Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Author: biomedicalopenaccessjournals
The only motto of Biomedical Journal of Scientific & Technical Research (BJSTR) Publishers is accelerating the scientific and technical research papers, considering the importance of technology and the human health in the advanced levels and several emergency medical and clinical issues associated with it, the key attention is given towards biomedical research. Thus, asserting the requirement of a common evoked and enriched information sharing platform for the craving readers.
BJSTR is such a unique platform to accumulate and publicize scientific knowledge on science and related discipline. This multidisciplinary open access publisher is rendering a global podium for the professors, academicians, researchers and students of the relevant disciplines to share their scientific excellence in the form of an original research article, review article, case reports, short communication, e-books, video articles, etc.
Oral Submucous Fibrosis: the Soft Tissue Marble of Asia
Introduction
Oral squamous cell carcinoma is the sixth most common malignant neoplasm worldwide. Each year it accounts for more than 300,000 cases worldwide. The 5-year survival rate for OSCC has remained at approximately 50% for the past several decades [1]. The impact of oral cancer is such that the disease and its treatment bring a heavy financial burden to both the social resources and the patient’s family with psychological stress affecting the quality of life [2]. It develops through a multistep process of genetic, epigenetic and metabolic changes resulting from exposure to carcinogens, with initially the presence of a precursor/pre-cancer such as oral leukoplakia, oral erythroplakia oral submucous fibrosis. The most frequently reported etiological agents being tobacco, alcohol, chewing of betel quid containing areca nut [3]. The global incidence of oral submucous fibrosis is estimated at 2.5 million individuals. It is one of the most predominant potentially malignant conditions in South Asia with a high rate of prevalence in India, but is now also being acknowledged in Europe and North America [4-6]. The prevalence in Indian populations is 5% for women and 2% for men, which is reflected by the fact that the habit is more common among women in some geographic areas [7].
Aetiopathogenesis
Oral submucous fibrosis (OSMF) is a chronic inflammatory disease of the oral soft tissues with progressive juxta-epithelial fibrosis resulting in increasing difficulty in chewing, swallowing, speaking and mouth opening, often associated with burning sensation inside oral cavity that is aggravated on exposure to spicy food [8]. The habit of chewing betel nut (Areca catechu) is considered to be the main etiological agent, with others factors being genetic predisposition, infections and viral agents, carcinogens, nutritional and immunologic factors [8]. The role of chilliin the pathogenesis of OSMF remains controversial and is postulated as an hypersensitivity reaction to capsaicin due to allergen induced eosinophilia [6]. The mixture of areca nut and tobacco has led to a sharp increase in the frequency of OSMF [5]. A relationship has been observed between the areca quid consumption and development of OSMF.
Areca nut (Figure 1) contains alkaloids notably arecoline and guavacoline, with a wide range of parasympatheticomimetic effects, which modulate matrix metalloproteinases, lysyl oxidases and collagenases, which affect the collagen metabolism leading to fibrosis [7]. Concomitantly, a decrease in the water-retaining proteoglycans will occur which favors an increase in type I collagen production and the flavonoids catechin and tannin in the betel nut stabilizes the collagen fibers and makes them resistant to degradation by collagenase [6]. Genetically, polymorphism of the gene coding for tumor necrosis factor α (TNF-α) leads to stimulation of fibroblasts and aberrations of other cytokines which include transforming growth factor β and interferon-γ, lead to increased production and decreased degradation of collagen. Concomitant to tobacco chewing, smoking and consumption of alcohol increases the risk of oropharyngeal malignancies. 7% to 13% lesions of OSMF can transform into oral cancer, especially squamous-cell carcinoma over a period of 10 years [6-8].
Figure 1:
Clinical Features
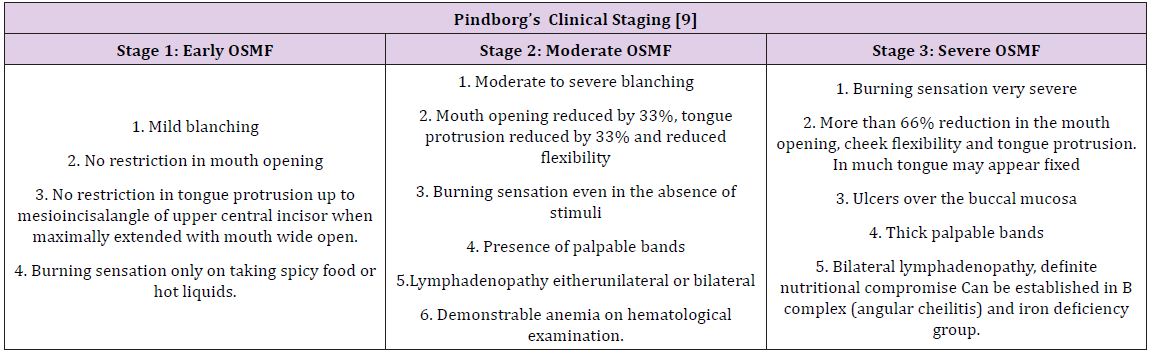
The buccal mucosa and retromolar area are the primary sites affected, followed by soft palate, palatal fauces, uvula, tongue and labial mucosa [6]. It occurs in the age group of 12–62 years with the mean age being 40 years. A definite female predilection, with the male: female ratio being 3:2 [6]. A difficulty in opening mouth accompanied with burning sensation is usually the reason for the patient’s initial visit. On examination, blanching of the oral mucosa is noted which imparts a marble-like appearance, attributed to inflammation, trailed by hypovascularity and fibrosis that may be associated with small vesicles and mucosal erosions [8]. As the disease progresses, there may be stiffness of the tongue, blanched and leathery floor of the mouth, fibrotic, depigmentation of gingiva, rubbery soft palate with decreased mobility and blanched and atrophic tonsils, and shrunken bud like uvula with impairment of activities such as eating, whistling, blowing, sucking [6]. Other symptoms are increased salivation, change of gustatory sensation, hearing loss due to stenosis of the Eustachian tubes, dryness of the mouth, nasal tonality to the voice anddysphagia to solids. Pindborg has classified OSMF into 3 stages as shown in Table 1.
Table 1: Pindborg has classified OSMF into 3 stages.
Diagnosis & Investigations
Diagnosis of the disease is mainly by clinical findings and can be confirmed by incisional biopsy. Other investigations include hematological, serological, immunological and biochemical factors which may reflect findings such as a raised ESR, slight eosinophilia, microcytosis and hyperchromic indicative of anemia. The differential diagnosis includes anemia and scleroderma which can be distinguished by other cutaneous, systemic and characteristic radiographic and laboratory findings [6].
Management
Management of OSMF includes use of hyaluronidase and corticosteroids or a combination of both. Other treatment modalities include antioxidants, Immunomodulators, Physiotherapy, Intereferon -γ, Hyper Baric Oxygen (HBO) therapy, Curcumin, Oxitard, Aloevera, Surgery [6,8,10]. Even though it is easy to diagnose but the irreversible condition reflects the failure of the present treatment modalities. The lack of knowledge and the delay in seeking treatment leads to the progression of the disease. Hence, more focus should be emphasized in detecting newer treatment modalities which is the need of the hour and the future.
Asperger syndrome is an autism spectrum disorder that is on the high functioning end of the autism spectrum it is also referred as “dash of autism”. Incidence is more in males as compared to females. It is important to note the characteristics of Asperger syndrome which can range from mild to severe [1].
a. Definition: Asperger syndrome (AS), also known as Asperger’s, is a developmental disorder characterized by significant difficulties in social interaction and nonverbal communication, along with restricted and repetitive patterns of behaviour and interests [2].
Cause
Cause of Asperger syndrome is not yet identified, although an inherited (genetic) component is believed to be involved. In special cases it may caused by pregnancy infections use of teratogens, and exposure to toxics [3].
Symptoms
Some of the symptoms that may be present are [4]:
a. Less social active;
b. Less friends;
c. Not interested in making friends;
d. Inability to express emotions;
e. No Eye contact;
f. Less facial expressions;
g. Inability to use gestures;
h. Ineffective communication;
i. Lack of relation;
j. Sensitive to external stimuli;
k. Dependent ; and
l. Repetitive actions like arm waving.
How it is Different from Classic Autism?
a. Asperger syndrome is in many ways a milder form of classic autism.
b. Whereas those with autism do not create to have relationships, children with Asperger syndrome attempts to have interaction with others, though they may have difficulty understanding conventional social rules.
c. Asperger syndrome does not usually affect language and communication skills as classic autism [5].
Diagnosis
A diagnosis is the formal identification of the condition, usually by a multi-disciplinary diagnostic team, often including a speech and language therapist, paediatrician, psychiatrist and/or psychologist [6].
Treatment
Treatments can include [7]:
a. Social skills training: In groups or one-on-one sessions, therapists teach child how to interact with others and express in appropriate ways. Social skills are learned through training.
b. Speech-language therapy: This helps in developing communication skills. This therapy provides training regarding two-way conversation and social cues like hand gestures and eye contact.
c. Cognitive behavioural therapy (CBT): It helps your child change his way of thinking, so he can better control his emotions and repetitive behaviours.
d. Parent education and training: You’ll learn many of the same techniques your child is taught so you can work on social skills with him at home. Some families also see a counsellor to help them deal with the challenges of living with someone with Asperger’s.
e. Support Group: A forum for counselling and sharing experiences among people with a similar condition or goal, such as depression or weight loss.
f. Anger management: Practicing mindfulness, coping mechanisms and trigger avoidance to minimise destructive emotional outbursts.
Conclusion
It is an autism spectrum disorder People with Asperger syndrome are of average or above average intelligence. They do not usually have the learning disabilities that many autistic people have, but they may have specific learning difficulties, Identification of the condition, usually done by a multi-disciplinary diagnostic team and treated by using therapeutic modalities.
Antimicrobial Peptides: A Wide Range of Novel Compounds and Their Role as Plant Defense Peptides
Introduction
Despite their sedentary lifestyle plants share some common aspects in their defense mechanisms against pathogens. These features are small peptides that have antimicrobial properties which is part of more ancient and widespread defense strategy in all organisms. These are a product of single gene that can be synthesized in a swift and flexible way, due to their small size they can be produced by host with minimal input of energy and biomass. Well known examples of antimicrobial peptides are cecropins that accumulate in the hemolymph of many invertebrates in response to injury or infection [1] and other example are magainins that are secreted by glands in the skin of amphibians [2].
Plant Defence Peptides
Antimicrobial peptides have long considered playing a key role in plant defense, both as a part of pre-existing, developmentally regulated defense barriers and as part of defense responses that occur upon infection. The antimicrobial peptides in animals may be linear or more complex globular structures in which antiparallel β- sheet are stabilized by disulphide bonds. But in plants only disulphide bonded peptides of second type have been identified till now [3]. The first antibacterial peptide isolated from a plant species was a purothionin from wheat flour (Triticum aestivum), which has the ability to inhibit the growth of some phytopathogens such as Pseudomonas solanacearum, Xanthomonas campestris and Cornybacterium michiganense [4]. Almost 40 years later, several additional peptides with antibacterial activity have been characterized, represented not only by thionins, now named defensins, but also by other groups of proteins such as cyclotides, glycine- rich proteins, snakins, 2S albumins and hevein-type proteins [5]. Peptides isolated from roots, seeds, flower, stem and leaves have shown activities towards pytopathogens as well as against bacteria pathogenic to humans. Over the last decade, antimicrobial peptides have become an interesting tool for the development of techniques in the control of crop loses and in the production of novel antibiotics for the treatment of various human infections [6,7].
Conclusion
Antibacterial peptides have described in a variety of plant species. They belong to a vast range of protein families. Some peptides show specificity towards gram-positive or gram – negative bacteria, but most of them are able to inhibit the activity of both. The study of their mechanism of action shows that these antibacterial peptides are involved in strong interaction with phospholipids from pathogen’s membrane. Parameters such as a molecular volume, aggregation ability and auto assembly on the membrane surface are critical for activity against bacteria. Although, the mode of action of these antibacterial peptides is well characterized, investigations on the importance of specific amino acid residues and their binding with the bacterial cell wall are still in progress.
Acknowledgement
The author is grateful to Dr. (Mrs.) Sushma Ahlawat, Assistant professor, Sam Higginbottom University of Agriculture, Technology & Sciences (SHUATS), Allahabad, India, for her kind support towards this study.
Assessment of Magnitude and Associated Factors of Adverse Birth Outcomes among Deliveries at Suhul Hospital Shire, Tigray, Ethiopia From September, 2015 to February, 2016
Introduction
Adverse birth outcomes such as prematurity, low birth weight and birth defects- represent significant problems in both developing and developed countries. Each year, about 15 million babies in the world, more than one in 10 births, are born too prematurely. More than one million of those babies die shortly after birth; countless others suffer from lifelong physical, neurological, or educational disabilities, often at great cost to families and societies [1]. Globally, an estimated 13 million babies are born before 37 completed weeks of gestation annually. Rates are generally highest in low and middle income countries and increasing in some middle and high-income countries. Complications of preterm birth are the leading direct causes of neonatal mortality and account for an estimated 27% of neonatal deaths. This comes to almost four million neonatal deaths every year [2]. From a global standpoint, the prevalence rate of preterm birth varies from 47.5 to 137 per 1000 live births. Grand multiparty, a previous history of preterm birth or abortion, younger maternal age, inadequacy of prenatal care, reported hypertension, ante partum hemorrhage, premature rupture of fetal membranes and induced labor are significant determinants of preterm birth [3,4].
Worldwide stillbirth rate has declined by 14%, from 22.1 stillbirths per 1000 births in 1995 to 18.9 stillbirths per 1000 births in 2009. But in the African region, there was only an annual decline of less than 1%. The stillbirth rate for developed countries is estimated between 4.2 and 6.8 per 1000 births, whereas for the developing world, the estimate ranges from 20 to 32 per 1000 births. Two thirds of all stillbirths occur in just two regions: South- East Asia and Africa [5,6]. In sub-Saharan Africa, an estimated 900,000 babies die as stillbirths. It is estimated that babies who die before the onset of labor, or ante partum stillbirths, account for two-thirds of all stillbirths in countries where the mortality rate is greater than 22 per 1,000 births [7]. From previous studies, preterm birth, increasing maternal age, history of stillbirth, reported hypertension, extremes of neonatal birth weight, cesarean delivery, operative vaginal delivery, and assisted breech delivery were all significantly associated with still birth [8]. According to Ethiopian Demographic and Health Survey in 2011, In Ethiopia, high rate of neonatal mortality (37 deaths per 1,000 live births)is reported and preterm birth is believe to be a major and direct cause of neonatal mortality [9]. In Ethiopia, adverse outcome of pregnancy are still major public health problems [10,11].
Adverse birth outcomes are the most important vital statistics used to assess maternal and child health program. They are indicator of the quality of antenatal care, medical services and general health services to the mother and the children [12]. Epidemiological data on the magnitude and risk factors of adverse birth outcomes are important for planning maternal and child health care services in developing countries. Most of the newborns who are admitted in neonatal wards are secondary to preterm birth and low birth weight. Most of them are also complicated with various health problems after they have been admitted with a diagnosis of either low birth weight or preterm birth. Mothers are also feeling unhappiness and become unsatisfactory after having a still birth [13]. Hence, this study aimed to determine magnitude and associated factors of adverse birth outcomes of pregnancy at a Suhul Hospital Tigray Ethiopia. The result of this study will serves as a baseline for other wide studies as well as for planning health intervention to improve the wellbeing of children and women [14-19].
Conceptual Frame Work
This frame work was developed by the principal investigator by reviewing different literatures and books (Figure 1).
Figure 1: Conceptual frame work of adverse birth outcomes and associated factors at suhul hospital from September, 2015 to February 2016.
Subjects and Methods
This was a cross sectional study conducted at Shire (Suhul) Hospital. Shire city is located in western zone of Tigray with an area of 30.0316km2 and total population of 47,284. It is 1100KM km far from the capital city of Ethiopia, Addis Ababa and 283km from Mekelle, which is a capital city of Tigray. The study was conducted between June 15 -July 15, 2016. The study population was sampled term new born babies delivered at Adwa General Hospital for the period July 1, 2014 to June 30, 2016. Individual term new born babies reviewed from mother’s chart or cards.
Source Population: were all mothers who gave birth at Suhul hospital from September, 2015 to February, 2016.
Study Population: selected cards of those mothers who gave birth at Suhul hospital from September, 2015 to February, 2016.
Study Unit: Maternal cards with adverse birth outcomes and normal birth out come.
Inclusion Criteria: All maternal cards with adverse birth outcomes and normal birth outcomes with no missing the most important information (detail records on demographic characteristics, current obstetric history, medical history and past obstetric history and delivery summary) were included.
Exclusion Criteria: maternal cards with birth outcomes of congenital anomaly.
Sampling and Sample Size Determination: The sample size was determined by using single proportion for finite population with 95% confidence interval, marginal error (d) of 4 %.
n=(z2 p(1-p))/d2
n= Sample size
z= the standard score (critical value) corresponding to 95% confidence level = 1.96.
d= the proportion of sampling error between the sample and the population = 4% (0.04).
p= prevalence
Calculation of the sample size was based on the Gondar’s prevalence which is as follows:
Equation 1:
Simple random sampling technique and card reviewing method was used. In Suhul hospital there were a total of 1590(N) deliveries from September 1, 2015 to February 30, 2016. The sample size was 425 (n). After identifying the number of cards at each month the calculated sample size was distributed to each month of study based on population proportion size and the study subjects were nominated randomly (Figure 2).
Figure 2: Sampling frame work of study participants.
Data Collection Methods: Since the file is kept at record office after discharge, data collection was done using structured checklist from clinical records of mothers’ (registration books and individual cards). Cases was identified from the records office through reviewing every record of women who gave birth at Suhul hospital from September 1, 2015 to February 30, 2016.The checklist was structured into four logical sections (socio demographic characteristics, obstetrics related factors; medical history and birth outcomes assessment). Data were collected by 3BSc midwives after giving 2 days training.
Data Quality Control: Data quality was ensured during collection, coding, entry and analysis. Pre prepared Structured checklist was used. Training was given to the data collectors and supervisors to prevent any confusion and have a common understanding about the study. Each card was checked for its consistency, provision of full information and appropriate documentation. Pretest was conducted on 21 maternal cards (with adverse birth outcome and normal birth outcome) that gave birth before September 2015. Based on the pretest modification on logical sequence, simplicity, and clarity of checklist had been done. Supervision of data collectors included observation of how the data collectors will collect data was done by supervisors. The data collectors were instructed to write cards number on the check list during the data collection so that any identified errors was traced back using the cards number. The filled checklist was checked for completeness by data collectors, supervisors and PI on a daily basis. Consequently, any problem encountered was discussed among the team and solved immediately. The collected data code was given to the completed questionnaire. The data was entered and analyzed using SPSS version 20 statistical package. Data cleaning was performed to check for frequencies, accuracy, and consistencies and missed values and variables. Any error identified was corrected.
Data Analysis: Frequencies, proportion and summary statistics were used to describe the study population in relation to relevant variables. Both Bivariate and multivariate logistic regression analysis was used to determine the association of each independent variable with the dependent variable. Variables significant in Bivariate analysis were entered into a multivariate logistic regression model to adjust the effects of cofounders on the outcome variable. Odds ratio with 95% confidence intervals was computed to identify the presence and strength of association, and statistical significance was declared if p < 0.05.
Study Variables
1. Dependent variable
• Adverse birth outcomes (Still birth, preterm birth and LBW)
2. Independent variables
3. Socio demographic characteristics
• Residence, age, marital status and ethnicity
4. Obstetric history
• Parity, gestational age, onset of labor, duration of labor, pregnancy status, mode of delivery, type of pregnancy, previous poor obstetric history, contraceptive use
Medical illness and other obstetric complications
• Anemia, UTI, Malaria, HIV/AIDS, Hypertension, Ante partum hemorrhage, HIV status, ART status, Hepatitis virus screening.
Operational Definitions
1. Adverse birth outcome: newborns delivered as preterm, low birth weight or still birth
2. Still birth: fetal loss after 28 wks of gestational age and during intra partum period.
Ethical Consideration
Ethical clearance was obtained from Mekelle University College of health science. Purpose of the study was informed for the managers, staff members and health professionals who were working at Suhul hospital.
Dissemination And Utilization Of Results
Results will be disseminated to Mekelle University, Tigray region health bureau and to Suhul hospital where the data had been collected.
Result
The Socio-Demographic Characteristics Of Women Attended Maternity Ward At Suhul Hospital, Shire, Tigray, Ethiopia: A total of 425 cards of mothers were reviewed in the study of which 283 (66.6%) were in the age group of 20-34, followed by 94 (22.2%) greater than 34 years with the mean age of 29 and standard deviation of +7. Majority of the mothers 375 (88.2) were married and more than half of mothers 234(55%) were urban residents. Regarding their ethnicity majority, 378 (88.9) of them were Tigrai followed by 41 (9.6%) were Amhara [20] (Table 1).
Table 1: Socio-demographic characteristics.
The Obstetrics Characteristics Of Women Attended Maternity Ward At Suhul Hospital, Shire, Tigray, Ethiopia: More than half of mothers 246(57.9%) were multipara and 119(28%) of mothers were Primipara. Most of the mothers, 407(95.8%) had history of ANC follow up, almost half of them 201(49.4%) had their first ANC visit during first trimester and 191(46.9%) mothers had at least four visits during current pregnancy. with regard to the status of current pregnancy 325(76.5%) of the pregnancies were wanted and planned. In this study majority of mothers 391(92%) were supplemented with Iron and Folic acid during ANC follow up. Majority of the mothers 392 (92.2%) had taken TT vaccination, of them around one third of the mothers had taken the fifth dose of TT vaccination. Regarding the type of pregnancy in this study 401(94.3%) of the pregnancy were singleton. The mean duration of labor was 13 hours with standard deviation of +4. More than three fourth of 350(82.4%) onset labor were spontaneous and majority of mothers 322(75.8%) were delivered by SVD. Two third of mothers had used contraceptives prior this pregnancy, of them 204(72.1%) had taken inject able (Table 2).
Table 2: Obstetrics characteristics.
The Medical Illness And Obstetric Complications Among Women Attended Maternity Ward at Shire Suhul Hospital Tigray Ethiopia: Fifty two (12.2%) of the mothers had medical illness, of them 16(38.2%) mothers had urinary tract infections. thirty seven (8.7%) and thirty two (7.5%) of mothers had hypertensive disorders of pregnancy and ante partum hemorrhage respectively. Twenty seven (6.4%) of mothers also had premature rupture of membrane during current pregnancy. More than three-quarter 345(81.2) of mothers were screened for HIV, of them 35(10.1%) were reactive for HIV test and 33(94.3%) of them had started HAART. All study participants were screened for hepatitis viral infection and syphilis, 28(6.6%) and 7(1.6%) of mother had positive results for hepatitis and syphilis respectively (Table 3).
Table 3: Medical illness and obstetric complications.
The ABO Among Women Attended Maternity Ward at Shire Suhul Hospital Tigray Ethiopia: The study finding showed that the prevalence of ABO among the study participant was 96(22.6%). Seven (14.3%) of low birth neonates and six (16.2%) of preterm births were still birth and 23(47%) of LBW neonates were preterm. almost half of the new born 213(50.1%) were males. The mean weight of newborns was 2.9kg with the standard deviation of + 0.6kg (Figure 3).
Figure 3: Magnitude of preterm birth, LBW and still birth.
Factors Associated With Adverse Birth Outcome Among Women Attended Maternity Ward at Shire Suhul Hospital Tigray Ethiopia: Bi-variate and multivariate logistic regressions were done to assess the predictors of ABO. Onset of labor, residence, hypertensive disorders of pregnancy, ante partum hemorrhage, PROM, previous BOH and type of pregnancy were significant at bi variate logistic labor. Mothers who had HDP were 6 times (AOR=6.368, (95%) CI: 2.880-14.080) more likely odds associated with ABO than mother without HDP. Women who had APH during respective pregnancy were 3 times (AOR=3.087, (95%) CI: 1.172-8.132) more likely odds associated with ABO than women who didn’t face APH. Mothers who had previous history of BOH were 2.3 times (AOR=2.290, (95%) CI 1.165-4.503) more likely odds associated with ABO than mothers who hadn’t bad obstetric history. Multiple pregnancies were 7 times (AOR: 7.230, 95%) CI 2.973-17.580) more likely odds associated with ABO than singleton pregnancy (Table 4).
The finding of this study showed that the magnitude of ABO among deliveries was 96(22.5%) among which the prevalence of still birth was 41(96/1000 births) and the magnitude of preterm birth and low birth weight were 37(8.7%) and 49(11.5) respectively. The prevalence is higher than the WHO estimation [20-22] and regional and worldwide estimation [5] of adverse birth outcomes this variation may be due to the difference that this study was institution based study and which was done in a zonal hospital, so that the magnitude may increase because of increasing number of referral cases from health centers and primary hospitals. The magnitude was also higher than studies done in Tanzania [23], Iran [24], China [25] and Ghana [26]. The variations between the findings may be attributable to the variations in methodological and socio-economic variations, quality of maternal health service and facilities explain differences in adverse birth outcomes in respective study areas.
The findings of this study were lower than from pervious reported studies in Jimma zone [27], Debremarkos [28,29] and Kersa east Ethiopia [30]. This variation may be due to methodological difference that the previous studies were used prospective study but in this study the methodology used was card review, hence it may limit the type and number of adverse birth outcomes. The Figure were also lower than the study findings done in north wello zone [31], this variation is attributable to the previous study was community based study. It were also a little beat lower than the study done in Gondar which showed that the prevalence of adverse birth outcome was 23% with the proportion of 14.3%, 11.2% and 7.1% preterm birth, low birth weight and still birth respectively [32]. This variation may due to methodological difference. Pregnancy induced hypertension one of the risk factors for adverse birth outcome and mother with HDP was 21.6 times more likely to associate with adverse birth outcome than mother without HDP. This finding was in line with other studies done in Iran [24]. Similar finding was also reported from the study done in India [33] which revealed that mothers with PIH were more likely to delivery adverse birth outcome as compared with those women without PIH.
This is again supported by a research done in Tanzania [34], China [25], Gondar [32], and Debremarkos [28]. This might be due to hypertension results in decreased blood flow through the spiral arterioles and decreased delivery of oxygen and nutrients to the placenta and fetus and Hypertension also might be associated with placental infarction. These researchers indicated that hypertensive disorders might play a critical role in the incidence of adverse birth outcome as supported by other studies. Evidence from earlier study showed that reduced placental blood flow leads to decreased fetal growth, with an increased risk of intrauterine growth restriction and low birth weight [29]. In this study Ante-partum hemorrhage during the current pregnancy is significantly associated with adverse birth outcomes this finding was in line with the previous studies in Iran [24], Tanzania [34] and Pakistan [35]. Similar study in Gondar also reported that Ante-partum hemorrhage is significantly associated with adverse birth outcomes, bleeding during pregnancy is one of the etiologies of anemia leading to intrauterine oxygen inadequacy [32].
Furthermore, mothers who had previous history of poor obstetric history were 2.3 times more likely to have adverse birth out comes than mothers who hadn’t bad obstetric history. This Figure was similar with previous study findings in Tanzania [23], Iran [30], China [25], Gondar [32], and north wello zone [31]. This might be due to most poor obstetrics histories are recurrent. Induced on set of labor was also significantly associated with a adverse birth out comes this may be due to different maternal and fetal indications like hypertensive disorders of pregnancy, ante partum hemorrhage, oligohydramnios, premature rupture of membrane etc, in order to prevent maternal and fetal complications. Multiple pregnancies were significantly associated with adverse birth outcomes. Similar studies in jimma zone [27] and Canada [9] also revealed Multiple pregnancies were risk factors for development of adverse birth outcome this might be due to chorionicity, in monochorionic placentation is associated with fetal mortality and morbidity in monochorionic twins the placenta is shared and inter twin vascular anastamoses, which produce various degree of twin to twin transfusion syndrome in 10% to 15% cases. Twin to twin transfusion syndrome causes discordant twin growth and, sometimes intrauterine demise of one twin. It may also result in fetal anemia or it may be related to uterine distension, increased intrauterine volume, or related complications such as cervical incompetence [9].
Conclusion
The magnitude of adverse birth outcome among the study population was higher than WHO estimation. Induced onset of labor, hypertensive disorders of pregnancy, ante partum hemorrhage, previous bad obstetric history and multiple pregnancies were the major predictors of adverse birth outcomes.
Acknowledgment
We would like to express our appreciation to Mekele University and the Department of Midwifery for their invaluable contribution towards the completion of this study. We also thank our friends and colleagues for their critical contributions.
Psychosocial Stressors among Suicide Attempters Attending JIPMER Hospital Puducherry
Introduction
Living life to the fullest is the significant challenge faced by most of the people in this world. The value of the life is determined by how people give meaning to their life. Each person is a part of life [1]. All human beings will periodically experience psychological burdens, pain, and stressors during their lifetime. Having transient thoughts of wanting to die may be a natural response to emotional pain. In the midst of the psychological pain, suicide can become a gripping and viable means of escape [2]. Suicide then may be considered as both a coping mechanism and a failure to cope [3]. Suicide is the act of purposefully killing oneself. In broad terms, an act is a suicide if a person deliberately brings about his or her death in a situation where others do not coerce him or her to the action [4]. Suicide is not a diagnosis or a disease; it is a behavior that should alert us to an underlying problem, difficulty or disorder [5].
According to the WHO estimation each year approximately one million deaths from suicide globally, 16 people per 100,000 or one death in every 40 second. Suicide attempts are up to 20 times more habitual than completed suicides notably; a prior suicide attempt is the single most potent risk factor for death in the general population. Suicide is one among the three leading reason of death in the age group of 15-44 [6]. Although suicide rates have been highest amongst elderly males, rates among young people have been growing [7]. Mental health disorders (particularly substance abuse and depression) are associated with 90% of all cases of suicide. Death results from many complicated socio-cultural factors and is more likely to occur during periods of individual family and socioeconomic crisis [8]. the highest number of suicide deaths (16.927) was reported in Tamil Nadu in 2012, accounting for 12.5% of total suicide deaths in the country.
Pondicherry reported the highest rate of suicide (36.8) followed by Sikkim (29.1), Tamil Nadu (24.9), Kerala (24.3). The male: female ratio of suicide victims for the year 2012 was 66.2:33 [9]. Suicide is complex with biological, social, psychological, cultural and environmental factors. These stress factors vary from person to person and time to time. Identification of these stressors at the earliest will be the only solution to control the death statistics due to suicide. Suicide attempt is an urge for help from the environment; in more than 42% cases repeat attempts are known [10]. According to a London study by Royal College of Psychiatry, the primary triggers for self-harm were social and family, issues, relationship break-up [11]. According to the study conducted in Fiji among the clients with attempted suicide, the major stressor was the interpersonal loss (69%) followed by family instability (36%) [12]. Study done in Belgium observed that 42% of the victims had academic failures, and 36.8% of them had criminal offences [13].
Multicentre study by WHO in Europe concluded that 94.1% suicide attempters had a history of relationship conflicts, 79.2% reported a death or loss and 65.5% reported stress due to physical abuse [14]. Suicide is a preventable phenomenon. The many psychosocial stressors contributing to the suicide attempt can be avoided with timely intervention [15]. Understanding these stressors largely contribute to the future prevention strategies. Studies assessing stress full life events and suicidal intent are done nationally and internationally [16-19]. These studies mainly try to focus on one aspect of the stressors. The Present study is focusing on stressful events as well as day to day life stressors, and attempting to assess all the areas of psychosocial stressors in suicidal clients
Methodology
This cross sectional descriptive survey aimed to assess the psychosocial stressors among suicide attempters. The study was conducted in medical wards and crisis intervention clinic of Jawaharlal Institute of Post-graduate Medical Education and Research (JIPMER) hospital Puducherry. Main objective of the study was to assess the psychosocial stressors and suicide intent among the suicide attempters and to identify any association of these with demographic and clinical variable. Study population was patients admitted to the Medical Ward or attending Crisis Intervention Clinic in Psychiatric OPD after a suicide attempt, at JIPMER hospital Puducherry. Sample consisted of 50 suicide attempters. Subjects selected through convenience sampling technique that fulfilled the inclusion and exclusion criteria during the 6 weeks of study period. Patients with an attempted suicide aged above 18 years, both sex and Patients who can comprehend and speak English or Tamil were included.
Medically unstable patients were excluded from the study. Research instruments used were Presumptive Stressful Life Events Scale [20], Revised Daily Hassles Scale [21], and Beck’s suicide intent Scale [22]. Data collected through direct interview technique. All the three instruments were validated in the Indian population and were standardized, at international, national settings. Reliability of Presumptive Stressful Life Event scale was assessed in Indian population and found to be satisfactory65 (0.8). Reliability studies of Beck’s Suicide Intent Scale showed that internal consistency of the total score was acceptable67 (0.81). Daily hassle’s scale was found to have good internal reliability66 (Cronbach’s alpha 0.88). The JIPMER Scientific Committee as well as Institute ethics committee, Human studies JIPMER approval was obtained to conduct the study (PGMRC /MHN1/2014). The investigator approached the study subjects with a brief self-introduction. A written informed consent was procured from the subjects.
Psychosocial stressors were assessed by using Presumptive Stressful Life Events Scale and Revised Daily Hassles Scale. The scales were explained to the subjects in their convenient language and assistance was given to those who required. Suicide intent of the patient was assessed by Beck’s Suicide Intent Scale; a clinicianrated scale and data collected by direct interview method. Privacy of the patients was taken care during the data collection, and the confidentiality was maintained throughout the research process. Statistical analysis was done using SPSS 20. Demographical and clinical variables were analysed with descriptive statistics. Patients mean stress scores and mean suicide intent score were computed using descriptive statistics. Chi square test and independent t test was used to find the association between socio demographicclinical variables and psychosocial stressors.
Results
Among the 50 participants females accounted for 56% (n=28) of the sample. Most of them were from nuclear family (58%) and was married (58%). Unemployed suicide attempters accounted for 58% of the sample and 74% of them hailed from rural area (Table 1). Alcohol use was reported by 28% of the subjects and only 10% of them had any history of Psychiatric illness. Chemical poisoning was the mode of attempt in majority of the attempters and only 10 % of them had a previous history of suicide attempt (Table 2). The most frequently occurred life event was family conflicts 31(62%). Second most commonly occurred event was financial loss or problem 25(50%), followed by alcohol or drug use of the family member 20(40%) and marital conflict 19(38%). Change in sleeping pattern was the stressful event for 18 (36%) subjects while 14 (36%) of them had self or family unemployment as a stressful event. Conflict with in-laws was the stressful event for 8 (16%) subjects and 6 (12%) of the subjects identified to have the lack of child as a stressful event. (Figure 1) Use of alcohol 9(18%) was the most frequently reported daily hassle. Troubling thoughts about the future, physical illness overload with family responsibilities 6(12%) equally occurred hassles. Among the study sample, at least 5(10%) had the hassles due to responsibilities, lack of money for food, television and menstrual problem (Figure 2).
Figure 1: life events.
Figure 2: daily hassles.
Table 1: Socio-demographic data of sample.
Table 2: Clinical variables of sample.
In the regard of the suicide intent of the study subjects Majority 26 (52%) of sample had medium suicide intent, while 23 (52%) of them had low intent. suicide intent and only 1 (2%) had high suicide intent. (Figure 3) & (Table 3) Association of psychosocial stressors score with suicide intent severity (N=50) Spearman’s correlation coefficient test showed that there was no significant correlation between the mean number of stressors obtained from Presumptive Stressful Life Event Scale and Daily Hassles Scale-R with suicide intent score. The association of demographic variables with suicide intent severity was established using Chi-square test results showed that there was no significant association between demographic variables and severity of suicide intent. Association of PSLE stresses scores with demographic variables. Independent t test results showed that employment status was associated with the life events score with p=.030. None of the other demographic variables were significantly associated with psychosocial stressors. Table 3 the association of PSLE scores with the clinical variables. Independent t test results elicited no significant association between psychosocial stressors and clinical variables except medical history with p=.053. The association of DHS-R with clinical variables were assessed using Independent t test showed no significant association between DHS-R stress score and clinical variables except medical history with p=.05
Figure 3: suicidal intent.
Table 3: Association of PSLE score with demographic variables N=50.
*significant
Discussion
Supporting to the current study findings various national and international studies also reports increased suicide attempts among the females. Chinese study [23] reported that the females are at higher risk of attempting suicide. Similar demographic descriptions were found from an Indian study [24] done by Mathew in Southern India. Majority of the suicide attempters were females 62(62%), and 84 (84%) were from the nuclear family. Among the attempters 70 (70%) of them were Hindus. Concerning employment 80 (80%) of them had high school education and 55 (55 %,) were unemployed. History of suicide attempt was found in 8 (8%), and 4 (4%) of them had physical illness. Another Indian study [25] resulted that the male-female ratio of suicide attempters was almost equal to one (1:1.4). Higher proportion 80 (54.3%) of the suicide attempters were married which coincided with the findings of the current study, stating that marriage is a possible risk for suicide attempts. The majority 146 (98.6%) of the attempters were of Hindu religion as seen in our study. There were some findings contradicting to the current study results. In the current study majority 29 (58%) of them belonged to nuclear family, and most were 42 (84%) literate and. Very low number of subjects 5 (10%) had past history of suicide attempt, and psychiatric illness. Study from Orissa [26] reported that majority 129 (87%) of the suicide attempters had an extended family, and most of them were educated.
South Indian [27] study reported that 13 (13.3%) suicide attempters had a family history of suicide attempts and majority 78 (78%) of the suicide attempters had history of psychiatric illness. However, there are also reports which suggest that psychiatric illness is very low in suicide attempters from Asia [18]. Family conflicts accounted for the major stressful life event of 62% of the study subjects while 50% of the subjects had financial loss or problems. Excessive alcohol or drug use by a family member was a reason for stress for 40% of the subjects. Marital conflicts and change in sleeping pattern accounted for stress in 38% and 36% of the study subjects respectively. Mean stressors score of 50 study subject for the presumptive stressful life event scale was 206.8 with a standard deviation of 88.2.
The results of a Belgium study [28] on life events of suicide attempters showed that 8 (42.1%) of them had relational problems, but the majority of them had academic failures since majority of the study subjects were adolescence. Another international study [29] also supported the present study results that 44 (72.1%) of the study subjects had family-related conflicts and 39 (63.9%) of them had marital conflicts. The reviewed studies have given various results. An international study done in UK reported a high suicide intent score in 63% of males 79% of females. Another study [30] done among 229 suicide attempters in Finland resulted that 40% of them had severe suicide intent followed by another 40% of them with moderate suicide intent. Mild suicide intent was present in 20% of the attempters. Indian studies done on suicide intent had tried to classify the high and low intent attempters; study done by Kumar et al.
The present study assessed the association of suicide intent with the psychosocial stressors of suicide attempters. No significant association was elicited between psychosocial stressors and suicide attempt in the study. Neither the stress arising from major life events nor stress arising from daily hassles showed association with the suicide intent. A study done in the same setting [31] of the present study failed to observe an association of suicide intent with any of the demographic or clinical variable except a significant (p=0.04) association with psychiatric illness. There was a significant association found with the PSLE score and employment status. Being unemployed may indirectly increases stress by adding financial burden and family conflict. Other studies have not commented on this. There were no studies with a similar result. Study done by Pompli [32] reported that psychosocial stressors are significantly higher in repeaters than that of first time attempters. Another study from Iran found a significant difference (p<0.001) in the stress score of male and female suicide attempters. Study Limitations were samples were limited to 50 due to the inclusion and exclusion criteria, The study period was limited to 6 weeks, Sampling technique adopted in the study was convenience sampling, There were some sensitive issues like emotional distress anxiety familial conflicts; however asking about them by using questionnaires always carries concerns about the truthfulness of the participants.
Acknowledgement
The authors thank all the clients who participated in the study as well as JIPMER hospital for giving permission and support to conduct the study.
Child Abuse and Dental Practice: Finding the Nexus
Introduction
Many reports indicate that children are abused everyday worldwide. They are abused in many different ways [1]. Literature suggests that the numbers of reported abuses against children are a mere tip of an iceberg accordingly, there are many unreported cases – some are hidden or covered. Thus, child abuse becomes a social problem. Many seem to ignore child abuses, others of course will justify. Admittedly there are a few who will hide such abuses under a carpet or give a blind eye. In some societies child abuse has become a part of an accepted cultural practice- for example corporal punishments or female genital mutilations. Fortunately, there are some of us in the society who will voice against abuse of children. The social responses to child abuse are reflected in clinical sets up in similar ways. This means that some clinicians will ignore abuses while others may not care. The problem becomes aggravated in clinical scenarios especially when the clinician is not trained in identifying an imminent child abuse. In this context, this paper seeks to find a connection between clinical dental practice and child abuse. In short, I will argue and demonstrate in this paper that the presentations of cases of child abuse are not uncommon to the dental clinician, but that they are often times presented with alternate histories so that they can be easily missed by the clinician, if not looked through forensic lenses.
Contextualising Child Abuse
According to international law, especially based on the United Nations Convention of the Right of the Child (UNCRC), any person below the age of eighteen years is considered as a child. In this sense any violence or abuse against a person below eighteen years can be considered as child abuse. While child abuse can be presented in different forms, including physical, sexual, emotional or neglect forms, the perpetrator is usually a family member, care giver, custodian or a neighbour or at least a relative. Despite the fact that child abuse is frequently seen as an ongoing event with multiple chronological encounters, it can certainly happen as a single event. Further, child abuse can result from an action by the perpetrator or by inaction, for example not giving food or care. Given the serious impact it has on the child in his physical and psychological development, abuse and violence against children should be identified early to avoid further harm.
Connecting the Dental Clinician
While injuries to teeth and face are common among children, according to research, considerably a large number of them are due to abuse and violence [2]. Owing to their obvious appearance, swelling, bleeding and pain, usually the child will be presented to the dental clinician, of course with a misleading history. Those that are not presented to the clinician by parents or care givers, outsiders may notice injuries and may proceed to enquire – for example school teachers or neighbours. It is essential that the dental surgeon conduct an intra oral and peri oral examination carefully with a forensic eye in dealing with a suspected case of child abuse. Apart from the history from the guardian, a private interview with the child in the clinical set up may reveal some important information. The possibility of child abuse as a differential diagnosis has to be considered while attending to a child with a history of fall or accident, especially when the child is brought repeatedly. In the event where the clinician reasonably suspects child abuse, the case should be reported for medico-legal management-which is a legal requirement under almost all jurisdictions.
Presentations of Abuses
There have been instances of inflicting oral injuries with feeding instruments, for example using feeding bottles perhaps due to forced feeding. Further, fractures of teeth, contusions in and around the mouth and face, abrasions especially by finger nails or another object, fractures of mandible or maxilla due to violent assault, finger tip contusions around the mouth , burnt marks in and around the mouth especially with cigarettes, firewood or heated electric instruments, scalding resulted with hot water or liquids are common. The lips, teeth, buccal mucosa tongue and facial bones, gingival, alveolar bone are the commonest anatomical sites that are reported to have been affected [3]. Despite oral sex is a common type of sexual abuse among children, more often than not the child may not show physical features. However, it is possible that contusions occur inside the oral cavity mucosa or in and around the mouth due to refusal by the child and the concomitant force by the assailant. The confirmation of oral or peri-oral gonorrhoea or lesions associated with HIV for example oral candidacies are highly likely to be associated with child sexual abuse.
Another frequent presentation will be bite marks [4]. While it can be alleged that the bites were made by peers or siblings, or as self inflicted, a careful forensic investigation may reveal whether or not the bites were made by an adult. In these scenarios it is important to distinguish a human bite mark from that of an animal origin and then from a peer child or an adult. A swab taken from the site for DNA and a careful forensic bite mark investigation can reveal the perpetrator. However, taking photographs, taking a swab for DNA and then timely attending to the analysis is important in this regard for administering justice. Dental neglect is another common occurrence. According to American Academy of Paediatric Dentistry, ‘dental neglect is wilful failure of parent or guardian to seek and follow through with treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and discomfort’. If oral diseases of the child are left untreated without taking the child to a suitable clinician, then it can constitute dental neglect. In countries like Sri Lanka where all dental and medical health care is free for people, the responsibility of the guardian to seek dental health care rises. On the contrary, if the dental clinicians attending to children, neglect them either by not treating or not preventing dental diseases among the children they treat, that too can constitute dental neglect. With authors experience in a forensic set up, the commonest presentations of child abuse in Sri Lanka are contusions intra and peri oral, then fracture, dislocation or exfoliation of teeth. Author has reported mandibular fractures and fractures in teeth in chronic physical child abuse cases [5]. Further, corporal punishments especially by school teachers and parents where assault to face lead to dental injuries are common in Sri Lanka due to the cultural acceptance of physical child control.
Conclusion
Child abuse is prevalent in any society and the dental clinician should be aware and vigilant in managing children with suspected dental or oral presentations. Given the focus is more on the clinical management of the condition, a busy dental clinician can easily missing a child abuse being detected especially when the history given by the parents or guardian is misleading. Further, if the patterns of injuries are inconsistent with the history provided or there is evidence of repeated oral and dental injuries with multiple time intervals, it is highly likely that the child is being abused. In such a suspicious situation, it is the responsibility of the dental clinician to initiate a medico-legal management involving the authorities.
Pregnancy with Myelomeningocele Foetus: A Case Study
Introduction
Neural tube defects are the congenital malformation of the CNS resulting from defective closure of the neural tube during early embryogenesis between 3rd and 4th week of intrauterine life. It involves defect in the skull, vertebral column, the spinal cord and other portion of CNS. It occurs about 1 to 5 per 1000 live births. Risk in second siblings is high. The exact cause is not known, but the triggering factors are maternal radiation exposures, anticonvulsive drugs, exposure to chemicals, folic acid deficiency and genetic determinant [1]. The most common neural tube defect is Spina bifida contributing one in 1000 births. Spina bifida is the congenital defect of the spinal column due to failure of the fusion of vertebral arches with or without protrusion of the meninges and dysplasia of the spinal cord [1]. It is classified as spina bifida occulta and spina bifida cystica. Myelomeningocele is most common and severe form of spina bifida cystica, characterized by protrusion of spinal cord through the open vertebrae into the amniotic fluid. The severity of disability varies in accordance to the neurological and extent of intracranial abnormalities. The malformation is associated significant lifelong disability including motor and sensory deficits, neurogenic bowel and bladder, hind brain herniation and associated hydrocephalus, orthopaedics abnormality and cognitive deficits [2].
Case Report
We report a case of 25years old multigravida woman with 5 months of amenorrhea with meningomyelocele foetus admitted to labour room for termination. Her history says that she has 6 years of marital life and it was nonconsanguineous marriage. There was history of use of oral contraception for four years after marriage. Regarding her obstetrical history, she underwent induced abortion one and half year back as she was diagnosed as anencephalic foetus at 12weeks. The patient given a history of regular menses. After one year of her induced abortion she again conceived naturally. Ultrasonography was done at 8weeks in which no abnormality was detected. After this she was not regular for her follow up. But at 20weeks she visited OPD for follow up, USG was done and report showed Lumbosacral Meningomyelocele measuring 1.76cm and 0.85cm. According to patient she was not taking the folic acid supplements due to the side effects. Genetic counselling was given to her and her husband and was advised for termination of pregnancy. Induction of labour was started as per prostaglandin regimen. She delivered dead male foetus weighing about 520gms. Mother was counselled for pre conceptional care and regular follow up in future (Figure 1).
Figure 1: Induction of labour was started as per prostaglandin regimen. She delivered dead male foetus weighing about 520 gms.
Discussion
Meningomyelocele results in injury of spinal cord tissues and requires lifelong support and rehabilitation. If neural tube defects occurred in a woman’s previous pregnancy, increased antepartum foetal surveillance is required for the current pregnancy [3]. This surveillance should include consultation with a geneticist and targeted foetal ultrasonography to assess the foetal spine and cranium. In addition, preconception supplementation with folic acid at 4 mg/day is recommended; this dosage is higher than that advised for a woman without such a history. A recent RCT named management of Meningomyelocele showed that prenatal correction by fetoscopic or open surgery resulted in improved neurological outcomes. Prenatal meningomyelocele surgery is a complex surgical procedure that requires an experienced multidisciplinary team with dual focus on both the mother and the foetus. Despite of confirmed benefits there is a chance of PPROM, Oligohydramnios, Uterine Dehiscence and preterm labour are the challenging out comes [4]. Neurological defects in foetus occur dueto many reasons. The identified cause in present case is deficiency of folic acid and history of pregnancy with anencephaly. Women planning to become pregnant should avoid all alcohol consumption, smoking, and use of illegal drugs before and during the pregnancy, because these activities may have serious deleterious effects on the foetus. It is also advisable for the prescribing provider to review all medications and supplements the woman is taking to assess for possible teratogenicity.
Conclusion
All women of childbearing potential should be receiving folic acid at a dosage of 0.4 mg/day, in accordance with the recommendation of the US Center for Disease Control and Prevention (CDC). In this case if patient had come for regular check-up and taken folic acid regularly this incidence could be prevented. This is very important to stress on folic acid supplementation and regular follow up in antenatal advice.
Comparison of various Cement less femoral Stems in Total Hip Arthroplasty
Introduction
Total hip Arthroplasty is becoming routine procedure for various hip diseases, such as osteonecrosis of the femoral head, development dysplasia hip, and hip arthritis [1]. The evolution of various femoral stem design, fixation methods, size, and bearing surface of implants for total hip replacement have led to considerable improvement and survival in the implant life in turn leading to a great change in the quality of life of patient. The need to determine the most optimal combinations of Total hip Arthroplasty implant is based on various factors like age, bone quality and even financial constraints. In primary Total hip Arthroplasty, basically the Cementless stems comes in 2 types of prostheses, which are available as: conventional stems are a standard length of ~150 mm, compared with Short Stems, which are <120 mm in length [2].
Conventional Cementless implants in total hip Arthroplasty have shown excellent clinical results; however, it is unclear whether Short Stem prostheses can obtain the same clinical and radiological outcomes. With conventional femoral stems proximal stress shielding and thigh pain often occur after surgery. Advantages in case of Short-stem prostheses are less resection of the femoral neck, helps in having a physiological load pattern in the proximal femur, reduce stress shielding, and aids bone conservation. Hence these are beneficial for young patients as it conserves bone mass and extend the service life of prostheses. Also providing favourable conditions for revision. The short stems are mainly based on metaphyseal fixation. Few authors conducted meta-analysis found strong evidence indicated no difference in HHS and WOMAC when comparing Short Stems to Conventional Stems after Total Hip Arthroplasty.
From their studies, it was found that the short follow-up time (6 weeks) did not influence the heterogeneity of the pooled results of HHS and WOMAC. And meta-analysis found that there were no significant differences in the presence of femoral offset and leglength discrepancy. Short Stem prostheses achieved the same clinical and radiological outcomes as conventional implants, and were superior in terms of reducing thigh pain. But whether the postoperative thigh pain applied in 2nd-generation Cementless prosthesis still needs further large-scale multicenter studies with longer follow-up to confirm [3]. Short-stem hip Arthroplasty (SHA) was designed to preserve bone stock and provide an improved load transfer. To gain more evidence regarding the load transfer, this review analysed the periprosthetic bone remodelling of SHA in comparison to standard hip Arthroplasty. Periprosthetic bone remodelling is also present in SHA, with the main bone reduction observed proximally. However, certain SHA stems show a more balanced remodelling compared to Total Hip Arthroplasty, arguing for a favourable load transfer. Also, the femoral length where bone remodelling occurs is clearly shorter in SHA [4].
In another study which has compared the bone quality by using Bone mineral density noted the following findings – With a mean follow-up was 3.35 years in two groups. Bone mineral density was significantly increased in femoral zone 1 but slightly decreased in zone 7 in the short, metaphyseal-fitting stem group. In the conventional metaphyseal and diaphyseal-fitting stem group, bone mineral density was markedly decreased in both zones 1 and 7. Clinical and radiographic results were similar between the 2 groups. No hip in either group required revision of the components [5]. One of the studies on ultra short stems came out with following findings: At follow up into the second decade, ultra short stems showed no differences from conventional cement less stems in terms of validated outcomes scores or fixation, while showing slightly less stress shielding and less thigh pain, although this difference may not have been clinically important; in the conventional group, thigh pain was mostly mild, and there were no differences in hip scores. Reduction of stress shielding may reduce the long-term risk of periprosthetic fracture, but this was not shown here. Future studies might document the reduction of the long-term risk of periprosthetic fracture by reduction of stress shielding [6].
Finally to conclude choosing the right kind of femoral stem, the surgeon should keep an optimal distribution of stress in proximal femur, implant design should have maximal preservation of bone without compromising stability and for long term survival. So with the recent trend going towards maximal bone preserving and Cement less fixation, there are results with an array of stems showing difference in results and implant survival. There is a lot of observational data presented in the large National Registry reports which are updated annually (e.g. UK NJR, Australian Registry, Swedish Registry), and have data on important outcomes, even revision rates of hundreds and thousands of patients who have received different variety of prostheses over one decade and more. But still these have shortcomings like delay in reporting, misclassification of outcomes and few missing reports.
Obesity is considered the most common chronic metabolic disease associated co morbidities such as diabetes mellitus and hypertension [1]. The public health problem results primarily from an energy imbalance whereby dietary energy intake exceeds energy expenditure. The dynamics of this imbalance are complex, especially the appetite regulation are not fully understood [2]. Nutrition in early stages of growth may be essential in the development of obesity in adulthood, supporting the concept of “nutritional programming” [3,4]. However, the mechanisms that link nutrition with long-term obesity risk are not well defined. Several systematic reviews have linked breast milk intake with a protective effect against obesity and other metabolic diseases [5,6]. Breastfeeding may play an important role in this “nutritional programming”. Human milk is a source of various growth bioactive factors, namely leptin, adiponectin, ghrelin, resistin and obestatin, which are involved in food intake regulation and energy balance. Some study referred the preventing function due to these bioactive factors’ roles other than nutrition [7,8]. In this review, we talk about bioactive factors contained in human milk and their potential protective effect on obesity.
Breast-Feeding and Childhood Obesity
The rapid growth velocity during the early postnatal period ,especially 0~3 months, have been associated with an increase in the number of adipocytes, a higher ratio of fat mass to lean mass, a greater central fat deposition and insulin resistance and consequently an increased risk of metabolic syndrome, namely obesity, type 2 diabetes et al. Some systematic reviews confirmed that the link between greater growth acceleration and later increased risk of obesity [9,10]. As we known, formula feeding is associated with a greater weight and length gain after birth, according to the breast feeding. Various hypotheses have been proposed to explain how breastfeeding protects against faster weight gain and consequently against later obesity [11]. Breastfeeding babies can self-control the amount of milk they consume, and so they may learn to self-regulate their energy intake better than FF infants [12].
Furthermore, the different of the nutrient composition is an important factor determining a higher risk of later obesity. Another study showed that the mother’s pre pregnant BMI, duration of breast-feeding and timing of complementary food introduction are associated with infant weight gain from birth to 1 year of life [13]. The protective role of breast milk may be attributable not only to its nutritional composition but also to many bioactive factors. These bioactive factors in human milk, such as Leptin, adiponectin, ghrelin that may control nutrient use, protect infants from pathogens and play a role in regulating metabolic pathways [14].
Hormones In Mother’s Milk
I. Leptin: Leptin can be produced by mammary epithelial cells. It exerts an orexigenic effect by signaling satiety and decreasing the sensation of hunger [15]. Breast milk leptin level is higher in colostrum than in transitional milk and is decreased during the first 180 days, showing a significant inverse relation with the ongoing days of lactation [16]. Schuster et al. and Fields et al. [17,18] demonstrated that leptin concentration in milk had been positively correlated with circulating levels of leptin and maternal BMI, suggesting that BF infants nursed by overweight/ obese mothers might be exposed to higher amounts of leptin than infants nursed by lean mothers. Although the mechanisms are unknown, a higher concentration of circulating leptin has been found in infants fed breast milk than in infants fed formula [19]. Maybe the higher level of breast milk leptin could regulate the appetite and exert a long-term effect on energy balance and body weight regulation. Dundar et al. [20] found that SGA infants grew more rapidly during the first postnatal 15 days than AGA and LGA infants, and that human milk leptin levels were significantly lower in the SGA group. However, there is some inconsistent view. Wang et al. [21] found that the leptin level of human milk showed no significant difference between preterm groups with term group, had no correlation with weight, length at 42nd day.
II. Adiponectin: In humans, adiponectin regulates lipid and glucose metabolism, improves insulin sensitivity, inversely related to the degree of adiposity and inhibits hepatic glucose production [8]. It is regulated by factors such as IGF-1 that stimulates its gene expression and secretion [22]. In 2006, it was the first time to report the presence of immuno reactive adiponectin in human breast milk. The authors also found the adiponectin levels in human milk were significantly higher than leptin levels, and decreased with the duration of lactation [23].
This adipokine secreted in human milk can cross the intestinal barrier and may modify infant metabolism. The levels of this hormone in human milk correlate positively with the serum level and inversely with infant weight and anthropometry during the first months of life [14,24]. Andreas et al reported that premature newborns have a lower concentration of adiponectin than term infants [25]. In the study of obese mothers, although serum adiponectin levels were low in obese mothers, their colostrum exhibited high levels of this hormone. Maternal BMI was positively associated with serum adipokine levels and negatively correlated with colostrum adipokine levels [26]. The offspring of obese mothers has the occurrence risk of metabolic syndrome, breast-feeding is a protective method.
III. Ghrelin: Ghrelin is also produced in the mammary gland, it can influence glucose metabolism, energy balance, gastrointestinal motility, gastric acid secretion, and cardiovascular and immune system function [27]. It can stimulate food intake in rats and humans.64 by acting primarily on the accurate nucleus of the hypothalamus [28]. In fact, ghrelin occurs in both term and preterm human breast milk, the level is higher in breast milk than in plasma its levels, higher in whole milk than in skim milk [29]. The ghrelin level increases gradually in colostrum, and in transitional and mature milk [30]. Cesur et al. [31] reported that active ghrelin level in breast milk at the 4th month of lactation significantly and positively correlated with weight gain of the infants. In new borns’ levels of ghrelin were higher in SGA babies than in AGA babies. Reduced ghrelin suppression and higher postprandial ghrelin levels in SGA infants could result in a sustained orexigenic drive and could contribute to postprandial catch-up growth in these infants [32].
Savino et al. [33] observed significantly higher serum ghrelin levels in formula-fed compared to breast-fed infants. They suggested that formula fed infants received a higher amount of ghrelin, thus it was possible that they had a greater feeding stimulus than breast-fed infants and this correlates positively with a greater infant weight gain, possibly with an influence on the growth of the childhood. The resist in human breast milk was first identified in 2008 where the levels in milk decrease throughout lactation [14]. Its physiologic role in humans is still under debate and very little is known in children. Resist in has been shown to be associated with insulin resistance in obese mice [34]. It suggested that resist in could be involved in appetite regulation and in the metabolic development of infants. Moreover, it was advanced that it plays a role in controlling bodyweight through effective regulation of adipogenesis by negative feedback. However, in humans, the role of resist in fetal and infantile growth remains to be elucidated [35]. Other bioactive factors, such as apein, obestatin, nesfatin-1, can identified in breast milk. These substances may be regulate food intake and metabolism, however, the role of these bioactive factors in breast milk affecting the childhood growth is still not reach an agreement.
Conclusion and Perspective
Breast milk contains necessary nutrients and bioactive factors for infant health. The composition of breast milk varies according to stage of lactation and to the nutritional requirements of the infant. It is an advantage that is not comparable by formula feeding. The bioactive factors may represent the link between breast-feeding and protection against obesity in later life, which need large scale long term cohort study to confirm.
Factors Associated with Low Back Pain Among Nurses in Critical Care Units, Hospital Universiti Sains Malaysia
Introduction
Low back pain (LBP) is one of the most serious health problem of tremendous medical and socioeconomic dimension and a major cause of disability. Low back pain can defined a pain localized between the 12th rib and the interior gluteal folds, with or without leg pain. Nurses are known to be a high risk group for occupational low back pain [1,2]. Direct care nursing personnel around the world report high numbers of work-related musculoskeletal disorders. The impact of LBP for nurses includes time off work, increased risk of becoming chronic, as well as associated personal and economic costs [3]. Nurses who suffer from chronic back pain will have an impact on them while standing up from sitting and lifting the patients. For direct care nursing staff, manual handling of patients such as moving or repositioning a patient using their own body strength is the major cause of these injuries [3]. Indeed, 80% of the general active population suffers from LBP at least temporarily [4]. His study with 350 employees shows that common LBP is the first reason of affections limiting professional activities before 45 years and the third after respiratory and traumatic affections between 45 and 65 years. In western countries, many of studies researched on back pain as a common problem for nurses [5]. Statistics in Hospital Universiti Sains Malaysia (HUSM) show that number of patients with back pain including nurses in year 2007 was 37, in year 2008 was 31 and in year 2009 were 26 as in physiotherapy records. Thus, this study intends to identify factors associated with back pain among nurses in critical care unit at HUSM, Kubang Kerian, Kelantan. The general objectives of this study was to identify employment profile of the nursing profession that were associated with LBP; determine personal factors of nurses related to LBP and explore work related factors associated with LBP.
Materials and Method
A cross-sectional study design was used to examine factors that are associated with LBP among nurses using a self-administered questionnaire conducted among nurses working in critical care units (CCUs) in HUSM. The questionnaire used consists of three sections; Section A is on the demographic data consisting of 10 items and Part B consists of 25 items on nursing and LBP and Part C is on treatment options consisting of 10 items. The questionnaire items were adopted from Branney and Newell [1]. The English version of the questionnaire was translated into Bahasa Malaysia and back translated to English by two independent professional translators. After it was back translated, it was found to be similar to the original one. To ensure the validity of items in the questionnaire, a pilot study was done at Hospital Raja Perempuan Zainal II (HRPZ II). A total of 30 nurses participated in this pilot study with informed consent. The questionnaire took approximately 15 to 20minutes to complete. Cronbach’s alpha obtained for this pilot study was 0.75 which indicates a reasonable internal consistency. This study was approved by the Human Research Ethics Committee USM, USMKK/PPP/JEPeM [246.4.(1.4)] and Jawatankuasa Etika & Penyelidikan Perubatan Kementerian Kesihatan Malaysia, (2) dlm KKM/NIHSEC/08/0804/P12-41.
Results
The total population of nurses working in all five wards adds up to 180; 8 Selatan consists of 31 nurses, ICU 51 nurses, Kristal 24 nurses, CCU 25 nurses, and HDU 49 nurses. However, only 110 (81.5%) participated in this study in February 2012. Majority of the participants were female nurse 85 (77.3%) while 25 (22.7%) participants were male nurses. The majority of the participants were Malays 101 (91.8%), there were six Chinese (5.5%) and three Indians (2.7%). Their qualifications differ; two (1.8%) with masters degrees, 11 (10%) with basic degrees, 94 (85.5%) diplomas and three (2.7%) with school certificates. The participants form four age groups. There were 50 (45.5%) nurses aged between 20-30 years, followed by 46 (41.8%) nurses aged between 31-40 years, then nine (8.2%) nurses aged between 41-50 years and lastly five (4.5%) nurses aged between 51-60 years. The majority of the nurses 90 (81.8%) in this study were married while 20 (18.2%) were single. The majority of nurses, 51(46.4%) have a total of 1-3 children, 34 (30.9%) have none, 19 (17.3%) with 4-5 children and lastly six (5.5%) of the nurses have more than five children.
When the nurses were categorized based on their BMI, most of the nurses 57 (51.8%) were overweight, 47 (42.7%) had normal BMI while six (5.5%) were underweight. (Table 1) shows the association between employment profile of nurses and LBP. Results show that working experience in current ward and years of nursing experience were significantly associated with LBP. However, current working ward, working time, total hours of working per week and total patients who need mobilizing were not associated with LBP (Table 1). Table 2 shows the association between individual factors and occurrence of back pain. Crosstab Chi-square tests or tests of independence were carried out to determine individual factors related to LBP among nurses in CCUs. Age, marital status, total number of children, height, weight and BMI, smoking and regular exercise or sport were not significantly associated to LBP among nurses in CCUs (Table 2). After cross tabulation, Pearson Chi- Square test was used to determine the association between work-related factors and occurrence of LBP. Only one factor, frequency standing had significant association with low back pain (p=0.021). However factors such as frequency of lifting patients in bed during shifts, helping patients to get out of the bed during shifts, poor body mechanics during lifting of patients, frequent carrying of heavy medical equipment during shifts, frequent moving of the beds during shifts, too much work to do, staff shortage in ward and stress were not significantly associated with low back pain among nurses (Table 3).
Table 1: Association between Employment Profile and LBP.
Table 2: Association between Individual Factors and LBP.
Table 3: Association between Work Related Factors and LBP.
*Significant difference at p<0.0.
Discussion
There was a significant difference in LBP between pre entering nursing and since entering nursing (p<0.001). This study demonstrates that the prevalence of LBP among the nurses studied increased from 16.4% pre nursing to 68.2% since entering nursing, which is rather close to studies done in western countries. Low back pain is a major problem in the nursing profession and it was reported that 30% and more nurses experienced low back pain during the nursing course of one year [6]. It was reported that only 15.9% nurses had LBP before nursing while 84.5% complained they had LBP after nursing [7]. There was a six percent increased risk of LBP from pre-nursing prevalence while the cumulative lifetime prevalence of LBP increased from 31% at entry to 72% at the end of nursing school [4]. Working experience at current ward and total years of nursing experience were related to LBP among nurses. The findings of this study show nurses with more than 20 years experience reported the highest LBP (32.7%) whereas nurses working less than one year reported the least (4.5%). Occupational back pain and level of seniority were positively related [8].
In another study on those with LBP, 59.5% had more than five years of nursing experience and another 12% had more than 20 years nursing experience [7]. Findings from this study indicate that the nurses working in Intensive Care Unit, ICU (29.1%) and High Dependency Unit, HDU (20.1%) were more likely to report current back pain compared to other units. In both ICU and HDU, most patients are usually dependent, frail and need more help from nurses for their daily activities and transfer compared to those in other wards [9]. Nurses who are working in ICU experienced an increased rate of LBP compared with other CCUs. Similar results were obtained in 65 ICU in 22 South Korean hospitals and among 1345 subjects where 90.3% had back pain [10]. In addition, Nurses with 2-4 years of working experiences in ICU had the greatest probability of back pain and needed treatment. Although most hospitals allow patient’s family to stay in the ward help to take care of the patient, the availability of family members to do this caring in hospital was low in busy city [9]. Report had shown a 65% lifetime and 70% point prevalence for low back pain among nurses working in the orthopaedic unit as well as 58% lifetime and 75% point prevalence of low back pain for those working in the intensive care unit [5]. More nurses with more than 20 years nursing experience including year three student nurses had LBP (40%) compared to nurses with 1-10 years working experience (24.5%). In another study, 12% of nurses with more than 20 years working experience suffered LBP [7].
This study found most nurses working shift had LBP (64.5%). Comparing the back pain prevalence across AM, PM and nightshifts, the staff working on AM shift are more likely to experience back pain (28.3%). However there was a higher prevalence of back pain during the night shift (6.6%) compared to the PM shift (1.5%) [8]. There was a 64% increase in LBP among those who reported staff shortage and working six or more night shifts per month [10]. Nurses working on the AM shift were more likely to experience back pain. Most of patients’ hygiene needs such as bed sponging, assisted baths and treatment procedures are carried out during the AM shift, which involves a lot of patient lifting and transferring. Nurses with total working hours between 31-40 hours per week had higher occurrence of LBP (21.8%) while those working between 10-20 hours per week had less LBP (1.8%). Nurses working more than 50 hours per week had the most LBP (50.0%). Study had shown that nurses working more than 20 hours per week had symptoms of LBP [11]. Nurses who were handling and mobilizing between 1-5 patients per shift had the most LBP (47.3%) while those without such patients the least (5.5%). Study had reported LBP among 58.4% of nurses handling and mobilizing between 1-5 patients but only 6.7% among nurses who did not have to [7].
Younger nurses aged between 20-30 years (37.3%) had the highest LBP while older nurses aged between 51-60 years had least LBP (4.5%). Studies had shown that nurses between the ages of 20 to 30 years had the highest prevalence of occupational back pain [8,12,13]. Junior nurses had higher rate of back pain because they were more involved in manual work, while the senior staffs were assuming more of organisational and managerial roles. Junior nurses were also less knowledgeable in the proper techniques of lifting and body mechanics. Senior nurses could have developed effective coping strategies over time. Younger nurses also had more problems related to job stress than older nurses [8]. Another study showed that nurses aged 50-59 years were most affected by LBP [14]. However, there is the healthy worker effect, that is those who suffers from LBP tend to leave their hospital jobs, whereas the healthy nurses stay [1,9]. Female nurses tend to experience more back pain [1,7,12,15-18]. Results of this study showed that 64.5% of female nurses and 20% of male nurses had LBP. More married women had LBP compared to unmarried women. The finding of this study indicated that 69.1% married women had LBP in their lifetime. Various studies reported that more married women had LBP. As high as 85.8% women who were married had LBP [4]. LBP are more common among nurses with multiple pregnancies. Our study found that 34.5 % nurses with 1-3 children have LBP.
This is similar to the report that 51.5% nurses with multiple pregnancies experienced LBP [4]. Female participants reported that their back pain was attributed to pregnancy and childbirth [19]. Obesity, which is one of the contributing factors for lumbar pain, leads to decreased abdominal muscle strength and increases the level of lumbar-lordosis. This is supported by this study where 46.4% of those who were overweight had LBP. Studies showed that lifting, prior injury, and being overweight were risk factors for workrelated low back injury (WLBI) among nurses [5]. Age, increased BMI and disturbed psychological profile were among other individual factors shown to be related to increased risk of WLBI [4]. Smoking was cited in the literature as having a negative effect on the circulatory system. Cigarette nicotine causes vasoconstriction that reduces the blood flow to the muscles and intervertebral discs. This predisposes smokers to low back injuries [5]. Increased coughing among smokers may be related to increased risk of low back injuries in this group [4]. There was a strong relationship between smoking more than 20 cigarettes a day and having back pain and intervertebral disc degeneration. Study done in Japan indicated that smoking was associated with LBP [7].
There was no significant relationship between smoking and back pain in this study, only 12.7% of the nurses smoked and had LBP while 71.8% had LBP but did not smoke. Smoking can cause other illnesses related to smoking in addition to back pain [20]. A smaller percentage of the nurses who exercised regularly (35.5%) had LBP compared to 49.1% of nurses who did not exercise regularly. Although there was no significant relationship between exercise and back pain, the group of people who did not exercise regularly are at a greater risk for back pain. However exercise or sports did not play a protective role against LBP [7]. Several factors can cloud these results namely, the level of competition, nature of sports activities as well as the volume and the intensity of the exercises. In this study professional factors chosen by nurses as causes of LBP were frequent lifting of patients in one shift (78.2%), helping patient to ambulated (80.0%), poor body mechanics (72.2%), frequency of moving the bed (72.2%), frequent standing (63.6%), too much work (61.8%), shortage of staff (51.8%), and stress (86.7%). The nursing job is more to helping, turning and lifting the patient from chair or bed [9]. This study shows that 78.2% nurses who did frequent lifting and 80% nurses who helped patients had LBP.
Considering that nurses often work 12 hour-shifts, the amount of lifting adds up and the job could be very hard to manage physically [5]. Some studies suggest that positioning patients in bed leads to LBP more often than other manual patient transfer procedures conducted by nurses [21,22]. Nurses who handled patients more frequently have low back pain prevalence rates that were 3.7 times higher [23]. Among nurses who had LBP, 72.7% chose poor body mechanics as the factor. According to National Institute of Occupational Safety and Health (NIOSH) lifting guidelines, the maximum recommended weight to be lifted by women in the 90th percentile of strength is 46 lbs. Nurses were commonly led to believe that the primary way to prevent back injuries was to always use proper body mechanics. However, the fact remains that some tasks were so stressful to the body that even with proper body mechanics, a back injury resulted [22]. Rooms in hospital are often small, and nurses had to move the furniture around so that they can do their jobs. Most of the time nurses are lifting devices that would not even fit in these rooms; these are some causes of LBP [5]. Some patients may also be combative, contracted, or uncooperative. Any unpredictable movement or resistance from the patient may throw the nursing personnel off balance during the transfer, resulting in back injury [5].
In addition, fatigued muscles can no longer serve their protective function and may add to the risk of acute trauma [22]. Workplace guidelines should limit manual handling exposure in general or enable nurses to undertake reduced manual handling activities when in pain [12]. Shortage of staff is also one of the factors contributing to LBP. This study indicated that 51.8% nurses who suffered LBP chose staff shortage in wards as the factor. Surprisingly, low work support, low mood, and boring work tasks were not identified as MSD risk factors in this study. In this study 59.1% of nurses who complaint of stress had LBP while only 25.5% of those who did not complaint of stress had LBP. This is supported by study where 57.3% of stressed nurses suffered from LBP [7]. As such, these results suggest that psychosocial issues are fast becoming increasingly important MSD risk factors for nurses in Asia as elsewhere.
Conclusion
The results of this study demonstrated that the prevalence of low back pain among nurses at HUSM was only 16.4% before entering nursing but 68.2% upon entering nursing. The difference in LBP between pre nursing and since nursing was significant (p=0.001). Furthermore, nursing employment profile such as working experience in current ward (p=0.004) and nursing experience (p=0.038) were significantly related to LBP. Current working ward, working time, total working hours per week and total patient need mobilizing were not associated with LBP. None of the individual factors studied were significantly associated with LBP among the nurses. As for the work related factors, frequency standing during shift was found to be associated with LBP (p=0.021) while other factors were not significantly associated with occurrence of LBP.