Biomedical Journal of Scientific & Technical Research (BJSTR) is a multidisciplinary, scholarly Open Access publisher focused on Genetic, Biomedical and Remedial missions in relation with Technical Knowledge as well.
Autologous Expanded Mesenchymal Stem Cell Implantation for Orthopedics Conditions as a Non- Surgical Approach
Introduction
This article aims to address best practices in regenerative medicine using autologous expanded mesenchymal stem cells (MSCs) combined with platelet-rich plasma (PRP). We summarize our findings from various literature reviews and our experience using combined fat-derived expanded MSCs-PRP therapy in many hundreds of clients for osteoarthritis (OA) and tendinopathy, namely tendon tear(s). Generally, the doses we use in large areas ranging between 50-100 million MSCs in 2 MLS of fluid combined with 5-8 MLS of PRP in the same syringe depending on the size of the area(s), but in smaller joints, we modify the number of cells and PRP volume. We also found that concentrated MSCs without PRP is more effective for small joints of the hands and feet. The number of MSCs used in the expanded technique makes the therapy more effective than the low number used in the same-day procedure, i.e., the stromal vascular fraction (SVF); thus, expansion of MSCs is encouraged if the regulatory authority allows this practice. Additionally, we can adjust the volume accordingly by adding more PRP to the mixture to cover more expansive areas. There are three main questions to ask; what is the mechanism of action of this combined therapy? Does it work? And is it safe? MSCs are multipotent cells with a regenerative effect via both direct and indirect effects. The explicit incorporation into injured and adjacent tissue (i.e., cellular engraftment), while the indirect pathway is related to un-engrafted MSCs producing paracrine signals cytokines that contribute to tissue regeneration by promoting growth and differentiation of local cells [1]. They have an anti-inflammatory effect, immune modulation, and anti-apoptosis (programmed cell death) effect. In addition, MSCs can self-renew and differentiate into various cells like chondrocytes, tenocytes, or other cells depending on where we implant them [2]. PRP works by the activation of the platelets by the release of their intracellular cytoplasmic granules. Those particles contain inflammatory and growth factors which could be responsible for the healing process. The common ones are Platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), transforming growth factor (TGF)-beta, fibroblast growth factor (FGF), and epidermal growth factor (EGF) [3]. Randomized and non-randomized clinical trials showed positive outcomes to the MSC therapy, particularly in knee OA [4]. In our practice, we found a success rate of an average of 70-80 %, with best results for the knee involvement followed by the hip and shoulder OA; the good results are more seen in appropriately selected candidates with osteoarthritis “non-boneon- bone pathology.” We calculated success rate based on symptom control, quality of life improvement, slowing or stopping the radiologic progression, and eliminating the need for surgery at least in the first five years of its use. We might need to repeat the implantation in some cases. This therapy is favored over the surgery by speedy recovery, comfort in performing routine daily activities, quick return to work and sport. We noticed good effect does vary starting from two weeks post-therapy for up to a year to see the maximum benefit. The good news with this technique is that we can cryopreserve the MSCs in liquid nitrogen for up to fifteen years; this will allow us to repeat the implantation if needed or implicate it in other joints. While the degenerative process takes many years thus regeneration is also a slow process; therefore, we feel repeating imaging too early will not reveal the appropriate comparison. We have concluded MSC therapy stops or slows the progression of osteoarthritis and, on some occasions, recovers some of the cartilage thickness, but those are inconsistent findings and slow processes [4,5]. The main obstacle with cartilage regeneration is the lack of direct blood supply but instead takes it from the subchondral bone and nutrients from synovial fluid. Modified scaffolding techniques like exosomes and hyaluronic acid (HA) might potentiate the effect of stem cell therapy. Exosomes are micro-RNA particles that enhance cell-cell communication [6]. HA has viscous-supplementation physiologic and anti-inflammatory, anti-oxidative, and immune-regulatory pharmacologic positive effects in OA [7]. We believe any scaffold(s) with anabolic effect including PRP, HA, exosomes, and collagen would add substantial synergistic benefit to the MSC therapy. In terms of tendons regeneration, we have found that the combined MSCs-PRP therapy is significantly effective in symptom control, substantially improves range of motion, and may eliminate the need for surgery [8-11]; in our practice, the success rate is 80-90% of the cases. The clinical benefit was noticed even when there was no clear radiological evidence of tendon healing. We have observed MRI healing of rotator cuff tears and Achilles’ tendinopathy, although the result was inconsistent. Some factors might affect the Efficacy of MSCs-PRP therapy, including local anaesthesia use inside the joint or tendon injected due to its toxicity to both MSCs and platelets. Alcohol and non-steroidal anti-inflammatory medicine before and after the stem cell implantation can reduce its Efficacy, while the use of turmeric/Boswellia as natural preparation help to reduce the inflammatory response post-implantations of the stem cells. The safety of autologous MSCs is well tested in several clinical trials; it has shown no evidence of rejection given both the blood and the cell-based therapies are derived from the same individual. There is no evidence of developing malignancies in autologous adult MSCs [12,13]. We avoid using MSCs-PRP in patients with active cancer or in remission with invasive cancer for at least five years from its onset to prevent overstimulation of the pre-existing cancer cells. Additionally, both PRP and MSCs have some antimicrobial activity [14,15]; thus, infection is infrequent, particularly we sterilize the expanded cells with both antibiotics and antifungal solutions. Also, we adapted single-use sterile PRP tubes. In summary, we believe this is future medicine. However, more work and research are needed to advance and standardize the best protocol by choosing the correct number of MSCs used in each area and the PRP dose and centrifuge technique to ensure the maximum effective and safe doses.
In our classical view, inflammation is triggered by environmental changes; may it be pathogens or tissue damage. The stimuli activate a complex transcriptional program that is both cell type and stimulus specific. At the cellular level, a complex gene expression programs that include hundreds of genes is activated within minutes after the initial activation through a stimulus [1]. But this response can vary not only between cell types [2], but even within a cell population depending on their niche environment [3]. In response to inflammatory stimuli, several response pathways can be initiated, including signal transducers and activators of transcription (STAT) [4], activator protein 1 (AP-1) [5], the nuclear factor of the κ light chain enhancer of B cells (NF-κB) [6], and interferon regulatory factors (IRFs) [7]. All these triggers have distinct binding specificities and have different receptor – ligand interaction that leads to a specific transcriptional output. For example, cytokines acting primarily through the activation of STAT TFs such as IFN-γ, are in general unable to activate NF-κB and AP- 1, which are broadly responsive to a large panel of inflammatory stimuli (stretching from LPS and other microbial products to tumor necrosis factor [TNF]-α) [8]. Inflammation in general, is therefore essential for survival in the adult. Specifically, the blood system responds with cell proliferation, HSC self-renewal and progenitor expansion and differentiation.
Hence, it is all the more striking that these pathways are essential for the HSC generation in the embryo, although the mammalian fetus is protected from pathogens by a robust innate immune system at the maternal/fetal interface [9]. During embryonic development, the first Transplantable HSCs are detected between E10.25-E11.5 in the aorta- gonad and mesophephros region (AGM) [10-12] as residents of Intra-aortic hematopoietic clusters (IAHC) that are closely associated with the ventral wall of the dorsal aorta [13-15]. Although to total number of hematopoietic (cKIT) positive cells in the AGM is believed to total around 600 cells, only a small fraction is HSCs [10,16]. In general, blood cells trans-differentiation of specialized endothelial-like cells that can generate blood, termed hemogenic endothelium (HE), to hematopoietic fate during early development. This process is called endothelial to hematopoietic transition (EHT) [17-24]. All the more, it´s remarkable that IL-1RI, that is a receptor for IL1 and leads to NF-κB and c-Jun N-terminal kinase (JNK) activation [25], is expressed by cells in the E11 aortic endothelial and mesenchymal cells, and at low levels in the IAHC [26].
Upon stimulation with IL1β, AGM explants show higher levels of CXCR4, a chemokine receptor that is specific for stromal cellderived factor-1(SDF-1) required for homing of hematopoietic cell to their niches. The importance of signaling through IL1R1 was further confirmed in transplantation settings; IL1R1 mutant AGM cells showed reduced HSC activity [26]. In fact, recent reports show a correlation of CXCR4 expression and HSC activity in the AGM [27]. In agreement with these findings, Tnf α and TnfR2 morphant zebrafish embryos have decreased expression of the hematopoietic markers runx1 and cmyb, and a NF κB reporter line confirms its activity within the ventral domain of the aorta [28]. Interestingly, the authors find aberrant notch signaling, eg decreased levels of Jag1a, which is required for IAHC formation [28,29]. In parallel, a study on Tlr4, MyD88 and NF κB, a core of inflammatory signaling axis leading to nuclear p65, came to comparable conclusions; they found decreased numbers of hematopoietic cells in the aorta of these morphants, and established a link to aberrant notch signaling in this study, the authors found a reduced induction of the notch downstream effectors Hey1/2 and her15.1 [30]. If this lower notch status is due to reduced Jag1a expression as suggested by Espin-Palazon et al. is not known. Interestingly, in the same study, the authors also investigated the HSC activity in the AGM of TLR4 deficient mouse embryos. TLR4 deficient hematopoietic cells in the AGM could generate CFU-C, albeit at a reduced number, but strikingly, almost all HSC activity was diminished in transplantation assays [30]. These studies highlight the high susceptibility of HSC to NF κB signaling, but the HSPCs, the more differentiated cells show a less substantial dependency. Nevertheless, it´s still unclear which target genes are activated by p65 mediated NFkB signaling in HSCs and HSPCs.
In an elegant study by Li et al. the authors subjected E10.5 embryos that express GFP under the Ly6a/Sca1 promoter, a marker of HSPCs, including HSCs, to different cytokines [31]. Here they found moderate increases in Sca1 expression after treatment with IL1β, IL6 and TnfA in the AGM region, but treatment the Inf α4 or Inf γ lead to a huge increase of Sca1 expression in the AGM, including the aorta. The increase in Ly6aGFP+ was due to both, higher expression of Sca1GFP, and enhanced proliferation [31]. In order to determine if there were HSPCs that can receive both Ifnγ and Tnfα simultaneously, combinatorial MO knockdown of Ifnα and Tnfγ was used in zebrafish embryos. Knockdown of both cytokines together caused a greater decrease in hematopoietic gene expression (runx1) in the dorsal aorta than the knockdown of either gene alone, indicating that multiple inflammatory cytokines can cooperate in the formation and expansion of embryonic HSPCs in the absence of pathological stimulation.
Interestingly, blood flow is needed for the expression of ifng1-2, as ifng1-2 was nearly absent from the axial vessels of tnnt2 (silent heart) morphants that don’t have a blood circulation [32]. The reason for this curious observation was not further clarified, but recent studies might provide a plausible explanation. Blood flow might be needed to enhance the sources of inflammatory cytokines to the dorsal aorta.
Detailed analysis of the cellular composition of the AGM microenvironment using mass cytometry (CyTOF) revealed the presence of yolk sac derived macrophages closely associated with IAHC [33]. Prior to HSPC generations in the AGM, the yolk sack produces HSC independent blood progenitors, including macrophages that express different receptors to interact with their niche cells, including Cx3cr1 and Csfr1 [34,35]. Time course analysis with a Csf1r:GFP transgenic mouse model that labels Yolk sac derived macrophages, the study elegantly demonstrates their arrival in the AGM from E9.5 and significantly increasing in abundance by E11.5, ie in time for the HSPC and HSC emergence [33]. Cx3cr1, a chemokine receptor was identified on the macrophages, whereas the possible interacting ligand, Cxcl12, was highly expressed by HE cells. Ablation of Cx3cr, or pharmacological of macrophages with BLZ945, an inhibitor of the colony stimulating factor 1 receptor (CSF1R) reduced CFU-C numbers and HSC activity in transplantation assays. The authors further identified a subpopulation of macrophages based on their cell surface expression of CD206 that specially upregulate cytokine expression of Tnf, Ccl24, Ccl9, Igf1, Bmp2, Pf4, Ccl2, and Ccl7, Whereas Ifnα, Ifnγ, and IL1β expression was observed in all AGM macrophages [33].
In summary, inflammatory signaling pathways are essential for hematopoiesis in the AGM in general, and most importantly, positively influence HSC activity. There is some evidence that some cells are susceptible to more than on the cytokine stimulus at a time [32]. In summary, during development, inflammatory signaling pathways are activated to establish cell identity. It will be important to study the impact of cytokines individually or combined in different cell populations in order to understand the gene expression changes that they inflict. Perhaps the multitude of single cell data sets on AGM cells can give us more clues. Here, we can readily distinguish between the blood cell types and profile their gene expression for inflammatory signaling members. In fact, several single cell data sets of AGM derived cells showed enrichment of inflammatory signaling pathway activation in HE and IAHC [36- 38]. Further, detailed analysis of these data sets can help to improve our understanding of these stimuli in HSC emergence and helps us to improve in vitro approaches to generate HSC by artificially fine tuning these cytokines in culture conditions.
Ultrasound-Guided Aspiration Therapy for Surgical Site Infection After Spinal Surgery:A Report of three Cases
Introduction
Surgical site infection (SSI) is a common and dreaded complication after posterior spinal surgery. Reported risk factors for infection include patient factors such as age, male sex, diabetes, obesity, smoking, malnutrition and being immunocompromised, as well as intraoperative factors such as long operation time, blood transfusions, open surgery, a greater number of levels operated on and employment of intraoperative equipment including microscopes or CT [1-3]. The infection following spinal instrumentation remains a challenging and controversial subject, as it is positively associated with prolonged hospitalization, increased healthcare costs and rate of reoperation, poorer longterm outcomes, and greater dissatisfaction with the initial surgery [4-7]. To treat SSI, surgical removal of internal fixation is sometimes required, although the loss of fixation can contribute to spinal instability [8-11]. CT-guided aspiration and drainage and drainage is a useful treatment that drains exudates, pus and necrotic tissue to reduce the chance of wound bacterial growth [12]. But these cases required multiple treatments that increased radiation and expenditure. Compared with CT, ultrasound imaging has its unique advantages: non-electromagnetic radiation, economical and convenient. Here, we report three cases of SSI of posterior spine surgery with aspiration under ultrasound guidance was successfully used to promote wound healing.
Case Reports
This study aimed to report the cases of three patients of infection after spinal surgery who underwent ultrasound-guided aspirating incisional effusion (Table 1). The cases we reported here all wrote informed consent for publication of anesthesia.
Case 1
History and Examination. A 79-year-old woman with several years of low-back pain that radiated to her feet was described. She had tried conservative management using pain medications or acupuncture but the pain continued. On examination she had hallux dorsiflexion muscle IV level. Superficial sensation was impaired over the lower legs and lateral dorsum of feet. Meanwhile she had a positive straight leg–raise test at 60°. An MRI study of her lumbar spine revealed L4–L5, L5–S1 para-central disc herniation. The patient also had a history of hypertension and diabetes that required chronic, long-term medication. Operation: This woman underwent posterior spinal L4, L5, and S1 pedicle screw fixation. Her pain improved obviously and ended the treatment of vacuum sealing drainage (VSD) on the third postoperative day. The patient received 1 intravenous antibiotics (cefuroxime) 30 min preoperatively, and 5 additional doses during 5 days postoperatively, then ceftriaxone replaced. Fifteen days after the operation, the patient presented increased low-back pain. Laboratory tests: white blood cell count (WBC): 7.7 10^9/L (normal range 4-10 10^9/L), neutrophils% NE%: 51.2% (normal range 50-70%), hypersensitive C-reactive protein (HS-CRP): 41.58 mg/L (normal range 0-3 mg/L), erythrocyte sedimentation rate (ESR): 103 mm/h (normal range 0-15% mm/h) (Figure 1). Three days after vancomycin treatment, the pain was unremitting and the HS-CRP and ESR were still higher then normal. Procedure under ultrasound guidance. The patient was placed in a right lateral position and a low-frequency linear ultrasound transducer was placed in a longitudinal orientation lateral to the L4-S1 spinous process. Incisional effusion was identified. A tuohy needle was used to tap 15 ml of dark brown fluid. Post-procedural Course. This woman was treated vancomycin 4 days after the procedure, and experienced immediate improvement in her low-back pain. Fifteen days later, she was discharged home.
Figure 1: The trend chart of laboratory tests which were related to infections of the first case during perioperative period.
Case 2
History and Examination. A 49-year-old man was referred to the hospital with a 2-year history of low-back pain and a 4-month history of lower limb weakness. An MRI study founded that he had the thickening of ligamentum flavum (TLF) in the L4-L5 and thoracic spinal cord compression. Operation: This patient was performed posterior spinal L4- L5 total laminectomy and pedicle screw fixation. Six days after the operation, he had tenderness to palpation and drainage at the surgical site. Laboratory tests: WBC: 16.5 10^9/L, NE%: 82.7%, HSCRP: 5.18 mg/L, ESR: 13 mm/h (Figure 2). First procedure under ultrasound guidance. Similar to the procedure in the first patient, 80 ml of pink fluid was tapped from superficial plane to the erector spine muscle (ESM) under the ultrasound guided. After 10min, the patient reported that his pain had diminished significantly. Second procedure under ultrasound guidance. His pain aggravated gradually in a week. Laboratory tests showed that WBC and NE%have dropped off, but HS-CRP and ESR have gone up. A large amount of effusion in the surgery site was confirmed again by ultrasound. We drained 100 ml of pink fluid this time. The antibiotic changed from ceftriaxone to vancomycin. Third procedure under ultrasound guidance. Four days later, this man told that his pain had alleviated. The visualized effusion decreased and only 40 ml of pink fluid was tapped. Post-procedural Course. Eighteen days after the third procedure there was no sign of infection, and the pain was resolved. Then the man was discharged home.
Figure 2: The trend chart of laboratory tests which were related to infections of the second case during perioperative period.
Case 3
History and Operation. A 72-year-old man, complained of severe low-back pain that radiated to his right feet. He was performed posterior spinal L4–L5 total laminectomy and pedicle screw fixation. A week after the operation, he was racked by high fever (40.1℃), chills and pain at the surgical site. Laboratory tests: WBC: 3.5 10^9/L, NE%: 79.7%, HS-CRP: 112.63 mg/L, ESR: 97 mm/h, PCT: 27.88 ng/ml (Figure 3). During the four days, although sulperazone and amikacin was used, the infection had maintained. First procedure under ultrasound guidance. Similar to the above-mentioned procedure, ultrasound was used to guide access to the area lateral to the lumbar spinous process and 30 ml of pink fluid was drained (Figure 4). Second procedure under ultrasound guidance. His temperature decreased to normal, but the pain continued. Laboratory tests: WBC: 7.2 10^9/L, NE%: 70.3%, HS-CRP: 50.97 mg/L, ESR: 45 mm/h, PCT: 2.03 ng/ml (Figure 3). Ultrasonography study was used to determined the effusion, and 30 ml of dark brown fluid was drained (Figure 5). Post-procedural Course. The day after the procedure, the patient experienced immediate improvement in his pain. He was discharged home 7 days after the second aspiration and at his follow- up evaluation nearly 1 month later had continued resolution of his symptoms (Figure 6).
Figure 3: The trend chart of laboratory tests which were related to infections of the third case during perioperative period.
Figure 4: Ultrasound image of aspiration in the level of L4-L5. Arrowheads indicate the tip of needle. ESM: erector spine muscle.
Figure 5: Dark brown fluid was drained under ultrasound guidance.
Figure 6: MRI studies. A. Preoperative MIR graph of the patient’s spine showing L4-L5 intervertebral disc bulges around and the compression of dura mater. B. Image at the level of L4–L5 showing that a signal of mixed before the first procedure. C. Before the second procedure graph showing the area of signal mixed changed large. D. Image of the patient’s follow-up evaluation nearly 1 month after the discharge showing that the mixed signal area had disappeared.
Discussion
Spinal operation is commonly used in the therapy for spinal disease. Post-operative surgical site infection is a dreadful complication with reported rates ranging from 0.7–20% [1-5]. At present, there are many modalities being used for therapy including antibiotic, vacuum sealing drainage (VSD), instrumentation removal, debridement and continuous irrigation and suction [11- 14]. There remains no consensus on indications for maintenance of the stabilization devices versus removal. These devices are often removed to facilitate infection control for the bacteria associated with these infections form biofilms attached to the internal fixator. However, reoperation means higher costs, more pain and longer hospital stay. Studies showed that significant loss of correction in deformity patients after instrumentation removal, even if stable fusion was observed. In our report described here, after undergoing posterior spinal surgery three patients developed SSI. By aspirating incisional effusion with ultrasound-guidance and retaining stabilization devices, their symptoms, the risk of spinal instability and neurological risks decreased, resulting in increased quality of life. It is widely agreed that deep infection should be managed with aspiration drains pus, and necrotic tissues that can hinder the antiinfective function of para-spinal muscle and granulation tissues. Vacuum sealing drainage (VSD) is a negative-pressure technique, which can achieve safe and rapid healing of soft wounds and infections. However, these patients [13,14] required wound opening during the VSD treatment and a second surgery to close the wound, which increased patient discomfort and the expense, limited patient activity, and required advanced medical facilities. Comparing to VSD, ultrasound-guided aspiration has more advantage including small trauma, less pain, economical and convenient. In our institution we operated 1258 patients of degenerative disc diseases from June 2015–February 2018. There were 1040 patients of posterior spinal surgery. Of these 1040 discs, 115 cases (1.1%) suffered the surgical site infection. Some cases with less severe infection and few effusion could be treated with several weeks of antibiotics. Ultrasound-guided aspirating incisional effusion was performed in those patients whose infection has progressed on MRI despite appropriate antibiotic therapy. Twenty cases undergone this procedure, which all of them have received satisfactory effect. For other cases with severe infection including suppurative spondylitis and septicaemia, aspiration alone cannot completely eliminate bacteria and suggests that surgery was an effective option. For these cases, ultrasound-guided aspiration could help to identify the effusion and correctly choose and use antibiotics.
Conclusion
Based on our small experience with postoperative surgical site infection after spine surgery, we recommended an ultrasonography study to determine the effusion, to determine the infection, to determine causative organisms, to choose correct antibiotic and to aspirate effusion.
Times for Peaks of Stress in Quadriceps Muscles During the Force-Velocity Test
Introduction
Among the intermittent tests with increasing loads, there is the Force-Velocity test (FVt) which consists of successive sprints of few seconds separated by recovery periods of a few minutes on an ergo cycle as Monark ergo cycle [1] against increasing braking loads. These authors found the increases of the mechanical power with the increase in the braking loads up to a maximal Power Output (POmax) despite the decrease in the pedaling speed, then its decrease despite the increase in the braking loads. The evolution in surface Electromyogram (EMG) power spectral and the Power Output (PO) concomitant with the increased in braking loads during the FVt were reported [2]. They showed an increase in EMG from the start of FVt to the peak load (Lpic), and then its decrease at the Lpic +1 kg. Thus, during the FVt, the muscle fatigue started after Lpic. Rouffet & Hautier (2008) found the root-mean-square (RMS) of EMG of Vastus Lateralis (VL) and Rectus Femoris (RF) muscles during the Isometric Maximal Voluntary Contractions (IMVC) and torque–velocity bicycling tests (T-V) increased from zero to approximately before 4 seconds during T-V and after 5 seconds during IMVC. Their results agreed those of Vandewalle (1987) who suggested the participants to reach the peak of pedaling speed before the end of the sprint (6 seconds). Due to these variations of the time to reach the maximum peak of EMG during intense exercise [3], the other question was to localize the time of muscle fatigue during each sprint of the FVt. For that, the aim of this study was to examine the EMG evolution of RF, VL, and VM of the quadriceps superficial muscles during the FVt to localize the peak of each EMG signal during the six seconds of each sprint.
Methods
Study Design
The approach was to determine the time to attack the peak of the EMG signal during each sprint of the FVt and, to examine if this time depends to the load and to the muscle. So, EMG signal were collected during each sprint in three quadriceps superficial muscles. In order to have good results during the FVt, only athletes suitable for intense and repetitive exercises such as soccer players were selected during maximum exercise tests.
Participants
Eighteen soccer players (age, 25 ± 4 years; height, 181 ± 3 cm, and weight, 77 ± 7 kg) participated in two tests each: a maximum test to determine their physical fitness and a FVt to examine the evolution of RMS and PMF for EMG in RF, VL, and VM at each sprint. Each participant was informed to refrain from doing intense exercise at least two days before the maximal exercise test or FVt. Both tests were performed at ~20°C between 3 and 6 p.m. in a laboratory. All participants were informed of the experimental procedures complying with the ethical standards of Helsinki Declaration as revised in 1989, before giving written their consent to the adhesion of the study.
Procedure
The maximal exercise test allowed the assessment of the maximal heart rate (HRmax), maximal power output (POmax), and maximal oxygen uptake (VO2max). The protocol consisted of 2 min cycling against a workload of 1 kg at 60 rev·min–1 on the ergometer (824 Monark-Crescent, AB, Varberg, Sweden) as a warm-up, then the load was increased every 1 min until volitional exhaustion by 0.5 kg. The following criteria: a) Inability of the participants to maintain the frequency at 60 rev·min-1 in spite of verbal encouragement, b) Attainment of age-predicted HRmax, and c) Respiratory exchange ratio greater than 1.10 were used to well achieve maximum performance. The results allowed selecting participants having physical capacity to complete a test in spite of the increase the intensity as the FVt. HR monitor (Polar Accurex Plus, Polar Electro, Kemple, Finland) was used for continuously record. An open circuit technique with the CPX system (Medical Graphics Corporation, St. Paul, Minn., USA.) permitted the measures of the oxygen consumption. Each participant completed the FVt at least three days after the maximal exercise test on the 824 Monark-Crescent. The FVt consisted of performing a maximal sprint against each load in a sitting position for 6 seconds, the maximal time for a participant to attain his maximal velocity after the starting signal. The accuracy of the frequency measurement was ± 3.3 ms. The feet were fixed to the pedals with the toe clips. Each participant started the first sprint of FVt against a load of 2 kg and then recovered for 5 min before repeating the 2nd sprint against the load increased by 2 kg. When the velocity was under 130 rev·min-1, the load was increased by only 1 kg for each sprint to attain more precise the peak load (Lpic) for the peak power output (POpic). We assumed that the participant attained the POpic if an additional + 1 kg (Lpic + 1kg) to the Lpic induced a PO decrease. An automatic system was used to determine the peak velocity (Vpic) for each load and to calculate the PO as the product of load and Vpic (F×Vpic). Surface EMG evolution of VM, RF, and VL were examined during the FVt for each participant. The EMG signals were collected by Beckman bipolar surface electrodes (9 mm diameter, physiosystems, Noisy-le-Grand), spaced by 20 mm distance, placed over the centre of the belly of each muscle of the right leg of each participant. The ground electrode was placed at the right wrist. EMG signals were conditioned and stored on magnetic tape (TEAC R-71, TEAC Corp., Tokyo, Japan), after differential amplification with bandwidth ranging from 2 Hz to 2 kHz along with the output signal from the dynamometer. EMG signals were sampled by a spectrum analyser (model 3582A, Hewlett-Packard, Les Ulis) at 1024 Hz. Power Spectral Density (PSD) of surface EMG was calculated from 0.5-s time intervals and was defined by 256 points in amplitude and phase in the 2−514 Hz bandwidth. Each PSD was then computed and divided into 10 bands, the bandwidth being 24 Hz, except for the highest band (56 Hz). EMG signals were analysed using acquisition and spectrum analyzer software (Spatol, Divergent, Compiègne, France) and a data-computing software (Calvise, Divergent, Compiègne, France). Calvise software permitted the transformation of PSD into four parameters, among which were the RMS and the mean power frequency (MPF) [4]. For each participant, the RMS and the MPF were determined for RF, VL, and VM at each sprint in real-time during 6 seconds by the computer. HR was collected continuously with the same monitor using during the maximal exercise test. The mean value of five rest minutes and the higher values after each sprint were conserved for analysis. For each participant, his blood was collected using microcapillary tubes at rest (r0) and at three minutes after each sprint by micro puncture at the fingertips, then the lactate (La) concentration was analyzed at the end of the FVt using a Mini photometer Plus LP 20 (Monitor-8, Anglet-France). The skin temperature (sT) was measured at many periods: r0, three minutes after each sprint. The single probe thermometer TH-5 (Physitemp Instruments, Inc., Clifton, NJ, USA) was applied to the RF to measure the sT. Three successive measures of the sT were realised at each period and the largest value was retained. For each sprint, the sT of RF was considered as the quadriceps muscle sT for each participant.
Statistical Analyses
StatView software (Abacus Concepts, Berkeley, California, USA) was used for all analysis and the results were presented as mean ± standard deviation for POmax, HRmaxth, HRmax, VO2max, and sT during maximal exercise test, then for PO, HR, La, and sT at each braking load during the FVt. Anova one-way analysis of variance with repeated measures was used to illustrate the kinetics of absolutes RMS and MPF data in arbitrary unit (a.u.) obtained at each second during the 6 seconds of each sprint. Then, RMS and MPF were illustrated in curve for each sprint for all participants in real time. The curves of RF, VL, and VM were then compared to determine the degree of the participation of each quadriceps superficial muscles during the FVt.
Results
The mean theoretical maximum heart rate (HRmaxth) was 194 ± 3 bpm. The Maximal aerobic power (POmax = 265±33 w), maximal oxygen uptake (VO2max = 45.8 ± 2.3 mL/min/kg), and maximal heart rate (HRmax = 181 ± 6 bpm), respiratory ratio (1.14 ± 0.02), and skin temperature (sT = 34.6 ± 0.6 °C) were obtained during the maximal incremental exercise test. Table 1 showed the Heart Rate (HR), lactate (La), skin Temperature (sT), and Power Output (PO). The values of the four parameters increased simultaneously with the increase of the load. The peak of sT were attained with the attack of the peak of PO (POpic) at the peak load (Lpic = 8.7 kg). The values of sT decreased at Lpic+1kg like that of the PO. In contrast, after the Lpic, the value of the HR and that of La continued to increase despite the decrease of the PO at the Lpic + 1 kg (9.7 kg). During the FVt, the RMS and PMF increased with the increase of load until Lpic and decreased with Lpic+1kg (Figure 1). At each sprint of the FVt, the curves of RMS and MPF of RF, VL, and VM increased quickly from zero about 4th second, then remained stable or decreased until 6th second. The RMS curves of RF and VL evolved similar from the start to the end of each sprint and were larger than those of VM. In contract, the MPF curves of RF and VL evolved similar from the start to the end of each sprint and were lower than those of VM.
Table 1: Physiological responses during Force velocity test.
Note: HR: Heart Rate, La: Lactate, sT: skin Temperature, and PO: Power Output
Figure 1. Quadriceps suvitroperficial muscles RMS and MPF evolution at each sprint during the FVt.
Note: RA: rectus femoris, VL: vastus lateralis, VM: vastus medialis, RMS: root-mean-square, and MPF: mean power frequency.
Discussion
The main result of this study was a rapid increase of EMG signals of the three superficial muscles of the quadriceps from the start of each sprint until 4-5 seconds, then a tendency to form a plateau or a decline until the end of the 6th second. This increase of EMG signals could inform on the muscle activity illustrated by RMS which was greater for the RF and VL muscles than for the VM muscle at all sprints. On the other hand, these increases in the activities of the three muscles became more significant with the increase in loads until the peak power reached at the load peak (Lpic). Then a slight drop in the activities of the three muscles was observed with Lpic + 1kg. Muscle fatigue was illustrated by smaller increases in the MFP of RF and VL muscles compared to that of VM whose intervention in FVt was late regardless of the braking load. The participants of this study had anthropometric characteristics similar to those of league (1 and 2) or national soccer players [4-6]. The average age of the participants in this study was similar to that of European soccer players (25 years) and lower than that of 2018 World Cup soccer players (27.4 years). As for the anthropometric parameters, the participants of this study had an average size and an average weight similar to those of the 2018 World Cup soccer players (181.7 cm and 77 kg). The physiological conditions (POmax, HRmaxth, VO2max, and HRmax) of the participants of this study recalled their level of physical activity as sedentary. The participants in the present study had a lower HRmax than their own HRmaxth. Their POmax and VO2max were lower than those of professional and even amateur soccer players [6-9]. This study just needed adult’s participants able to participate in a rough test on an ergocycle (the forcevelocity test) to avoid as much as possible, cases of accident [10] linked to poor physical condition during this kind of exercise. The increase in PO from 363 ± 25 to 979 ± 99 w (POpic), then its fall to 926 + 90 w on average had shown a change in the gallows of this physical parameter (POpic) of the FVt test. Similar evolutions of HR and EMG signals concomitant with that of PO have shown a close relationship between physical and physiological parameters during FVt [11-14]. The POpic obtained by sedentary participants in this study was considerable if we compare it to those reported by Vadewalle (1987). These authors had obtained 1221 ± 192 w in 26 ± 6 year old rugby attackers, 1021 ± 152 w in 26 ± 3 year old soccer players and 813 ± 137 w in 29 ± 5 year old recreational players. The successive evolutions of HR, lactate and sT associated with those of PO could also be considered. However, if the HR and the La had evolved in the form of a gallop from 2kg to Lpic+1kg with the PO, the sT had increased until the end of FVt. It had gone from 31.4 + 1.3 at the rest to 34.1 + 0.8 ° C at the end of FVt. These results showed that the sT evolved in a linear fashion with the increase in braking force during this kind of exercise and not as a function of mechanical power like HR or lactate. At all sprints, the evolution of the RMS and MPF of RF, VL or and VM during pedaling presented in Figure 1 showed the level of participation of these three superficial quadriceps muscle. The EMG signals of these muscles were previously illustrated. The significant increase in RMS for RF and VL compared to that of VM showed a strong participation of RF and VL compared to that of VM during each sprint. The decrease in RMS of RF, VL and VM after 4-5 seconds during each sprint could illustrate muscle fatigue. This suggests that a muscle gets fatigue just after a few seconds (4-5 seconds) when it is used at a very high speed regardless of resistance. This muscular fatigue was well illustrated with the presentation of the MPF of RF, VL and VM. Fatigue was much greater for RF and VL than for VM. The MPF of VM was higher above those of RF and VL for all sprints. This result agreed that of Camata (2011). These authors found the RF more stressed earlier and tired more quickly than VL and VM. However, the increase in RMS of RF, VL and VM with that of load from 2 kg to Lpic despite the decrease of speed could show the dominant effect of force on speed during cycling. Also, the significant increase in the MPF (illustrating the fatigue level) of RF and VL compared to that of VM with the increase in the load could show more the influence of the force on the speed during the FVt. These simultaneous increases in RMS, MPF, HR, and La with that in PO agreed with the study of Temfemo (2011).
Acknowledgement
The authors thank all the participants and the members of the Physiology and Medicine of Physical Activity and Sports (UPM-APS) of the University of Douala for their collaboration.
Clinical and Laboratory Features of Primary Sjögren’s Syndrome Complicated with Mild to Severe Thrombocytopenia
Introduction
Sjögren’s syndrome (SS; also known as Sicca syndrome) is a chronic systemic autoimmune disease characterized by xerophthalmia (dry eyes) and/or xerostomia (dry mouth). In addition to the impaired function of exocrine glands, other organs may be also involved, such as the skin, joints, lungs, liver, kidneys, and hematological system. Hematological system involvement is common in SS patients, and a third of patients with SS have cytopenias such as leukopenia, anemia, and thrombocytopenia [1]. In primary SS (pSS), one of the most common complications of the hematological system is leukopenia, while a few cases were complicated with autoimmune hemolytic anemia and thrombocytopenia [2]. A study analyzed 99 pSS patients and reported that 61 (61.5 %) developed lymphopenia and leukopenia and 7 (7.1%) had thrombocytopenia [3]. Although thrombocytopenia is not common in pSS patients [4], severe thrombocytopenia can increase the occurrence of adverse events, which are sometimes fatal. Some patients were misdiagnosed because they lack the typical signs in their eyes and mouths [5]. Thus, in 2015, the European League Against Rheumatism (EULAR) has promoted and supported an international collaborative study group (EULAR-SS Task Force) aimed at developing consensual recommendations to provide a homogeneous approach to pSS patients presenting with systemic involvement. The guideline mentioned that patients with thrombocytopenia accompanied with positive Ro/SS-A and/or La/SS-B autoantibodies have possible diagnosis of SS [6]. Because of its low prevalence, large-sample controlled studies on thrombocytopenia in pSS are scarce. Thus, in this study, we aimed to investigate the clinical and laboratory characteristics of pSS complicated with mild to severe thrombocytopenia and compared them with those of pSS patients without thrombocytopenia.
Methods
Design
In this medical records review study, we identified 841pSS patients hospitalized in the Department of Rheumatology of the First Affiliated Hospital of Soochow University between March 2007 and March 2018. Of these pSS patients, 43 developed mild to severe thrombocytopenia (thrombocytopenia group), and 45 patients who did not developed thrombocytopenia were included in the analysis as the control group. The age and sex of the control group were matched to those of the thrombocytopenia group. Patients’ demographic data, clinical manifestations, laboratory examinations, and other results were analyzed retrospectively.
Patients
PSS diagnosis was confirmed either by pathological or clinical method based on the 2002 American College of Rheumatology Classification Criteria [7]. Patients with other diseases such as chronic hepatitis C, human immunodeficiency virus infection, previous lymphoproliferative processes, or other autoimmune diseases were excluded. The study was approved by the Institutional Ethics Board of Medical College, Soochow University (No. 2018- 012).
Clinical Features
The clinical characteristics of pSS are as follows: fever, axillary temperature >37.5℃; Raynaud phenomenon, cool skin and cutaneous color changes of the fingers and toes exposed to cold and/or stress; articular feature, arthralgia or non-erosive arthritis involving two or more peripheral joints; pulmonary complications, chronic and persistent cough, dyspnea, or both, with alveolitis or fibrosis in computed tomography (CT) scans; nephropathy, permanent proteinuria (>0.5 g/day), continuously increasing serum creatinine level (>111 μmol/L), renal tubular acidosis, or glomerular nephritis; liver damage, altered plasma liver function (aminotransferase, alkaline phosphatase, gamma glutamyl transferase, and bilirubin) and/or altered bile ducts in ultrasonography, CT, or magnetic resonance imaging; hemorrhagic manifestations, skin bleeding (skin purpura or bruises), oral bleeding (oral blood blister or gingival bleeding), nasal hemorrhage, gastrointestinal bleeding (visible bleeding or fecal occult blood), urinary bleeding (urinating blood or microscopic hematuria), vaginal bleeding (massive bleeding or prolonged menstrual period), conjunctival bleeding, and intracerebral hemorrhage. Bleeding seriousness was assessed using the immune thrombocytopenic purpura (ITP) bleeding scoring system [8].
Laboratory Features
The laboratory features were as follows: mild to severe thrombocytopenia manifested by platelet count <50×109/L, leukopenia as leucocyte count <4.0×109/L, anemia as hemoglobin <120 g/L, and hypocomplementemia with complement C3 <0.79 g/L and/or complement C4 <0.16 g/L. Rheumatoid factor (RF) (latex test positive at a value >20 IU/mL) was analyzed by enzymelinked immunosorbent assay. Antinuclear antibodies (ANAs; positive at a titer 1:100 by indirect immunofluorescence) and 60- kDa and 52-kDa forms of anti-Ro/SSA and anti-La/SSB antibodies were tested independently.
Statistical Analysis
SPSS software version 21.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Continuous variables were compared using the Wilcoxon test, and proportions were analyzed using chisquare and Fisher’s exact test. A value of p<0.05 indicated statistical significance.
Results
Patient Characteristics
In this study, the total incidence rate of mild to severe thrombocytopenia in pSS patients was 5.1%. Among 43 patients with mild to severe thrombocytopenia, only 3 (6.9%) were men. pSS patients with mild to severe thrombocytopenia were 17–70 years old, with a mean age of 51.69±12.43 years, while control patients were 41.46 ± 14.89 years old. The median disease duration in the thrombocytopenia group was 18 months versus 44 months in the control group (Table 1).
Table 1: Characteristics of pSS patients with or without mild to severe thrombocytopenia.
Note: *p<0.05; **p<0.01
Clinical Features in pSS Patients with Mild to Severe Thrombocytopenia
Table 2 presents the clinical features of the patients in the thrombocytopenia group. The classic manifestations of SS, such as dryness of the mouth and eyes, rampant caries, and other clinical features like fatigue, fever, and weight loss were observed. The incidence rates of xerostomia and xerophthalmia were significantly lower in the thrombocytopenia group than in the control group (P = .0028, and P = .0024, respectively). Of the 43 patients in the thrombocytopenia group, 17 sought admission because of thrombocytopenia and/or hemorrhagic manifestations, without exocrine gland features. While pulmonary interstitial disorders were more common in the control group (P = .0088). The frequency of fever, rashes, arthritis, and Raynaud phenomenon did not show statistically significant difference between the two groups. As expected, the thrombocytopenia group had significantly higher EULAR Sjögren’s syndrome disease activity index than the control group (ESSDAI scores) (P < .001).
Table 2: Clinical features in pSS patients with or without mild to severe thrombocytopenia.
Note: *p<0.05; **p<0.01
Difference in Serologic Features
Not surprisingly, the platelet count in the thrombocytopenia group was significantly lower than that in the control group (P < .001). The thrombocytopenia group had significant hypocomplementemia (C4 level) than the control group (P = .0024). However, the existence of ANA, anti-SSA 60-kDa and 52- kDa, anti-SSB, M2, anti-dsDNA, and anticentromere antibodies (ACAs) was not obviously different between the two groups (Table 3). Levels of erythrocyte sedimentation rate, C-reactive protein, and RF were not markedly different between the two groups. The levels of immunoglobulin A (IgA) were significantly lower in the thrombocytopenia group than in the control group (P = .0019); however, no difference was found in the levels of IgG and IgM between the two groups. Among the regular chemical parameters, the level of glutamic-pyruvic transaminase (alanine transaminase) were significantly increased in the thrombocytopenia group (P = .043) (Table 4).
Table 3: Serologic features in pSS patients with or without mild to severe thrombocytopenia.
Note: *p<0.05; **p<0.01
Table 4: Serologic features in pSS patients with or without mild to severe thrombocytopenia.
Note: *p<0.05; **p<0.01
Disease and Prognosis in pSS Patients with Mild to Severe Thrombocytopenia
In the thrombocytopenia group, the most common hemorrhagic manifestations were skin bleeding, such as purpura/bruises (21 of 43, 48.8%), and gingival bleeding (17 of 43, 39.5%). There were no hemorrhagic manifestations in 14 of 43 patients (32.6%) (Table 4). At baseline, the ITP bleeding score was 1.32±1.17, and no correlation was found between hemorrhagic manifestations and treatment effect (Table 5). No patient died during the study period. Mild to severe thrombocytopenia was treated with highdose corticosteroids and/or intravenous gamma-immunoglobulin, and hydroxychloroquine and cyclosporine were also used. During hospitalization, among 43 patients, 35 were responsive and 8 were not responsive to the treatment. One patient had undergone splenectomy because of refractory thrombocytopenia.
Table 5: Characteristics of pSS patients with mild to severe thrombocytopenia.
Discussion
To the best of our knowledge, this is the first study to show a negative relation between mild to severe thrombocytopenia and lung involvement in pSS. pSS is one of the major chronic inflammatory autoimmune diseases associated with B lymphocyte hyper-reactivity. Recently, the reported prevalence of pSS ranges from 0.05% to 0.23% [9,10], and in China, it is approximately 0.33% to 0.77% [11]. Although most patients have exocrine gland involvement, such as labial gland and lacrimal gland involvement [12], their clinical manifestation is usually quite nonspecific and varied, resulting in the delay in the diagnosis for 3-8 years from the onset of first symptoms [13,14]. In our study, all 88 patients had pathological examination of lower lip biopsy. Among pSS patients with mild to severe thrombocytopenia, 4 had no lymphocytic foci, but in pSS patients without thrombocytopenia, 1 had no lymphocytic foci. Thrombocytopenia is not common in pSS patients. In our study, 5.1% of the pSS patients developed mild to severe thrombocytopenia; among them, 95.3% were female. Moreover, our participants were inpatients, making our cohort similar to those in other studies. Studies reported that 5%-16% of pSS patients developed thrombocytopenia [15,11,16]. Although there was no real distinction in the median time for diagnosis confirmation between patients with or without mild to severe thrombocytopenia, pSS patients with mild to severe thrombocytopenia obviously had higher ESSDAI scores than those without, and they needed longer hospitalization. Leukopenia is the most frequent hematologic abnormality noted in pSS, and 30%-40% of pSS patients may have leukopenia [2]. In our study, 29.5% of the patients have leukopenia, but among patients with mild to severe thrombocytopenia, the prevalence of leukopenia was significantly lower than in those without thrombocytopenia. All patients responded remarkably well to corticosteroids. Antineutrophil antibody may be responsible for autoimmune neutropenia [17], but the low frequency of neutropenia in pSS patients with mild to severe thrombocytopenia was not reported in previous studies; thus, further research is required. In our study, decreased levels of C4 and IgA were more common in the thrombocytopenia group, indicating the possible important complex immune mechanism in the pathogenesis of thrombocytopenia in pSS patients. A large proportion of patients in both groups were positive for ANA. The prevalence of all autoantibodies such as anti-SSA and anti-SSB, AIM-M2, CENPB, ACA, anti-dsDNA, and U1RNP showed no remarkable difference between the two groups. For some antibodies, the absence of a significant difference may have resulted from a relatively small sample size. There was lung involvement in 10%-20% of pSS patients [18]. Among 88 patients, 21.6% had lung involvement, which fairly accorded with the results in previous studies [19]. However, in pSS patients with mild to severe thrombocytopenia, the incidence of lung involvement reduced markedly in our study. Platelet-derived growth factor was reported to contribute directly to the migration of fibrocytes to the injured lungs [20]. Current understanding of the pathophysiology of lung disease in pSS suggests a similar process as those in the salivary glands, with epithelial cells playing a critical role in the initiation [19]. It can be assumed that pSS with lung involvement and pSS with hematological involvement have different pathological and clinical manifestations. However, this study has limitations that hindered the generalization of the results: small sample size, retrospective design, single-center setting, etc. More research is needed on the relationship between thrombocytopenia and lung involvement in pSS.
Conclusion
our study explored the clinical features of pSS accompanied with mild to severe thrombocytopenia. pSS patients with mild to severe thrombocytopenia could have higher ESSDAI scores than those without thrombocytopenia, but the incidence of some complications such as leukopenia and lung involvement was low. In pSS patients with mild to severe thrombocytopenia, the incidence of xerostomia, xerophthalmia, and lung involvement reduced markedly. Thrombocytopenia could be present upon the onset of pSS development, without any involvement of the exocrine glands. Thus, there is an urgent need for more detailed classification of pSS based on its clinical manifestations and pathology. Knowledge on the features of pSS associated with thrombocytopenia will help in early and better diagnosis and treatment.
Acknowledgement
We would like to thank Editage (www.editage.cn) for English language editing.
Telemedicine and Metabolic Diseases in Practice – Weight Predictor Localized for the Czech Population
Telemedicine has been gaining in importance recently. The term telemedicine is derived from two Greek words – tele (“distance”) and medicine (meden = treatment “). According to the European Commission, it is defined as:” Rapid access to shared and remote medical expertise through telecommunications and information technology, regardless of where the patient or relevant information is located. Sometimes the term “telehealth” is used instead of telemedicine [1]. The history of modern telemedicine dates back to the invention of the traditional telephone in the 19th century. At that time, physicians could give information and medical advice by phone. In simple terms, telemedicine can be defined as a supportive medical service using telecommunication technologies [2]. The concept of telemedicine has become established in medical terminology at the instigation of the WHO (World Heat Organization). Another term used for telemedicine is “distance medicine”. However, there are differences in definition within individual fields of telemedicine. The view of individual specializations in telemedicine is inconsistent and may vary. In general, however, the goals of telemedicine can be characterized as follows: to speed up and improve communication between doctors, between doctor and patient, to use modern communication tools and effective information transfer, to improve overall patient care and to improve diagnostic and therapeutic processes [1]. Telemedicine is defined by the WHO as a general term for health activities, services and systems operated remotely through information and communication technologies to promote global health, prevention and health care, as well as education, health care and medical research. The general definition of telemedicine is the provision of medical services at a distance, and this term covers a wide range of different applications. There are two basic areas. First, applications that allow real-time monitoring of the patient, eg. in the form of video calls, online transmission of heart rate data, etc. Second, applications that work asynchronously, eg. by storing physiological data (weight, blood pressure, blood glucose, heart rate records from exercise units, etc.) from home monitoring and their subsequent transfer to the database in the medical facility or reconditioning center [3].
The main goal of telemedicine is to provide medical services remotely. Reducing the need for clinical visits is one of the many benefits that telemedicine brings to patients and offers them obvious convenience. Thanks to the use of IT technologies, the patient can receive basic medical care at home. By evaluating the level of medical support provided over the last two to three decades, IT technologies have undoubtedly provided huge benefits to the general public. More powerful, faster computers, and more efficient use of features have allowed more types of services to be extended to more users. For example, several decades ago, a simple request for medical help could only be obtained by searching for a landline at the clinic where the doctor was present. Thanks to the availability of “Voice over Internet Protocol” (VoIP) mobile technology, you can easily pick up your mobile phone and make a video call with your doctor, ie. the doctor providing the consultation does not necessarily have to be present at the clinic. This is just one of many examples where advances in IT technology have contributed to more affordable healthcare [2]. Thanks to the rapid development of technology, telemedicine is currently gaining more and more space and use across medical specializations. In addition, it enables the so-called remote monitoring of the patient, or the data collection from the patient and their subsequent control with professional recommendations with regard to the patient’s goals. It is potentially widely used, for example, in diabetology, where it uses subcutaneous sensors in patients with DM, which read the patient’s blood glucose level, store data and send it to the physician via a mobile phone connected to the sensor. The physician can evaluate the data and provide feedback to the patient.
The use of telemedicine has common elements in various medical fields. Remote clinical care helps remove barriers and improves access to health services. It is therefore a benefit in urgent and intensive care as well as in the care of chronic patients. Regardless of the medical field in which telemedicine is used, its basic areas of activity can be divided into four categories [1]: 1) Information transfer 2) Remote monitoring 3) Distance therapy 4) Telemedicine education Telemedicine communication can be further divided into: 1) Voice: The simplest telemedicine service using an analog or digital telephone network. These are, for example, helplines, security lines, consulting and advisory lines. 2) Visual: This includes various imaging methods – teleradiology, CT, MRI, angiography, etc., but also, for example, video conferencing. 3) Data: Data exchange, telemetry, access to databases. It takes place mainly using the Internet and the TCP / IP family of protocols. Includes telemetry – remote monitoring of physiological functions.
Telemedicine in the Treatment of Obesity
Obesity is one of the civilization diseases, which, together with type 2 diabetes mellitus, has been growing since the 1940s, although it seems to be peaking and the increase is no longer so great. However, according to the latest actual data from 2013, approximately 23% of the adult population is obese and another 34% are overweight. Thus, a total of 57% of the adult population struggles with overweight and obesity (Figure 1) [4]. Obese people are 6 times more likely to get type 2 diabetes. If they exercise regularly, only 3.5 times more often. The development of obesity is undoubtedly due to a decrease in physical activity, and although the increase from 2010 to 2013 appears to have virtually stopped, the time spent on physical activity is still shortening [4]. The only result is a logical decrease in physical ability, which is a key prognostic factor in cardiovascular mortality, especially in old age. The main problem of effective treatment is to obtain quality data and this is the use of telemedicine. Questionnaires, whether related to physical activity or frequency questionnaires, appear to have too large deviations from actual energy intake or expenditure. Although there is no doubt that in a large amount of data, they can provide relatively accurate information about diet and physical activity with quality processing. The validity of the questionnaires on physical activity and their use for epidemiological research has been repeatedly confirmed [5]. However, the individual deviations tend to be large and the recommendations based on the questionnaire survey are not effective.
Figure 1: Incidence of obesity in the Czech Republic 2001-2013.
It is not entirely possible to individually calculate the energy value or the proportion of individual components of food in the diet by doctors or nutritional therapists. Various applications are used for this purpose, the quality of applications is often determined by the database that is formed at the time of its creation, but above all by regular updates, which are often greatly underestimated. It is often not even possible to use foreign food databases, because the composition of different foods with similar names is a wellknown problem that is currently being addressed at European Commission level. The specifics of various recipes can be gradually eliminated by entering your own recipes, which quality databases or applications should allow. However, accurate quantity data are much more important for evaluation. This is the only way to get approximately the right result. Immediate recording after a meal is very important. If we record in the evening, even the best applications or food databases will not help us and the error rate will be close to 40% [4].
Telemedicine procedures will be beneficial especially in the rural population, where there is no good availability of clinical specialists (nutrition therapists, psychologists, etc.). This is also proven by a study by Brown from South Carolina. She says that the key is the availability of care at greater distances for the possibility of regular visits, respectively. interventions. The study showed the same effect of weight reduction in clinical interventions during faceto- face visits as when using telemedicine (videoconferencing, etc.) in the rural population [6]. Similarly, another study demonstrates the effectiveness of smartphone engagement and increased physical activity compared to the control group [7]. There is no doubt about cost-effectiveness in the use of telemedicine, although we have not found a detailed study on this topic. Our unpublished data show that weight loss efficacy increases by approximately 15-20% when patients use online energy intake and expenditure monitoring. Adherence to the reduction regime is then about 5-6 months longer. According to [8] [9], there are a small number of long-term studies that show that wearables can improve the results of long-term physical activity and weight loss. However, there was insufficient evidence to show a greater benefit compared to the control groups.
Another randomized study [10] shows that the differences between the control group and the group monitored by smartphone were statistically insignificant. However, the remote monitoring group showed better compliance with the regime. The combination of mobile technology with occasional personal interventions appears to be one of the effective tools in the clinical treatment of obesity. Obesitology is a medical field in which the effective application of distance communication is possible. Self-monitoring, lifestyle change, diet and physical activity are absolutely essential in a reduction mode. Professional medical supervision is possible via information and telecommunication technologies, via the Internet or via smartphones. The advantage of the previous is the possibility of regular communication, whether synchronous or asynchronous. In this context, modern technologies have great potential to help fight obesity, especially in young patients. However, recent study results show that information technologies are not fully utilized in treatment. In the Czech Republic, where the research was conducted, it is not possible to look for barriers only on the part of the patient, because it is not quite common practice on the part of the doctor to use online communication and data sharing in this way. However, for physicians, continuous monitoring of patient outcomes can mean faster detection of patients’ health risks [11].
The advantages of telemedicine in obesitology include monitoring patients, reducing the time required for hospitalization, reducing waiting times for personal examinations, streamlining consultations and improving the overall quality of care provided [11,12]. As mentioned above, obesitology mainly uses patient selfmonitoring, in particular the control of dietary records, physical activity and other monitored data such as glycaemia, blood pressure, weight, etc. The main advantage of telemedicine is to support patient motivation and improve treatment cooperation, and not only in obese or overweight patients. In terrain we can use modern technologies such as pedometers, smart bracelets or watches, heart rate sensors, glucometers, blood pressure monitors, scales (more expensive scales can measure the bioimpedance method of body composition, i.e. the amount of fat, muscle, water in the body) that are connected to a mobile phone (usually via Bluetooth) or online questionnaire completion (nutritional or psychological). Eating habits are monitored online (web or mobile application) on a website with a large food database. The most used application in our country with the widest and regularly updated database is the portal http://www.kaloricketabulky.cz. The application is free and can be used both in web form and in a mobile phone or tablet as an application. To summarize the above, telemedicine has an important role in obesitology and its use consists mainly in (self) monitoring of patients and subsequent data processing, their evaluation and rapid feedback without the acute need for personal contact.
Materials and Methods
As part of improving patient care and simplifying cooperation with the patient in obesitology, the “Weight Predictor” portal for the Czech population is being developed. The main goal of this portal is, based on data obtained from the patient, to predict the development of his weight. The purpose of the predictor is to learn from quality data and on the basis of this data and to create a so-called artificial neural network that will be able to respond to changes in the “behavior” of the patient.
At the Moment, the Predictor has Completed the 1st Phase of Data Collection. The Following Data were Collected from Patients (Figure 2)
1) Energy Intake: Obtained from the applications caloricketabulky.cz, MyFitnessPal and Nutridata.cz 2) Energy Expenditure: Data obtained from smart devices Garmin (Figure 3), Fitbit or others connectable to Google Fit or Apple Health in a mobile phone 3) Questionnaires: a. Lifestyle questionnaire b. Psychological profile c. Lifetime history of weight d. Anamnestic questionnaire
Figure 2: Weight Predictor Data Collection Scheme (Energy intake using the online platform kaloricketabulky.cz, myfitnesspal. com or nutridata.cz. Most often used kaloricketabulky.cz. Energy expenditure – monitored habitual activity (steps) using bracelets with a pedometer via GoogleFit, Fitbit AppleHealth or Garmin. Furthermore, data were collected from questionnaires).
The Data Collection Methodology Included a Total of 6 Weeks of Patient Monitoring with thorough Control of Data Collection. The Data Collection Schedule was as follows
1) Filling in the form – control of the meeting the criteria for inclusion in the program 2) Boot regime a. Explanation of the program in details b. Setting up one of the monitoring systems for energy intake and output – see Figure 1. c. Body composition measurement d. Ordering a placement visit 3) Placement visit a. After 1-2 weeks from the first visit b. Thorough compliance check: i. Recording the weight, filling in the energy intake and expenditure (steps) ii. Weighing and measuring body composition iii. Completion of anamnestic questionnaire iv. Completion of a psychological questionnaire v. Record of lifelong weight development 4) Controls a. A personal visit with consultation and measurement of body composition each week b. 2 online control of data collection in a week c. Possibility of online consultation 5) Final Visit a. Weighing and measuring body composition b. Quality control of data and data sending c. In case of a successful regime, it was possible to extend to the second successor regime and possibly to the third
Results
A total of 1193 applicants were registered in the predictor, but unfortunately there was a very large decrease of applicants, so only 248 programs were successfully completed. An overview of data collection participants is shown in Tables 1A-1C and Figures 4A-4E. The biggest problems in data acquisition were mainly the technological barrier in the elderly population (70+) and also less interest in the male population. The best response was in the 40-50 age group in both sexes. From the above, however, it is clear that the obtained data will not be able to “train” the neural network. The “success” of completed programs is shown in Tables 2A & 2B. It can be seen from Table 2 that out of 1193 applicants, only 248 completed, which is less than 21% of all participants involved. In the beginning, most of the applicants were motivated, but over time, the decrease of probands was great. 203 participants did not complete the program due to time constraints, 386 did not fill in calorie tables or weight, 306 probands had insufficiently filled in data during data collection and therefore it was not possible to use the data. 53 probands did not complete due to health reasons. The biggest problems in data acquisition were mainly the technological barrier in the elderly population (70+) and also less interest in the male population. The best response was in the 40-50 age group in both sexes. From the above, however, it is clear that the obtained data will not be able to “train” the neural network. The “success” of completed programs is shown in Tables 2A & 2B. It can be seen from Table 2 that out of 1193 applicants, only 248 completed, which is less than 21% of all participants involved. In the beginning, most of the applicants were motivated, but over time, the decrease of probands was great. 203 participants did not complete the program due to time constraints, 386 did not fill in calorie tables or weight, 306 probands had insufficiently filled in data during data collection and therefore it was not possible to use the data. 53 probands did not complete due to health reasons. The calculated correction coefficients are shown in Tables 3A-3C, both for the whole set and even with the division into men and women. As can be seen in Table 3, the correction factor is on average comparable for both sexes and is around 5.5. Which is a relatively large number (Figures 5 & 6).
Table 1: Set of probands:
A. General overview of probands who completed the program and had sufficiently written or transferred data, B. Set of men, C. Set of women.
Table 2: Overview of completed programs
A. Percentage overview of completed programs, B. Absolute numbers of involved and completed programs according to age categories.
Table 3:
A. Total values of correction coefficients for a group of probands, B. Calculated correction coefficients for a set of men, C. Calculated correction coefficients for a set of women.
Figure 3: Garmin device for steps collection.
Figure 4: Box plots for: A. A age, B. Height, C. Weight, D. BMI, E. Waist circumference
Figure 5: Demonstration of the development of the real weight of a random proband (blue color) and predicted development according to the equation of dr. Hall (green color) in time.
Figure 6: Demonstration of the development of the real weight of a random proband (blue color), predicted development according to the prediction equation of dr. Hall (green color) and predicted scales with correction factor (orange) over time.
Discussion
Telemedicine certainly has a place in obesity and its importance will undoubtedly take on. In addition to monitoring applications and systems, we tried to create software for predicting the weight of Czech patients based on their eating and exercise habits. Based on the collected data, it was not possible to build a neural network that would learn from its data and be able to predict the development of the weight of the individual. The amount of data to create the model was not enough. We therefore used the dynamic-mathematical model of Dr. Hall [13] as a starting model for prediction. as a basis for calculating the prediction. Due to the development of this model on laboratory data, it could not be fully utilized for our purposes. The question is what is the cause of the big difference in the prediction of the used model and real data in our probands. Our probands collected data by self-collection and therefore the collected data could be distorted. No large variations were observed in mostly middle-aged women. There were variations in men’s diet, we called them “score lies.” A possible explanation is that men tend to underestimate portions (they are lazy to weigh). One possible explanation is that a “normal” portion entered in caloric tables does not normally satisfy a man, which is related to the previous one. When a man enters a regular portion in caloric tables, but does not weigh the food, he will increase his income (compared to caloric tables), because his normal portion according to caloric tables exceeds its caloric value. Given the above, we calculated and applied a correction factor to our data, which eliminated the deviations and after incorporating the correction factor, the model showed more significant results for our population [14].
To further refine the model, it would be necessary to test other parameters of the model such as output, content of elements and vitamins in the diet of the Czech population and it was appropriate to test the model on data where the diet remains the same throughout the measurement. The next step in the development of the model should also be the implementation of glycaemia and their influence on the development of body weight, which will be the result of our further work.
Funding
The study was supported by the Ministry of Health, Czech Republic, RVO-VFN 64165 and by the Charles University in Prague, project GA UK No. 316120 and Progres Q25.
Analysis of Latent Factors Underlying Conceptions of People with Dementia and the Effects of Social Resources
Against the backdrop of Japan’s fast-declining birth rate and growing-ageing population, support measures for people with dementia, estimated to be around 7 million in 2025, are drawing attention. In the Dementia Policy Promotion Outline promulgated by the Ministry of Health, Labour and Welfare in June 2019, ‘symbiosis’ is listed as a pillar, and ‘dissemination and enlightenment / personal dissemination support’ is listed as Factor 1 in the section on specific measures [1]. This can be interpreted as a message that we must deepen our understanding of dementia to ensure that people with dementia and their families can continue living in their own way in their communities. Globally, many OECD countries have designated the promotion of dementia awareness as a preeminent national strategy for supporting dementia. In the 2019 World Alzheimer Report released by the International Association for Alzheimer’s Disease, the need to reduce stigma for people with dementia was strongly emphasized, and 10 recommendations were proposed [2]. These recommendations include the creation of communities that are kind to people with dementia and to practice person-centred care. In other words, these recommendations encourage people to cultivate positive conceptions about dementia, and countries throughout the world are being asked to create policies that deepen understanding and awareness of the condition.
Person-Centred Care & Stigma
A positive keyword for dementia understanding and awareness is ‘person-centred care’, and a negative keyword is ‘stigma’. The former is a concept proposed in the 1990s by Dr Tom Kitwood of the University of Bradford, England, which advocates for a reimagining of our conception and perception of dementia, based primarily on traditional medical models of the condition, and instead emphasizes respect of the ‘personhood’ of people with dementia, a quality encompassing the entirety of their personality. Based on this concept of ‘person-centeredness’, Dr Kitwood listed five simple items as the emotional needs of a people with dementia: comfort, identity, occupation, inclusion, and attachment [3]. Brooker lists the four elements of person-centered care: valuing people (acknowledging the worth and value of a person’s existence), individualized care (respecting a person’s individuality), personal perspective (looking at the world from that person’s perspective), and social environment (providing a social environment to support the dementia-affected individual) [4]. Person-centredness goes beyond the medical/caregiving setting and is a concept useful for broadly deepening the understanding of dementia; it serves as a base for helping community individuals understand the lives and circumstances of people with dementia.
On the other hand, one of the primary factors hindering understanding of dementia is ‘stigma’. Byrne describes stigma as a discriminatory attitude toward or negative outlook on the conspicuous or unusual characteristics or traits of individuals [5]. The World Alzheimer Report 2019 cites the existence of stigmas as a major obstacle to both the provision of dementia-related information to those that seek it and the delivery of care and support to those that need it [2]. In the 2013 ‘G8dementia Summit’, the 11th item of the Global Action against Dementia agenda was the strengthening of efforts to lessen stigma towards dementia [6]. Kudo has conducted analyses of stigmas toward people with dementia in Japan and pointed out that when it comes to supporting them, their surrounding environment—especially their relationships with other individuals—is particularly important, and that stigma serves as an obstacle to early community detection of and intervention for people with dementia [7]. In the same paper, Kudo lists behavioural impairment among people with dementia, lack of knowledge of the condition itself, and anxieties about one’s own future condition as factors connected to dementia-related stigma. Removing these stigmas is not an easy task. Since they are often rooted in the history and culture of a nation or region, rather than proposing sweeping policies to counteract dementia-related stigma, the idea of stigma reduction itself should be hoisted as a global directive, and communities should work at the local level to encourage and deepen dementia awareness.
Hypothesis and Study Purpose
The two opposing concepts described above represent the opposite ends of the spectrum upon which our conceptions of people with dementia as an illness and our attitudes and expectations when confronting the condition lie. Philipson’s research team at Wollongong University has created a scale to holistically capture individuals’ stigmas toward dementia, which are classified into the following three categories: Isolation and avoidance of individuals with dementia, Positive perceptions of people with dementia, and Conceptions of oneself if one were to develop dementia; this scale reveals that both positive and negative aspects are involved in conceptions of condition [8]. Further, Philipson et al. (2014) targeted 616 people in Australia to derive four latent concepts that comprise conceptions of dementia in the Australian public: Avoidance, Fear of labelling, Fear of discrimination, and Person-centredness [9]. Thus, scales meant to measure stigma toward dementia and the results of analyses of latent factors have revealed that person-centredness and stigma are key factors affecting dementia understanding. We can, therefore, hypothesize that in Japan too, conceptions of people with dementia are made up of these sorts of positive and negative elements.
In 2019, the Alzheimer’s Association Japan (AAJ) carried out a ‘Survey of Feelings of People with Dementia and their Families, Care Status, and Public Attitudes towards Dementia’. In this study, we used the results of the “Survey of General Public Attitudes toward Dementia,” which was part of that survey, to conduct our analysis. As we test the aforementioned hypothesis, the objective of this study is to clarify the conceptions of people with dementia and to ascertain how existing initiatives and social resources affect dementia understanding and awareness among the general public.
Materials and Methods
The details of the attitude survey (questionnaire format) used in this study are provided below.
Questionnaire Survey Procedure
With the cooperation of AAJ chapters in the 47 administrative districts of Japan, the survey was carried out by targeting attendees and participants of public events held by each chapter, including lectures, university festivals, community events, elderly persons’ clubs, and dementia cafés. The survey was administered by AAJ staff members, and staff members/research collaborators periodically collected responses and sent them back to the main research office. Further, the survey was also uploaded to the AAJ website, distributed via a bulletin and related organizations, and implemented as a web survey. At lecture sessions, to prevent the content of lectures, etc., from influencing participant answers, the surveys were distributed and filled out prior to the event itself. These surveys were conducted between June 1 and November 15, 2019. The attitude survey conducted in this study was carried out anonymously, and no questions that would allow anyone to ascertain the identity of the respondent were set forth. Respondents were provided with an explanation of the objectives behind the survey and were told that the survey itself and analyses of the results would be exhibited to the country and the public and that responding to the survey would be deemed to provide consent to participate. This study was carried out with the approval of the Alzheimer’s Association Japan’s Ethics Committee (approval no. 2019-2003). The authors declare no conflicts of interest.
Content of Attitude Survey
The attitude survey polled respondents on their basic attributes (age, sex, place of residence, occupation), connections with people with dementia, conceptions of people with dementia (18 items), and use and knowledge of social resources (dementia supporter training courses, long-term care insurance, dementia cafés, and AAJ). The 18-item questionnaire on conceptions of people with dementia was formulated after referencing similar material by the Cabinet Office [10], Saitama Prefecture [11], Sugihara [12], Hirotani [13], and Yamada [14] (Table 1). Participants were asked to respond to the following question items using a 4-point scale (1. Agree 2. Somewhat agree 3. Somewhat disagree 4. Disagree).
Table 1: 18 Questions on Conceptions of People with Dementia.
Analysis
A total of 12,410 individuals responded to the questionnaire (556 completed it online). Of these, 10,485 individuals responded to all 18 items regarding conceptions of people with dementia. These 10,485 responses were, therefore, used as the analysis set for this study. In this study, the results of our attitude survey of conceptions of people with dementia were analysed via exploratory factor analysis and tests of mean differences. First, reverse-coded items for each of the 18 question items regarding conceptions of dementia were created, after which exploratory factor analysis (main factor method/Promax rotation) was carried out. At that time, items whose factor communality fell below 0.3, were excluded from the analysis. Next, extracted factor loadings were used to group and name questionnaire items, and Cronbach’s α coefficients were calculated to examine reliability (values ≥ 0.70, indicating high internal validity). The validity of the factor analysis was confirmed by Kaiser-Meyer-Olkin’s sample validity measure (determined to be valid at ≥ 0.5) and Bartlett’s sphere test.
Further, to examine the effects that use or knowledge of social resources for dementia understanding and experience interacting with people with dementia had on the factor scores of factors comprising positive conceptions of dementia (extracted via exploratory factor analysis), we separated respondents into groups. First, we separated them into two groups based on whether or not they had taken a dementia supporter training course, as determined by responses to a question (1. Yes, I have, 2. No, I have not), and compared the mean factor score of Factor I between these groups. Next, we separated respondents into a high-awareness and lowawareness group based on their answers (1. Informed, 2. Somewhat informed, 3. Not very informed, 4. Uninformed) to each of the three questions about knowledge of long-term care insurance, Knowledge of dementia cafés, and Knowledge of AAJ; Individuals who answered 1 or 2 were placed into the high-awareness group, and those who answered 3 or 4 were placed into the low-awareness group. After doing so, we once again compared the mean factor scores of factors related to positive conceptions about dementia between groups for each question. Finally, for question item which asked participants about their level of experience in interacting with people with dementia, we sorted respondents into three groups based on their answers (Experienced, Somewhat experienced, No experience) and compared the mean factor scores for Factor I between groups using a one-way analysis of variance. Statistical analyses were performed using the IBM SPSS Statistics Ver. 27.01 for Macintosh.
Results
The results of the attributes (age, gender, occupation) of the 10,485 analysed respondents are shown in (Table 2). The results of this survey tended to show a high percentage of pensioner and housewife/house husband due to the relatively high age range of the respondents, as well as a relatively high number of respondents in the medical and welfare professions, and this is described as a limitation of the study below. The responses to questions regarding attendance at dementia supporter training courses, awareness of social resources related to dementia (long-term care insurance services, dementia cafés, and AAJ), and experience with people with dementia are shown in (Table 3). The results of our exploratory factor analysis of answers to questions regarding conceptions of people with dementia are shown in (Table 4). The four items whose communality fell below 0.3 during the factor analysis process were excluded. After extracting the factors for the remaining 14 items, four factors with initial eigenvalues greater than 1.0 were extracted (cumulative contribution rate 61.2%). The Cronbach’s α coefficient for these 14 items was 0.75, confirming their internal validity.
Table 2: 18 Questions on Conceptions of People with Dementia.
Table 3: 18 Questions on Conceptions of People with Dementia.
Table 4: Results of exploratory factor analysis on conceptions of people with dementia.
Note: Cronbach’s α coefficient for all items: 0.745 Factor extraction method: main factor method / Promax rotation ※ Indicates reverse-coded factors
The value for the Kaiser-Meyer-Olin sample validity test, which expresses the validity of the factor analysis, was 0.83, and the result of the Bartlett sphere test was p<0.00, demonstrating that the analysis was valid overall. Based on the nature of the question items comprising each factor, the following names were chosen – Factor I: ‘Person-centredness’, Factor II: ‘Behavioural and psychological symptoms of dementia’, Factor III: ‘Forgetfulness’, and Factor 4: ‘Unknown anxiety’. Next, we tested mean difference to determine whether the use/awareness of dementia-related social resources and experience interacting with people with dementia affected the factor score of Factor I, Person-centredness (hereafter referred to as PC score). In our analysis, the Levene test was performed to verify the homoscedasticity of each item. As a result, in this analysis, Welch’s t-test was adopted to compare the two groups (four items), and Welch’s test was also adopted for analysis of variance among the three groups (one item). First, a significant difference in mean PC score was observed between the two groups: Had and had not attended a dementia supporter training course. Significant differences were also observed for high- and low-awareness groups for long-term care insurance awareness, Dementia café awareness, and AAJ awareness. Finally, a one-way ANOVA test between the three groups divided by (5) level of experience with people with dementia also revealed significant differences. The results are presented in (Table 5).
Table 5: The effects of use/awareness of social resources and level of experience interacting with people with dementia have on PC score.
Note: *p<0.001
Discussion
Conceptions of People with Dementia
In this study, the first stage of our factor analysis revealed the compositional elements of conceptions of people with dementia in Japan. The factors extracted were as follows: Person-centeredness, Behavioral and psychological symptoms of dementia, Forgetfulness, and Unknown anxiety. The fact that our results resemble those of the analysis conducted by Philipson et al. insofar as ‘Personcenteredness’ was extracted as a latent factor in the positive understanding of dementia is of significant importance.
At the beginning of the ‘Future Directions for Policies on Dementia’ promulgated in 2012 by the Ministry of Health, Labor and Welfare, the history of cruel treatment of people with dementia, including ostracization and physical confinement, was outlined [15]. Furthermore, psychiatric hospitals and old-age homes have long served as receptacles for people with dementia. Miyazaki details how they have lived under horrible conditions and have been targets of discrimination [16]. However, in the 1980s, the acceptance of people with dementia into special nursing homes for the elderly began, and national qualifications for care workers and social workers who could play a central role in dementia care were developed. Since then, Alzheimer’s disease International has set a policy of eradicating stigma worldwide, and various national measures for understanding dementia have been taken in Japan as well.
The extraction of person-centeredness as the first among the latent factors that comprise conceptions of people with dementia is a sign that we are finally breaking away from our long history of treating people with dementia unfairly. We can believe it positively as a tolerant society that understands people with dementia is being fostered.
On the other hand, “II. Behavioural and psychological symptoms of dementia (BPSD)” and “III. Forgetfulness” factors were extracted, which means that negative conceptions of people with dementia persist. However, the fact that BPSD contributes to people’s conceptions of people with dementia is not entirely negative; it can be interpreted as a natural consequence of the nature of the illness. Memory impairment is the most emblematic of dementia symptoms, and it is medically correct to state that the BPSD interfere with and impede activities of daily living (ADL). It is important to realize that BPSD is the result of cognitive decline and other impairments caused by degeneration of neurons and cerebral vasculature and that they prevent individuals from properly interacting and engaging with their surroundings, forcing them into a state of confusion. Once we understand this, an attitude of acceptance (sympathetic attitude) can be achieved.
It is also interesting that ‘unknown anxiety’ exists as a latent factor in the conceptions of people with dementia. While this can be interpreted as a negative factor, but this can be seen as a negative factor, but it is also a result of the information confusion that has surfaced as Japan faces the social challenge of an aging population. In our highly advanced information-oriented society, most media sources depict ageing as a problem to be solved. Identifying correct information and determining what people needs to understand is particularly difficult in modern society, in particular, individuals that do not normally interact with elderly persons can have limited opportunities to experience dementia proximally, and negative conceptions pushed by media narratives take precedence. Ogawa holds that a deep understanding and acceptance of people with dementia are necessary for the realization of an inclusive society (a ‘dementia-friendly community’) [17], and it is not difficult to imagine how ‘unknown anxiety’ could serve as an obstacle to such a goal. We hope that it will eventually become commonplace for individuals to be fully informed of and understand how to properly interact with them.
Factors Affecting Positive Conceptions of Dementia
The second stage of our factor analysis involved using tests of mean difference to analyse the effects of using and awareness of dementia-related resources and degree of experience interacting with people with dementia had on the PC score of Factor I as extracted by our exploratory analysis. All items polled at this stage of the questionnaire showed significant differences. First, we found that attending dementia supporter training courses improved the respondents’ PC scores. Dementia supporter training courses are actively promoted in the Outline for Dementia Policy Promotion (2019) to encourage understanding of dementia, but, at the local level, there is much debate about regional differences in session content and the actual impact of the sessions themselves. While we will not touch upon the content of these courses here, we hope for further expansion of efforts to promote education for dementia understanding and empathy among individuals who live near people with dementia.
Awareness of long-term care insurance, dementia cafés, and AAJ also raised PC scores. The fundamental principle underlying long-term care insurance is not to simply serve the individual needing care or to attend to their needs, but to support their independence. This idea of supporting independence is similar to that of personhood as posited by Kitwood, and we can surmise that it should be possible for correct knowledge of long-term care insurance to improve PC scores. Participation in organizations that work with people with dementia and their families affords individuals opportunities to directly feel the difficulties that these individuals experience in their daily lives and the often invisible tribulations of a caregiving family. The best way to deepen one’s sympathetic understanding is to listen to the voices of affected persons and their families.
Significant differences were also observed in our tests of mean PC scores (analysis of variance) across the three groups of individuals sorted according to their level of experience in interacting with people with dementia (1. Experienced, 2. Somewhat experienced, 3. No experience). Even outside of the realm of interactions with them, repeated experiences of anything acclimate one to it (normalization). This is a concept that most of us are quite familiar with. The Outline for Dementia Policy Promotion explains ‘symbiosis’ as ‘allowing people with dementia to live with dignity and hope, even with their condition, and enabling all people to participate in society, regardless of whether or not they have dementia’. As we can see, encouraging understanding of dementia among the public and expanding opportunities for people to interact with people with dementia will foster a sense of personcentredness.
While determining how and when to set up these opportunities for both groups to interact with one another is a project for the future, unbiased information provision (education) that takes place before stigmas can take hold is necessary. We believe that the findings obtained through this study will be important for future policy considerations for promoting dementia understanding and awareness. Changing the stigmas in people’s hearts to positive conceptions will undoubtedly lead to the early discovery of dementia and the realization of warm, personable care environments. Therefore, it will be necessary to continue to examine the meaning and impact of existing measures, such as dementia supporter training courses, and awareness-raising activities for understanding dementia in society in Japan. In addition, greater use of social resources aimed at dementia awareness or expanded educational efforts to teach individuals about people with dementia will help us understand the condition as one that is very proximal to all members of society, and will help grow a society rich in personcenteredness. Against such a backdrop, people with dementia will also have more opportunities to enter and engage with society, thereby growing person-centredness of people further. To truly realize a society of symbiosis with dementia, we must work to create a positive cycle that heightens our levels of person-centredness.
Limitations of this Study and Future Issues
The data we analysed in this study was based on a survey conducted at events where the elderly was relatively likely to participate, and some of the responses included those from medical and welfare professionals. Therefore, there was a possibility that some of the respondents already had an interest in dementia. Future research needs to understand the views of those who do not have preconceived notions about dementia in order to further explore the reality of stigma against people with dementia. In addition, since this study is a cross-sectional study, we cannot deny that there is a reverse causal relationship between the use and knowledge of social resources for dementia understanding and experience interacting with people with dementia raised PC scores. These points will be mentioned as limitations of this study at the end.
Acknowledgment
This paper analyses the results of the ‘Survey of Feelings of People with Dementia and their Families, Care Status, and Public Attitudes towards Dementia” conducted by the Health Promotion Project for the Elderly subsidy. We would like to express our deepest appreciation to the Alzheimer’s Association Japan main office, administrative office, and all employees of the branch offices that made this research possible. We would also like to extend our deep gratitude to everyone who answered the questionnaire.
Severe Acute Respiratory Syndrome Coronavirus 2(SARS-CoV-2)
i. SARS-CoV-2 is a positive-stranded RNA virus with envelope, a kind of a ‘Beta Corona Virus’. ii. It is speculated that its RNA sequence and that of the bat coronavirus are more than 80% similar. There is a strong theory that the pangolin acted as an intermediate between bats and humans.
Infection Route of COVID-19
i. Although it is estimated that human-to-human transmission through droplets is the primary route of transmission, a number of research results suggesting the possibility of airborne transmission have recently been published. ii. Although there are reports that SARS-CoV-2 was cultured in secretions such as feces or urine, it is not clear whether transmission through feces or urine can actually occur.
Infectivity of COVID-19
i. Summarizing the results of the studies which have so far been conducted, it seems that COVID-19 patients become contagious 2-3 days before the onset of symptoms. Infectivity usually lasts 5-7days after which it decreases.
Clinical Symptoms and Complications of COVID-19 Disease
i. Asymptomatic (50%), mild-to-moderate (40%), severe (10%) including respiratory failure. ii. Cough (50%), high fever (40%: 38°C or higher), headache (35%), dyspnea (30%), sore throat (20%), diarrhea (20%), nausea and vomiting (15%). iii. Other symptoms include loss of smell, loss of taste, fatigue, decreased appetite, hemoptysis, dizziness, runny nose, nasal congestion, chest pain, conjunctivitis, skin changes, etc. iv. Respiratory Complications: Lung fibrosis due to ARDS and pneumonia v. Cardiovascular Complications: Elevated blood pressure, acute myocardial injury, arrhythmia, myocarditis, heart failure, acute coronary syndrome, atherosclerotic event and venous thromboembolism vi. Acute Kidney Injury: Acute kidney injury due to high fever and dehydration and poor oral intake vii. Gastrointestinal Complications: poor oral intake, indigestion, diarrhea, nausea and vomiting, elevated hepatobiliary function parameters and pancreatic enzyme levels. viii. Cytokine Release Syndrome: ARDS, sepsis, DIC, multiple organ failure pattern ix. Nervous system-related symptoms and complications: Ischemic stroke, encephalitis, meningitis, impaired consciousness, Ataxia, convulsions, neuralgia.
COVID -19 Disease Patterns and Severity Risk Factors in Patients with Pre-Existing Diseases
i. Elderly patients with many underlying diseases are considered to have a high mortality rate because they cannot endure the symptoms and clinical manifestations itself of COVID-19 (high fever, high blood pressure, dehydration, breathing difficulty, thromboembolic events etc.). ii. Patients with pre-existing diseases such as high blood pressure, diabetes, hyperlipidemia generally suffer of a worsening of these diseases which then become difficult to control and require a higher medication. iii. In many instances patients develop newly diagnosed disease in the course of their COVID-19 infection, such as high blood pressure, diabetes, hyperlipidemia, which need to be continually followed up even after the patients recovers from COVID-19. iv. Another chronic underlying diseases that are well controlled (solid cancers, hematologic diseases, autoimmune diseases, etc.) do not have much influence on the conversion of COVID-19 to severe form. v. Obesity is a risk factor for severe respiratory failure regardless of age or underlying disease.
Clinical Course and Treatment of COVID-19 Disease
i. Each person has a different incubation period (7-10 days) depending on the individual’s immunity, the duration of the illness and the transition period of the corona virus test to negative (14-21 days). The clinical features and complications experienced by each person are different. ii. Continued intake of medications to control existing chronic diseases. iii. Popular treatment (fluid treatment, antibiotic treatment, antipyretic analgesic, and anti-inflammatory drugs, etc.) for symptom relief and normalization of test values, control of abnormal findings such as high fever, cough, sputum and pain by public medications is also helpful to overcome mild to moderate COVID-19 disease. iv. Monoclonal Antibody (Regdanvimab) is effective in preventing progression to severe disease pattern when administered within 7 days of a diagnosed pneumonia (by CT scan) for patients under 60 years and in any case for patients older than 60 even when oxygen saturation is maintained above 95%. v. The antiviral drug(Veklury) has been proven effective when administered as early as possible in case of pneumonia(confirmation by CT scan) and an oxygen saturation level below 94%.
The current study is an urgent warning on the Earth Day 2020 to prevent the blast of the COVID-19 pandemic to apocalypse. It is shown that the pandemic equations become unstable at reproduction numbers above 3.5, which could reflect in a chaotic catastrophe. There are many complex models describing pandemic kinetics [1,2]. In the current study we propose as chemists a minimalistic model based on chemical kinetics. Such type of equations describes different phenomena due to the universality of non-equilibrium thermodynamics developed by Onsager [3]. If X(t) is the fraction of infected people, its temporal dynamics will obey, the following nonlinear evolutionary equation
The first term on the right-hand side describes transfer of coronavirus from infected to healthy people with a characteristic frequency ϖ . Obviously, it corresponds to a second-order chemical reaction, since there are two different sets of people. Meetings among healthy or infected people do not affect the infection rate. The other relaxational term in Eq. (1) is due to either recovery or death of infected people and τ is the mean lifetime of infection. The favorite solution of Eq. (1) is but there is another stationary solution , which could be high at large reproduction number R =ϖτ . The deterministic logistic function is the solution of Eq. (1), which tends at large time to the healthy if or the pandemic if . The maximal infection rate appears in the meddle at . One can recognize in Eq. (1) the well-known SIS model from epidemiology.
A peculiarity of the nonlinear Eq. (1) is the chaotic behavior. Introducing the dimensionless time , being the natural scale of the infection evolution, Eq. (1) can be rewritten as
The discreetness of the society requires to be expressed by a finite difference and in this case Eq. (2) reduces straightforward to the standard logistic map [4,5]
The bifurcation diagram of the map (3) shows at Figure 1 that the pandemic solution is unique in the range 1≤ R ≤ 3.
Figure 1: The stationary fraction of infected people as a function of the reproduction number.
At larger reproduction number R > 3 a bifurcation hierarchy takes place [6]. Any bifurcation indicates oscillations between healthy-rich and infected-rich states, and this could trigger social segregation and confrontation. The onset of deterministic chaos at R > 3.5 marks the beginning of a cascade of chaotic apocalypses with unpredictable stochastic behavior. An unforeseen salvation is, however, that according to Figure 1 commensurable probabilities hold for the End ( X =1) and a new Beginning ( X = 0 ) at R = 4 . Though Einstein did not believe that God plays dice with the Universe, this would be the case here, because the logistic map has no solution at R > 4 .
Conclusion
The present study aims either educational or scientific goals. The used standard mathematical apparatus is well known in the classical theory of the chaotic systems and the paper is a useful demonstration how it could be applied to important living systems as well. The main contribution to science is the application to epidemiology. The traditional pandemic studies try to solve complex systems of nonlinear differential equations. Outstanding scientists have developed sophisticated models for precise predictions of pandemic but they never considered the bifurcation dynamics of their models. Indeed, the described SIS model is too simple to forecast the exact evolution of the COVID pandemic but we just wanted to stress that any epidemic model is non- linear, due to the infection spreading step, and this can result in a chaotic behavior. In conclusion, to fight effectively with the coronavirus epidemy people should try to reduce the reproduction number R =ϖτ either by suppressing ϖ via social distancing, masks and immunization, for instance, or by decreasing τ via advanced medical care. In any case R should be capped below 3.5 to prevent chaotic disasters. Of course, the present minimalistic model is oversimplified and its numerical predictions could be far from the reality. However, the exact models are even more nonlinear, which presumes a more complex chaotic behavior. But the World knew already that an apocalyptic pandemic was coming [7].
Acknowledgment
The author is thankful to Dr. V. Tonchev for inspiring discussions and grateful to Dr. A. Fauci and Dr. R.W. Eisinger for encouragement. Baron May of Oxford passed away at the day of the first publication of the paper online, R.I.P. Robert M. May [4].
Epidemiology of Life-Threatening Disease and Inflammation
Opinion
Various life-threatening diseases were studied in this analysis of epidemiology [1]. Diabetes, allergy and associated diseases, arthritis, metabolic diseases, kidney disease and infection, inflammatory bowel disease and infection are covered here for epidemiology study and analysis. Diabetes, roughly 463 million people living with diabetes worldwide [2] and diabetes caused 4.2 million deaths [3]. According to the predictions, over 700 million people will be affected by diabetes by 2045 worldwide [3]. According to the survey of the National Diabetes Statistics Report, US, in 2018, more than 26.9 million people are suffering from it, and about 8.2% of the US population facing complications because of it [4]. Diabetes is not infectious and is underlined as a chronic inflammatory disease having several complications. The understanding of the emerging role of inflammation in its pathophysiology and allied metabolic disorders will be helpful. It was suggested that by controlling or treating inflammation, the prevention and control of diabetes can be possible. Several scientific observations explore the link between high levels of inflammation and the progression of type 2 diabetes. Elucidation of inflammatory pathways is a good strategy for developing medical remedies for the prevention and controlling of diabetes and associated complications. The severity of coronavirus disease 2019 (COVID-19) infection is higher in those patients who are already suffering from diabetes mellitus and it is one more complication of it. Arthritis, a large number of the population affected by rheumatoid arthritis and it is approximately 350 million in the world and 120 million people in European [5]. In the US, nearly 54.4 million people out of 22.7 % of the population being affected in 2015 by it [6]. According to an estimation, a large number of patients are affected by rheumatoid arthritis and it will exceed up to 130 million individuals by 2050 [7]. Arthritis has a close association with inflammation. At some times, the immune system triggers an inflammatory response, no reaction from the body, then these physiological complications are notified as autoimmune diseases. Arthritis, which is initiated by inflammation, affects joints, was further classified into different category i.e., rheumatoid arthritis, psoriatic arthritis, gouty arthritis, and systemic lupus erythematosus. Allergy and associated diseases: The occurrence of allergic diseases is frequently growing worldwide. The understanding of the multifactorial etiology of these diseases is interesting. Several allergic illnesses including asthma, allergic conjunctivitis, atopic dermatitis, and allergic rhinitis share similar risk factors. Around 300 million patients have been suffered from asthma worldwide and will be around 100 million by 2025 [8]. In the United States affecting more than 50 million people are affected by allergy-induced diseases every year [9]. In Asia, this disease affects 27% overall population in South Korea and near about 32% in the United Arab Emirates [10]. One of the diseases initiated due to allergy, (asthma) affects more than 24 million people in the United States, including more than 6 million children. Moreover, allergic diseases, such as anaphylaxis, asthma, hay fever, and eczema now afflict roughly 25% of people in the developed world [11]. Therefore, clinicians are trying their best to expose the epidemiological routes of atopic disease and associated factors to design new strategies for effective treatment and prevention for putting into practice. In allergic diseases, insistent or repetitive exposure to allergens present in the environment, consequences in chronic allergic inflammation. Thus, understanding of the concerned features and consequences of acute and chronic allergic inflammation, and especially, when mast cells initiate several characteristics of various routes and paths of immunological reactivity. It was evident that the influences of environmental exposures, numerous environmental variations, alternations in the features of microbial, and environmental exposure to numerous pollutants. Metabolic diseases, about 54 metabolic disorders considered for clinical and public health significance, such as osteopenia, mild-moderate hypovitaminosis D, impaired glucose tolerance, obesity, metabolic syndrome, erectile dysfunction, diabetes mellitus, impaired fasting glucose, osteoporosis, dyslipidaemia and thyroiditis [12]. According to the physiology of a few diseases were observed in the minimum possible, including pituitary adenomas, adrenocortical carcinoma, and pheochromocytoma. The possibilities of detection of disorders such as hyperparathyroidism and thyroid were in a higher range and the prospects of their incidences are more frequent in female patients. Many metabolic diseases originate from the abnormal features and functioning of the pituitary, adrenal, and gonadal. Several metabolic disorders such as obesity, atherosclerosis, and type 2 diabetes underlined as lipid storage disorders and have a concern with nutrition. The role of chronic inflammation in the initiation, propagation, and expansion of metabolic disorders are deeply examined and outputs confirmed its title role in their beginning. Recently, transcription factor NF-κB was specified as one of the key reasons for the progression of these diseases, and this evidence confirmed the involvement of inflammation in the etiology of metabolic disorders. Inflammatory bowel disease and infection, according to an estimate of the U.S. Centers for Disease Control and Prevention, more than 3 million people in the United States are affected by inflammatory bowel disease (IBD) [13]. Moreover, Crohn’s and the Colitis Foundation of America assessed the situation and reported that nearly 1.6 million patients in the United States have IBD. Ulcerative colitis (UC) and Crohn’s disease identified as inflammatory bowel disease. Further, Crohn’s disease has four types of it, including Ileocolitis or Ileoceceal Crohn’s disease, Ileitis, Gastroduodenal Crohn’s disease, Jejunoileitis, and Crohn’s (granulomatous) colitis. IBD is an immune-mediated disease, which persisted in the gastrointestinal tract. According to the evidence of epidemiological research, obesity and obesity-associated metabolic syndrome triggered IBD. The predicted treatment methodology can be applied for treating chronic inflammatory bowel diseases by supporting immunosuppression, but in some cases, infectious complications make it worse. Numerous clinical observations have identified the role of infection in the initiation and progression of inflammatory bowel disease, and after that, the clinical suggestions were illustrated for inhibiting bacterial intestinal load. IBD is a type of chronic intestinal inflammation and is identified as a group of autoimmune diseases and host-microbial interactions are its key initiators. The persistent inflammation easily induced Crohn’s disease and ulcerative colitis. The patient who suffered from IBD experienced abdominal symptoms, including diarrhea, vomiting, abdominal pain, and bloody stools. Kidney disease and infection, chronic kidney diseases are leading health problems worldwide and are detected commonly. According to the data analysis of the global level, CKD has an estimated prevalence is 13.4% (11.7-15.1%), In the US, about 15% of adults, or nearly 37 million people, have chronic kidney disease. Insistent, inflammation is underlined as an important factor, which initiates CKD that plays a unique role in its pathophysiology. Inflammation of the kidney is also known as nephritis. In Greek terminology, nephron defined as “of the kidney” and itis represents “inflammation.” Various causes are underlined that initiate nephritises include autoimmune disorders, infections, and toxins in the body. Various factors i.e., pro-inflammatory cytokines, oxidative stress, AGEs, homocysteine, and acidosis, and their excess physical and chemical concentration and their decreased clearance directly influence the chronic inflammatory status, which further triggered the initiation of chronic kidney disease.
Acknowledgment
Author (Rajiv Kumar) gratefully acknowledges his younger brother Bitto for motivation.
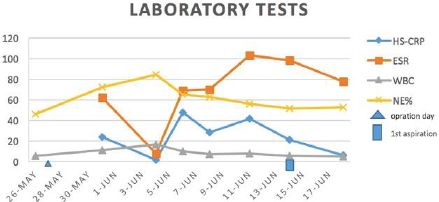
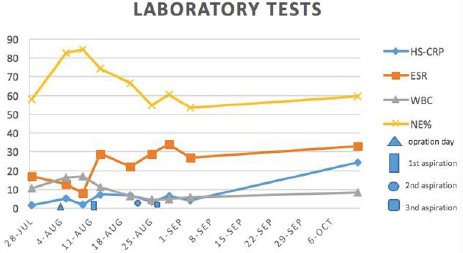
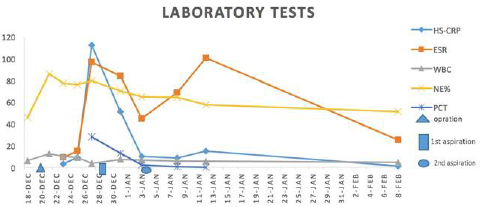
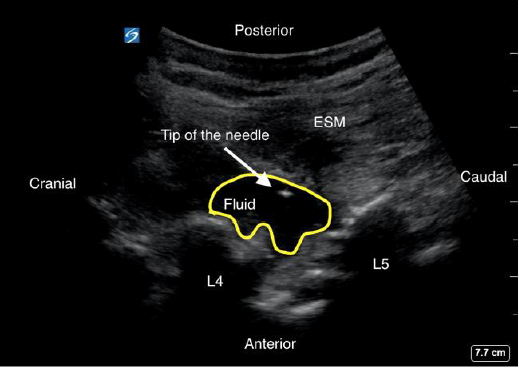

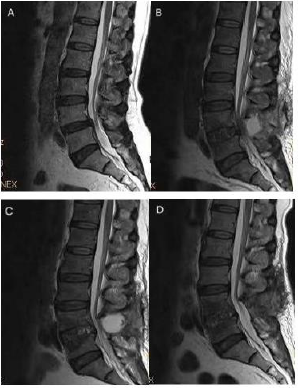



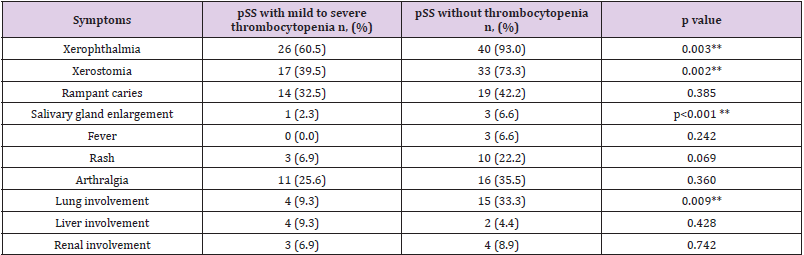
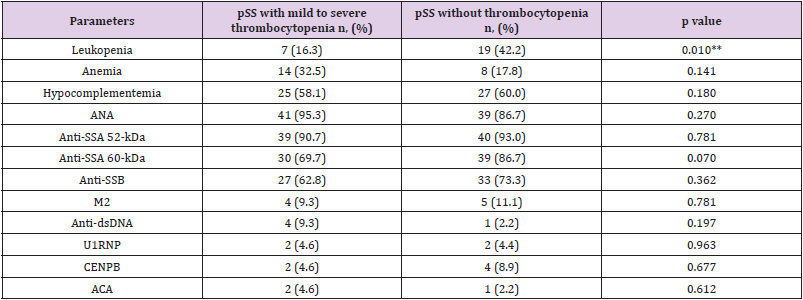
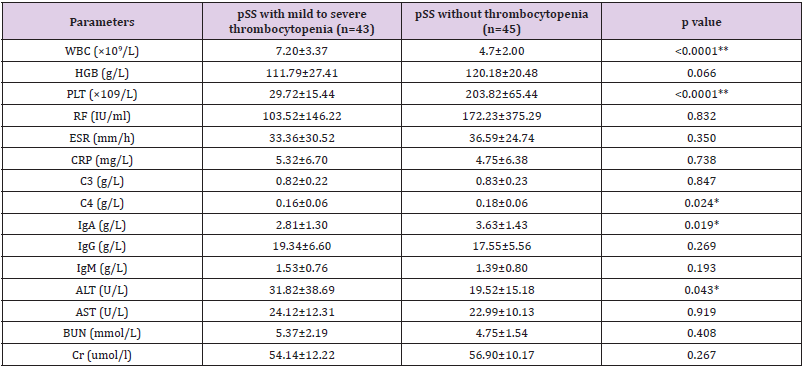
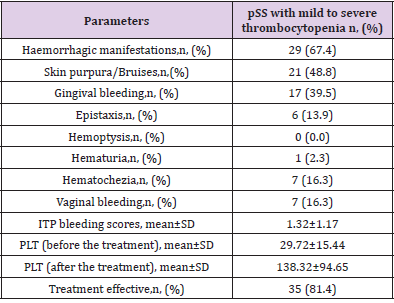
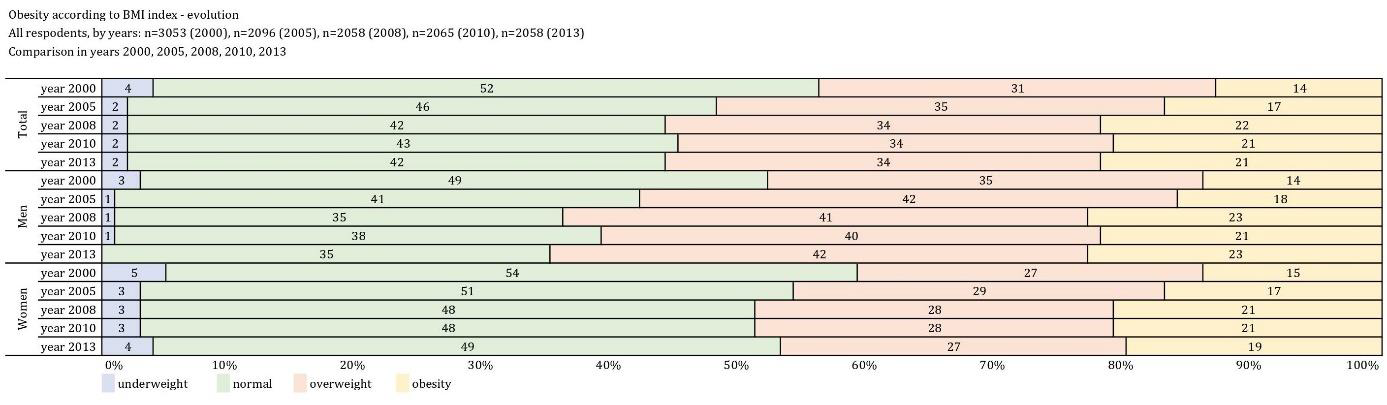
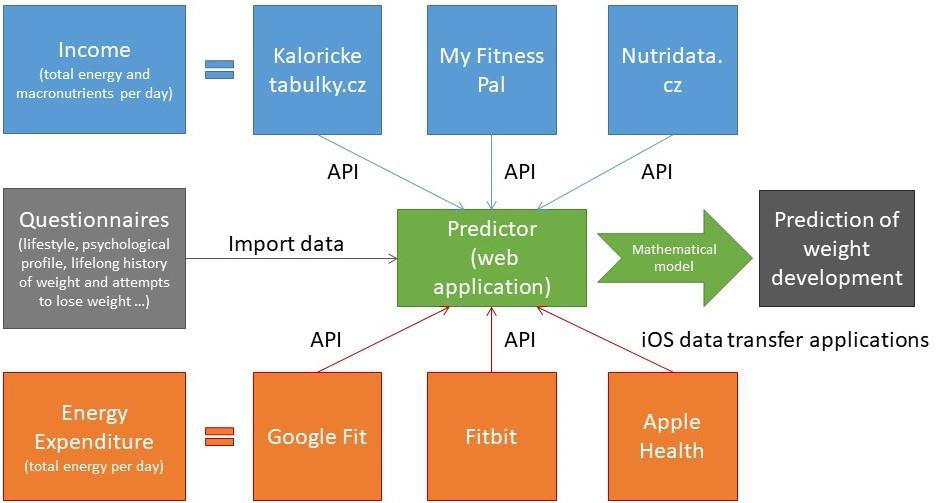

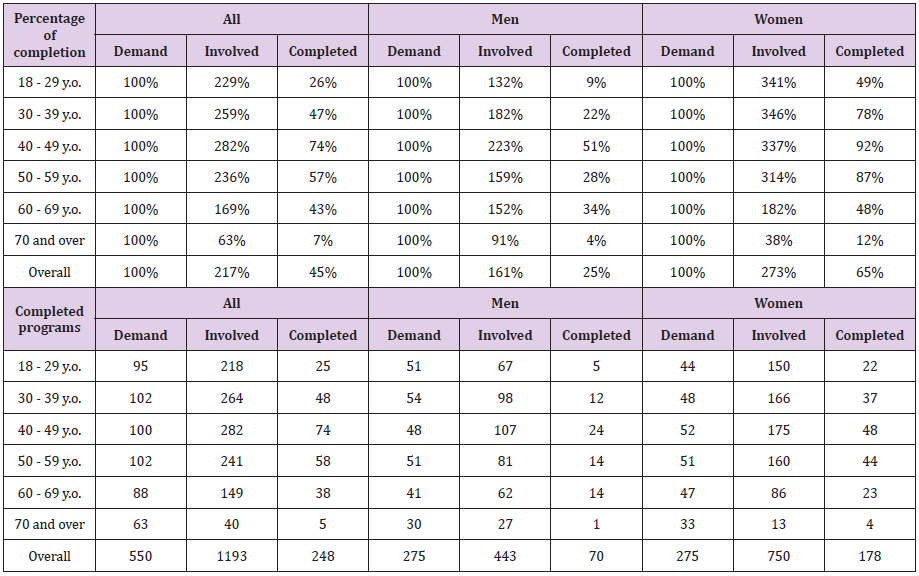
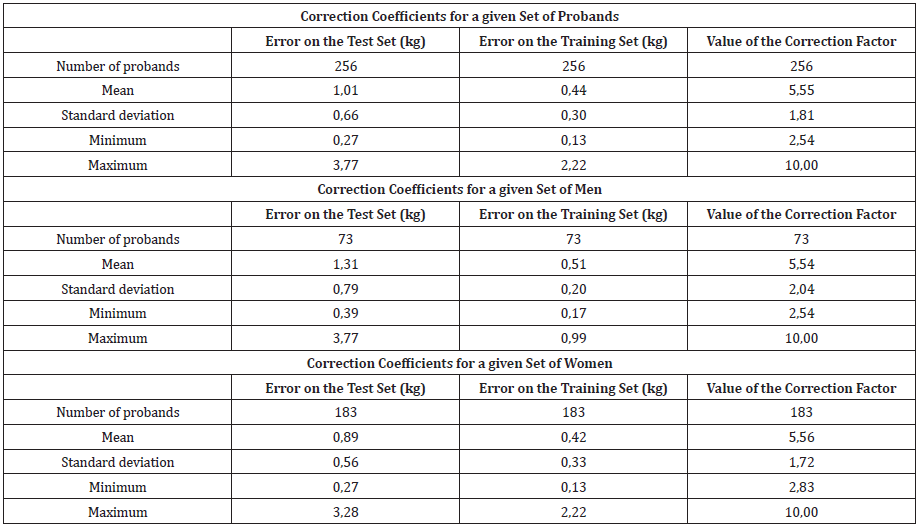

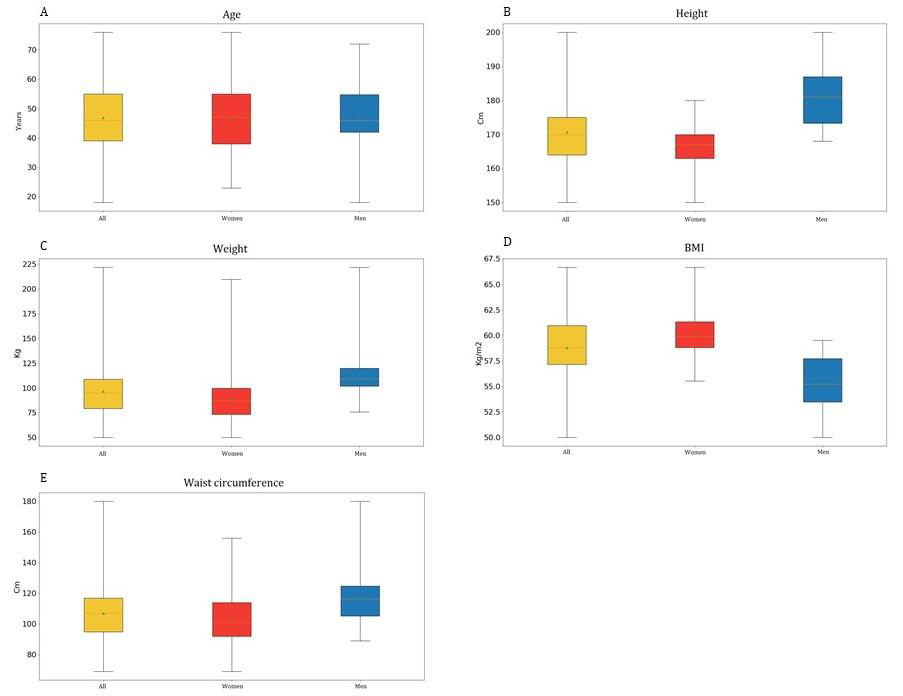
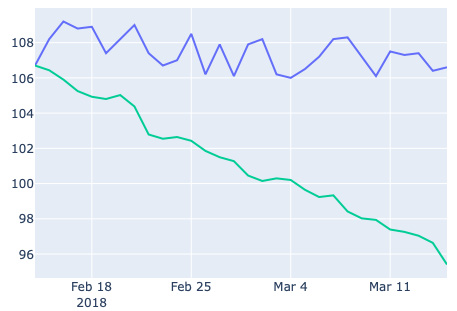
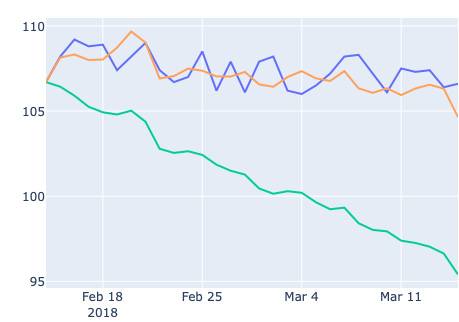
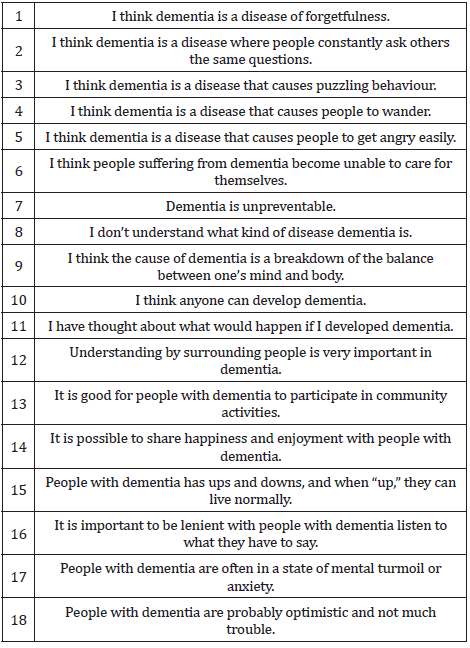
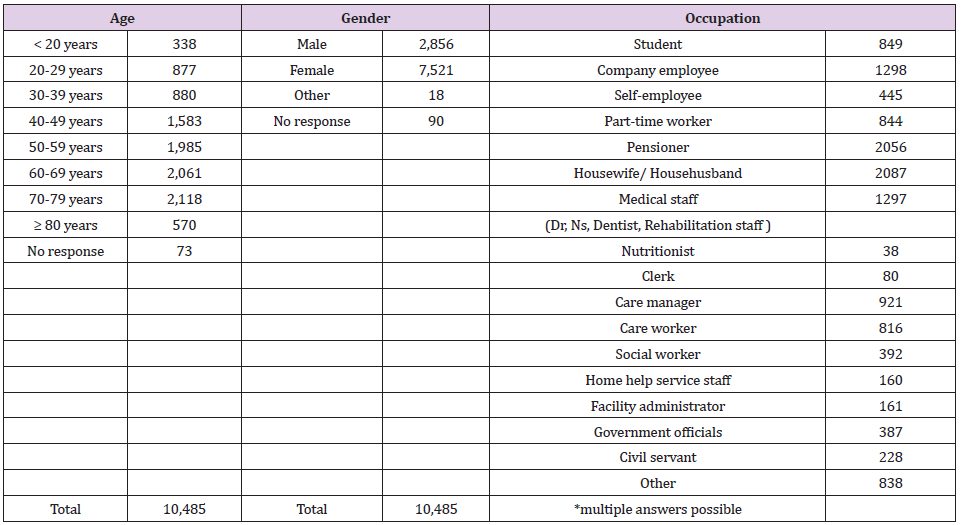
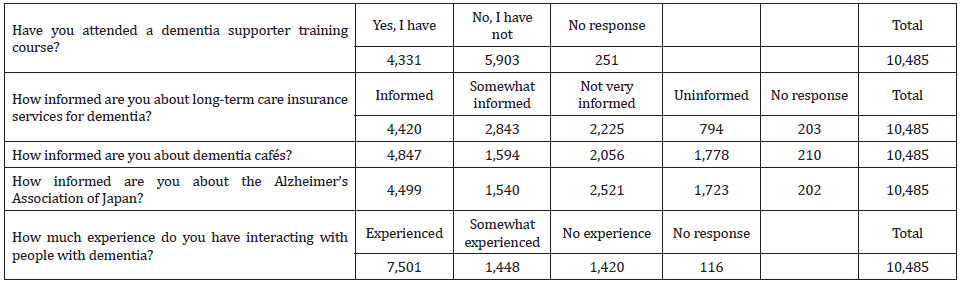
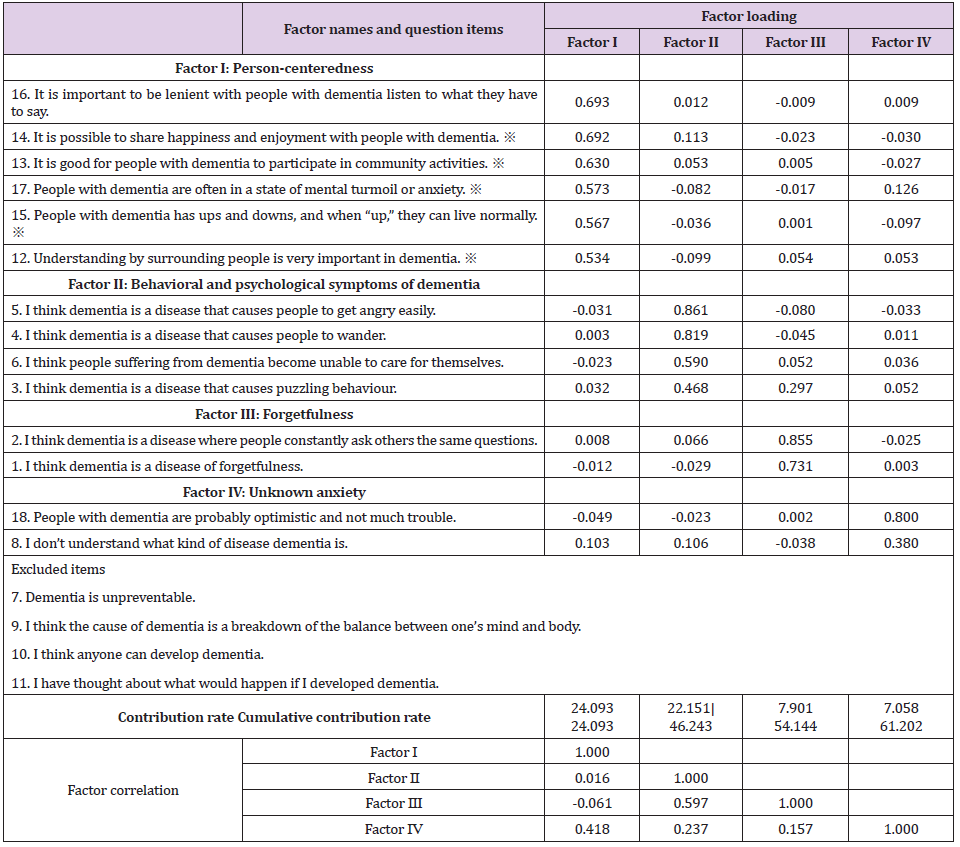
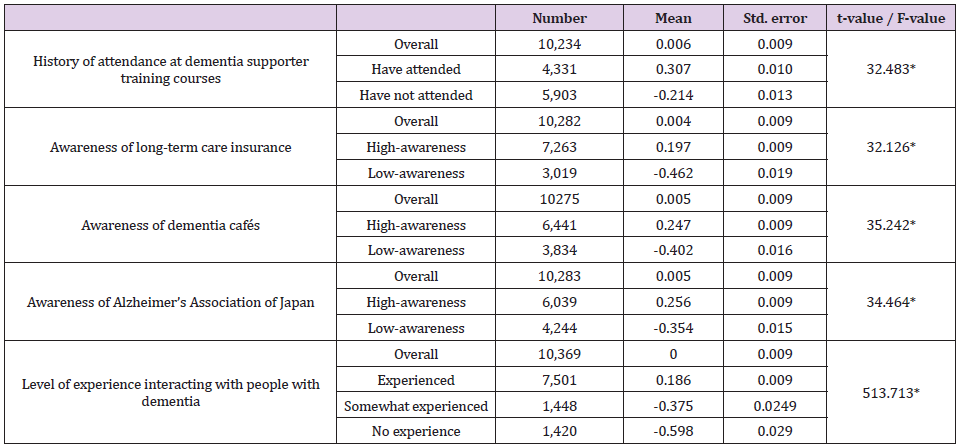

 but there is another stationary solution
but there is another stationary solution  , which could be high at large reproduction number R =ϖτ . The deterministic logistic function is the solution of Eq. (1), which tends at large time to the healthy
, which could be high at large reproduction number R =ϖτ . The deterministic logistic function is the solution of Eq. (1), which tends at large time to the healthy  if
if  or the pandemic
or the pandemic  if
if  . The maximal infection rate appears in the meddle at
. The maximal infection rate appears in the meddle at  . One can recognize in Eq. (1) the well-known SIS model from epidemiology.
. One can recognize in Eq. (1) the well-known SIS model from epidemiology. , being the natural scale of the infection evolution, Eq. (1) can be rewritten as
, being the natural scale of the infection evolution, Eq. (1) can be rewritten as
 to be expressed by a finite difference and in this case Eq. (2) reduces straightforward to the standard logistic map [4,5]
to be expressed by a finite difference and in this case Eq. (2) reduces straightforward to the standard logistic map [4,5]
 is unique in the range 1≤ R ≤ 3.
is unique in the range 1≤ R ≤ 3.