techniques, artificial digestion and the hematoxylin-eosin technique were performed; indirect MIDD and Western Blot techniques were performed on the sera [11,26,28-32]. g) To evaluate the protective effect of Trichinella spiralis Total Soluble Antigen combined with bacterial vaccine and VITS via sublingual route in Long Evans rats and to evaluate Lactobacillus casei and VITS in intestinal infection by T. spiralis in a murine model [11]. h) In all treatment models, groups of 5 animals were used, the healthy control, Trichinella spiralis infection control, and the different groups according to the treatment, and direct and indirect techniques were performed. And the results were analyzed by statistical analysis of ANOVA or Student’s t test. i) Epidemiological studies in humans, pigs, dogs, and domestic rats for the detection of Trichinella spiralis, by indirect techniques of double microimmunodiffusion, Dot-ELISA and Western Blot [33-35]. j) Evaluation of a Diagnostic Kit by Dot-ELISA for detection in the field.
Methodology
Used in the experiments were obtained from the animal facility of the Academic Unit of Biological Sciences of the Autonomous University of Zacatecas. The parasite (Mexican strain) was identified with Edoardo Pozio PhD, in the Istituto Superiore di Sanita in Rome, Italy 2000, and has been maintained by serial passage in mice and rats since 1986 at the Laboratory of Cell Biology and Microbiology at the Academic Unit of Biological Sciences from the Autonomous University of Zacatecas, Mexico. All the animals were maintained in controlledtemperature rooms and fed with rodent balanced food [6,13].
Ethical Approval
This study was reviewed and approved by the Bioethics Committee of the Biology Faculty of the Autonomous University of Zacatecas, in accordance with the Official Mexican Norm (NOM-062- ZOO-1999), published by the Secretariat of Agriculture, Livestock, Rural Development, Fisheries and Food (SAGARPA) in the Official Gazette of the Federation (Mexico) on June 28, 2001 [13].
Direct Techniques
Plate Compression Technique
For the plate compression technique, approximately 5 mg of tissue were used (diaphragm, masseter, tongue, intercostals, leg), each sample was placed between 2 lamellae and compressed, occupying an area of 1 x 5 mm, it was observed to the optical microscope, with the 10x and 40x lens [10,11,33,36, 37].
Artificial Digestion Technique
30 g samples were used of homogenized tissue, and they were incubated at 37 °C, in a sack-shaped tulle sieve, suspended in a 0.3% solution of pepsin (10,000 U) and 37% HCl (0.2M) in 500 ml of distilled water, inside a separating funnel; 24 hours later, the larval package was separated with the ILs, which were deposited at the bottom of the funnel, observed in a newbawer camera under an optical microscope with a 10X lens, and the larval package was quantified [7,25,36, 38].
Hematoxylin-Eosin Staining
Hematoxylin-Eosin (H-E) stain. Leg, tongue, and diaphragm samples were taken from each experimental model. The tissues were fixed in 10% buffered formalin for 24-48 hours. Subsequently, they were transferred to 70% ethyl alcohol for automatic processing for approximately 12 hours in two steps of 70% OH, 80% OH, 96% OH, 100% OH and xylol. From this last step, the samples were removed and embedded in paraffin, forming support blocks for making 5-8 μm thick histological sections on a Leica Model 820 microtome. The sections were placed in a float bath at 50 °C and they were lifted on a slide to dry, deparaffinize for an hour in an oven and then go on to the staining process with the Hematoxylin and Eosin technique according to the criteria of Viloria [28].
Indirect Techniques
Double Microimmunodiffusion Technique (MIDD)
For double immunodiffusion, a 1% agar gel was made in distilled water with sodium azide, to avoid contamination; It was placed in an amount of 4.5 mL at 55 °C on a glass slide, once in solid form, the rosette was formed with a hole-hole, ensuring an equidistance of 0.5 cm between well and well; the comparison was carried out by always placing the antigen in an amount of 10 μL (10 μg) in the center and, around it, a serum of known reactivity, (in the same proportion by undiluted volume), leaving at room temperature environment in a humid chamber for 24 to 48 hours, until precipitation lines are observed between the positive serum and the antigen; then the gel was stained with Coomassie brilliant blue G 250, 25% by volume [10].
Dot-ELISA
Several nitrocellulose papers were squared, depending on the number of samples to be used, each 1 cm2 square a 10×5 cm paper. The antigen was placed on the undiluted paper placing the equivalent of 10 μg / μL, then it was allowed to dry at room temperature and once dry, it was proceeded to block with 3% fat-free milk in PBS this for 18 hours. Once the blocking time had concluded, it was washed once with PBS 0.5% Tween 20 for 10 minutes and 2 consecutive times with PBS for 10 minutes each time, then, 10 μL of each test serum was placed in each square and incubated again with 3% fat-free milk in PBS for an hour and a half, at the end of this time we proceeded to wash again with PBS 0.5% Tween 20 for 10 minutes and 2 consecutive times with PBS for 10 minutes, then the second antibody, Anti-IgG, Anti-IgM or Anti-IgA at a concentration of 1: 2000 in PBS conjugated with peroxidase, 10 μL of the second antibody and allowed to dry at room temperature, once dry it was incubated once more with Milk 3% fat free in PBS for an hour and a half and the container containing the paper was completely covered with aluminum foil. At the end of the hour and a half, the paper was washed with PBS Tween 20 at 0.5% for 10 minutes and 2 consecutive times with PBS for 10 minutes. The paper was then developed with 3,3-diaminobenzidine DAB, using 37% hydrogen peroxide as substrate [11,19,27].
Indirect Immunofluoresence (IFI)
The infective larvae (IL) were obtained from the rat muscle infected with T. spiralis, 20 μL of IL were taken and washed for three periods with PBS for 5 min in magnetic stirring, they were incubated with 20 μL of the first Ab with a 1: 100 dilution for 45 min with PBS, they were washed with PBS on 3 occasions for 5 min in magnetic stirring, the liquid was extracted with care to avoid absorbing the LI, 200 μL of the monovalent anti-gamma-fluorescein conjugate was added (IgG dilution 1: 1000), it was incubated for 45 min at 37 °C, the liquid phase was extracted, 3 washes were carried out with PBS in magnetic stirring for 5 min each, lamellae were mounted with the IL, covering them with cover objects and sealed with resin, they were observed under a confocal microscope [38].
Western Blot (WB)
The product obtained from the polyacrylamide gel run was transferred to NC paper [17], using the Transblot-Cell camera (Bio- Rad) at 35 volts, overnight at 4 °C. The NC paper was dyed with fast green for 5 min. With constant stirring, the dye was removed and decolorized in distilled water, to verify protein transfer, it was allowed to dry and the strips of the approximate width of each lane (0.5 cm) were cut. After the above, each strip was covered with a solution of PBS-3% milk powder and 0.15% sodium azide at 4 °C, with constant stirring overnight. They were then washed 3 times for 10 min. with PBS, incubation was continued for 1.5 h. with the sera of the rats in a dilution of 1: 100 in PBS-3% milk powder at 37 °C with constant agitation, subsequently they were washed twice with PBS-0.3% Tween 20 for 10 min and three more with PBS for another 10 minutes. Then, they were incubated with the second anti-rat IgG antibody, conjugated with peroxidase 1: 2000 PBS-3% milk powder for 1 h., At room temperature, with shaking, then they were washed 2 times with PBS-Tween 20 at 3% and rinsed with PBS, for 10 min. The Banding pattern of each strip was developed with 3,3´ di amino-benzidine (DAB), 50 mg in 100 mL of PBS, using, as a substrate, 37% hydrogen peroxide [39].
Intradermal Reaction (IDR)
Intradermal reaction was applied with Total Soluble Antigen of T. spiralis which were 10 units (10 μg of protein), the area of application of the AST was observed at 2, 24 and 48 hours [17,11].
Obtaining Immunogens
The antigen of T. spiralis was obtained, by means of extraction with liquid nitrogen, the infecting larvae were obtained by the artificial digestion technique, liquid nitrogen was added in sufficient quantity to cover the IL and by bursting the exit of antigenic components were centrifuged at 3500 rpm for 1.5 hrs. The supernatant was the soluble antigen of T. spiralis, whose protein concentration was determined and used in the different immunological tests, and as an immunogen (secretion / excretion antigens) in protection studies [6,7, 18,19,11,36].To determine that the antigen had the adequate protein concentration, a standard curve was obtained using bovine serum albumin, according to the methodology of Bradford, 1976, adjusting the concentration of proteins obtained to an optical density of 610 nm using Coomassie blue at 0 .06 % prepared in 2.2% HCl. The value of the optical density of the antigen was interpolated, to that of the standard curve of albumin, the concentration of proteins contained in the two types of antigenic extract was obtained [18].To obtain the immunogenic protein of 45kDa, the AST was subjected to polyacrylamide gel electrophoresis to separate by molecular weight (MW) the proteins that were identified by a PM marker of the 45kDa protein and by elution of bands the required protein was obtained.
Results
The experimental models of infection were implemented in a murine model, Balb / C mouse, Long Evans rat, domestic dog, rabbit, York pig (Figure 1), in all there was the reproduction of the infection and the life cycle, handling an IL per gram of weight. It was in pigs that we observed the clinical picture of the disease: diarrhea in the intestinal phase, and in the systemic and muscular phase: eyelid edema, joint injury, increased temperature. At sacrifice, IL was detected in muscle and brain tissue.
Characterization of the Life Cycle of Trichinella Spiralis
The 3 stages of Infective Larvae (IL) were observed in muscle, male and female adults in intestine and Newborn Larvae (NL) in intestine and muscle. Male and female adults (Figure 4), technical observation of plaque compression and the small intestine was performed with the Fernandez Balls Technique
Direct Diagnose Techniques
In all the experimental models by plaque compression (Figure 7), artificial digestion (Figure 8) and the Hematoxylin-Eosin technique, IL from Trichinella spiralis (Figure 9) were observed. Indirect Techniques: Indirect techniques, double microimmunodiffusion (MIDD, Figure 9.), Dot-ELISA, Immunofluorescence (IFI, Figure 10), Wester Blot (WB, Figure 11) and Intradermoreaction were positive, in WB a triplet of 42,45 and 48 kDa. The intradermal reaction is effective from the first month of infection with T spiralis, which is a very timely diagnosis for the pig without the need for a specialized infrastructure, as well as being inexpensive and can easily be carried out to the field with simple animal handling and not very aggressive, with a presumptive diagnosis after 2 hours of application of the intradermal reaction and confirmatory after 24 and 48 hours, which can prevent infection in man and even other animals in a timely manner. Evaluation of treatment with albendazole, it was effective from day 7, 10 and 14, both in intestinal and muscular phase (Figure 12), murine and pig models, being statistically significant compared to the infected control without treatment with a -P <0.001, by ANOVA, when evaluating the parasite load by artificial digestion.When performing the trypan blue technique to see viability of the IL obtained from the digestion, they were dead, there was penetration of the dye.
Evaluation of the Total Soluble Antigen of Trichinella spiralis in Murine and Pig Models
A statistically significant protection effect was observed in muscle phase, by analysis of variance p <0.0001. (Figure 14), in relation to the infection control group.When evaluating the T. spiralis implant at 30, 60, 90 and 120 days it is observed how the recovery of the tissue occurs, The modifications in the nurse cell of T. spiralis in tissues of Long Evans rats immunized with AST and sacrificed in Different times were evident with the direct techniques of C / P, D / A and H / E staining (Figure 15), it is observed how the encystment is lost and the spiral is no longer viable, being statistically significant with a value of P < than 0.01. By ANOVA.
Evaluation of the Soluble Antigen of T. Spiralis, VITS, Bacterial Vaccine and Lactobacillus Casei
The administration of commercial Lactobacillus casei confers protection at the intestinal mucosa level in T. spiralis infection. Furthermore, based on the results obtained, administering a treatment in the early stages of the infection protects the host against infection by this parasite. The administration of an immunomodulator (VITS) and treatment with commercial Lactobacillus casei promotes a potentiated immune response by producing a greater degree of intestinal mucosa. Immunization with VITS in the experimental model prepares the organism to act against the parasite with a greater degree of effectiveness, thus observing an effective immune response against T. spiralis. An ANOVA statistical analysis was performed with the GraphPad Prism 6 program using the parasite loads obtained from the artificial digestion of each individual and with 95% confidence, resulting in that the groups treated with VITS, Bacterial Vaccine, Lactobacillus casei and soluble antigen of Trichinella spiralis compared to the infection control had a P <0.0001.
Epidemiological Studies
From the sampling of 1096 sera from backyard and technical farm pigs from various municipalities of the state in 1998, an 8% incidence of Trichinellosis was found, the Dot ELISA technique for its diagnosis being reliable and affordable .A study was carried out in pigs in the municipal slaughterhouse of Zacatecas, Jerez, and Ojocaliente in 2006, where 85 samples were obtained from each of them, taking 15 grams of masseter which was analyzed by compression and artificial digestion, resulting in 2 positives.51 languages of dogs collected in the Department of Pharmacology of the Academic Unit of Human Medicine and Health Sciences, of the UAZ, 3 (5.82%) were positive with infection with T. spiralis, which allows defining that the parasite is found in domestic dogs, more often than you might think. In 2002.Analysis of 100 diaphragms of domestic rats and serum from the municipal garbage dump of Zacatecas. Diagnosis by direct techniques of compression and artificial digestion and indirect by MIDD, WB, Results: Trichinella spiralis was detected in 3 diaphragms of domestic rats by direct compression and artificial digestion technique, and by indirect MIDD and WB techniques. In 2006.A study was carried out on 3490 open population sera, of which 640 correspond to sera from children under 15 years of age and 2850 from adults, which were analyzed using MIDD techniques, presenting. In human sera from the Zacatecas Health Center, Zacatecas in 2006, 3 positives were detected by MIDD and WB with a predominance of the triplet of 42,45 and 48 kDa, From the 2008 Guadalupe Zacatecas Health Center, 12 were positive by MIDD, Dot-ELISA and IET techniques with a predominance of the 42,45 and 48 kDa triplet, examining 1209 human serum samples. In human sera from the open child population of the Calera Zacatecas Health Center, from 2011, 3 positives were detected by MIDD techniques, and 12 by Dot-ELISA and IET with a predominance of the triplet of 42,45 and 48 kDa. Ninety-two sera were collected, which were evaluated using the indirect techniques of MIDD, Dot- ELISA and WB, from a technical high school in Fresnillo and 2 were positive by the three techniques in 2017.
Diagnostic Kit
Diagnostic kit based on the Dot-ELISA technique for which a murine model infected with different parasite loads from five to 1500 infective larvae (IL) of T. spiralis was used. The Dot-ELISA technique shows sensitivity from the second week after infection with T. spiralis IL. When making modifications to this technique, a non-significant difference was observed compared to the standardized technique. The objective of making the Trichinellosis Diagnostic Kit in the field was met. Which decreased time and steps. The statistical analysis was carried out in the GraphPad Prism 6 program applying an ANOVA between the results obtained with the standardized technique and after making the modifications. Resulting a non-significant variation with a value of P = 0.5382.
Discussion
The present study is an analysis of the work carried out in the Department of Cell Biology Microbiology of the UAZ, in the line of research of Trichinella spiralis, from 1986-2021.Which has allowed to carry out research work, teaching, training of undergraduate and postgraduate human resources, 80 theses, which have contributed results to the study of Trichinella spiralis., In implementation of experimental models, characterization of the life cycle of T. spiralis, establishment of direct and indirect techniques, evaluation of treatment with drugs and immunogens, epidemiological studies for the detection of the parasite and the proposal of a low-cost and accessible diagnostic kit for the field. Our results coincide with other authors, the investigations have been published. For us it is very important to continue with this line of research, because unfortunately the infection in many cases is not diagnostic, hence our interest in having effective treatments, diagnostic techniques that are preventive against this zoonosis that is increasingly distributed worldwide. climate change favors their presence, the loss of ecosystems, and all this contributes to diminishing and impacting the quality of life not only of humans but also of animals and ecosystems.
Conclusions
The Autonomous University of Zacatecas has a research line in Trichinella spiralis, which has allowed to carry substantive functions, including teaching, research, extension, dissemination, and having an impact on the training of human resources. The findings reported in this research include: a reproducible experimental model for the study of Trichinellosis, reliable diagnostic techniques and confirmatory WB, an effective treatment using albendazole (which must be used under medical prescription), and the study of products such as the bacterial vaccine, the VITS immodulator, the Lactobacillus casei strain, which decrease the parasite load as well as the immunogen of the total soluble antigen of Trichinella spiralis. The contribution of this study has been to provide deeper insights in a disease which is present in the state of Zacatecas, Mexico and is commonly not properly diagnosed or confused with other diseases, we consider very important to continue promoting having a proper diagnosis and prevention of the disease.
Pregnancy Induced Hypertension in Kabo Local Government Area of Kano State, Nigeria
Introduction
Despite the high technological inclination in the 21st century, especially in the area of health, the rates of maternal mortalities and morbidities are still very high in women worldwide. The occurrence of maternal hypertensive disorders is found to have about 20.7 million women in 2013 and about 10% of pregnancies globally are complicated resulting from pregnancy induced hypertension Sharma, et al. [1]. In the United States, hypertensive disease of pregnancy affects about 8% to 13% of pregnancies Mohan, et al. [2]. Annually, an estimated 2.9 million babies die during the neonatal period and 2.6 million babies are stillborn around the world due to PIH. According to WHO (2018), the rate of stillbirth is 21.9 per 1000 births in women with a pregnancy induced hypertension (PIH) and normotensive women 8.4 per 1000 live births in china Xiong T, et al. [3]. Pregnancy Induced Hypertensions (PIHs) are responsible for 70,000 maternal deaths universally, killing one woman every 11 minutes Magee, et al. [4]. It is the second leading cause of maternal mortality in Bangladesh, according to the Bangladesh Maternal Mortality Survey (2017), about 24 percent of the country’s maternal deaths are caused by pre-eclampsia/eclampsia (PE/E) NIPORT, et al. [5], which affects women during pregnancy, childbirth, as well as postpartum. Factors, such as lack of health care provider capacities to detect, prevent, and manage PE/E, late referrals of HIP clients, late attendance and lack of antenatal care (ANC) and awareness about PE/E among communities have been associated as reasons for most of these preventable deaths Warren, et al. [6]. Deruelle, et al. [7] reported that about 25 percent of women with PIH, especially those with a dangerous condition, experience a decline of end-organ functions during puerperium (the 6 to 8 weeks after delivery, during which pregnancy changes return to baseline). PE early in pregnancy (less 34 weeks of gestation), presenting in a severe form, or persistence of proteinuria more than three to six months after delivery suggests possible chronic hypertension or renal disease. Women with pre-eclampsia are also at increased risk for venous thromboembolism in the postnatal period (after delivery), and those women should receive thromboembolic prophylaxis after delivery until they are fully recovered, usually within four to six weeks RCOG [8]. Similarly, women with preterm pre-eclampsia and gestational hypertension have been found to develop persistent cardiovascular impairment one year after delivery Melchiorre, et al. [9], including other chronic diseases such as chronic hypertension, stroke, renal disease, diabetes mellitus, and ischemic heart disease. Infants born to women with PIH also require special attention in the immediate postnatal period due to a combination of short and long term risks. Standard international guidelines recommend lifelong care and monitoring, or a minimum of care and monitoring for six months to one year after delivery. Studies propose that complications associated with PIH continue in the immediate postnatal period and longer NICE [10]. One of the goals of the United Nations Sustainable Development Goal (SDG) is to reduce the global maternal mortality ratio to less than 70 per 100,000 live births by 2030 United Nations [11]. The SDGs aim to uphold the momentum of the Millennium Development Goals (MDGs), which in its relentless effort catalyzed a global reduction in maternal deaths from approximately 390,000 in 1990 to 275,000 in 2015 Graham, et al. [12] United Nations, 2018). The strains of maternal mortality remain unduly borne by women in less-developed countries, particularly in sub-Saharan Africa (66%, 201,000 deaths) and southern Asia (22%, 66,000 deaths). One of the leading causes of maternal death (and disability) worldwide is pregnancy induced hypertension Payne, et al. [13]. The statistical figures of this problem in less developed countries have varied from 4.0% to 12.3% (Sebastia et al., 2015; Berhe et al., 2018). Pregnancy induced hypertension is also one of the major leading causes of pregnancy associated with morbidity and it is the most recurrent cited cause of maternal death Ethiopian Journal of Health Science [14]. Despite the fact that hypertensive conditions in pregnancy is leading causes of maternal morbidity and mortality during pregnancy, little is known about its magnitude among pregnant women in Kano and, specifically in Kabo Local Government Area. This study therefore aims to fill this gap by considering pregnancyinduced hypertension, the signs, associated risk factors and prevention and management among pregnant woman attending antenatal service in Kabo.
Basic Tools of Scientific Inquiry
The study was guided by the following research questions: 1. What are the signs of pregnancy induced hypertension among women in Kabo Local Government Area of Kano State? 2. What are the risk factors associated with pregnancy induced hypertension among women in Kabo Local Government Area of Kano State? 3. What are the preventions measures of pregnancy induced hypertension in Kabo Local Government Area of Kano State?
Literature Review
Pregnancy Induced Hypertension (PIH) known as toxemia or preeclampsia is a form of high Blood Pressure (BP) in pregnancy. PIH is one developing after 20 weeks of gestation without other signs of preeclampsia. It is a known cause of premature delivery, intrauterine growth restriction (IUGR), placental abruption and fetal death, as well as maternal mortality and morbidity (Gombe et al., 2011). It is characterized by either blood pressure levels of 140/90 mm Hg or higher after 20 weeks of gestation, or a blood pressure rise greater than 30/15mmHg from early or prepregnancy baseline or a rise of mean arterial pressure of more than 105 mmHg. This due to the development of arterial high pressure in a pregnant mother after 20 weeks of gestation, which may or may not have protein in urine and has a blood pressure of or more than 140/90 mmHg (National Guidelines for Quality Obstetrics, 2004). Of all the pregnancy related complications in the world, pre-eclampsia and eclampsia present 10% major causes of maternal and prenatal morbidity and mortality, with pre-eclampsia affecting 5-7 % of all pregnancies, Srinivas, et al. [15]. Hypertensive disorders during pregnancy is among the leading cause of maternal and fetal mortality in obstetric practice that can prevent the baby from getting enough blood and oxygen harming their liver, kidney, brain, and heart, causing end organ damage, Palacios, et al. [16]. Pregnancy induced hypertension is a major cause of maternal morbidity and mortality in the United States. There is an approximately one maternal death due to preeclampsia-eclampsia per 100,000 live births, with a case-fatality rate of 6.4 deaths per 10,000 cases Livington, et al. [17]. The outcome of hypertension in pregnancy is affected by multiple factors. These include gestational age at onset, severity of disease, and the presence of comorbidities like diabetes mellitus, renal disease, thrombophilia, or pre-existing hypertension Heard, et al. [18]. Similarly, a study conducted in Latin America and Caribbean, Pakistan, New York, and Sri Lanka identified null parity, multiple pregnancies, history of chronic hypertension, gestational diabetes, fetal malformation and obesity as the risk factors for developing pregnancy induced hypertension Dolea [19]. Furthermore, life-threatening maternal age (less than 20 or over 40 years), history of PIH in previous pregnancies, preexisting diseases like renal disease, diabetes mellitus, cardiac disease, unrecognized chronic hypertension, positive family history of PIH, which shows genetic susceptibility, psychological stress, alcohol use, rheumatic arthritis, very underweight and overweight, and low level of socioeconomic status are the risk factors for PIH Abeysena, et al. [20]. One important aspect of diagnosing and managing hypertension in pregnancy is presiding out secondary causes. These causes can add to both the maternal, fetal morbidity and mortality. Records from the Nationwide Inpatient Sample (NIS) of hospitalizations for delivery between 1995 and 2008 showed that out the patients with chronic hypertension (1.15% of the sampled population), 11.2% had secondary causes. Secondary hypertension had higher odds of adverse maternal and fetal outcomes when compared to essential hypertension (odds ratio (OR), 11.92 vs 10.18 for preeclampsia, 51.07 vs 13.14 for acute renal failure, 4.36 vs 2.89 for spontaneous delivery < 37 weeks) Bateman, et al. [21]. Examples of secondary forms of hypertension are chronic kidney disease (most common cause), hyperaldosteronism, Reno vascular disease, obstructive sleep apnea, Cushing’s syndrome, pheochromocytoma, thyroid disease, rheumatologic diseases (e.g. scleroderma or mixed connective tissue disease), and coarctation of the aorta; lack of understanding on how to diagnose and treat these conditions during pregnancy may lead to a higher morbidity and mortality Malha [22].
Pregnancy Induced Hypertension in Nigeria
In Nigeria, an incidence of 20.8% of pregnancy induced hypertension had been reported in a study of pregnant women attending antenatal clinics in a Teaching Hospital in South-South Ebeigbe, et al. [23]. Similarly, prevalence rates of hypertensive conditions of pregnancy range from 17% to 34.1% Singh, et al. [24]. In 2009, the occurrence of PIH ranges between 2% to 16.7% Abubakar, et al. [25]. In 2011, Enugu town had 3.3% per 77 cases of PIH out of 2337 cases Ugwu, et al. [26]. In 2014, according to Singh, et al. [27], the prevalence of hypertensive disorders was estimated to be higher than 17% in Nigeria. Akeju, et al. [28] suggested that women have health seeking behaviors, which range from buying over the counter drugs to relieve headache, consulting families on what to do with odema, epigastric pain and blurred vision, consulting a spiritual or traditional healer on convulsing and coming to hospital. All these health-seeking behaviors may delay coming to hospital, worsening the PIH complications. Between the periods of 1990 and 2015, 10.7 million maternal deaths were stated globally, in spite of the fact that maternal mortality ratio had fallen by 44% over these periods. WHO [29]. Out of this total number, developing countries accounts for about 99% of the global deaths in 2015, with Sub-Saharan Africa accounting for bumpily 66%. Study by WHO [29] showed that Nigeria and India are estimated to account for over one third of all maternal deaths globally in 2015, contributing 19% and 15% respectively. Furthermore, the study also revealed that in the West African sub-region, Nigeria with a maternal mortality ratio (MMR) of 814 ranks second, after Sierra Leone 1360 MMR. With this MMR, Nigeria could not meet the MDG5A target in 2015, which aims to reduce maternal mortality ratio by 75% of its 1990 level by 2015.Among the causes of maternal mortality, hypertension ranks second (14%) after hemorrhage Say, et al. [30]. In Nigeria, hypertensive disorders of pregnancy could be a contributory factor to the rising prevalence of hypertension, which has been predicted to escalate up to 39.1 million by 2030, if the current inclination in figures continues Adeloye, et al. [31].
Empirical Review
Studies conducted by Butalia, et al. [32] and Regitz Zagrosek, et al. [33] revealed that there remain terminology and definition disagreements across international guidelines for hypertension. Hypertension itself has been defined over the years by diastolic or systolic readings alone, as well as by changes in pressures throughout pregnancy Chappell, et al. [34]. Similarly, limits for what is considered severe hypertension have been different. Semantics have clinical implications, and systematic reviews often have to compare studies or populations, which are assumed to be the same, rather than standardized Abalos, et al. [35]. Therefore, the International Society of the Study of Hypertension in Pregnancy (ISSHP) identified this as one of the factors for the range of controversies surrounding the treatment of hypertension during pregnancy and appointed a committee to address them beginning in 1998 Brown, et al. [36]. Moreover, studying several international guidelines, definitions are more standardized; however, there are still disagreements in sphygmomanometer intervals that define hypertension, precise definitions of proteinuria, the terms used to characterize blood pressure in the non-severe range, and even terminology used to classify the hypertensive disorders themselves Redman [37,32,33]. All of these reflect that the understanding of hypertensive disorders of pregnancy remains unsolidified and further research is necessary before a universal unanimity is reached on how to treat these disorders. Hypertensive Disorder of Pregnancy (HDP) is defined as high blood pressure during pregnancy, is one of the direct causes of maternal and child mortality AOM [38]. It is measured by blood pressure level greater than 140/90 mm Hg after 20 weeks of gestation. Austere forms of HDP are reflected through blood pressure intensities of 160/100 mm Hg and more NHLBI [39]. Furthermore, studies by Magee, et al. [40] revealed that HDP are responsible for 70,000 maternal deaths globally, killing one woman every 11 minutes. HDP is the second leading cause of maternal mortality in Bangladesh, according to the Bangladesh Maternal Mortality Survey 2017, with approximately 24 percent of the country’s maternal deaths caused by pre-eclampsia/eclampsia (PE/E) NIPORT [5], which affects women during pregnancy, childbirth, as well as postpartum. Factors, such as lack of health care provider capacities to detect, prevent, and manage PE/E, late referrals of HDP clients, late attendance and lack of antenatal care (ANC) and awareness about preeclampsia or eclampsia among communities have been associated as reasons for most of these preventable deaths Warren et al. [6].
Theoretical Framework
This study is anchored on two theories, which include: the Theory of Reasoned Action (TRA) and the Theory of Planned Behavior (TBP). Theory of Reasoned Action was formulated by Martin Fishbein and IcekAjzen towards the end of the 1960s. On the other hand, IcerkAjzen proposed the Theory of Planned Behaviour in 1985; which was an extension from the TRA. The Theory of Reasoned Action and Theory of Behaviour Planned combine two sets of belief variables, which are ‘behavioural attitudes’ and ‘the subjective norms’. The behavioural attitudes are defined as the multiplicative sum of the individual’s relevant likelihood and evaluation related to behavioural beliefs. On the other hand, subjective norms are referent beliefs about what behaviors others expect and the degree to which the individual wants to comply with others’ expectations. The summary of the two theories suggest that a person’s health behavior is determined by their intention to perform a behavior (behavioural intention) is predicated by a person’s attitude toward the behavior, and the subjective norms regarding the behavior. The Theory of Reasoned Action has been criticized because it is said to ignore the social nature of human action Kippax [41]. These behavioural and normative beliefs are derived from individuals’ perceptions of the social world they inhabit, and are hence likely to reflect the ways in which economic or other external factors shape behavioural choices or decisions. In addition, there is a compelling logical case to the effect that the model is inherently biased towards individualistic, rationalistic, interpretations of human behavior. Its focus on subjective perception does not essentially permit it to take meaningful account of social realities. Individuals’ beliefs about such issues are unlikely going to reflect the accurate potential and observable social facts. As such, the Theory of Planned Behaviour updated the Theory of Reasoned Action to include a component of perceived behavioural control, which brings about one’s perceived ability to enact the target behavior. Actually, perceived behavioural control was added to the model to extend its applicability beyond purely volitional behaviours. Previous to this addition, the model was relatively unsuccessful at predicting behaviours that were not mainly under volitional control. Therefore, the Theory of Planned Behaviour proposed that the primary determinants of behaviour are an individual’s Behavioural intention and perceived behavioural control. A constructive use of the TRA and TBP in research and public health intervention programmers might well contribute valuably to understanding issues related to health inequalities and the roles that other environmental factors have in determining health behaviours and outcomes. In spite of the criticism, the general theoretical framework of the TRA and TPB have been widely used in the retrospective analysis of health behaviours and to a lesser extent in predictive investigations and the design of health interventions Hardema, et al. [42]. This is why there is a connection between the study and the theory, since the tenets of the theories are located within the pore of the study.
Methodology
The study was conducted in Kabo Local Government Area of Kano State, Nigeria. It has an area of 341km2 and a population of 153,828 NPC [43]. The study comprises of women within the reproductive ages of 14-45, pregnant and married in Kabo Local Government Area of Kano State. Women were purposively selected for the study not just because of their ability to conceive but they are the ones that do encounter pregnancy induce hypertension. Two nurses were selected from the Cottage Hospital in the local government based on their long working experiences and competencies in the facility. This makes a total sample of twenty one (22) respondents. The study used Interpretative Phenomenological Analysis (IPA). Purposive sampling method was used in selecting the respondents for in-depth interview. Kabo Cottage Hospital was purposively selected, which is bigger compare to other two in the local government with an average of 52Anti-natal Care Attendance (ANC) and 36 live births in the facility monthly. The 22 respondents were interviewed by structural interview method, using tape recorder, note book and biro as data gathering instruments. The respondents were tag with codes like respondent 1, 2, 3, 4 and 5, etc. Based on the in-depth interview method, the data was presented using interpretative analysis.
Findings and Discussion
In attempt to mention the signs of pregnancy induced hypertension, respondent 1 states that: “signs of pregnancy induced hypertension are many, however, she stated the following as part of the signs as follows: chest pain and headache”. Corroborating, respondent 2 put forward the followings as some of the signs: “blurred vision and dizziness,” while respondents 3, 4, 5 and 6 agreed that pedal oedema and epitaxies are also among the signs. Similarly, a study by Haque [44] stated that high blood pressure, headache, blurred vision, swelling in extremities, nausea or vomiting, fatigue and sudden weight gain are among the signs of pregnancy induced hypertension. Furthermore, Magee, et al. [45] noted that the patient with severe PIH should be evaluated for signs of preeclampsia, as generalized edema, including that of the face and hands, rapid weight gain, blurred vision or scotomata (ie, areas of diminished vision in the visual field), throbbing or pounding headaches, epigastric or pain associated with upper quadrant, oliguria (urinary output < 500 mL/d),nausea with or without vomiting, hyperactive reflexes, chest pain, tightness and shortness of breath. Blood pressure should be measured and recorded at every prenatal visit, using the correct-sized cuff, with the patient in a seated position. Leeman [46] said gestational hypertension is a clinical diagnosis confirmed and established by at least two accurate blood pressure tests in the same arm in women without proteinuria, with readings of ≥ 140 mm Hg systolic and ≥ 90 mm Hg diastolic. It should then be determined whether the patient’s hypertension is mild or severe (i.e. blood pressure > 160/110 mm Hg). When asked about the risk factors associated with pregnancy induced hypertension, respondent 1 states that: “parts of the risk factors associated with pregnancy induced hypertension are indefinitely large numerically, nonetheless, she listed the followings as part of the risk factors: “multiple gestations, elderly prim gravida and high parity.” Moreover, respondent 2 stated “polyhydramnios and essential hypertension,” while respondent 3 stated “kidney disease.” All the respondents agreed that high salt intake (in diet), obesity and stress also contribute to the risk factors associated with pregnancy induced hypertension. Bansode [47] also found that some of the factors associated with pregnancy induced hypertension include first pregnancy, new partner/paternity, age <18 years or >35years, black race, obesity (Body Mass Index, BMI ≥ 30), inter-pregnancy interval <2 years or > 10 years and use of selective serotonin reuptake inhibitors (SSRIs) beyond the first trimester; while placental or fetal risk factors include multiple gestation, hydropsfetalis, gestational trophoblastic disease and triploidy. Similarly, Umegbolu [48] reported that the overall incidence of PIH among pregnant women in Enugu State, Southeast Nigeria (2006-2015) was found to be 5.9%. The study identified annual variations in the incidence of PIH (rising and falling trends between 2006 and 2015) among the pregnant women. The incidence of PIH was highest among those women above 35 years (13.5%), compared to those whose age is less than 20 years (9.1%) and those between 20-35 years (5.1%). The occurrence was also higher in the nulliparous (prim gravidae) (7.7%) compared to the multiparous ones (5.5%). Furthermore, Anujeet, et al. [49] stated that hypertension, collagen vascular disease, obesity, black race, insulin resistance, diabetes mellitus, gestational diabetes, increased serum testosterone concentrations and thrombophilia, clotting disorders, and hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome are also responsible risk factors for PIH. Similarly, age and parity are two of the identified maternal risk factors for the development of pregnancy induced hypertension. Extreme ages (age below 20 years and above 35 years) are known to be associated with higher incidence of pregnancy induced hypertension. Like the overall incidence of pregnancy induced hypertension, incidence among various age groups and parity varies from place to place. In Karachi, Rehman, et al. [50] found an incidence of 9% among older women and 27% among prim gravidae. However, Sajith, et al. [51] reported an incidence of pregnancy induced hypertension of 41.3% among 18-22 years old patients in their study. Furthermore, Ahmed, et al. [52] states that educational attainment of women is also a factor that contributes to developing pregnancy induced hypertension. This is because illiterate mothers are more likely to suffer from hypertension during pregnancy than their counter parts. There is every tendency that educated mothers are likely to be aware of pregnancy related complications and its consequences, marry educated husband that facilitate couples discussion on maternal health care utilization, likely to be autonomous in decision making and hence meeting her reproductive needs. Generally, education increases health seeking behaviours of women. The study of Swati, et al. (2014) stated being unmarried as a risk factor and prognosticator of PIH, which is an exceptional result from this study. The study further explains that although marital status is hardly reported as a risk factor in the literature, a possible explanation in a resource poor country like Nigeria could be due to worry about the financial burden of single parenting in environment, which lacks any form of child welfare support. Moreover the stigma of having a child outside marriage is a potential source of concern and anxiety. In addition, Zusterzeel, et al. [53] had emphasized immunological intercourse as the prevention of this maternal-fetal conflict called pregnancy induced hypertension. There is an association of pregnancy-induced hypertension with duration of sexual co-habitation before the first conception. Male ejaculation is said to protect a woman if she has been repeatedly been exposed to it. Regarding the prevention and management of pregnancy induced hypertension, respondent 10 states that “regular antenatal care and regular check-up/ BP checking are sine qua non.” Corroborating, all the respondents agreed that low salt intake, avoiding alcohol, regular intake of water drug therapy for severe hypertension, treatment of underlying medical conditions like kidney problem and avoidance of strenuous exercises or stress are parts of the prevention and management. The findings of the studies are similar with Singh [54] that PIH can be prevented and managed by low salt intake, drinking at least eight glasses of water a day, regular BP check-up, increase the amount of protein-rich foods and decrease the amount of fried and junk foods, regular exercise and enough rest, elevate your feet several times during the day, avoid drinking alcohol and beverages containing caffeine, prescription of drug therapy and additional supplements by a medical doctor. In drug management of pregnancy induced hypertension, ACOG [55] states that labetalol and extended-release nifedipine are first line drugs as they are safe and effective. Similarly, Morgan, et al. [56] emphasized, although beta-blockers other than labetalol are less well investigated, if labetalol cannot be used metoprolol, propranolol, pindolol and acebutolol may be considered. Extendedrelease nifedipine is the most widely used calcium channel blocker. Amlodipine has been used, but the data are limited. Inhibitors of the Renin Aangiotensin Aaldosterone System (RAAS) are totally contraindicated. This includes angiotensin converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs) and direct renin inhibitors. The package insert of these agents comes with a black box warning stating that usage during the second and third trimesters can cause injury and death to the developing fetus; therefore, discontinuation is indicated as soon as pregnancy is detected. RAAS inhibitors use in the second and third trimesters is associated with renal agenesis, pulmonary hypoplasia and intrauterine growth retardation, IUGR. The proof of fetal injury during first trimester exposure is unclear. Post-delivery lactating mothers may use enalapril, captopril or quinapril because they have low concentration in breast milk; labetalol may be continued only in lactating mothers Colaceci [57]. In addition, Donovan [58] says the choice of antihypertensive drugs to be used depends on whether breastfeeding is tried or attempted. When the woman desires to breastfeed, deliberation must be given to potential transfer of the drug into breast milk. This is due to the established evidence that most drugs safely used in pregnancy are excreted in low amounts into breast milk and are compatible with breastfeeding. (Table 1) shows antihypertensive drugs of those to use and those to avoid during lactation.
Table 1: Relatively Safe Antihypertensive Drugs in Pregnancy.
In an instance when there is no desire to breastfeed and adequate contraception is used, the choice of antihypertensive drug is the same as for any other non-pregnant woman or patient. While (Table 2) shows the antihypertensive drugs used in pre-eclampsia, which are the same as those used to treat chronic and PIH Lowe et al. [59-61].
Table 2: Antihypertensive Drugs during Breastfeeding. Source: Donovan [58]
Conclusion
The strains of maternal mortality remain unduly borne by women in less-developed countries, particularly in sub-Saharan Africa. Between the periods of 1990 and 2015, 10.7 million maternal deaths were stated globally, in spite of the fact that maternal mortality ratio had fallen by 44% over these periods. Out of these total numbers, developing countries account for about 99% of the global deaths in 2015, with Sub-Saharan Africa accounting for bumpily 66% with 201,000 deaths. PIHs are responsible for 70,000 maternal deaths universally, killing one woman every 11 minutes. Nigeria, in 2014, recorded the prevalence of pregnancy induced hypertension and was estimated to be about 20.8% among pregnant women attending antenatal clinics in Teaching Hospitals in South-South. Based on these problems, the findings of this study attest that the signs of pregnancy induced hypertension in Kabo Local Government include chest pain, headache, blurred vision, dizziness, pedal oedema and epitaxies. Finally, the risk factors are multiple gestations, elderly prim gravida, high parity, polyhydramnios, essential hypertension, kidney disease, high salt intake (in diet), obesity and stress.
Recommendations
The study recommends the following, based on the finding of the study: 1. The study recommends that pregnant women in Kabo Local Government should visit the hospital regularly; especially to check their blood pressure. 2. The women in Kabo Local Government should be educated about the signs of pregnancy induced hypertension. This will help them to know how to seek for medical services early. 3. Finally, women in Kabo Local Government should be educated on factors that will assist them to stay healthy and avoid pregnancy induced hypertension.
Morus rubra Linn (MR), generally known as red mulberry belong to the Moraceae, mulberry family. It is originated from the eastern part of the United States of America and is now universally cultivated and naturalized in the areas of China, Korea and Japan. Edible fruits that are reddishly maturing to dark purple or black in colour. The fruits are soft, juicy and aggregate with a sweet taste and a hint of sourness, which is more evident in the less mature fruits. In addition, red mulberry sap was used by several tribes to treat ringworm while the stem bark is used as purgative and vermifuge. The fruits have also been utilized to treat diabetes, hypertension, anaemia and arthritis in traditional medicine, particularly in Chinese medicine [1] (Figures 1-4). It is also demonstrated that Morus rubra (MR) fruit leads to control over hyperglycaemia and may be a good antimicrobial agent against gram negative bacterial infections. The first documented use of mulberry fruits was described in the mid-1500s by De Soto expedition, who discovered consuming these dried fruits [2]. Diabetes is a heterogeneous disease affecting almost 6% of the world population. It is characterized by hyperglycemia and insulin resistance or a combination of both of these factors.
Figure 1: Morus rubra tree.
Figure 2: Morus rubra fruit.
Figure 3: Fruits of Morus rubra.
Figure 4: Leaves and flowers of Morus rubra.
Table 1: Taxonomical Classification of Morus rubra L. (Miljkovic et al., 2014).
The treatment of diabetes with allopathic drugs causes moderate to severe adverse events. Hence, the alternative systems of medicine from plant and marine sources are being explored to treat diseases [3] (Tables 1-4). Fully ripened mulberry fruit has a delicious, mouth-watering taste with a pleasant aroma and flavor. It is valued for both direct consumption and the creation of value-added products. Mulberry fruits are known for their nutritional value, which makes them beneficial to human health. Principal sugars present in mulberry are fructose and glucose, which increase with ripening [4,5]. Whereas the primary fatty acid that found in the mulberry fruit are oleic acid, palmitic acid and linolenic acid [6,7]. Citric acid, tartaric acid, malic acid, succinic acid and fumaric acid are among the organic acids found in mulberry fruits; nonetheless, malic acid is the most abundant organic acid present. Mulberry is also high in a number of essential minerals including calcium, phosphorus, potassium, magnesium and sodium.
Table 2: Vernacular Names of Morus rubra L. (Lim, 2012).
Table 3: Organoleptic Characteristics of Red Mulberry (MR).
Table 4: Red Mulberry (MR) with Pharmacological Actions. (Elbaz, et al. [10,12-14]) (Thabti et al., 2020) (Wei et al., 2018).
Materials and Methods
The raw material was collected and purchased from a loca Indian market. sun dried at a temperature of 30˚C under the shade for several days to eliminate the excessive moisture content. The dried sample was preserved in a dry container with low humidity conditions to prevent the absorption of the moisture by the dried sample. The dried sample was ground into powder grinding machine. The extraction process started by placing the dried sample and solvent together in a vessel or extraction instrument. The extractions of MR were carried out with ethanolic Soxhlet extraction and maceration.
The cultures were used for the antibacterial assay. These cultures were obtained from microbial culture bank of Faculty of Pharmacy (FOP), Aimst University. a) Escherichia coli (E. coli) ATCC 8739. b) Staphylococcus aureus (S. aureus) ATCC 29737. c) Bacillus subtilis (B. subtilis) ATCC 6633. d) Salmonella typhi (S. typhi) ATCC 19430.
Maceration Extraction
510gm of mulberry ground fruits were weighed and soaked in 1 L of 95% ethanol. The conical flask was kept at dark, in the cupboard for 9 days and swirling was done on daily basis throughout the maceration process. After 9 days, the maceration process was completed and the mixture was filtered by using muslin cloth. The volume of maceration extract collected from this process was 850 ml. The maceration extract was evaporated using rotary evaporator (Rotary evaporated R-210 BUCHI, Corporation) at 75°C and the speed of the rotator was set to 100 rpm. The final volume of maceration semi solid product collected from this process was 300 ml.
Soxhlet Extraction
450 gm of fruits ground powder were weighed and 1L ml of 95 % ethanol was poured into the soxhlet flask. The heating mantle was kept at 80 ºC. The duration for this Soxhlet extraction process to be completed was about 17hours. Decolorization of purple colour of the fruits was observed. The total volume of Soxhlet extract collected from this process was 350 ml. The extract was evaporated using rotary evaporator at 75°C and the speed of the rotator was set to 100 rpm. The extract was evaporated using rotary evaporator (Rotary evaporated R-210 BUCHI, Corporation) at 75°C and the speed of the rotator was set to 100 rpm. The final volume of product collected from this process was 250 ml. Figures 5 & 6 shows the evaporated extracts for maceration and hot extraction respectively.
Figure 5: Final maceration product semi-solid form.
Phytochemical Analysis
Phytochemical tests were carried out to identify the presence of carbohydrates, monosaccharides, polysaccharide, reducing sugar, pentose sugar, hexose sugar, galactose, protein, amino acid, free fatty acid, saturated fatty acid, neutral lipid, volatile oil, steroid, terpenoid, glycoside (anthraquinones glycoside, cardiac glycoside, cyanogenic glycoside, coumarin glycoside, saponin glycoside), alkaloid, flavonoid, phenol and tannin. The total phenolic content of MR using 50 and 200μg/ml solution was determined by Folin– Ciocalteu reagent method using gallic acid as standard [8].
Antioxidant Assay
Antioxidant activity of ethanolic extract of MR is studied using DPPH method. The DPPH is a stable free-radical which has a colour of purple, as the antioxidants react with the DPPH, the DPPH will be converted into non-radical DPPH-H form. Besides that, the colour of the DPPH will be decolorized from purple to light yellow colour. The degree of decolorization indicates the potency of the plant extracts in scavenging the free radicals. 0.1M of methanolic DPPH was freshly prepared by dissolving 3.94mg of DPPH crystalline powder in 100ml of methanol and kept in a clean beaker. Extracts (0.2 ml) at different concentrations (50–1000 μg/ml) was mixed with 0.8 ml of tris hydrochloric acid (HCl) buffer (100 mM; pH 7.4). One millilitre DPPH (500 mM in 1.0 ml ethanol or methanol) solution was added to the mixture. The mixture was shaken vigorously and incubated for 30 min at room temperature. The absorbance of the resulting solution was measured spectrophotometrically at 518 nm (Model UV 1800, Shimadzu, Japan). BHT is used a standard. All the determinations were carried out in triplicate. The following formula was used for the antioxidant activity determination [9]. DPPH Radical Scavenging Activity (%) = 𝐴𝑐𝑜𝑛𝑡𝑟𝑜𝑙−𝐴𝑠𝑎𝑚𝑝𝑙𝑒𝐴𝑐𝑜𝑛𝑡𝑟𝑜𝑙 𝑥 100.
Antibacterial Assay
The 10 mg/ml stock solution of ethanolic extract of MR is prepared using 0.5% DMSO (prepared using distilled water). The antimicrobial activity of ethanolic extract of MR against four pathogenic microorganisms (namely Escherichia coli [ATCC 8739], Staphylococcus aureus [ATCC 29737], Bacillus subtilis [ATCC 6633], Salmonella typhi [ATCC 19430]) was carried out. Using stock, the primary culture was prepared and used for preparation of sub-cultures of microorganism. The antibacterial activity was tested by agar well diffusion method. E. coli, S. aureus, B subtilis and S. typhi were spread onto the surface of nutrient agar with sterile swab (0.1 ml containg106 cell/ml). Six mm diameter wells were punched into the agar and filled with 0.1ml of the ethanolic extract or standards (penicillin and ciprofloxacin). Then incubated at 37ᵒC for 24 hours. After 24 hours, zone of inhibition were measured. All experiments were carried out in triplicates.
Minimum Inhibitory Concentration (MIC) is determined by using the broth dilution method. Serial dilution was made between 1000 mg/ml and 62.5 mg/ml. Mueller- Hinton (MH) broth was prepared and 1ml was added into test tubes alongside 100μl of selected ATCC strains. Then, 1ml of extracts with the concentrations mentioned above were introduced into the test tubes contained the broth and ATCC strain and mixed for even distribution. These test tubes were then incubated for 36 hrs at 37°C. As a positive control, 1 ml of selected antibiotics was added to the test tube while the negative control only contained selected ATCC strains [10]. The results obtained after incubation were compared to both the positive and negative control. The concentration of the extract that gave clear results (absence of turbidity) was considered as the MIC of the extract. The Minimum Bactericidal Concentration (MBC) was determined as the lowest concentration of extract that killed at least 99% of the initial bacterial number [11].
Antidiabetic Activity
Healthy, adult, Sprague-Dawley (SD) rats (180 ± 20 g) were used for the studies. The animals were obtained from Central animal house, AIMST University, Malaysia. Approval from the AIMST University Human and Animals Ethics Committee was obtained. The animals were housed in large, spacious polyacrylic cages at ambient room temperature with 12 h light/12 h dark cycle. A minimum of 5 days of acclimatization period was allowed before the animals are used in the experiment. The animals were fed with water and normal rodent pellet diet ad libitum. Diabetes mellitus will be induced in overnight-fasted rats by administration of single intraperitoneal (I.P.) injection of freshly prepared streptozotocin (STZ) with a dose of 60 mg/kg/mL [12]. To prevent the STZ-induced hypoglycaemia, rats administered with 10% dextrose solution after 24 h of STZ administration for next 24 h. Induction of diabetes was verified after 72 h by measuring blood glucose level with strips using glucometer and the animals allowed 14 days for the stabilization of blood glucose level [13]. On day 14, animals having a blood glucose level higher than 220 mg/dL were considered diabetic and included in the experiments. Diabetic animals were randomly divided into five groups (Group II–VI) as follows: Group I: Normal control Group II: Diabetic control Group III: Diabetic animals treated with glibenclamide (20 mg/ kg/P.O.) Group IV: Diabetic animals treated with ethanolic extract of MR (100 mg/kg/P.O.) Group V: Diabetic animals treated with ethanolic extract of MR (200 mg/kg/P.O.) Group I (normal control) and group II (diabetic control) rats were given 0.5% w/v carboxymethylcellulose (CMC) while the rats in group III treated with 20mg/kg body weight (BW) of glibenclamide and rats in group IV-V were administered with ethanolic extract of MR of 100mg and 200mg per kg. The standard and test drugs were suspended in 0.5% w/v CMC and administered once daily through oral gavage for 28 consecutive days. Throughout the study, variations in experiment animals’ body weight will be monitored at regular intervals. At the end of the study, the blood samples withdrawn from all the experimental rats through retroorbital plexus puncture. The serum was separated from the blood sample and used for biochemical analysis.
Statistical Analysis
The value in the antidiabetic activity was expressed as mean ± Standard Error of the Mean (SEM). The data was analysed using one-way analysis of variance (ANOVA), followed by Tukey’s posthoc test. P < 0.05 will be considered as statistically significant.
Results
Phytochemical analysis showed the presence of carbohydrates, monosaccharides, reducing sugar, hexose sugar, galactose, protein, amino acid, neutral lipid, terpenoid, glycoside, anthraquinones glycoside, coumarin glycoside, alkaloid, flavonoid, phenol and tannin. The phytochemical screening is shown in Tables 5 & 6. The total phenolic content found was 6.420 mg GAE/g and 6.097 mg GAE/g for the concentrations of 50 and 200µg/ml respectively. Antioxidant activity of ethanolic extract of MR is studied using DPPH method and BHT was used as standard. In DPPH radical scavenging method, BHT and MR extract showed 50% inhibition (IC50) at 84.04µg/ml and 182.82µg/ml, respectively. The antibacterial activity of ethanolic extract of MR was tested by using the E. coli, S. aureus, S. typhi, and B. subtilis. The extract concentrations used in the agar well diffusion method were 0.1, 0.2, 0.4, 0.6, 0.8 and 1.0 mg/ml, other than that, 5mg/ml of penicillin and ciprofloxacin was playing the role as a standard in this study. In the present study, there was no zone of inhibition observed in all concentrations of ethanolic MR extract. The microorganism used were all in active condition, this can be proven as the ciprofloxacin as well as penicillin showed a clear zone of inhibition.
In antimicrobial screening, ethanolic extract of MR exhibited antibacterial activity against E. coli with equivalent MIC and MBC identified at the concentration of 500 mg/ml, 250 mg/ml and 125 mg/ml and did not inhibit S. aureus. Anti-hyperglycaemic activity of ethanolic extract of MR was studied using STZ-induced diabetic rats. The diabetic animals were showed decreases in body weight but the results were not significant. The diabetic rats showed significant increases in the levels of glucose throughout the study when compared with that of control animals. Whereas the diabetic animals treated with glibenclamide or ethanolic extract of MR (100/ 200 mg/kg) showed significant decreases in the glucose levels when compare with that of diabetic control animals.
Antimicrobial Screening
The antimicrobial activity of Morus Rubra (MR) ethanolic Soxhlet fruit extract was analyzed against the gram negative bacteria Escherichia coli and gram positive bacteria Staphylococcus aureus at 4 different concentrations: 500 mg/ml, 250 mg/ml, 125 mg/ml and 62.5 mg/ml. It was expressed by identifying the MIC and MBC of fruit extract through the broth tube dilution method. The obtained result from the MIC test showed that turbidity was observed in all the assay tubes that tested against the S. aureus. Therefore, three tubes with the least turbidity were selected and subjected for MBC.
Preparation of Tryptic Soy Agar Plate
Tryptic soy broth or trypticase soy broth (frequently abbreviated as TSB) is used as a culture broth to grow aerobic bacteria. It is a complex, general purpose medium that is routinely used to grow certain pathogenic bacteria, which tend to have high nutritional requirements (i.e., they are fastidious). Its agar counterpart is Tryptic Soy Agar (TSA). One of the components of Tryptic soy broth is Phytoene which is an enzymatic digest of soybean meal). TSB is frequently used in commercial diagnostics in conjunction with the additive sodium thioglycolate which promotes growth of anaerobes. Tryptic Soy Agar was only applied for the Bacillus subtilis out of the 4 chosen bacterial strains. 20g of tryptic soy agar powder was weighed and transferred into 500ml of distilled water. The conical flask was subjected to sterilization with the use of autoclave for 2 hours at the temperature of 121˚C. In the biosafety cabinet, the freshly prepared sterilized tryptic soy agar was poured into the sterilized Petri plates. The inoculation loop was used to eliminate the bubble formed on the surface of the tryptic soy agar before solidification occurs. Approximately, 25ml of the tryptic soy agar was poured into the sterilized Petri plates, these plates were allowed to cool down and solidified in the biosafety cabinet. These plates were incubated in an upside-down position at the temperature of 37˚C and were taken out during the agar well diffusion test.
Agar Well Diffusion
Before the initiation of the agar well diffusion test, the biosafety cabinet was sterilized with 70% alcohol and the UV light was switched on for 10 minutes. Apart from that, the plant extract dilutions, antibiotic dilutions with the concentration of 5mg/ml (Penicillin and Ciprofloxacin), bacteria strains, bacteriological loop, sterilized cork borer, sterilized micropipette tips and micropipette (p100), Bunsen burner and nutrient agar plate were prepared in prior of the test. After switched off the UV light and placement of all materials in the biosafety cabinet, gloves were worn and 70% alcohol was applied properly to sanitize the gloves to prevent contamination occurs. NA/TSA (nutrient agar/tryptic soy agar), date, name, bacterial strain, ATCC code and antibiotics were labelled accordingly at the bottom side of the plates. 0.1 ml of broth that contained bacterial strain was pipetted into the Petri plates with the use of a micropipette. The sterilized glass spreader was used to spread the bacterial strains evenly on the plate. After every spreading, the glass spreader should be sanitized with 70% alcohol and showed to the flame.
Then the sterilized cork borer was used to make wells on the agar plate. There were 4 wells punched in one Petri plate, each well was separated from each other in equal distance. The plates were prepared in a triplicate manner for the comparison purpose, as well as the positive and negative plates. The cork borer was sterilized every time after use. The agar which was fitted inside the cork borer after punching the wells was discarded. The different concentrations of plant extract as well as different antibiotics were added into the wells by using a micropipette. The wells were filled until 60% of the height of the wells. The micropipette tips were discarded after each concentration of plant extract and antibiotics was performed. This can prevent an alteration of the concentration of plant extract and antibiotics. The Petri plates were then incubated in an incubator at the temperature of 37˚C for 24 hours. The zone of inhibition of the plates was observed and recorded.
Minimum Inhibitory Concentration (MIC)
5 loops of the bacterial strains were cultured in each sterile nutrient broth and then incubated at 37 ͦ C for 24 hours, centrifuged at 5000 rpm for 10 minutes.
Preparation of Standard McFarland Bacterial Culture: The nutrient broth as well as tryptic soy broths were prepared freshly. These broths were sterilized for 2 hours at the temperature of 121˚C and were allowed to cool down. In the biosafety cabinet, 5 loop full of Bacillus subtilis bacteria colonies were inoculated into the tryptic soy broth. This step was repeated for the other three bacteria which were inoculated in the nutrient broth. These broths were incubated for 24 hours at the temperature of 37˚C in an incubator. Then, these broths that contained bacteria strains were centrifuged at 5000rpm for 10 minutes. The supernatant was discarded and the cell pellet formed was collected and re-suspended in the sterile nutrient broth and tryptic soy broth. By using the UV spectrophotometer, the seeded broths were standardized to the value 0.5 of the absorbance according to McFarland standard at the wavelength of 517nm.
Preparation of Sample: The extracts were obtained from the Soxhlet extraction method using 95% ethanol. 4 different concentrations of the extracts were prepared at 25, 50, 100, 200μg/ml. 2 mg of extracts was dissolved in 10ml of ethanol, forming a stock solution with a concentration of 200μg/ml. Then it was double-diluted by mixing 2ml of the stock solution and 2ml of ethanol to obtain the concentration of 100μg/ml. The same procedure was repeated and obtained 50μg/ml in concentration. Next, 1ml of stock solution was taken and mixed with 2ml of ethanol to obtain a concentration of 25μg/ml. 4 test tubes were prepared and 0.2ml of the sample solution were taken and transferred into the test tube prepared. 4ml of 2.5% sodium carbonate and 0.2ml of Folin-Ciocalteu reagent was added to each of the test tubes. The test tubes were allowed to sit for 2 hours. The absorbance of the standard solution was examined by 750nm UV spectrophotometry and was recorded.
Preparation of Blank: 0.2ml of Folin-Ciocalteu reagent, 4ml of 2.5% sodium carbonate and 0.2ml of ethanol were added into the test tube and it was allowed to sit for 2 hours. The absorbance of the standard solution was examined by 750nm UV spectrophotometry. The values of absorbance of standard and sample obtained were then utilized in plotting the graph of UV absorbance against the concentration of sample and standard.
Serial Dilution of Minimum Inhibitory Concentration (MIC) Assay
Before starting the MIC assay, the biosafety cabinet was sanitized with 70% alcohol and the UV light was switched on for 10 minutes. 2.5 g of plant extract was measured using an analytical balance and mixed with 25ml of 0.5% DMSO (dimethyl sulphoxide), forming the stock solution with a concentration of 10mg/ml. The mixtures with the concentration of 50, 25, 12.5, 6.25, 3.125, 1.5625 mg/ml were formed upon two-fold serial dilution. 2 ml of the stock solution and 2ml of the standard McFarland seeded broth were taken by using a micropipette and mixed in the sterilized test tube, thus obtained a concentration of 50mg/ml. 2 ml of the stock solution and 2ml from the first test tube were taken by using a micropipette and mixed in the sterilized test tube, thus obtained a concentration of 25mg/ ml. 2 ml of the stock solution and 2ml from the second test tube were taken by using a micropipette and mixed in the sterilized test tube, thus obtained a concentration of 12.5mg/ml. 2 ml of the stock solution and 2ml from the third test tube were taken by using a micropipette and mixed in the sterilized test tube, thus obtained a concentration of 6.25mg/ml. 2 ml of the stock solution and 2ml from the fourth test tube were taken by using a micropipette and mixed in the sterilized test tube, thus obtained a concentration of 3.125mg/ml. 2 ml of the stock solution and 2ml from the fifth test tube were taken by using a micropipette and mixed in the sterilized test tubes.
2ml of the mixture was pipetted and discarded, thus obtained a concentration of 1.5625mg/ml. The positive tube that contained seeded broth and the negative tube that contained sterile nutrient or tryptic soy broth were prepared accordingly. The micropipette tips were discarded after finished transferring each set of test tubes. These tubes were fitted with cotton wool and covered with double-folded aluminium foil the tubes were incubated for 24 hours at the temperature of 37˚C. The turbidity of each of the tubes were observed and recorded. In contrast, the extract that tested against the E. coli showed clear solution at concentration of 500 mg/ml, 250 mg/ml and 125 mg/ml. This indicated that ethanolic Soxhlet extract of Morus rubra did not exhibit antibacterial action against E. coli at these concentrations. Hence, these three assay tubes were subculture on fresh sterilized nutrient agar plates to find out the MBC of the fruit extract on E. coli. From the MBC analysis, the nutrient agar plates for the S. aureus showed the bacterial growth revealed that the ethanolic fruit extract had bacteriostatic or bactericidal effect against S. Aureus. However, positive results were obtained for the E. coli in which there is no observed bacterial growth on all three nutrient agar plates. Therefore, the fruit extract possessed equivalent MIC and MBC on E. coli, ranged from 125 mg/ ml to 500 mg/ml. These results suggested that ethanolic Morus rubra extract was more susceptible to the gram positive bacteria than gram negative bacteria. The antibacterial properties of the red mulberry may be due to the presence of phenolic compounds in abundance such as flavonoid. At a low concentration, the phenols were acted as bacteriostatic and at a high concentration, phenols may act as bactericidal. The results are shown in Table 7. MCB results are laid down.
Antioxidant screening
The MR were cleanly washed and air-dried at room temperature for 1 week to prevent deterioration. MR were passed through a sieve 1.40 mm to remove the unwanted impurities and then pulverized into powder form using the mortar and pestle. The extraction of the seeds was carried out using ethanol as an extracting solvent. The Soxhlet extraction method was employed to extract the chemical constituents in the MR. 19.38 gm of the MR powder was inserted into a thimble 300 ml of ethanol was measured accurately and added into the round bottom flask. The running of tap water has remained until the whole apparatus cools down. The MR extract contained in the round bottom flask was poured into a cleaned and dried conical flask (1000 ml). The conical flask was covered with cotton wool and aluminium foil to prevent evaporation. The ethanolic extract of MR was evaporated by using the rotary evaporator. The temperature of the rotary evaporator was set at 80˚C. The process was continued until no notable changes were observed. The MR extract was poured into a clean beaker. The collected pure extract was introduced into a China dish and placed on the hot water bath for further evaporation.
Determination of total Phenolic Content Preparation of Standard
Gallic acid was used as a standard in this assay and compared with the sample to identify the presence of phenolic compounds in the plant extract. Five different concentrations of Gallic acid were prepared at 1, 2, 4, 6, 8 and 10μg/ml. The stock solution was prepared by dissolving 10mg of Gallic acid in 10ml of 95 % ethanol. Then, 1ml of the solution was diluted with 9ml of ethanol to obtain a concentration of 100μg/ml. The same procedure was repeated until the final concentration of 1μg/ml was obtained. From the stock solution, 1.0, 0.8, 0.6, 0.4, 0.2, 0.1ml were pipetted into 6 different tubes and labelled accordingly. The volume was then made up to 10ml with 95% ethanol. Another 6 clean tubes were prepared. 0.2ml of the standard solution were taken and transferred into the test tube prepared. 4 ml of 2.5% sodium carbonate and 0.2ml of Folin-Ciocalteu reagent was added to each of the test tubes. The test tubes were allowed to sit for 2 hours. The absorbance of the standard solution was examined by 750nm UV spectrophotometry and was recorded.
Preparation of Sample: Four different concentrations of the extracts were prepared at 25, 50, 100, 200μg/ml. 2 mg of extracts was dissolved in 10ml of ethanol, forming a stock solution with a concentration of 200μg/ml. Then it was double-diluted by mixing 2ml of the stock solution and 2ml of ethanol to obtain the concentration of 100μg/ml. The same procedure was repeated and obtained 50μg/ml in concentration. Next, 1ml of stock solution was taken and mixed with 2ml of ethanol to obtain a concentration of 25μg/ml. 4 test tubes were prepared and 0.2ml of the sample solution were taken and transferred into the test tube prepared. 4ml of 2.5% sodium carbonate and 0.2ml of Folin-Ciocalteu reagent was added to each of the test tubes. The test tubes were allowed to sit for 2 hours. The absorbance of the standard solution was examined by 750nm UV spectrophotometry and was recorded.
Preparation of Blank: 0.2ml of Folin-Ciocalteu reagent, 4ml of 2.5% sodium carbonate and 0.2ml of ethanol were added into the test tube and it was allowed to sit for 2 hours. The absorbance of the standard solution was examined by 750nm UV spectrophotometry. The values of absorbance of standard and sample obtained were then utilized in plotting the graph of UV absorbance against the concentration of sample and standard.
Preparation of DPPH Solution: 0.1mM of methanolic DPPH was freshly prepared by dissolving 3.94mg of DPPH crystalline powder in 100ml of methanol and kept in a clean beaker. The beaker was covered with aluminium foil to prevent oxidation.
Preparation of Standard: BHT was used as a standard in this assay. Six different concentrations of BHT solutions were prepared at 10, 20, 40, 60, 80 and 100μg/ml. The stock solution was first prepared by dissolving 10mg of BHT in 10ml of methanol. 1ml of the solution was then diluted ten-fold with 9ml of methanol to obtain a concentration of 100μg/ml. From the stock solution, 10, 8, 6, 4, 2, 1ml were pipetted into 6 different test tubes and made up to 10ml with methanol. Then, 3ml of 0.1mM DPPH reagent was added to 2.5ml of different concentrations of methanolic extracts. The mixtures were shaken and labelled accordingly. The test tubes were allowed to keep in the dark for 30 minutes. The absorbance was measured at 518nm using a UV spectrophotometer.
Preparation of Sample: The steps in preparation of DPPH solution were repeated in the preparation of the sample, in which the BHT was changed to the plant extract. The absorbance was measured at 518nm using a UV spectrophotometer.
Preparation of Blank: The blank solution was prepared by mixing 3ml of 0.1mM DPPH reagent and 2.5ml of methanol, the solution was allowed to stand in the dark for 30 minutes. The absorbance was measured at 518nm using a UV spectrophotometer. The values of absorbance of standard and sample obtained were then utilized in plotting the graph of UV absorbance against concentration of the sample and standard.
Antibacterial Assay
Sterility Test of Ethanolic MR Extract
Before the initiation of phytochemical screening, antibacterial and antioxidant assay of MR extract. The extract was streaked on nutrient agar and was incubated for 24 hours at the temperature of 37˚C. Due to the movement control order in Malaysia, the plant extract was kept in the fridge for about 3 months, therefore the growth promotion test is able to determine whether microbes were present in the plant extract. This enables us to ensure positive results for all tests, especially antibacterial assay. There was no bacterial growth observed after 24 hours of incubation.
Serial Dilution of Extract: Before the dilution of plant extract, the 0.5% DMSO was prepared by measured 0.5ml of DMSO and mixed with 99.5ml of sterilized distilled water. 400mg of plant extract was weighed with the use of analytical balance and it was transferred to a clean beaker that contained 40ml of 0.5% DMSO. This gave rise to the formation of a stock solution with a concentration of 10mg/ml. Next, the beaker was subjected to sonication to ensure complete mixing of the two different liquid. From the stock solution, 10, 8, 6, 4, 2, 1ml were pipetted into 6 different sterilized universal tubes and were labelled accordingly. The volume was then made up to 10ml with 0.5% DMSO. The universal tubes were tightly screwed and kept in the refrigerator for storage.
Preparation of Bacterial Strains: 1.95g of nutrient broth powder and 1.5g of tryptic soy broth powder were weighed accurately using an analytical balance and transferred into 4 different conical flasks (100ml). These conical flasks were labelled accordingly.
Preparation of Nutrient Agar Plate: 11.2g of nutrient agar powder was weighed 3 times and transferred into 3 conical flasks (1000ml). 400ml of distilled water was measured accurately and poured into each of the flasks. After putting magnetic beads into 3 of the conical flasks, these conical flasks were placed on the magnetic stirrer to facilitate the dissolving process. The mouth of the conical flasks was fitted with cotton wool and covered with double-folded aluminium foil. The conical flasks were subjected to sterilization with the use of autoclave for 2 hours at the temperature of 121˚C. In the biosafety cabinet, the freshly prepared sterilized nutrient agar was poured into the sterilized Petri plates. The inoculation loop was used to eliminate the bubble formed on the surface of the nutrient agar before solidification occurs. Approximately, 25ml of the nutrient agar was poured into the sterilized Petri plates, these plates were allowed to cool down and solidified in the biosafety cabinet. These plates were incubated in an upside-down position at the temperature of 37˚C and were taken out during the agar well diffusion test.
Preparation of Tryptic Soy Agar Plate: Tryptic soy broth or Trypticase soy broth (frequently abbreviated as TSB) is used as a culture broth to grow aerobic bacteria. It is a complex, general purpose medium that is routinely used to grow certain pathogenic bacteria, which tend to have high nutritional requirements (i.e., they are fastidious). Its agar counterpart is tryptic soy agar (TSA). One of the components of Tryptic soy broth is Phytoene which is an enzymatic digest of soybean meal). TSB is frequently used in commercial diagnostics in conjunction with the additive sodium thioglycolate which promotes growth of anaerobes. Tryptic Soy Agar was only applied for the Bacillus subtilis out of the 4 chosen bacterial strains. 20g of tryptic soy agar powder was weighed by using an analytical balance and transferred into a 1000ml conical flask.
500ml of distilled water was poured into the conical flask and labelled accordingly. After putting the magnetic bead into the conical flask, the conical flask was placed on the magnetic stirrer to facilitate the dissolving process. The mouth of the conical flask was fitted with cotton wool and covered with double-folded aluminium foil. The conical flask was subjected to sterilization with the use of autoclave for 2 hours at the temperature of 121˚C. In the biosafety cabinet, the freshly prepared sterilized tryptic soy agar was poured into the sterilized Petri plates. The inoculation loop was used to eliminate the bubble formed on the surface of the tryptic soy agar before solidification occurs. Approximately, 25ml of the tryptic soy agar was poured into the sterilized Petri plates, these plates were allowed to cool down and solidified in the biosafety cabinet. These plates were incubated in an upside-down position at the temperature of 37˚C and were taken out during the agar well diffusion test.
Phytochemical Screening of Ethanolic MR Extract: The MR was extracted with 95% ethanol, and the plant extract was undergone phytochemical screening. In the present study, the results obtained for the phytochemical screening of MR ethanolic extract was analysed and it was found out that alkaloids, anthraquinone, carbohydrate and flavonoids were present in the sample. The alkaloid content was tested with Mayer’s and Wagner’s reagent. Mayer’s reagent is an alkaloidal precipitating reagent which its function is to determine the presence of alkaloids in natural products. Most alkaloids will be precipitated in a neutral or slightly acidic solution owing to Mayer’s reagent. Cream colour precipitate will be obtained upon observation. The ethanolic extract of MR showed positive results for both Mayer’s and Wagner’s tests, which indicates the MR contained alkaloids component.
Antioxidant Assay
Determination of Total Phenolic Content (TPC): In this research, the antioxidant potential of the MR was determined by using DPPH free radicals scavenging method and BHT was used as a standard. The DPPH is a stable free-radical which has a colour of purple, as the antioxidants react with the DPPH, the DPPH will be converted into nonradical DPPH-H form. Besides that, the colour of the DPPH will be decolorized from purple to light yellow colour. The degree of decolorization indicates the potency of the plant extracts in scavenging the free radicals.
Subsequently, the plant extract was prepared in the concentration of 10, 20, 40, 60 , 80 and 100 μg/ml and mixed with the DPPH, the absorbance was determined at 518nm after kept the tubes in the dark for 30 minutes. Phenolic compounds are very essential plant constituents which responsible for the antioxidant activity due to its redox properties. As a basis, Folin-Ciocalteu reagent was used to measure the phenolic content of different concentrations of plant extract. In this test, the Gallic acid was used as a standard and the total phenolic content was calculated by using the formula C = (A/B) x dilution factor. The results were derived from the calibration curve of Gallic acid, it was expressed as Gallic acid equivalents (GAE) per gram of samples. In the present study, the total phenolic content found was 6.420 mg GAE/g and 6.097 mg GAE/g for the concentrations of 50 and 200μg/ml respectively. The following formula was used for the antioxidant activity determination.
The concentration and absorbance of Gallic acid determined by U.V and concentration of MR ethanolic absorbance is shown in Table 8 and Graph 1 is drawn, respectively. The concentration, absorbance and the corresponding percentage of scavenging of BHT for DPPH Free Radical Scavenging Assay is shown in Table 9. The concentration, absorbance and the corresponding percentage of scavenging of ethanolic MR extract is placed Table 10 while Graph of percentage scavenging against the standard concentration is drawn in Graph 2. Table 11 represents The concentration, absorbance and the corresponding percentage of scavenging of ethanolic MR extract. The Graph of percentage scavenging against the sample concentration is shown in Graph 3.
Antihyperglycaemic Activity Screening of Maceration Extract
Animal
Healthy, adult, Sprague-Dawley (SD) rats (180 ± 20 g) were used for anti-hyperglycemic studies. The animals were obtained from Central animal house, AIMST University, Malaysia. Approval from the AIMST University Human and Animals Ethics Committee was obtained.
Induction of Diabetes
Healthy, adult male SD rats were used for the experiment. Diabetes mellitus will be induced in overnight fasted rats by administration of single intraperitoneal (I.P.) injection of freshly prepared streptozotocin (STZ) with a dose of 60 mg/kg/mL [12]. Anti-hyperglycaemic activity of ethanolic extract of MR was studied using STZ-induced diabetic rats. The diabetic animals were showed decreases in body weight but the results were not significant (Table 2). The diabetic rats showed significant increases in the levels of glucose throughout the study when compared with that of control animals. Whereas the diabetic animals treated with glibenclamide or ethanolic extract of MR (100/ 200 mg/kg) showed significant decreases in the glucose levels when compare with that of diabetic control animals. As shown in Tables 12 & 13, the normalized blood glucose levels of 200 and 400 mg/kg Morus rubra treated groups did not exhibit significant difference as compared to the 20 mg/ kg glibenclamide treated group since week one. This revealed that the anti-hyperglycaemic effect of the Morus rubra was comparable with that of glibenclamide.
Discussion
One of the objectives of this research was to determine the phytochemical properties of MR. The MR extracted with 95% ethanol and the plant extract was undergone phytochemical screening. The presence of phytochemicals is a marker that the plant can be an essential source of precursors in the formation of newer synthetic drugs. In the present study, the results obtained for the phytochemical screening of MR ethanolic extract was analysed and it was found out that alkaloids, anthraquinone, carbohydrate and flavonoids were present in the sample. Moreover, the extractive value estimation should be carried out to determine the amount of the active constituents in a given amount of plant material and identify which extraction solvent is more suitable for the given plant sample. By using this method, phytochemicals present in the plant were extracted maximally. Phenolic compounds are very essential plant constituents which responsible for the antioxidant activity due to its redox properties. As a basis, Folin-Ciocalteu reagent was used to measure the phenolic content of different concentrations of plant extract. In this test, the Gallic acid was used as a standard and the total phenolic content was calculated by using the formula C = (A/B) x dilution factor. The results were derived from the calibration curve of Gallic acid, it was expressed as Gallic acid equivalents (GAE) per gram of samples. In the present study, the total phenolic content found was 6.420 mg GAE/g and 6.097 mg GAE/g for the concentrations of 50 and 200μg/ml respectively.
In this research work, the antioxidant potential of the MR extract was determined by using DPPH free radicals scavenging method and BHT was used as a standard. The DPPH is a stable freeradical which has a colour of purple, as the antioxidants react with the DPPH, the DPPH will be converted into non-radical DPPH-H form. Besides that, the colour of the DPPH will be decolorized from purple to light yellow colour. The degree of decolorization indicates the potency of the plant extracts in scavenging the free radicals. According to the results obtained, the IC50 was calculated for the BHT. The antibacterial activity of MR was tested by using the Escherichia coli, Staphylococcus aureus, Salmonella typhi, and Bacillus subtilis. The extract concentrations used in the agar well diffusion method were 0.1, 0.2, 0.4, 0.6, 0.8 and 1.0 mg/ml, other than that, 5mg/ml of penicillin and ciprofloxacin was playing the role as a standard in this study. In the present study, there was no zone of inhibition observed in all concentrations of ethanolic MR extract. The microorganism used were all in active condition, this can be proven as the ciprofloxacin as well as penicillin showed a clear zone of inhibition. In addition, the bacteria strains utilized were susceptible towards MR as stated [15-20], therefore it was concluded that the extracts have no antibacterial activity at the concentration of 0.1, 0.2, 0.4, 0.6, 0.8 and 1.0 mg/ml against gram negative. In the case of MIC test, the plant extract with the concentration of 0.1, 0.2, 0.4, 0.6, 0.8 and 1.0 mg/ml were utilized.
Conclusion
In conclusion, the phytochemical screening of ethanolic extracts of MR had determined the presence of alkaloids, flavonoids, carbohydrates and anthraquinones. The antibacterial activity of MR was determined by using the agar well diffusion and MIC assay. The micro-organism used were Escherichia coli, Staphylococcus aureus, Salmonella typhi, and Bacillus subtilis. There was no antibacterial activity observed in the agar well diffusion with Escherichia coli and the MIC assay [21-29]. The antioxidant activity of the plant extract was assessed through the method of DPPH test while the total amount of phenolic compounds in the extract can be determined through the TPC test. It was suggested that MR can be a potential source as a natural significant antioxidant and less marked antimicrobial agent. The MR is a natural source that worth for further explore as it is inexpensive, natural, harmless and easy to obtain.
Interests of Conflict
The authors declare that there is no conflict of interests in the present publication.
Remote Monitoring of the Health Status of Pregnant Women at Risk for Preeclampsia
The Role of Remote Technologies in the Quality Management System and Safety of Medical Care
On April 26, 2021, Deputy Chairman of the State Duma Irina Yarovaya at a meeting of the Presidium of the Council of Legislators of the Russian Federation under the Federal Assembly of the Russian Federation called for simplifying the exchange of data between medical institutions and patients. In the Sverdlovsk region, an automated information system of mobile notifications “AIST_SMART” for pregnant patients and doctors began to operate. Using a smartphone or, say, a tablet, pregnant patients in their personal account get the opportunity to keep an electronic diary of self-control of their health. The diary has the functions of automatic interpretation of the results and the formation of signal information for the obstetrician-gynecologist. Now pregnant women do not need to fill out paper diaries of self-control (Figure 1), call their doctor or the reception of the antenatal clinic in order to report the results – the process is fully automated.
The women’s consultation received an IT tool for remote interaction with pregnant women and women in child child. The introduction of “AIST_SMART” technologies made it possible to replace paper diaries with electronic ones. Medical data of the patient are collected in a single database and allow you to track the dynamics of the patient’s health around the clock. The results of electronic diaries are automatically processed by the system and if no abnormalities are detected, the data is simply recorded in the system and does not disturb the doctor (Figures 2 & 3). In case of detection of deviations in the patient’s state of health, the system marks the identified deviations and sends a notification to the doctor about the current state (Figure 4). Mobile notifications instantly convey accurate and detailed information about the patient’s state of health and thus contribute to the timely decision to hospitalize in case of detection of preeclampsia / severe arterial hypertension. Remote health monitoring functions as follows.
Figure 1: Paper diary – as it WAS.
Figure 2: Data of the diary of self-control of blood pressure, the norm.
Registration in the System “AIST_SMART”
To register the patient in the personal account at the initial appointment of a pregnant patient, a consent-instruction [1] is issued to connect to the mobile service “AIST_SMART” with an individual QR code. At home, the patient reads the QR code using the camera of her smartphone or tablet and, according to the instructions, undergoes the registration procedure, forming a digital four-digit PIN-code. From now on, it is guaranteed 24/7 technical support. The QR code serves as the patient’s identifier and the link between her electronic medical record (EHR) in the AIST “RAM” and the personal account in the “AIST_SMART” system. To register a doctor in your personal account, you must log in to the medical information system – AIST “RAM”, in which all medical personnel of the obstetric service in the region work. Open the “Personal Account” tab and register by scanning an individual QR code. So, in order to access electronic self-control diaries, the doctor and the patient connect to the AIST_SMART service, and after registering in the system, notifications about the results of remote health monitoring will be received on their mobile device. The doctor does not need to call on the phone to find out how she feels, what her blood pressure, temperature, etc.
How the Mobile Alert System Works
Formation of Notification of the Result of Self-Control Diaries
This process is fully automated. AIST_SMART performs the role of an intellectual assistant to the obstetrician-gynecologist/ midwife. The patient fills in the diary data, and the doctor receives ready-made results with automatic interpretation. Now the patient will not forget her paper diary at home, and the doctor will be able to make decisions on the tactics of management, taking into account not only the data on a face-to-face visit, but comprehensively taking into account the results of the patient’s home self-control, which is important when selecting antihypertensive therapy in patients with arterial hypertension.
Pregnancy with Arterial Hypertension and at Risk for Preeclampsia
All patients in this category should carry out home monitoring of blood pressure with keeping a diary [2]. The self-control diary can be kept both by filling out the extended web-form of the diary, and by means of a chatbot in AIST_SMART, where the patient can send data in the format of a simple message: “pressure 120 70” and the service automatically recognizes, processes the data and records them in her personal account. If deviations of blood pressure above the norm are detected, AIST_SMART will automatically offer the patient a further algorithm of actions:
Indicate Complaints and the Presence of Proteinuria According to the Results of the Test Strip (Figure 5)
Emergency Hospitalization without Further Action is Recommended (Figure 6)
All notifications in case of deviations are automatically sent to the attending physician and the doctor in the Obstetric Remote Consultation Center (hereinafter referred to as the ADCC) for the routing of the patient 24/7. Doctor of the ADC on the basis of the results of the self-control diary (Figure 7) and obstetric status according to the data in the electronic medical record (hereinafter – EHR) in the AIST “RAM”, where there is information about all the results of the examination, the course of pregnancy and diagnoses, decides on further management tactics: to continue outpatient treatment or hospitalization in an obstetric hospital. The ADCC doctor fixes his decision in the EHR, making out a remote consultation for the attending physician of the antenatal clinic or obstetric hospital, if the patient is hospitalized in the MO level 1.2.
In the absence of indications for hospitalization, the results of the remote consultation are sent automatically to the attending physician of the antenatal clinic. Subsequently, the attending physician within the framework of the next outpatient visit will be able to track the patient’s condition, the effectiveness of the prescribed antihypertensive therapy, viewing trends in diaries, and adjust the therapy based on a comprehensive analysis. If a decision is made on the need for hospitalization, the doctor of the ADC through a confidential “working” chat in AIST_SMART can contact the patient and clarify her consent to hospitalization and the possibility of transportation by personal transport. If consent is obtained (Figure 8), the doctor of the ADCC draws up an add. The patient receives a notification about the issued referral indicating the obstetric hospital, the date and time of hospitalization (Figure 9). In turn, the doctor of the obstetric hospital also receives information that the patient is sent to him both through the AIST “RAM” (Figure 10) and in the personal account of AIST_SMART through automatic notifications in the directions (Figures 9&10).
You do not Need to Receive a Paper Direction
If necessary, you can print the direction at the place of treatment of the patient, using a single information space of the regional obstetric monitoring of AIST “RAM”. All the directions that a woman received during pregnancy are reflected in her personal account in the “My directions” section. The patient can open any document, even if the connection with the Internet has disappeared.
Advantages of Remote Monitoring of Health
The transition to electronic diaries of self-control allows you to identify complications of the gestational process in the case of arterial hypertension and timely send the patient to hospitalization to prevent adverse events, which is from the main directions of the quality management system and safety of medical care. AIST_ SMART allows you to create constant feedback with the patient and thereby form a patient-centric model of care as one of the priority areas for the development of modern medicine and healthcare in general. All of the above increases the compliance of doctor-patient interaction and directly affects the quality and safety of medical care in the context of the widespread prevalence of arterial hypertension in the population (pregnant women are no exception), which meets modern needs of society and solves the tasks set by the Government of the Russian Federation in the field of digitalization of healthcare [3-5].
Conflict of Interest
No conflict of interest with any institution/organization.
Level of Activity Limitation Due to Joints Pain among Hemophilia Patients
Introduction
Hemophilia is an inherited type of disease in which clotting factor VIII cannot produce properly in the body. These diseases can lead to prolonged bleeding after injury or surgery and sometimes bleeding in the joint [1]. The first time hemophilia was discovered in the 2nd century AD and a full description of hemophilia was written in the 19thcentury.The ant hemophilic factor was discovered in the middle of 20 century [2]. Approximately 40,000 peoples are affected by hemophilia worldwide and it is the most complicated disease in the world [3]. Hemophilia is the type of X-linked group disease in which blood coagulation factor VIII cannot produce. Based on clotting factor hemophilia has two types. The deficiency of clotting factor VIII is called hemophilia A and the deficiency of clotting factor IX is also called hemophilia B [4]. Hemophilia A is the most common genetic disorder about 80 % of people have hemophilia A in the overall population of hemophilia diseases. The prevalence of hemophilia A (HA) 1 per 5000 in the general population and the prevalence of hemophilia B (HB) is 1 per 30,000 in overall general papulation .Hemophilia is mainly present in the male population .on based on coagulation factor activity hemophilia is also divided into three further groups .Clotting activity less than 1 percent is severe if 1-5 % is moderate and if clotting greater than 5-30 %. The intensity of bleeding is depending on hemophilia severity. If the intensity of hemophilia is severe, the spontaneous bleeding occurs in soft tissues, joints, nose, and other parts of the body, and if the intensity of diseases is moderate or mild the prolonged bleeding occurs after injury or surgery [5]. Bleeding in joints is more common in hemophilia patients due to a lack of clotting factors. The bleeding in the joint produces more complications in joint. Inflammatory reactions start due to hem arthrosis. Hemophilic arthropathy starts due to repeated episodes of bleeding in joints. The inflammation of the synovial membrane in a joint can lead to a breakdown of articular cartilage of the joint. The articular breakdown starts in early childhood in hemophilic patients. Chronic pain starts in hemophilic joints due to the breakdown of articular cartilage. Chronic hemophilic arthropathy can various effects on bone health, it can cause chronic pain in joints, swelling, limit the daily activities of life, decrease the range of motion of joints and also decrease the quality of life in hemophilic patients. The most common joints which are affected by hemophilia are ankle, knee, hip, elbow, and shoulder joints. There are usually weight-bearing joints that have a bad impact on physical movements. The bleeding the joints cause hypertrophy of physics which lead to valgus deformity in hemophilia patient [6]. Joint illness linked with recurrent joint bleeding causes discomfort and functional impairment in people with hemophilia (PWH) (hemarthroses). Discomfort is common in PWH, according to many studies [7,8] and pain associated with hemophilia has been linked to a worse health-related quality of life (HRQoL). PWH also has mental health problems [9,10]. According to the EQ-5D- 3L, depression affects around one-third of PWH, and the Patient Health Questionnaire (PHQ-9), a scale used to evaluate the severity of depressive symptoms in adults, 37 percent of PWH fulfilled the criteria for depression in another research [11]. The influence of hemophilia on emotional well-being, like other elements of HRQoL, is rarely studied in the therapeutic context. In the comprehensive care environment or to individualize hemophilia therapy, neither general nor disease-specific patient-reported outcome (PRO) tools are routinely employed [12]. Greater expertise with and validation of PRO instruments in PWH may expand their usage for clinical outcome monitoring, as well as provide possibilities to improve patient dialog and treatment of specific outcomes. The repeated episode of bleeding in joints can start the inflammatory reaction in joints. This inflammatory reaction starts the breakdown process in joints. The breakdown has a serious impact on bone and joint health it can lead to osteoporosis of bone, articular cartilage damage, and bony osteophytes formation in joints, decrease the range of motion of joints and also decrease the daily activity of life. Hemophilia patients have a great risk of depression. The main reason for depression in hemophilia patients is a decrease in the activity of life [13]. Swelling, heat, and immobility are all symptoms of joint bleeding. Furthermore, acute bleeding produces significant discomfort in the affected joint, a symptom that has received little attention in prior research. The bulk of studies in this area focused on the management of pain in general and the use of analgesics [14]. The hemophilia patient faced many psychosocial problems. This problem related to their education and jobs and is also a problem for the caregiver of children with hemophilia and barrier for happy living the people with hemophilia because they cannot perform the daily activity due to pain in joints and difficulty to concentrate his work [15]. Recurrent bleeding, in addition to the acute discomfort, triggers a persistent process that results in synovitis, increased cartilage degradation, and bone deterioration, eventually leading to hemophilic arthropathy. Despite the existence of numerous potential pathophysiological ideas, the actual underlying processes for either blood-induced arthropathy or, more specifically, joint bleedinginduced pain are yet unknown. Similar to other inflammatory joint diseases, the associated inflammatory response might be addressed as one possible source of pain complaints [16,17]. All of these mechanisms, on the other hand, contribute to hemophilia’s reported joint discomfort. As a result, current research is focusing on the causes and effects of persistent pain caused by hemophilic arthropathy. Because pain therapy is often ineffective, and many analgesic and anti-inflammatory medications are prohibited due to their clotting-inhibitory effects, a deeper pathophysiology understanding of pain in persons with hemophilia (PWH) is vitally necessary [18]. Hemophilic patients faced many problems in our society. They face social, mental, and physical problems. The reason for study in hemophilia to find out the activity limitation due to pain or hemarthrosis.
Literature Review
J Michael soucie (2015) et al. Conduct a cross-sectional study in a hemophilic treatment center in the USA. The study sample size was 4343 males aged 2-19 years with hemophilia diseases. They collect the data to assess the joint range of motion. They concluded that the range of motion limitation in hemophilia patients depends on the severity of disease and damage of articular cartilage due to bleeding in joints [19]. M. Witkop (2017) et al. Purpose a crosssectional study to find the prevalence and joint pain due to bleeding joint in people with hemophilia. Their study sample size was 381 whose age is middle to 37. They found that 71 % of people have a severe type of hemophilia and pain in the joint more common the people with hemophilia. In this study, they concluded that the functional activity limitation and quality of life decrease in people with hemophilia are due to chronic pain in the joint [7]. Tyler and W Buckner (2018) conducted a study in which they find the prevalence of functional limitation or living quality in hemophilia patients. The study sample size was 381 adult patients with hemophilia whose age was medial to 34 old. They use the visual analogs scale and brief pain inventory v2 short form to collect the data. They found that patients present severe pain in joints and functional limitation and also decrease the quality of life due to pain in joints. They concluded that early asses of joints bleeding and proper history improve the quality 0f life and activity of daily life [20]. Heng Zhang (2019) et al purpose a cohort study in China to identify the health-related quality of life in children. The study sample size was 42 children and the data was collected from kid’s life assessment tools. The conclusion of that study was health-related quality of life decrease in the children with hemophilia which depend on the severity of hemophilia or joint bleeding and bleeding joint decrease the activity of limitation [21]. MjidDavari and Zahra Gheribnaseri (2019) et al. conducted a cross-sectional study to determine the joints health status and living quality in hemophilia patients. The data was collected from the HR-QO2 questioner and joint health is to collect from hemophilic joint health score the study sample size was 38 people with hemophilia. They concluded that health-related quality of life in hemophilia patients was very low and many joints problems are found due to bleeding in joints [22]. Merel A and timmer (2020) purpose a study to determine the movement or behavior pattern in hemophilia patients. The study sample size was 107 people who have hemophilia. They collect the data from the Kruskal wall test and HJHS TOOLS. They found that runner and bike person with hemophilia is a few limitations in their life and they also concluded that sitting or standing was better for joint health [23]. In 2019 Dr. Edward Nguyo Maina purpose a cross-sectional study to find the prevalence of musculoskeletal problems in people with hemophilia. His study sample size was 37 people with hemophilia. He was data collected from the gilbert joint scoring system. He found that 86.5 % recurrent bleeding in joint, 75.7% of people have limited range of motion, and 70% have flexion contracture formation in joint with hemophilia. They found that musculoskeletal problems was linked with the severity of diseases [24].
Objective
The objective of this study was to determine the: “Level of activity limitation due to joint pain among hemophilia patients.”
Rationale
Hemophilia causes activity limitation or other health disorders in children. The Research gap exist to determine the level of activity limitation occur in hemophilia patients due to pain in joints. This study may also helpful for physiotherapy field to find the best physiotherapy treatment for hemophilia patients regarding their activity limitation. The main rationale of my study to find advance prevention and eliminates the activity limitation risk factor in further studies.
Operational Definitions
Outcome measure tools that was used in the study is Activilm Questionnaire. The ACTIVILM Questionnaire focus on assessing the basic knowledge of activity limitation by different question their correct answer [25]. Variables: a) Dependent variable: Activity limitation & pain b) Independent variable: Hemophilia patient are independent variable. Value of sensitivity/ specificity/validity/ reliability=0.95.
Materials and Methods
A. Study Design: Design of study was Cross-Sectional. B. Study Settings: Data for this research was gathered from hemophilic center in Lahore. C. Duration of Study: 06 months. D. Sample Size: Sample size is calculated using following formula and parameters.
Here Z 1−α/2 = is standard normal variate (at 5% type 1 error (P<0.05) it is 1.96 and at 1% type 1 error (P<0.01) it is 2.58). As a majority of studies P values are considered significant below 0.05 hence 1.96 is used in formula. p = Expected proportion in population based on previous studies or pilot studies. d= Absolute error or precision − Has to be decide by researcher Using 75.7% proportion of the condition sample size is 152 (Table 1).
Table 1: Antibody characterics used for immunohistochemistry.
Nguyo, E.M., Prevalence of musculoskeletal complications among hemophilia patients as seen at Kenyatta National Hospital. 2020, University of Nairobi.
E. Sample Technique: Non-probability convenient sampling was used. F. Criteria of Sample Selection: a) Inclusion Criteria: i. Hemophilia patients. ii. Age between 5-19 years. b) Exclusion Criteria: The people who have joint bleeding due to hematoma or other joint disorder such as juvenile arthritis.
Data Collection Procedure
The data was collected after approval from the ethical board of concerned institute. The study design for the study was a descriptive cross-sectional study. The data collected from only people with hemophilia diseases. A convenience non-probability is used as a sampling technique for a minimum sample size of 152 and father data was added according to study requirement to minimum choice of error. The duration of the study was of 6 months and eligibility criteria for participants include volunteers. The data was collected from the ACTIVLIM questionnaire that including the activity limitation assessment and knowledge. The data was collected in the different hemophilic centers in Lahore city. The data collected in the form of a hard copy. And distribute to hemophilia patients. Hemophilia patient was filled the form.
Ethical Consideration
The data was collected after the approval of the ethical board. The participant was provided with information regarding the study and informed consent was signed by the participant. Volunteers were preferred. The identity of participants kept confidential and the participant was allowed to withdraw from the study.
Statistical Analysis
Data was analyzed by using SPSS software for the questionnaire.
Results
a) Among 152 participants, male were 146(96.1%) and female were 6(3.9%) ( Figure 1).
Figure 1: Frequency distribution of Difficulty in gender.
Discussion
A study conducted by Buckner, Tyler Win 2018, Study aimed to determine the Assessments of pain, functional impairment, anxiety and depression in US adults with hemophilia. According to this study, participants reported feeling tired (93 percent), worn out (86 percent), very nervous (68 percent), downhearted and depressed (55 percent) and so down in the dumps that nothing could cheer them up (41 percent). According to our study Among 152 participants, male were 146(96.1%) and female were 6(3.9%). Putting on a T Shirt was difficult among 27(17.8%) and Easy among 125(82.2%).Washing ones upper body was difficult among 35(23.0%) and Easy among 117(77.0%).Dressing ones lower body was difficult among 83(54.6%) and Easy among 69(45.4%). Taking a Shower was Impossible among 2(1.3%), difficult among 87(57.2%) and Easy among 63(45.4%).Sitting on the toilet was Impossible among 12(7.9%), difficult among 91(59.9%) and Easy among 49(32.2%).Taking a bath was Impossible among 4(2.6%), difficult among 85(55.9%) and Easy among 63(41.4%) [25]. A study revealed patient was unable to perform the activity, or need complete assistance to perform the activity like transfers/ squatting and running. Some need partial assistance/aids/ modified instruments/modified environment to perform the activity like eating, bathing, dressing going up a stairs, walking running. The other group able to perform the activities without aids or assistance, but with slight discomfort, unable to perform the activities similar to their healthy peers like eating, bathing, dressing going up a stairs, walking and running. A few subjects were able to perform the activities without any difficulty similar to their healthy peer. According to our study among 152 participants, walking upstairs was Impossible among 9(5.9%), difficult among 96(63.2%) and Easy among 47(30.9%). Stepping out of a bath tub was impossible among 1(0.7%), difficult among 53(34.9%) and Easy among 98(64.5%).Opening a door was difficult among 12(7.9%) and Easy among 140(92.1%).Walking outdoor on level ground was Impossible among 4(2.6%), difficult among 52(34.2%) and Easy among 96(63.2%). Washing ones face was difficult among 25(16.4%) and Easy among 127(83.6%). Hanging up a jacket on a hat stand was difficult among 67(44.1%) and Easy among 85(55.9%). Wiping ones upper body was Impossible among 1(0.7%), difficult among 52(34.2%) and Easy among 99(65.1%). walking upstairs was Impossible among 6(3.9%), difficult among 134(88.2%) and Easy among 12(7.9%) [26]. According to another study knees (23.7 percent), elbows (23.7 percent) and ankles (37.4 percent) were the most often reported sore joints (18.9 percent) among hemophilia patients. On the International Physical Activity Questionnaire, 51% said they had done nothing in the previous week. The median sub scores for four physical health domains were lower than the median sub scores for four mental health domains on the SF-36v2 health survey. Leg functions (median, 66.7) and lying/sitting/kneeling/standing (median, 67.5) were the most impacted Hemophilia Activities List domains (range 0 (worst)-100 (best)), whereas self-care was the least impacted (median, 100.0). Ankle scores (median, 6.0; range, 0-40) on the HJHS were lower than elbow/knee scores (median, 4.0/4.0).and according to our study Among 152 participants, Carrying a heavy load was Impossible among 13(8.6%), difficult among 133(87.5%) and Easy among 6(3.9%). Getting in to a car was difficult among 24(15.8%) and Easy among 128(84.2%). Standing for a long time was Impossible among 12(7.9%), difficult among 117(77.0%) and Easy among 23(15.1%). Walking more than 1 km was Impossible among 23(15.1%), difficult among 117(77.0%) and Easy among 12(7.9%). Closing a door was difficult among 8(5.3%) and Easy among 144(94.7%). Hopping on one foot was Impossible among 5(3.3%), difficult among 97(63.8%) and Easy among 50(32.9%). Putting on a backpack was Impossible among 3(2.0%), difficult among 105(69.1%) and Easy among 44(28.9%). Running was Impossible among 17(11.2%), difficult among 134(88.2%) and Easy among 1(0.7%) [27].
Conclusion
Pain was observed most common problem that affected daily activities and quality of life among hemophilia patients. Respondents reported functional impairment that limit the daily routine work and activities they participated in especially with activities involving the lower extremities.
Limitations
a) Due to low population of hemophilia so data collection took time. b) The data was collected from single hemophilia center in Lahore. c) Difficulties in collection of data because of Covid-19.
Recommendation
a) Study should be analyzed through clinical analysis in future. b) Seminars can be conducted to spread the awareness among patients. c) Longitudinal study should be conducted to evaluate the long term effects of hemophilia on joint pain. d) The data should be collected from all over hemophilia treatment centers of Pakistan.