Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Grayish Metal to White Ceramic; Iso Standards Are the Only Passports for Ceramic Dental Implants
Introduction
The long-term success of titanium osseointegrated implants in periodontally healthy patients has been documented in various studies [1]. However, additional data are still needed to confirm the long-term predictability of dental implants in general. Titanium and titanium alloys are commonly used as dental implant materials. The process of integration of titanium with bone has been firstly termed by Brånemark [2] as “osseointegration”. Currently, most of the commercially available implant systems are made of pure titanium or titanium alloy. However, even though titanium alloys were exceptionally corrosion-resistant because of the stability of the TiO2 oxide layer, they are not passive to corrosive attack [3]. Moreover, one of the most famous problems regarding titanium is hypersensitivity [4,5]. Due to the possible negative effects of titanium, the clinical application of implants made from different novel ceramic biomaterials has become more active. Such ceramic materials include single- and poly-crystal alumina [6], bioactive glasses [7], hydroxyapatite [8], and zirconia [9]. To date, there are several commercially available zirconia implant systems on the market [10]. Some provide both one- and two-piece designs and the others provide only one-piece designs. In order to bring dental implants into markets, they should firstly pass several mechanical tests like fatigue and dynamical loading tests.
These tests are mainly related to the ability of implant to withstand loading strength as a simulation to what is comparable to the oral cavity. Loading tests for dental implants can be denoted according to predefined standards or norms (i.e. ISO, DIN, or EN). For instance, DIN 50100 describes a load-controlled fatigue testing design at constant load amplitudes on metallic specimens and components. The endurance limit can be displayed, for example, in a fatigue strength diagrams [11]. However, this standard is not usually applicable for testing dental implants. ISO 13356:2015 specifies the requirements and corresponding test methods for a biocompatible and bio-stable ceramic bone-substitute material based on yttriastabilized tetragonal for use as a material for surgical implants. This norm imposes that a maximum of 25 wt% of monoclinic phase is present in test specimens after an accelerated aging test (134°C in a humid atmosphere with an air pressure of 0.2 MPa) [12]. ISO DIN 14801:2016 [previously known as ISO 14801:2007] specifies a method of dynamic testing of single post endosseous dental implants of the trans mucosal type in combination with their premanufactured prosthetic components [13,14], and is used in 162 member countries around the world. It is most useful for comparing endosseous dental implants of different designs or sizes [15].
This international standard is not a test of the fundamental fatigue properties of the materials from which the endosseous implants and prosthetic components are made, and, moreover, is not applicable to dental implants with endosseous lengths shorter than 8 mm nor to magnetic attachments. While ISO 14801:2016 simulates the functional loading of an endosseous dental implant under “worst case” conditions, it is not applicable for predicting the in vivo performance of an endosseous dental implant or dental prosthesis, particularly if multiple endosseous dental implants are used for a dental prosthesis. In our opinion, although ISO standards are equipped to encounter all possible loading situations that could take place in the mouth, they still lack more real conditions that should be taken into consideration. To simulate intraoral aging to the extent possible and, in particular, address the degradation susceptibility of metastable zirconia ceramics, an experimental setup by Spies et al. [15] tried to add some modifications that differed from ISO 14801. The mentioned norm does not include horizontal loading components or degradation accelerating environmental factors. By placing the samples of the mentioned study in a warm fluid of 60°C during the dynamic loading procedure, the applied testing protocol was designed to account for the specific nature of zirconia ceramics and its behavior in aqueous environments.
Furthermore, ISO 14801 dictates the simulation of a 3mm bone recession. In another important trial to enhance the testing conditions of ISO 14801, Castolo et al. [16] tried to use finite element analysis to assess the influence of design parameters on the mechanical performance of an implant in regard to testingconditions of ISO 14801 standard. In their study, an endosseous dental implant was loaded under ISO standard 14801 testing conditions by numerical simulation, with 4 parameters evaluated under the following conditions: conditions of the contact surface area between the implant and the loading tool, length of the fixation screw, implant embedding depth, and material used for implant stiffness. Finite element analysis was used to compare the force that needed to reach the implant’s yield and fracture strength. It was shown that finite element analysis made it possible to evaluate 4 performance parameters of a dental implant under ISO standard 14801 conditions. Under these conditions, the contact surface area was found to be the major parameter influencing implant performance.
Conclusion
Zirconium implants have an obvious esthetic advantage over titanium implants being “pure white”, making them indistinguishable from natural teeth. Fracture, corrosion, fatigue, the possible abrasion actions that take place within the connected parts of implant, and other relevant terms are all important mechanical factors that should be taken into consideration before introducing ceramic dental implants in the market. Such mechanical features should be tested through previously defined standards or norms. To date, two separate international ISO standards are available for testing dental implants; namely ISO 13356 and ISO 14801. However, there is still a recent debate regarding these currently applicable ISO standards due to the fact that they are not addressing the in vivo aging behavior of zirconia dental implants to verify their real pre-clinical safety.
Rare Diagnosis of Benign Schwannomas after Right Thyroid Lobectomy in A 12-Year-Old Female
Abstract
Schwannomas are benign neoplasms arising from neural sheath cells. Schwannomas most commonly arise in the head and neck region, most commonly developing from the vestibulocochlear nerve. On rare occasions, primary schwannomas have been described originating from the thyroid. Traditional diagnostic modalities are often ineffective in diagnosing schwannomas of the thyroid preoperatively, leading to an incidental finding after surgical intervention has occurred. The case we present is of a 12-year-old female who underwent a right thyroid lobectomy after two fine needle aspirations that raised concern for follicular malignancy, Hurthle cell type. Final pathology revealed a benign, S-100 positive, primary schwannoma of the thyroid.
Keywords: Thyroid Schwannoma
Introduction
Schwannomas are benign, peripheral nerve neoplasms originating from neural sheath cells (Schwann cells) [1]. These well-circumscribed, encapsulated masses develop from nerve roots throughout the body, with 25% to 45% originating in the head and neck [2]. In a majority of cases, benign Schwannomas arise from the vestibulocochlear nerve (CN VIII), followed by trigeminal nerve (CN V) and facial nerve (CN VII) [2]. On rare occasions primary Schwannomas have been reported in the thyroid gland, with the first case reported in the literature in 1964 [3]. Since then, a vast majority of cases reported of schwannomas involving the thyroids are in adult patients. In 2004, one case was published involving a twelve-year-old female [4].In 2010, a primary schwannoma of the thyroid was reported in a fourteen-year-old male [5]. The case we present is an additional schwannoma of the thyroid in a twelveyear- old female.
Case Report
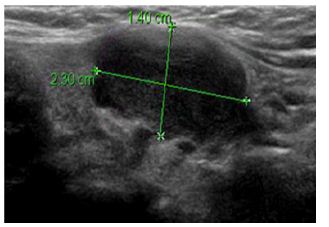
A twelve-year-old female patient first presented to the University of Kansas Pediatric Department with increased rightsided neck swelling after experiencing recent upper respiratory tract infection. The neck was non-tender. There was no reported dysphagia, dysphonia or hoarseness and no hyperthyroid or hypothyroid symptoms were noted. Past medical history was only significant for mild asthma with occasional use of an albuterol inhaler. No surgical history was reported and no family history of thyroid disorders or thyroid cancer. The patient did not smoke or consume alcohol. Physical exam revealed right neck swelling that was non-tender to palpation. Thyroid function tests were within normal limits. An ultrasound was ordered and revealed a right thyroid hypoechoic mass in the middle portion of the thyroid at and along the isthmus measuring 2.3 cm by 1.4 cm by 1.8 cm (Figure 1). The margins were slightly lobulated and irregular with some vascularity seen at the inferior medial edge. Mild mass effect was noted on the adjacent trachea with no evidence of tracheal invasion. The left thyroid lobe was unremarkable. Small, normal appearing lymph nodes were noted within the neck. At this point, the differential diagnosis included a complex hemorrhagic cyst versus a hypovascular solid thyroid neoplasm.
Figure 1: A right thyroid hypoechoic mass in the middle portion of the thyroid at and along the isthmus measuring 2.3 cm by 1.4 cm by 1.8 cm.
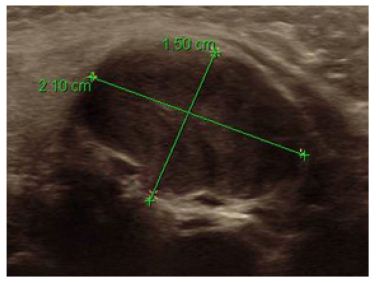
The patient was referred to University of Kansas Pediatric Surgery for further evaluation. The patient continued to be asymptomatic with physical exam noting fullness of the right thyroid that was non-tender to palpation. At this time it was recommended that a biopsy by fine needle aspiration be obtained and a repeat ultrasound be completed in two months. A repeat thyroid ultrasound was obtained two months after the initial study and revealed a stable right thyroid mass in the medial right lobe and isthmus measuring 2.1 x 1.5 x 1.9 (Figure 2). The differential continued to be hemorrhagic cyst versus benign or malignant neoplasm. A biopsy by fine needle aspiration was again encouraged. Three months following initial presentation a biopsy was obtained by fine needle aspiration. Cytology was suspicious for a follicular neoplasm, Hürthle cell type and the patient was referred to Surgical Oncology at the University of Kansas. During the evaluation by surgical oncology, the patient continued to report no dysphagia, dysphonia or hoarseness and no hyperthyroid or hypothyroid symptoms. Physical exam remained unchanged with a palpable, non-tender right-sided neck mass noted with no lymphadenopathy noted. Repeated thyroid function tests were again within normal limits. Because the patient presented at such a young age, the case was presented at a multidisciplinary endocrine tumor conference at the University of Kansas. After detailed discussion, it was recommended that a second biopsy by fine needle aspiration be obtained with Afirma molecular genetic testing.
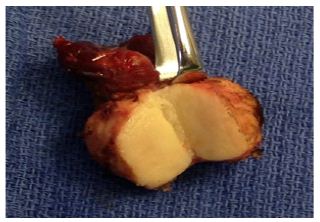
The repeat fine needle aspiration was again suspicious for a follicular neoplasm, Hürthle cell type. The repeat fine needle aspiration using Afirma thyroid FNA analysis was suspicious for malignancy, with the probability of malignancy from 10-30% to 40%. However, the test is not validated on patients under twentyone years old. The gene expression classifier also identified a genetic signature similar to malignant melanoma. As a result of the second fine needle aspiration, combined with the molecular genetic testing, surgical lobectomy with the possibility of bilateral neck exploration and total thyroid ectomy was recommended. The patient underwent right thyroid lobectomy with intraoperative monitoring of the recurrent laryngeal nerve. Surgical findings revealed an enlarged, firm, right inferior thyroid lobe with effacement of the anterolateral tracheal surface, requiring a shave dissection of the nodule off the tracheal rings (Figure 3). No lymphadenopathy was noted within the neck. Final pathology revealed a benign schwannoma in the right thyroid lobe (Figure 4). The mass was less than 4 centimeters, lacked mitotic activity, necrosis or nuclear pleomorphism, all of which are factors that support a benign cellular process. The tumor was positive for S-100 and negative for TTF-1, which supported diagnosis of benign schwannoma.
The case was again discussed in multidisciplinary endocrine tumor conference to determine adequate follow-up. Because pathology showed positive margins at the anterior tracheal margin, risk of recurrence remained. It was decided that the patient would be followed with a thyroid ultrasound six months postop to monitor for recurrence. Subsequent serial ultrasound evaluations over the following three years have demonstrated no evidence of recurrence and the patient continues to do well.
Radiology Images
(Figures 1-4)
Figure 2: A stable right thyroid mass in the medial right lobe and isthmus measuring 2.1 x 1.5 x 1.9.
Figure 3: Gross surgical specimen of the nodule off the tracheal rings.
Figure 4: Gross surgical specimen of a benign schwannoma in the right thyroid lobe.
Discussion
Primary schwannomas of the thyroid gland are exceptionally rare. To our knowledge, less than twenty cases have been reported in the literature, with only two other cases reported involving a child. One case involving a fourteen-year old male [5] and our case being the second case reported of a primary schwannoma in a twelveyear- old female. Fine needle aspiration is the foundation of initial management of a thyroid nodule. The technique has reduced the number of thyroid ectomies and increased the number of malignant diagnoses after thyroidectomy [6]. In the case presented; fine needle aspiration was performed on two occasions. Each fine needle aspiration was suspicious for follicular neoplasm, Hürthle cell type. The results of the fine needle aspiration combined with the ultrasound images raised concern for malignancy, which lead to surgical intervention. It has been suggested that multiple diagnostic modalities combined with fine needle aspiration should be considered. Ultrasound, CT and MRI can be used to help differentiate between solid and cystic masses, but cannot be used to obtain a definitive diagnosis [7]. PET-CT has also been described as having a possible role in pre-operative diagnosis of thyroid schwannomas. It has been shown that both benign schwannomas and malignant peripheral nerve sheath tumors show FDG uptake [8]. This may be useful when distinguishing between schwannoma and other benign masses of the thyroid where FDG uptake would not occur [7], but would have been of little use in our case, due largely to the fact that malignancy was our greatest concern. Recurrence of schwannomas is uncommon and due largely to the inability to fully resect the tumor. Although rare, malignant transformation from benign schwannoma in sites outside the thyroid has been reported in the literature. For this reason we have decided to follow up with ultrasound every six months.
Conclusion
In conclusion, schwannomas originating from the thyroid gland are rare and difficult to diagnose pre-operatively. They frequently present as a painless neck mass and are difficult to distinguish in appearance from most thyroid nodules on ultrasound. Definitive diagnosis of a thyroid schwannoma prior to thyroid lobectomy is an uncommon occurrence and is often found incidentally by pathology after surgical intervention.
Improved Early Stage (T1/2) Oral Tongue Cancer Medial Pathology Margins Using Horizontal Mattress Suture Technique
Abstract
Objectives: Description of a novel surgical technique for partial glossectomy in oral tongue cancer patients with comparison of pathologic margins to conventional technique.
Patients and Methods: Patients with oral tongue cancer underwent partial glossectomy using a new horizontal mattress surgical technique developed by the senior author and were compared retrospectively to an age, sex and stage matched cohort. Anterior, posterior, and medial pathology margins were compared utilizing the student’s t-test for normally distributed variables, and Wilcoxon-Mann-Whitney test for variables which were not normally distributed.
Results: 10 patients underwent partial glossectomy with the new technique. The mean medial pathology margin was significantly greater in the new technique group (1.40 cm vs 0.88 cm, p=0.04). There were no significant differences in anterior margin or posterior margin, age, tumor size or depth of invasion.
Conclusions: The new surgical technique using horizontal mattress sutures for dissection guidance and specimen orientation yielded improved medial pathology margins compared to conventional technique.
The oral tongue is the most common site for oral cavity cancers. Squamous cell carcinoma (SCCa) is responsible for over 90% of cases with an estimated incidence of 3.0/100,000 in the United States [1,2]. Males with a history of tobacco and alcohol use are at greatest risk and commonly present with early stage lesions. Treatment involves wide local excision, neck dissection if indicated and possibly post-operative radiation therapy depending on pathological features. The 5 year survival is 75-89% for early stage disease [2].
Unfortunately, locoregional recurrence is the most common cause of treatment failure. Inadequate surgical resection margins are often attributed to local recurrences while tumor depth, occult metastasis, and insufficient treatment of the neck contribute to regional recurrences. Locoregional recurrences of 23% have been reported in T1/T2 oral tongue cancer patients with margins <5mm despite adjuvant therapy [3]. In contrast, local recurrence has been shown in only 11% with tumor free margins, showing that establishing adequate negative margins is imperative to preventing recurrence [2,4]. Operative success in terms of negative margins is largely determined by the surgeon’s experience and frozen section analysis. Achieving clear pathologic margins is often challenging as distortion of the specimen during mobilization may compromise an adequate margin around the specimen. Although various techniques are utilized to remove tongue cancers, information is limited in regards to obtaining consistently acceptable surgical margins. We describe a novel technique to improve accuracy and consistency of tumor resection using horizontal mattress sutures.
Patients and Methods
Patients were prospectively selected between February 2011 and July 2013. All patients of the senior author (NV) with a diagnosis of T1 and T2 squamous cell carcinoma of the oral tongue were eligible for the study provided mattress suturescould be adequately applied around the lesion’s resection margin. Patients with significant tumor extension to the base of tongue and floor of mouth were excluded as the sutures become difficult to insert. Approval for the study was obtained from the University of Oklahoma institutional review board. The operations were performed at the University of Oklahoma Health Sciences Center. Patients who underwent partial glossectomy with the new technique were compared with a cohort of patients who had undergone partial glossectomy with conventional technique i.e. no mattress sutures.
Patients were matched based on age, sex, and stage to a retrospective comparison cohort selected from prior tongue cancer patients of the department. Observations were classified into two groups: new suture technique and conventional technique. Comparisons of margins at the anterior, posterior, and medial aspects of the pathologic specimens were made between the groups. Mean values were compared with the student’s t-test for normally distributed variables, and median values were compared with the Wilcoxon-Mann-Whitney test for variables which were not normally distributed. P<0.05 was considered a significant result.
Description of Procedure
Depending on the extent of resection, a tracheostomy may be required to secure the airway before or after the resection as deemed necessary by the surgeon. The tumor is assessed both visually and by palpation after reviewing preoperative imaging studies. The tongue is tethered using 4-0 silk sutures around its anterior and lateral borders to maintain orientation and provide traction. A 1.5 cm margin5 is then marked around the lesion. A semi-circle is drawn from the posterolateral margin medially around the cancer and connected to the anterior margin on the dorsal surface. A similar line is drawn on the ventral surface and connected to dorsal markings at the lateral surfaces.
To maintain the plane of dissection and preserve margins, 2-0 silk horizontal mattress sutures are placed along the tongue markings in a sequential fashion usually using at CT1 curved needle. Each suture is placed through the dorsal and adjacent ventral surfaces, passed back through the tongue to the dorsal surface and tied. The concave aspect of the needle faces the cancer lesion to maximize suture distance away from the cancer. A suture scaffold is created to maintain normal anatomic position as the specimen is mobilized (Figure 1).
Anterior traction is applied using the tethering sutures for exposure. Resection is performed using electrocautery to dissect along the medial aspect of the mattress sutures. A surgical plane is maintained without undermining of surrounding normal tissue of either the specimen or the residual tongue (Figure 2). The mattress suture prevents tissue stretching and distortion during manipulation and maintains both specimen orientation and integrity for pathological analysis [5]. In most instances of early tongue cancer, the surgeon does not need to manually manipulate the tongue. The tumor is removed having uniform clean edges with the mattress sutures intact on the specimen. Following removal of the specimen, tissue is oriented for frozen section and transported to the pathologist with the mattress sutures intact. Tissue splaying and shrinkage of margin distance that occurs with retraction and manipulation are reduced by these sutures which also maintain anatomic integrity of the excised specimen.
Results
Between February 2010 and July 2013, a total of 10 patients underwent partial glossectomy utilizing the new suture technique. The mean age was 60.8 years old (range: 24-88). The male to female ratio was equal at 1:1. The tumors were all T1 or T2 and ranged in size from 1.2 to 3.3 cm. Sixty percent of the tumors were staged as pT1. The median depth of invasion was 0.65 cm and ranged from 0.4 to 1.6 cm. Upon comparing the two groups, there were no significant differences with regard to the mean tumor size (1.91 cmvs. 1.71 cm, p=0.67) and depth of invasion (0.65 cm vs. 0.80 cm, p=0.73). The mean age was 60.8 years for the new technique group and 61.5 years for the conventional group (p=0.93).
The mean medial pathology margin however was significantly greater in the new suture technique group compared to the conventional group, 1.40 cm vs 0.88 cm respectively (p=0.04). No significant differences were found between the two groups for either the mean anterior margin (1.10 cm vs. 1.25 cm, p=0.79) or the mean posterior margin (1.47 cm vs.1.13 cm, p=0.15). Average tumor free margins were increased by 0.65 cm in the new suture technique group, although this difference was not found to be significant (p=.14).
Discussion
Adequate tumor resection is important for local disease control of oral tongue squamous cell carcinoma. Wide local excision of the tumor remains the primary treatment modality for this subsite as 5-year disease specific survival has been shown to be significantly lower when clear margins are not obtained (43% vs 59% for patients with pathologically clear margins) [6]. It has previously been shown that 84% of errors occurring during intra-operative consultation for margin adequacy were the result of incorrect sampling [7,8]. Also, repeat frozen sections impose potentially avoidable pathology expenses and operative fees to the patient. Our technique for partial glossectomy of early oral tongue cancers describes a simple approach to maintain consistency of pathologic margins and help improve accuracy. Tissue splaying and margin shrinkage are reduced as the horizontal mattress sutures preserve normal anatomic integrity and orientation.
This technique is quick and easy, especially for more anteriorly located oral tongue cancers. Larger lesions extending towards the tongue base can make placement of the sutures difficult however the senior author has used this method in T3 lesions including those that approach the tongue base. The technique is also easy to implement for surgeons in training as is the case in our practice. The scaffolding provides concrete landmarks to assist excision and prevent unnecessary manipulation and interruptions in the procedure to evaluate the surgical plane and margin. We have found that consistent margin distance is more frequently obtained using the horizontal mattress technique. We recognize that we have presented a small number of early stage cases; however, this is a reflection of our referred patient population which tends to be mainly those with advanced stage disease (T3/4) for which this technique has limited application i.e. composite resections with glossectomy for example. This study is also limited by the retrospective nature of the comparison group although they were age, sex, and stage matched. A prospective trial could be undertaken to confirm these results.
Introduction: The Gamma 3 nail is widely used for AO31A1-3 fractures. The aim of this study was to compare outcomes in patients with 31A2 fractures treated with two lengths of Gamma3 nail.
Material: A prospective study of 104 non-pathological 31A2 fractures treated January 2012-January 2014. 14 patients were eliminated due to inadequate follow up. Mean follow-up was 18 months (range 12-36). Average age was 81 years (range 50-99), 78% of the patients were female. We studied two groups: Long Gamma3 Nail (LGN) and Short Gamma3 Nail (SGN). Preoperative variables included: age, medical pathologies, gait, anesthetic risk, associated fractures, hemoglobin and hematocrit values. Postoperatively, we evaluated: functional and radiographic results, quality of life, hemoglobin concentration, hematocrit, transfusion, gait and pain. Intraoperative and postoperative complications were recorded: malunion, nonunion, infection rates, cut-outs and periprosthetic fractures.
Results: We obtained a correct reduction in 73% of cases. We found two intraoperative complications (greater trochanteric fractures) in two LGN cases. 38% of the patients with LGN presented nail tip impaction upon the distal anterior femoral cortex, associated with anterior knee pain. Blood loss was statistically different between groups but neither clinical outcomes nor quality of life presented any differences.
Conclusion: Our results with these two sizes of the Gamma3 Nail in 31A2 fractures showed no overall differences in clinical outcomes and complication rates. Despite this, the LGN presented a statistically significant higher decrease of the postoperative hematocrit and more transfused blood concentrates. We therefore recommend the use of locked SGN to treat the 31A2 fractures.
The treatment of proximal femoral fractures is a constant subject of interest due to their high incidence. The present study considers a particular type of fracture characterized by instability, also known as unstable intertrochanteric fracture. This fracture presents a special pattern with a fracture line extending from lateral-proximal to medial-distal affecting the lesser trochanter. The instability of these fractures is exerted by the iliopsoas muscle that inserts in the fractured lesser trochanter and therefore medializes the comminuted postero-medial cortex of the fracture; this reduces the area of contact between the two ends of the fracture, delaying bone callus formation and increasing the risk of implant failure [1]. This fracture´s controversy seems to center on the type of treatment used: extramedullary devices versus intramedullary nail [2-5]. The different biomechanical forces involved because the extramedullary devices to produce distraction of the fracture, which leads to a high percentage of implant failures. Few studies have examined the true behavior of intramedullary nails in these fractures, and the existing publications involve a great diversity of nails, thereby complicating interpretation of the results [6-11]. Many publications showed good results of former gamma nails to treat proximal fractures [12-17]. Recently, with the evolution of the gamma nail many studies published and compared the outcomes of the previous generations with the actual Gamma3 [18-24].
In order to study our experience at the Hospital Clinico San Carlos in Madrid, a retrospective study of the treatment of the intertrochanteric fractures with gamma nail was done [12]. In 2000 a total of 348 intertrochanteric femoral fractures, excluding pathological fractures were reviewed. Among the various data collected, the phenomenon of cut out screw was seen in 21 cases, which accounted for 8% of the series, being therefore the most frequent cause of reoperation. The study of these patients revealed the existence of a combination of factors that could be involved in the failure of the fixation [16]. Some years after, with the new nail generation, we decided to analyze if the results of the long dynamic gamma3 nail (LGN) were comparable to short static gamma nails (SGN) for the treatment of 31A2 fractures in our department.
Materials and Methods
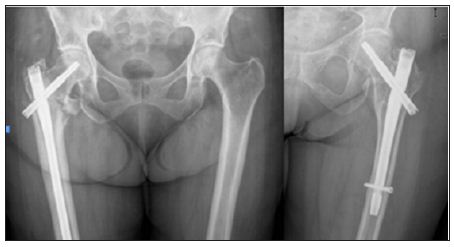
We present a prospective study of 104 non-pathological unstable trochanteric femoral fractures treated with the third generation of Gamma nail ® between January 2012 and January 2014. The patients were aleatorized and divided in 2 groups according to the implant: SGN or LGN (Figure 1). Mean follow-up was 18 months (range 1-3 years). 14 patients were eliminated from the study due to inadequate monitoring (one immediate postoperative death and 13 patients with incomplete record but intact implant in their last visit). The recorded preoperative variables included: patient age, associated diseases, type of gait, anesthetic risk, the presence of associated fractures, hemoglobin and hematocrit concentration and fracture etiology. The preanesthesic risk was collected using the ASA (American Society of Anesthesiologists) classification. The type of gait was classified according to the need of walking aids (cane or walker), the absence of walking ability or the capacity of the patient to walk autonomously without help of any kind. The fractures were classified according to the AO classification (Orthopedic Trauma Association) [6].
Figure 1: Plain radiographs of unstable pertrochanteric fractures treated with long Gamma 3 nail and short locked Gamma 3 nail.
Postoperatively, we evaluated the following parameters: hemoglobin and hematocrit concentration in the immediate postoperative period, the need for transfusion, the type of gait at discharge from the outpatient clinic and the presence of pain that was scored as follows: no pain, occasional pain, or disabling pain. Functional results and quality of life was queried. Radiographic evaluation was also made including the assessment of fracture reduction and evaluation of cephalic screw location. Intraoperative and postoperative complications were studied; such as malunion, nonunion, infection rates, cut-outs and periprosthetic fractures. Statistical analysis was performed using SPSS 15.0 (SPSS Inc, Chicago Illinois). Student t test was used to compare study outcomes with parametric means. Chi-square test and Fisher´s exact test were used to compare non-parametric means. To level of statistical significance was set as a two-sided P value of 0.05.
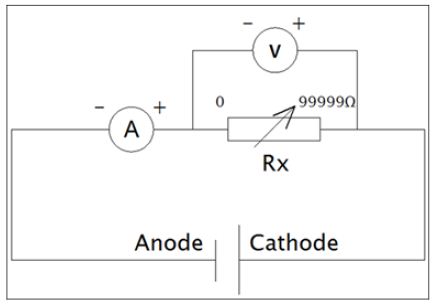
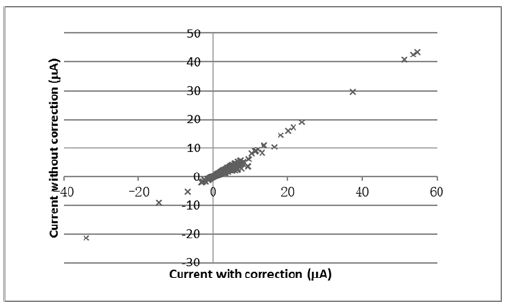
The internal resistance of the MFC was determined in a closedcircuit arrangement shown in Figures 1& 2. Closed circuit voltages were measured in different external resistance of 3,000Ω, 2,000Ω, 1,000Ω, 800Ω, 600Ω, 400Ω or 200Ω. Using the equation 1, the corresponding electric currents were calculated. A polarization curve, that was a plot of electric current with voltage, was generated, and the internal resistance Rint was determined by the slope of the regression [11]. Electric current with the correction of internal resistance was calculated as in equation 2.
Results
Preoperative Period
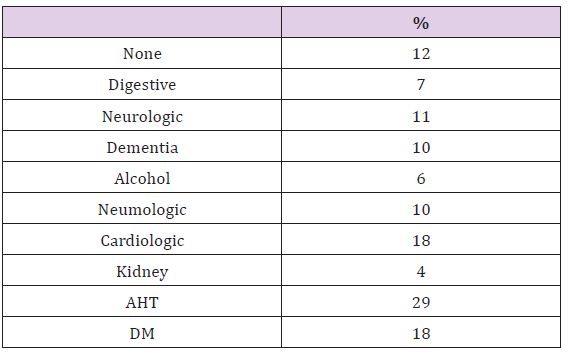
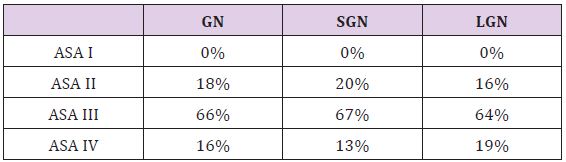
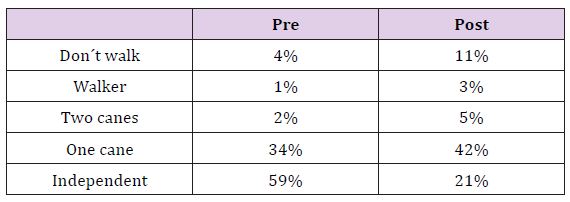
The mean age of the patients was 81 years (range 50-99) and 78% of the patients were female. The associated medical conditions are summarized in Table 1, and are seen to be very prevalent: 88% had at least one pathology and 62% had more than two. By means of the ASA classification: 44% of the patients corresponded to ASA II, 40% to ASA III and 16% were ASA III. The fractures were classified according to the AO classification: 31A2.1: 28%, 31A2.2: 34% and the most commonly found 31A2.3: 38%. We found associated upper limb fractures in 7.1% of cases (distal radius fractures and proximal humerus fractures). Other associated injuries were seen in 5% of the cases, the most frequent was traumatic brain injury which was usually mild. The quality of life prior to fracture was: 25% needed personal care assistance, 33% were independent at home, 39% were independent outside their home and only 3% were able to do physical activities. The type of walking was: 3% unable to walk, 25% used two sticks, 38% used one stick and 34% walked autonomously. The percentages shown refer to the total of patients, which suggests a very high rate of pathological associations in our patients. The two studied groups were homogeneous and the small differences seen in the distribution were not statistically significant (Table 2).
Table 1: Associated medical conditions.
Table 2: Preoperative Study/Implant used.
Surgery
The patients were operated upon following preanesthetic evaluation, an average of 3 days from admission. Spinal anesthesia was performed in 74% of cases, epidural anesthesia in 14% and general anesthesia in 12%. The most commonly used nail was the 130º cervical-cephalic angled nail (52%) and the most common length of the cephalic screw was 90 mm (33%). There were no significant differences between the distribution of angle and the length of the head screw used between both groups. The diaphyseal locking screw of the long gamma nails was dynamic while the short gamma nails had a static distal locking screw. The average time of surgery was 48 minutes (range 30-68). The only intraoperative complication found was a greater trochanteric fracture in two cases treated with long nails.
Postoperative Hospital Period
The local complications in the early postoperative period were limited to a single case of a significant hematoma. The most frequent general complications registered during the immediate postoperative period were urinary tract infection (no differences between groups). Mean hemoglobin in the immediate postoperative period was 9 g/dl (SGN9.5g/dl, LGN8.5g/dl), whereas the hematocritwas 27% (29.2%SGN, 26%LGN). The blood loss recorded was significantly lower in SGN (p=0.05). It was necessary to transfuse an average of 1.4 blood units / patient (SGN0.8, LGN1.65), this difference isn’t statistically but clinical significant.
Full limb loading was allowed after 24 hours. The hospital stay was on average 6 days including the preoperative period (5 SGN, 7 LGN). The destinations were elderly care homes, rehabilitation centers or secondary hospitals in 65% of cases and the patient´s home in 35% of cases. No significant differences were found in hospital stay or destinations.
Outpatient clinic
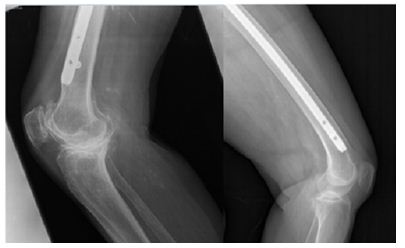
The mean time to fracture consolidation was 3.1 months without differences between groups. To be considered as consolidation an evident bone callus formation had to be present of both the anteroposterior and axial projection. Fracture reduction was evaluated in the postoperative x-ray. In 73% a correct reduction of the fracture was obtained (73% SGN, 74% LGN), 18.5% of the cases didn´t have medial cortex contact (21% SGN, 13% LGN), in 7% the lateral reduction was unsatisfactory (SGN 6%, LGN 10%) while 1,5% presented a complete lack of reduction (SGN 0%, LGN 3%), no significant differences were found. The placement of the cephalic screw was studied in both the anteroposterior radiographs and in the axial, without significant differences between the locations in both groups. In all cases treated with SGN the cephalic screw was placed in the two inferior thirds of the head and neck as in 97% of the LGN. Concerning the axial x-ray, both SGN and LGN head screws were placed in the posterior part of the head. The mean screwsubchondral bone distance was 9 mm (range 4-20 mm). 38% of the patients with LGN presented nail tip impaction upon the distal anterior cortical of the femur, this radiographic impaction was associated with pain in the anterior zone of the knee (Figure 2).
Figure 2:Plain radiographs showing a long Gamma Nail tip impaction upon the distal anterior cortical of the femur.
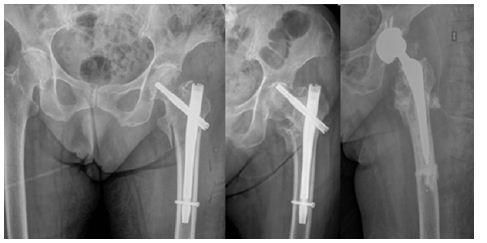
Since this situation is not to be found in the SGN group, it was a significant difference between the groups. There were not any statistically significant differences between groups concerning the late complications studied, even though they were more frequent in the LGN group. We found one case of delayed consolidation that required surgery revision with replacement of the LGN. We also had one LGN with cephalic screw lateral protrusion two months after surgery. Loading of the affected limb was avoided until complete consolidation was obtained and the material was finally extracted. Finally we found one SGN case of cephalic screw cut-off that required extraction and hip arthoplasty (Figure 3). The patients were discharged from the outpatient clinic after an average followup of 24.3 weeks (SGN 24, LGN 25, no differences found). Before the discharge the functional results were evaluated. The type of gait at discharge from the clinic is reported in Table 3. Sixty-eight percent of the patients were free of pain, however, 15% of the LGN reported discomfort in the anterior zone of the knee, 2% of these patients referred a disabling pain. In all cases this coincided with impaction of the nail on the distal anterior cortical layer of the femur but only 3 cases underwent surgery with removal of the implant. There were no statistically significant differences between groups about the lower limb pain. It was described as disabling by only 2% of all the patients.
Figure 3: Plain radiographs showing a case with cephalic screw cut-off that ended in arthroplasty.
Table 3: Gait pre- and post-operatively.
Discussiont
The results obtained with the two sizes of the Gamma3 Nail in unstable pertro chanteric femoral fractures did not show any important differences in neither clinical outcomes nor complication rates. Theses unstable fractures, also called 31A2 fractures account for 37- 42% of all intertrochanteric fractures of the femoral region [12,16]. The treatment of these fractures is subject to controversy, particularly concerning the use of intramedullary versus extramedullary devices. However, there is one point on which the different studies seem to agree: extramedullary sliding devices (e.g., SHS) are not adequate for fractures of this kind [2- 5]. As a result of their distinct biomechanics, these devices distract rather than compress the fracture fragments thus leading to a high percentage of failures. The great diversity of implants used within the same study contributes to perplex the situation. In series such as those published by Parker, Chinzei, Barton, Michael or Cheng, as many as four different types of nails have been used [6-11]. In our study we have only used the Gamma3 nail (Stryker Howmedica), a fact that allows us to adequately define its behavior. In unstable fractures, intramedullary nailing theoretically affords increased stability since the leverage is less and the proximal portion of the nail is supported against the proximal fragment. In our series, the percentage of implant failure (0,7% cutting phenomenon, 0,7% than with extramedullary fixation and slightly lower than other published intramedullary series [8,9].
Many studies have used intramedullary nails for the treatment of unstable trochanteric fractures [6-11]. On one hand the problem of these studies is that unstable fractures are not only A.2 fractures but also A1.3 and inverse fracture patterns (A3.1, A3.3) and on the other hand the series where only the A.2 fracture was contemplated, the patient series were of limited in size [14]. The advantages of the endomedullary nail are lesser blood loss and a lower percentage of failures, the latter being essential in order to avoid reinterventions that pose an important risks for the elderly patient [12,15,17]. On the other hand, the consolidation rate obtained is high (with only one case of pseudoarthrosis in our series), and with the use of short nails one of the most common complications in endomedullary nailing procedures is diminished: diaphyseal refracture fundamentally associated with the use of long gamma-nails (not seen in our series) [13]. Failure of closed fracture reduction is relatively infrequent, since perfect anatomical reduction is not necessary for implantation, the consolidation can be achieved provided that there is sufficient contact between the bone fragments. However, we agree that a positive medial cortical support allows limited sliding of the neck fragment and achieve secondary stability [8].
This leads to clinical-radiological discordance in many cases. The need to access the fracture focus is only considered in those cases where all the non-aggressive reduction options have been exhausted, and the open reduction might be related to pseudoarthrosis and intraoperative fractures. We agree with Pervez [14] and López-Vega [19] concerning the distal nail locking to get additional stabilization to the nail. In 13% of the patients the nail impacted upon the distal anterior cortical layer of the femur. This situation is more than a simple radiological finding, since in contradiction to others authors, impaction caused clinical manifestations in our patients (pain in the anterior knee region). This circumstance could be related to the characteristics of the femur in our elderly population, which are different to those found in the central European population [15]. The decision to adopt the Gamma3 Nail as our implant in this type of fractures was based on the findings of last year´s studies between the previous gamma-nail and the Gamma3, in which the Gamma3 afforded the best results [18-24]. We agree with most authors that the best way to prevent complications is to ensure a careful surgical technique, with special attention to medullary cavity drilling and the manual insertion of the nail [13]
In our study we recorded a single cutting phenomenon, in contrast to the 6% rate reported in another series reviewed in our hospital, involving 348 trochanteric fractures treated with the short gamma-nail, and where 37% were A.2 type fractures. This could, in part, be related to an improved surgical technique as well as the increased stability afforded by the long gamma3-nail, due to its lesser leverage and increased length [16]. There are no publications to be found that studies the difference between two different types of the same implant. Although our study are not enough to rise statistically significant differences between the groups some are clinical significant. The data obtained allow us to affirm that the clinical and radiological results with SGN and the LGN in the treatment of the AO/OTA 31A2 proximal femur fractures are similar. We found that there are statistically significant differences of transfused blood concentrates and higher decrease in the postoperative hematocrit, the LGN caused more blood loss and could there for potentially cause major medical complications. We found differences in favor of the use of SGN opposite the LGN, such as the presence of pain in the distal third of the femur as some late complications.
An Alternative Method to Reconstruct Severely Atrophic Mandible: Case Report
Introduction
The prosthetic rehabilitation of atrophic jaws has always been a challenge for the professionals involved in it. Depending on the degree of bone atrophy present not even the conventional prosthesis (dentures) cannot estore the aesthetics and function due to insufficient retention of the prosthesis, nerve compression pain, alteration of the proportions between the facial thirds and difficulties in the speech and Chewing. Due to increasing longevity, more active life and a growth in the elderly relationship in the percentage of the population, there has been an increase in the frequency of patients seeking the rehabilitation of the jaws for improving the quality of life.
The modern implant dentistry began in 1966 with the studies of Branemark precisely in this group of edentulous patients to enable aesthetic-functional rehabilitation through protocol type prostheses, where 6 implants were installed in the mandible and the patients received fixed prosthesis after 4 months. Branemark studies have demonstrated long-term predictable results being currently widely used for rehabilitation of these patients. The purpose of this article is to present a viable alternative to severely atrophied jaw rehabilitation with the use of osseointegrated implants and Branemark protocol prosthesis.
Case Report
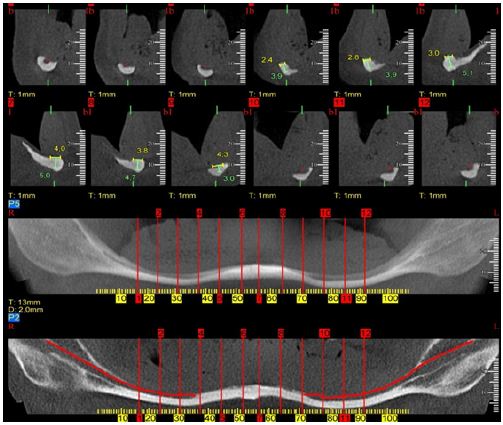
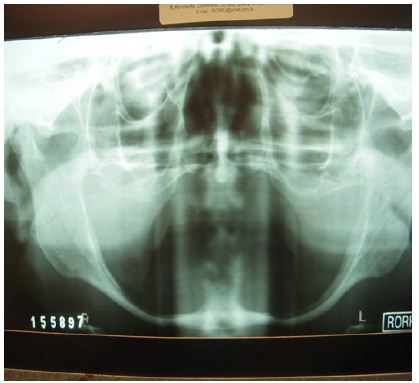
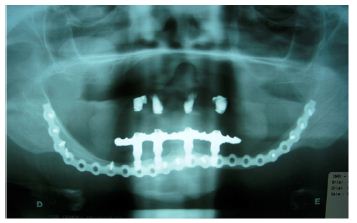
Patient, N.S.A, 72 years old, was referred to the private practice with complaints of feeding and phonation difficulties due to the impossibility of using her inferior prosthesis. She said that at the age of 20 she no longer presented teeth in the mandible and maxilla due to socioeconomic problems that motivated the extraction of decayed elements. A Cone Bean computed tomography scan demonstrated severe bone atrophy with bilateral total inferior alveolar nerve exposure and mean available bone height at the mandibular symphysis of 4 mm (Figures 1 & 2). For the imminent risk of pathological fracture of the mandible, the planned treatment for the patient was the placement of four Cone Morse WS (5.0×5.0mm) implants (Neodent, Curitiba, Brazil) at the mandibular symphysis associated with grafting with Bio oss® (Geistilich Pharma AG, Switzerland) for gain of 1mm in height.
Figure 1:
Figure 2:
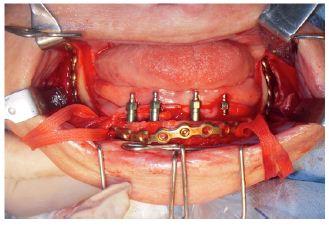
A Unilock® 2.0mm, 21-hole high profile (Synthes Maxillofacial, Paoli, PA) miniplate was used to strengthen the mandible using the area of the mandibular branches and mandibular symphysis for fixation (Figure 3). This plate was modeled prior to surgery with the aid of a biomodel made from the DICOM images of cone bean tomography. Pre-modeling of the miniplate allowed its insertion to be performed by trans-oral access, reducing the time and morbidity of the surgical procedure. After 4 months the creation of the Branemark protocol prosthesis type was started and the patient was extremely satisfied with the result obtained (Figures 4 & 5). After 5 years of radiographic control we did not observe perimplant or any intercurrent bone loss (Figure 6).
Figure 3:
Figure 4:
Figure 5:
Figure 6:
Discussion
The physiological changes associated with aging are factors that modify the physical, social and economic life of geriatric patients. These physiological changes may predispose or increase the susceptibility of elderly patients to dysfunction. The reduction of osteogenesis in elderly patients associated with loss of dental elements and consequent reabsorption of the alveolar bone are the main causes related to atrophy of the mandibular bone Bruce et al. [1]; Luhr et al. [2] developed a classification of the degree of mandibular atrophy with the purpose of establishing the level of difficulty in the treatment of fractures in atrophic mandibles. Jaws with 16-20 mm in height of remaining bone are classified as Class I.
Those with 11 to 15 mm of bone height remaining in Class II and finally those with less than 10 mm are classified as extremely atrophic or Class III. The classification of Cawood & Howell [3] evaluates the degree of bone resorption from the moment the tooth was extracted. This classification ranged from 1 to 6 with 6 being the bone resorption end with the maintenance of the basilar bone alone. In the case in question the bone height in the anterior region of the mandible varied from 3.9 to 5mm and in the region of mandible body was 2mm demonstrating a residual bone extremely susceptible to pathological fracture of the mandible. In the past different surgical techniques have been proposed to allow the rehabilitation of atrophic jaws, including osteogenic distraction, onlay grafts, sandwich osteotomy, osteotomy, and graft in mandible basilar bone.
Many of these techniques presented predictable results, however, with increased morbidity of the surgical procedure and some of them with more than one surgical procedure to allow definitive prosthetic rehabilitation. In addition complications such as infection, loss of grafts and fracture of the mandible have been reported and are complications of difficult solution mainly in this group of patients. Bosker in 1996 developed the trans-mandibular implant system to be used on severely atrophied mandibles. Although the original article and subsequent articles have never defined the term “severely atrophied mandible”, most patients included in these studies had residual bone in the anterior region of the mandible of 12 mm or less. The system consisted of a base plate that was attached to the basilar bone of the mandible that contained 4 trans-osseous pins where the prosthesis was made.
The disadvantage of this system is the need for extra-oral access for its insertion and the need for residual bone in the mandibular basilar of good quality for fixation of the anchor screws of the system. Some studies have shown success rates varying from 56% to 75% Bosker and VanDijk et al. [4-6]. In a study conducted in PubMed revealed 14 cases of atrophic mandible fractures secondary to the installation of implants in the anterior region in the period between 1990 and 2012. The authors excluded mandibular fractures secondary to lateralization of the inferior alveolar nerve associated with implant installation Almasri & El-Hakin, Karlis [7]. In most reports the fracture occurred distally the installation of the implants.
The first author to describe the technique used in this patient was Lopes et al. [8] combining concepts of treatment of atrophic mandible fractures and current concepts in Implantology, using a 2.0mm system locking plate and 04 short implants that supported a Branemark protocol type prosthesis. Later, Lopes Alvarenga et al.[9] published a clinical case where they used a locking plate of the 2,4mm system only in the anterior region of the mandible associated with 4 implants that supported an overdenture type prosthesis. The use of the locking plate in a severely atrophied mandible is justified by the necessity of support of the load bearing after the insertion of the prosthesis preventing the pathological fracture of the mandible. We understand that the region of the mandibular body is usually the region of greatest bone atrophy in extreme cases and due to the presence of the inferior alveolar nerve and inadequate bone height it is not always possible to use this region for plate fixation.
For this reason we understand that the plate has to be extended to the mandibular angle region bilaterally. In this case we chose to use 2.0mm system plate because of the low bone height available for fixing the screws. In a randomized clinical study comparing 3 treatment modalities (trans mandibular implant, autogenous bone grafting for vertical gain followed by the installation of 4 implants and the installation of 4 short implants) of severely reabsorbed jaws, Stellingsma et al. [10] concluded that the use of short implants was the best modality of treatment due to the low rate of complications, high implants survival rate, stable implant-bone interface and the possibility of outpatient treatment. Freiberg et al. [11] demonstrated predictable long-term success rates with the use of short implants (Branemark implants 6-7mm) in mandibles without the use of bone grafts (95.5% success rate at 5 years and 92.3% at 10 years of control). Deporter et al. [12] also demonstrated a 92.7% survival over 10 years with 0.03mm mean annual bone loss in short implants that retained overdentures [13-14].
WS Neodent implants were chosen due to the lack of availability of short implants in the national market at the time of surgery. The Cone Morse platform can be easily modified with the placement of tapered minipillars during the prosthesis preparation. As a conclusion, this technique allows the rehabilitation of atrophic mandibles with a single surgical procedure and lower morbidity when compared with bone grafting procedures. A careful medical evaluation of the comorbidities present in this group of patients should be performed as well as the discussion about the advantages, disadvantages and possible complications.
A Perceptive of Mass Spectrometry in Clinical Chemistry: Hyphenation for Benefit of Mankind
Abstract
Clinical chemistry is associated with the metabolonomics which is the characterization of metabolome, which is a set of small molecular mass organic compounds found in a given biological medium. Metabolonomics is very important for understanding the toxicity and biomarkers. Mass spectrometry is a very important analytical technique which is used extensive in clinical chemistry. Different types of mass spectrometers are available and thus there is an improvement in the field of clinical chemistry. This overview will touch upon the various aspects of both the clinical chemistry and the mass spectrometry.
Keywords: Clinical chemistry; Mass spectrometry; Ion suppression; Metabolome
Abbreviations: MS: Mass Pectrometry; SPE: Solid-Phase Extraction; NAPQI: N-acetyl-p-benzoquinone Imine; NIH: Institute of Health; HPLC: High-speed high Performance Liquid Chromatography; MALDI: Matrix Assisted Laser Desorption / Ionization; SELDI: Surface Enhanced Laser Desorption Ionization
Introduction
What is clinical chemistry?
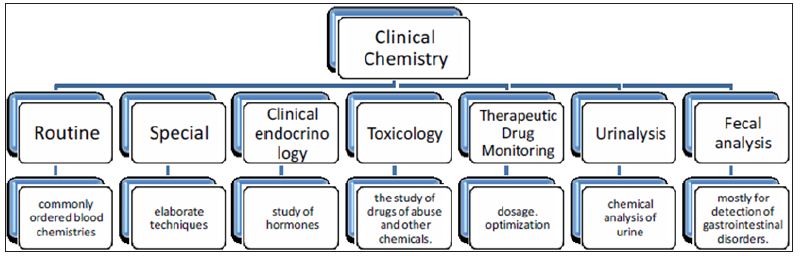
Clinical chemistry [1] can be defined as is the area of clinical pathology that is generally concerned with analysis of bodily fluids. It is also known as chemical pathology, clinical biochemistry or medical biochemistry. The initial study in clinical chemistry in late 19th century was the analysis of various components of blood and urine by simple chemical tests. Then the use of improved technology like spectrophotometric techniques made these analyses more easy and accurate as these are nowadays automated and can be used for a large number of samples. The different biochemical tests can be classified under chemical pathology and are performed mostly on the serum or plasma though can be applied to any body fluid. A large medical laboratory will accept samples for up to about 700 different kinds of tests. Even the largest of laboratories rarely do all these tests themselves, and some must be referred to other labs. This large array of tests can be further sub-categorised into sub-specialities as shown in the organization chart below (Figure 1). Thus it is clear that various types of analysts are present in the samples and techniques like mass spectrometry would definitely be an important tool in terms of sample throughput and detection limits.
Figure 1:
Simply put, mass spectrometry (MS) is an analytical technique that produces spectra (singular spectrum) of the masses of the atoms or molecules comprising a sample of material. The spectra are used to determine the elemental or isotopic signature of a sample, the masses of particles and of molecules, and to elucidate the chemical structures of molecules, such as peptides and other chemical compounds. Mass spectrometry works by ionizing chemical compounds to generate charged molecules or molecule fragments and measuring their mass-to-charge ratios [2-4]. In the present overview, the importance of mass spectrometry will be highlighted with reference to its use in clinical chemistry. Analysis of analyte is carried out in three stages of sample preparation, chromatographic separation and data collection and its interpretation. Each of these stages is extensive in nature and the details are available in literature [5]. This article will attempt to give a brief insight of the various aspects of mass spectrometry in clinical chemistry and the challenges normally encountered.
Experimental Aspects
Sample preparation prior to analysis by mass spectrometry is very crucial and the method adopted depends on the chemical characteristics of the analytes (acidic/basic, lightly/heavily bound) and sample type chosen for analysis (serum/urine). There are a large number of procedures like protein precipitation, liquid-liquid extraction, immunoaffinity purification, dilution and solid phase extraction. However in practice, it is usually a combination of all these procedures that are used [6-12]. This is because the sample matrix decides the procedure adopted. Blood samples are the most difficult samples that need sample preparation because of the complex matrix and low concentration of analytes in the sample. Urine samples can be diluted easily as the concentrations are often higher. Moreover the chemical differences between the analytes of interest and sample matrix decides the preference of sample preparation. Solid-Phase Extraction (SPE) is a separation process by which analytes are separated from matrix owing to differences in their chemical attraction for a solid through which the sample is passed (known as the stationary phase).
The portion that passes through the stationary phase is collected or discarded, depending on whether it contains the desired analytes or undesired impurities. If the portion retained on the stationary phase includes the desired analytes, they can then be removed from the stationary phase for collection in an additional step, in which the stationary phase is treated with an appropriate eluent. SPE results in a rudimentary separation of analytes from potentially interfering matrix components. Immunoaffinity purification (known as immunoextraction) uses antibodies bound to a solid phase to allow for separation of the antibody-bound analytes from the unbound matrix components. For samples with analytes at higher concentrations and less complex matrices, dilution of the sample can be carried out. Introduction of sample into mass spectrometer is an important aspect and it is commonly carried out using a chromatographic method in order to spread out the deliverance of analyte and components of matrix into the mass spectrometer. The chromatographic techniques involve Gas and Liquid Chromatography, wherein the mobile phases are gas (He) and liquid (mixture of aqueous and organic solvents) respectively. The column temperature affects the affinity of the molecules for the stationary phase thus is an important parameter for separating the volatile analytes from matrix components.
The hindrance of functional groups in the analytes in GC analysis can be reduced by derivatization of these compounds. GC-MS is used for comprehensive drug screening in the clinical laboratory. Liquid chromatography (LC) encompasses a variety of analytes and the need for derivatization does not arise. The ratio of the aqueous/organic ratio solvents in the mixture used as mobile phase alters the attraction power between the analytes/matrix with the stationary phase. LC separation though appear similar to SPE is far more precise than the latter.
Analysis by mass spectrometers is possible only when the analytes is in the form of gaseous ions. Therefore ionization methods (convert analytes in solution to gaseous ions) become an important part of mass spectrometry. The main ionization methods adopted in clinical chemistry are electro spray and atmospheric pressure chemical ionization. Electro spray ionization produces smaller droplets of the liquid eluting off from a chromatographic column using combination of voltage, heat, and air, thus increasing the charge per unit volume and the ions (including larger protein species) are sent into the gas phase for analysis by mass spectrometer. In Atmospheric pressure chemical ionization, ions are produced by vaporization of the sample and the electrical discharge produced by plasma, known as coronal discharge ionizes the sample. Different types of mass analyzers are available for analysis.
Basically a mass spectrometer uses a given molecule‘s mass/ charge ratio (m/z) to distinctively identify components of the sample. Different types of mass analyzers are available based on various characteristics like the mass range limit, speed of analysis, mass accuracy and resolution. Time-of-flight (TOF) mass spectrometers use an electric field to accelerate bundles of gas phase ions toward a detector and the time taken is dependent on the m/z of an ion (low m/z ions travel faster). TOF analyzers have in effect indefinite m/z range, very high sensitivity, mass accuracy, and percentage of ion transmission, but a limited dynamic range. Quadrupole analyzers have 4 parallel rods arranged in a square and the charge on these alternate at a set frequency to achieve balanced attraction and repulsion of the ion of interest and thereby a stable path is achieved.
The charge can be changed over the analysis period thus facilitating sequential detection. During the dwell time (period on a millisecond time scale, for which the analyzer remains at a given voltage and frequency), one m/z is detected. Quadrupole analyzers have a limited m/z range, high sensitivity and mass accuracy, but low percentage of ion transmission. Tandem Mass Spectrometry became popular as analyte identification using m/z (morphine / hydromorphone, has m/z peak at ~286) alone does not always give the required specificity. These spectrometers use multiple sets of quadrupoles arranged in series. A common tandem massspectrometry (MS/MS) analyzer will have 3 quadrupoles (referred to as a triple quadrupole mass spectrometer or – triple quad‖). There are many methods of analysis.
The methods of analysis based on linear quadropoles are extensively used in the clinical laboratories. The different methods differ on basis of selectivity of ions detected. Full Scanning is the acquisition of full-spectrum data from a sample and very useful in drug screening and is applicable to more than 200 different drugs or metabolites. However the main disadvantage is the lack of specificity and highly complex mass spectrum thereby reducing its use for routine analysis. When the analyte is known, then the voltage and frequency can be optimized to reduce the interferences from most of the other components in the matrix. This is known as selected ion monitoring (SIM). Thus in this monitoring, both selectivity and specificity for an analyte is high and the spectrum is less complex. It is used for the analysis of very long chained fatty acids. Multiple Reaction Monitoring (MRM) offers best specificity with mass spectrometry. The spectra obtained are less complex and can be used for drug confirmation testing.
Applications in Clinical Chemistry
MS-based analysis in clinical chemistry has been carried out since 1970s, based on targeted methods focusing on particular metabolites or chemical families [13-16]. Toxicological screening is very common in clinical chemistry and it is involved with the metabolomics [17-20]. The metabolome is a set of small molecular mass organic compounds found in a given biological medium. The analysis of complex proteins known as shotgun proteomics is carried out to a lesser extent. Metabolome consists of molecules that are metabolites (organic substances naturally occurring from the metabolism of a living organism). There are two different kinds of metabolites viz endogenous and exogenous metabolites based on their origin.
Endogenous metabolites could be classified as primary (directly involved in essential life processes e.g. amino acids/ glycolysis) and secondary (species for specific biological function e.g. hormones for mammals) metabolites. Exogenous metabolites represent the biotransformation or metabolism products of exogenous compounds, resulting from modification of the original molecule to introduce a functional group and/or conjugation in enzymatic conversion [21,22]. Metabolomics / metabonomics is the analysis of metabolome in a given condition. Nicholson’s definition underlines the role of two major scientific disciplines used in metabonomics: analytical chemistry and biostatistics. Metabolomics is based on the interpretation of data intended facilitate understanding of biological processes. Biological markers or biomarkers are measurable internal indicators of molecular and/or cellular alterations that may appear in an organism after or during exposure to a toxicant and possible disease [23-25]. According to the National
Institute of Health (NIH), a biomarker is -a characteristic that is objectively measured and evaluated as an indicator of normal biologic processes, pathogenic processes, or pharmacological processes to a therapeutic intervention [25]. Metabolites are highly diverse in chemical characteristics and therefore there is no single technique available for their analysis in biological media. Mass spectrometer is one such instrument for metabolite characterization [26-29]. LC/MS is a very important hyphenation technique used for the clinic chemistry. There are large numbers of reports on the analysis for different compounds to understand nephrotoxicity and hepratoxicity [30-33] by analysis of urine and serum samples. These studies were carried out to understand the mechanism or as biomarkers. Acetaminophen (also known as N-acetyl-p-aminophenol, APAP) is frequently used as a model drug for hepatotoxicity. Normally it is removed from the body through hepatic glucuronide and sulphate conjugation.
Presence of larger amounts results in production of reactive metabolites such as N-acetyl-p-benzoquinone imine (NAPQI) which form a conjugate with glutathione (GSH) and finally is degraded to mercapturic acid derivative that can be detected in urine sample. Thus to understand the mechanism of the changes due to toxicity, the mass spectrometric analysis of urine sample becomes helpful. Also NAPQI can also oxidize glutathione and itself form paracetamol [34]. When GSH is completely removed, the reaction with cell macromolecules occurs and this mechanism is given for understanding the hepatic necrosis that occurs. Mass spectrometric analysis of plasma samples could also be used for understanding the mechanism of hepatotoxicity using long-chain acylcarnitines as biomarkers. Studies could also be used to understand the effect of drugs and the time needed for these to cause some effects. Nowadays studies are also focussed on the understanding of various diseases including cancer [35-38]. Clinical diagnostic measurements are carried out to understand the differences between healthy and diseased states.
Pharmokinetics is a branch of pharmacology that deals with the study of the substances administered externally to a living organism. It derives its name from the Greek words pharmakon and kinetikos which mean drug and moving respectively. It is the study of tracing and monitoring the nature of the drug from the moment it is administered to the point where it is completely eliminated from the body. Pharmokinetics also gives an idea of the absorption and distribution of the drug, chemical changes in the body and the effects and routes of excretion of the metabolites [39]. The dose and site of administration of the drug can also affect its pharmokinetic properties [40]. Mass spectrometry is used for the studies of pharmokinetics as the matrix is very complex and there is a need for a technique which is highly sensitive. The most commonly used instrumentation is the LC-MS with a triple quadrupole mass spectrometer. The use of tandem mass spectrometry enhances the specificity. The determination involves the use of calibration curves and internal standards.
The blank samples prior to drug administration need to be done to ensure the validity of the determination as the sample matrix is quite complex. The calibration curves are mostly linear but the curve fitting with complex functions are also reported as the linear range is much lower than the concentration ranges normally encountered [41]. High-speed high performance liquid chromatography (HPLC) in combination with tandem mass spectrometry was used to analyze phenylbutazone and its metabolites and also propiopromazine and promazine.
Challenges in Clinical Mass Spectrometry
Ion suppression occurs when something present in the sample interferes with the ionization process of the analytes. The presences of none or less volatile components reduce the droplet formation and the efficiency of solvent evaporation, resulting in decrease of ion formation. There are various reasons like sample matrix, coelution that can cause ion suppression and these have detrimental effects on both electrospray and atmospheric pressure chemical ionizations. However it has been reported that the effect is more pronounced for electrospray ionization [42]. The studies on biological extract revealed that the main cause of ion suppression is the change in the properties of the spray droplet due to the presence of non-volatile / less volatile components [43]. The presence of non volatile materials like salts, ion pairing agents, endogenous compounds, drugs or metabolites result in the change in the efficiency of the formation or evaporation of droplet. This in turn affects the amount of charged ion that reaches the detector. The mass and charge of individual analytes can cause ion suppression. The molecules with higher mass will suppress the signal of the smaller molecules [44] and also the more polar analytes are prone to suppression [45]. There are different experimental procedures that can be adopted to evaluate the ion suppression. The response of instrument for different calibrators including any internal standards that are injected into the mobile phase. The comparison of the standards added to the pre-extracted samples before extraction or to the specimen matrix can also be used [46].
The different procedures can give different information. The data using the calibrators provides a check of the response value. However the other approaches can show the effect of sample matrix on the Mass spectrometry signal and give an idea whether the loss of signal is due to matrix or due to ion suppression. Ion suppression may result due to the presence of various specimens, both inorganic and organic. The effect of endogenous matrix on ion-suppression is understood by studies [46] wherein it is seen that the donor serum samples were subjected to three separation techniques namely solid-phase, solvent extraction and protein precipitation. To the extracts, caffeine solution was added and analyzed. The results showed that the three extracts contained endogenous components that produced ion suppression > 90% when compared with a caffeine reference solution of same concentration. The injection of drugs or metabolites that maybe present in the specimen is adopted as a coeluting drug does not produce similar mass fragments does not indicate that this compound may not cause ion suppression. The post-column continuous infusion (process of extracting chemical compounds or flavors from plant material in a solvent) into the MS detector [47,48] will give a constant response if there is no ionization interferences.
However, in practice it is seen that there is a suppression of signal corresponding to the void volume of column. The degree of suppression of signal and the time needed for full response is dependent on the nature of the compound [45], sample and its preparation method. It is also possible that ion suppression is not only limited to the column void or initial analysis. It can become more evident during subsequent injections. The ion suppression is also dependent on the concentration of the analyte as this is correlated to the ratio of matrix to analyte. van Hout et al. [48] showed that the ion suppression in the analysis of clenbuterol in urine was 37% and 69 % for a concentrations of 93 and 45 μg/L respectively. These studies showed the advantages of decreasing the matrix to analyte ratio and also the importance of validation of ion suppression measurements in the concentration levels of the analyte normally encountered. Apart from the sample matrix, various other factors also result in ion suppression. The chromatographic ion pairing reagents present in the mobile phase can also affect the signal intensity. Moreover, since these are present in the mobile phase, the effect on ion suppression will be observed throughout the analysis. The solution to this problem is to select an alternative ion pairing agent which is normally a weaker acid. This kind of approach is adopted where in acids like acetic, formic etc are used instead of trifluoroacetic acid.
However if the need to use trifluoroacetic acid arises, then its concentration can be reduced or surface tension lowering modifiers can be added to decrease the effect on ion suppression [49]. There is a process known as – TFA Fix‖ wherein the post-column addition of a sheath liquid of propanoic acid (10%) in 2-propanol is added. There are reports wherein 2-(2-methoxyethoxy) ethanol has been used as a signal enhancer [50] to eliminate the ion suppression due to acetate ions and a 100 fold enhancement was achieved. Another approach is to use the chromatographic conditions to enable the elution of compounds of interest in a region of low or no ion suppression. However this may increase the elution time [51]. As most of the HPLC assays include an internal standard, the conditions are modified so that both the compound of interest and internal standard coelute [52] and the ion suppression for both the compounds will be equal as the peaks coincide. If a stable isotope internal standard is available then the degree of ion suppression will be identical. However it is worth noting that even the use of an internal standard may not completely overcome the problems associated with the accuracy or precision of an analysis which is associated with ion suppression as the ion suppression results in decrease of signal and the signal to noise ratio will be reduced to such an extent that the accuracy and precision will be severely affected. Thus the evaluation of ion suppression is of great importance even when internal standard is used. The ion suppression is also an important parameter that has to be evaluated not only in ESI interfaces but also other MS techniques such as Fourier transform (FTMS), matrix assisted laser desorption / ionization (MALDI) and surface enhanced laser desorption ionization (SELDI) [53-55].
Summary
The metabolome is characterized by a large diversity of chemical structures. The use of LC-MS has gained popularity due to its versatility, sensitivity. This overview gave an insight to the some of the applications of LC-MS in clinical chemistry. The main focus of this over view was to give a simple picture of the both technical and non-technical aspects in a very concise manner. The applications of LC-MS in field of toxicology and as biomarkers have been touched upon. It needs to be understood that the field of clinical chemistry is one among its kind as the information needed is always growing and no study can final. The Literature of course gives the readers the understanding to these problems but in reality the toxicity could arise due to various complex factors and to understand these combinations of many targeted approaches are needed to provide the clinical chemist with the information.
However it is to be mentioned without fail that the constant improvements in mass spectrometry has improved the efficiency of the approaches by making it possible to identify metabolites of interest. Metabolomics is the combination of analytical chemistry, statistics and bioinformatics tools used separately or together to perform the various steps of sample preparation, viz, acquisition of metabolic fingerprints, automatic detection of ions, statistical analyses and identification. Each step is itself a complete science in its own way. The data generated is so large that it needs correct understanding and discrimination to be able to analyze them. This is one of the most important challenges in the field of metabolomics. The mass spectral libraries (available for APIMS- based metabolomics: mass spectral and CID mass spectral libraries) are useful for interpretation of biological datasets and to characterize unknown components. Ongoing improvement in this field is becoming a reality with the information obtained from various researchers and sharing of the spectral libraries in order to help in the characterization of unknown metabolites of toxicological and clinical relevance.
A Case Report about Small Intestinal Metastasis from Esophageal Carcinoma Combined with Bowel Obstruction
Abstract
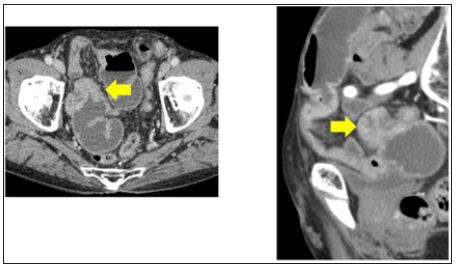
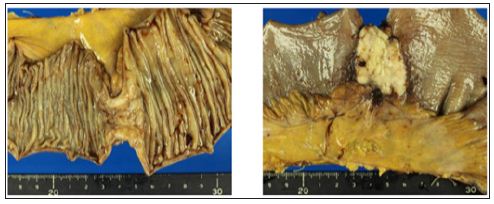
It is extremely rare for metastatic tumors derived from extra-abdominal sites to arise in the small intestine [1, 2]. Herein, we report a case of the metastasis of esophageal squamous cell carcinoma (SCC) to the small intestine. A 72-year-old male, who had previously undergone subtotal esophagectomy for esophageal carcinoma at our hospital, was admitted with abdominal pain and abdominal distension. Abdominal computed tomography revealed an increase in the thickness of part of the small intestinal wall, which had caused mild bowel obstruction. The patient had no severe symptoms, so we initially administered conservative therapy (a fast venal transfusion), and his symptoms temporarily improved. However, the ileus did not improve so we conducted laparotomy. A solitary tumor was identified in the ileum, which was determined to be the cause of the intestinal obstruction, but no other tumors were seen at intra-abdominal sites. Based on the postoperative pathological findings, the lesion was diagnosed as a metastatic tumor derived from esophageal SCC. After surgery, the ileus vanished, and the patient was discharged without symptoms. We encountered an extremely rare case of small intestinal metastasis from esophageal carcinoma.
Introduction
Recently, some cases of small intestinal metastasis from extraabdominal sites have been reported, but such cases are rare. In patients with esophageal carcinoma, we often encounter liver, lung, and bone metastases, but small intestinal metastasis from esophageal carcinoma is extremely rare. It was first reported by Wang et al. in 1985 [1-4]. Herein, we report a case of small intestinal metastasis from esophageal carcinoma combined with bowel obstruction. We had performed subtotal esophagectomy and 2-field lymphadenectomy because of esophageal squamous cell carcinoma (SCC) 6 years ago to treat the primary tumor.
Case Report
A 72-year-old male underwent subtotal esophagectomy and 2-field lymphadenectomy because of esophageal SCC in the middle thoracic esophagus (pT1bN0M0 stage II) 6 years ago [5]. After surgery, he received chemotherapy, involving 5-fluorouracil, cisplatin, and docetaxel, but it was interrupted during the first course due to kidney dysfunction. Four years and 9 months later, lung metastasis was detected in the right lung on computed tomography (CT). We performed a partial pulmonary resection and found other tumors, which were not detected on pleural preoperative imaging. All of the tumors were resected, and the diagnosis of metastasis from esophageal SCC was confirmed. No additional treatment was administered because the patient exhibited renal hypo function. One year later, some pleural dissemination and lung metastases appeared; however, the patient did not have any symptoms. He subsequently visited our hospital regularly. About 6 years after the subtotal esophagectomy, he presented to our hospital with abdominal pain.
A physical examination revealed slight abdominal pain in his lower abdomen, abdominal distension, and a surgical scar from the medial incision made in the abdomen during the subtotal esophagectomy. A laboratory analysis produced the following results: white blood cell count, 6.3 × 103/mm3 (normal range, 3.5-9.0 × 103/mm3); hemoglobin count, 10.8 g/dL (normal range, 13.5-18.0 g/dL); platelet count, 42.7 × 104/mm3 (normal range, 13.0-37.0 × 104/mm3); total bilirubin, 0.5 mg/dL (normal range, 0.4-1.5 mg/dL); albumin, 3.3 g/dL (normal range, 4.1-5.1 g/dL); C-reactive protein; 3.68 mg/dL (normal range, 0-0.3 mg/dL); blood urea nitrogen, 60.0 mg/dL (normal range, 8.0-20.0 mg/dL); and creatinine, 1.71 mg/dL (normal range, 0.-1.1 mg/dL). The patient’s serum level of SCC antigen was 10.8 ng/ml (normal range, <1.5 ng/ ml), and his serum level of carcinoembryonic antigen was 6.6 ng/ ml (normal range, <5 ng/ml). All of these parameters, except the white blood cell count and total bilirubin level, exhibited abnormal values.
Abdominal CT revealed an increase in the thickness of part of the small intestinal wall, which had caused bowel mild obstruction (Figure 1). It was possible that the patient had a malignant neoplasm, such as small intestinal carcinoma or a gastrointestinal stromal tumor. His symptoms included slight abdominal pain and abdominal distension, so we initially administered conservative therapy, and his symptoms temporarily got better. However, his ileus did not improve so we conducted a laparotomy. A solitary tumor was identified in the ileum about 80 cm proximal to the terminal ileum, and it was determined to be the cause of the bowel obstruction. No other tumors were seen in the abdominal cavity, including the small intestine (Figure 2). Thus, we conducted a partial resection of the small intestine.
Figure 1: Abdominal CT revealed that part of the small intestinal wall had become thicker, causing bowel obstruction.
Figure 2: A solitary tumor was identified in the ileum about 80 cm proximal to the terminal ileum, and it was determined to be the cause of the patient’s bowel obstruction.
Macroscopically, the surgical specimen contained a mass measuring 3.0 × 2.5 cm in size, and it occupied the whole circumference of the ileal lumen, resulting in stenosis (Figure 3). Histologically, the lymphatic sub mucosal infiltration of viable SCC tumor cells was observed from the mucous membrane to the serosa. These histological findings revealed that the metastasis was not derived from peritoneal dissemination. In addition, there was no mesenteric lymph node metastasis from the SCC. The patient was discharged without symptoms, but ileus appeared again at 1 month after the partial resection of the small intestine, and so he was re-hospitalized. CT showed that the lung and liver metastases were getting worse, and some bone metastases had appeared.
Figure 3: The surgical specimen contained a mass measuring 3.0 × 2.5 cm, and it occupied the whole circumference of the ileal lumen.
Discussion
Some types of cancer are reported to be associated with intestinal metastases, such as lung cancer, breast cancer, and malignant melanoma. However, metastatic intestinal tumors derived from extra-abdominal sites are very rare [1,2]. We usually examine esophageal cancer patients for liver, lung, and bone metastases, whereas intestinal metastatic tumors derived from esophageal cancer are extremely rare [3,4]. SCC of the esophagus is characterized by extensive lymphatic dissemination via the longitudinal lymphatic system, which runs along the esophagus and drains into the large number of (widespread) lymph nodes found in the thorax and abdomen [6]. It has been reported that the retrograde spreading of esophageal SCC cells into the cervical, mesenteric, or iliac lymph nodes is unusual [7,8].
The intra-abdominal region can be reached from the esophagus via the lymphatic network connecting the esophagus and intestines, lymphatic embolization, and peritoneal seeding of the tumor during surgery. The intra-abdominal region can also be reached via the hematogenous route, especially via the vertebral venous plexus [9,10]. In esophageal cancer, metastases can arise in the intestinal tract via any of these routes. In our case, it is unlikely that tumor seeding during the operation was responsible for the patient’s metastasis because only one small intestinal metastatic lesion formed. Microscopically, the lymphatic submucosal infiltration of viable SCC tumor cells was observed. Based on this finding, lymphoid metastasis is the most likely mechanism by which metastasis occurred in this case, but hematogenous spread cannot be excluded.
One interesting aspect of this case is why the solitary metastasis occupied the whole circumference of the ileal lumen. The lymphatic network develops on the mesenteric side of the small intestine, so mesenteric dissemination via the lymphatic network usually causes metastatic lesions to appear on the mesenteric side, as is seen in breast cancer. This might be explained by the characteristics of SCC. There have been several reports about small intestinal metastasis derived from esophageal SCC [3,4,11]. The tumors in these cases were detected based on their clinical symptoms, such small bowel obstruction and perforation, or were detected via imaging in symptomless patients.
In some cases, multiple metastases arose. In our case, an isolated small intestinal metastasis derived from esophageal carcinoma caused small bowel obstruction. The patient was disease-free for about 4 years and 9 months after undergoing subtotal esophagectomy until a metastatic lesion developed in his right lung. After undergoing partial intestinal resection, he wasdischarged, but the ileus recurred. CT showed that the lung and liver metastases had got worse, and some bone metastases subsequently appeared. Small intestinal metastases derived from esophageal carcinoma might be a significant finding that is generally associated with a poor prognosis. In conclusion, intestinal metastatic tumors derived from esophageal cancer are extremely rare. In addition, such tumors can develop with or without symptoms. Thus, physicians should keep in mind the possibility of small intestinal metastasis derived from esophageal carcinoma when patients who have a history of advanced esophageal cancer present with acute abdominal problems, such as bowel obstruction or perforation.
A Technique to Monitor the Real-Time Proton Leak Status of Cells
Introduction
Proton leak was a detour of protons from their original path leading to the reduction of mitochondrial membrane potential. It leads to the decrease of ATP production per glucose molecule. It is a form of energy loss [1]. Proton leak was found to reduce the reactive oxygen species (ROS) level [2]; therefore, it plays a role in aging [3], diet [4-5] and health [6-9]. A method to monitor the real-time proton leak in cells would help for the understanding of physiological system and disease conditions. When protons were leaked out from mitochondria, it increased the leaking of electrons from electron transport chain [10]. The leaked electron would generate electric signal in Microbial Fuel Cells (MFC). Measuring the electric signal sent out during the process of proton leak would be a way to quantify thereal-time status of proton leak in live cells. Theoretically, higher the electric signal means higher is the proton leak. However, the accuracy of MFC measurements is influenced by the internal resistance of the apparatus. The internal resistance is contributed by the activation loss from electron transfer from cells to the anode, the characteristics of cellular metabolism, the flux of reactants and ohmic loss [11].
Activation loss and cellular metabolism are cell-specific, while flux of reactants and ohmic loss arise more from the MFC equipment and operating conditions, for example the resistance of the electrodes and membrane, the conductivity of the electrolyte solutions and the quality of the electrical contacts [12]. However, the measurement of internal resistance was very time consuming. Therefore, experiments were done to see if there was correlation between electric current with and without correction.
Methods
MFC has two chambers, a cathode and an anode, that are separated by a proton exchange membrane. The cathode was filled with 100ml of 50mM potassium ferricyanide (III) (C6N6FeK3) to function as an electron acceptor, while 100ml of isolated cells (4 x 107 cells/ml) were added to the anode as electron donors. Nitrogen gas was pumped into the anode chamber for 5 min to remove oxygen from the headspace of the anode. A carbon electrode was placed in each chamber connected with external wire that are connected with a digital multi-meter (Tektronix DM4020, USA) to monitor the open circuit voltage (EMF) across the electrodes. Current I, without correction for internal resistance, was calculated using equation 1 with an external resistance (Rext) of 1000Ω.
EMF=IRext (1)
The internal resistance of the MFC was determined in a closedcircuit arrangement shown in Figures 1& 2. Closed circuit voltages were measured in different external resistance of 3,000Ω, 2,000Ω, 1,000Ω, 800Ω, 600Ω, 400Ω or 200Ω. Using the equation 1, the corresponding electric currents were calculated. A polarization curve, that was a plot of electric current with voltage, was generated, and the internal resistance Rint was determined by the slope of the regression [11]. Electric current with the correction of internal resistance was calculated as in equation 2.
EMF=I(Rint + Rext) (2) (Figure 1)
Figure 1: Electrical circuit diagram for internal resistance determination.
Figure 2: Plot of electric current without corrected with internal resistance versus electric current with correction (correlation coefficient = 0.9913).
Result and Conclusion
A good correlation was observed between electric current with or without correction (Figure 2). It indicated that it was possible to use the electric current without correction to correlate with the degree of proton leak in cells. When the experimental conditions were consistently controlled, the changes in electric signal should reflect to the biological changes in cells. In this experiment, 30-minute survival was good for the hepatocytes the cells used in the studies, which further supports the use of MFC in monitoring the proton leak status of live cells. The present technique had advantages over other chemical testing method, because it provided instantaneous information on metabolic changes in tissues.
A Cross-Over Study to Evaluate the Effect of Glucagon-Like Peptide 1 on Women with Polycystic Ovarian Syndrome
Abstract
Background: Crossover design is very popular for a study of new and developmental drugs. However this design tends to be misused regardless of whether it is suitable for underlying research questions.
Method: Given that in clinical practice 2×2 cross over is the most commonly used design, the Hills- Arbitrage approach is suggested to analyze data. Furthermore, we propose fitting a linear mixed model and then conducting a likelihood ratio test to yield a single p-value on data with multiple time points within each stratum.
Finding: Applying these methods to a real data, we evaluate effect of glucagon-like peptide 1 (GLP-1) on women with polycystic ovarian syndrome (PCOS). Despite absence of statistically significant results, this study as the first study to explore direct administration of GLP-1 to PCOS women is nevertheless clinically meaningful. Not only does it show a longer washout period is desired, but also it suggests GLP-1 may have the same positive effect on PCOS as MET does.
Improvement: A larger parallel study is warranted, and clinicians and biostatisticians should collaborate more so that data can be analyzed appropriately and interpreted from both statistical and clinical points of view.
In a crossover study, subjects receive a sequence of different treatments in a random order usually separated by a washout period. One major advantage of the crossover design is that the trial requires fewer patients to produce the same precision as a parallel trial, since each subject receives all treatments and thus serves as his or her own control. However, with data from crossover design trials, it is difficult to separate out treatment effects from both period and carry-over effects. Unlike a parallel clinical trial, a crossover study is typically longitudinal. However, entry- level data analysts tend to ignore the longitudinal data structure and adopt over-simplified methods intended for cross-sectional studies Mills [1] . Even when the longitudinal data structure is taken into account,period and carry-over effects are still often ignored. For example, the typical 2×2 crossover design is often mistakenly analyzed by a paired t-test Diaz-Uriarte [2,3]. Another tendency is to report the results separately for each sequence, i.e., AB and BA separately, which ultimately yields two separate estimates for the treatment effect, sometimes conflicting conclusions in which one sequence indicated treatment effect while no or hazard effect in the other.
The linear mixed effects model (LMM) and the generalized estimation equations (GEE) method are two appropriate and commonly used approaches for longitudinal data. In fact, when Zenger and Liang. Reviewed potential applications of their milestone work, GEE, they specifically used a 2×2 crossover design as an example. Unfortunately, these methods can appear computationally complicated and theoretically difficult for a clinician or an entry-level statistician. Yet in clinical practice, a 2×2 crossover design is the most commonly used design. We suggest to use the Hills-Arbitrage approach Grizzle, Hills and Arbitrage [1,4,5] to analyze data from such a design. The Hills-Arbitrage approach is essentially a two-sample t-test for a continuous variable, and is thus likely to be familiar to clinicians and entry-level statisticians. Furthermore, it had been demonstrated there were connections among LMM, GEE, and Hills-Arbitrage approach by Diaz-Uriarte [4], thus adding further appeal to the Hill-Arbitrage [1] approach. Further, we propose fitting a linear mixed model and conducting a likelihood ratio test to yield a single p-value on data from a 2×2 crossover study with multiple time points longitudinally measured within each sequence and treatment stratum. Clinicians are often concerned about whether there is a treatment effect, and thus having a single p-value on which they can make a decision is a very appealing feature. Polycystic ovarian syndrome (PCOS), a common endocrine disorder affecting 5-10% of reproductive-aged women, is a common cause of menstrual irregularity, hirsutism, and anovulatory infertility Knochenhauer, Asunción [2,6] So far, the crossover design is also a prevalent choice of evaluating the treatment effect of an intervention to PCOS, e.g., Wang [7]. It has been reported that women with PCOS may have altered in cretin hormone response Svendsen [8]. Metformin (MET) is widely used as a treatment for PCOS, probably by increasing glucagon-like peptide 1 (GLP-1) biosynthesis and secretion, thus increasing the incretion effect Svendsen [8]. This motivated us to propose direct administration of GLP-1 to women with PCOS.
Materials and Methods
Hills-Arbitrage approach: First, we give a brief describe on Hills-Arbitrage approach. Using the notation in (Diaz-Urinate 2002; Jones and Ken ward 2003), the statistical model for a 2 by 2 crossover study can be expressed as,
where πj is the period effect for the period j=1, 2, τ d is the direct treatment effect for the treatment d=A,B, Sik is the random subject effect for subject k in sequence i, and eijk is the random noise for subject k in period j and sequence I, and it is assumed that eijk ~ N (0, σ ) 2. Without loss of generality, the response variable yijk is assumed to be quantitative and to have a normal distribution. For each sequence (i.e., AB and BA), the treatment difference was calculated, yielding d12AB, namely, Y1AB -Y2AB and d21BA, namely, Y2BA-Y1BA. The Hills- Arbitrage approach tests the treatment effect (or treatment difference between A and B) by averaging the means of d12AB and d21BA. With some algebra, it can be shown that the estimator given by HA approach is unbiased for the treatment difference,τ 1– τ 2. In addition, one half of the difference between the means of d12AB and d21BA can be used as a test statistic to evaluate the period effect. Even though there is no specific parameter for the sequence effect in Equation 1, the inequality of carry-over effect in both sequences still can be tested by comparing Y1AB +Y2AB with Y1BA+Y2BA. When this is tested to be statistically significant, the Hills-Arbitrage approach suggests a two-stage procedure to evaluate on the treatment effect because the average between the means of d12AB and d21BA is subject to biases. This procedure was criticized by Freeman, Senn [6,9,10] mainly for its inflated type I error and thus potential misleading conclusions. For detailed descriptions on the Hills-Arbitrage approach, see Hills and Arbitrage, Diaz-Uriarte [1,4]. Also, interested readers are referred to Senn [9] for the diagram of the two-stage procedure of HillsArbitrage approach.
The Approach for 2×2 Longitudinal Cross-Over Design
To implement the Hills-Arbitrage approach more smoothly, we may rewrite the statistical model in Equation 1 as below,
Where I(x) is an indicator function and equals to one if x is true, 0 otherwise. Sik and eijk are the same as in Equation 1. In this equation, it can be easily shown that β 3 is the parameter representing treatment effect. β 1 corresponds to period effect, and β 2 corresponds to carry-over effect, providing a means to test the inequality of carry-over effects in both sequences. Using these indicators, all effects of interest are presented by a single coefficient. In a longitudinal crossover study (without loss of generality, suppose there are only 2 time points), Equation 2 may be then extended to include time points,
Where if both β 3 andβ 6 are zeros, there is no differences between A and B at either time point. The simpler model without these two parameters (the corresponding model under the alternative hypothesis) is nested within the above model (the model under the null hypothesis), thus a likelihood ratio test can be used to examine which model is a better fit. Similarly, if both β 1 and β 4 are zeros, there is no period effect. And if both β2 and β 5 are zeros, carry-over effects for both sequences are equal at either time point.
Miscellaneous
Baseline characteristics (such as age, BMI) were presented as median and Inter-quantile range (IQR). A Wilcoxon test was conducted to determine if a specific characteristic variable has the same distribution between two sequences of this crossover study. Data on those markers (e.g., GLP-1, LC) were log-transformed. A p-value < 0.05 is regarded as statistical significance. The statistical analysis was carried out in the R language version 3.1(www.r- project.org).
Experiment and Data
In this study, there were 28 PCOS accompanying with hyperinsulinemia women without use of any drugs known to alter glucose and insulin metabolism within 3 months before the study. The study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committee of Jilin University. These participants were randomized into either MET/ GLP or GLP/MET group (14 subjects in each group), and given MET (0.5g tid) and GLP-1 (5ug during the first month, then followed by 10ug for a duration of 2months) for a period of 3months. After 10 days of washout, they were crossed-over to the other treatment. Venous blood was drawn for the detection of blood lipids including triglyceride (TG), total cholesterol (TC), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) using biochemical methods (Beckman, USA), the detection of 6 sex hormones including familial hyper cholesterolaemia (FH), follicle-stimulating hormone (FSH), estradiol (E2), testosterone (T), luteinizing hormone (LH), and prolactin (PRL) using radio immunoassays, the detection of fasting blood glucose levels using an oral glucose tolerance test (OGTT) with 75 g of glucose, the detection of 1-h postprandial blood glucose, and the detection of 2-h postprandial blood glucose (BIOSEN5030 blood glucose analyzer). In addition, insulin, C-peptide (electro chem. iluminescence immunoassay, Roche, Germany), active GLP-1, and total GIP levels (Enzyme-linked immuno sorbent assay, ELISA) were measured during fasting (0 min) and 15min, 30min, 60min, 120min, and 180min after glucose administration. All these measurements took place repeatedly at the baseline and at the end of each period.
Table 1: The baseline characteristics (median + IQR for continuous variables).
Results and Discussion
The primary objectives of this study are to compare the effects of MET vs. GLP-1 on women with PCOS accompanying with hyper insulinemia and to assess whether GLP-1 has beneficial effects on PCOS. More details of the study are provided in the Methods section. Our cross-sectional analysis on the 2×2 crossover data indicated there is no difference between GLP-1 and MET (Tables 1 & 2). However, there might exist a period effect (e.g., p=0.0039 and 0. 0029 for progesterone and PRL, respectively) and inequality of carryover between two sequences (p=0.0307 for testosterone). The washout period of 10 days was chosen based upon our preliminary studies (unpublished work) on the pharmacokinetics behaviors of GLP-1. Considering this is the first experiment testing the effect of GLP-1 on PCOS and the first test implementing crossover design, it remains unclear whether 10 days is sufficiently long to wash out the effects of GLP-1 or MET in either sequence. Our analysis suggested a longer washout period for GLP-1 might be required. (Table 3) no statistically significant difference between GLP-1 and MET on summarizes the treatment effect and period effect estimates at longitudinally measured markers, i.e., glucose, insulin (INS), and C- each time point for the longitudinal 2×2 crossover data. There is peptide.
Table 2: The comparison between GLP-1 and MET on simple endpoint.
Note: The values of these markers were logarithm transformed. * p<0.05.
Table 3: The comparison between GLP-1 and MET on multiple endpoints.
Note: The values of these markers were logarithm transformed. *p<0.05.
For the period effect testing, all p-values at all time points were bigger than 0.05 for the analysis on glucose. Based on those p-values, it may be concluded that no period effect for glucose since there exists no period effect at each time point. However, for INS and C-peptide, no definitive conclusion can be drawn because inconsistent p-values were obtained at different time points. Thus, we conducted a likelihood ratio test (see the Materials and Methods section for more details) to obtain a single p-value. P-values are 0.6921, 0.0009, and 0.0052 for INS on treatment (GLP versus MET) effect, period effect, and carry-over, respectively. P-values are 0.8181, <0.0001, and 0.0036 for treatment effect, period effect, and carry-over, respectively. It is evident that both the period effects and inequality of carryover in two sequences exist in the study. Interestingly, as shown in (Figure 1), there is an obvious pattern in the treatment difference of C-peptide and INS between GLP-1 and MET over time in spite of no statistical significance. For C-peptide, the differences reached their nadirs at the extreme time points and their peak at the middle time points (although for the GLP1- MET sequence, the peak was attained earlier than for the MET- a sharp decline followed by a gradual ascent. Further investigation GLP-1 sequence). Meanwhile, the change patterns for INS were is warranted on the biological implication beneath those patterns. approximately identical for both sequences, i.e., peak at 30 minutes, a sharp decline followed by a gradual ascent. Further investigation is warranted on the biological implication beneath those patterns.
Figure 1: Change pattern of the treatment difference between GLP-1 and MET over time. A. C- peptide: the differences reached their nadirs at the extreme time points and their peak at the middle time points. B. INS: the change patterns for INS were approximately identical for both sequences.
Conclusion
The crossover design is very popular for the study of new and developmental drugs. However the crossover design tends to be adopted for its sample size savings, but without regard to whether such a design is suitable for the research question Mills [11] . Furthermore, a naïve method of analysis (e.g. paired t-test) that ignores the complexity of the design is often chosen. Another misleading preference is to obtain separate treatment effect estimates for each sequence or for each period, which sometimes yields inconsistent messages and inconclusive results. Even with consistent estimates, there is nevertheless no overall estimate of the treatment effect. Badly, these results often contribute as preliminary evidence in the literatures. Given that GEE and mixed models, two major methods used to analyze the data from a longitudinal study, are complicated for a clinician, Hills-Arbitrage approach turned out as a handy tool to deal with a crossover study. This approach is essentially a pooled t-test, and thus can be easily implemented with the aid of any statistical software. When we applied the Hills-Arbitrage approach to a PCOS data, no statistically significant results came up. First, we emphasize that GLP-1 is compared with another active agent MET, right now we only can not find evidence to support that GLP-1 is superior to MET. That cannot exclude the possibility that both GLP-1 and MET might have equal beneficial effects on PCOS in the considered markers (i.e., glucose, INS, c-peptide) herein. Also, another experiments conducted by us showed (unpublished work) that GLP-1 did improve upon some biomarkers and clinical outcomes (e.g., pregnancy).
Second, the size of this study is small even though the sample size calculation at the planning stage of this study indicated 14 per group can provide a good enough power, which was based on a large predetermined difference between the GLP-1 and MET groups. Our results may have yielded different results if we had powered the study to detect a smaller, yet still clinically significant, treatment difference. In this study, we used the raw data and have them log- transformed. Let Y1, Y2, Y3, Y4 represent period 1 baseline, period 1 outcome, period 2 baselines, and period2 outcome, respectively. Some clinicians questioned that why not use the change from the baseline instead. As demonstrated by Senn [12] that unless there is a very long washout period, the estimator using the raw data (Y2, Y4) is more efficient than that using the change from the baseline (i.e., Y2– Y1 and Y4– Y3) . Let alone there is no baseline measures (i.e., Y3) at the second period (right after the washout) in this study. If as suggested by them, the changes from the first baseline measures were evaluated (i.e., Y2-Y1and Y4-Y1 the results for treatment and period effect tests will be the same as two Y1 are cancelled out each other. For the effect of including baseline measures on carryover test, the interested readers are referred to Freeman [11] for details. However, it is always good to incorporating the baseline measures as a covariate, as suggested by Fleiss [12-16]. The results of such analysis are not shown here because of approximate same results produced. Despite the absence of statistically significant results, this study, being the first study to explore the effects of direct administration of GLP-1 to PCOS patients, is nevertheless clinically meaningful. Not only does it show a washout period longer than 10 days is desired, but also it suggests GLP-1 may have positive effect on PCOS. Certainly, a larger study using a parallel design is warranted to evaluate the treatment effects of GLP-1 on PCOS thoroughly.
Flavanoids from Saraca asoca– Ideal Medication for Breast Cancer: A Molecular Simulation Approach
Abstract
Breast cancer is one of the major causes of mortality in women. The estrogen receptor becomes positive in such patients. Many of the currently available anti breast cancer drugs produces severe side effects. It demands natural products with low toxicity to fight against estrogen receptor. In this point, we tried to establish antiestrogen potential of some natural flavonoids from the bark of Saraca asoca. The vitality of these drugs is well described in terms of pharmacokinetic parameters and molecular orbital analysis. In the light of molecular simulation studies we reports a set of lead compounds having natural origin in the treatment of breast cancer.
Keywords: Breast cancer; Estrogen receptor; Flavanoids; Catechins; Saraca asoca
Introduction
Breast cancer is one of the most widely affected malignancies in women, with 2,52,710 new case reports and death of 40,610 in 2016 [1]. It is well known that breast cancer is associated with steroid hormone estrogen receptor (ER) and it becomes the best target for the development of therapeutics [2]. Tamoxifen is one of the commonly used antiestrogens in the treatment of breast cancer, which act as a selective estrogen receptor modulator (SERM) [3]. But it harmfully affects oncologic, musculoskeletal, metabolic, hepatic, cardiovascular and even nervous systems [4- 9]. Hence it is necessary to suggest natural medications which are of low toxicity than tamoxifen for the metastasis in breast cancer. Saraca asoca possess various medicinal values, its stem bark is the principal constituent of major ayurvedic preparations for leucorrhoea, haematuria, menorrhagia and other diseases of the female genitourinary system [10]. Saraca asoca was extensively interpreted for its anti platelet aggregation, cytotoxic, anti inflammatory anti acne and anti oxidant activities [11-15]. The dried bark extract of Ashoka mainly contains lignan glycosides and flavonoids [16]. The flavanoids includes catechin monomers such as catechin, epicatechin, epigallocatechin, leococyanidin, gallocatechin and leucopelargonidin [17]. The importance of three dominant polyphenolic catechins-epigallocatechin, epigallocatechin gallate and epicatechin gallate in breast cancer cell proliferation was reported in 2002 [18]. Ryoko et al. studied the simultaneous effect of tea catechins in anti estrogenic activity [19]. As part of our interst in the development natural anticancer therapeutics, we are concentrating to elaborate the ER inhibitory activities of monomeric catechins from Saraca asoca and defined it as an ideal medication for breast cancer based molecular simulation studies.
Methodology
The crystal structure of ER (PDB ID: 3OS8) was retrieved from RCSB Protein Data Bank [20]. The X-ray crystal structure has a resolution of 2.03Å and it contains 258 amino acids. It was cleaned and prepared for docking studies using Protein preparation wizard of Schrodinger suite 2017-2 [21]. The different conformers of the ligands-catechin(+) (1), catechin(-) (2), epicatechin(+) (3), epicatechin(-) (4), epigallocatechin(+) (5), epigallocatechin(-) (6), leucocyanidin(+) (7), gallocatechin(+) (8), gallocatechin(-) (9) and leucopelargonidin(+) (10) were prepared by ligprep and their absorption, distribution, metabolism, excretion and toxicity(ADME/T) were described by QikProp analysis. The prepared ligands were docked against the 3OS8 using Glide programme of Schrodinger suite and the compounds were screened based on D-score and G-score values.
Results and Discussion
The ten monomeric flavanoids selected were optimized at B3LYP/6-311++G**, the prepared ligands were docked against the grid generated around the highest scored site of 3OS8. From the binding scores, all of the ligands show excellent D-Score/G-score of less than -10.8kcal/mol, confirms the strong binding capacityof the ligands inside the active site of 3OS8 (Table 1). The scores are better than the values reported for flavanoids by Suganya [22]. The drug ability parameters such as #stars, CNS, FISA, HBA, HBD, QPlogPo/w, QPlogS and QPlogKhsa are well within the acceptable range with minimum deviation from Lipinski rule of five (Ro5). The low molecular weight of 290-306 range increases the cell permeability of the ligands with blood brain barrier permeability of -2. The predicted skin permeability and oral absorptions are also in the recommended range. Most of the clinically successful drugs in the market have had the tendency to inhibit hERG with QPlogHERG value less than -5, but our ligands are exception to this threat. The hydrophobic and π-components of solvent accessible surface areas are matched well with the site volume of 204.77Å3 of 3OS8. The globularity descriptor value of 0.86 shows the spherical character of the ligands which may facilitate the binding of them in the binding pocket (Table 1).
Table 1: D-score/G-score and pharmacokinetic parameters for 1-10.
M.W.(Molecular Weight):130.0-725.0; #stars (few stars-more drug-like): 0-5; CNS (Central Nervous System activity): -2 to +2; FISA (Hydrophilic component of total solvent accessable area): 7.0-333.0; HBA(Hydrogen bond acceptor): 2.0-20.0; HBD(hydrogen bond donor): 0.0-6.0; QPlogPo/w (octanol/water partition coefficient): -2.0-6.5; QPlogS (Aqueous solubility): -6.5-0.5; QPlogKhsa (binding to human serum albumin): -1.5-1.5; Ro5 (Number of violations of Lipinski’s rule of five): maximum is 4.
The close observation of interaction diagram Figure 1 shows that all of the ligands almost closely packed in the binding site which gives the appreciable values. All the ligands except 5 forms H-bond with negatively charged Glu353 while the eight ligands except 5 and 9 have H-bond with positively charged Arg394 and 5 forms only one bond with His524. The HOMO-LUMO diagrams Figure 2 depict the electronic transition from HOMO to LUMO by a distance of 5eV, which is favorable for interaction of terminal hydroxyl groups with the aminoacid residues. The electron density in the HOMOs are concentrated on the benzene ring on 1, 2, 5, 6, 7, 8 and 9 while it is on chromenyl moiety in the case of 4 and 10. The hydrogen of OH from the corresponding rings is in strong interaction with the negatively charged glutamic acid. At the same time the oxygen’s of OH have the tendency to interact with positively charged arginine. These interactions from hydroxyl groups cause the strong binding of the ligands inside the binding pocket (Figures 1 & 2).
Figure 1: Interaction diagrams of 7, 6 and 3.
Figure 2: HOMO-LUMO diagrams of 1-10.
Conclusion
We are able to suggest a set of lead molecules from the natural source, bark of Saraca asoca. The interaction diagram shows the strong interactions of hydroxyl groups with negatively charged glutamic acid and positively charged arginine, which favors the strong binding. The molecular orbital analysis clearly tells the delocalization of electron density in the benzenyl and chromenyl hydroxyl groups. The pharmacokinetic parameters strongly support the druggability of these ligands. This study is expected to pave the way of generating new chemotherapeutics in the treatment of metastasis in breast cancer with low toxic effects.